Back to Journals » Orthopedic Research and Reviews » Volume 14
The Unpredictable Palmaris Longus Tendon Variation in Distal Radio-Ulnar Joint Reconstruction: A Technical Consideration for Undersized Graft
Authors Hidajat NN, Arsa W ![]() , Fadli S, Nong I
, Fadli S, Nong I ![]() , Aprilya D
, Aprilya D ![]()
Received 14 July 2022
Accepted for publication 3 September 2022
Published 12 September 2022 Volume 2022:14 Pages 319—326
DOI https://doi.org/10.2147/ORR.S381694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Nucki Nursjamsi Hidajat,1 Widya Arsa,1 Sanditya Fadli,2 Ira Nong,3 Dina Aprilya4
1Hand, Upper Limb and Microsurgery Division, Department of Orthopaedic and Traumatology, Hasan Sadikin General Hospital, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Orthopaedic and Traumatology, Hasan Sadikin General Hospital, Universitas Padjadjaran, Bandung, Indonesia; 3Department of Orthopaedic and Traumatology, Wahidin Sudirohusodo General Hospital, Hasanuddin University, Makassar, Indonesia; 4Department of Orthopaedic and Traumatology, Siloam Agora Hospital, Jakarta, Indonesia
Correspondence: Widya Arsa, Hand, Upper limb and Microsurgery Division, Department of Orthopaedic and Traumatology, Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, 40161, West Java, Indonesia, Tel +6222-2034953, Fax +6222-2032216, Email [email protected]
Background: Distal radioulnar joint (DRUJ) instability results from the disruption of the triangular fibrocartilaginous complex consisting of DRUJ’s primary and secondary stabilizers. The gold standard of stabilization procedure remains ligament reconstruction that utilizes tendon grafts to reanimate the volar and dorsal radioulnar ligament (RUL) as the primary stabilizers of the joint. The palmaris longus (PL) tendon, the graft of choice in reconstructive surgery, is commonly used in DRUJ reconstruction. However, it can exhibit anatomic variations from agenesis to the variation in morphology, location, and attachment that is rarely encountered other than in cadaveric studies.
Case Presentation: We present a case of a 14-year-old boy with ulnar-sided wrist pain and instability following an injury in a boxing match four months before admission. The clinical and radiological results suggested a DRUJ injury with extensor carpi ulnaris (ECU) tendinitis. A ligament reconstruction using the PL tendon graft was planned. Intraoperatively, the PL was found anomalous with dual distal attachments and a short graft length.
Results: We performed Adams ligament reconstruction technique with some modifications to the original design. To overcome the under-sized graft, instead of passing it around the ulnar neck, we added one more bone tunnel on the ulna to enhance the construct stability by a tendon to bone healing.
Conclusion: In reconstructive surgeries, surgeons should consider the other sources of grafts as graft variations exist. Otherwise, as in our case, modifications to the standard technique can be made.
Keywords: DRUJ instability, palmaris longus, anatomical variation, tendon graft, ligament reconstruction
Introduction
The distal radio-ulnar joint (DRUJ) is commonly injured after a traumatic event to the wrist, either isolated or accompanied by the distal radius fracture and triangular fibrocartilage complex (TFCC) tear. For symptomatic patients, reconstructing the dorsal or volar radio-ulnar ligament (RUL) offers optimum restoration of the DRUJ kinematics.1 The palmaris longus (PL) is the first choice of tendon donor for ligament reconstruction using the technique described by Adams and Berger in 2002.1–3
Although the PL tendon is dispensable and fully fulfills the necessary requirements for tendon graft due to its length, diameter, and availability, the PL is also one of the most variable muscles in the human body. Namely, the absent PL, bi-tendinous, multiple muscle bellies, palmaris profundus, reverse palmaris, and palmaris brevis are all types of variations that are mostly found in cadaveric studies.2,3 The absent PL has been reported with a range between 1.5% and 63.9% that was discovered either clinically, intraoperatively, or in cadaver dissections.4 While, other variations were rarely found and only found during the cadaveric anatomical study. Unfortunately, other than absent PL, it is hard to evaluate the existence of PL variations.5,6 Thus, it is potentially missed pre-operatively.
