")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Trends of Suicidality Over the Past 10 Years (1999–2022) in the Ethiopian General Population and the Way Forward in Tackling It
Authors Kassaw C , Alemayehu S
Received 20 May 2023
Accepted for publication 7 August 2023
Published 14 August 2023 Volume 2023:16 Pages 3231—3236
DOI https://doi.org/10.2147/PRBM.S419426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Chalachew Kassaw,1 Selamawit Alemayehu2
1Department of Psychiatry, Dilla University, Dilla, Ethiopia; 2Departments of Psychiatry, St. Paul Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Selamawit Alemayehu, Departments of Psychiatry, St. Paul Hospital Millennium Medical College, P.O.Box, Addis Ababa, 46453, Ethiopia, Email [email protected]; [email protected]
Abstract: Suicide is defined as a death caused by willful acts of taking one’s own life. It might be a way for people to get away from suffering or anguish. Globally, an estimated a million people individuals lose their life due to suicide annually. Before the age of 50 years old more than half (58%) of all suicide deaths occur. This commentary aims to highlight the Ethiopian context, feasible preventive measures, and the way forward in tackling suicidal behavior. Worldwide in adolescent age groups between the ages of 15 and 29, suicide is the fourth leading cause of death. Even though suicide occurs everywhere in the world, according to data in 2019, 77% of all suicides that occurred in the world reside in developing countries. Due to the numerous psychosocial pressures present in Ethiopia, one in four citizens suffers from a mental disorder. According to Ethiopian national data figures, suicide ideation affects 9%, 5– 16% of people, whereas suicidal attempt affects 4%, 1– 8%. Even though, there is a variation of prevalence over the years based on the variation in design, settings, and sample size. There is an increment in the prevalence’s suicidal ideation and attempts in the past 10 years. The country’s Ministry of Health needs to act to address and prevent this urgent public health situation. The prevention of suicide should be a top concern, and working with numerous stakeholders is an efficient and practical approach.
Keywords: suicide, Ethiopia, prevention, public health emergency
Introduction
Suicide is described as a death brought by self-inflicted harm and is intended to bring about one’s own death. Suicidal ideation is when someone considers, mulls over, or plans to taking their own life.1 Suicide attempt is a potentially harmful, self-directed behavior that is done to end one’s life. Every year, around a million people lose their life because of suicide out of these 86% of those deaths occur in developing countries.2 Suicide is higher in the young age below 25 and it is the top three causes of death in these age groups. Women in 1-year post-delivery time suicide accounts for 10–20% of deaths.3 Other factors COVID-19 pandemic showed a rapid increment in suicidal behaviors. A study done on suicidal ideation and suicidal thinking in the era of COVID-19 among university students showed the pooled average prevalence of suicidal ideation and thoughts was 17.8%. The review illustrated an increment in suicidal behaviors during the COVID-19 pandemic.4
Suicide occurs when the psychache is unbearable to the individual. The occurrence of suicide can be influenced by individual thresholds for enduring psychological pain.5 Psychache and physical pain tolerance have been identified as risk factors for suicide.5 Individuals with repeated exposure to psychological pain or fear-inducing and physically painful life events will develop fearlessness and pain insensitivity referred to as acquired capability to enhance lethal and nonlethal suicidal behaviors.6 Previous evidence suggests the risk of suicide become high psychache becomes unbearable, tolerance decline.7
According to the world health organization’s mental health gap action program (MH-GAP), suicide is one the important health-related issue that fosters urgent action. The guideline recommends strategies for data recording, early screening of mental illness and giving emphasis to special populations (children, elderly, and women), and limiting access to suicide methods.8 It is a significant public health issue that can have a long-lasting impact on families, and communities. Most persons who suffer from mental illness do not take their own lives. Yet, more than 90% of people who took their own life have battled a mental illness in the past.9 Suicidal behavior does not necessarily result from mental disease alone. Suicidal thoughts and actions may arise from the distress brought on by a mental condition combined with extreme living circumstances. This commentary aims to highlight the Ethiopian context, feasible preventive measures, and a way forward in tackling suicidal behavior.
