Back to Journals » ImmunoTargets and Therapy » Volume 15
The Value of the Preoperative Hematological Inflammatory Markers for Predicting Lymphovascular Invasion in Gastric Cancer
Authors Li C, Wang Y, Liang S, Shi H, Mao X, Wang X, Mo D ![]()
Received 30 August 2025
Accepted for publication 31 December 2025
Published 9 January 2026 Volume 2026:15 564201
DOI https://doi.org/10.2147/ITT.S564201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah Wheeler
Cong Li,1,* Yanyan Wang,1,* Shumei Liang,2,* Huina Shi,1 Xuelian Mao,1 Xiao Wang,3 Dongping Mo1,4
1Department of Clinical Laboratory, Jiangsu Cancer Hospital & Nanjing Medical University Affiliated Cancer Hospital & Jiangsu Institute of Cancer Research, Nanjing, People’s Republic of China; 2Department of Clinical Laboratory, the Third People’s Hospital of Chengdu, Chengdu, People’s Republic of China; 3Department of CT, Jiangsu Cancer Hospital & Nanjing Medical University Affiliated Cancer Hospital & Jiangsu Institute of Cancer Research, Nanjing, People’s Republic of China; 4Jiangsu Key Laboratory of Molecular and Translational Cancer Research, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongping Mo, Department of Clinical Laboratory, Jiangsu Cancer Hospital & Nanjing Medical University Affiliated Cancer Hospital & Jiangsu Institute of Cancer Research, Nanjing, People’s Republic of China, Email [email protected]
Background: Gastric cancer (GC) is a prevalent malignant tumor of the digestive system, with high morbidity and mortality. Lymphovascular invasion (LVI) is a risk factor for recurrence and metastasis of GC and an independent predictor of poor postoperative prognosis in GC patients. Accumulating evidence suggests that blood-based inflammatory indicators are linked with the pathogenesis of GC. The study delves into hematological inflammatory markers to explore their potential applications in preoperative LVI in GC.
Methods: We retrospectively collected and analyzed data from inpatients diagnosed GC at our hospital from December 2020 to October 2024, with LVI confirmed by pathological examination after surgery. Preoperative hematological inflammatory indicators were calculated from peripheral blood samples. Lasso logistic regression and multivariate logistic regression analyses were utilized to verify independent risk factors for LVI-positive GC patients and constructed the nomogram model. The correlation between hematological inflammatory indicators and clinical TNM staging was assessed through Spearman’s analysis.
Results: In the study, 624 patients were pathological diagnosed with LVI-positive. The variables screened by Lasso logistic regression including CA199, PLR, SII, PNI, cT staging, and cN staging. Multivariate logistic regression analysis confirmed that CA199 (OR = 1.349, 95% CI: 1.016– 1.790), PLR (OR = 1.396, 95% CI: 1.005– 1.939), PNI (OR = 0.706, 95% CI: 0.515– 0.968), cT staging (OR = 1.737, 95% CI: 1.511– 1.996) and cN staging (OR = 2.272, 95% CI: 1.975– 2.613) were independent risk factors of LVI-positive. PLR was positively correlated with cT and cN staging, while PNI was negatively correlated with both. The C-statistic of the nomogram model was 0.845, with a sensitivity of 86.86% and a specificity of 69.90%.
Conclusion: We provided a new perspective on the clinical application of preoperative hematological inflammatory markers in the auxiliary diagnosis of LVI-positive in GC patients.
Keywords: gastric cancer, lymphovascular invasion, inflammatory marker, nomogram model
Introduction
According to recent statistics, gastric cancer has become the fifth most frequently diagnosed cancer and the third-leading cause of cancer deaths worldwide, with high morbidity and mortality.1,2 Owing to the deficiency of representative symptoms and effective markers, gastic cancer is typically diagnosed at an advanced stage, which results in a poor prognosis.3 Postoperative distant metastasis, along with the drug resistance to chemotherapy and resistance to immunotherapy, contribute to a 5-year survival rate of under 30% among advanced gastric cancer patients.4,5 Lymphovascular invasion (LVI) is defined as the invasion of vessel walls by tumor cells and/or the presence of tumor emboli within an endothelial-lined space, which leads to vascular function and blood circulation disorders, and often indicated poor prognosis for various tumors.6–8 In gastric cancer, regional LVI is closely related to patient recurrence and prognosis, with LVI-positive patients having a higher recurrence rate and a lower 5-year survival rate.9,10 At present, gastric cancer patients are mainly stratified based on TNM staging. Due to the crucial role of LVI in determining treatment regimen and its impact on the prognosis of gastric cancer, studies suggested that incorporating LVI into the TNM staging system might have a better efficiency for predicting the overall survival rate of gastric cancer patients.11,12 Currently, the status of LVI can only be obtained from histopathologic examination after surgery, which is invasive, time-consuming, and unsuitable for preoperative decision-making.13 Therefore, in the clinical treatment of gastric cancer, it is necessary to find a reliable preoperative predictive method to guide surgery or adjuvant therapy.
An increasing number of studies have indicated that the malignant progression of gastric cancer is closely associated with the tumor inflammatory microenvironment.14,15 There are various inflammatory cells such as neutrophils, lymphocytes, macrophages, and monocytes in tumor inflammatory microenvironment.16 During inflammation, these cells are often abnormally expressed, manifested in abnormal peripheral blood routine.17,18 It is believed that neutrophils infiltrating within the tumor tissue can produce various inflammatory mediators and inflammatory factors to promote the formation of the tumor microenvironment, facilitating tumor growth, invasion, angiogenesis, and metastasis.19–21 During the invasion and metastasis of tumor cells, platelets and macrophages facilitate angiogenesis, basement membrane rupture, and extracellular matrix remodeling, enabling tumor cells to invade and infiltrate blood vessels and lymphatic vessels for distant metastasis.22 Lymphocytes can not only activate other immune cells such as macrophages to assist in killing tumor cells, but also play a role in tumor immune evasion, promoting vascular growth and proliferation, increasing tumor growth and metastasis,23 and providing favorable conditions for the formation of LVI. Growing evidence suggested that the complete blood count-derived inflammatory markers, such as platelet to lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), and systemic immune inflammation index (SII), have been proved to be related to the prognosis and progression of a variety of tumors.24–26 Importantly, all of the above indicators can be easily measured through routine blood tests for cancer patients. In our previous research, we confirmed that CEA, FLR, D-dimer, PLR, CA199, and CA724 as independent risk factors for gastric cancer patients with perineural invasion. Meanwhile, a prediction model with good discrimination and accuracy has been successfully established and validated.27 Currently, imaging techniques are commonly employed for preoperative prediction of LVI in gastric cancer patients.28,29 However, imaging methods struggle to accurately identify subclinical lymph node micrometastasis and hematogenous micrometastasis. Therefore, this raises the question of whether inflammatory markers derived from peripheral blood can also offer clinical application for LVI assessment in gastric cancer. To our knowledge, there are few studies on LVI and hematological indicators in gastric cancer.
