Back to Journals » Journal of Inflammation Research » Volume 19
Therapeutic Approaches for Cutaneous Lupus Erythematosus: a Changing Landscape of Clinical Trials
Authors Wei E ![]() , Lopes Almeida Gomes L, Jun S, Saksena S, Werth VP
, Lopes Almeida Gomes L, Jun S, Saksena S, Werth VP ![]()
Received 18 November 2025
Accepted for publication 17 January 2026
Published 4 February 2026 Volume 2026:19 547944
DOI https://doi.org/10.2147/JIR.S547944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adrian Lee
Elena Wei,1,2 Lais Lopes Almeida Gomes,1,2 Sarah Jun,1,2 Sarini Saksena,1,2 Victoria P Werth1,2
1Corporal Michael J. Crescenz Veterans Affairs Medical Center Philadelphia, Philadelphia, PA, USA; 2Department of Dermatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Correspondence: Victoria P Werth, Department of Dermatology, University of Pennsylvania, Perelman Center for Advanced Medicine, 3400 Civic Center Boulevard, Philadelphia, PA, 19104, USA, Email [email protected]
Abstract: Cutaneous lupus erythematosus (CLE) is an autoimmune skin disease that can occur with or without systemic lupus erythematosus (SLE). To date, there are no specific FDA-approved therapies specifically for CLE. Historically, SLE clinical trials showed promising skin-related outcomes as secondary endpoints; however, these drugs have not received FDA approval specifically for CLE, which limits their availability and insurance coverage for patients with only CLE. Clinical trials for drugs to treat SLE have often utilized primary endpoints such as the SLE Responder Index (SRI) and BILAG-Based Composite Lupus Assessment (BICLA), which are systemic-focused endpoints. With the recent acceptance of Cutaneous LE Disease Area and Severity Index (CLASI) as an endpoint, it can now be used to study response in skin as a primary outcome for clinical trials in LE. The goal of this review paper is to examine the therapeutic use of several existing SLE drugs and new emerging therapies in CLE and their clinical trial and real-world outcomes. Existing SLE drugs such as belimumab and anifrolumab have shown potential promise as a treatment for CLE, and a Phase III CLE clinical trial for anifrolumab is ongoing. Other emerging therapies such as deucravacitinib, litifilimab, and enpatoran have been successful with skin-related endpoints in Phase II CLE trials. A phase II/III CLE clinical trial for litifilimab is ongoing, and phase III trials for enpatoran are planned. As CLASI has become an accepted primary endpoint for clinical trials, drug development is shifting to prioritize cutaneous outcomes and to use endpoints that measure skin-specific effects. This targeted approach represents a fundamental change that may ultimately increase FDA-approved therapies specifically for CLE and expand treatment options for patients with CLE.
Keywords: cutaneous lupus erythematosus, CLASI, clinical trials, quinacrine, litifilimab, enpatoran
Introduction
Cutaneous lupus erythematosus (CLE) is an autoimmune skin disease that can occur with or without systemic lupus erythematosus (SLE). There are three major subtypes of CLE, acute CLE (ACLE), subacute CLE (SCLE), and chronic CLE (CCLE), which includes discoid LE (DLE).1 The subtypes are often distinguishable based on clinical presentation of the lesions, and although presentation may overlap, the treatment strategies may be similar between the various subtypes, as a high type I interferon (Type I IFN) signature and subsequent pro-inflammatory environment is present for nearly all lesional CLE subtypes.2 One strategy to treat CLE is to prevent triggers through high SPF sun protection and smoking cessation.3 In cases of limited dermatologic manifestations, another approach is with topicals such as topical glucocorticoids, with caution regarding the side effects of high potency topical glucocorticoids, or topical calcineurin inhibitors.4 To date, there are no specific US Food and Drug Administration (FDA)-approved therapies specifically for CLE.
In addition to CLE as its own clinical entity, SLE also has dermatologic manifestations in addition to other systemic symptoms. About 70–85% of SLE patients have skin involvement.5 Additionally, approximately 5–30% of CLE (especially DLE) will eventually develop systemic lupus.6 Several drugs have been developed and approved for SLE based on systemic endpoints, and their effects have not always been studied with skin endpoints. For over fifty years since 1958, there were no new drugs approved for SLE until belimumab was approved in 2011, and skin improvement was not the primary focus of this drug.
Clinical trials have often utilized primary endpoints such as the SLE Responder Index (SRI) and BILAG-Based Composite Lupus Assessment (BICLA), which are systemic-focused endpoints that will be described later. Skin-focused endpoints such as the Cutaneous LE Disease Area and Severity Index (CLASI) were often used as secondary endpoints.
Recently, the CLASI was accepted as a primary endpoint for clinical trials in LE. In the past the CLASI has only been used as a secondary endpoint in SLE trials. With the acceptance of CLASI as an endpoint, it can now be used to study response in skin as a primary outcome. There are now clinical trials with a focus on the skin, and this will hopefully improve the treatment options for patients with CLE.
The goal of this review paper is to examine the therapeutic use of several existing SLE drugs and new emerging therapies in CLE and their clinical trial and real-world outcomes. The primary focus is on newer emerging therapies and biologics and will highlight the evolution of drug therapy development to include primary outcomes examining the skin. Currently, the only drugs that are approved for treatment of CLE are corticosteroids and hydroxychloroquine. Drugs such as corticosteroids and immunosuppressants have been used for a long time to treat CLE; this paper will therefore focus on other emerging therapies and biologics.
