Back to Journals » Journal of Inflammation Research » Volume 18
Therapeutic Effect of Brain Awakening and Mind Opening Acupuncture Combined with Simiao Pill on Mice with Benign Prostatic Hyperplasia
Authors Luo Z ![]() , Yang X, Zhang J, Zhang B, Zhao Q, Cui L, Bo H
, Yang X, Zhang J, Zhang B, Zhao Q, Cui L, Bo H
Received 5 July 2025
Accepted for publication 27 November 2025
Published 15 December 2025 Volume 2025:18 Pages 17663—17675
DOI https://doi.org/10.2147/JIR.S546797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Zhiyuan Luo,1,* Xiaomei Yang,2,* Jingting Zhang,1 Bingqian Zhang,1 Qingjie Zhao,2 Longtao Cui,3 Huajun Bo1
1Department of Acupuncture and Massage, Shanghai Fourth People’s Hospital, Tongji University, Shanghai, 200434, People’s Republic of China; 2State Key Laboratory of Discovery and Utilization of Functional Components in Traditional Chinese Medicine, Shanghai Frontiers Science Center for TCM Chemical Biology, Innovation Research Institute of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 3School of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Longtao Cui, School of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China, Email [email protected] Huajun Bo, Department of Acupuncture and Massage, Shanghai Fourth People’s Hospital, Tongji University, Shanghai, 200434, People’s Republic of China, Email [email protected]
Purpose: Benign prostatic hyperplasia (BPH) is a common condition in older men, but treatment is often associated with complications and high recurrence rates. Previous clinical studies have shown that Brain Awakening and Mind Opening (BAMO) acupuncture and Simiao Pill can improve lower urinary tract symptoms in patients with BPH. This study explores the potential mechanisms behind these treatment methods for BPH using a mice model.
Methods: Six-week-old ICR male mice were divided into 5 groups (n=10). The Mice were injected subcutaneously with TP (5mg/kg/d) / corn oil (equal volume) for 28 days to establish a BPH model and a control group. After successful modelling, the mice were treated with distilled water for 21 days, while the BAMO acupuncture group, the Simiao pill group, and the mixed group were treated accordingly (BAMO acupuncture at Neiguan (PC6), Sanyinjiao (SP6), and Guanyuan (CV4) acupoints for 30 minutes every other day, or Simiao pill once a day).
Results: BAMO acupuncture, Simiao pills, and their combination effectively reduced prostate hyperplasia in mice. The observed therapeutic effects likely involve multiple mechanisms: suppression of dihydrotestosterone (DHT) synthesis via reduced testosterone levels and downregulated SRD5A2 expression (P< 0.01), promotion of prostate cell apoptosis (indicated by an increased BAX/BCL-2 ratio, P< 0.05), and mitigation of inflammation through decreased levels of pro-inflammatory cytokines IL-6 and TNF-α (P< 0.05).
Conclusion: BAMO acupuncture and Simiao pill can restore normal prostate tissue structure in mice through multiple mechanisms: (1) reducing DHT production; (2) promoting apoptosis; (3) reducing inflammatory responses. Future studies could further investigate the hormonal regulation and apoptosis of BAMO acupuncture in mice.
Keywords: BAMO acupuncture, Simiao pill, BPH, mechanism study
Introduction
The Benign prostatic hyperplasia (BPH) is a widespread urological condition, affecting over 50% of men worldwide aged 60 years or older, and represents a major global health challenge. It is mainly manifested by lower urinary tract symptoms (LUTS), such as urinary frequency, urgency and difficulty urinating, which significantly reduce patients’ quality of life.1 Research indicates that its incidence correlates positively with age, with a high prevalence among men over fifty. Autopsy studies reveal a histological prevalence of BPH reaching 50–60% in men aged 60–69, rising to 80–90% in those over seventy.2 As the proportion of older individuals in the population continues to grow, BPH has garnered increasing attention.3 TCM therapeutic tools play an important role in the treatment of BPH. Chinese medicine compound treatment has the synergistic advantage of “Network-based multi-component, multi-target, multi-pathway interactions”.4 The efficacy of acupuncture in improving patients’ quality of life is widely recognized,5,6 and it demonstrates significant benefits in treating urinary retention caused by various conditions.7–9 The pathogenesis of BPH is still unclear. Currently, the theories that are more widely accepted include the androgen-estrogen synergy theory, the imbalance of cell proliferation and apoptosis theory, the inflammation-driven theory, the epithelial–mesenchymal cell interaction theory, and the neuroendocrine regulation theory.10–13 The treatment for BPH mainly consists of surgical treatment and drug therapy. Surgery is the most effective treatment for BPH, particularly in refractory or high-risk cases, but there are complications such as bleeding, urinary incontinence, erectile dysfunction, retrograde ejaculation, infection, and recurrence.14 The main forms of drug treatment include 5α-reductase inhibitors and α1-adrenergic receptor blockers. The combination of these two drugs is the preferred treatment option for BPH in clinical practice. However, α1-blockers can cause orthostatic hypotension, while 5α-reductase inhibitors can lead to adverse reactions such as sexual dysfunction, breast enlargement, and compressive pain.15
The animal models of benign prostatic hyperplasia (BPH) can be classified into several main types based on the modeling mechanism: spontaneous BPH models, sex hormone-induced models, inflammation-induced models, urogenital sinus (UGS)-induced models, deoxy noradrenaline (PE)-induced models, xenograft models, and transgenic/ knockout models.16 Among them, the spontaneous BPH model is the closest to the clinical pathological features because it can replicate the natural pathological process of the disease, such as in elderly chimpanzees17 and dog models.18 However, this model is difficult to obtain, and canine BPH compresses the rectum while human BPH with lower urinary tract symptoms, which are inconsistent.19,20 The sex hormone-induced model is currently the most widely used BPH model, with rats and mice as the main experimental animals. It induces hyperplasia by subcutaneous injection of testosterone propionate (TP) (dose 3–10mg/kg/d, for 21–35 days), and it can be divided into castration and non-castration subtypes. The castration model excludes the interference of endogenous hormones and make the model phenotype more stable and uniform,21 providing better conditions for the study of hormone-related molecular mechanisms;22 the non-castration model retains endogenous hormone secretion and can form a more realistic physiological environment similar to the “estrogen/androgen (E/T) imbalance” of elderly men.23 It can more realistically reproduce the pathological features of human BPH dominated by matrix hyperplasia and can better support the study of the “hormone-inflammation” synergistic pathogenic mechanism,24–26 but its homogeneity is poor due to fluctuations in endogenous testosterone levels in individual animals.25 Other models have specific research values.
Traditional Chinese medicine (TCM) offers a holistic approach rooted in centuries of clinical practice, emphasizing symptom alleviation with minimized adverse effects through multi-target regulatory mechanisms. BPH is classified as “essence and urine”, “urinary retention”, and “gonorrhoea” in TCM.27 For BPH, excess patterns should be treated with clearing heat, draining dampness, promoting qi movement, and dissipating blood stasis; deficiency patterns should be treated with warming and tonifying the spleen and kidney, assisting yang to transform qi, thereby promoting urination.28 Both the excess and deficiency patterns can achieve therapeutic effects by promoting qi movement and draining dampness. Simao Pill is composed of atractylodes, phellodendron, achyranthes, and coix Seed. Modern pharmacological studies have shown that the main active components of Simao Pill include adenosine, phellodendrine, mangnoflorine, β-ecdysterone, etc.29 The pharmacokinetic study on rats showed that the main components absorbed by Simao Pill in the gastrointestinal tract include berberine, berbamine, maeckenine, berbamine methyl ether, and berbescoside.30 Simao pill has the effects of anti-inflammation31 and antioxidation.32 Simiao pill is commonly used to treat rheumatoid arthritis and hyperuricemia. In urological conditions, it is primarily employed for chronic prostatitis, though its application in BPH has not been extensively studied. However, chronic prostatitis combined with its symptoms is thought to be attributed to the categories of “semen catarrh”, “gonorrhoea”, and “leucorrhoea”, which have certain commonalities with BPH.27 Modern medical development also believes that chronic prostatitis is an important factor in the development of prostatic hyperplasia, and prostatic hyperplasia can develop in combination with chronic prostatitis.33 Simiao pill can promote glandular tissue metabolism by improving microcirculation and dilating blood vessels, effectively inhibit tissue hyperplasia, reduce urethral pressure, and decrease urine reflux.34,35 Therefore, Simiao pill can be used to treat BPH, and this experiment will initially explore the mechanism of Simiao pill in treating BPH.