In this study, we performed a retrospective analysis to evaluate the clinical significance of inflammatory markers derived from peripheral blood test results in gastric cancer patients with LVI. Additionally, we employed the Lasso regression to screen parameters and calculated the optimal cut-off value for LVI and established a nomogram based on multivariate logistic regression results. Our present study may provide a new non-invasive auxiliary method for preoperative diagnosis of gastric cancer patients with LVI. The prediction of LVI in preoperative assessment of whether the tumor has reached a locally advanced stage, offering supportive evidence for the administration of neoadjuvant therapy and holding significant potential for improving the prognosis of gastric cancer patients.30,31
Materials and Method
Study Patients and Processing
We retrospectively collected and analyzed data from inpatients diagnosed gastric cancer at the Jiangsu cancer hospital from December 2020 to October 2024. The present study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and approved by the Ethical Committee of Jiangsu cancer hospital (No. KY-2024-012-GZ-01 and No. KY-2024-119). Patients were included if they met the following criteria: (1) Age over 20 years old; (2) Primary gastric cancer; (3) Not receiving any anti-tumor therapeutic before admission; (4) Complete clinical and laboratory data; (5) Received upper endoscopy, barium meal examination, computed tomography or magnetic resonance imaging prior to therapeutic. Patients were excluded if they presented with the following: (1) History of other malignant tumors; (2) Distant metastasis; (3) Recurrent tumors or residual gastric cancer; (4) Gastrointestinal stromal tumor; (5) History of serious immune disorders, malignant hematologic disease; (6) History of severe hepatic or renal disease. After applying these criteria, 1232 gastric cancer patients were included in the present study. The clinical stage of all patients was determined by clinical examination and the imaging examinations.32 All patients were staged according to the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) 8th edition staging system. The clinicopathological characteristics of these cases were shown in Table S1.
The research procedures of this study were as follows: Firstly, we obtained laboratory data, clinical data and pathological characteristics in gastric cancer patients treated with curative gastrectomy. Then, we calculated inflammation markers based on laboratory data, and analyzed laboratory indicators that showed differences between LVI-negative and LVI-positive groups. Thirdly, lasso logistic regression was used to screen variables, and receiver operating characteristic (ROC)–area under curve (AUC) analysis was employed to calculate the optimal cut-off value for LVI. Finally, we formulated the nomogram based on multivariate logistic regression results. A flow diagram of subjects enrolled in this study is provided in Figure 1.
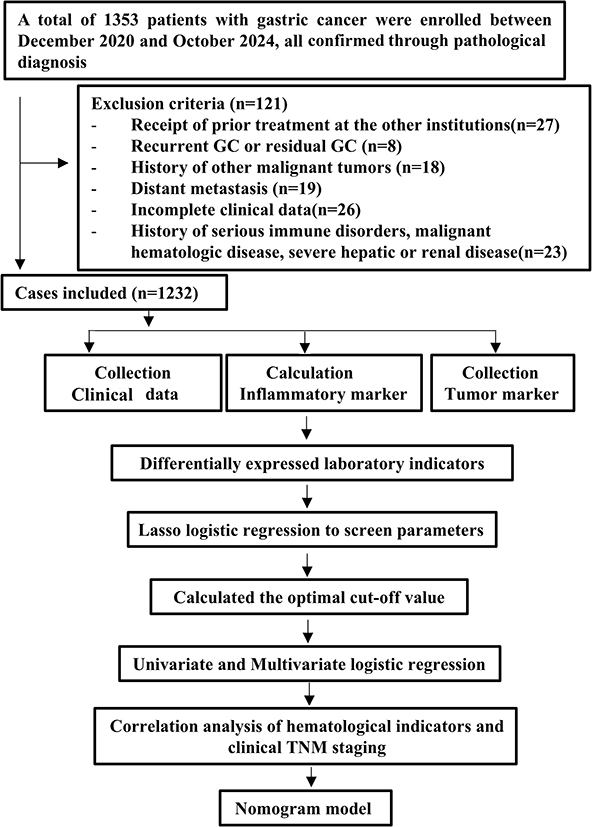 |
Figure 1 The flowchart of the study design and analysis. Abbreviations: GC, gastric cancer; TNM, tumor-node-metastasis. |
Laboratory Data Collection and Calculation
Blood samples were collected from all patients in the morning. All laboratory indicators were checked before the cases received clinical treatment. The laboratory indicators included neutrophils count (NE), lymphocytes count (LY), monocytes count (MO), platelets count (Plt), albumin (Alb), carcinoembryonic antigen (CEA) and carbohydrate antigen 199 (CA199). The calculation formula of peripheral blood derived inflammatory markers according to the following equations: neutrophil to lymphocyte ratio (NLR) = NE/LY, PLR = Plt/LY, LMR = LY/MO, albumin-to-lymphocyte ratio (ALR) = Alb/LY, SII = (NE×Plt)/LY, prognostic nutritional index (PNI) = Alb(g/L)+5×LY, systemic inflammation response index (SIRI) = (NE×MO)/LY, aggregate index of systemic inflammation (AISI) = (NE×Plt×MO)/LY, (neutrophil + monocyte)-to-lymphocyte ratio (NMLR) = (NE+MO)/LY.
Histopathological Evaluations of LVI
All surgical specimen were processed according to standard pathological procedures and stained with hematoxylin-eosin (HE). For each specimen, three independent representative tissue sections were prepared. The pathological diagnosis was determined after a discussion between two experienced pathologists. LVI was defined as the invasion, destruction, or intraluminal thrombosis of small veins, arteriole, or lymphatic vessels of the tumor.33 All patients were divided into an LVI-positive group (624 cases, 50.65%) and an LVI-negative group (608 cases, 49.35%) in the present study.
Statistical Analysis
All data in the present study were tested for a normal distribution using the Kolmogorov–Smirnov test. Continuous variables were presented as means ± standard deviations or medians (interquartile range [IQR]), and the results were compared using Student’s t-test or Mann–Whitney U-test, when appropriate. Categorical variables were presented as count (%) and compared with Chi-square tests or Fisher’s exact test. Lasso logistic regression was employed for variable selection. The ROC-AUC was employed to evaluated the diagnostic accuracy of all variables for patients with LVI. Univariate and multivariate logistic regression analyses of relative risks for patients with LVI, and OR and 95% CI were calculated. Spearman’s analysis was used to assess the correlations between variables and cTNM stage. Finally, Nomogram model was developed to evaluate LVI-positive gastric cancer based on multivariate logistic regression results. A P-value less than 0.05 was considered statistically significant, and all statistical test were two-sided. All statistical analysis was performed using IBM SPSS Statistics Version 20.0, GraphPad Prism v9.4.1 and R version 4.2.1.
Results
Analysis of Patient Clinical Characteristics According to Status of LVI
Based on the status of LVI, the 1232 patients were categorized into two groups. Compared with the LVI-negative groups, the medians of age and preoperative CEA, CA199, NLR, PLR, ALR, SII, SIRI, NMIR and SIRI were significantly increased (P < 0.05), and the medians of LMR and PNI were markedly decreased (P < 0.01). What’s more, there were statistically significant difference in clinical T staging and N staging between patients with LVI-negative and those with LVI-positive (P < 0.001). All detailed data were shown in Table 1.
