Back to Journals » Clinical Ophthalmology » Volume 12
The UK Paediatric Ocular Trauma Study 2 (POTS2): demographics and mechanisms of injuries
Authors Sii F ![]() , Barry RJ
, Barry RJ ![]() , Abbott J
, Abbott J ![]() , Blanch RJ, MacEwen CJ, Shah P
, Blanch RJ, MacEwen CJ, Shah P
Received 31 October 2017
Accepted for publication 17 November 2017
Published 9 January 2018 Volume 2018:12 Pages 105—111
DOI https://doi.org/10.2147/OPTH.S155611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Freda Sii,1,2 Robert J Barry,1 Joseph Abbott,3 Richard J Blanch,1,4 Caroline J MacEwen,5 Peter Shah1,2,6,7
1Department of Ophthalmology, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham NHS Foundation Trust, Birmingham, 2Birmingham Institute for Glaucoma Research, Institute of Translational Medicine, University Hospitals Birmingham NHS Foundation Trust, Birmingham, 3Department of Ophthalmology, Birmingham Children’s Hospital NHS Foundation Trust, Birmingham, 4Academic Department of Military Surgery and Trauma, Royal Centre for Defence Medicine, Birmingham, 5Department of Ophthalmology, Ninewells Hospital and Medical School, Dundee, 6National Institute of Health Research Biomedical Research Centre, Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, 7Centre for Health and Social Care Improvement, School of Health and Wellbeing, University of Wolverhampton, Wolverhampton, UK
Purpose: Pediatric ocular trauma is an important cause of visual morbidity worldwide, accounting for up to one-third of all ocular trauma admissions. It has long-term implications for those affected and significant economic consequences for healthcare providers. It has been estimated that 90% of all ocular trauma is preventable. Targeted strategies are required to reduce the incidence and the severity of pediatric ocular trauma; this requires an understanding of the epidemiology and characteristics of these injuries and the children involved.
Methods: Prospective, observational study of pediatric ocular trauma cases presenting to UK-based ophthalmologists over a 1-year period; reporting cards were distributed by the British Ophthalmological Surveillance Unit, and clinicians were asked to report incidents of acute orbital and ocular trauma in children aged ≤16 years requiring inpatient or day-case admission. A validated, standardized questionnaire was sent to reporting ophthalmologists to collect data on the demographics and circumstances of injury.
Results: Median age at presentation was 7.7 years, with boys more than twice as likely to be affected than girls (M:F =2.1:1.0). Almost 50% of injuries occurred at home, with 25% occurring in school or nursery. A total of 67% of injuries occurred during play, and 31% involved a sharp implement.
Conclusion: Pediatric ocular trauma remains an important public health problem. At least three-quarters of all injuries are preventable through measures, including education of children and responsible adults, restricting access to sharp implements, improving adult supervision, and appropriate use of eye protection.
Keywords: etiology, childhood eye injury, epidemiology, penetrating eye injury, perforating eye injury, prevention
Background
Pediatric ocular trauma is a significant cause of morbidity. It is estimated that there are up to 280,000 hospital admissions worldwide due to ocular trauma in children <15 years of age each year.1 This is, however, likely to be only a small proportion of all ocular injuries, since it is thought that ocular trauma cases requiring hospital admission account for only 5% of the total.2 Extrapolation of these figures suggests that there are ~6 million episodes of ocular trauma affecting children <15 years of age worldwide each year. Of those admitted to secondary eye care services, up to 24% have suffered a penetrating eye injury.3 As a result, global estimates suggest that there are 3.9 million people living with bilateral vision loss, and over 18 million with unilateral vision loss due to ocular trauma sustained during childhood or as an adult.4
Ocular injury is almost never life-threatening, and affected individuals must therefore live with the consequences of their injury for many years. Visual impairment can have a profound impact on schooling and activities of daily living, with marked socio-economic implications for the patient, their family, and healthcare providers.5
Fortunately, up to 90% of all ocular trauma is thought to be preventable, through a combination of use of protective eyewear and education of supervising adults.6–8 However, before such targeted interventions can be implemented, it is necessary to have a detailed understanding of the demographics and characteristics of these injuries and the children affected. Data collection in this field has been sporadic to date, with a lack of standardized, validated collection tools. As a result, the ability to draw meaningful comparisons between existing studies, and to extrapolate published data to target populations is currently limited. Detailed epidemiological and health–economic analyses have not been possible, but are essential.