We present a case of chronic dislocation DRUJ in a young man treated with ligament reconstruction using PL tendon. Intraoperatively, the tendon was anomalous, so we made several modifications to the Adams technique of DRUJ reconstruction. Consent was obtained from the guardian of the patient for the publication of this report. This work has been reported in line with the CARE guidelines.7
Case Presentation
A 14-year-old boy was admitted to the outpatient clinic with ulnar-sided wrist pain following an acute injury after hitting the opponent during a boxing match four months prior to hospital admission. At the time of the injury, the wrist was suddenly locked and felt very painful. The patient went to the general practitioner and had the wrist treated conservatively with a brace. Although the acute pain and swelling had improved, the patient was still troubled with the pain associated with wrist rotation and weight lifting, particularly during his boxing activities. Moreover, there was a sense of instability, including weakness and a joint “clunk”.
On the physical examination, there was a bony prominence over the ulnar styloid and tenderness over the distal ulnar region and ulnar side of the wrist (Figure 1A). The foveal sign and ulnar grinding tests were negative. The piano key sign and the intraoperative ballottement test revealed DRUJ instability with the most stable position in supination. The ECU synergy test was positive with pain elicited through the course of ECU on dorso-ulnar side of the wrist. The PL tendon was evident on physical examination. The plain radiograph suggested DRUJ subluxation (Figure 1B and C) and the MRI revealed an absence of volar radio-ulnar ligament (Figure 2). There was also evidence of ECU sub-sheath injury (Figure 2).
 |
Figure 1 (A) Bony prominence on the ulnar side of the left wrist. (B) Normal gap on the PA view wrist radiograph. (C) A radioulnar distance greater than 6 mm. |
 |
Figure 2 Magnetic Resonance Imaging. (A) Axial T1-weighted image revealed a lack of volar RUL, redundant extensor retinaculum, and flipped ECU sub-sheath that trapped between the ECU and the bony surface. (B) The axial T2 weighted image showed hyperintensity suggesting ECU tendinitis. (C) Coronal T2 images suggested an ulnar avulsion of the TFCC palmer 1B (dotted red circle). (Pink asterisk: dorsal RUL; yellow asterisk: ECU tendon; blue arrow: extensor retinaculum; red arrow: flipped ECU sub-sheath; green arrow: tendinitis). |
The patient was diagnosed with chronic DRUJ injury associated with ECU tendinitis and underwent the reconstructive procedure. Surprisingly, during tendon harvesting, the PL tendon was anomalous. Initially, after the identification of the distal attachment, the tendon was difficult to obtain through small separate incisions. Thus, we extended the incision and found that the PL had two tendinous insertions into the palmar aponeurosis, with the point of bifurcation being 2.5 cm from the distal wrist crease. The lateral division lies superficially, has a 0.4 cm width, and is 0.5 cm shorter than the medial division. The medial division has a 0.6 cm width and lies between the flexor retinaculum and the transverse carpal ligament. The total length obtained from the harvesting was only 13 cm (Figure 3). We prepared the tendon for grafting with both divisions used and the Krakow sutures were applied on both ends.
