Back to Journals » Clinical Ophthalmology » Volume 16
The Vivity Extended Range of Vision IOL vs the PanOptix Trifocal, ReStor 2.5 Active Focus and ReStor 3.0 Multifocal Lenses: A Comparison of Patient Satisfaction, Visual Disturbances, and Spectacle Independence
Authors Hovanesian JA ![]() , Jones M, Allen Q
, Jones M, Allen Q
Received 15 November 2021
Accepted for publication 29 December 2021
Published 18 January 2022 Volume 2022:16 Pages 145—152
DOI https://doi.org/10.2147/OPTH.S347382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Dr Scott Fraser
Video abstract presented by John Hovanesian.
Views: 33605
John A Hovanesian,1 Michael Jones,2 Quentin Allen3
1Harvard Eye Associates, Laguna Hills, CA, USA; 2Quantum Vision Centers, Swansea, IL, USA; 3Florida Vision Institute, Stuart, FL, USA
Correspondence: John A Hovanesian
Harvard Eye Associates, 23961 Calle De La Magdalena, #300, Laguna Hills, CA, 92653, USA
Tel +1 949 951 2020
Fax +1 949 951 9244
Email [email protected]
Purpose: To compare patient-reported outcomes (PROs) after intraocular lens (IOL) implantation with the AcrySof IQ Vivity IOL or Vivity Toric IOL to those achieved with other multifocal IOLs.
Patients and Methods: Prospective, open-label, multicenter analysis of PROs, including spectacle independence, dysphotopsia, and overall satisfaction among patients who underwent cataract surgery at least 1 month previously with bilateral Vivity or Vivity Toric lenses (n=60). Results were compared to outcomes from two similar prospective studies of bilateral AcrySof IQ PanOptix or PanOptix Toric trifocal IOLs (n = 59), blended AcrySof ReSTOR 2.5/3.0 IOLs (n=72) or bilateral ReSTOR ActiveFocus 2.5 D IOLs with a mini-monovision target [n = 95]).
Results: Patients in the Vivity cohort were significantly less likely to notice glare and halo in dim light (85% “none” or “just a little”) compared to PanOptix (69%, p< 0.03), 2.5 mini-monovision (75%, p< 0.05) or 2.5/3.0 (71%, p< 0.05) patients. Complete spectacle independence for all visual activities combined (never need glasses) with Vivity was comparable to the mini-monovision and 2.5/3.0 groups (33%, 36%, and 31%, respectively) but significantly lower than in the PanOptix cohort (83%, p < 0.0001). Satisfaction was high across all groups. There were no statistically significant differences in best-corrected visual acuity, and no new safety concerns were reported.
Conclusion: The AcrySof IQ Vivity extended depth of focus IOL offers an expanded range of vision and better spectacle independence than has typically been achieved with traditional monofocal IOLs, with high rates of satisfaction and a favorable dysphotopsia profile compared to diffractive multifocal IOLs.
Keywords: cataract surgery, spectacle independence, glare, multifocal intraocular lens
Plain-Language Summary
In this prospective, open-label, multicenter analysis evaluating patient-reported outcomes 1 month after scheduled cataract surgery, patients reported lower rates of dysphotopsia with the AcrySof IQ Vivity IOL compared to other multifocal IOLs tested, but were more likely to need spectacles for reading than patients with PanOptix IOLs.
Introduction
Older Americans more likely than in previous generations to be working and active, leading to increased visual demands and expectations of cataract surgery.1 Internet and smart phone usage by Americans over age 65 has risen significantly in the past decade,2,3 increasing the need for functional vision and spectacle independence at near, intermediate and distance post-cataract surgery.4,5
Historically, diffractive multifocal IOLs have provided improved visual acuity at near and intermediate distances and a greater likelihood of spectacle independence than monofocal IOLs.6–9 However, patients implanted with these IOLs have noted more frequent dysphotopsia (unwanted visual phenomena) and worse contrast sensitivity, especially in low-light or glare conditions, than do patients implanted with monofocal lenses.7–9 In guiding patients who are considering cataract surgery with advanced technology IOLs, it is important for surgeons to understand not only the objective visual acuity outcomes achieved in clinical trials, but also patients’ subjective experience with the IOLs.