Outcome Measures and Clinical Trial Endpoints
In clinical trials that evaluate drugs for SLE, the primary outcome measures are primarily designed to evaluate systemic manifestations. The Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) is an outcome measure that weights nine organ systems for disease activity.7 This outcome measure is heavily weighted against the skin compared to other organ systems impacted by SLE and thus loses the nuance in how the skin is affected by the drug under investigation. Any CLE lesions must completely resolve to score improvement on the SLEDAI. The British Isles Lupus Assessment Group (BILAG) index allocates separate scores (Category A through E, A being the most severe) to different organ-based symptoms, with some skin measures.8
The SLEDAI and BILAG were used to develop further composite endpoints such as the SRI and BICLA. The SRI-4 response criteria consist of, 1) a ≥4-point reduction in SLEDAI score, 2) no new BILAG A score in any organ domain and no more than 1 new BILAG B score, and 3) no worsening in physician’s global assessment (PGA, a ranking of disease activity on a scale from 0 [no disease activity] to 3 [severe disease]) score > 10%.9 A British Isles Lupus Assessment Group (BILAG)–based Composite Lupus Assessment (BICLA) response consists of, 1) a reduction in all baseline BILAG-A to ≤ B and BILAG B to ≤ C, 2) no worsening of PGA >10%, 3) no worsening of SLEDAI, 4) no discontinuation of the trial intervention, and 5) no use of medications restricted by the protocol.10
While these endpoints focused on systemic manifestations leaving little nuance to the treatment of skin symptoms, other endpoints such as CLASI are better able to capture skin-related changes. One such endpoint that is used in current clinical trials is the change in CLASI-Activity (CLASI-A) score from baseline, which quantifies disease activity based on the degree of erythema, scale, mucous membrane lesions, and non-scarring alopecia.11,12 CLASI-50 response is defined as at least 50% improvement in CLASI-A score, and it has been shown to be predictive of a meaningful quality of life change in patients with a baseline CLASI-A score ≥8.13 Likewise, CLASI-70/90/100 indicates at least 70%/90%/100% improvement in CLASI-A score. Another endpoint that focuses on skin-specific symptoms is CLA-IGA-R, which scores the three disease components of erythema, other morphological characteristics, and follicular activity separately with a five-point scale indicating severity.14 Other patient-reported outcome measures assess disease-specific quality of life, including the Skindex 29+3 and cutaneous lupus erythematosus quality of life (CLEQoL). Skindex 29+3 is a validated survey, adapted from the prior Skindex-16 and Skindex-29 surveys, which captures patient-reported outcomes in multiple domains, functioning, emotions, symptoms, body image/cosmetic issues, and photosensitivity (in the past week, how often…[eg have you been bothered], never, rarely, sometimes, often, all the time).12,15,16 Skindex 29+3 has been shown to have a high degree of correlation with CLASI-A and CLASI-D, particularly in the symptoms, emotions, and functioning domains.15 CLEQoL is another survey with strong reliability and validity, consisting of the same 32 questions from Skindex 29+3 with an additional four questions from vitiligo-specific quality of life (VitiQoL).17 Skin-related quality of life, which includes symptoms, are becoming its own important endpoint in clinical trials, such as with the recent FDA-approval of CLASI as an endpoint, and we hope to see the landscape of clinical trials have more focus on the skin and thus improve the treatment options for patients with CLE.
Current and Emerging Therapeutics for CLE
Hydroxychloroquine
Hydroxychloroquine (HCQ) is a drug that was FDA-approved in 1955 for use in SLE and DLE. Antimalarials such as hydroxychloroquine and chloroquine have multiple mechanisms which result in symptom relief in lupus and other autoimmune diseases. The primary immunomodulatory action of HCQ is the inhibition of toll-like receptors (TLRs), particularly those that sense nucleic acids (TLRs 7 and 9), which are located in endosomes.18 HCQ inhibits the acidification of endosomes required for TLRs to bind ligands and transmit signals, blocking processes such as antigen processing in macrophages and other antigen-presenting cells.18,19 It may also provide some photoprotective effect against ultraviolet (UV) light as a trigger for lupus flare, absorbing UV light in the skin in a concentration-dependent manner.20 Hydroxychloroquine is also widely used as first-line therapy for the treatment of CLE. A systematic review of twelve studies showed that a hydroxychloroquine dosage up to 400 mg/day is effective for most CLE patients, with a range of 50–97% efficacy.21 Due to long-term risk of retinopathy, SLE guidelines limit hydroxychloroquine doses to <5 mg/kg/day.22 One such study was a double-blinded, randomized, parallel-controlled phase III trial of 103 patients with active CLE (with or without SLE), which showed that mean CLASI score at week 16 was improved from baseline in both HCQ (mean change −4.6; 95% confidence interval (CI), −6.1 to −3.1; p< 0.0001) and placebo (mean change −3.2; 95% CI, −5.1 to −1.3; p=0.002) groups.23 The change in CLASI score was greater in the HCQ group, although the between-group difference was not statistically significant (p=0.197).23 The investigator’s global assessment was another endpoint used, which showed a greater percentage of “improved” and “remarkably improved” patients in the HCQ group compared to placebo, with a statistically significant difference between the groups (51.4% versus 8.7% in the placebo group; p = 0.0002).23 The success of trials such as this supports the efficacy of HCQ as a current first-line treatment for CLE. However, in some recalcitrant cases or those with adverse events, additional treatment options are needed.
Quinacrine
Quinacrine is another antimalarial drug with many varied mechanisms of action that are not wholly understood, including DNA intercalation and binding and telomerase and topoisomerase inhibition, which also provides antitumor effects.24 Other mechanisms of action suggested by the literature include inhibition of DNA and RNA polymerase, activation of p53-induced cell death, and inhibition of Nuclear Factor kappa-light-chain-enhancer of activated B cells (NF-κB), all with subsequent anti-inflammatory effects.24 The Office of New Drugs advised that quinacrine may be safe at 100 mg/day dose for rheumatic skin diseases such as lupus after the Pharmacy Compounding Advisory Committee raised safety concerns about quinacrine-associated aplastic anemia.25 Due to its long history of use as a malaria treatment, it is well known to be tolerable, with mostly minor reactions of mild headache, dizziness, or gastrointestinal symptoms and infrequent serious side effects.24 It may be used as adjuvant therapy for SLE and CLE patients who are intolerant or unresponsive to HCQ.25 However, in the past 30 years, its availability in the USA has become increasingly scarce, and it is not routinely covered by insurance.26 Very recently, a phase II blinded, randomized placebo-controlled clinical trial is being planned for quinacrine in CLE with or without SLE. This will be the first clinical trial specifically for quinacrine monotherapy in patients with CLE.
