Back to Journals » Journal of Pain Research » Volume 15
The Value of Dynamic Fracture Mobility in Determining the Optimum Operation Choice for Acute Osteoporotic Vertebral Compression Fracture
Authors Ren H, Feng T, Hu Y, Yao G, Yu D, Cao J
Received 31 March 2022
Accepted for publication 27 July 2022
Published 13 August 2022 Volume 2022:15 Pages 2327—2336
DOI https://doi.org/10.2147/JPR.S368493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
Hu Ren, Tao Feng, Yaning Hu, Guangqing Yao, Dahai Yu, Jianhui Cao
Department of Orthopedic Surgery, Shijiazhuang People’s Hospital, Shijiazhuang, People’s Republic of China
Correspondence: Jianhui Cao, Department of Orthopedic Surgery, Shijiazhuang People’s Hospital, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected]
Purpose: This retrospective study aimed to verify whether the use of a balloon in balloon kyphoplasty (BKP) could offer a higher degree of vertebral height restoration and deformity correction than percutaneous vertebroplasty (PVP) after adjustment for preoperative dynamic fracture mobility. We expect that this research will help surgeons to determine the optimum operation choice (PVP or BKP) for treating osteoporotic vertebral compression fractures (OVCFs).
Patients and Methods: We evaluated retrospectively 262 patients who were treated by PVP or BKP for acute, single-level OVCF at our institution from July 2015 to July 2019. According to the presence or absence of dynamic fracture mobility, the patients were divided into two groups: mobile group and fixed group. We compared the changes in the vertebral height and kyphotic angle for PVP and BKP, respectively, within each group.
Results: In the mobile group, the anterior vertebral height restoration (BKP group, 8.73± 5.27%; PVP group, 2.96± 1.59%), middle vertebral height restoration (BKP group, 7.58± 5.18%; PVP group, 2.74± 1.24%) and kyphotic angle correction (BKP group, 4.41± 4.46°; PVP group, 1.38± 1.60°) due to percutaneous vertebral augmentation technique itself were more obvious in BKP group compared with PVP group (P < 0.05). The BKP group has lower incidence of bone cement leakage (BKP group, 10.17%; PVP group, 25.53%, P < 0.05). In the fixed group, differences from comparison of changes were not statistically significant between PVP and BKP (P > 0.05).
Conclusion: The use of a balloon in BKP could offer greater kyphosis correction, higher vertebral body height restoration, and lower cement leakage rate than PVP if a fractured vertebral body existed dynamic mobility. However, all these advantages of BKP over PVP are not obvious and could be overrated for a fixed fracture exhibited no mobility. BKP is recommended for a fractured vertebral body with dynamic mobility. PVP is suggested for a fixed fractured vertebral body with no mobility as it produces similar capability of vertebral height restoration, kyphosis correction, and cement leakage as BKP.
Keywords: dynamic fracture mobility, optimum operation choice, osteoporotic vertebral compression fracture, balloon kyphoplasty, percutaneous vertebroplasty
Introduction
Osteoporosis is recognized as a serious public health problem.1 The worldwide prevalence of osteoporosis among the elderly was reported to be 21.7%.2 Osteoporotic vertebral compression fractures (OVCFs) account for 27% of total osteoporosis-related fractures,3 which is a common clinical issue in modern society.4 In addition to the debilitating symptoms of pain that OVCFs can cause, progressive loss of sagittal alignment can have a tremendous impact on quality of life.5–7 Since percutaneous vertebroplasty (PVP) was introduced in 1987, multiple studies have documented the effectiveness of the procedure for relieving or decreasing pain caused by OVCFs.8 However, PVP was limited in correcting local kyphosis, restoring the vertebral body height and reducing bone cement leakage.9 Balloon kyphoplasty (BKP) was developed to compensate for these shortcomings of PVP.10,11 However, this capability remains controversial up to now. Many clinical studies reported that balloon inflation did not significantly further increase vertebral height or correct local kyphosis.12–15 Compared with PVP, BKP has longer operation time, more complex operation process and higher material cost.16 Because there is no clearly proven superiority of one technique over the other, there is still no consensus on how to choose vertebral augmentation technique (PVP or BKP) for a patient with a unique OVCF.17,18
McKiernan et al demonstrated the previously unrecognized occurrence of dynamic fracture mobility in many OVCFs for the first time in 2003.19 Spontaneous reduction in deformity that may occur when the patient is placed in prone position has not been taken into adequate account before this study was published. They concluded that there must be control for the occurrence of dynamic mobility of the fractured vertebrae as long as vertebral height restoration and deformity correction are claimed. From then on, many authors have reported that the presence of vertebral mobility greatly influenced the vertebral height restoration and deformity correction achieved with PVP or BKP.20–22 These studies have taken account of dynamic fracture mobility but studied on patients with either PVP or BKP procedure. There is a lack of comparison and study regarding height restoration and deformity correction across PVP and BKP. Therefore, it is hard to draw meaningful conclusion about independent effect of surgery.