Ethiopian Context on Trends of Suicidal Behavior
In Ethiopia, the prevalence of common mental disorders is 7.93%, while the percentage of years spent with a mental illness-related disability is 10.99%.10 Mental diseases are not regarded as life-threatening conditions in low-income countries like Ethiopia. In Ethiopia, despite several contradictory different studies on the total lifetime suicidal thoughts (1% to 55%), attempted suicide (0.6% to 14%), and suicide as a cause of death (7.2 to 8.4 per 100,000). Limited attention is given to suicide when compared to other nationwide causes of death like highly contagious mortalities.11 Furthermore, the lack of readily available healthcare facilities, a skilled workforce, and guilt, transgressive, and social criticism of those who engage in suicidal behavior can delay mental health care. The Ethiopian’s pathway to mental health care is late and most use traditional methods to treat mental illness.12 In addition to this, there were 150 psychiatrists in the country serving about 115 million.13 There is still a lot of need to be done by policymakers and treatment providers to improve these limitations. An epidemiological study of suicidal behavior is necessary to create culturally specific suicide therapies. According to national data figures, suicide ideation affects 9%, 5–16% of people, whereas suicidal attempt affects 4%, 1%-8%.14 Even though, there is a variation of prevalence over the years based on the variation in design, settings, and sample size. There is an increment in the prevalence’s suicidal behaviors in the past 10 years, as shown in Figure 1 and Table 1. To support efforts to promote the population’s mental health and fulfill the needs of Ethiopians with mental, neurological, substance use (MNS), and psychosocial disorders, the Ministry of Health (MoH) has developed the National Mental Health Plan 2020–2025, its second strategic plan.15 For every 100 million Ethiopians, there were 150 trained psychiatrists, 2461 psychiatric nurses, 274 psychologists, and three social workers, according to a 2019–2022 research by the National Mental Health Plan (of Ethiopia).13
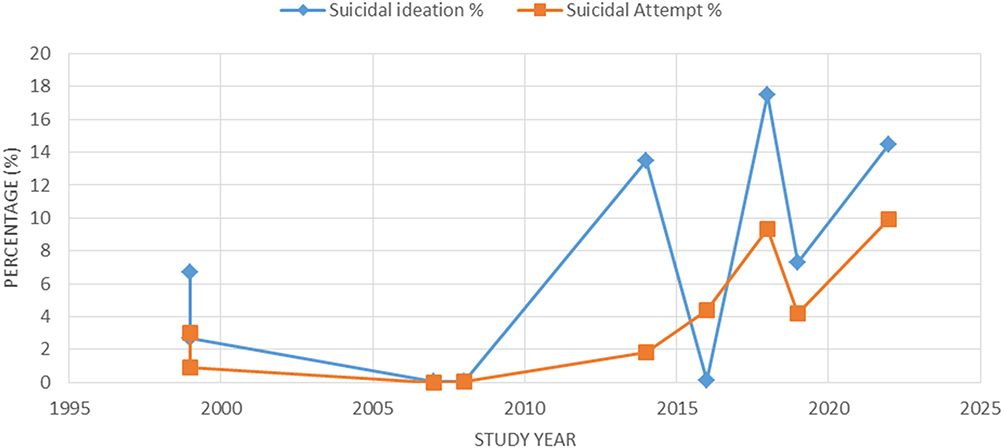 |
Figure 1 A 10-year trend (1999–2022) of suicidal behavior in Ethiopia. |
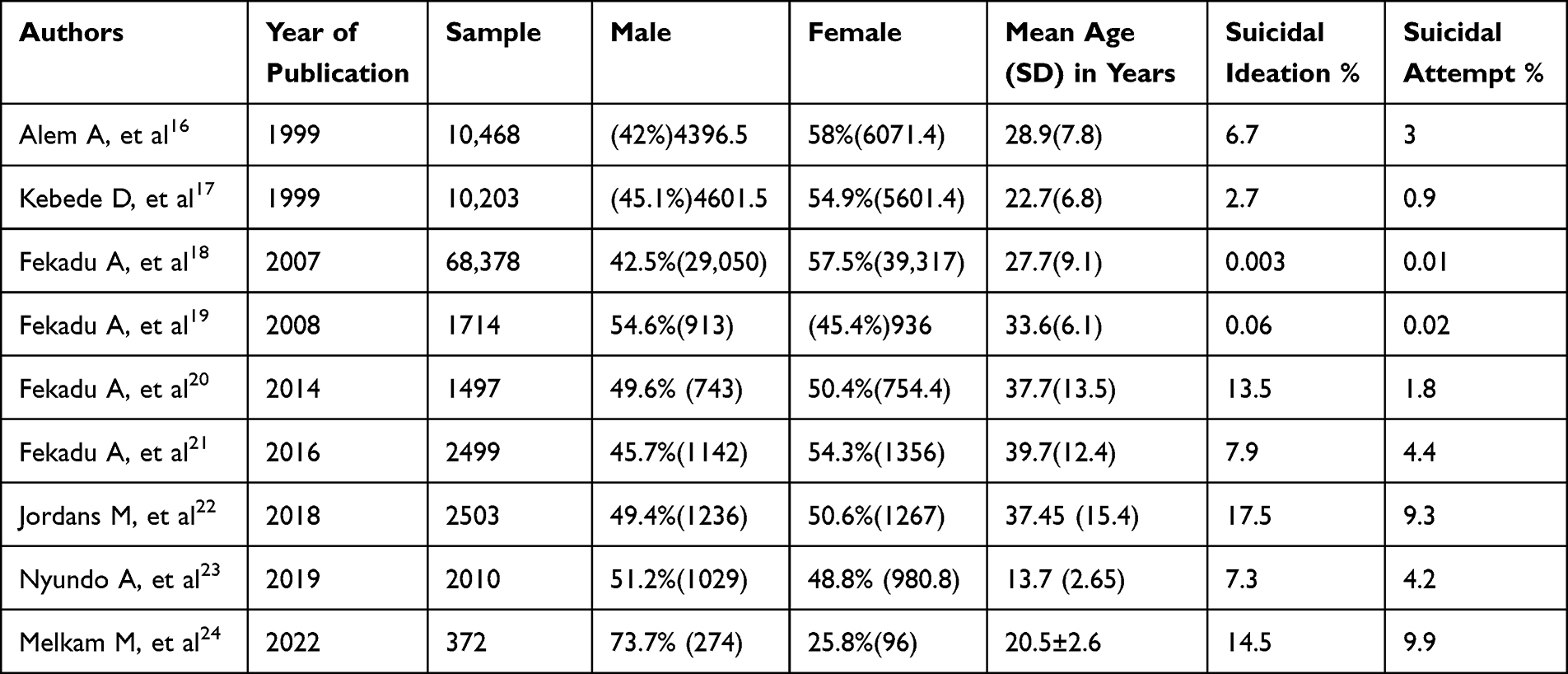 |
Table 1 Summary of Studies Illustrating 10 Year Trends (1999–2022) of Suicidal Behavior in Ethiopia |
It’s a positive idea that suicide can be prevented. Every level of society needs to have strategies in place to prevent suicide.25 This covers protection and proactive measures for people, families, and communities. By being aware of the warning signs, encouraging prevention and resilience, and being committed to societal change, everyone may help prevent suicide. Three levels of interventions are suggested in the general suicide prevention action plan: universal suicide prevention strategies, intended to reach every member of the population; selected suicide prevention strategies, which focus on vulnerable members of the population; and indicated suicide prevention strategies, which are intended to