To help address this problem, we have previously published a series of standardized data collection tools, designed and validated specifically for use in pediatric ocular trauma.9 The UK Paediatric Ocular Trauma Study (POTS) questionnaires were developed to enable collection of standardized, prospective epidemiological data concerning the demographics, incidence, circumstances, and outcomes of serious ocular injury in children.9 This project collected prospective data through the Royal College of Ophthalmologists British Ophthalmological Surveillance Unit (BOSU) reporting card system. In this paper, we present the first data related to the incidence, demographics and causes of childhood ocular injury, and make policy recommendations for prevention of injury.
Methods
The UK POTS incident questionnaire was developed to collect data on the incidence of serious pediatric ocular trauma, demographic characteristics of injured children, and causes and places of injury.9
Questionnaires were sent to UK-based ophthalmologists over a 12-month period between 1 June 2014 and 30 May 2015. The study was conducted using the BOSU reporting card scheme; at the end of each month, cards were sent to all UK consultant ophthalmologists in the BOSU database. Clinicians were asked to report any new cases of ocular trauma in children aged ≤16 years presenting in the preceding month that required hospital admission for observation, treatment, or surgery. Ophthalmologists were requested to include both patients referred to them, and patients they referred on to other ophthalmologists; this was used to cross-reference to ensure each case was recorded only once.
Reporting cards were returned to BOSU, which informed the principal investigator (FS) of each case. The investigator then contacted the reporting ophthalmologist directly. The reporting clinicians were requested to fill out and return the incident data collection questionnaire to the POTS team. A follow-up request was sent to the reporting ophthalmologists if no response was received within 3 months of the initial request. Specific strategies that were used to increase the response rate during the study period have previously been described in detail.9
Data were entered into a Microsoft Excel spreadsheet for initial coding and calculation of descriptive statistics. Statistical analysis was performed using GraphPad Prism (Version 7.0, GraphPad, La Jolla, CA, USA); comparisons between groups of categorical data were performed according to Fisher’s exact test or Chi-square analysis depending on sample size.
Ethics approval
This study was approved by the Cambridge South Research Ethics Committee, Cambridge, UK. R&D approval was granted by Birmingham Children’s Hospital Research and Development Department, Birmingham, UK.
Results
A total of 126 reporting cards were returned to BOSU during the study period, which were followed up immediately by the investigator with the incident questionnaire.9 Eleven cases did not meet the inclusion criteria and 8 were duplicates, and were excluded from further analysis. Of the remaining 107 eligible cases, questionnaires were not returned for 20 cases and 1 case was excluded due to an incomplete dataset. This left 86 cases suitable for further analysis (86/107 eligible cases; 80.4% response rate).
According to census data from the Office for National Statistics (UK), the mid-2014 pediatric population (aged <16 years) was estimated at 12,908,948 individuals.10 Based on our data, this indicates an estimated incidence rate for reported severe ocular trauma of 0.7 per 100,000 for this population (95% CI: 0.5–0.8).
Demographic data is illustrated in Table 1. The sample comprised 58 (67.4%) boys and 27 (31.4%) girls (gender not specified in 1 case). Median age was 7.7 years (range 0.7–15.8 years). There was an even distribution of laterality of injury (50.0% right eye, 50.0% left eye). The ethnic demographics of cases were as follows: White 76.7%, Asian 10.5%, and Black 5.8%. There was no significant difference in ethnic demographics between this sample and the UK population aged <16 years (according to mid-2014 census data from the Office for National Statistics, UK).