For these reasons, this retrospective study aimed to verify whether the use of a balloon in BKP could offer a higher degree of vertebral height restoration and deformity correction than PVP after adjustment for preoperative dynamic fracture mobility. We expect that this research will help surgeons to determine the optimum operation choice (PVP or BKP) for treating OVCFs.
Materials and Methods
Patient Population
We evaluated retrospectively 262 patients who were treated by PVP or BKP for acute (fracture duration <6 weeks), single-level OVCF at our institution from July 2015 to July 2019. Because the cost of the two procedures varies greatly, the choice of surgery has to depend partly on the patient’s financial situation. Surgical indications included focal, severe, intractable pain at the level of a known acute OVCF with no or minimally responded to a course of conservative medical treatment. Contraindications included infection, pain not related to a fracture and definite neurological deficits. The patients without complete clinical and radiological data were excluded. If the nearest nonfractured vertebra is deformed, the case was also excluded because the referent vertebral height (see later) could not be measured. There were 45 males and 217 females, and the mean age was 71.88 years (range, 58–91 years). The mean fracture duration was 3.49 weeks (range, 1–6 weeks) before surgery. The mean follow-up time was 12.6 months (range, 6 to 18 months).
Surgical Technique
All PVP and BKP procedures were done by the same operator with local anesthesia under lateral and anteroposterior fluoroscopic guidance. The patient was monitored and placed in the prone position using the Cawley technique.23 Supports were positioned under the iliac crests and either side of the upper thorax. The arms were abducted. Two columns of pillows were positioned under the legs so that the hips were maximally extended. The table can be flexed as needed to increase. While in this position, an intraoperative prone position radiograph centered on the fractured vertebra was obtained for each patient. The spontaneous height restoration and deformity correction during this position were considered to be solely due to dynamic fracture mobility. Then, PVP or BKP was performed with a bipedicular approach according to the standard operating procedures. Polymethylmethacrylate bone cement was injected until a satisfactory distribution of the cement or cement leakage was noted. The additional height restoration and deformity correction during this process were attributed to the percutaneous vertebral augmentation technique itself. After the procedure, the patient was transferred to the patients’ room for further guardianship. If the condition was steady, they were discharged later and were advised on anti-osteoporosis treatment.
Imaging Evaluation
All the patients underwent routine preoperative imaging: standing anterior-posterior and lateral radiographs centered on the fractured vertebra, computed tomography (CT), and magnetic resonance imaging (MRI). CT examination was used for evaluating the integrality of vertebral body wall. MRI studies were obtained and reviewed to analyze other causes of symptoms and persistence edema in the fractured vertebrae. An intravertebral cleft was defined as an intravertebral, abnormal, well-demarcated, linear or cystic hypointensity similar to air on preoperative radiography or T1-weighted MRI sequences; an abnormal, well-demarcated, linear or cystic hyperintensity similar to cerebrospinal fluid on STIR sequences.24 Fracture morphology was classified according to the classification of Genant et al.25 The mean bone density of lumbar vertebrae was measured by dual-energy X-ray absorptiometry (DEXA) prior to surgery. After operation, postoperative antero-posterior and lateral radiographs and CT examination were also examined for the evaluation of surgical effect and the presence of leakage of cement.
The anterior, middle vertebral height and kyphotic angle were measured at three different time points: 1) Preoperative standing lateral X-ray, 2) intraoperative after placing the patient in prone hyperextended position on the operation table, 3) postoperative (at last follow-up after surgery) standing lateral X-ray on the basis of the techniques used in previous studies. The fractured vertebral height was expressed as a percentage of referent vertebral height (the nearest nonfractured vertebra).26,27 This process cancelled out possible magnification effects and inter-radiographic precision errors and allowed direct radiographic comparisons. Kyphotic angle was measured from the superior and inferior endplates of the fractured vertebra.28
Dynamic fracture mobility was considered to be present when any measurable change in vertebral body kyphotic angle or vertebral body height occurred between preoperative standing lateral radiographs and intraoperative prone position radiographs.29 Fractures with no measurable changes were considered fixed. Based on this standard, the patients were divided into two groups: mobile group and fixed group.
Clinical Evaluation
The patients were assessed by visual analogue scale (VAS) (ranged from 0 to 10; 0: no pain, 10: worst pain) before and after surgery. We assessed the following clinical and radiological characteristics of patients: age, sex, fracture duration, bone mineral density, spinal segment of fracture, fracture morphology, vertebral body wall violation, intravertebral cleft, cement volume injected, cement leak, anterior vertebral height, middle vertebral height, and kyphotic angle.
Statistical Analysis
Software (SPSS 17.0) was used for statistical analysis. The results are expressed as the mean± SD. Comparison of the preoperative, intraoperative, and postoperative assessments with each treatment were analyzed by paired-sample t-test. Differences between the two treatment techniques were analyzed by the Mann–Whitney U-test for continuous variables and Chi-squared test for categorical variables. P < 0.05 was considered to indicate a statistically significant difference.