help people who have engaged in non-fatal suicidal behavior or who are left behind.26 The following universal strategies are employed: encouraging ethical media coverage of suicide; religious and cultural practices; school-based parenting education and awareness programs, guidance counselors, etc.; mental health services provided through training of the health workforce, the infrastructure of hospitals and psychiatric wards, etc.; and pesticide means restriction.27 Selective techniques include programs for disadvantaged women and children, drop-in centers, outreach centers, rehabilitation services, community resilience, and support initiatives, and counseling services like those provided by peer, health, and social counselors. The respective strategies are recommended: access to care and services for people who are more likely to taking their own life, such as crisis hotlines, health information services, etc.; survivor rehabilitation services, which include lowering the risk of further suicidal behavior and preventing suicide contagion by identifying other family members who are at high risk.28 Health professionals need to perform a comprehensive assessment of suicide risk and involve the family in the therapeutic process. In compressive suicide risk assessment using formal risk assessment instruments. Suicide prevention is one of the cost-efficient interventions. Early detailed evaluation of potentially suicidal patients by a physician should be acquainted with the assessment of ten major risk factors (sex, age, depression, previous attempt, ethanol abuse, rational thinking loss. And Social supports lacking) as described in SAD PERSONS scale. This scale has a positive influence on performance in evaluating suicidal patients and early prevention.5 SAD PERSONS scale is scored from 10; scores of 3–4 should be closely monitored, scores of 5 and 6 hospitalizations should be strongly considered and patients with scores of 7–10 should be hospitalized for further assessment.6 In addition, involving multidisciplinary teams in mental health care can be beneficial.29
The Way Forward in Tackling Suicidal Behavior
Although suicide has a complex nature, it is unrealistic to expect doctors alone to prevent suicide. But doctors can perform a critical role in preventing suicide or reducing the impact of suicide on families. Multi-faceted approaches to address all the potential risk factors are required.30 Policy interventions, such as controlling the means of suicide and other risk factors, should be top of the list of any preventive approach. Every clinician must be aware of assessing suicide risk. It is important to understand that deliberately seeking to harm oneself is not healthy behavior, even though it is normal for doctors to feel upset by patients who appear to be wasting their time away from “real” responsibilities.31 Any expression of hopelessness or suicide thoughts should be taken seriously, and intervention should be planned. These could be family members, priests, or traditional healers in Ethiopia and other impoverished nations. The person who is expressing hopelessness