Belimumab
As B cells play a central role in the pathogenesis of CLE and SLE, such as in autoantibody production and antigen-presenting cells for T cell activation, B cell-targeting therapy holds potential for effective treatment. In 2011, belimumab became the first biologic approved for SLE, and in 2020 it was approved for lupus nephritis. Belimumab is a monoclonal antibody against B-lymphocyte stimulator (BlyS), also known as B cell-activating factor (BAFF), which inhibits binding to B cell receptors and thus prevents B-cell survival and differentiation into plasma cells.27,28
A phase III trial of belimumab at 10mg/kg (1mg/kg in SLE) was conducted using the SRI response rate at week 52 as the primary endpoint.29 It showed that belimumab plus standard therapy significantly improved SRI response rate and reduced SLE disease activity and severe flares, with comparable serious and severe adverse events, including infections, laboratory abnormalities, malignancies, and deaths across all groups.29 Belimumab has also been shown to be superior to placebo in inducing improvement and preventing flares of mucocutaneous manifestations of SLE in a meta-analysis of five phase III clinical trials (BLISS-52, BLISS-76, BLISS-NEA, EMBRACE, BLISS-SC; n=3086), using mucocutaneous BILAG and mucocutaneous SLEDAI-2K as endpoints.30 These clinical trials investigating belimumab focus on the treatment of SLE rather than CLE. In participants with refractory CLE (BELI-SKIN; EUDRA-CT, 2017–003051-35), a phase III multicenter trial was conducted with the primary endpoint of relative change in revised CLASI-A score at 24 weeks.31 The results were not statistically significant (mean change in CLASI-A score [95% CI], belimumab −0.33 [−0.44 to −0.22]; placebo −0.21 [−0.43 to 0.004]).32 This is the first major trial with belimumab specifically designed for CLE with skin-specific primary endpoints. Other studies support belimumab as an effective therapy for CLE with or without concomitant SLE. However, the efficacy is not well characterized using skin-specific endpoints. One observational, non-randomized study (BeRLiSS-JS 2.0, n=443) of SLE patients, including those with SCLE, CCLE, and ACLE, used CLASI score among its outcome variables.30 At 6 months, there was a significant decrease in CLASI-A score in ACLE (median CLASI-A at baseline versus 6 months (interquartile range), 3.0 (1.0–6.0) versus 1.0 (0.0–2.0); p<0.001) and SCLE patients (5.0 (2.0–7.0) versus 2.0 (0.0–5.0); p<0.001), but not CCLE (6.0 (3.0–7.0) versus 2.0 (1.0–6.0); p=0.380) patients treated with belimumab versus placebo.33 Although this study was observational and not randomized, it shows the potential efficacy of belimumab for some skin-specific symptoms.
Anifrolumab
Anifrolumab is a human monoclonal antibody to the receptor of type I IFNs, a central contributor to CLE and SLE pathogenesis.34 Type I IFN generates a pro-inflammatory environment by inducing both innate and adaptive immune system response, including B cell and T cell activation.2 An upregulated IFN gene signature has been identified in peripheral mononuclear cells of SLE patients.35 Anifrolumab targets the type I IFN receptor and has been shown to result in a IFN blockade, with downregulation of downstream gene pathways and proteins.36 Anifrolumab was approved in 2021 for treatment of moderate to severe SLE, and is generally well tolerated over 52 weeks with an acceptable safety profile. In a pooled analysis of 925 patients with moderate to severe SLE, anifrolumab was associated with an increased incidence of herpes zoster and respiratory tract infections.37
The history of clinical trials involving anifrolumab exemplifies why the primary endpoint is of critical importance. A previous phase III trial that used SRI-4 response at week 52 as its primary endpoint did not show a significant effect.38 A second phase III trial, TULIP-2, then used a secondary endpoint from the first phase III trial as the primary endpoint. This was a phase III trial studying anifrolumab (300 mg, n=362) in patients with SLE which used a primary endpoint of a BICLA response at week 52.10 Results showed that 47.8% in the anifrolumab group versus 31.5% in the placebo group had a BICLA response at week 52 (difference, 16.3 percentage points; 95% CI, 6.3 to 26.3; p=0.001).10 CLASI-50 at week 12 was included as one of five secondary endpoints among patients with moderate-to-severe cutaneous activity (CLASI≥10) at baseline.10 Results showed that the CLASI-50 endpoint was met in 49.0% of the patients (24 of 49) receiving anifrolumab and in 25.0% (10 of 40) receiving placebo (adjusted difference, 24.0 percentage points; 95% CI, 4.3 to 43.6; adjusted p=0.04).10 These results demonstrated potential promise of anifrolumab as a treatment for skin. Following the success of this trial showing that anifrolumab may improve cutaneous symptoms of lupus, a new phase III trial (LAVENDER; NCT06015737) is investigating anifrolumab in patients with CLE with a primary endpoint of CLASI-70.39 This trial is highly anticipated as it may lead to FDA approval of anifrolumab for use in CLE specifically.
Litifilimab
Litifilimab is another drug that may potentially be approved for CLE and cutaneous manifestations of SLE. It is an antibody against blood dendritic cell antigen 2 (BDCA2), located uniquely on plasmacytoid dendritic cells (PDCs), which then suppresses type I IFNs as well as cytokine and chemokine production involved in SLE and CLE pathogenesis.40,41 Administration of litifilimab has been shown to reduce IFN gene signature scores and IFN concentrations, which correlate with clinical response to the drug.42
A modified phase II trial (LILAC) was conducted in 102 participants with SLE, arthritis, and active skin disease, assigned to either litifilimab 450mg or placebo.40 The initial primary endpoint was the change in total number of active joints (swollen and tender joints) at week 24.40 There was significant greater reduction in active joints in the litifilimab group compared to placebo (15.0±1.2 with litifilimab versus 11.6±1.3 with placebo; mean difference, –3.4; 95% CI, –6.7 to –0.2; p=0.04), with two cases of herpes zoster and one case of herpes keratitis for adverse events associated with litifilimab.40 Skin-related secondary endpoints such as CLASI-50 and change in CLASI-A score showed differences between treatment and placebo arms, with a reduction of at least 7 points from baseline in CLASI-A score in 56% of the litifilimab group and 34% of the placebo group (least-squares mean difference, 21.6 percentage points; 95% CI, 0.1 to 43.1).40 A separate CLE study showed statistically significant improvement on litifilimab. 132 participants with CLE with or without systemic manifestations received 50mg, 150mg, or 450mg of litifilimab or placebo.43 Each group showed a statistically significant difference in change from baseline in CLASI-A score at week 16 compared to placebo (−24.3 percentage points; 95% CI, −43.7 to −4.9) in the 50-mg group, −33.4 (95% CI, −52.7 to −14.1) in the 150-mg group, and −28.0 (95% CI, −44.6 to −11.4) in the 450-mg group.43 After the success of the primary endpoint of this study, a phase II/III trial (as CLASI was not yet accepted as a primary outcome measure for phase III trials at the commencement of this study) is currently underway (Amethyst, NCT05531565).44 It consists of an estimated 474 participants with CLE with or without SLE with a baseline CLASI-A score ≥10, and its primary endpoint is the percentage with CLASI-70 response at week 24.44 This study is ongoing. We hope it will provide further results as to whether litifilimab is an effective treatment for CLE and cutaneous manifestations of SLE, potentially leading to approval of a drug for cutaneous lupus.