Results
Of these 262 patients, 122 patients received PVP and 140 patients received BKP. Almost all of the patients had rapid and significant improvement in back pain following surgery and no serious complications occurred. Both procedures appeared to provide a similar level of pain relief after surgery (P > 0.05).
According to the presence or absence of dynamic fracture mobility, the mobile group had 106 patients including 47 PVP patients and 59 BKP patients, the fixed group had 156 patients including 75 PVP patients and 81 BKP patients. Clinical and radiological characteristics of patients in two groups were, respectively, shown in Tables 1 and 2. There was no significant difference between the two treatment groups in all the following clinical and radiological characteristics: age, sex, fracture duration, bone mineral density, spinal segment of fracture, fracture morphology, vertebral body wall violation, intravertebral cleft, cement volume injected, preoperative VAS, preoperative anterior, middle vertebral height and preoperative kyphotic angle (P > 0.05), which made them comparable.
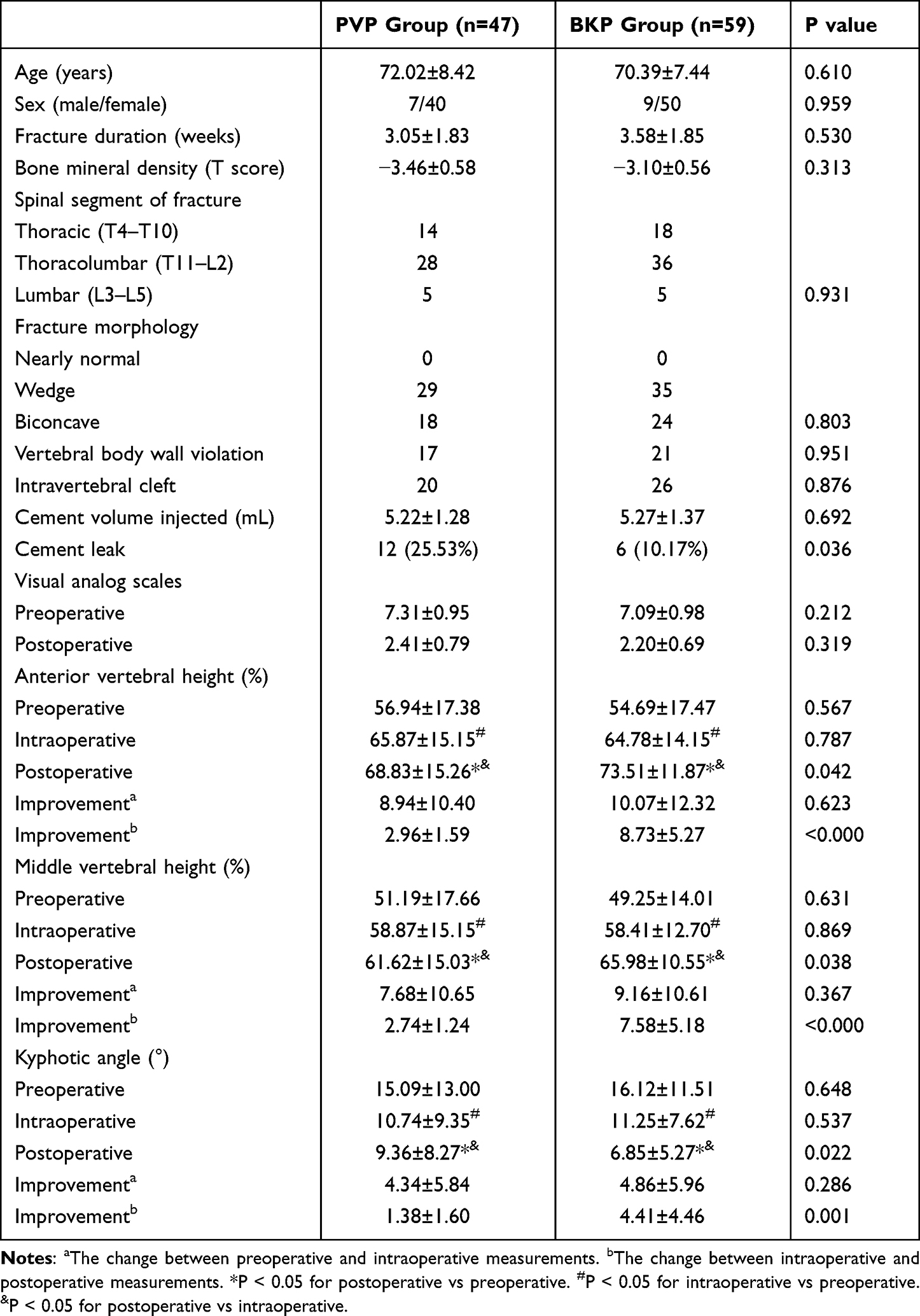 |
Table 1 Clinical and Radiological Characteristics of Patients in Mobile Group |
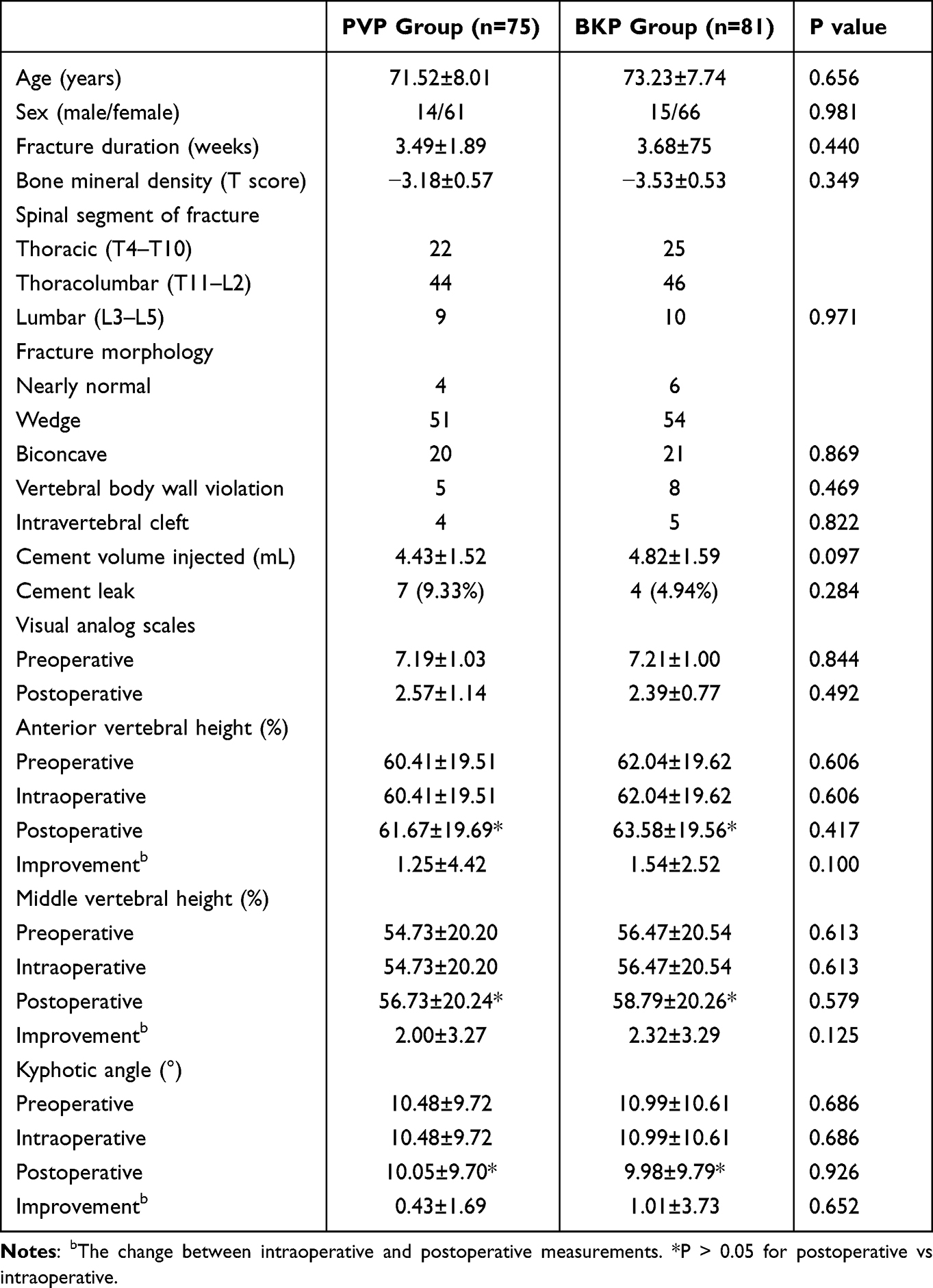 |
Table 2 Clinical and Radiological Characteristics of Patients in Fixed Group |