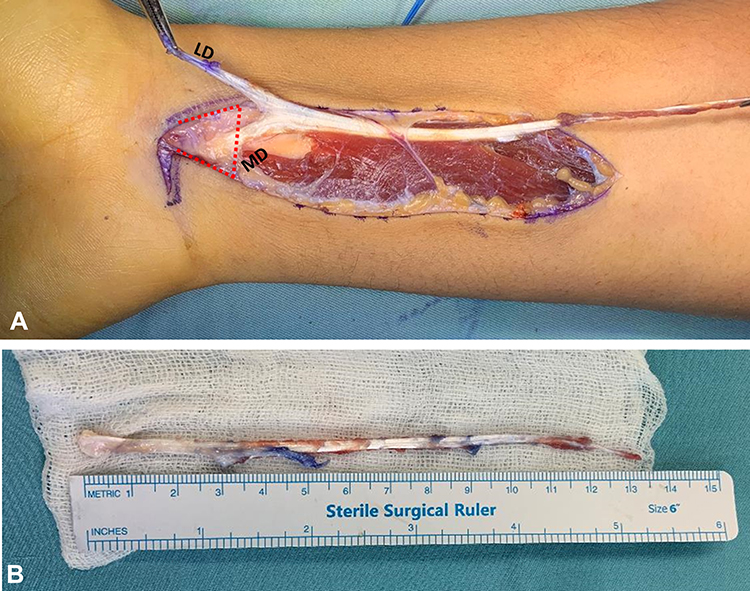 |
Figure 3 (A) PL variation with a bitendinous portion at the distal attachment. The lateral division (LD) lies superficial to the flexor retinaculum (red dots) and the medial division (MD) lies under the flexor retinaculum. (B) The harvested 13-cm-long tendon. |
Surgical Technique
We reconstructed the dorsal and volar RUL using PL tendon using the modification of Adams’ technique of DRUJ reconstruction.3 A dorso-ulnar incision was made over the DRUJ and the extensor retinaculum was opened to expose the 5th compartment. The extensor digiti minimi (EDM) tendon was retracted radially and an inverted L-shaped capsular incision was made to expose the DRUJ, with the smaller limb of the L-shaped being made just proximal to the triangular fibrocartilage complex (TFCC). The TFCC remnant was debrided to expose the fovea and make an interosseous tunnel from the fovea to the ulnar side of the ulnar styloid. The 4th dorsal compartment was elevated subperiosteally to reflect the dorsal margin of the sigmoid notch and lunate fossa of the distal radius. A 3.5 mm drill hole was made in the lunate fossa approximately 5 mm radial to the radial edge of DRUJ and 5 mm to the radio-carpal joint to avoid breaching the sigmoid notch (Figure 4A).
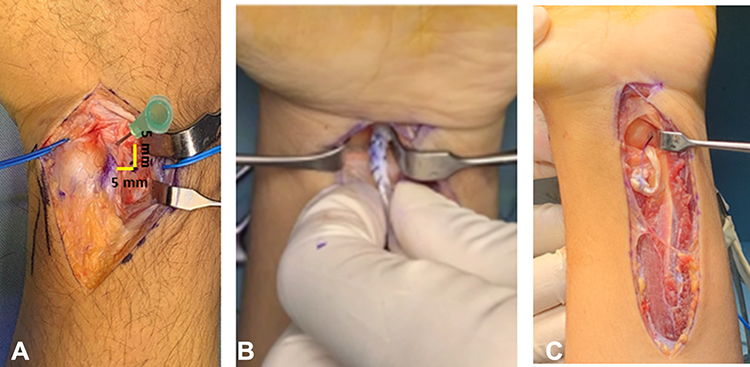 |
Figure 4 (A) Dorsally, the whole fourth extensor compartment was retracted radially and subperiosteally. The radial tunnel is made by drilling the ulnar column of distal radius 5 mm radial to the DRUJ and 5 mm proximal to the radiocarpal joint. (B) At the palmar side, a longitudinal incision proximal to the wrist crease is made to harvest the tendon and pass the graft. (C) The volar limb of the graft is passed dorsally to be secured at the fovea interosseous tunnel. |
Volarly, the radial tunnel was made on the ulnar column of distal radius approximately 0.5 cm radial to the sigmoid notch and 0.5 cm proximal to the radiocarpal joint. The bone was exposed through the PL harvesting incision by retracting the whole carpal tunnel content radially. After the graft preparation, the PL graft was passed through this radial tunnel with a suture retriever from dorsal to volar (Figure 4B). The volar limb of the graft was passed back dorsally through the soft tissue tunnel from volar to dorsal DRUJ capsule (Figure 4C).
Both limbs of the PL graft were then passed to the ulna interosseous tunnel with one end pulled longer than the other. A second ulnar tunnel was made proximally to pass the longer limb. Both limbs were fixed with Pulvertaft’s weave technique after appropriate graft tensioning in the neutral wrist and compressed DRUJ (Figure 5). The summary of the technique is illustrated in Figure 6.