Acupuncture, as a unique therapeutic tool of Chinese medicine, can largely improve patients’ lower urinary tract symptoms and quality of life in the treatment of BPH. The BAMO acupuncture technique is based on regulating the spirit and opening the orifices to facilitate communication. By adding or subtracting specific points according to the condition, it achieves both disease differentiation and syndrome differentiation in treatment. The fundamental points include Neiguan (PC6), Sanyinjiao (SP6), and Guanyuan (CV4) as determined by the specific pathology. A survey study on acupuncture treatment for BPH has shown that Guanyuan (CV4) and Sanyinjiao (SP6) are commonly selected acupoints for managing this condition.33,36,37 It has been reported that Guanyuan (CV4) acupoint can treat urinary retention, yellowish urine, heat-induced dysuria, and five types of urinary disorders including stone-induced dysuria. Sanyinjiao (SP6), the convergence point of the spleen, kidney, and liver meridians in TCM, is clinically employed to harmonize these three meridians, invigorate qi, and regulate bladder function. Clinical studies demonstrate that stimulation of the Sanyinjiao (SP6) acupoint—located on the medial aspect of the ankle—effectively alleviates urinary retention in patients with diverse underlying pathologies. Acupuncture at the Sanyinjiao (SP6) acupoint reduces bladder pressure and ameliorates urinary retention in rats.38–40 Besides, although Neiguan (PC6) is not a commonly used acupoint for treating urinary system disorders, it can enhance analgesic effect,41 inhibit inflammation-mediated fibrosis,42 improve anxiety state43 and quality of life of patients.44 Many BPH patients experience frequent urination, urinary urgency, incomplete voiding, and increased nighttime urination, which significantly affect their emotional state and quality of life. All of these indicated that the selection of acupoints for the BAMO acupuncture technique is well-founded and demonstrates certain efficacy in treating BPH, though the underlying mechanism remains unclear.
Acupuncture does indeed demonstrate efficacy in the treatment of clinical diseases; however, its effectiveness remains questionable when compared to pharmacological interventions.45 Consequently, it is frequently combined with medication in the hope of achieving enhanced therapeutic outcomes.46–48
Therefore, this study aimed to observe the regulation by Simiao Pill, BAMO acupuncture (Guanyuan (CV4), Sanyinjiao (SP6), and Neiguan (PC6)), and their combined application to treat BPH and to further explore the mechanism by in vivo tests, which is helpful in elucidating the related transduction mechanism of BPH to provide a basis for clinical treatment.
Materials and Methods
Experimental Animals
Six-week-old ICR SPF male mice were obtained from Beijing Viton Lihua Laboratory Animal Company Limited (License Number: SCXK [Beijing] 2021–0011). The mice were housed in a specific pathogen-free (SPF) animal facility with a controlled temperature of (22±2) °C, humidity of (50±10) %, and a 12-h light/dark cycle. Five mice were placed per cage, with free access to standard chow and sterile water. For all invasive procedures requiring sedation or anesthesia, isoflurane was used in conjunction with an anesthesia machine (induction: 2–3% isoflurane with oxygen supplementation; maintenance: 1–1.5% isoflurane) to ensure stable anesthesia and minimize animal distress. At the end of the experiment, mice were euthanized by overdose of isoflurane inhalation (5% concentration with continuous oxygen supply) until respiratory and cardiac arrest. All animal experiments were conducted at the Laboratory Animal Centre of Shanghai University of Traditional Chinese Medicine, which holds a valid experimental permit (Permit Number: SYXK [Shanghai] 2020–0009). The experimental protocol was reviewed and approved by the Experimental Animal Ethics Committee of Shanghai University of Traditional Chinese Medicine (Approval Number: PZSHUTCM2503280009) and conducted in strict compliance with the ARRIVE Guidelines 2.0 and the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (NIH, USA), as well as the relevant regulations of the People’s Republic of China (Experimental Animal Administration Regulations, Decree No. 2 of the State Council).
Medications and Reagents
Simiao pill was obtained from Zixin (Jilin, China); testosterone propionate was obtained from Adamas (Shanghai, China); corn oil was obtained from Yuan Ye (Shanghai, China); general dihydrotestosterone ELISA kit (DHT), general testosterone ELISA kit (T), general estradiol (E2) ELISA kit, and ABplex mouse 3-plex custom panel were obtained from ABclonal (Wuhan, China); isoflurane was obtained from RWD (Shenzhen, China), BAX rabbit monoclonal antibody was obtained from ABclonal (A20227, 1:100, Wuhan, China) for IHC; BCL-2 rabbit monoclonal antibody was obtained from ABclonal (A19693, 1:100, Wuhan, China) for IHC; SRD5A2 rabbit polyclonal antibody was obtained from Bioss (bs-6700R, 1:100, Beijing, China) for IHC.
Mouse Modelling and Grouping
In this experiment, six-week-old SPF males ICR mice were acclimatised and reared for one week and then divided into 5 groups (n=10). Mice were injected subcutaneously with TP (5mg/kg/d) / corn oil (equal volume) for 28 days to establish a BPH model and a control group. The treatment groups, based on the BPH model, comprised the BAMO acupuncture group, the Simiao pill group, and the combined BAMO + Simiao pill group.
Drug Administration to Mice
The dose of Simiao pill in mice was 1.56 g/kg (human dose: six grams twice daily, converted proportionally to body surface area). Simiao pill was prepared as a 1.56 g/mL suspension solution in distilled water, and the mice were gavaged in equal doses according to their body weights, while the control and model groups were given distilled water for 21 consecutive days.
BAMO Acupuncture in Mice
Neiguan point (PC6): the inner side of the forelimb of mice, about 2 mm from the carpal joint between the radial-ulnar suture, 1.5 mm; Guanyuan point (CV4): about 10 mm below the navel of the mice, 3 mm; Sanyinjiao point (SP6): the tip of the inner ankle of the hind limb of the mice, about 5 mm directly above the tip of the hind limb, 3 mm. Prior to acupuncture, all mice were anaesthetised for two minutes using an anaesthesia machine before being placed in a mouse restraint device. Needling was performed at a frequency of once every other day, with the sequence being Sanyinjiao (SP6), Guanyuan (CV4), and Neiguan (PC6). Typically, mice awoke immediately upon insertion into the Neiguan (PC6) point. Needles were retained for 30 minutes, with mice in other groups similarly restrained for 30 minutes and BAMO+Simiao group received oral gavage followed by BAMO acupuncture treatment.
H&E Staining and Masson’s Staining
Mice prostate tissues were harvested 24 hours after the final drug administration. Post-fixation, tissues were processed for paraffin embedding and sectioned. Histological evaluation involved H&E staining, wherein sections were deparaffinized, rehydrated, stained with hematoxylin and eosin to differentiate cellular components, and subsequently dehydrated, cleared in xylene, and mounted. Additionally, Masson’s trichrome staining was performed, employing a sequential protocol with Weigert’s iron hematoxylin, acid fuchsin/ponceau S, phosphomolybdic acid, and aniline blue to specifically identify nuclei, cytoplasmic structures, non-collagenous elements, and collagen fibers, respectively, followed by dehydration, clearing, and mounting. Microscopic imaging of both H&E and Masson’s trichrome stained sections was conducted, with subsequent quantitative analysis performed using ImageJ software.
Immunohistochemical Staining
Mice prostate tissues were dissected and harvested 24 h after the final drug administration, carefully dissected, and processed for immunohistochemical (IHC) analysis. Paraffin-embedded tissue sections were dewaxed and rehydrated using a graded ethanol series, followed by antigen retrieval to unmask epitopes. Endogenous peroxidase activity was quenched by incubation with hydrogen peroxide, and nonspecific binding sites were blocked with serum. Sections were then incubated sequentially with primary antibodies (specific to the target antigen) and horseradish peroxidase (HRP)-conjugated secondary antibodies. 3,3′-Diaminobenzidine (DAB) was applied to visualize antibody–antigen complexes, and nuclei were counterstained with hematoxylin to enhance histological detail. After dehydration through an ethanol-xylene series, the sections were mounted with a resinous medium and imaged under microscope.