Deucravacitinib
Deucravacitinib is an oral selective allosteric inhibitor of tyrosine kinase 2 (TYK2) that also reduces type I IFN gene signature, as well as downstream signaling such as interleukin 10 (IL-10), IL-12, and IL-23.45,46 It binds and locks TYK2 in an inactive state, which distinguishes it from JAK inhibitors that bind the active domains.46 It is currently approved for treatment of plaque psoriasis and is currently undergoing clinical trials for both SLE and CLE. A phase II trial was conducted for both SLE and CLE (PAISLEY-SLE, PAISLEY-CLE) for discoid and subacute CLE, in which deucravacitnib showed an acceptable safety profile, with higher rates of infections and cutaneous events including rash and acne and no opportunistic/tuberculosis infections, major adverse cardiovascular events, thrombotic events, or deaths.46 For the SLE trial, the primary endpoint was the SLE Responder Index 4 (SRI-4) response at week 32, which showed increased response rates in all treatment groups compared to placebo (58% with deucravacitinib 3 mg twice daily compared to 34% with placebo; odds ratio (OR) 2.8 [95% CI, 1.5 to 5.1]; p<0.001 versus placebo), 50% with 6 mg twice daily (OR 1.9; 95% CI, 1.0 to 3.4; p=0.02 versus placebo), and 45% with 12 mg once daily (OR 1.6 [95% CI, 0.8, 2.9]; nominal p=0.08 versus placebo).46 CLASI-50 was used as a secondary endpoint, and CLASI-50 response was significantly higher than placebo at week 48 (58% vs 34%).46
In the PAISLEY-CLE trial, participants had active DLE and/or SCLE with or without SLE (patients with SLE were limited to ≤50% of the population) with a baseline CLASI-A score ≥8.47 The trial met its primary endpoint with improvement in mean percent CLASI-A change from baseline compared to placebo at 16 weeks (placebo −28.4% vs deucravacitinib 3 mg BID −47.5% (p=0.0670) and 6 mg BID −50.0% (p=0.0385).47 Additionally, more patients treated with deucravacitinib achieved CLASI-50 (19.0% (placebo) vs 56.7% (3mg BID) [p=0.0092] and 52.3% (6mg BID) [p=0.0193]) and CLASI-70 (15.9% vs 49.5% [p=0.0184] and 29.5% [p=0.2713].47 The skin-focused endpoints showed meaningful results in both the SLE and CLE trials. Deucravacitinib then progressed to two phase III SLE trials which are currently underway, POETYK SLE-1 (NCT05617677) and POETYK SLE-2 (NCT05620407).48 Given the decision to pursue an SLE indication, the primary endpoint is the SRI-4.48 The CLASI is a secondary endpoint for the phase III trials. Additional trials that are focused on CLE and skin as the primary endpoint would be needed to make the drug accessible to patients who have CLE.
Enpatoran
Enpatoran is an orally-administered, highly selective small molecule inhibitor of toll-like receptor 7/8 (TLR7/8), modulating processes in CLE and SLE pathogenesis.41 Studies have shown that enpatorn reduced proinflammatory cytokines such as IL-6 and interferon α in a dose-dependent manner.49,50 A Phase 1b trial showed that enpatoran was well-tolerated and demonstrated favorable safety profiles in patients with SLE and CLE, with rates of treatment-emergent adverse events comparable to placebo (60.6% to 64.2%).51,52 Enpatoran underwent a phase II clinical trial (WILLOW; NCT05162586) with two cohorts; cohort A for CLE and cohort B for SLE.53 In cohort A, various doses of enpatoran and placebo were studied in 100 participants with CLE or SLE with active rash. At week 16, a significant dose response was detected in its primary outcome measures, which was reduction of CLASI-A from baseline (p=0.0002).53 Additionally, up to 92.3% of patients achieved a CLASI-50 at week 24, and up to 60.9% achieved a CLASI-70 response compared to 38.5% and 11.5% in placebo groups, respectively.54 Phase 3 trials are being planned.
Iberdomide
Iberdomide is a drug that was tested in an SLE population, and although results in skin were potentially promising, it will not proceed to a CLE population. Iberdomide is a cereblon modulator promoting the degradation of the transcription factors Ikaros and Aiolos involved in leukocyte development.55 It was evaluated for treatment of SLE in a phase II trial (n=288).55 Its primary endpoint of SRI-4 at 24 weeks was met in 54% of those treated with the highest dose of iberdomide (0.45mg) compared to 35% in the placebo group (adjusted difference, 19.4 percentage points; 95% CI, 4.1 to 33.4; p=0.01).55 CLASI-50 was also included as a secondary endpoint; however, it did not show a statistically significant difference between the treatment versus placebo groups in the 64 patients with a CLASI-A ≥10 at baseline (14.2 percentage points (95% CI, −19.5 to 44.5) in the 0.45-mg group, 5.3 percentage points (95% CI, −27.6 to 39.4) in the 0.30-mg group, and 24.0 percentage points (95% CI, −12.4 to 53.1) in the 0.15-mg group).55 A sub-analysis of patients with SLE with CLE showed that iberdomide is potentially more effective in CLE than in SLE; in patients with baseline CLASI-A≥8, mean CLASI-A improvement was 39.7% for iberdomide 0.45 mg versus 20.1% for placebo at week 4 (p=0.032), with a trend of continued improvement through week 24 (66.7% vs 54.2%; p=0.295).56 The proportion that met CLASI-50 at week 24 was greater for iberdomide 0.45 mg versus placebo in patients with SCLE (91.7% vs 52.9%, p=0.035) and CCLE (62.1% vs 27.8%; p=0.029).56 This underscores the importance of conducting clinical trials in a population focused on patients with CLE.