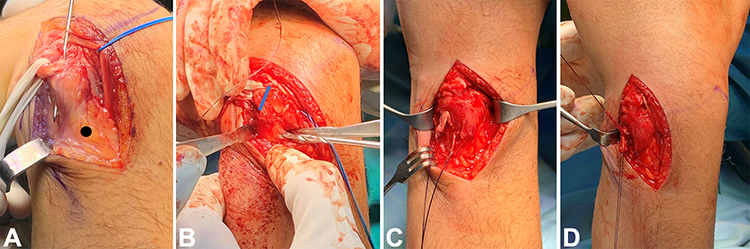 |
Figure 5 (A) A longitudinal skin incision was made over the DRUJ. The EDM in the 5th compartment was retracted, then, an ulnarly-based flap of dorsal retinaculum is raised over the distal ulna, exposing the DRUJ capsule. In a hyperflexed wrist, a 3.5-mm bony tunnel was made from the fovea to the ulnar neck. (Black dot: Second ulnar tunnel) (B). The second ulnar interosseous tunnel (2.5 mm) is made proximally to pass one of the limbs. (Blue line: the first ulnar tunnel). (C and D) Both limbs are tied with the Pulvertaft weave technique. |
 |
Figure 6 An illustration of the intra articular RUL reconstruction technique using a PL graft. Both graft limbs are shown in different colors. (A) Dorsal view. (B) Radio-carpal view. |
A Muenster anti-rotation splint was applied with the forearm in a neutral to slight supination position up to 6 weeks postoperative. Heavy lifting, boxing, and other strenuous exercises for the wrist are discouraged for the first 6 months after surgery. On the 3rd and 6th months follow-up, the wound healed uneventfully and the DRUJ remains stable in prono-supination movement and is pain-free.
Discussion
The DRUJ instabilities are common among athletes due to either acute trauma or repetitive ulnar and compressive loading on the hand and wrist. It may coexist with distal radius fracture, TFCC injury, DRUJ arthritis, or ECU subluxation and tendinitis. Numerous techniques have been described that are generally classified into intra- and extra-articular reconstruction techniques.1,8 To our knowledge, limited human studies have proven the superiority of one over another. Even though studies on cadavers have shown that the extra-articular method is a good choice and less invasive, the intra-articular anatomical reconstruction methods can restore the DRUJ’s stability to where it was before the surgery.1,8–11 In our case, instability is the main problem, and the patient has a demanding boxing activity that requires a stable wrist with a strong grip. Thus, an intra-articular ligament reconstruction using a tendon graft is the treatment of choice.
Preoperatively, we have examined the existence of the palmaris longus tendon as the donor tendon by physical examination. However, as we proceeded to the PL harvesting, the anatomical variance was unavoidable. The PL is a slender fusiform muscle in the forearm region that shares a common origin with the flexor digitorum superficialis (FDS), the flexor carpi radialis (FCR), and the flexor carpi ulnaris (FCU) muscle. It is characterized by a long tendon and short muscle belly which generally meets the requirement for donor tendon graft due to its superficial location and adequate dimension without necessarily causing a functional deformity (dispensable tendon).2,5,6 These values make the PL tendon of great surgical importance and become the first donor of choice for tendon graft procedures in various reconstructive surgeries.12
The PL varies in the incidence of its absence, morphology, number, attachment, and ability to have accessory slips and substitute structures.5 The PL variations are suggested to have clinical importance as they potentially cause or aggravate space-occupying lesion–associated diseases such as carpal tunnel syndrome, Guyon’s canal syndrome, or even compartment syndrome. Uniquely, these variations are hard to interpret by radiological examination and are usually found during routine cadaveric dissection or as an incidental intraoperative finding, as in our case.12
The PL agenesis has been documented well by many literatures in different populations.5 This knowledge brings an important consideration to the donor choice for tendon grafting. Moreover, the muscle belly is also of interest because a number of cases have been reported with nerve compression syndrome, which may be associated with a fusiform swelling over the volar distal forearm.5,13,14 The PL variation highlighted in our report is a short bi-tendinous PL that, to our knowledge, has never been reported other than in cadaveric dissections.2,15
The incidence of PL duplication varies between 0.8 and 3.1%, and the incidence of attachment variation is even rarer (0.5%).9 Some structures have been identified as the PL insertion sites, such as fascia (antebrachial, thenar, and hypothenar fascia), carpal bones (scaphoid, lunate), muscles (thenar or hypothenar muscles), tendons (flexor carpi ulnaris, long flexor tendons), transverse carpal ligament, and the interosseous membrane. The end of the PL tendon may be split in two, and an extra slip may be added to any of the above structures.12 Furthermore, Kumar et al16 also described the PL tendon with multiple attachments in one cadaver. The tendon was divided and attached to the fascia covering the abductor pollicis brevis, flexor retinaculum, and the tendon of flexor carpi ulnaris.