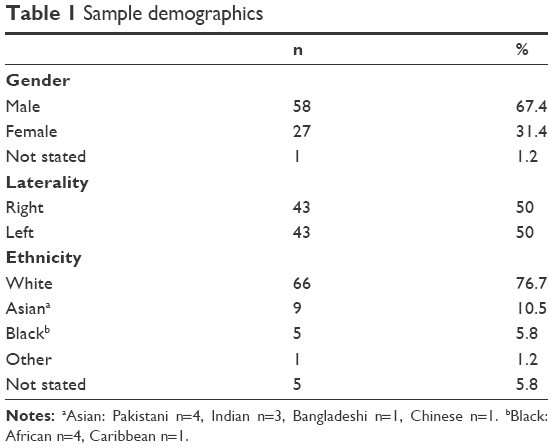 | Table 1 Sample demographics |
Most injuries were reported at play (n=57, 66.2%), with a significant proportion of injuries occurring during education (n=8; 9.3%) or sport-related activities (n=6, 7%). The most common location of injury was in the child’s own home (n=41; 47.7%); however, almost 1 in 4 injuries were sustained at school or in the nursery (n=21; 24.4%) (Table 2). Injuries occurred at a constant rate throughout the year (n=22 January–March, n=22 April–June, n=20 July–September, n=22 October–December). A higher proportion of injuries were sustained outdoors in spring and summer months (19/42; 45.2%) compared with autumn and winter months (11/44; 25.0%); however, this was not statistically significant (p>0.05).
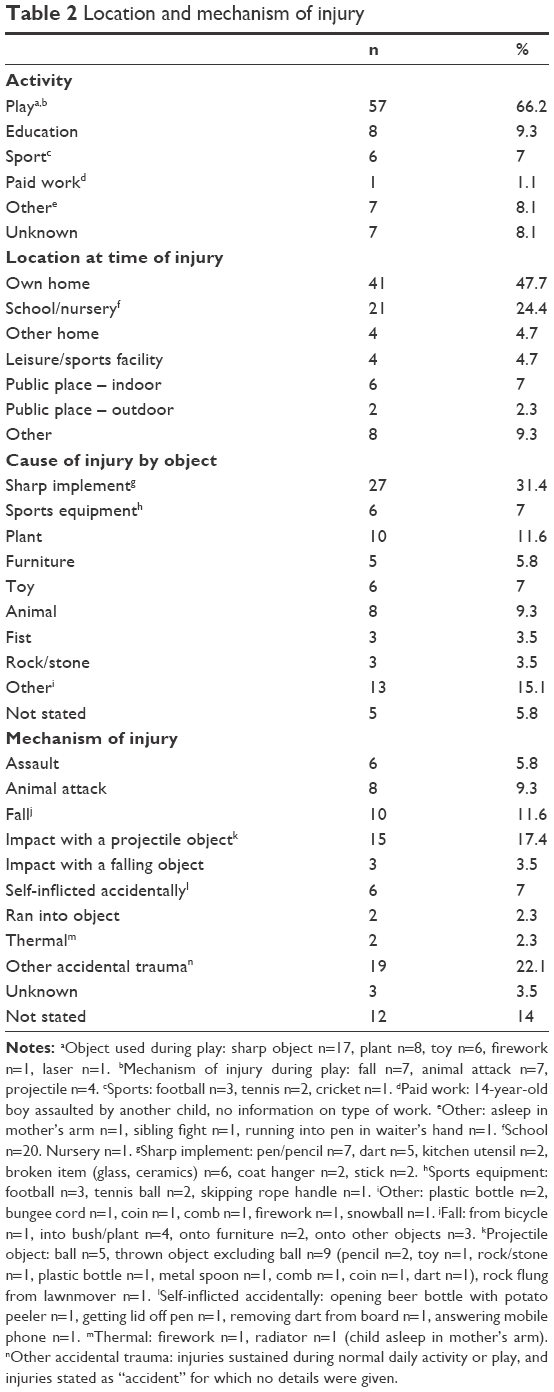 | Table 2 Location and mechanism of injury |
Sharp instruments were the most commonly reported object involved in ocular injury (n=27; 31.4%), followed in order of frequency by plants (n=10; 11.6%), animals (n=8; 9.3%, of which 6 were caused by dogs), and toys or sports equipment in joint fourth position (n=6 each; 7.0%). Impact with a projectile object was the leading causes of injury, occurring in 15 (17.4%) cases, followed by falls in 10 (11.6%) (Table 2). The reporter found no injuries to be associated with alcohol or substance misuse. There were no cases of suspected non-accidental injury reported in this series.
For children aged <4 years, ocular injuries were significantly more likely to occur in their own home compared with older children (76% vs 36.1%, p=0.0009 by Fisher’s exact test). No other statistically significant associations were observed between age or gender, and activity, place, object or mechanism of injury (p>0.05).