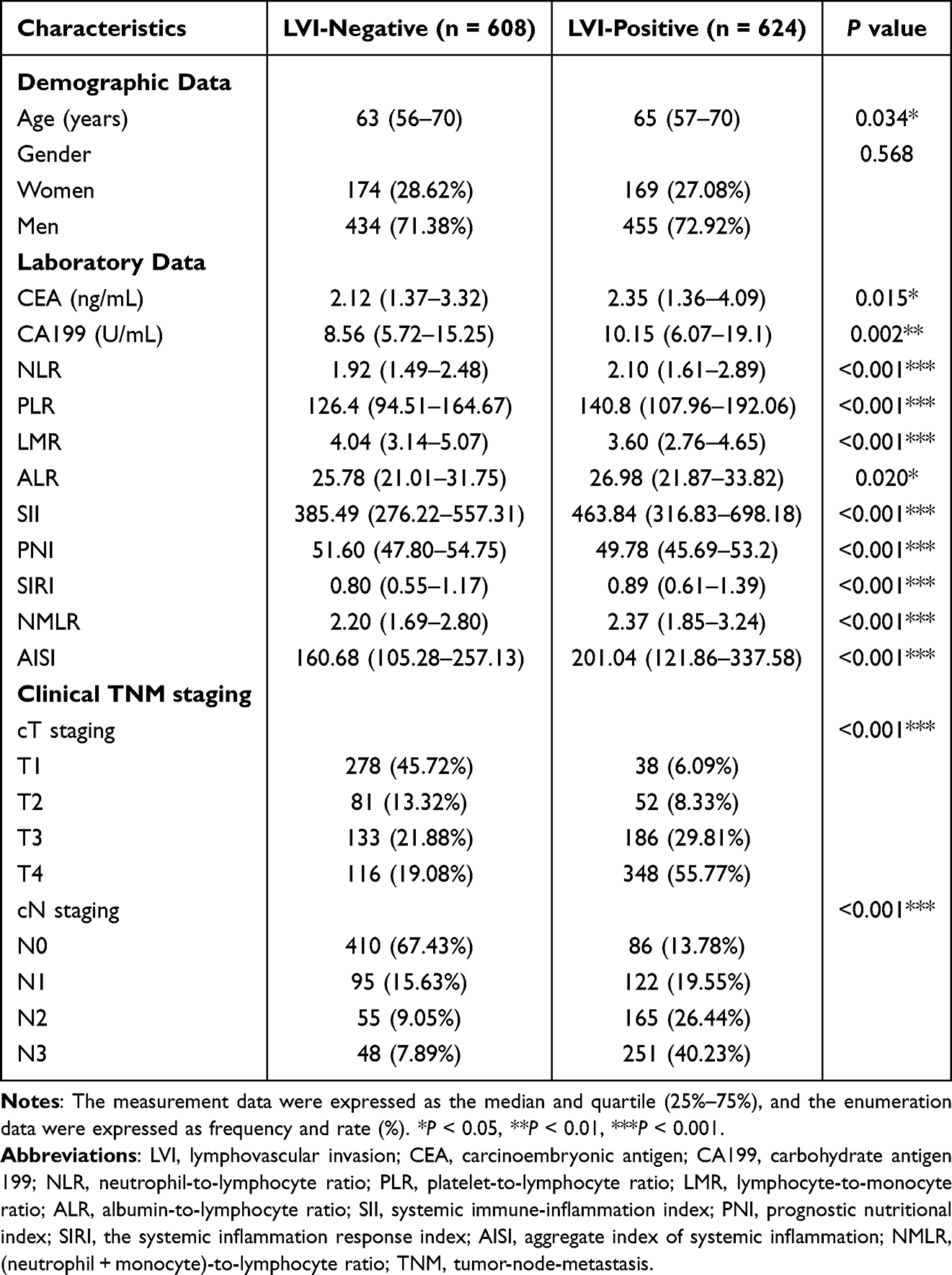 |
Table 1 Comparison of Characteristics According to Status of LVI in Gastric Patients |
Prediction Model Built Based on Lasso Logistic Regression
In order to prevent overfitting, we utilized Lasso logistic regression for parameter selection during model construction. There are 14 variables that differences between LVI-negative and LVI-positive groups, including age, CEA, CA199, NLR, PLR, ALR, SII, SIRI, NMIR, SIRI, cT staging and cN staging. Herein, a 10-fold cross-validation was implemented to determine to optimal penalty term lambda, with a more stringent selection to minimize the number of covariates. Figure 2A displays the coefficient distributions of predictors, and Figure 2B shows the cross-validation error plot of the Lasso model. Finally, six non-zero variables with optimal lambda (λ = 0.012) in the Lasso model were cT staging, cN staging, CA199, PLR, SII and PNI.
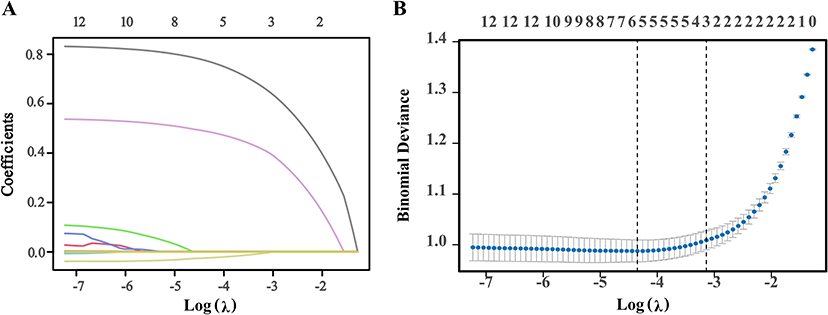 |
Figure 2 Screening of variables based on Lasso logistic regression. (A) Lasso regression coefficient path plot for 14 variables. X-axis is log (lambda) and Y-axis is partial regression coefficients. (B) Lasso regression cross-validation plot. The optimal parameter (lambda) in the Lasso model was selected using a 10-fold cross validation based on the minimum criterion. |
Diagnostic Efficiency of Hematological Indicators for Patients with LVI
ROC curve analysis was conducted to determine the ability of hematological indicators to distinguish LVI-positive patients. The cut-off value of the CA199 was 10.25 U/mL (AUC = 0.551, 95% CI: 0.519–0.583, sensitivity: 49.36%, specificality: 59.70%). The cut-off value of the PLR was 171.43 (AUC = 0.597, 95% CI: 0.565–0.628, sensitivity: 35.42%, specificality: 78.95%). And then, the cut-off value of SII and PNI were 387.77 and 47.78, respectively. The AUC of SII was 0.591, the 95% CI was 0.559–0.622, the sensitivity was 63.62%, and the specificity was 50.66%. The AUC of PNI was 0.593, the 95% CI was 0.562–0.596, the sensitivity was 38.46%, and the specificity was 75.66%. Details of the accuracy, positive predictive value, negative predictive value and Youden’s index are shown in Table 2.
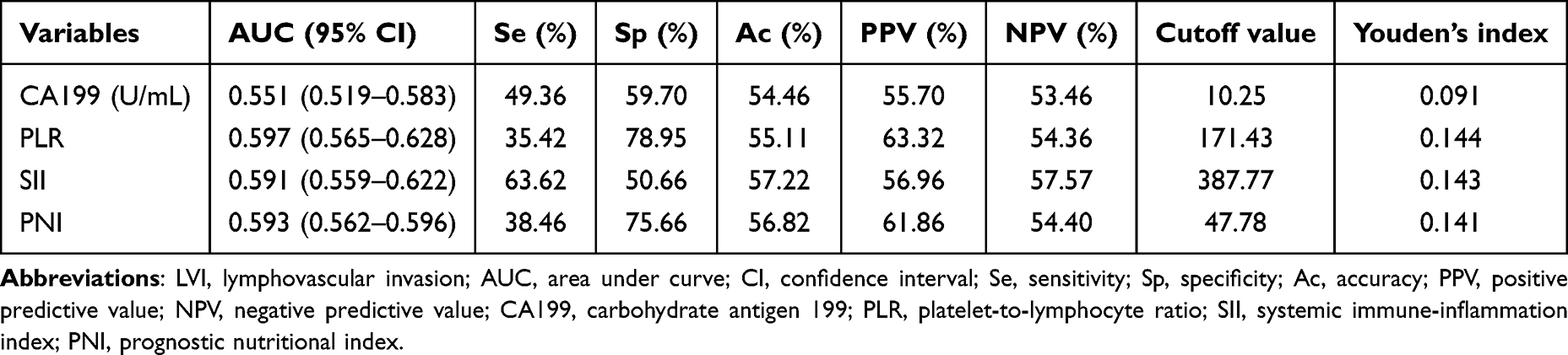 |
Table 2 Diagnostic Efficiency of Hematological Indicators for Patients with LVI |
Univariate Logistic Regression Analysis for LVI in GC Patients
Perform univariate logistic regression analysis with the occurrence of LVI as the dependent variable (negative = 0, positive = 1), CA199 (≤10.25U/mL = 0, >10.25U/mL = 1), PLR (≤171.43 = 0, >171.43 = 1), SII (≤387.77 = 0, >387.77 = 1), PNI (≤47.78 = 0, >47.78 = 1), cT staging (T1 = 0, T2 = 1, T3 = 2, T4 = 3), and cN staging (N0 = 0, N1 = 1, N2 = 2, N3 = 3) as independent variables. The results displayed that the above variables were significantly correlated with LVI-positive patients (Table 3).