In our case, we incidentally found the anomalous bifid tendon intraoperatively. To our knowledge, this PL variation has never been reported in a clinical setting. The overall length was undersized compared to the normal PL, which is generally above 15 cm in length.5,11 We neither look for the exact inserting point of the tendon nor the muscle belly attachment as it requires a thorough dissection. The tendon in our case was bifurcated with the lateral division lying superficially, 0.5 cm shorter, and relatively thinner than the medial division. The medial division lies beneath the retinaculum but was still lying superficially in the carpal tunnel. However, unlike the most common symptomatic PL anomaly, this patient had never experienced carpal tunnel syndrome, which is commonly caused by the anomalous reversed PL muscle.12 As we had already been in the middle of harvesting this tendon, we decided to use the undersized graft with some modification of the graft fixation.
Although there are many modifications to simplify the technique and move towards a more minimally invasive fashion, the DRUJ reconstruction method that was first described by Adams and Berger3 in 2002 remains the gold standard for stabilizing the DRUJ.3,9 The graft is passed into two interosseous tunnels within the ulnar styloid and lunate facet of the distal radius. If the graft has an adequate length, both limbs are sutured to each other after passing around the neck. Alternatively, the limbs are sutured to each other after they pass through two divergent tunnels through the fovea. In a series of 14 patients tested with a mean follow-up of 2 years, instability resolved in 12 patients.3 In another series observing 22 patients, it was concluded that the Adams technique not only restored pronation and supination but also the DASH and PRWHE scores.17 Gillis et al18 used the Adams procedure on 95 wrists that were fixed with three distinct techniques: sutures alone, anchors, or interference screws. The failure rate was 14% in a mean of 5.5 years of follow-up.
In our case, the graft was too short to be wrapped around the neck. The ulnar styloid was also relatively small, so drilling two divergent holes risked fracture. Thus, we passed one longer limb to another hole through the proximal cortices. Sanders described a technique that utilizes less than a 15 cm graft by securing the graft to adjacent radial soft tissues instead of through the radial bony tunnel.11 We opted to make more bone tunnels to enhance the stability of the construct by a tendon to bone healing. However, a long-term follow-up is needed to evaluate the stability of the construct in restoring wrist function.
Conclusion
The palmaris longus tendon is a dispensable donor graft that is greatly utilized in various reconstructive surgeries. However, the variety of the muscle belly and the tendon is hardly identified in preoperative clinical and radiological examination. It is also rarely reported other than in cadaveric studies. Thus, physicians should be aware of the PL tendon varieties when considering them as donor grafts, and other sources of grafts or allografts should be kept in mind. Otherwise, modifications to the standard technique can be made.
Disclaimer
No patient or author details are included in the figures.
Ethical Approval
Ethical approval to report this case was obtained from the Ethics Committee of Hasan Sadikin General Hospital, Bandung, Indonesia.