Discussion
In this prospective survey of pediatric ocular trauma presenting over a 12-month period in the UK, there were 86 cases requiring hospital admission in children aged ≤16 years. Ocular trauma is a significant cause of morbidity with lifelong implications, yet little data exist on the demographics of the affected population, and the location and mechanisms of such injuries. Through the use of previously developed POTS questionnaires,9 we have initiated the process for standardized reporting of this important public health concern.
Our results show a number of striking trends. Boys are more than twice as likely as girls to sustain significant ocular trauma (M:F =2.1:1.0), the majority of injuries occur during play (66.2), and the most common location for such injuries to occur is within the home (47.7%), particularly for preschool-age children (p<0.05).
These findings are consistent with previously reported data from other parts of the Western world, identifying a preponderance of injuries in boys, most of which occur in the home.11–13 These trends are likely to be explained by the tendency for boys to engage in more active and vigorous play than girls,14 and the fact that most play occurs within the home or garden environment.15 Preschool-age children spend the majority of their time within the home, and the opportunity to sustain injury away from the home is therefore more limited. These factors are also likely to explain the lack of seasonal variation, which is seen in adult ocular trauma16 and has previously been observed in studies of more minor ocular injuries in older children.17
When considering the location of the injury, it was found that 76.8% of ocular trauma was sustained in environments where direct supervision of the affected children would have been expected (own home, other home, school or nursery), whereas only 14.0% of injuries occurred in relatively unsupervised locations (public places or sports facilities). It follows that at least three-quarters of all ocular injuries are potentially preventable through appropriate supervision by a responsible adult.
It is concerning that a significant proportion of injuries were caused by a sharp implement (31.4%). Ophthalmologists have warned of the risks of ocular injury due to darts for nearly 30 years; perforations by darts are often small, with the child, parents and carers often failing to appreciate the severity of the injury.18 Presentation to health care providers is thus often delayed, and affected children are placed at increased risk of developing post-traumatic endophthalmitis.19 It is evident that further publicity is required to highlight this danger, and there is a strong argument to promote the use of protective eyewear for children playing with darts.
Eight of the projectile injuries were caused by inappropriately thrown objects. It would be beneficial to make parents, carers, teachers, and other supervising adults aware of the potential for serious ocular trauma from everyday objects, particularly if thrown.20 Preventing children from throwing objects outside of a safe sports environment would prevent these injuries, and throwing dangerous objects is clearly irresponsible behavior. Thrown objects are a significant concern at football matches, which has led some clubs to adopt a zero-tolerance approach to throwing projectiles. Zero-tolerance policies for offences, including drugs and violence have also been adopted in US schools.21 However, such policies do not allow for mitigation, may divert attention from more serious offences and, when applied to children, can fail to recognize cognitive differences between children and adults in their ability to understand and anticipate long-term consequences of actions.21,22 Nevertheless, educating children about the risks of throwing projectiles, together with a strictly enforced policy of “no-thrown projectiles” in schools could prevent many serious eye injuries.
One relatively simple approach is to advocate the use of suitable eye protection when engaging in potentially high-risk activities as has been advocated by several previous authors.23–26 It is now mandatory for squash players <19 years of age to wear protective eyewear when playing in England squash tournaments. This is a beacon of best practice.
Animal attack-related hospital admissions appear to be increasing in the UK.27 In our series, 8 injuries were caused by domestic animals, all in the home. This is a notable increase when compared with a similar population 18 years previously11 when no animal attacks were reported and is greater than that reported range in other series (0.2%–3%).28 Children are particularly prone to maxillofacial injuries caused by animals;29 attributed to their shorter stature, tendency to behave erratically, and inability to recognize agitation in animals.30
Some injuries are more difficult to prevent; all injuries involving items of furniture were sustained by children aged <5 years. In each case, the child had accidentally tripped or fallen, resulting in periorbital injury. It is difficult to avoid such occurrences in toddlers and preschool-age children, however, parents can be educated regarding strategies to make the home environment safer, such as the use of cushioned guards for furniture edges or corners.