The AcrySof IQ ReSTOR +3.0 D multifocal IOL (Alcon, Ft. Worth, Texas), along with its toric counterpart, has been widely perceived by surgeons as providing distance and near vision with some sacrifice in intermediate, while the subsequent ReSTOR +2.5 D helped patients achieve distance and intermediate with some limitations at near. The Panoptix trifocal IOL addressed all three ranges of vision.
Our previous work compared patient-reported outcomes (PROs), including unwanted visual phenomena, satisfaction, and spectacle independence, among patients who underwent cataract surgery with all of these lenses. Specifically, we examined blended, bilateral, or mini-monovision approaches using the AcrySof IQ ReStor +2.5 D and ReStor +3.0 D.10 These cohorts were compared with each other and with patients implanted with bilateral PanOptix.11 We found that the mini-monovision cohort achieved better spectacle independence, particularly at intermediate distances, and lower rates of dysphotopsia than the blended or bilateral multifocal groups, although patient satisfaction was similar across all three cohorts.10 Compared to these cohorts, bilateral PanOptix trifocal IOLs provided higher rates of patient satisfaction, much higher rates of complete spectacle independence, but also slightly higher rates of dysphotopsia.11
Recently, a new IOL, the AcrySof IQ Vivity IOL (Alcon), was introduced. This IOL is the first to mitigate the effects of presbyopia with nondiffractive, extended-depth-of-focus (EDOF) optics. In clinical trials, the lens was shown to deliver monofocal-quality distance vision with excellent intermediate and functional near vision, while maintaining a monofocal-like visual disturbance profile.12 In a prospective study of early real-world experience, Italian researchers confirmed that the lens provided excellent distance and intermediate, while patients needed some spectacle correction at 30 cm.13
To date, patient-reported satisfaction beyond glare/halo has not been compared between the AcrySof IQ PanOptix and the AcrySof IQ Vivity IOLs. This study was designed to assess how satisfaction rates, spectacle independence, and unwanted visual phenomena with the AcrySof IQ Vivity IOL compare to PROs with the multifocal IOL cohorts previously evaluated.
Materials and Methods
This trial was a prospective, open-label, multicenter analysis of PROs among patients who underwent bilateral cataract surgery at least 1 month previously with AcrySof IQ Vivity or Vivity Toric extended depth of focus IOLs, with a target of plano sphere in both eyes. Comparisons were made to the cohort of PanOptix trifocal patients and two previous cohorts of multifocal IOL patients (blended or mini-monovision) who were recruited prospectively and had responded to a similar PRO questionnaire in a similar postoperative time frame.10,11 In those studies, PanOptix patients received either the PanOptix or the PanOptix toric implant bilaterally with a target of plano sphere in both eyes. Among multifocal patients, the “2.5 mini-monovision” cohort received the AcrySof IQ ReStor ActiveFocus +2.5 D or AcrySof IQ ReStor ActiveFocus +2.5 D toric implant bilaterally, with the dominant eye targeted for emmetropia and the nondominant eye targeted for −0.5 D sphere. The blended or “2.5/3.0” cohort was implanted with the AcrySof IQ ReStor ActiveFocus +2.5 D implant in the dominant eye and the AcrySof IQ ReStor +3.0 D multifocal lens in the nondominant eye.
Across all cohorts, all eyes underwent phacoemulsification cataract surgery using either a manual or a femtosecond laser-assisted technique, with a target refraction as close to the established refractive target as the available lens powers allowed, erring on the side of the first myopic lens choice when necessary. Patients were excluded from all cohorts if they had significant ocular pathology that could alter their perception of the outcome of surgery, or if they had more than grade 1 posterior capsule opacity (PCO).
In both the present study and our previously-published PanOptix study,11 patients were excluded if they had residual refractive error in either eye of >0.5 D sphere or >0.75 D cylinder. To account for the difference in exclusion factors between these studies and our blended/mini-monovision study,10 we performed a subgroup analysis in which the raw data from the earlier study was examined to determine overall satisfaction and overall spectacle independence (our primary and secondary endpoints) for the subset of 2.5 mini-monovision and 2.5/3.0 cohort patients meeting the stricter refractive criteria of the later studies (residual refractive error within 0.5 D sphere and 0.75 D cylinder).