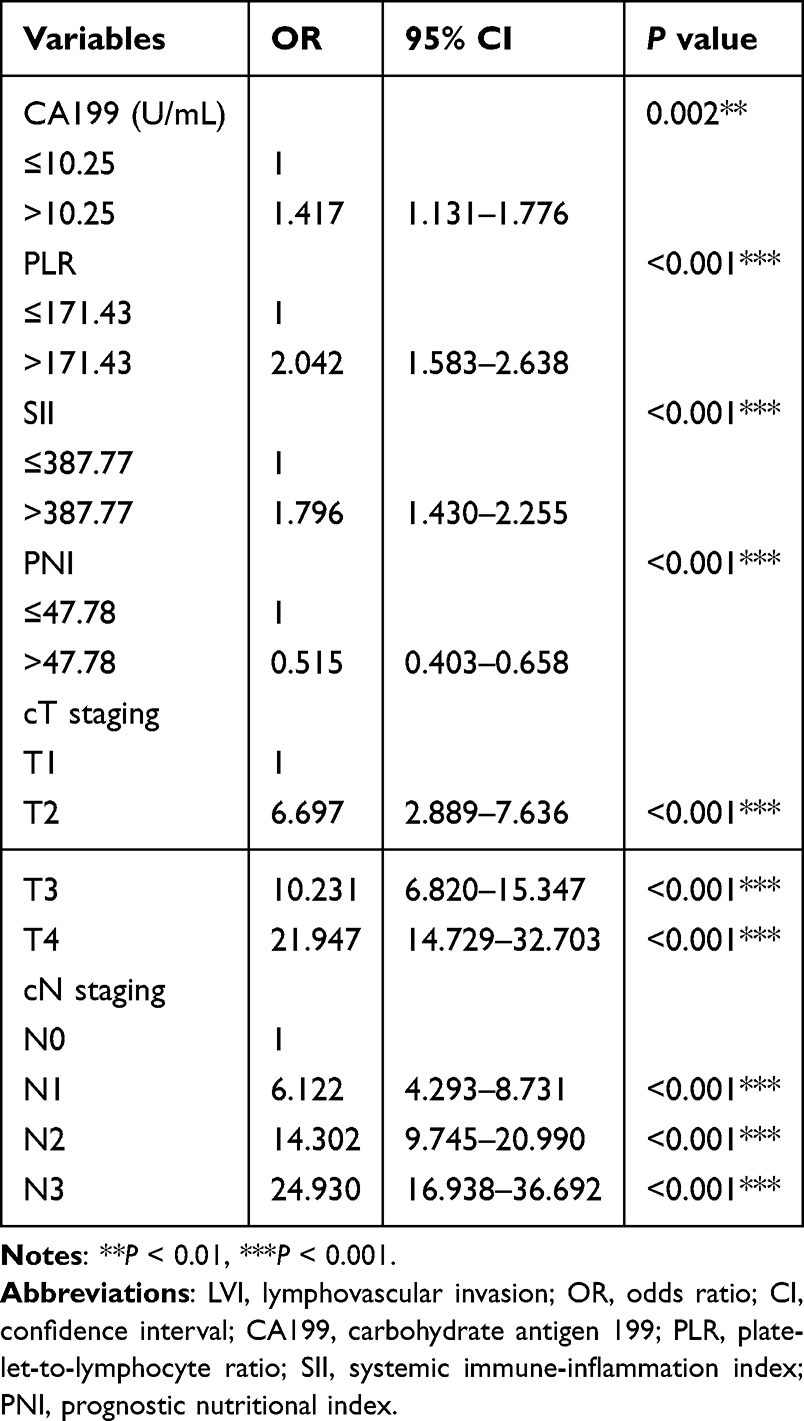 |
Table 3 Univariate Logistic Regression Analysis of LVI in Gastric Cancer Patients |
Multivariate Regression Analysis for LVI in GC Patients
Subsequently, we included variables with P < 0.05 in the univariate regression analysis into the multivariate regression analysis, employing a likelihood ratio test with maximum partial likelihood estimation (forward: LR). The results showed that CA199 (OR = 1.349, 95%: 1.016–1.790, P = 0.038), PLR (OR = 1.396, 95%: 1.005–1.939, P = 0.046), PNI (OR = 0.706, 95%: 0.515–0.968, P = 0.030), cT staging (OR = 1.737, 95%: 1.511–1.996, P < 0.001), and cN staging (OR = 2.272, 95%: 1.975–2.613, P < 0.001) were independent risk factors of LVI-positive patients (Table 4). Then, we obtained a classification discriminant equation using the above results to ascertain whether gastric cancer patients with LVI-positive, as follow: logit (P) = −2.504+0.299*CA199+0.334*PLR-0.348*PNI+0.552*cT+0.821*cN (χ2 = 506.73, P < 0.001), for which the critical value is 0.50, thus, if the logit (P) of a case is larger than 0.50, it belongs to LVI-positive patients. Otherwise, it belongs to the LVI-negative groups. And the model prediction accuracy is 77.10%.
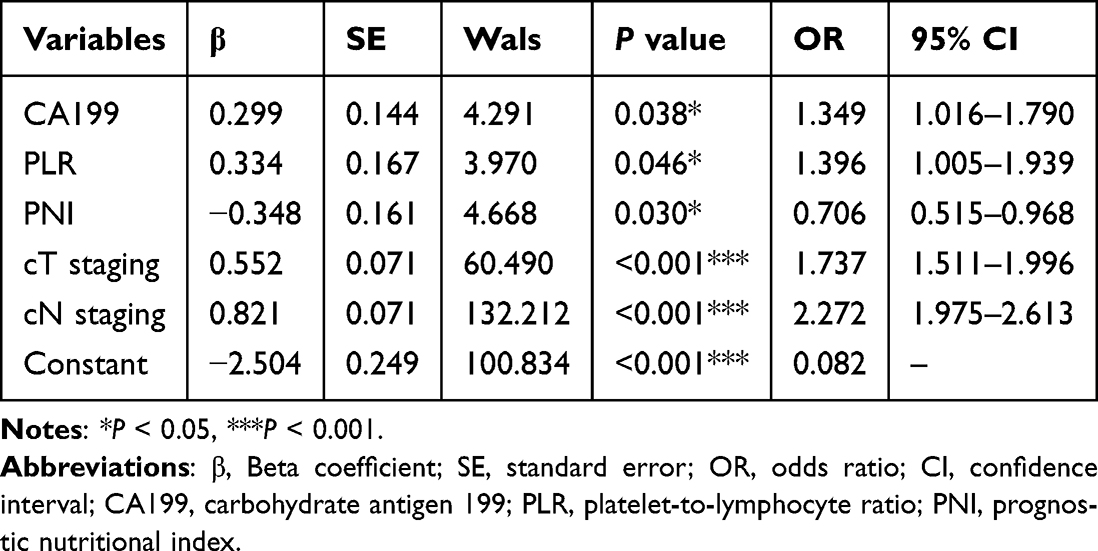 |
Table 4 Multivariate Analysis of Logistic Regression Model for Predicting LVI |
Correlation Analysis of Hematological Indicators and Clinical TNM Staging
The Spearman correlation test was used to examine the correlation between levels of CA199, PLR and PNI. There was a negative correlation between PLR and PNI (r = −0.450, P < 0.001; Figure 3A). However, there is no significant correlation between CA199 and PLR or PNI (P > 0.05). Immediately after, we divided all subjects into 4 group cohorts: cT1, cT2, cT3 and cT4 according to the cT staging. As shown in Figure 3B and C, PLR was positively correlated with cT staging (r = 0.180, P < 0.001), while PNI was negatively correlated with cT staging (r = −0.159, P < 0.001). When we grouped the all subjects based on cN staging (cN0, cN1, cN2 and cN3), the similar results were found (CA199: r = 0.065, P = 0.023; PLR: r = 0.139, P < 0.001; PNI: r = −0.127, P < 0.001; Figure 3D–F).