Individual injuries deserving special mention include 1 incident where a stone was flung from a lawnmower, and another of a child playing “tug of war” with a bungee cord. Gardening and do-it-yourself (DIY) activities have previously been highlighted as common causes of ocular injury, although the risks are often overlooked by those engaging in such activities,31 and the dangers associated with misuse of bungee cords are widely known.32,33 Each of these has the potential to cause serious ocular injury, but are easily preventable, have previously been highlighted in the medical press, yet continue to be reported in this pediatric population.
This series also included a 13-year-old boy who suffered an accidental penetrating ocular injury caused by a mobile phone; the responding ophthalmologist stated that the child had “accidentally stabbed himself in the eye while answering the phone”. While the use of mobile phones has previously been implicated in a range of musculoskeletal34,35 and dermatological injuries (through exploding batteries),36,37 to our knowledge, this is the first example of serious ocular trauma due to mobile phone use.
We found a lower incidence of firework and air gun-related ocular injuries than previously reported; Knox et al described 13 episodes of ocular trauma due to fireworks presenting to UK ophthalmologists involving children aged <18 years over a 2-year period,38 and Shuttleworth et al reported 78 cases of ocular injury due to air gun pellets presenting to UK ophthalmologists involving children aged <18 years over a 1-year period.39 In comparison, we observed only 1 firework-related injury and none due to firearms or air guns. Reasons for these differences may reflect differences in the reporting population, response bias, or changes in behavior over recent decades, including changes in the management of blunt trauma, which is less likely to be managed by inpatient care.
Overall, the incidence of severe pediatric ocular trauma reported in this series (0.7 cases per 100,000 population) is considerably lower than previously reported in 1991–1992 (8.85 cases per 100,000 population).40 We are currently undertaking further work to try and ascertain the number of serious injuries that may not have been reported to BOSU during the study period. Preliminary findings indicate that in some ophthalmic units, up to 75% of open globe injuries were not reported via the BOSU system (Blanch R 2017, personal communication, 15 August).
Potential limitations of data collection via BOSU include: 1) incomplete or changing data on UK consultant ophthalmologists, 2) reporting ophthalmologists may not keep track of reported patients and their hospital identification at the initial stage of reporting, resulting in subsequent difficulty tracing the patient, and 3) clinicians are often under severe pressure and may not have the time to engage with BOSU.
Multiple studies have stated that a high proportion of pediatric ocular trauma is preventable.6–8 However, a Cochrane review found no reliable evidence that educational interventions can reduce the incidence of eye injuries.7 In contrast, targeted and tailored interventions with educational components as well as monitoring and enforcement of behavioral change can dramatically reduce eye injuries in an occupational setting.41,42 It is recognized that primary legislation on specific issues in the society, such as wearing seatbelts can greatly reduce eye injuries in the general population.43 Health and safety legislation regulates the provision of eye protection and safe practices in the working environment, and broad legislation regulates schools and nurseries (EN 1176 and 1177). Health and safety legislation states that employees must work safely and in accordance with their training. Responsible adults in school and nursery environments should receive education and training in the prevention of serious ocular trauma in children.
Perhaps more challenging, but more relevant in view of the findings of this study, is the implementation of educational programs for those supervising children in domestic environments. Educational programs could potentially tackle some of the carers’ attitudes associated with injury; interviews after childhood injury found several significant associations, including unrealistic expectations, acceptance of injuries as the norm, lack of anticipation of risk, and ignorance of normal development. However, there is a fine balance to strike between “promoting ocular health” and “interfering” parenting approaches, and as health care professionals, we must acknowledge that children need an appropriate level of independence for intellectual and social development.
Many of the injuries reported in this series are avoidable through sensible restrictions on access to age-inappropriate items and careful supervision. By highlighting trends in the incidence and epidemiology of pediatric ocular trauma, it is hoped that we can continue to reduce the morbidity associated with this important public health concern. Perhaps the time has come to set up a UK Registry of Serious Pediatric Ocular Trauma to enable us to map trends in this area and demonstrate the impact of interventions.
Data availability
Data supporting the results reported in this manuscript are available from the corresponding author on request.
Acknowledgments
The authors wish to thank the Royal College of Ophthalmologists British Ophthalmological Surveillance Unit (BOSU), in particular Mr Barny Foot, for his advice at various stages of this project’s inception. We also acknowledge the BOSU review committee members for their contribution to the design of POTS data collection questionnaires. This study was supported by a bursary from the British Ophthalmological Surveillance Unit (BOSU).