Patients were asked to complete a validated questionnaire, assisted by a research staff member, that evaluated their satisfaction with the surgery and with their spectacle independence (See Supplemental Information). The PRO questionnaire (Research InSight, LLC, Laguna Beach, Ca, USA) was specifically developed and validated to evaluate the effect of unwanted visual phenomena on patients who have undergone cataract surgery with presbyopia-correcting lenses, as well as satisfaction and spectacle independence. The assessment of these subjective outcomes differentiates this questionnaire from the National Eye Institute Visual Function Questionnaire-14 (VF-14 QOL) and other general-use visual function questionnaires. This questionnaire has been available for use in U.S.-based cataract practices since 2014 and has been used in our prior studies, as well.11,14,15
To determine the sample size needed for this analysis, a calculation was performed based on a 10% margin of error, a 95% confidence interval, and a response distribution of 80%. This resulted in a sample size of 62 patients.
All aspects of this study were conducted under the surveillance of Aspire Institutional Review Board (Santee, CA, USA) following the principles of the Declaration of Helsinki, and patients completed an informed consent process to participate. Reasonable requests to the corresponding author for original data will be honored for a period of 2 years from the publication date of this study.
Results
Demographics
Sixty patients with a mean age of 69±9.9 years (range 41–99) were enrolled in the study. There were no statistically significant demographic differences between the Vivity cohort and the three comparator cohorts (p = 0.78, Table 1). A higher percentage of patients in the Vivity (n-52, 88%) and PanOptix cohorts (n=52, 88%) underwent femtosecond laser-assisted cataract surgery compared to the 2.5 mini-monovision cohort (n=57, 56%) or the 2.5/3.0 cohort (n=18, 22%).
 |
Table 1 Demographics |
In the subgroup analysis, 74 patients in the 2.5 mini-monovision cohort (73%) met the residual refractive error criteria, as did 33 patients (80%) in the 2.5/3.0 cohort.
Glare and Halos
Patients in the Vivity cohort reported significantly less glare and halos than did those in other cohorts. In response to the question, “How much do you notice glare or halos around lights in dim light situations?” 51 Vivity patients (85%) responded “none” or “just a little,” compared to 69%, 75%, and 71% for Panoptix, 2.5 mini-monovision, and 2.5/3.0, respectively (p<0.03 vs Panoptix, p< 0.05 vs 2.5/3.0 and 2.5 mini-monovision, Chi-squared test). Among Vivity patients, 28 (47%) responded “none,” compared to 37%, 42%, and 33% for Panoptix, 2.5 mini-monovision, and 2.5/3.0, respectively (p<0.02 vs Panoptix, p< 0.03 vs 2.5/3.0 and 2.5 mini-monovision, Chi-squared test). Vivity patients were significantly less likely to notice glare and halos “a fair amount” or worse compared to all other IOL cohorts. (p<0.02 vs Panoptix, p<0.03 vs 2.5/3.0 and 2.5 mini-mono, Chi squared test). The distribution of responses to this question is shown in Figure 1.
 |
Figure 1 Responses to the question, “How much do you notice glare or halos around lights in dim light situation?” suggest that patients implanted with Vivity IOLs were significantly less likely to notice glare and halos more than “just a little” and significantly more likely not to notice these symptoms at all compared to all other IOL cohorts. (p<0.02 vs Panoptix, p<0.03 vs 2.5/3.0 and 2.5 mini-mono, Chi squared test). |
Spectacle Independence
Overall spectacle independence (Figure 2) for all visual activities combined was comparable for Vivity, mini-monovision, and 2.5/3.0 and significantly higher in the PanOptix cohort. In the Vivity cohort, 33% of patients said they “never” needed glasses for any activity versus 83% of patients in the Panoptix cohort, 36% in the 2.5 mini-monovision cohort, and 31% in the 2.5/3.0 cohort (p < 0.0001, Chi-squared test). Use of glasses “frequently or always” was reported by 27% of patients with Vivity, 3% with PanOptix, 11% with 2.5 mini-monovision, and 34% with 2.5/3.0 (p < 0.0001 for PanOptix vs all other cohorts, Chi-squared test).