Enzyme-Linked Immunosorbent Assay
24 h after the final drug administration, blood samples were collected. Serum was isolated by centrifugation, diluted according to the manufacturer’s protocol, and analyzed using a competitive enzyme-linked immunosorbent assay (ELISA). Briefly, 50 μL of standard or diluted serum samples were loaded into pre-coated wells, followed by the addition of 50 μL of assay buffer and 50 μL of enzyme conjugate. After thorough mixing, the plate was incubated at 37°C for 1 h. Unbound components were removed by washing, and 100 μL of substrate solution was added to each well for 20 min at room temperature to initiate chromogenic development. The reaction was terminated with 50 μL of stop solution, and absorbance was immediately measured at 450 nm (primary wavelength) and 630 nm (reference wavelength) using a microplate reader.
Multiparameter Flow Cytometry
24 h following the final drug administration, blood samples were collected. Multiplex flow cytometry experiments were conducted in collaboration with ABclonal using the ABplex® Mouse 3-plex Custom Panel kit. Prior to formal analysis, pre-experimental conditions were optimized on the ABplex-100 multi-parameter flow cytometer in accordance with the manufacturer’s protocols. Once calibration and antibody titration were validated, the company performed formal experiments and provided raw datasets, including technical replicates, to facilitate subsequent data analysis.
Statistical Analyses
Statistical analysis was performed using R software to assess normality within groups and homogeneity of variance between groups. GraphPad Prism 9.0 software was employed for data plotting. All data are presented as mean ± standard error of the mean (SEM). Statistical analysis employed one-way analysis of variance (ANOVA). Statistical significance was defined as a P value < 0.05, denoted, respectively, as *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001.
Statistical analysis of epithelial thickness in mouse prostates via HE staining for each slide, six measurements were taken from distinct fields of view representing thin, medium, and thick sections respectively, with the mean calculated. These three field values constituted the statistical data for each slide. GraphPad Prism 9.0 software was employed for graphical representation and statistical significance testing. For IHC of mouse prostates, six images per group were selected showing no or minimal non-specific staining. Three random fields per image were analysed (non-specific staining was minimal; eosinophilic fluid within the prostatic lumina may undergo non-specific staining during IHC and required exclusion). Statistical analysis employed ImageJ software to perform colour deconvolution and optical density correction, followed by measurement of positive areas for relevant indicators. Data were then statistically analysed and plotted using GraphPad Prism 9.0 software.
Results
Inhibition Effect of Prostate Hyperplasia by BAMO Acupuncture and Simiao Pill
After 21 days therapy, mice’ seminal vesicles (a), prostates (b) and bladders (c) were harvested from control, model, BAMO acupuncture, Simiao pill and BAMO+Simiao groups. In the study, the physiological morphology of the prostate tissue in the model group exhibited significant enlargement (Figure 1A-a), the seminal vesicles of the drug-administered group and the model group mice showed atrophy (Figure 1A-b). Wet weight of the prostate and prostate index (PI) of mice in the model group was significantly higher than those in the control group. Compared with model group, BAMO acupuncture group, Simiao pill group and BAMO+Simiao group all showed a significant trend towards reduction (Figure 1B–D).
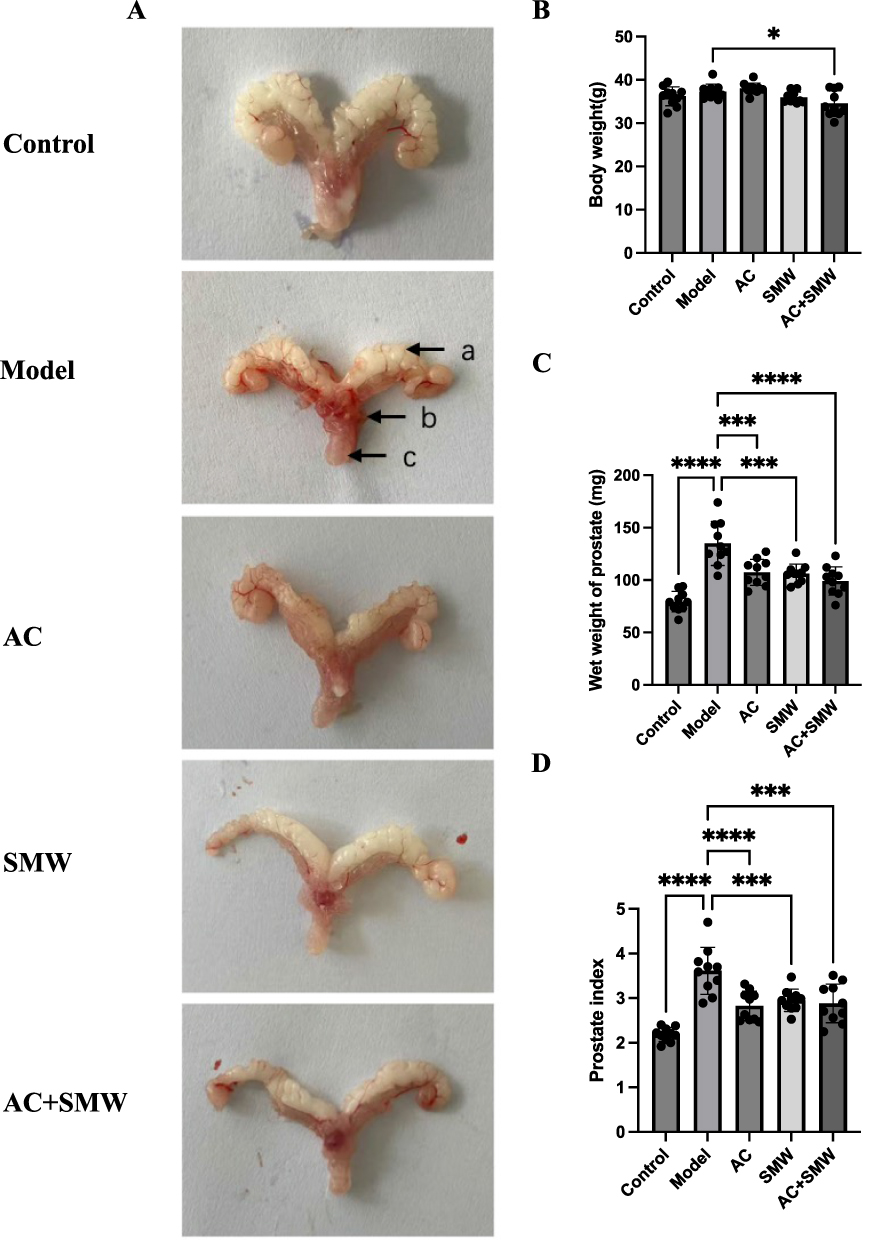 |
Figure 1 Effects of different groups on prostate in mice. (A) Physiological morphology of the mice (a: seminal vesicles; b: prostate; c: bladder). Control: control group (n=10); Model: model group (n=10); AC: BAMO acupuncture group (n=10); SMW: Simiao pill group (n=10); AC+SMW: BAMO Acupuncture+Simiao group (n=10). (B) Body weight of mice, *P<0.05 (n=10). (C) Wet weight of prostate in mice (n=10), ***P<0.001, ****P<0.0001. (D) Prostate index of mice (prostate wet weight (mg) / body weight (g) of the mice, n=10), **P<0.01, ***P<0.001, ****P<0.0001. |
Improvement of Prostate Histopathological Structure by BAMO Acupuncture and Simiao Pill
To further explore the effects of BAMO acupuncture and Simiao pill on histopathological structure for BPH therapy, H&E and Masson’s staining were applied for pathological analysis. The results of H&E staining of mice prostate tissues are displayed in Figure 2A. Compared to control group, the state of model group was changed. The thickness of epithelial cells in the field of view of the prostate tissue was increased to 160.57% of control values. Moreover, the epithelial cells were irregularly arranged, and most of the cells protruded inward in the form of ridges into the cavity of the alveoli. Eosinophilic substances in model group were seen to be reduced in the lumen of the gland, and prostate hyperplasia was more severe. A marked improvement was observed in the status of the remaining experimental groups. There was a 45.63%, 42.32%, and 49.49% decrease in BAMO acupuncture group, Simiao pill group and BAMO+Simiao group relative to the model group, respectively (Figure 2C). This pathological profile was further substantiated by Masson’s staining, which revealed a significant increase in blue-stained collagen fibers within the interstitial spaces (Figure 2B).