Conclusion
The landscape of clinical trials is shifting towards incorporating more skin-related endpoints, with ongoing trials that use CLASI as a primary endpoint. Novel emerging therapeutics for CLE are being evaluated in ongoing clinical trials, including anifrolumab (LAVENDER), litifilimab (AMETHYST), and Enpatoran (WILLOW) (Figure 1, Table 1). Historically, SLE clinical trials showed promising skin-related outcomes as secondary endpoints; however, these drugs have not received FDA approval specifically for CLE, which limits their availability and insurance coverage for patients with only CLE. This gap highlights the critical importance of using CLASI in trials specifically designed for CLE populations. As CLASI has become an accepted primary endpoint for clinical trials, drug development is shifting to prioritize cutaneous outcomes and to use endpoints that measure skin-specific effects. This targeted approach represents a fundamental change that may ultimately increase FDA-approved therapies specifically for CLE and expand treatment options for patients with CLE. While the field has already made substantial progress in CLE therapeutics, continued support for clinical trials prioritizing cutaneous endpoints is critical to improve outcomes for patients with cutaneous manifestations of CLE and SLE.
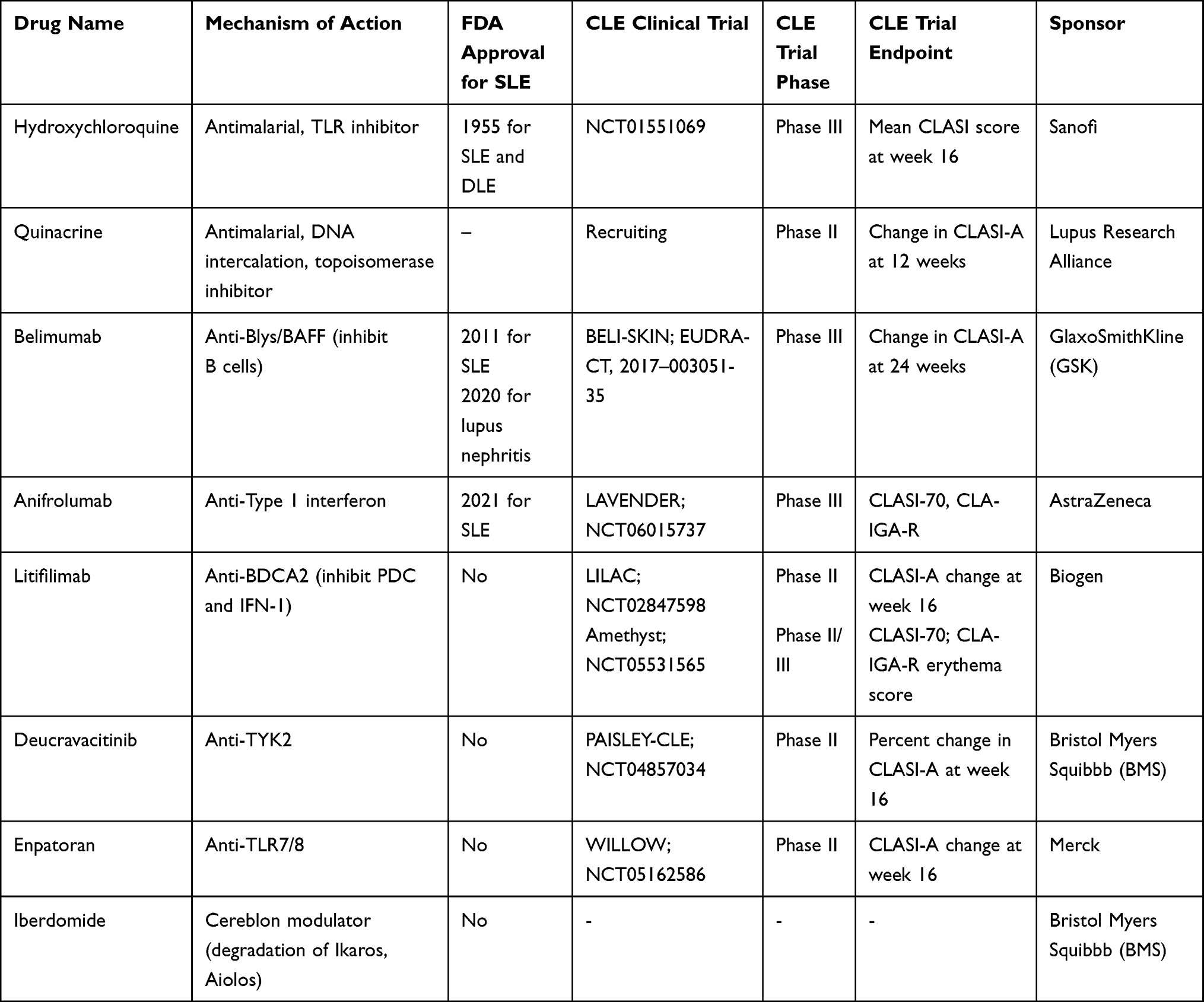 |
Table 1 Summary of SLE Drugs and Emerging Therapies for CLE |
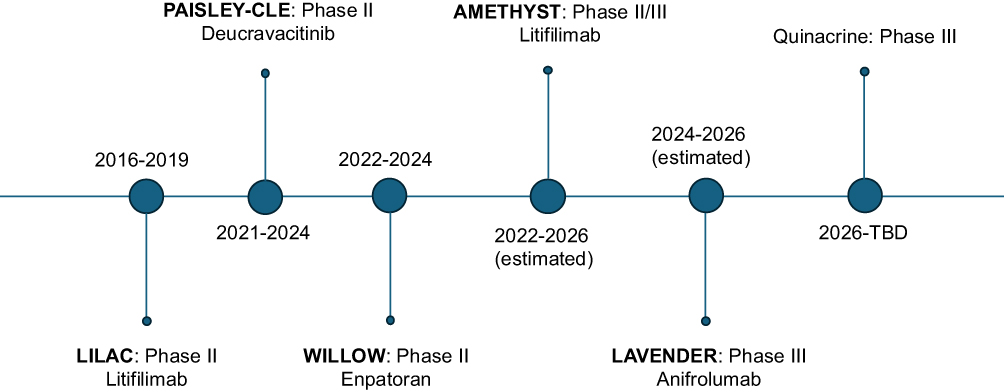 |
Figure 1 Timeline of landmark CLE clinical trials. Timeline of important CLE clinical trials including the name of the trial, the drug under investigation, phase of the trial, and the years that the trial was being conducted. |
IRB Approval Status
Ethics approval was not required for this review paper as it involved review of published clinical trials, exempting it from ethics review under institutional guidelines.