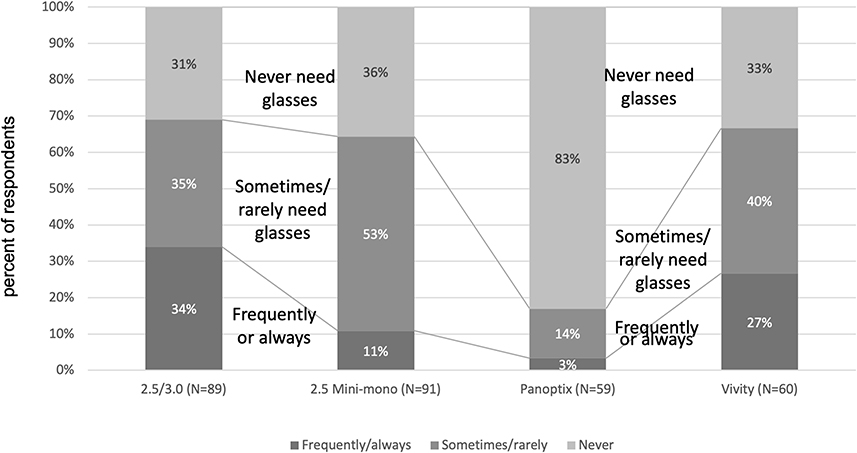 |
Figure 2 Frequency of spectacle use. |
No Vivity patients required spectacles for driving or sports/hobbies; one (2%) Vivity patient required glasses for television (Table 2). For computer use, a low rate of ≤20% reported needing spectacles across all lens cohorts (Table 2). For reading, glasses were needed “some of the time” for 65% of Vivity cohort patients, 17% of PanOptix patients, 64% with 2.5 mini-monovision, and 60% with 2.5/3.0 (p < 0.0001 for PanOptix vs all three other cohorts, Chi-squared test).
 |
Table 2 Patient-Reported Spectacle Dependence (Response to the Question, “Do You Ever Need to Use Spectacles for the Following Activities?”) |
There were no statistically significant differences in outcomes between patients who underwent femtosecond laser-assisted cataract surgery and those who underwent manual phacoemulsification.
In the subgroup analysis (those with <0.5 D of residual sphere and <0.75D of residual cylinder), complete spectacle independence was reported by 33% of patients with Vivity, 83% with PanOptix, 35% with 2.5 mini-monovision, and 33% with 2.5/3.0 (p < 0.0001 for PanOptix vs all three other groups, Chi-squared test).
Patient Satisfaction
No statistically significant differences were noted in overall satisfaction among the cohorts, with “very satisfied” or “somewhat satisfied” being reported by 95% of the Vivity cohort, 97% of the PanOptix cohort, 93% of the 2.5 mini-monovision cohort, 92% of the 2.5/3.0 cohort (Figure 3). “Very satisfied” was reported by significantly more Panoptix than Vivity patients (p < 0.05, Chi squared test). Patients were “very likely” or “somewhat likely” to refer friends and family for the same procedure in 98% of the Vivity cohort, 99% of the PanOptix cohort, 96% of the 2.5 mini-monovision cohort, and 88% of the 2.5/3.0 cohort. The difference between the Vivity and the 2.5/3.0 cohorts was statistically significant (p < 0.01, Chi squared test). Conversely, one patient (2%) in the Vivity cohort, one patient (2%) in the PanOptix cohort, four patients (4%) in the 2.5 mini-monovision cohort, and four patients (4%) in the 2.5/3.0 cohort reported they were either “very” or “somewhat” dissatisfied with their vision. Qualitative analysis of free-text responses from patients who reported dissatisfaction showed that dissatisfaction was generally related to unwanted visual phenomena (glare/halos) in the PanOptix cohort and the need for reading glasses in the Vivity and other multifocal cohorts. Some patients in all cohorts described ocular surface discomfort or other complaints (ie implant cost) that were not related to the quality of the implants themselves or to the patients’ vision.
 |
Figure 3 Satisfaction ratings of the Vivity lens were similar to other lenses among patients responding “very satisfied” or “satisfied”. Significantly more patients responded “very satisfied” to the Panoptix lens compared to all others. |
In the subgroup analysis (<0.5 D of residual sphere and <0.75D of residual cylinder) 95% of Vivity patients reported being “very satisfied” or “somewhat satisfied” overall, compared to 97% of PanOptix patients, 96% of patients with 2.5 mini-monovision, 94% with 2.5/3.0. None of the differences in satisfaction was statistically significant.