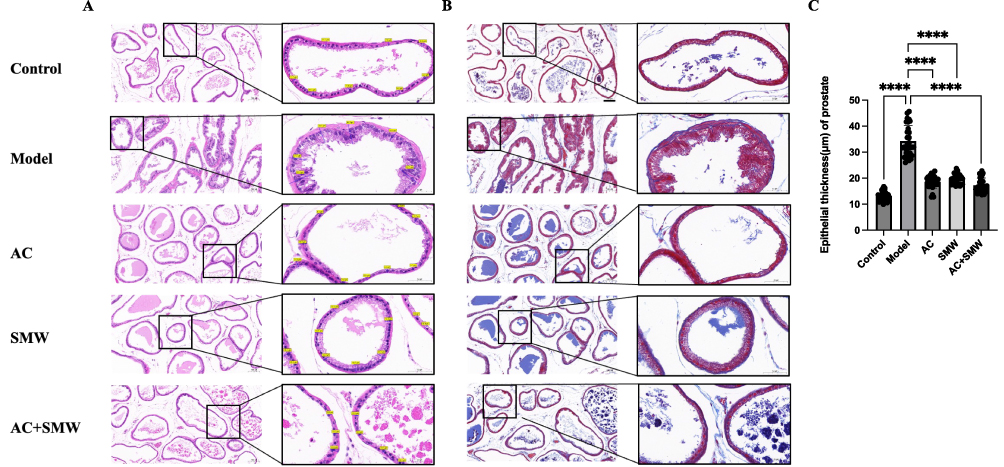 |
Figure 2 Effects of different groups on pathological tissues of mouse prostate; Control: control group (n=10); Model: model group (n=10); AC: BAMO acupuncture group (n=10); SMW: Simiao pill group (n=10); AC+SMW: BAMO Acupuncture+Simiao group (n=10). (A) H&E staining (X10, X40, n=10); (B) Masson’s staining (X10, X40, n=10); (C) Statistical graph of prostate epithelial thickness in mice (n=10); ****P<0.0001. |
Improvement of Hormone Level by BAMO Acupuncture and Simiao Pill
To delineate the hormone-modulating mechanisms of the therapeutic regimen, serum concentrations of T, DHT, and E2 were quantitatively profiled using multiplex flow cytometric assays in murine models. Subsequent IHC of SRD5A2 expression patterns was systematically performed to evaluate SRD5A2 dynamics in prostatic tissues. Compared with the counterparts in control group, levels of T and DHT in plasma but not E2 were significantly higher in Model group. Then plasma levels of T and DHT were significantly lower in BAMO acupuncture group, Simiao pill group and BAMO+Simiao groups than those in model group, and the levels of E2/T were significantly higher in BAMO acupuncture group than that in model group (Figure 3A–D). Furthermore, compared with the counterparts of control group, the expression of SRD5A2 were higher in model group significantly, which were attenuated in BAMO acupuncture group, Simiao pill group and BAMO+Simiao groups (Figure 3E and F). Quantitative analysis indicated a 93.54% increase trend of SRD5A2 in the model group compared to controls. In addition, BAMO acupuncture group, Simiao pill group and BAMO+Simiao group had 56.33%, 54.97%, and 58.77% decrease collagen deposition compared to model group.
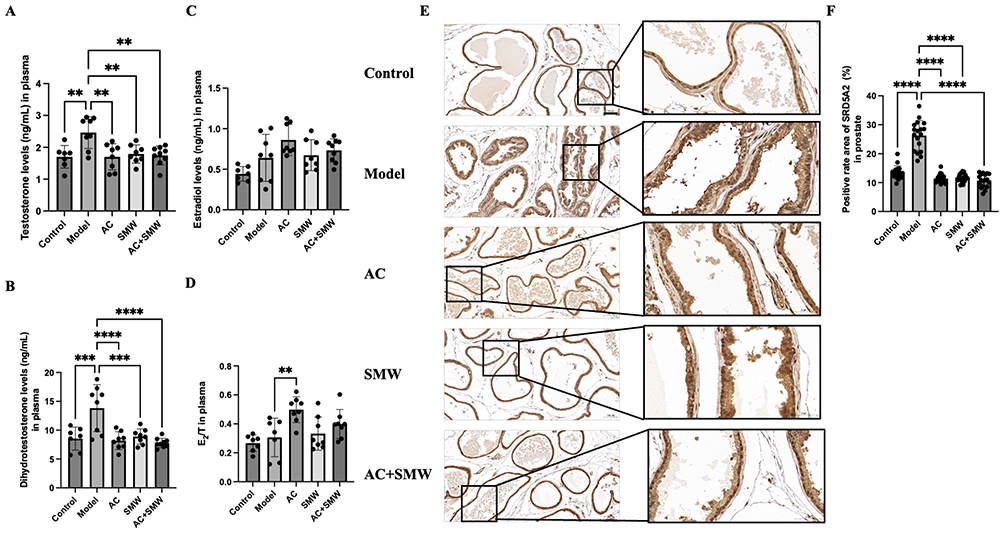 |
Figure 3 Improvement of hormone levels by BAMO acupuncture and Simiao pill. Control: control group (n=10); Model: model group (n=10); AC: BAMO acupuncture group (n=10); SMW: Simiao pill group (n=10); AC+SMW: BAMO Acupuncture+Simiao group (n=10). (A) ELISA kit to detect T level in plasma (n=10), *P<0.05, **P<0.01, ***P<0.001; (B) ELISA kit to detect DHT level in plasma (n=10), ***P<0.001, ****P<0.0001; (C) ELISA kit to detect E2 level in plasma (n=10), p>0.05; (D) E2/T level in plasma (n=10), **P<0.01; (E) IHC staining for the antibody of SRD5A2 (X10, X40, n=6*3); (F) Number of SRD5A2-positive cells (n=6*3), ****P<0.0001. |
Promoting Apoptosis of Prostate Cells by BAMO Acupuncture and Simiao Pill
In order to further explore the impact of BAMO acupuncture and Simiao pill on the apoptosis pathway modulation, IHC assays were conducted to quantify the expression profiles of apoptosis-related biomarkers BAX and BCL-2. The expression of BAX and BCL-2 were displayed in Figure 4A and B, and quantitative levels of BAX, BCL-2, and BAX/BCL-2 were showed (Figure 4C–E). Quantitative analysis indicated a 30.96% decrease trend of BAX/BCL-2 in the model group compared to controls. In addition, BAMO acupuncture group, Simiao pill group and BAMO+Simiao group had 42.12%, 26.95%, and 43.87% increase collagen deposition compared to model group, indicating the pro-apoptosis mechanism of BAMO acupuncture and Simiao pill.