Author contributions
RJB drafted and prepared the manuscript for submission. All other authors developed the data collection protocol and were involved in proofreading and editing of the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Abbott J, Shah P. The epidemiology and etiology of pediatric ocular trauma. Surv Ophthalmol. 2013;58(5):476–485. | ||
May DR, Kuhn FP, Morris RE, et al. The epidemiology of serious eye injuries from the United States Eye Injury Registry. Graefes Arch Clin Exp Ophthalmol. 2000;238(2):153–157. | ||
Strahlman E, Elman M, Daub E, Baker S. Causes of pediatric eye injuries. A population-based study. Arch Ophthalmol. 1990;108(4):603–606. | ||
Négrel AD, Thylefors B. The global impact of eye injuries. Ophthalmic Epidemiol. 1998;5(3):143–169. | ||
Rahi JS, Cumberland PM, Peckham CS. Visual function in working-age adults: early life influences and associations with health and social outcomes. Ophthalmology. 2009;116(10):1866–1871. | ||
Pizzarello LD. Ocular trauma: time for action. Ophthalmic Epidemiol. 1998;5(3):115–116. | ||
Shah A, Blackhall K, Ker K, Patel D. Educational interventions for the prevention of eye injuries. Cochrane Database Syst Rev. 2009;4:CD006527. | ||
Philip SS, Hoskin AK. Children’s protective eyewear: the challenges and the way forward. Med J Aust. 2014;201(2):87–88. | ||
Sii F, Barry RJ, Blanch RJ, Abbott J, MacEwen CJ, Shah P. The UK Paediatric Ocular Trauma Study 1 (POTS1): development of a global standardized protocol for prospective data collection in pediatric ocular trauma. Clin Ophthalmol. 2017;11:449–452. | ||
Office for National Statistics. Population Estimates Analysis Tool [Internet]. [cited August 7, 2017]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesanalysistool. Accessed August 17, 2017. | ||
MacEwen CJ, Baines PS, Desai P. Eye injuries in children: the current picture. Br J Ophthalmol. 1999;83(8):933–936. | ||
Haavisto AK, Sahraravand A, Holopainen JM, Leivo T. Paediatric eye injuries in Finland – Helsinki eye trauma study. Acta Ophthalmol. 2017;95(4):392–399. | ||
Yardley AE, Hoskin AK, Hanman K, Sanfilippo PG, Lam GC, Mackey DA. Paediatric ocular and adnexal injuries requiring hospitalisation in Western Australia. Clin Exp Optom. 2017;100(3):227–233. | ||
Baquet G, Ridgers ND, Blaes A, Aucouturier J, Van Praagh E, Berthoin S. Objectively assessed recess physical activity in girls and boys from high and low socioeconomic backgrounds. BMC Public Health. 2014;14(1):192. | ||
Veitch J, Bagley S, Ball K, Salmon J. Where do children usually play? A qualitative study of parents’ perceptions of influences on children’s active free-play. Health Place. 2006;12(4):383–393. | ||
Okeigbemen VW, Osaguona VB. Seasonal variation in ocular injury in a tertiary health center in Benin City. Sahel Med J. 2013;16(1):10–14. | ||
Mowatt L, McDonald A, Ferron-Boothe D. Paediatric ocular trauma admissions to the University Hospital of the West Indies 2000–2005. West Indian Med J. 2012;61(6):598–604. | ||
Patel BC, Morgan LH. Serious eye injuries caused by darts. Arch Emerg Med. 1991;8(4):289–291. | ||
Li X, Zarbin MA, Bhagat N. Pediatric open globe injury: a review of the literature. J Emerg Trauma Shock. 2015;8(4):216–223. | ||
Kelly SP, Reeves GM. Penetrating eye injuries from writing instruments. Clin Ophthalmol. 2011;6(1):41–44. | ||
Freeman M. Bringing up baby (Criminals): the failure of zero tolerance and the need for a multidisciplinary approach to state actions involving children. Quinnipiac Law Rev. 2002;21(3):533–562. | ||
Elrod L. Restructuring schools as families: report of a conference. Fam Law Q. 1994;28(3):347–361. | ||