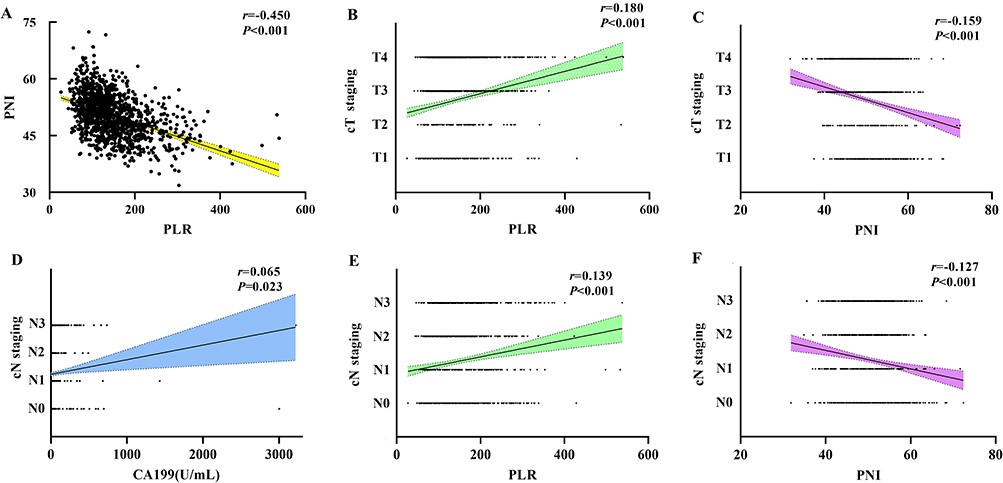 |
Figure 3 Correlation analysis of hematological indicators and clinical TNM staging. (A) Correlation analysis between PLR and PNI. (B and C) Association between the cT staging and PLR, PNI. (D–F) Association between the cN staging and CA199, PLR, PNI. Abbreviations: CA199, carbohydrate antigen 199; PLR, platelet-to-lymphocyte ratio; PNI, prognostic nutritional index. |
Nomogram Model for Risk Assessment of GC with LVI
Based on the results of multivariable logistic regression, we establish a nomogram model for LVI-positive patients using the R language rms package. The C statistic for the nomogram was 0.845, with a sensitivity of 86.86% and a specificity of 69.90%, indicating that the model had certain accuracy (Figure 4A). Hosmer-Lemeshow goodness of fit test was used to evaluated the calibration ability of the model, and the results indicated that there was no statistically significant difference between the predicted values of the model and the actual observed values (χ2= 13.80, P = 0.087, Figure 4B). Besides, the DCA suggested that the clinical net benefit of intervention based on the predicted probability of the model is highest when the threshold probability is between 0.12 and 0.83 (Figure 4C). And then, the plotting function was constructed, and the nomogram was plotted (Figure 4D). That is, a score of cT4 staging was 70 points, while a score of cT1 staging was 0 points; a score of cN3 staging was 100 points, while a score of cN0 staging was 0 points; a score of CA199 = 2000 U/mL was 47.5 points; a score of PLR = 450 was 50 points; a score of PNI = 30 was 57.5 points. The total score was 205 points, suggesting that the probability of LVI-positive in gastric cancer was greater than 80%. The risk of LVI-positive can be predicted based on the total points (Table 5).
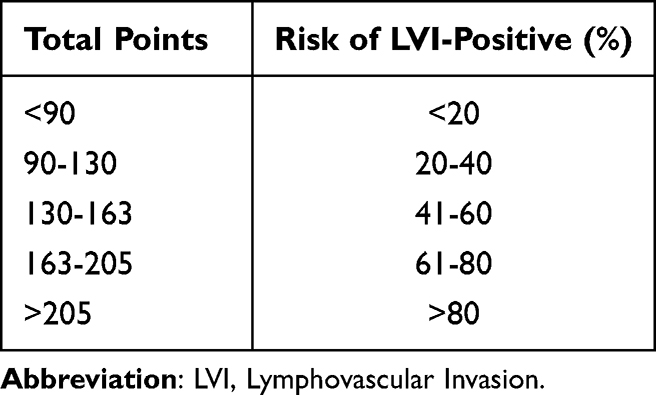 |
Table 5 Relationship Between Total Points and Risk of LVI for Gastric Cancer Patients |
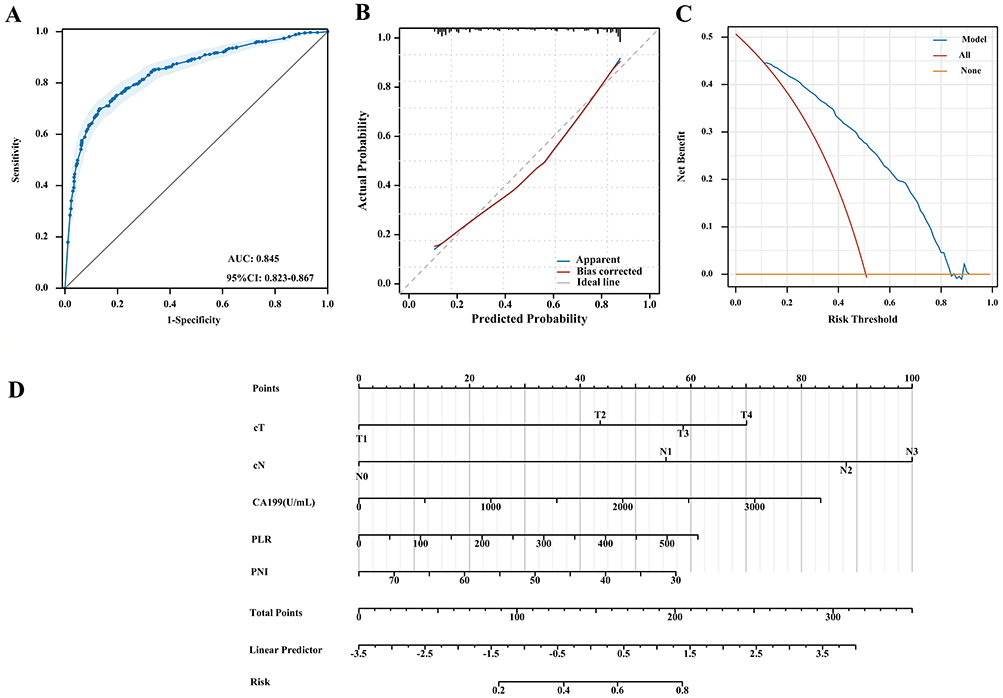 |
Figure 4 Prediction model for risk assessment of gastric cancer with LVI. (A) ROC curve of the combined factors; (B) Calibration curve of mo (C) DCA of mo (D) Nomogram of the logistic regression model. Abbreviations: LVI, Lymphovascular Invasion; AUC, area under the curve; CI, confidence interval; CA199, carbohydrate antigen 199; PLR, platelet-to-lymphocyte ratio; PNI, prognostic nutritional index; DCA, decision curve analysis. |
Discussion
Actually, we have displayed that PLR, cT staging and cN staging were independent risk factors for LVI in gastric cancer patients in our previous research, with a total of 341 cases at that time.34 The present study expanded the sample size on the basis of the original, established a nomogram model to obtain more reliable results. Similarly, apart from PLR, cT staging and cN staging, CA199 and PNI also serve as independent predictors for LVI in gastric cancer in this study. Some individual markers, such as CA199, PNI or PLR, have limited predictive power on their own, whereas combinations of markers demonstrated better predictive performance within the model. Compared to previous study, the present study has elevated the prediction accuracy from 67.26% to 77.10%, and the C-statistic from 0.733 to 0.845. In short, our study provided a simple and effective non-invasive auxiliary method for predicting preoperative LVI patients with gastric cancer.