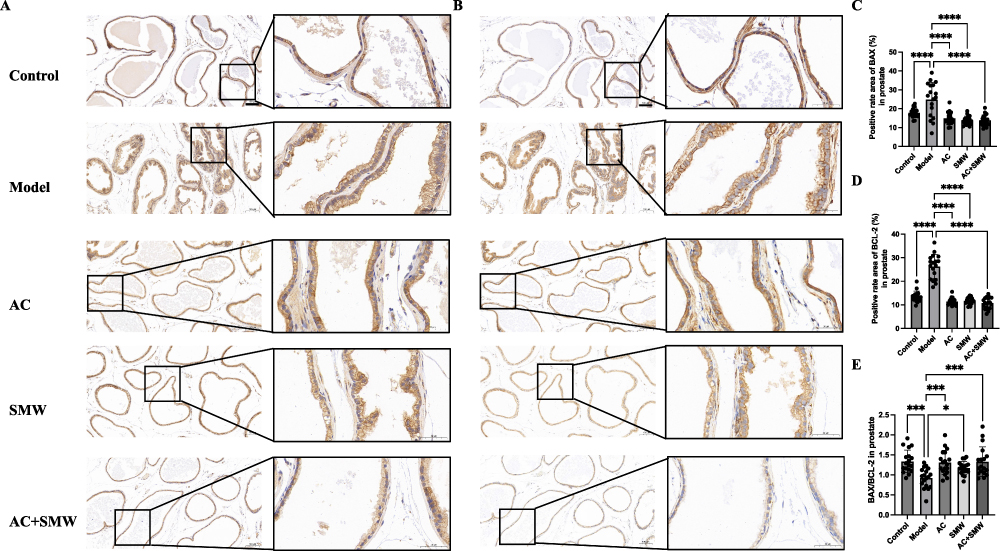 |
Figure 4 Promotion of apoptosis in different groups: Control: control group (n=10); Model: model group (n=10); AC: BAMO acupuncture group (n=10); SMW: Simiao pill group (n=10); AC+SMW: BAMO Acupuncture+Simiao group (n=10). (A) IHC staining for the antibody of BAX (X10, X40); (B) IHC staining for the antibody of BCL-2(X10, X40); (C) Number of Bax-positive cells (n=6*3), ****P<0.0001; (D) Number of BCL-2-positive cells (n=6*3), ****P<0.0001; (E) BAX/BCL-2 ratio (n=6*3), *P<0.05, ***P<0.001. |
Down-Regulated Inflammation Level by BAMO Acupuncture and Simiao Pill
To further explore the inflammation level of treatment protocol on inflammation levels, the serum contents of IL-6 and TNF-α were analyzed by ELISA (Figure 5A and B). Compared with the control group, the levels of IL-6 and TNF-α were significantly higher in model group. At the same time, the concentrations of IL-6 were reduced in BAMO acupuncture group, Simiao pill group and BAMO+Simiao groups by 47.61%, 39.86%, and 39.24% compared with model group. Meanwhile, the contents of TNF-α were decreased to 14.77%, 13.74%, and 19.76%, respectively.
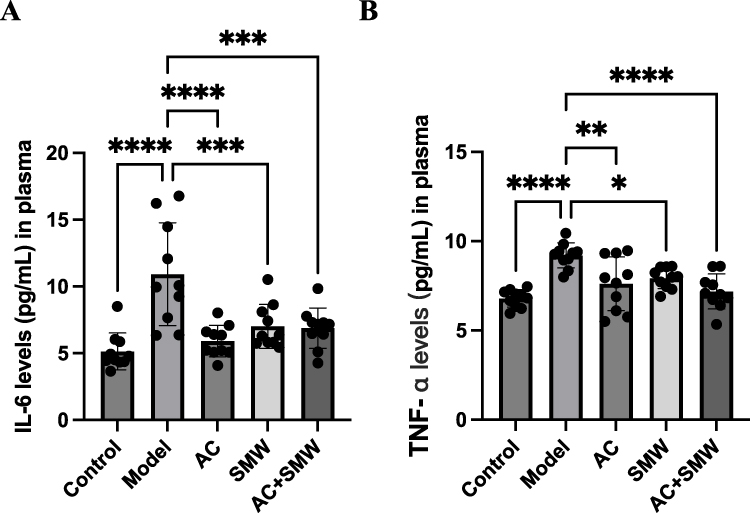 |
Figure 5 Reduction of inflammation level by BAMO acupuncture and drug administration. Control: control group (n=10); Model: model group (n=10); AC: BAMO acupuncture group (n=10); SMW: Simiao pill group (n=10); AC+SMW: BAMO Acupuncture+Simiao group (n=10). (A) IL-6 level was detected by multifactor flow assay (n=10), ***P<0.001, ****P<0.0001; (B) TNF-α level was detected by multifactor flow assay (n=10), *P<0.05, **P<0.01, ****P<0.0001. |
Discussion
Whether the BPH model is valid is mainly verified by the wet weight of the prostate and PI (prostate wet weight (mg) / body weight (g) of the mice). The research shows that the wet weight of the prostate and PI in the model group of mice have significant differences compared to the model group (P < 0.0001, Figure 1C and D). Moreover, the prostate images of the mice in the BPH model group also indicate that the prostate tissue is more prominent, while it is not obvious in the control group (Figure 1A). The HE staining and Masson staining of the prostate tissues of the mice in the model group were used to determine that the epithelial cells of the prostate tissues of the mice in this group were thickened and there was deposition of matrix fibrous collagen, which was in line with the pathological features of BPH (P < 0.0001, Figure 2). However, the BPH model employed in this experiment was induced by exogenous TP stimulation in six-week-old mice, which cannot simulate the ageing process in elderly males. Furthermore, the rapid modelling approach does not align with the pathological progression of BPH. The absence of a sham acupuncture group in this study precludes the exclusion of non-specific effects of needle insertion. Although grounded in clinical practice, this research lacks validation using human prostate tissue, necessitating further assessment of whether the model conclusions translate to clinical applications.
T, the primary circulating androgen, is enzymatically converted to its potent bioactive metabolite DHT by SRD5A2, an enzyme localized on the nuclear membrane of stromal mesenchymal cells.49,50 DHT binds to the androgen receptor (AR) in prostate cells to form a nuclear complex that promotes the synthesis of growth factors and cytoplasmic proteins, leading to aberrant cell proliferation and the formation of BPH.51–53 The major male estrogen is E2, which is converted from T in peripheral tissues by aromatase, controls, and regulates the prostate organ.54 E2 stimulates prostate cell proliferation and promotes epithelial–mesenchymal transformation of prostate cells through its action on the estrogen receptor,55,56 which can lead to prostate hyperplasia. Dysregulation of the estrogen/androgen ratio is also a major cause of BPH. In aging males, serum T levels exhibit a progressive decline, whereas E2 concentrations remain stable or show a compensatory rise. This age-related hormonal imbalance elevates the estrogen-to-androgen ratio, which disrupts prostatic tissue homeostasis by promoting imbalanced proliferative/apoptotic signaling pathways, a hallmark mechanism driving BPH pathogenesis.57 Animal research models have confirmed that dysregulation of the estrogen/androgen ratio contributes to prostate enlargement and urinary incontinence.58 Studies have shown that the Simiao pill acts on the AR and ER-β genes in the body, and acupuncture can reduce T and DHT levels in patients.59–61 The results of this study were that the T and DHT levels of mice in the model group were elevated compared with the control group (P<0.01, P<0.001) and decreased in the treatment group (P<0.05, P<0.001) compared with the model group, at the same time, the E2/T ratio increased, which showed the hormone modulation effects of the Simiao pill and BAMO acupuncture (Figure 3A–D). Furthermore, we observed the downregulation of SRD5A2 (the key enzyme responsible for DHT synthesis, Figure 3E and F) in the treatment group, which meant the inhibition of the androgen metabolic pathway.
BPH arises from smooth muscle cell and epithelial cell proliferation, primarily within the transition zone of the prostate.62 Apoptosis and inflammation play important roles in the control of cell growth and in the maintenance of tissue homeostasis.63 Disturbances in molecular mechanisms of apoptosis machinery have been linked to BPH.64 Apoptosis is primarily triggered by specific stimuli, such as an activation or inactivation of several molecules through a multifaceted regulation. Cells showing a higher expression of Bax undergo apoptosis, while those over expressing BCL-2 often undergo suppression of apoptosis.65 It has been suggested that the BAX/BCL-2 ratio is very important for the regulation of apoptosis, determining cell fate.66 Acupuncture has a unique advantage in promoting apoptosis, which is closely related to the role in promoting blood circulation and activating meridians and collaterals, and a large number of studies have confirmed that acupuncture plays a pro-apoptotic role by increasing BAX and decreasing BCL-2.67–69 Studies have shown that acupuncture on Guanyuan (CV4), Zhongji, and Sanyinjiao (SP6) can reduce the volume and mass of rat prostate, reduce prostate inflammation and fibrosis,70 increase the apoptosis rate, decrease the expression of BCL-2 and increase the expression of BAX in rat prostate cells.71 Our results suggested that Simiao Pill, BAMO acupuncture, and their combined application could upregulate the ratio of BAX/BCL-2, namely, promote the apoptosis of hyperplastic prostate cells (P<0.05, Figure 4). Regarding the up regulation of BAX expression in mice prostate tissues, mainly because that the prostate cells in the model group were abnormally proliferated, the epithelial thickness was increased, and the area of positive expression was also increased.