At a vertebra-by-vertebra level analysis in mobile group, a significant gain of the vertebral height and a significant reduction of the kyphotic angle were observed when the patient was placed in prone position compared with the preoperative imaging (P < 0.05). There was no significant difference between the two treatment groups in the anterior, middle vertebral height restoration and kyphotic angle correction due to dynamic fracture mobility (P > 0.05). After operation, both PVP and BKP improved vertebral body height and kyphotic angle of the fractured vertebral body compared with the intraoperative imaging (P < 0.05). The anterior vertebral height restoration (BKP group, 8.73±5.27%; PVP group, 2.96±1.59%), middle vertebral height restoration (BKP group, 7.58±5.18%; PVP group, 2.74±1.24%) and kyphotic angle correction (BKP group, 4.41±4.46°; PVP group, 1.38±1.60°) due to percutaneous vertebral augmentation technique itself were more obvious in BKP group compared with PVP group (P < 0.05) (Figures 1–3). The BKP group has lower incidence of bone cement leakage (BKP group, 10.17%; PVP group, 25.53%, P < 0.05). In the fixed group, the anterior vertebral height restoration (BKP group, 1.54±2.52%; PVP group, 1.25±4.42%), middle vertebral height restoration (BKP group, 2.32±3.29%; PVP group, 2.00±3.27%) and kyphotic angle correction (BKP group, 1.01±3.73°; PVP group, 0.43±1.69°) due to percutaneous vertebral augmentation technique itself were not statistically significant between PVP and BKP (P > 0.05) (Figure 4). The cement leakage rate was not statistically different when PVP and BKP were compared (BKP group, 4.94%; PVP group, 9.33%, P > 0.05).