LVI refers to the invasion of tumors into lymphatic vessels and/or blood vessels, which is an important pathway for local metastasis.35 It plays an important role in tumor recurrence and lymph node metastasis, and increases the risk of micrometastasis.36 In the present study, the rate of LVI positivity was 50.65%, which is consistent with LVI detection rate of 55.60% reported in previous study.37,38 Previous studies have shown that gastric cancer patients with LVI have a higher degree of malignancy and lower postoperative survival rate, and LVI is an independent risk factor affecting patient prognosis.9,39 Currently, preoperative LVI prediction remains challenging due to its histopathological nature, which is associated with biologically aggressive diseases and can only be confirmed through postoperative histopathological examination.40
Therefore, there is a need for a convenient and accurate tool to comprehensively predict LVI status in gastric cancer patients. Some studies revealed that radiomics features of positron emission tomography/computed tomography (PET/CT) and enhanced CT can evaluate the preoperative status of LVI in gastric cancer.41,42 Hematological indicators are renowned for their simplicity and clinical practicality in tumor screening and have become a common method for cancer evaluation. At present, the clinical potential significance of derived inflammatory markers of peripheral blood in gastric cancer patients with LVI is still limited. This study explores the correlation between derived inflammatory indicators and LVI, hoping that they could become an auxiliary diagnostic tool beyond imaging examinations.
Nowadays, with the deepening of research on the interaction between tumor microenvironment and immune response, the close relationship between inflammatory response and tumor occurrence and development has been gradually emerged. Inflammation alters the tumor microenvironment, creating a suitable environment for the proliferation of cancer cells.43 LVI means that the invasion and accumulation of cancer cells in the blood vessels and lymphatic system during growth, proliferation, and metastasis, leading to a series of pathological and physiological changes. When the body undergoes an inflammatory response, blood inflammatory indicators such as neutrophils, platelets, and lymphocytes often show abnormal expression. Tumor stroma can recruit various inflammatory cells through chemokines, forming an important component of the tumor microenvironment and promoting tumor cell proliferation and infiltration. Among them, platelets utilize the encapsulation function of blood clots to protect circulating tumor cells (CTCs) from immune system surveillance, avoiding antigen presentation by mononuclear macrophages and dissolution and elimination by natural killer cells.44 To enhance the adhesion and aggregation between tumor cells and platelets, tumor cells produce a series of special mechanisms to activate platelets. This is also the main reason why cancer patients have a high coagulation state and a high risk of thrombosis.45 Activated platelets release lysophosphatidic acid (LPA), which plays a significant role in enhancing the invasive ability of tumor cells, vascular permeability, and promoting transendothelial migration.46 Lower levels of lymphocytes indicate insufficient immune response to tumors and weakened ability to delay cancer cell infiltration.47 Besides, low levels of serum albumin are often associated with tumor related inflammatory reactions and affect the prognosis of malignant tumors.48 In our study, PLR and PNI were independent risk factors for LVI-positive patients, indicating an increase in platelets, a decrease in lymphocytes and albumin levels, and a corresponding increase in the risk of LVI in gastric cancer. Moreover, PLR was positively correlated with cT staging and cN staging, while the PNI was negatively correlated with both. The results suggested that LVI-positive patients with high infiltration and lymph node metastases have higher platelets, lower lymphocyte and worse nutritional status. Unfortunately, SII was not an independent risk factor for LVI-positive patients. SII is associated with peripheral blood neutrophils, but there was no significant difference in the median neutrophils between LVI-negative group and LVI-positive group in this study (3.18 vs 3.33, P > 0.05). The occurrence of such results may be attributed to the fact that multivariate analysis incorporates multiple variables into the model simultaneously. The statistical model automatically assigns the influence to stronger variables, such as PLR and PNI in this study, while excluding SII from the model. Given that this study is a single-center investigation, a multi-center analysis will be conducted in future studies to verify the impact of the aforementioned variables.
A previous study showed that PLR > 129 (OR: 1.64, 95% CI: 1.00–2.67) is associated with LVI in the univariate logistic analysis, but not an independent risk factor for LVI in gastric cancer patients. The analysis may be due to the small sample size (N = 262).49 The present study has over 1000 research subjects, and the results are more convincing. In our previous research, we displayed that PNI could be used as screening biomarker in diagnosing gastric cancer, especially in the early stage.50 Beyond that, higher PNI was markedly associated with better overall survival in gastric cancer, and higher PNI patients had a protective effect regarding postoperative morbidity and mortality.48 Because of this, lower PNI is more likely to present in LVI-positive gastric patients, indicating poor prognosis. The therapeutic strategy for gastric cancer, including the extent of gastric resection and lymphadenectomy, is determined based on cT (T1 or T2-T4) and cN (N0 or N+).51 Therefore, this study included clinical cTNM staging for model construction, and the results suggested that cT staging and cN staging were also independent risk factors for LVI-positive patients. The underlying reason could be that as the tumor progresses, tumor cells infiltrate and invade blood vessels, subsequently proliferating at the infiltrated vascular sites and continuously releasing tiny cancer emboli into the circulation. In addition, gastric cancer patients with LVI-positive exhibit elevated levels of vascular endothelial growth factor (VEGF) within their tumor tissues.52 The production of VEGF stimulates neovascularization, and the incomplete basement membrane of these newly formed vessels enhances the likelihood of cancer cell invasion into the vascular system, thereby increasing the counts of vascular cancer thrombus and lymph node metastasis also increases.53 This offers an explanation for the correlation between LVI and both tumor infiltration and lymph node metastasis.
Finally, we establish a nomogram model for gastric cancer with LVI-positive. The C-statistic of the nomograms model evaluation was 0.845, with a sensitivity of 86.86% and a specificity of 69.90%, indicating that the model had certain accuracy. The calibration curve also indicated that the predictive results were good in accordance with the actual results. What’s more, assign a score to each value level of each indicator based on their contribution to the outcome variable in the model. And then add up these scores to obtain the total score, which can be transformed into a function of the probability of clinical outcome events to ultimately calculate the predicted value of a specific event.54 Nomograms have significantly benefited in diagnosis of gastric cancer. For instance, Tong et al38 have established a nomogram based on Borrmann classification, CA724, tumor thickness, and iodine concentration in the venous phase, with an AUC of 0.864 for LVI patients with gastric cancer. But CA199 and PLR were not included in the model of this study, potentially due to factors such as inclusion criteria, sample size, and detection methods. Besides, Zhang et al28 have also reported a nomogram model for predicting LVI in gastric cancer patients, consisting of vascular entry sign, clinical T stage, and clinical N stage. The AUC of this model is 0.878, similar to the results obtained in this study, and both offer valuable tools for clinical decision-making and the formulation of personalized treatment approaches. Although the AUC of the prediction model in the present study is largely consistent with previous research findings, it can be further enhanced by integrating imaging and comprehensive clinical pathological data in subsequent stages to improve the diagnostic efficacy for LVI patients gastric with cancer.