IRB Use of AI
AI was not used in manuscript composition.
Abbreviations
ACLE, acute CLE; BAFF, B cell-activating factor; BICLA, BILAG-Based Composite Lupus; BID, twice a day; BILAG, British Isles Lupus Assessment Group; BlyS, B-lymphocyte stimulator; CCLE, chronic CLE; CLE, Cutaneous Lupus Erythematosus; CLASI, Cutaneous LE Disease Area and Severity Index; CLASI-A, Cutaneous LE Disease Area and Severity Index- Activity; CLASI-D, Cutaneous LE Disease Area and Severity Index- Damage; CLASI-50, 50% reduction in Cutaneous LE Disease Area and Severity Index Activity score; CLASI-70, 70% reduction in Cutaneous LE Disease Area and Severity Index Activity score; CLASI-90, 90% reduction in Cutaneous LE Disease Area and Severity Index Activity score; CLASI-100, 100% reduction in Cutaneous LE Disease Area and Severity Index Activity score; DLE, discoid LE; FDA, US Food and Drug Administration; HCQ, hydroxychloroquine; IL, interleukin; LE, lupus erythematosus; SCLE, subacute CLE; SLE, Systemic Lupus Erythematosus; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index; SRI, SLE Responder Index; TLR, toll-like-receptor; Type I IFN, Type I interferon.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Author Contributions
V.W., E.W., and L.L.A.G. conceived and designed the review paper. E.W. created the visualization, wrote the original draft of the paper, and substantially revised the article. S.J. and S.S. substantially revised the article. All authors contributed to reviewing and editing the manuscript. V.W. reviewed and revised the article and supervised the research. All authors V.W., E.W., L.L.A.G., S.J., S.S. gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was funded by the National Institutes of Health-USA (NIH-USA) grants R01AR071653 (to VPW) and NIH (NIAMS) grant 1UC2AR081039 (to VPW), and the United States Department of Veterans Affairs Merit Review BX005921 (Veterans Health Administration, Office of Research and Development and Biomedical Laboratory Research and Development, to VPW).
Disclosure
VPW has grants from Celgene, Janssen, Pfizer, Biogen, Gilead, Corbus Pharmaceuticals, Genentech, AstraZeneca, Viela, Syntimmune, Amgen, Regeneron, Argenx, CSL Behring, Ventus, q32 Bio, BMS, Horizon, Rome Pharmaceuticals; has consulted for Celgene, Genentech, Janssen, Lilly, Pfizer, Biogen, BMS, Gilead, Amgen, Medscape, Nektar, Incyte, EMD Sorona, CSL Behring, Principia, Crisalis, Viela Bio, Argenx, Kwoya Kirin, Regeneron, Principia, AstraZeneca, Abbvie, Octapharma, GSK, Astra-Zeneca, Cugene, UCB, Corcept, Beacon Bioscience, Rome Pharmaceuticals, Horizon, Gilead, Merck, Kezar, Sanofi, Bayer, Akari, Calyx, Cabaletta Bio and received personal fees from Nuvig Pharmaceuticals, Takeda Pharmaceuticals, Immunovant, Anaptysbio, Evommune, Innovaderm, Boehringer Ingelheim Pharmaceuticals, Quotient Therapeutics, Duality Biologics, Gycoera, Almirall, Atticus, Inmagene, Exo Therapeutics, Novartis, Xencor, Architect Therapeutics, Bimmunity, during the conduct of the study; In addition, Dr Victoria Werth has a patent CLASI with royalties paid to many, a patent CLA-IGA with royalties paid to man.
The University of Pennsylvania owns the copyright for the CLASI.
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the paper apart from those disclosed.
References
1. Gilliam JN, Sontheimer RD. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol. 1981;4(4):471–10. doi:10.1016/S0190-9622(81)80261-7
2. Klein B, Billi AC, Abernathy-Close L, Kahlenberg JM. Cutaneous lupus erythematosus — from pathogenesis to targeted therapy. Nat Rev Rheumatol. 2025;21(12):703–718. doi:10.1038/s41584-025-01318-6
3. Kuhn A, Gensch K, Haust M, et al. Photoprotective effects of a broad-spectrum sunscreen in ultraviolet-induced cutaneous lupus erythematosus: a randomized, vehicle-controlled, double-blind study. J Am Acad Dermatol. 2011;64(1):37–48. doi:10.1016/j.jaad.2009.12.053
4. Chang AY, Werth VP. Treatment of cutaneous lupus. Curr Rheumatol Rep. 2011;13(4):300–307. doi:10.1007/s11926-011-0180-z
5. Stull C, Sprow G, Werth VP. Cutaneous involvement in systemic lupus erythematosus: a review for the rheumatologist. J Rheumatol. 2023;50(1):27–35. doi:10.3899/jrheum.220089
6. Elmgren J, Nyberg F. Clinical aspects of cutaneous lupus erythematosus. Front Med Lausanne. 2023;9:984229. doi:10.3389/fmed.2022.984229
7. Bombardier C, Gladman DD, Urowitz MB, et al. Derivation of the sledai. A disease activity index for lupus patients. Arthritis Rheum. 1992;35(6):630–640. doi:10.1002/art.1780350606
8. Hay EM, Bacon PA, Gordon C, et al. The BILAG index, a reliable and valid instrument for measuring clinical disease activity in systemic lupus erythematosus. QJM: Int J Med. 1993;86(7):447–458.