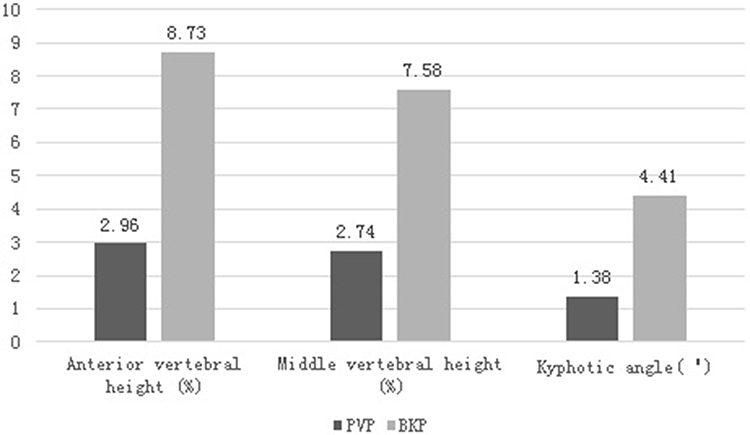 |
Figure 1 The vertebral height restoration and kyphotic angle correction attributed to the percutaneous vertebral augmentation technique in mobile group. P < 0.05 for PVP vs BKP in every measurement. |
 |
Figure 2 The patient was a 69-year-old woman with a T12 osteoporotic vertebral compression fracture and balloon kyphoplasty was performed. The yellow line indicates the kyphotic angle. The kyphotic angle changed from 22.06° in preoperative standing lateral radiographs (A) to 17.66° in intraoperative prone lateral radiographs (B). So the dynamic fracture mobility was present. After operation, the kyphotic angle changed to 9.27° in postoperative standing lateral radiographs (C). The kyphotic angle correction due to balloon kyphoplasty itself was 8.39°. |
 |
Figure 3 The patient was a 65-year-old woman with a T12 osteoporotic vertebral compression fracture and percutaneous vertebroplasty was performed. The yellow line indicates the kyphotic angle. The kyphotic angle changed from 20.61° in preoperative standing lateral radiographs (A) to 17.36° in intraoperative prone lateral radiographs (B). So the dynamic fracture mobility was present. After operation, the kyphotic angle changed to 15.87° in postoperative standing lateral radiographs (C). The kyphotic angle correction due to percutaneous vertebroplasty itself was 1.49°. |
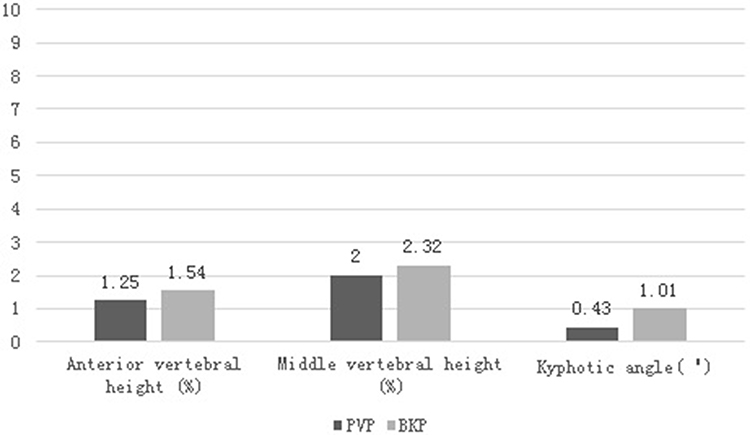 |
Figure 4 The vertebral height restoration and kyphotic angle correction attributed to the percutaneous vertebral augmentation technique in fixed group. P>0.05 for PVP vs BKP in every measurement. |
Discussion
During the past two decades, PVP and BKP have been widely used for treating OVCFs. Both techniques are safe and effective with a similar long-term pain relief in an elderly patient.30 However, there is some debate about the effectiveness of both procedures in vertebral height restoration and deformity correction.12–15 McKiernan et al demonstrated the previously unrecognized occurrence of dynamic fracture mobility in many OVCFs for the first time in 2003.19 The fractured vertebral height spontaneously expands due to the prone position during surgery which has not been considered in previous studies on vertebral augmentation technique. Reporting any intervention that claims to restore vertebral body height and correct local kyphosis but does not carefully control for dynamic fracture mobility seems untenable.19 From then on, there is broad agreement that dynamic fracture mobility is attributed to restore height and reduce kyphotic angle.20–22 However, the effect of the vertebral augmentation technique itself remains inconsistent. Chen et al found that the restoration of vertebral body height in PVP seems to be mostly due to the dynamic fracture mobility and PVP itself does not contribute much to the restoration of vertebral height.20 Chee Kidd Chiu et al also supported the above view.21 They found that the dynamic mobility stress radiographs can predict the postoperative vertebral height restoration and kyphosis correction after PVP for OVCFs. In terms of BKP, Yokoyama et al found that the vertebral height restoration and kyphotic change largely depended on the preoperative vertebral mobility in both PVP and BKP groups. The use of a balloon itself contributed little to resolution of the vertebral deformities.31 But Shindle et al had inconsistent results, they reported on 25 consecutive patients with a total of 43 OVCFs treated with BKP and found that many fractured vertebrae can be moved with positioning, balloon inflation enhanced the height reduction >4.5-fold over the positioning maneuver alone and accounted for over 80% of the ultimate reduction.22 Although these studies considered dynamic fracture mobility, they looked at only one procedure in the same group of patients. Different methods in the assessment of height restoration and deformity correction in these studies make it difficult to provide a direct comparison of independent effect of surgery.