The main limitation of this study was that data from a single center were retrospectively analyzed, although we have a relatively large sample size. There were biases in participant selection and clinical data extraction, thereby potentially impacting the study’s conclusions to some extent. Secondly, the cut-off value of laboratory data was only calculated only by mathematical methods, and their clinical potential should be further validated through multi-center studies with larger sample sizes. Moreover, the LVI group was not differentiated into lymphatic cancer emboli, vascular cancer emboli, and microvascular cancer emboli, which will be the focus of future research endeavors.
Conclusions
In summary, the predictive model for LVI-positive patients, established by combining CA199, PLR, PNI, cT staging, and cN staging, exhibits significant clinical value, providing supportive evidence for clinicians in developing surgical plans and implementing neoadjuvant therapy. Furthermore, we have initiated a multi-center retrospective analysis and will further refine data from auxiliary diagnostic tools such as laboratory testing and medical imaging examinations, aiming to enhance the accuracy and reliability of LVI prediction. We aspire for hematological indicators to become an additional auxiliary diagnostic method for predicting LVI patients with gastric cancer patients.
Data Sharing Statement
The data that support the results of this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Clinical Research Ethics Committee of Jiangsu Cancer Hospital (No. KY-2024-012-GZ-01 and No. KY-2024-119). Due to retrospective characteristics of the study, informed consent was waived. All patient data was treated with confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Research Fund of Jiangsu Cancer Hospital (No: ZJ202312 and No: XHZD202404).
Disclosure
All authors have no conflicts of interest to declare for this work.
References
1. Kusano C, Ishibashi F, Ichita C, et al. Current status of gastric cancer screening and future perspectives. DEN Open. 2025;6(1):e70148. doi:10.1002/deo2.70148
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
3. Lin L, Wang J, Sheng S, et al. Corosolic acid increases the therapeutic effect of cisplatin on gastric cancer by regulating Gpx4-dependent ferroptosis. Cancer Drug Resist. 2025;8:40. doi:10.20517/cdr.2025.94
4. Zeng F, Cao J, Chen Y, et al. Fra-1 affects chemotherapy sensitivity by inhibiting ferroptosis in gastric cancer cells. Cancer Drug Resist. 2024;7:44. doi:10.20517/cdr.2024.101
5. Wu J, Zhang PF, Zeng Y, et al. Effects of FAP+ cancer-associated fibroblasts on anti-PD-1 immunotherapy and CD4+ T cell polarization in gastric cancer. Cancer Drug Resist. 2025;8:38. doi:10.20517/cdr.2025.97
6. Takano K, Ashikari K, Tamura S, et al. Clinicopathological features of endoscopically treated early gastric cancer with lymphovascular infiltration. J Cancer Res Clin Oncol. 2023;149(9):5781–5790. doi:10.1007/s00432-022-04536-7
7. Wei C, Deng Y, Wei S, et al. Lymphovascular invasion is a significant risk factor for non-sentinel nodal metastasis in breast cancer patients with sentinel lymph node (SLN)-positive breast cancer: a cross-sectional study. World J Surg Oncol. 2023;21(1):386. doi:10.1186/s12957-023-03273-6
8. Dulf DV, Burnar AL, Dulf PL, et al. Lymphovascular invasion is a predictor of clinical outcomes in bladder cancer patients treated with radical cystectomy. J Clin Med. 2025;14(14):5120. doi:10.3390/jcm14145120
9. Jiao X, Wang Y, Fu H, et al. Prognostic significance of lymphovascular invasion in pN0 stage gastric cancer: a propensity score matching analysis. BMC Surg. 2024;24(1):402. doi:10.1186/s12893-024-02705-8
10. Alangari AI, Kim S, Lee HH, et al. Prognostic impact of lymphovascular invasion in node-negative gastric cancer: a retrospective cohort study. World J Surg Oncol. 2024;22(1):340. doi:10.1186/s12957-024-03629-6
11. Sun B, Li H, Gu X, et al. Prognostic implication of lymphovascular invasion in early gastric cancer meeting endoscopic submucosal dissection criteria: insights from radical surgery outcomes. Cancers. 2024;16(5):979. doi:10.3390/cancers16050979
12. Osumi H, Kawachi H, Murai K, et al. Risk stratification for lymph node metastasis using Epstein-Barr virus status in submucosal invasive (pT1) gastric cancer without lymphovascular invasion: a multicenter observational study. Gastric Cancer. 2019;22(6):1176–1182. doi:10.1007/s10120-019-00963-7
13. Wu L, Liang Y, Zhang C, et al. Prognostic significance of lymphovascular infiltration in overall survival of gastric cancer patients after surgery with curative intent. Chin J Cancer Res. 2019;31(5):785–796. doi:10.21147/j.issn.1000-9604.2019.05.08
14. Rihawi K, Ricci AD, Rizzo A, et al. Tumor-associated macrophages and inflammatory microenvironment in gastric cancer: novel translational implications. Int J Mol Sci. 2021;22(8):3805. doi:10.3390/ijms22083805
15. Ma J, Shi Y, Lu Q, et al. Inflammation-related gene ADH1A regulates the polarization of macrophage M1 and influences the malignant progression of gastric cancer. J Inflamm Res. 2024;17:4647–4665. doi:10.2147/JIR.S452670
16. Piotrowski I, Kulcenty K, Suchorska W. Interplay between inflammation and cancer. Rep Pract Oncol Radiother. 2020;25(3):422–427. doi:10.1016/j.rpor.2020.04.004
17. Wang Y, Wang J, Xie K, et al. The role of systemic inflammation in the formation and rupture of intracranial aneurysms in moyamoya disease: a retrospective cohort study. Ann Med. 2025;57(1):2521448. doi:10.1080/07853890.2025.2521448
18. Mantovani A, Garlanda C, Allavena P. Molecular pathways and targets in cancer-related inflammation. Ann Med. 2010;42(3):161–170. doi:10.3109/07853890903405753
19. Coffelt SB, Wellenstein MD, de Visser KE. Neutrophils in cancer: neutral no more. Nat Rev Cancer. 2016;16(7):431–446. doi:10.1038/nrc.2016.52
20. Fridlender ZG, Albelda SM. Tumor-associated neutrophils: friend or foe? Carcinogenesis. 2012;33(5):949–955. doi:10.1093/carcin/bgs123
21. Granot Z, Jablonska J. Distinct functions of neutrophil in cancer and its regulation. Mediators Inflamm. 2015;2015(1):701067. doi:10.1155/2015/701067
22. Smith HA, Kang Y. The metastasis-promoting roles of tumor-associated immune cells. J Mol Med. 2013;91(4):411–429. doi:10.1007/s00109-013-1021-5
23. Bai Z, Zhou Y, Ye Z, et al. Tumor-infiltrating lymphocytes in colorectal cancer: the fundamental indication and application on immunotherapy. Front Immunol. 2022;12:808964. doi:10.3389/fimmu.2021.808964
24. Yang Z, Wang Y, Wang C, et al. Preoperative platelet-to-lymphocyte ratio and lymphocyte-to-monocyte ratio predict poor prognosis in patients diagnosed with salivary gland adenoid cystic carcinoma. J Craniomaxillofac Surg. 2025;53(7):970–976. doi:10.1016/j.jcms.2025.01.017