may be convinced that they are deserving of respect as people and that life is worthwhile if they are given a compassionate approach, good rapport, and attentive listening.32 Most patients are relieved when their loved ones learn of their suicidal thoughts. Approximately 90% of people who take their own life have a co-morbid mental illness. All medical professionals should be capable of treating a suicidal attempt victim in an emergency.33 When a loved one commits suicide, the survivors experience a range of emotions, including sadness, remorse, humiliation, anger, perplexity, and terror. They might start a torturous quest for a purpose. The grieving process could be difficult. It’s critical to comprehend these feelings, to be kind, and to offer assistance.34 All medical practitioners should pay close attention to trends that go beyond information at the individual level and carefully observe, note, and gather data on them. All physicians are clinical scientists with the potential to have a big impact on the policy if they take their duties as practitioners of applied research seriously.35 There is limited data available about suicide in Ethiopia, including typical causes, accessibility to resources, options for therapy, regions with a greater mortality rate, and the work that has to be carried out on a nationwide scale.36 “Creating hope through action” is set to be World Suicide Prevention Day’s three-year focus from 2021 to 2023. By encouraging that there are plenty of solutions to suicide, this concept aims to foster hope and optimism in every one of us.37 This can be shown via our acts of kindness that there is hope for individuals that are considering suicide as well as that we care about them and desire to be the source of assistance to them. It also suggests that our efforts, no matter how large or small, might provide individuals who have difficulty with hope.38 Last, but not least, it highlights how important it is for governments to make prevention of suicide an immediate concern for the health of the public, particularly in circumstances where access to mental health services and access to scientifically proven solutions has become inadequate.39 By developing the subject and spreading the message throughout a three-year period, it is feasible to envision a world where suicides are less likely. We can all aid those who are in a suicidal crisis or who have lost a loved one to suicide as members of society, whether we be children, parents, friends, employees, or someone with lived experience.40
Conclusion
Suicide is a global health concern that can be prevented. A key role in the preventative process can be played by healthcare professionals. Every clinician should be capable of performing basic skills in assessing suicide risk, managing suicide attempts, and providing support for policy contributions. In doing so, healthcare professionals should understand self-compassion and self-care. We can all raise awareness of the issue, provide assistance to those in need, and share our personal stories. There is a need for all to share hope and light with our deeds.