For the above reasons, this study is to explore the independent effects of two surgical methods. We compared the changes in the vertebral height and kyphotic angle between patients treated by PVP and BKP after adjustment for preoperative dynamic fracture mobility. Our results showed that after hyperextended prone positioning was established, BKP could bring more significant improvements in vertebral body height and kyphotic angle compared with PVP in mobile group. At the same time, we also found that the incidence of bone cement leakage is lower in BKP group if a fractured vertebral body existed dynamic mobility. We speculate that the structure of a mobile fracture is more severely damaged compared with a fixed fracture. And, there is more space for expansion in the discontinuous fracture gaps. The height restoration and deformity correction in PVP itself is only attributed to the diffusion of bone cement which was injected under greater pressure. Compared with PVP, the use of a balloon in BKP can squeeze the surrounding bone for greater expansion force and less bone cement injection pressure. It can obtain better purpose of correcting the deformity and restoring the vertebral body height while reducing the risk of bone cement leakage. However, all these advantages of BKP over PVP are not obvious for a fixed fracture with no mobility.
It has been widely accepted that percutaneous vertebral augmentation offers a minimally invasive therapy to reduce pain and improve functional outcomes in patients with OVCFs. But the optimum operation choice (PVP or BKP) remains controversial.17,18 The early adoption of BKP by surgeon can partially be attributed to the utility of BKP had greater kyphosis correction, higher vertebral body height restoration, and lower cement leakage rate when compared with PVP. However, this technique has longer operation time, more complex operation process and higher material cost.16 In addition, each different type of vertebral fracture is unique and can change over time. Dynamic fracture mobility has not been considered as a reference index to determine the optimum operation choice for treating OVCFs in previous studies. As the results shown in this study, dynamic fracture mobility can help surgeon estimate the postoperative vertebral height restoration, kyphosis correction, and cement leakage rate after PVP or BKP. We speculate that this observational index will help surgeon to determine appropriate surgical technique for a patient with a unique OVCF. If dynamic mobility of a fractured vertebral body existed, BKP is recommended as the first-line surgical augmentation technique due to the merits as described above. If a fractured vertebral body is fixed, PVP may be an adequate and favorable option. It could produce similar capability of vertebral height restoration, kyphosis correction, and cement leakage as BKP for this type of fracture. In the meantime, the operation time is shorter, the procedure is simpler, and the cost is more affordable. All of these factors are important for a frail elderly patient.
It is important to investigate the evidence of dynamic fracture mobility before surgery. The traditional standing flexion and extension lateral radiographs are difficult to examine in many cases of OVCFs because the patients are unable to follow the exact position due to severe pain. In addition, the risk of further collapse is also a limitation of this examination. Several authors adopt supine cross-table lateral radiographs examination for evaluating dynamic mobility.21,32 A bolster with the diameter of about 13.0 cm should be placed at the level of painful fracture vertebra on the back. For old OVCF patients, this examination is also difficult to obtain due to severe pain. The supine position cannot reflect a real operative position. For these reasons, we adopted intraoperative prone cross-table lateral radiographs as a diagnostic tool for dynamic fracture mobility, which was recommended by Cawley et al.23,29,33,34 This positioning technique reduced provoked pain, advanced anterior vertebral height restoration, and supported vertebral deformities correction.
There were several limitations to this study. First, there might be measurement error even with attempts to cancel out possible radiograph magnification effects. Second, this study was a retrospective study among a small number of patients, so the sample size is relatively small. A larger multicenter study may help confirm this result.
Conclusions
The use of a balloon in BKP could offer greater kyphosis correction, higher vertebral body height restoration, and lower cement leakage rate than PVP if a fractured vertebral body existed dynamic mobility. However, all these advantages of BKP over PVP are not obvious and could be overrated for a fixed fracture exhibited no mobility. BKP is recommended for a fractured vertebral body with dynamic mobility. PVP is suggested for a fixed fractured vertebral body with no mobility as it produces similar capability of vertebral height restoration, kyphosis correction, and cement leakage as BKP.