25. Chen X, Mohammed AF, Li C. Assessment of the clinical value of platelet-to-lymphocyte ratio in patients with hepatocellular carcinoma. Clin Appl Thromb Hemost. 2024;30:10760296231221535. doi:10.1177/10760296231221535
26. Zhang L, Liu X, Yang R, et al. The diagnostic value of the systemic immune-inflammation index for venous thromboembolism in lung cancer patients: a retrospective study. Mediators Inflamm. 2022;2022:9215311. doi:10.1155/2022/9215311
27. Jiang P, Zheng L, Yang Y, et al. Establishment and validation of a prediction model for gastric cancer with perineural invasion based on preoperative inflammatory markers. Transl Cancer Res. 2024;13(10):5381–5394. doi:10.21037/tcr-24-481
28. Zhang J, Shen PH, Wu JB, et al. Development and validation of a nomogram model based on vascular entry sign for predicting lymphovascular invasion in gastric cancer. Abdom Radiol. 2025;50(9):4015–4022. doi:10.1007/s00261-025-04812-3
29. Xue XQ, Li XF, Shi X, et al. The correlation between preoperative total lesion glycolysis and lymphovascular invasion based on 18F-FDG PET/CT and its predictive value in primary gastric cancer: a cross-sectional study. Quant Imaging Med Surg. 2025;15(9):7738–7748. doi:10.21037/qims-2025-644
30. Lee SH, Kim MC, Jeon SW, et al. Risk factors and clinical outcomes of non-curative resection in patients with early gastric cancer treated with endoscopic submucosal dissection: a retrospective multicenter study in Korea. Clin Endosc. 2020;53(2):196–205. doi:10.5946/ce.2019.123
31. Lu J, Dai Y, Xie JW, et al. Combination of lymphovascular invasion and the AJCC TNM staging system improves prediction of prognosis in N0 stage gastric cancer: results from a high-volume institution. BMC Cancer. 2019;19(1):216. doi:10.1186/s12885-019-5416-8
32. Kubota K, Ito R, Narita N, et al. Utility of prognostic nutritional index and systemic immune-inflammation index in oral cancer treatment. BMC Cancer. 2022;22(1):368. doi:10.1186/s12885-022-09439-x
33. Ryan MP, Winsett FT, Armenta AM, et al. Lymphovascular invasion in cutaneous squamous cell carcinoma. Dermatol Surg. 2024;50(8):699–704. doi:10.1097/DSS.0000000000004187
34. Mo DP, Wang CX, Wang X, et al. Predictive value of preoperative inflammatory markers in gastric cancer with lymphovascular invasion (in Chinese). Chin J Clin Res. 2023;36(09):1307–1311. doi:10.13429/j.cnki.cjcr.2023.09.006
35. Kikuchi E, Margulis V, Karakiewicz PI, et al. Lymphovascular invasion predicts clinical outcomes in patients with node-negative upper tract urothelial carcinoma. J Clin Oncol. 2009;27(4):612–618. doi:10.1200/JCO.2008.17.2361
36. Chen W, Wang Y, Bai G, et al. Can lymphovascular invasion be predicted by preoperative contrast-enhanced CT in esophageal squamous cell carcinoma? Technol Cancer Res Treat. 2022;21:15330338221111229. doi:10.1177/15330338221111229
37. Zhang F, Chen H, Luo D, et al. Lymphovascular or perineural invasion is associated with lymph node metastasis and survival outcomes in patients with gastric cancer. Cancer Med. 2023;12(8):9401–9408. doi:10.1002/cam4.5701
38. Tong YX, Ye X, Chen YQ, et al. A nomogram model of spectral CT quantitative parameters and clinical characteristics predicting lymphovascular invasion of gastric cancer. Heliyon. 2024;10(7):e29214. doi:10.1016/j.heliyon.2024.e29214
39. Sumiyoshi S, Ohashi T, Kubota T, et al. Lymphovascular invasion is associated with poor long-term outcomes in patients with pT1N0-3 or pT2-3N0 remnant gastric cancer: a retrospective cohort study. World J Surg Oncol. 2024;22(1):86. doi:10.1186/s12957-024-03371-z
40. Chen X, Yang Z, Yang J, et al. Radiomics analysis of contrast-enhanced CT predicts lymphovascular invasion and disease outcome in gastric cancer: a preliminary study. Cancer Imag. 2020;20(1):24. doi:10.1186/s40644-020-00302-5
41. Wu C, Hu H, Bao F, et al. Development of a multimodal predictive model using PET/CT radiomics and clinical data for preoperative assessment of lymphovascular invasion in gastric cancer. Am J Transl Res. 2025;17(7):5441–5452. doi:10.62347/PBNU9406
42. Sun X, Wang P, Ding R, et al. Preoperative prediction value of 2.5D deep learning model based on contrast-enhanced CT for lymphovascular invasion of gastric cancer. Sci Rep. 2025;15(1):25646. doi:10.1038/s41598-025-11427-7
43. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
44. Gan J, Zhang X, Guo J. The role of platelets in tumor immune evasion and metastasis: mechanisms and therapeutic implications. Cancer Cell Int. 2025;25(1):258. doi:10.1186/s12935-025-03877-w
45. Raskov H, Orhan A, Agerbæk MØ, et al. The impact of platelets on the metastatic potential of tumour cells. Heliyon. 2024;10(14):e34361. doi:10.1016/j.heliyon.2024.e34361
46. Ward Y, Lake R, Faraji F, et al. Platelets promote metastasis via binding tumor CD97 leading to bidirectional signaling that coordinates transendothelial migration. Cell Rep. 2018;23(3):808–822. doi:10.1016/j.celrep.2018.03.092
47. Feng F, Zheng G, Wang Q, et al. Low lymphocyte count and high monocyte count predicts poor prognosis of gastric cancer. BMC Gastroenterol. 2018;18(1):148. doi:10.1186/s12876-018-0877-9
48. Nogueiro J, Santos-Sousa H, Pereira A, et al. The impact of the prognostic nutritional index (PNI) in gastric cancer. Langenbecks Arch Surg. 2022;407(7):2703–2714. doi:10.1007/s00423-022-02627-0
49. Xu R, Xiao S, Ding Z, et al. The value of the C-reactive protein-to-lymphocyte ratio for predicting lymphovascular invasion based on nutritional status in gastric cancer. Technol Cancer Res Treat. 2022;21:15330338221106517. doi:10.1177/15330338221106517
50. Zheng J, Zheng L, Wang X, et al. The clinical value of the combined detection of systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and prognostic nutritional index (PNI) in early diagnosis of gastric cancer. J Inflamm Res. 2025;18:813–826. doi:10.2147/JIR.S496703
51. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017;20(1):1–19. doi:10.1007/s10120-016-0622-4
52. Maehara Y, Kabashima A, Koga T, et al. Vascular invasion and potential for tumor angiogenesis and metastasis in gastric carcinoma. Surgery. 2000;128(3):408–416. doi:10.1067/msy.2000.107265
53. Zhang X, Zhao W, Yu Y, et al. Clinicopathological and prognostic significance of platelet-lymphocyte ratio (PLR) in gastric cancer: an updated meta-analysis. World J Surg Oncol. 2020;18(1):191. doi:10.1186/s12957-020-01952-2
54. Jia H, Tan Y, Li H, et al. A nomogram model for predicting risk factors and the outcome of skin ulcer. Ann Med. 2025;57(1):2525404. doi:10.1080/07853890.2025.2525404
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.