9. Furie RA, Petri MA, Wallace DJ, et al. Novel evidence-based systemic lupus erythematosus responder index. Arthritis Rheum. 2009;61(9):1143–1151. doi:10.1002/art.24698
10. Morand EF, Furie R, Tanaka Y, et al. Trial of anifrolumab in active systemic lupus erythematosus. N Engl J Med. 2020;382(3):211–221. doi:10.1056/NEJMoa1912196
11. Albrecht J, Taylor L, Berlin JA, et al. The CLASI (cutaneous lupus erythematosus disease area and severity index): an outcome instrument for cutaneous lupus erythematosus. J Invest Dermatol. 2005;125(5):889–894. doi:10.1111/j.0022-202X.2005.23889.x
12. Klein R, Moghadam-Kia S, LoMonico J, et al. Development of the CLASI as a tool to measure disease severity and responsiveness to therapy in cutaneous lupus erythematosus. Arch Dermatol. 2011;147(2):203. doi:10.1001/archdermatol.2010.435
13. Faden DF, Xie L, Stone CJ, et al. Cutaneous lupus erythematosus: expanding clinical trial eligibility criteria based on quality of life data. J Am Acad Dermatol. 2024;91(6):1203–1205. doi:10.1016/j.jaad.2024.07.1478
14. Zhang AJ, Perez-Chada LM, Werth VP, Merola JF. Expert consensus achieved on a working core outcome set for cutaneous lupus erythematosus research in survey following the 5th international conference on cutaneous lupus erythematosus (ICCLE). Lupus Sci Med. 2024;11(1):e001165. doi:10.1136/lupus-2024-001165
15. Sprow G, Dan J, Feng R, Werth VP. Comparing dermatologic patient-reported outcome measures in cutaneous lupus erythematosus. Lupus Sci Med. 2022;9(1):e000827. doi:10.1136/lupus-2022-000827
16. Chren -M-M. The skindex instruments to measure the effects of skin disease on quality of life. Dermatol Clin. 2012;30(2):231–236. doi:10.1016/j.det.2011.11.003
17. Ogunsanya ME, Cho SK, Hudson A, Chong BF. Validation and reliability of a disease-specific quality-of-life measure in patients with cutaneous lupus erythematosus. Br J Dermatol. 2019;180(6):1430–1437. doi:10.1111/bjd.17636
18. Torigoe M, Sakata K, Ishii A, Iwata S, Nakayamada S, Tanaka Y. Hydroxychloroquine efficiently suppresses inflammatory responses of human class-switched memory B cells via toll-like receptor 9 inhibition. Clin Immunol. 2018;195:1–7. doi:10.1016/j.clim.2018.07.003
19. Fox RI. Mechanism of action of hydroxychloroquine as an antirheumatic drug. Semin Arthritis Rheumatism. 1993;23(2):82–91. doi:10.1016/S0049-0172(10)80012-5
20. Sardana K, Sinha S, Sachdeva S. Hydroxychloroquine in dermatology and beyond: recent update. Indian Dermatol Online J. 2020;11(3):453. doi:10.4103/idoj.IDOJ_280_20
21. Shipman WD, Vernice NA, Demetres M, Jorizzo JL. An update on the use of hydroxychloroquine in cutaneous lupus erythematosus: a systematic review. J Am Acad Dermatol. 2020;82(3):709–722. doi:10.1016/j.jaad.2019.07.027
22. Jorge AM, Mancini C, Zhou B, et al. Hydroxychloroquine dose per ophthalmology guidelines and the risk of systemic lupus erythematosus flares. JAMA. 2022;328(14):1458. doi:10.1001/jama.2022.13591
23. Yokogawa N, Eto H, Tanikawa A, et al. Effects of hydroxychloroquine in patients with cutaneous lupus erythematosus: a multicenter, double-blind, randomized, parallel-group trial. Arthritis Rheumatol. 2017;69(4):791–799. doi:10.1002/art.40018
24. Ehsanian R, Van Waes C, Feller SM. Beyond DNA binding - a review of the potential mechanisms mediating quinacrine’s therapeutic activities in parasitic infections, inflammation, and cancers. Cell Commun Signal. 2011;9(1):13. doi:10.1186/1478-811X-9-13
25. Mittal L, Werth VP. The quinacrine experience in a population of patients with cutaneous lupus erythematosus and dermatomyositis. J Am Acad Dermatol. 2017;77(2):374–377. doi:10.1016/j.jaad.2017.03.027
26. Yan D, Borucki R, Sontheimer RD, Werth VP. Candidate drug replacements for quinacrine in cutaneous lupus erythematosus. Lupus Sci Med. 2020;7(1):e000430. doi:10.1136/lupus-2020-000430
27. Dubey AK, Handu SS, Dubey S, Sharma P, Sharma KK. Belimumab: first targeted biological treatment for systemic lupus erythematosus. J Pharmacol Pharmacotherapeutics. 2011;2(4):317–319. doi:10.4103/0976-500X.85930
28. Wise LM, Stohl W. Belimumab and rituximab in systemic lupus erythematosus, a tale of two B cell-targeting agents. Front Med. 2020;7.
29. Furie R, Petri M, Zamani O, et al. A Phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63(12):3918–3930. doi:10.1002/art.30613
30. Grosso G, Giannopoulou N, Tsoi A, et al. Belimumab efficacy in mucocutaneous manifestations of systemic lupus erythematosus: a large post hoc analysis of five phase III clinical trials. Rheumatology. 2025;64(7):4257–4266. doi:10.1093/rheumatology/keaf145
31. Xie L, Lopes Almeida Gomes L, Stone CJ, Faden DF, Werth VP. An update on clinical trials for cutaneous lupus erythematosus. J Dermatol. 2024;51(7):885–894. doi:10.1111/1346-8138.17161