Abbreviations
BKP, balloon kyphoplasty; PVP, percutaneous vertebroplasty; OVCF, osteoporotic vertebral compression fracture; CT, computed tomography; MRI, magnetic resonance imaging; DEXA, dual-energy X-ray absorptiometry; VAS, visual analogue scale.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to the data is confidential patient data but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study protocol was approved by the Ethics Committee of Shijiazhuang People’s Hospital before acquiring and analyzing patients’ information. Informed written consent was obtained from all patients. This study was conducted in accordance with the Declaration of Helsinki.
Funding
This research was supported by the Department of Health of Hebei Province (20210580).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnston CB, Dagar M. Osteoporosis in older adults. Med Clin North Am. 2020;104(5):873–884. doi:10.1016/j.mcna.2020.06.004
2. Salari N, Darvishi N, Bartina Y, et al. Global prevalence of osteoporosis among the world older adults: a comprehensive systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):669. doi:10.1186/s13018-021-02821-8
3. Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22(3):465–475. doi:10.1359/jbmr.061113
4. Prost S, Pesenti S, Fuentes S, Tropiano P, Blondel B. Treatment of osteoporotic vertebral fractures. Orthop Traumatol Surg Res. 2021;107(1S):102779. doi:10.1016/j.otsr.2020.102779
5. Zhang YL, Shi LT, Tang PF, Sun ZJ, Wang YH. Correlation analysis of osteoporotic vertebral compression fractures and spinal sagittal imbalance. Orthopade. 2017;46(3):249–255. doi:10.1007/s00132-016-3359-1
6. Pradhan BB, Bae HW, Kropf MA, Patel VV, Delamarter RB. Kyphoplasty reduction of osteoporotic vertebral compression fractures: correction of local kyphosis versus overall sagittal alignment. Spine. 2006;31(4):435–441. doi:10.1097/01.brs.0000200036.08679.1e
7. Goldstein CL, Chutkan NB, Choma TJ, Orr RD. Management of the elderly with vertebral compression fractures. Neurosurgery. 2015;77(Suppl 4):S33–45. doi:10.1227/NEU.0000000000000947
8. Kushchayev SV, Wiener PC, Teytelboym OM, Arrington JA, Khan M, Preul MC. Percutaneous vertebroplasty: a history of procedure, technology, culture, specialty, and economics. Neuroimaging Clin N Am. 2019;29(4):481–494. doi:10.1016/j.nic.2019.07.011
9. Hu KZ, Chen SC, Xu L. Comparison of percutaneous balloon dilation kyphoplasty and percutaneous vertebroplasty in treatment for thoracolumbar vertebral compression fractures. Eur Rev Med Pharmacol Sci. 2018;22(1 Suppl):96–102. doi:10.26355/eurrev_201807_15370
10. Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001;26(14):1631–1638. doi:10.1097/00007632-200107150-00026
11. Lee JK, Jeong HW, Joo IH, Ko YI, Kang CN. Percutaneous balloon kyphoplasty for the treatment of very severe osteoporotic vertebral compression fractures: a case-control study. Spine J. 2018;18(6):962–969. doi:10.1016/j.spinee.2017.10.006
12. Hiwatashi A, Westesson PL, Yoshiura T, et al. Kyphoplasty and vertebroplasty produce the same degree of height restoration. AJNR Am J Neuroradiol. 2009;30(4):669–673. doi:10.3174/ajnr.A1442
13. Dohm M, Black CM, Dacre A, Tillman JB, Fueredi G; KAVIAR investigators. A randomized trial comparing balloon kyphoplasty and vertebroplasty for vertebral compression fractures due to osteoporosis. Am J Neuroradiol. 2014;35(12):2227–2236. doi:10.3174/ajnr.A4127
14. Evans AJ, Kip KE, Brinjikji W, et al. Randomized controlled trial of vertebroplasty versus kyphoplasty in the treatment of vertebral compression fractures. J Neurointerv Surg. 2016;8(7):756–763. doi:10.1136/neurintsurg-2015-011811
15. Xu C, Liu HX, Xu HZ. Analysis of related factors on the deformity correction of balloon kyphoplasty. AJNR Am J Neuroradiol. 2014;35(1):202–206. doi:10.3174/ajnr.A3617
16. Svedbom A, Alvares L, Cooper C, Marsh D, Ström O. Balloon kyphoplasty compared to vertebroplasty and nonsurgical management in patients hospitalised with acute osteoporotic vertebral compression fracture: a UK cost-effectiveness analysis. Osteoporos Int. 2013;24(1):355–367. doi:10.1007/s00198-012-2102-y