MacEwen CJ. Sport associated eye injury: a casualty department survey. Br J Ophthalmol. 1987;71(9):701–705. | ||
Capão Filipe JA, Rocha-Sousa A, Falcão-Reis F, Castro-Correia J. Modern sports eye injuries. Br J Ophthalmol. 2003;87(11):1336–1339. | ||
Eime R, Owen N, Finch C. Protective eyewear promotion. Sport Med. 2004;34(10):629–638. | ||
Hoskin AK, Yardley AM, Hanman K, Lam G, Mackey DA. Sports-related eye and adnexal injuries in the Western Australian paediatric population. Acta Ophthalmol. 2016;94(6):e407–e410. | ||
Hospital Episodes Statistics, Health and Social Care Information Centre. Provisional monthly topic of interest: admissions caused by dogs and other mammals [Internet]. NHS Digital. 2015 [cited August 11, 2017]. Available from: http://content.digital.nhs.uk/catalogue/PUB17615/prov-mont-hes-admi-outp-ae-April 2014 to February 2015-toi-rep.pdf. Accessed August 17, 2017. | ||
Yardley AM, Hoskin AK, Hanman K, Wan SL, Mackey DA. Animal-inflicted ocular and adnexal injuries in children: a systematic review. Surv Ophthalmol. 2015;60(6):536–546. | ||
Agrawal A, Kumar P, Singhal R, Singh V, Bhagol A. Animal bite injuries in children: review of literature and case series. Int J Clin Pediatr Dent. 2017;10(1):67–72. | ||
Schwebel DC, Li P, McClure LA, Severson J. Evaluating a website to teach children safety with dogs: a randomized controlled trial. Int J Environ Res Public Health. 2016;13(12):E1198. | ||
Bhogal G, Tomlins PJ, Murray PI. Penetrating ocular injuries in the home. J Public Health (Oxf). 2007;29(1):72–74. | ||
Da Pozzo S, Pensiero S, Perissutti P. Ocular injuries by elastic cords in children. Pediatrics. 2000;106(5):E65. | ||
Aldave AJ, Gertner GS, Davis GH, Regillo CD, Jeffers JB. Bungee cord-associated ocular trauma. Ophthalmology. 2001;108(4):788–792. | ||
Yang CY, Wang JC. An unusual case of rapidly progressed cervical compression myelopathy caused by overnight inappropriate usage of Smartphone device. J Clin Neurosci. 2017;39:82–84. | ||
Gilman L, Cage DN, Horn A, Bishop F, Klam WP, Doan AP. Tendon rupture associated with excessive smartphone gaming. JAMA Intern Med. 2015;175(6):1048–1049. | ||
Görgülü T, Torun M, Olgun A. A cause of severe thigh injury: battery explosion. Ann Med Surg (Lond). 2016;5:49–51. | ||
Mankowski PJ, Kanevsky J, Bakirtzian P, Cugno S. Cellular phone collateral damage: a review of burns associated with lithium battery powered mobile devices. Burns. 2016;42(4):e61–e64. | ||
Knox FA, Chan WC, Jackson AJ, Foot B, Sharkey JA, McGinnity FG. A British Ophthalmological Surveillance Unit study on serious ocular injuries from fireworks in the UK. Eye (Lond). 2008;22(7):944–947. | ||
Shuttleworth GN, Galloway P, Sparrow JM, Lane C. Ocular air gun injuries: a one-year surveillance study in the UK and Eire (BOSU). 2001–2002. Eye (Lond). 2009;23(6):1370–1376. | ||
Desai P, MacEwen CJ, Baines P, Minassian DC. Incidence of cases of ocular trauma admitted to hospital and incidence of blinding outcome. Br J Ophthalmol. 1996;80(7):592–596. | ||
Mancini G, Baldasseroni A, Laffi G, Curti S, Mattioli S, Violante FS. Prevention of work related eye injuries: long term assessment of the effectiveness of a multicomponent intervention among metal workers. Occup Environ Med. 2005;62(12):830–835. | ||
Gondusky JS, Reiter MP. Protecting military convoys in Iraq: an examination of battle injuries sustained by a mechanized battalion during Operation Iraqi Freedom II. Mil Med. 2005;170(6):546–549. | ||
Hall NF, Denning AM, Elkington AR, Cooper PJ. The eye and the seatbelt in Wessex. Br J Ophthalmol. 1985;69(5):317–319. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.