Acknowledgments
We thank all people who provide support throughout the writing of this commentary.
Author Contributions
All authors made a significant contribution to the work reported. Both authors were involved in the conception, study design, execution, acquisition of data, analysis, and interpretation, took part in drafting, and critically reviewing the article; gave final approval of the version to be published, have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was attained for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Snowdon J, Choi NG. Undercounting of suicides: where suicide data lie hidden. Glob Public Health. 2020;15(12):1894–1901. doi:10.1080/17441692.2020.1801789
2. Stone DM, Jones CM, Mack KA. Changes in suicide rates—United States, 2018–2019. Morb Mortal Wkly Rep. 2021;70(8):261. doi:10.15585/mmwr.mm7008a1
3. Kposowa AJ, Aly Ezzat D, Breault K. New findings on gender: the effects of employment status on suicide. Int J Womens Health. 2019;2019:569–575.
4. Jones LB, Vereschagin M, Wang AY, et al. Suicidal ideation amongst university students during the COVID-19 pandemic: time trends and risk factors. Can J Psychiatry. 2022;2022:7067437221140375.
5. Rizvi SJ, Iskric A, Calati R, Courtet P. Psychological and physical pain as predictors of suicide risk: evidence from clinical and neuroimaging findings. Curr Opin Psychiatry. 2017;30(2):159–167. doi:10.1097/YCO.0000000000000314
6. Smith PN, Cukrowicz KC, Poindexter EK, Hobson V, Cohen LM. The acquired capability for suicide: a comparison of suicide attempters, suicide ideators, and non-suicidal controls. Depress Anxiety. 2010;27(9):871–877. doi:10.1002/da.20701
7. Namlı Z, Emin Demirkol M, Tamam L, Onur Karaytuğ M, Yeşiloğlu C. Validity and reliability study of the Turkish version of the unbearable psychache scale. Alpha Psychiatry. 2022;23(4):166–172. doi:10.5152/alphapsychiatry.2022.21604
8. Keynejad R, Spagnolo J, Thornicroft G. WHO mental health gap action programme (mhGAP) intervention guide: updated systematic review on evidence and impact. BMJ Ment Health. 2021;24(3):124–130.
9. Elov ZS, Berdiyeva DS. Psychological reasons for suicide motivation in adolescents with deviant behavior. Oriens Renaissance. 2022;2(2):1003–1009.
10. Bifftu BB, Tiruneh BT, Dachew BA, Guracho YD. Prevalence of suicidal ideation and attempted suicide in the general population of Ethiopia: a systematic review and meta-analysis. Int J Ment Health Syst. 2021;15(1):1–12. doi:10.1186/s13033-021-00449-z
11. Tegegne KT, Tegegne ET, Tessema MK, et al. The association between depression and suicidal ideation: a systematic review and meta-analysis. J Psychol Mental Health Care. 2022;6(1):1–6. doi:10.31579/2637-8892/145
12. Alem A. Psychiatry in Ethiopia. Int Psychiatry. 2004;1(4):8–10. doi:10.1192/S1749367600006718
13. Zeleke WA, Nichols LM, Wondie Y. Mental health in Ethiopia: an exploratory study of counseling alignment with culture. Int J Adv Couns. 2019;41(2):214–229. doi:10.1007/s10447-018-9368-5
14. Liu RT, Bettis AH, Burke TA. Characterizing the phenomenology of passive suicidal ideation: a systematic review and meta-analysis of its prevalence, psychiatric comorbidity, correlates, and comparisons with active suicidal ideation. Psychol Med. 2020;50(3):367–383. doi:10.1017/S003329171900391X
15. Ayele BA, Ali S, Anbessie M, et al. The need for a tailored national dementia plan in Ethiopia: a call for action. Front Neurol. 2023;14:283.