The role of inflammation in BPH has been extensively studied in recent years. In approximately 70% of prostate tissue samples from BPH patients, inflammatory infiltration was observed. This inflammation is correlated with the volume and weight of the prostate.72–74 Simiao pill can significantly reduce the levels of IL-6 and TNF-α in various immune and inflammatory diseases, thus exerting anti-inflammatory effects.75–77 The anti-inflammatory effects of acupuncture have been extensively studied, primarily through the regulation of TNF-α, IL-6, IL-8, and other factors.78–80 This experiment confirms that Simiao Pill, BAMO acupuncture, and their combined application effectively reduce serum levels of IL-6 (P<0.01) and TNF-α (P<0.05) in BPH model mice (Figure 5), which served as inflammatory biomarkers to assess systemic inflammation.
Furthermore, we observed that all mice exhibited a micturition response within 3 to 5 min following acupuncture stimulation at the corresponding acupoints. This response may be attributable to acupuncture-induced relaxation of the urethral sphincter, concurrent with contraction of the detrusor muscle in the bladder wall, thereby facilitating urine expulsion. This finding is consistent with the established efficacy of acupuncture in alleviating urinary retention. However, this was not investigated further in the present experiment.
Conclusion
In conclusion, our study demonstrated that Simiao Pill, BAMO acupuncture, and their combined application had the effect of treating BPH in mice. They could regulate androgen metabolism of T and DHT, which playing a therapeutic role by downregulating the expression SRD5A2. On the other hand, they could inhibit the release of inflammatory factors such as IL-6 and TNF-α. Furthermore, the treatment protocol could induce apoptosis of prostate cells, and up-regulate the ratio of BAX/BCL-2 to exert therapeutic effects. Further research into the mechanism of this formulation will help to demonstrate the potential value of traditional Chinese medicine in the treatment of BPH.
Acknowledgments
The authors are grateful for “National Initiative for Advancing Traditional Chinese Medicine” project of Hongkou District (HKQGYQY-2022-04 and HKGYQYXM-2022-19) for financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ng M, Leslie SW, Baradhi KM. Benign prostatic hyperplasia. In: StatPearls. StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC; 2025.
2. Liu TT, Thomas S, McLean DT, et al. Prostate enlargement and altered urinary function are part of the aging process. Aging. 2019;11(9):2653–2669. doi:10.18632/aging.101938
3. Adil Mehmood M, Jehan S, Khan I, Ilyas M, Khan U, Ali W. The assessment of patient-reported outcomes in the medical management of patients with benign prostatic hyperplasia. Cureus. 2024;16(8):e67027. doi:10.7759/cureus.67027
4. Li X, Li X, Wang L, et al. Advancing traditional Chinese medicine research through network pharmacology: strategies for target identification, mechanism elucidation and innovative therapeutic applications. Am J Chin Med. 2025;53(7):2021–2042. doi:10.1142/s0192415x25500752
5. Cui F. A meta-analysis of acupuncture’s improvement of mood disorders, pain and quality of life in migraine patients. Altern Ther Health Med. 2024;30(11):304–311.
6. Rybicka M, Gąsowski J, Przeklasa-Muszyńska A, et al. NADA ear acupuncture and medical acupuncture for pain- and health-related quality of life among older patients with chronic nonspecific low back pain: a prospective clinical trial. Brain Sci. 2024;14:3. doi:10.3390/brainsci14030205
7. Chen S, Sun H, Xu H, Zhang Y, Wang H. Effects of acupuncture on hospitalized patients with urinary retention. Evid Based Complement Alternat Med. 2020;2020:2520483. doi:10.1155/2020/2520483
8. Cao D, Yang Q, Qi F, et al. Acupuncture improves the residual urine volume of bladder of middle age patients with urinary retention post-stroke: a protocol for systematic review and meta analysis. Medicine. 2022;101(47):e31697. doi:10.1097/md.0000000000031697
9. Lauterbach R, Ferrer Sokolovski C, Rozenberg J, Weissman A. Acupuncture for the treatment of post-partum urinary retention. Eur J Obstet Gynecol Reprod Biol. 2018;223:35–38. doi:10.1016/j.ejogrb.2018.01.029
10. Hata J, Harigane Y, Matsuoka K, et al. Mechanism of androgen-independent stromal proliferation in benign prostatic hyperplasia. Int J Mol Sci. 2023;24:14. doi:10.3390/ijms241411634
11. Tong Y, Zhou RY. Review of the roles and interaction of androgen and inflammation in benign prostatic hyperplasia. Mediators Inflamm. 2020;2020:7958316. doi:10.1155/2020/7958316
12. DaSilva J, Gioeli D, Weber MJ, Parsons SJ. The neuroendocrine-derived peptide parathyroid hormone-related protein promotes prostate cancer cell growth by stabilizing the androgen receptor. Cancer Res. 2009;69(18):7402–7411. doi:10.1158/0008-5472.Can-08-4687
13. Yokoyama T, Saino T, Nakamuta N, Yamamoto Y. Topographic distribution of serotonin-immunoreactive urethral endocrine cells and their relationship with calcitonin gene-related peptide-immunoreactive nerves in male rats. Acta Histochem. 2017;119(1):78–83. doi:10.1016/j.acthis.2016.11.011
14. Zeng XT, Jin YH, Liu TZ, et al. Clinical practice guideline for transurethral plasmakinetic resection of prostate for benign prostatic hyperplasia (2021 Edition). Mil Med Res. 2022;9(1):14. doi:10.1186/s40779-022-00371-6
15. Kirschner-Hermanns R, Funk P, Leistner N. WS PRO 160 I 120 mg (a combination of sabal and urtica extract) in patients with LUTS related to BPH. Ther Adv Urol. 2019;11:1756287219879533. doi:10.1177/1756287219879533
16. Zhang J, Zhang M, Tang J, et al. Animal models of benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2021;24(1):49–57. doi:10.1038/s41391-020-00277-1
17. Steiner MS, Couch RC, Raghow S, Stauffer D. The chimpanzee as a model of human benign prostatic hyperplasia. J Urol. 1999;162(4):1454–1461. doi:10.1016/S0022-5347(05)68340-1
18. Trachtenberg J, Hicks LL, Walsh PC. Androgen- and estrogen-receptor content in spontaneous and experimentally induced canine prostatic hyperplasia. J Clin Invest. 1980;65(5):1051–1059. doi:10.1172/jci109757
19. Lucas Cava V, Sánchez Margallo FM, Báez Díaz C, Dávila Gómez L, Lima Rodríguez JR, Sun F. Prostatic artery embolization with polyethylene glycol microspheres: evaluation in a canine spontaneous benign prostatic hyperplasia model. CVIR Endovasc. 2020;3(1):44. doi:10.1186/s42155-020-00130-5
20. Cazzuli G, Damián JP, Molina E, Pessina P. Post-castration prostatic involution: a morphometric and endocrine study of healthy canines and those with benign prostatic hyperplasia. Reprod Domest Anim. 2022;57(2):157–164. doi:10.1111/rda.14036