Refractive Accuracy
Among patients in the Vivity cohort, 100% had an absolute manifest refraction spherical equivalent (MRSE) within 0.75 D of emmetropia, 93% within 0.5 D, 42% within 0.25 D, and 10% exactly at emmetropia, compared to 100% within 0.75 D, 100% within 0.5 D, 90% within 0.25 D, and 36% at emmetropia in the PanOptix cohort. Values for other lens cohorts are shown in Figure 4.
 |
Figure 4 All four groups had very good refractive accuracy. Compared to the Vivity, 2.5/3.0, and 2.5 mini-monovision cohorts, the PanOptix cohort had significantly higher refractive accuracy among patients within 0.25 and 0 diopters of emmetropia (P< 0.0001, chi-squared test for both groups). |
BCVA
BCVA of 20/20 or better in both eyes was achieved by 41 Vivity patients (68%), 45 PanOptix patients (76%), 61 of the 2.5 mini-monovision patients (65%), and 46 of the 2.5/3.0 patients (64%). BCVA of 20/25 was achieved by 93%, 93%, 90%, and 90%, respectively. All patients had BCVA of 20/40 or better. These differences were not statistically significant. PCO (trace and grade 1+) occurred at a similar rate in all cohorts.
Femtosecond Laser Use
Femtosecond lasers were available to surgeons for all patient cohorts and were used for surgery in 32 of 60 Vivity patients (53%), 52 of 59 PanOptix patients (88%), 28 of 102 2.5 mini-monovision patients (27%), and 18 of 83 2.5/3.0 patients (22%), where these data were recorded (p < 0.002 for PanOptix vs each other group, Chi-squared test).
Discussion
This study examined real-world outcomes achieved with a new, nondiffractive EDOF lens intended to mitigate the effects of presbyopia. We found a significantly lower rate of glare and halo in patients implanted with the AcrySof IQ Vivity IOL compared to our prior studies with other multifocal IOLs.10,11
We have previously reported a very high rate of complete spectacle independence (83% of patients reporting that they never need glasses) with the PanOptix lens.11 Complete spectacle independence in the Vivity group was substantially lower than in the PanOptix cohort, but comparable to that of the 2.5/3.0 multifocal group and the 2.5 mini-monovision group. While the PanOptix and Vivity cohorts had similarly high rates of spectacle independence for intermediate to distance activities, there was a significant difference for near activities (reading), with PanOptix performing much better, as one might expect given the differences in IOL design. Some authors have suggested that binocular near vision with the Vivity lens may be improved with a mini-monovision target in the nondominant eye.16
Residual refractive error is a common source of postoperative dissatisfaction following implantation of advanced technology IOLs.17–19 In this study, refractive accuracy was high across all cohorts and particularly in the PanOptix (100% ± 0.5 D) and Vivity (93% ± 0.5 D) cohorts. Overall patient satisfaction was high for all the IOLs studied, with “very satisfied” or “somewhat satisfied” being reported by >90% across all lens groups, and ≥95% of those in the PanOptix and Vivity cohorts. This rate of satisfaction with the Vivity IOL is comparable to that achieved in the more tightly-controlled FDA studies of this lens.12 Satisfaction may be positively influenced by patients not paying for the procedure in FDA clinical trials or, conversely, negatively influenced by out-of-pocket costs in post-market studies. The high level of satisfaction in this study, therefore, is an important validation of the findings in the Phase 3 study for the Vivity lens.12
As surgeons’ armamentarium of advanced technology IOLs expands, it is worth considering which patients are the best candidates for each IOL type. Glare and halo have been commonly reported side effects of diffractive multifocal IOLs.17,20,21 Although night vision symptoms rarely lead to IOL exchange, they do contribute to dissatisfaction.22,23 Additionally, patients who are very risk-averse or those who frequently engage in night driving may be counseled against choosing a presbyopia-correcting IOL despite a desire for spectacle independence. Based on the findings of this real-world study, the ideal candidates for the Vivity extended depth of focus IOL may be those who want a greater range of vision but who are also very averse to unwanted visual phenomena or nighttime dysphotopsia. The nondiffractive Vivity IOL may also be a reasonable choice for patients with comorbid ocular disease or aberrated corneas who would not be good candidates for the PanOptix trifocal IOL or other diffractive presbyopia-correcting IOLs. Although data on such patients is limited, there is at least one report of a successful outcome with the Vivity lens in a patient with myotonic dystrophy and the potential for anterior capsular contraction.24 Patients who are willing to tolerate some unwanted visual phenomena in exchange for maximal spectacle independence may be best served by a diffractive trifocal or multifocal IOL with the potential to provide stronger reading vision.