Consent for Publication
The guardian provided informed consent for the case details and accompanying images to be published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lawler E, Adams BD. Reconstruction for DRUJ instability. Hand. 2007;2(3):123–126. doi:10.1007/s11552-007-9034-6
2. Sunil V, Rajanna S, Gitanjali KJ, Kadaba J. Variation in the insertion of the palmaris longus tendon. Singapore Med J. 2015;56(1):e7–e9. doi:10.11622/smedj.2015018
3. Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg Am. 2002;27(2):243–251. doi:10.1053/jhsu.2002.31731
4. Ioannis D, Anastasios K, Konstantinos N, Lazaros K, Georgios N. Palmaris longus muscle’s prevalence in different nations and interesting anatomical variations: review of the literature. J Clin Med Res. 2015;7(11):825–830. doi:10.14740/jocmr2243w
5. Lalit M, Piplani S, Mahajan A, Verma P. Morphological analysis of palmaris longus muscle and its anatomic variations: a cadaveric study in North India. Ital J Anat Embryol. 2019;124(3):443–454. doi:10.13128/ijae-11673
6. Park MJ, Namdari S, Yao J. Anatomic variations of the palmaris longus muscle. Am J Orthop. 2010;39(2):89–94.
7. Gagnier JJ, Riley D, Altman D, Koch CA, Sox H, Kienle G. The CARE guidelines: consensus-based clinical case reporting guideline development. Dtsch Arztebl Int. 2013;110(37):603–608. doi:10.3238/arztebl.2013.0603
8. Rodríguez-Merchán EC, Shojaie B, Kachooei AR. Distal radioulnar joint instability: diagnosis and treatment. Arch Bone J Surg. 2022;10(1):3–16. doi:10.22038/ABJS.2021.57194.2833
9. Delbast L, Pic JB, Marty-Diloy T, Dimet J, Lepetit C. Stabilization of the distal radioulnar joint by reconstructing the interosseous membrane’s distal oblique bundle: cadaver study. Orthop Traumatol Surg Res. 2020;106(8):1581–1587. doi:10.1016/j.otsr.2020.03.041
10. Sang L, Liu H, Liu J, Chen B, Xu S. A case report of distal radioulnar joint dislocation fixed by using mini-plate-button. Int J Surg Case Rep. 2017;34:69–73. doi:10.1016/j.ijscr.2017.02.042
11. Hearon BF, Frantz LM, Morris HA. The original anatomic reconstruction of palmar and dorsal radioulnar ligaments for distal radioulnar joint instability. J Hand Surg Am. 2020;45(11):
12. Iqbal S, Iqbal R, Iqbal F. A bitendinous palmaris longus: aberrant insertions and its clinical impact - A case report. J Clin Diagnostic Res. 2015;9(5):AD03–AD05. doi:10.7860/JCDR/2015/12182.5954
13. George SC, Hassan Z. A bifid reversed palmaris longus muscle causing median nerve compression in a child. J Hand Surg Eur Vol. 2018;43(6):665–666. doi:10.1177/1753193417751717
14. Acikel C, Ulkur E, Karagoz H, Celikoz B. Effort-related compression of median and ulnar nerves as a result of reversed three-headed and hypertrophied palmaris longus muscle with extension of Guyon’s canal. Scand J Plast Reconstr Surg Hand Surg. 2007;41(1):45–47. doi:10.1080/02844310500453708
15. Vyas JMV, Sampath Kumar SK. Bitendinous palmaris longus muscle: a case report. J Clin Diagnostic Res. 2018;12(11):11–12. doi:10.7860/JCDR/2018/35535.12289
16. Kumar N, Patil J, Swamy RS, et al. Presence of multiple tendinous insertions of palmaris longus: a unique variation of a retrogressive muscle. Ethiop J Health Sci. 2014;24(2):175–178. doi:10.4314/ejhs.v24i2.11
17. Kootstra T, van Doesburg M, Schuurman A. Doesburg M van, Schuurman A. Functional effects of the Adams procedure: a retrospective intervention study. J Wrist Surg. 2018;4(7):331–335. doi:10.1055/s-0038-1660812
18. Gillis J, Soreide E, Khouri J, Kadar A, Berger R, Moran S. Outcomes of the Adams-Berger ligament reconstruction for the distal radioulnar joint instability in 95 consecutive cases. J Wrist Surg. 2019;8(4):268–275. doi:10.1055/s-0039-1685235
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.