21. Sorokina IV, Zhukova NA, Meshkova YV, et al. Modeling of benign prostatic hyperplasia in rats with a high dose of testosterone. Bull Exp Biol Med. 2022;173(5):680–686. doi:10.1007/s10517-022-05613-0
22. Al-Trad B, Aljabali A, Al Zoubi M, Shehab M, Omari S. Effect of gold nanoparticles treatment on the testosterone-induced benign prostatic hyperplasia in rats. Int J Nanomed. 2019;14:3145–3154. doi:10.2147/ijn.S202645
23. Tang X, Liu Z, Ren J, et al. Comparative RNA-sequencing analysis of the prostate in a mouse model of benign prostatic hyperplasia with bladder outlet obstruction. Mol Cell Biochem. 2023;478(12):2721–2737. doi:10.1007/s11010-023-04695-2
24. Jin BR, Kim HJ, Seo JH, et al. HBX-6, standardized cornus officinalis and psoralea corylifolia l. extracts, suppresses benign prostate hyperplasia by attenuating E2F1 activation. Molecules. 2019;24(9):1719. doi:10.3390/molecules24091719
25. Nicholson TM, Ricke EA, Marker PC, et al. Testosterone and 17β-estradiol induce glandular prostatic growth, bladder outlet obstruction, and voiding dysfunction in male mice. Endocrinology. 2012;153(11):5556–5565. doi:10.1210/en.2012-1522
26. Wu S, Yin X, Yang P, Gong B, Wang Z. Beneficial effects of Akkermansia muciniphila on benign prostatic hyperplasia and metabolic syndrome. Arch Biochem Biophys. 2025;768:110294. doi:10.1016/j.abb.2025.110294
27. Zhou J, Zheng MY, Chen S, Zhao YY, Ma RJ. Therapeutic effect of electroacupuncture at “Sidi Points” on mild to moderate benign prostatic hyperplasia with lower urinary tract symptoms: a randomized controlled trial. Chin Acupunct Moxibust. 2024. doi:10.13703/j.0255-2930.20240322-k0003
28. Hu ZD, Xu L, Li LC, et al. Professor Qin Guozheng’s experience in treating benign prostatic hyperplasia based on “yang transforming qi and yin forming shape”. Chin J Ethnomed Ethnopharm. 2024;33(22):66–69. doi:10.16038/j.1003-7446.2024.22.016
29. Yang L, Sun Y, Wei S, Wen H, Liu R, Wang X. Chemical profiling of Simiao pill and quantification of main effective constituents in it by ultra-high-performance liquid chromatography coupled with Q Exactive Orbitrap and triple quadrupole mass spectrometry. J Sep Sci. 2024;47(1):e2300615. doi:10.1002/jssc.202300615
30. Liu CS, Hu YN, Luo ZY, Xia T, Tan XM. Comparative analysis of pharmacokinetics and intestinal absorption of six alkaloids between Sanmiao Pills and Simiao Pills in rats. Zhongguo Zhong Yao Za Zhi. 2021;46(23):6271–6277. doi:10.19540/j.cnki.cjcmm.20210727.202
31. Fan J, Liu K, Zhang Z, et al. Modified Si-Miao-San extract inhibits the release of inflammatory mediators from lipopolysaccharide-stimulated mouse macrophages. J Ethnopharmacol. 2010;129(1):5–9. doi:10.1016/j.jep.2010.02.002
32. Shang SW, Yang JL, Huang F, Liu K, Liu BL. Modified Si-Miao-San ameliorates pancreatic B cell dysfunction by inhibition of reactive oxygen species-associated inflammation through AMP-kinase activation. Chin J Nat Med. 2014;12(5):351–360. doi:10.1016/s1875-5364(14)60043-1
33. Hong YD, Chen Y. Exploring the law of acupoint selection in ancient acupuncture for stranguria based on data mining. Forum Prim Med. 2022;26(10):109–112. doi:10.19435/j.1672-1721.2022.10.036
34. Li H, Wu SW, Fu D, Guo HZ. Clinical evaluation of Simiao Pill combined with acupuncture at Sanyin Points in the treatment of prostatitis with damp-heat stasis syndrome. Sichuan J Tradit Chin Med. 2021;39(03):125–128.
35. Zhang SS, Zhang X, Zhou LB, Lü WL. Clinical study on modified Simiao Pill combined with western medicine in the treatment of type IIIA prostatitis with damp-heat stasis syndrome. J New Chin Med. 2021;53(17):62–65. doi:10.13457/j.cnki.jncm.2021.17.015
36. He YJ, Miao FR, Fan YS, et al. Analysis of acupoint selection rules for acupuncture treatment of benign prostatic hyperplasia based on data mining technology. Chin J Inf Tradit Chin Med. 2023;30(11):25–31. doi:10.19879/j.cnki.1005-5304.202303460
37. Liu XH, Yu XD, Liu MY, et al. Exploring the characteristics and differences of acupoint selection ideas in acupuncture for chronic prostatitis and prostatic hyperplasia using data mining technology. J Liaoning Univ Tradit Chin Med. doi:10.13194/j.issn.1673-842x.2024.03.012
38. Cheng LL, Wu CY, Sui MH. [Effects of electroacupuncture of “Weizhong” (BL 40), “Sanyinjiao” (SP 6) and “Yinlingquan” (SP 9) on intravesical pressure and bladder adenosine triphosphate content in rabbits with acute urinary retention]. Zhen Ci Yan Jiu. 2012;37(4):291–295. Hausa
39. Liu HR, Gu WY, Pan LJ, et al. Clinical observation on Tongdu Tiaoqi acupuncture combined with warming acupuncture for postoperative urinary retention. Zhongguo Zhen Jiu. 2022;42(1):41–44. doi:10.13703/j.0255-2930.20210504-k0002
40. Liu F, Shi RJ, Cao B, Deng WL, Dong YK. Postoperative acute urinary retention in anorectal diseases treated with acupuncture combined with grain-moxibustion: a randomized controlled trial. Zhongguo Zhen Jiu. 2019;39(7):709–712. doi:10.13703/j.0255-2930.2019.07.008
41. Xiao J, Yi W, Wu L. Effects of electroacupuncture on reducing labor pain and complications in the labor analgesia process of combined spinal-epidural analgesia with patient-controlled epidural analgesia. Arch Gynecol Obstet. 2019;299(1):123–128. doi:10.1007/s00404-018-4955-6
42. Hong H, Cao X, Deng T, et al. Acupuncture at Neiguan suppresses PVCs occurring post-myocardial infarction by alleviating inflammation and fibrosis. Chin Med. 2022;17(1):52. doi:10.1186/s13020-022-00606-7
43. Liao LY, Chien LW, Liu CF. Far-infrared stimulation of Neiguan acupoints improves heart rate variability and ameliorate fatigue in hemodialysis patients: a randomized trial. J Chin Med Assoc. 2024;87(3):340–345. doi:10.1097/jcma.0000000000001060
44. Yujuan YE, Yuting W, Jing J, Xingke Y. Efficacy of needling Baihui (GV20), Neiguan (PC6), Shenmen (HT7) and Taichong (LR3) on cerebral cortical blood oxygen level in rats with insomnia. J Tradit Chin Med. 2023;43(3):523–532. doi:10.19852/j.cnki.jtcm.20230404.005
45. Zhang N, Houle T, Hindiyeh N, Aurora SK. Systematic review: acupuncture vs standard pharmacological therapy for migraine prevention. Headache. 2020;60(2):309–317. doi:10.1111/head.13723
46. Kong F, Wang Z, Wang N, et al. The clinical observation of acupuncture combined with antiemetic drugs in the prevention and treatment of CINV in breast cancer patients. Front Oncol. 2022;12:888651. doi:10.3389/fonc.2022.888651
47. Li C, Chen S, Liu S, Mu Y, Su M. Effect of acupuncture combined with antidepressants on post-stroke depression: a network meta-analysis of nine acupuncture therapy. Front Neurol. 2023;14:979643. doi:10.3389/fneur.2023.979643
48. Sui KM, Li X. Clinical observation on acupuncture combined with medication for treatment of essential tremor. Zhongguo Zhen Jiu. 2010;30(2):107–109.