There are several weaknesses in the current study. The IOL cohorts represent temporally different patient populations, rather than truly randomized, contemporaneous comparative sample. Every effort has been made, however, to conduct the studies in the same fashion to allow for the closest possible comparison among the cohorts.
Comparisons were made to cohorts from a previous study that did not exclude refractive outliers, which could have introduced unintended biases in favor of the 2.5 mini-monovision and 2.5/3.0 cohorts. To compensate for this potential bias, we performed a subgroup analysis of patients meeting the same refractive criteria, and found no change in the primary or secondary outcomes in this study (satisfaction and spectacle independence) with the more restricted refractive population.
More of the patients in the Vivity and PanOptix cohorts underwent femtosecond laser-assisted cataract surgery (FLACS) than in the other cohorts. This was simply a result of the investigators’ practices trending toward greater adoption of FLACS in the time frame of approval of Panoptix and Vivity. However, manifest refraction and BCVA, a proxy for refractive precision, was similar across all cohorts. The differences in spectacle independence, therefore, are likely related to IOL design rather than the use (or not) of the femtosecond laser.
Patients with significant pathology that would be expected to affect their refractive outcome or satisfaction were excluded from all cohorts, including the Vivity group. Nevertheless, because the Vivity lens can be implanted in less-than-perfect eyes, it is possible that differences in the candidate pools may have affected the satisfaction, spectacle independence, refractive accuracy, and/or glare and halo results. Because this study was intended to be a real-world comparison we believe that comparing this new implant to its predecessors in subtly, yet meaningfully different patient populations is reasonable, much as when researchers compare morbidity of a new heart valve to its precursors when the new valve is implanted in less healthy subjects. Surgeons who consider adopting a new lens are likely to value real-world evidence examining the parameters that matter most to their own patients.
The limitations of the study are offset by its strengths, including the fact that it was a prospective, multicenter study. Future, real-world studies examining the outcomes of Vivity non-diffractive EDOF lenses in compromised eyes would be valuable, as would larger, randomized studies that compare Vivity to other presbyopia-mitigating lens options in normal eyes. As IOL options expand, these results may help guide surgeons in customizing IOL choice to each patient’s expectations and visual demands.
Conclusion
The AcrySof IQ Vivity extended depth of focus IOL offers a similar range of uncorrected vision to previous multifocal implants. While the Panoptix trifocal lens showed the highest spectacle independence, the Vivity lens provided a significantly better dysphotopsia profile than any of the lenses in the comparison groups.
Acknowledgments
A portion of this study was presented as a poster at the 2021 American Society of Cataract and Refractive Surgery annual meeting in August, 2021 (Las Vegas, NV). Research InSight Inc. funded this study through an independent investigator-initiated research study grant by Alcon.
Disclosure
Dr John A Hovanesian reports grants from Alcon, during the conduct of the study. Drs Michael Jones and Quentin Allen are consultants for Alcon. The authors report no other conflicts of interest in this work.
References
1. Kieval JZ, Al-Hashimi S, Davidson RS, et al. ASCRS refractive cataract surgery subcommittee. Prevention and management of refractive prediction errors following cataract surgery. J Cataract Refract Surg. 2020;46(8):1189–1197. doi:10.1097/j.jcrs.0000000000000269
2. Pew Research Center. Internet use by age; 2017. Available from: https://www.pewresearch.org/internet/chart/internet-use-by-age/.
3. Statista. Share of adults in the United States who owned a smartphone from 2015 to 2021, by age group; 2021. Available from: https://www.statista.com/statistics/489255/percentage-of-us-smartphone-owners-by-age-group/.