32. EudraCT Number 2017-003051-35 - Clinical trial results - EU Clinical Trials Register.
33. Bracalenti M, Zen M, Bianchi B, et al. Efficacy of belimumab on different joint and skin manifestations of systemic lupus erythematosus: real-life data from a new multicentric, nationwide Italian Cohort (BeRLiSS-JS 2.0). Biologics. 2025;19:651–663. doi:10.2147/BTT.S536660
34. Anderson E, Furie R. Anifrolumab in systemic lupus erythematosus: current knowledge and future considerations. Immunotherapy. 2020;12(5):275–286. doi:10.2217/imt-2020-0017
35. Crow MK. Type I interferon in the pathogenesis of lupus. J Immunol. 2014;192(12):5459–5468. doi:10.4049/jimmunol.1002795
36. Baker T, Sharifian H, Newcombe PJ, et al. Type I interferon blockade with anifrolumab in patients with systemic lupus erythematosus modulates key immunopathological pathways in a gene expression and proteomic analysis of two phase 3 trials. Ann Rheumatic Dis. 2024;83(8):1018–1027. doi:10.1136/ard-2023-225445
37. Tummala R, Abreu G, Pineda L, et al. Safety profile of anifrolumab in patients with active SLE: an integrated analysis of phase II and III trials. Lupus Sci Med. 2021;8(1):e000464. doi:10.1136/lupus-2020-000464
38. Furie RA, Morand EF, Bruce IN, et al. Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus (TULIP-1): a randomised, controlled, phase 3 trial. Lancet Rheumatol. 2019;1(4):e208–e219. doi:10.1016/S2665-9913(19)30076-1
39. Study details | NCT06015737 | a 2-stage, phase III study to investigate the efficacy and safety of anifrolumab in adults with chronic and/or subacute cutaneous lupus erythematosus | clinicalTrials.gov.
40. Furie RA, van Vollenhoven RF, Kalunian K, et al. Trial of anti-BDCA2 antibody litifilimab for systemic lupus Erythematosus. N Engl J Med. 2022;387(10):894–904. doi:10.1056/NEJMoa2118025
41. Cho YM, Furie R. The development of litifilimab (BIIB 059) for cutaneous and systemic lupus erythematosus. Immunotherapy. 2024;16(1):15–20. doi:10.2217/imt-2023-0086
42. Furie R, Werth VP, Milliman E, et al. Pharmacodynamic effects of litifilimab in lupus in a randomized, placebo-controlled phase 2 study: rapid and sustained reductions in type I interferon-associated gene expression and cytokines. Arthritis Rheumatol. 2025;77(12):1726–1738. doi:10.1002/art.43271
43. Werth VP, Furie RA, Romero-Diaz J, et al. Trial of anti-BDCA2 antibody litifilimab for cutaneous lupus erythematosus. N Engl J Med. 2022;387(4):321–331. doi:10.1056/NEJMoa2118024
44. Study details | NCT05531565 | a 2-part study to learn whether litifilimab (BIIB059) injections can improve symptoms of adult participants who have active cutaneous lupus erythematosus | clinicalTrials.gov.
45. Wrobleski ST, Moslin R, Lin S, et al. Highly selective inhibition of tyrosine kinase 2 (TYK2) for the treatment of autoimmune diseases: discovery of the allosteric inhibitor BMS-986165. J Med Chem. 2019;62(20):8973–8995. doi:10.1021/acs.jmedchem.9b00444
46. Morand E, Pike M, Merrill JT, et al. Deucravacitinib, a tyrosine kinase 2 inhibitor, in systemic lupus erythematosus: a Phase II, randomized, double-blind, placebo-controlled trial. Arthritis Rheumatol. 2023;75(2):242–252. doi:10.1002/art.42391
47. Merola JF, Gottlieb AB, Aranow C, et al. POS0781 EFFICACY AND SAFETY OF ORAL DEUCRAVACITINIB IN PATIENTS WITH CUTANEOUS MANIFESTATIONS OF LUPUS ERYTHEMATOSUS: RESULTS FROM PAISLEY CLE, A GLOBAL, RANDOMIZED, PLACEBO-CONTROLLED, PHASE 2 TRIAL. Ann Rheumatic Dis. 2025;84:940–941. doi:10.1016/j.ard.2025.06.141
48. Arriens C, Morand EF, Askanase AD, et al. Design of two randomized, placebo-controlled, phase 3 trials of deucravacitinib, an oral, selective, allosteric TYK2 inhibitor, in systemic lupus erythematosus. Adv Ther. 2025;42(11):5830–5844. doi:10.1007/s12325-025-03299-0
49. Vlach J, Bender AT, Przetak M, et al. Discovery of M5049: a novel selective toll-like receptor 7/8 inhibitor for treatment of autoimmunity. J Pharmacol Exp Ther. 2021;376(3):397–409. doi:10.1124/jpet.120.000275
50. Port A, Shaw JV, Klopp‐Schulze L, et al. Phase 1 study in healthy participants of the safety, pharmacokinetics, and pharmacodynamics of enpatoran (M5049), a dual antagonist of toll-like receptors 7 and 8. Pharmacol Res Perspect. 2021;9(5):e00842. doi:10.1002/prp2.842
51. Witte T, Fernandez-Ruiz R, Abramova N, et al. Enpatoran, a first-in-class, selective, orally administered toll-like receptor 7/8 inhibitor, in systemic and cutaneous lupus erythematosus: results from a randomised, placebo-controlled phase Ib study. Lupus Sci Med. 2025;12(2):e001705. doi:10.1136/lupus-2025-001705
52. EMD Serono presents results on efficacy and safety of enpatoran in SLE at EULAR 2025. EMD Serono.
53. Pearson D, Morand E, Wenzel J, et al. RANDOMIZED, PLACEBO-CONTROLLED PHASE II STUDY OF ENPATORAN, A SMALL MOLECULE TOLL-LIKE RECEPTOR 7/8 INHIBITOR, IN CUTANEOUS LUPUS ERYTHEMATOSUS: RESULTS FROM COHORT A. J Rheumatol. 2025;52(Suppl 1):11. doi:10.3899/jrheum.2025-0390.O010
54. EMD Serono presents positive phase 2 data for enpatoran demonstrating reduction in disease activity in patients with CLE and SLE with active lupus rash. EMD Serono.
55. Merrill JT, Werth VP, Furie R, et al. Phase 2 trial of iberdomide in systemic lupus erythematosus. N Engl J Med. 2022;386(11):1034–1045. doi:10.1056/NEJMoa2106535
56. Werth VP, Merrill JT, Furie R, et al. Effect of iberdomide on cutaneous manifestations in systemic lupus erythematosus: a randomized phase 2 clinical trial. J Am Acad Dermatol. 2025;92(3):435–443. doi:10.1016/j.jaad.2024.09.074
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.