49. Devlin CM, Simms MS, Maitland NJ. Benign prostatic hyperplasia - what do we know? BJU Int. 2021;127(4):389–399. doi:10.1111/bju.15229
50. Nicholson TM, Ricke WA. Androgens and estrogens in benign prostatic hyperplasia: past, present and future. Differentiation. 2011;82(4–5):184–199. doi:10.1016/j.diff.2011.04.006
51. Choi YJ, Fan M, Tang Y, Yang HP, Hwang JY, Kim EK. In vivo effects of polymerized anthocyanin from grape skin on benign prostatic hyperplasia. Nutrients. 2019;11(10):2444. doi:10.3390/nu11102444
52. Bhat SA, Rather SA, Islam N. An overview of benign prostatic hyperplasia and its appreciation in Greco-Arab (Unani) system of medicine. Asian J Urol. 2022;9(2):109–118. doi:10.1016/j.ajur.2021.05.008
53. Liu J, Fang T, Li M, et al. Pao pereira extract attenuates testosterone-induced benign prostatic hyperplasia in rats by inhibiting 5α-reductase. Sci Rep. 2019;9(1):19703. doi:10.1038/s41598-019-56145-z
54. Wynder JL, Nicholson TM, DeFranco DB, Ricke WA. Estrogens and male lower urinary tract dysfunction. Curr Urol Rep. 2015;16(9):61. doi:10.1007/s11934-015-0534-6
55. Jin R, Forbes CM, Miller NL, et al. Transcriptomic analysis of benign prostatic hyperplasia identifies critical pathways in prostatic overgrowth and 5-alpha reductase inhibitor resistance. Prostate. 2024;84(5):441–459. doi:10.1002/pros.24661
56. Khristi V, Ghosh S, Chakravarthi VP, Wolfe MW, Rumi MAK. Transcriptome data analyses of prostatic hyperplasia in Esr2 knockout rats. Data Brief. 2019;24:103826. doi:10.1016/j.dib.2019.103826
57. Asiedu B, Anang Y, Nyarko A, et al. The role of sex steroid hormones in benign prostatic hyperplasia. Aging Male. 2017;20(1):17–22. doi:10.1080/13685538.2016.1272101
58. Bernoulli J, Yatkin E, Konkol Y, Talvitie EM, Santti R, Streng T. Prostatic inflammation and obstructive voiding in the adult Noble rat: impact of the testosterone to estradiol ratio in serum. Prostate. 2008;68(12):1296–1306. doi:10.1002/pros.20791
59. Xu Z, Su P, Zhou X, Zheng Z, Zhu Y, Wang Q. Exploring the mechanism of action of Modified Simiao Powder in the treatment of osteoarthritis: an in-silico study. Front Med. 2024;11:1422306. doi:10.3389/fmed.2024.1422306
60. Gao J-Y, Liu H-J, Shi J, et al. Clinical efficacy of catgut embedment combined with moxibustion and bloodletting in the treatment of androgenic alopecia. World J Acupunct. 2015;25(1):1–6. doi:10.1016/S1003-5257(15)30001-5
61. Li Q, Xie Y, Zha X. The clinical effect of plum blossom needle acupuncture with qi-invigorating superficies-consolidating therapy on seborrheic alopecia. Ann Palliat Med. 2020;9(3):1030–1036. doi:10.21037/apm-20-909
62. Liu Z, Li S, Chen S, et al. YAP-mediated GPER signaling impedes proliferation and survival of prostate epithelium in benign prostatic hyperplasia. iScience. 2024;27(3):109125. doi:10.1016/j.isci.2024.109125
63. Arienti S, Barth ND, Dorward DA, Rossi AG, Dransfield I. Regulation of apoptotic cell clearance during resolution of inflammation. Front Pharmacol. 2019;10:891. doi:10.3389/fphar.2019.00891
64. Minutoli L, Rinaldi M, Marini H, et al. Apoptotic pathways linked to endocrine system as potential therapeutic targets for benign prostatic hyperplasia. Int J Mol Sci. 2016;17(8):1311. doi:10.3390/ijms17081311
65. Li X, Li L, Ouyang D, Zhu Y, Yuan T. The abnormal expression of kisspeptin regulates pro-inflammatory cytokines, cell viability and apoptosis of macrophages in hyperandrogenism induced by testosterone. Gynecol Endocrinol. 2021;37(1):72–77. doi:10.1080/09513590.2020.1811964
66. Batool S, Asim L, Qureshi FR, Masood A, Mushtaq M, Saleem RSZ. Molecular targets of plant-based alkaloids and polyphenolics in liver and breast cancer- an insight into anticancer drug development. Anticancer Agents Med Chem. 2025;25(5):295–312. doi:10.2174/0118715206302216240628072554
67. Jang J-H, Yeom M-J, Ahn S, et al. Acupuncture inhibits neuroinflammation and gut microbial dysbiosis in a mouse model of Parkinson’s disease. Brain Behav Immun. 2020;89:641–655. doi:10.1016/j.bbi.2020.08.015
68. Chen S, Li J, Yan L, Zhang X, Huang J, Zhou P. Electroacupuncture alleviates the symptom of depression in mice by regulating the cGAS-STING-NLRP3 signaling. Aging. 2024;16(8):6731–6744. doi:10.18632/aging.205596
69. Cheng WJ, Li P, Huang WY, et al. Acupuncture relieves stress-induced depressive behavior by reducing oxidative stress and neuroapoptosis in rats. Front Behav Neurosci. 2022;15:783056. doi:10.3389/fnbeh.2021.783056
70. Wang ZN, Fang HT, Yuan Q. Effect of acupuncture at Niaosan Points on prostatic cell apoptosis in BPH rats. Chin J Basic Med Tradit Chin Med. 2018;24(10):1454–1457. doi:10.19945/j.cnki.issn.1006-3250.2018.10.035
71. Wang ZN. Effect of Acupuncture on the Expression of BPH-Related Apoptosis Proteins Bcl-2 and Bax in Rats [Master’s Thesis]. 2018.
72. Zlotta AR, Egawa S, Pushkar D, et al. Prevalence of inflammation and benign prostatic hyperplasia on autopsy in Asian and Caucasian men. Eur Urol. 2014;66(4):619–622. doi:10.1016/j.eururo.2014.06.026
73. Nickel JC, Roehrborn CG, O’Leary MP, Bostwick DG, Somerville MC, Rittmaster RS. The relationship between prostate inflammation and lower urinary tract symptoms: examination of baseline data from the REDUCE trial. Eur Urol. 2008;54(6):1379–1384. doi:10.1016/j.eururo.2007.11.026
74. Cao D, Sun R, Peng L, et al. Immune cell proinflammatory microenvironment and androgen-related metabolic regulation during benign prostatic hyperplasia in aging. Front Immunol. 2022;13:842008. doi:10.3389/fimmu.2022.842008
75. Wang Y, Zhang F, Li X, et al. Integrated multi-omics techniques and network pharmacology analysis to explore the material basis and mechanism of simiao pill in the treatment of rheumatoid arthritis. ACS Omega. 2023;8(12):11138–11150. doi:10.1021/acsomega.2c07959
76. Wang XY, Liu MZ, Zhao J. Effect of Danggui Sini decoction combined with Simiao Pill on TCM syndrome scores and Wnt/β-catenin signaling pathway in the treatment of diabetic nephropathy. Liaoning J Tradit Chin Med. 2024;51(08):114–118. doi:10.13192/j.issn.1000-1719.2024.08.030
77. Li J, Zhao QT, Qin W, Piao SA, Hu XY. Research progress on modern clinical application and mechanism of action of Simiao Pill. Chin Arch Tradit Chin Med. 2023;41(10):5–9. doi:10.13193/j.issn.1673-7717.2023.10.002
78. Yu F, Li S, Li Z, et al. Usage, anti-inflammatory effect and safety of adjunctive acupuncture for cerebral infarction: an Apriori algorithm-based data mining and meta-analysis. Front Neurol. 2025;16:1546194. doi:10.3389/fneur.2025.1546194
79. Wang J, Lu S, Yang F, et al. The role of macrophage polarization and associated mechanisms in regulating the anti-inflammatory action of acupuncture: a literature review and perspectives. Chin Med. 2021;16(1):56. doi:10.1186/s13020-021-00466-7
80. Yang NN, Ma X, Li YJ, et al. Research progress and thinking of acupuncture in anti-inflammation by regulating autonomic nerve system. Zhen Ci Yan Jiu. 2023;48(6):610–617. doi:10.13702/j.1000-0607.20220132
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.