17. Kan SL, Yuan ZF, Chen LX, Sun JC, Ning GZ, Feng SQ. Which is best for osteoporotic vertebral compression fractures: balloon kyphoplasty, percutaneous vertebroplasty or non-surgical treatment? A study protocol for a Bayesian network meta-analysis. BMJ Open. 2017;7(1):e012937. doi:10.1136/bmjopen-2016-012937
18. Filippiadis DK, Marcia S, Masala S, Deschamps F, Kelekis A. Percutaneous vertebroplasty and kyphoplasty: current status, new developments and old controversies. Cardiovasc Intervent Radiol. 2017;40(12):1815–1823. doi:10.1007/s00270-017-1779-x
19. McKiernan F, Jensen R, Faciszewski T. The dynamic mobility of vertebral compression fractures. J Bone Miner Res. 2003;18(1):24–29. doi:10.1359/jbmr.2003.18.1.24
20. Chen YJ, Chen HY, Tsai PP, Lo DF, Chen HT, Hsu HC. Significance of dynamic mobility in restoring vertebral body height in vertebroplasty. AJNR Am J Neuroradiol. 2012;33(1):57–60. doi:10.3174/ajnr.A2726
21. Chiu CK, Lisitha KA, Elias DM, Yong VW, Chan CYW, Kwan MK. Do the dynamic stress mobility radiographs predict the postoperative vertebral height restoration, kyphosis correction, and cement volume injected after vertebroplasty for osteoporotic thoracolumbar vertebral fractures with intravertebral cleft? J Orthop Surg. 2018;26(3):2309499018806700. doi:10.1177/2309499018806700
22. Shindle MK, Gardner MJ, Koob J, Bukata S, Cabin JA, Lane JM. Vertebral height restoration in osteoporotic compression fractures: kyphoplasty balloon tamp is superior to postural correction alone. Osteoporos Int. 2006;17(12):1815–1819. doi:10.1007/s00198-006-0195-x
23. Cawley DT, Sexton P, Murphy T, McCabe JP. Optimal patient positioning for ligamentotaxis during balloon kyphoplasty of the thoracolumbar and lumbar spine. J Clin Neurosci. 2011;18(6):834–836. doi:10.1016/j.jocn.2010.10.009
24. Nieuwenhuijse MJ, van Rijswijk CS, van Erkel AR, Dijkstra SP. The intravertebral cleft in painful long-standing osteoporotic vertebral compression fractures treated with percutaneous vertebroplasty: diagnostic assessment and clinical significance. Spine. 2012;37(11):974–981. doi:10.1097/BRS.0b013e318238bf22
25. Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993;8(9):1137–1148. doi:10.1002/jbmr.5650080915
26. McKiernan F, Faciszewski T, Jensen R. Reporting height restoration in vertebral compression fractures. Spine. 2003;28(22):2517–2521. doi:10.1097/01.BRS.0000092424.29886.C9
27. Kuklo TR, Polly DW, Owens BD, Zeidman SM, Chang AS, Klemme WR. Measurement of thoracic and lumbar fracture kyphosis: evaluation of intraobserver, interobserver, and technique variability. Spine. 2001;26(1):61–65. doi:10.1097/00007632-200101010-00012
28. Sadiqi S, Verlaan JJ, Lehr AM, et al. Measurement of kyphosis and vertebral body height loss in traumatic spine fractures: an international study. Eur Spine J. 2017;26(5):1483–1491. doi:10.1007/s00586-016-4716-9
29. Voggenreiter G. Balloon kyphoplasty is effective in deformity correction of osteoporotic vertebral compression fractures. Spine. 2005;30(24):2806–2812. doi:10.1097/01.brs.0000190885.85675.a0
30. Zuo XH, Zhu XP, Bao HG, et al. Network meta-analysis of percutaneous vertebroplasty, percutaneous kyphoplasty, nerve block, and conservative treatment for nonsurgery options of acute/subacute and chronic osteoporotic vertebral compression fractures (OVCFs) in short-term and long-term effects. Medicine. 2018;97(29):e11544. doi:10.1097/MD.0000000000011544
31. Yokoyama K, Kawanishi M, Yamada M, et al. In not only vertebroplasty but also kyphoplasty, the resolution of vertebral deformities depends on vertebral mobility. AJNR Am J Neuroradiol. 2013;34(7):1474–1478. doi:10.3174/ajnr.A3424
32. Chen YJ, Chen HY, Chen HT, Lin RM, Hsu HC. Diagnosis of painful cemented vertebrae from failed vertebroplasty: modified dynamic radiographs play an important role. Eur Spine J. 2017;26(7):1953–1960. doi:10.1007/s00586-017-5056-0
33. Cho JH, Shin SI, Lee JH, Yeom JS, Chang BS, Lee CK. Usefulness of prone cross-table lateral radiographs in vertebral compression fractures. Clin Orthop Surg. 2013;5(3):195–201. doi:10.4055/cios.2013.5.3.195
34. Liu HX, Xu C, Shang P, Shen Y, Xu HZ. The effect of postural correction and subsequent balloon inflation in deformity correction of acute osteoporotic vertebral fractures. J Korean Neurosurg Soc. 2014;55(6):337–342. doi:10.3340/jkns.2014.55.6.337
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.