4. Ni W, Li X, Hou Z, et al. Impact of cataract surgery on vision-related life performances: the usefulness of Real-Life Vision Test for cataract surgery outcomes evaluation. Eye. 2015;29(12):1545–1554. doi:10.1038/eye.2015.147
5. Greenstein S, Pineda R
6. Sachdev GS, Sachdev M. Optimizing outcomes with multifocal intraocular lenses. Indian J Ophthalmol. 2017;65(12):1294–1300. doi:10.4103/ijo.IJO_1072_17
7. Shah S, Peris-Martinez C, Reinhard T, Vinciguerra P. Visual outcomes after cataract surgery: multifocal versus monofocal intraocular lenses. J Refract Surg. 2015;31(10):658–666. doi:10.3928/1081597X-20150611-01
8. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and meta-analysis based on randomized controlled trials. Surv Ophthalmol. 2019;64(5):647–658. doi:10.1016/j.survophthal.2019.02.012
9. Wang SY, Stem MS, Oren G, Shtein R, Lichter PR. Patient-centered and visual quality outcomes of premium cataract surgery: a systematic review. Eur J Ophthalmol. 2017;27(4):387–401. doi:10.5301/ejo.5000978
10. Hovanesian JA, Lane SS, Allen QB, Jones M. Patient-reported outcomes/satisfaction and spectacle Independence with blended or bilateral multifocal intraocular lenses in cataract surgery. Clin Ophth. 2019;13:2591–2598. doi:10.2147/OPTH.S227629
11. Hovanesian JA, Jones M, Allen QB. The PanOptix trifocal IOL vs the ReStor 2.5 active focus and ReStor 3.0-add multifocal lenses: a study of patient satisfaction, visual disturbances, and uncorrected visual performance. Clin Ophthalmol. 2021;15:983–990. doi:10.2147/OPTH.S285628
12. AcrySof® IQ vivity™ extended vision IOL DFU. Alcon Laboratories, Inc.; 2020.
13. Arrigo A, Gambaro G, Fasce F, Aragona E, Figini I, Bandello F. Extended depth-of-focus (EDOF) AcrySof® IQ vivity® intraocular lens implant: a real-life experience. Graefe’s Arch Clin Exp Ophthalmol. 2021;259:2717–2722. doi:10.1007/s00417-021-05245-6
14. Hovanesian JA. Patient-reported outcomes of multifocal and accommodating intraocular lenses: analysis of 117 patients 2–10 years after surgery. Clin Ophthalmol. 2018;12:2297–2304. doi:10.2147/OPTH.S182943
15. Hovanesian JA. What factors drive the highest patient-reported satisfaction with multifocal IOLs?
16. Gunderson KJ, Potvin R. The effect of spectacle-induced low myopia in the non-dominant eye on the binocular defocus curve with a non-diffractive extended vision intraocular lens. Clin Ophthalmol. 2021;15:3541–3547. doi:10.2147/OPTH.S329922
17. de Vries NE, Webers CAB, Touwslager WRH, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
18. Seiler TG, Wegner A, Senfft T, Seiler T. Dissatisfaction after trifocal IOL implantation and its improvement by selective wavefront-guided LASIK. J Refract Surg. 2019;35(6):346–352. doi:10.3928/1081597X-20190510-02
19. Gibbons A, Ali TK, Waren DP, Donaldson KE. Causes and correction of dissatisfaction after implantation of presbyopia-correcting intraocular lenses. Clin Ophthalmol. 2016;10:1965–1970. doi:10.2147/OPTH.S114890
20. Sheppard AL, Shah S, Bhatt U, Bhogal G, Wolffsohn JS. Visual outcomes and subjective experience after bilateral implantation of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2013;39(3):343–349. doi:10.1016/j.jcrs.2012.09.017
21. Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110(9):1789–1798. doi:10.1016/S0161-6420(03)00722-X
22. Oltulu R, Erşan İ, Şatırtav G, et al. Intraocular lens explantation or exchange: indications, postoperative interventions, and outcomes. Arq Bras Oftalmol. 2015;78(3):154–157. doi:10.5935/0004-2749.20150040
23. Jones JJ, Jones YJ, Jin GJ. Indications and outcomes of intraocular lens exchange during a recent 5-year period. Am J Ophthalmol. 2014;157(1):154–162.e1. doi:10.1016/j.ajo.2013.08.019
24. Baur I, Auffarth GU, Labuz G, Khoramnia R. Unilateral implantation of a new non-diffractive extended range-of-vision IOL in a young patient with Curschmann-Steinert myotonic dystrophy. Am J Ophthalmol Case Rep. 2021;17(22):101109. doi:10.1016/j.ajoc.2021.101109
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.