16. Alem A, Kebede D, Woldesemiat G, Jacobsson L, Kullgren G. The prevalence and socio‐demographic correlates of mental distress in Butajira, Ethiopia. Acta Psychiatr Scand. 1999;100:48–55. doi:10.1111/j.1600-0447.1999.tb10694.x
17. Kebede D, Alem A, Rashid E. The prevalence and socio‐demographic correlates of mental distress in Addis Ababa, Ethiopia. Acta Psychiatr Scand. 1999;100:5–10. doi:10.1111/j.1600-0447.1999.tb10687.x
18. Fekadu A, Alem A, Medhin G, et al. Utility of the concept of minor depressive disorder: evidence from a large rural community sample in a developing country setting. J Affect Disord. 2007;104(1–3):111–118. doi:10.1016/j.jad.2007.03.008
19. Fekadu A, O’Donovan MC, Alem A, et al. Validity of the concept of minor depression in a developing country setting. J Nerv Ment Dis. 2008;196(1):22–28. doi:10.1097/NMD.0b013e31815fa4d4
20. Fekadu A, Medhin G, Selamu M, et al. Population level mental distress in rural Ethiopia. BMC Psychiatry. 2014;14(1):1–13. doi:10.1186/1471-244X-14-194
21. Fekadu A, Medhin G, Selamu M, et al. Non-fatal suicidal behaviour in rural Ethiopia: a cross-sectional facility-and population-based study. BMC Psychiatry. 2016;16:1–9. doi:10.1186/s12888-016-0784-y
22. Jordans M, Rathod S, Fekadu A, et al. Suicidal ideation and behaviour among community and health care seeking populations in five low-and middle-income countries: a cross-sectional study. Epidemiol Psychiatr Sci. 2018;27(4):393–402. doi:10.1017/S2045796017000038
23. Nyundo A, Manu A, Regan M, et al. Factors associated with depressive symptoms and suicidal ideation and behaviours amongst sub‐Saharan African adolescents aged 10‐19 years: cross‐sectional study. Trop Med Int Health. 2020;25(1):54–69. doi:10.1111/tmi.13336
24. Melkam M, Demilew D, Kassew T, et al. Suicide ideation and/or attempt with substance use and associated factors among the youth in northwest Ethiopia, community-based. BMC Psychiatry. 2022;22(1):1–11. doi:10.1186/s12888-022-04157-x
25. Turner K, Sveticic J, Almeida-Crasto A, et al. Implementing a systems approach to suicide prevention in a mental health service using the zero suicide framework. Aust N Z J Psychiatry. 2021;55(3):241–253. doi:10.1177/0004867420971698
26. Mann JJ, Michel CA, Auerbach RP. Improving suicide prevention through evidence-based strategies: a systematic review. Am J Psychiatry. 2021;178(7):611–624. doi:10.1176/appi.ajp.2020.20060864
27. Hofstra E, Van Nieuwenhuizen C, Bakker M, et al. Effectiveness of suicide prevention interventions: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2020;63:127–140. doi:10.1016/j.genhosppsych.2019.04.011
28. Wolitzky-Taylor K, LeBeau RT, Perez M, Gong-Guy E, Fong T. Suicide prevention on college campuses: what works and what are the existing gaps? A systematic review and meta-analysis. J Am Coll Health. 2020;68(4):419–429. doi:10.1080/07448481.2019.1577861
29. Rothes I, Henriques M. Health professionals facing suicidal patients: what are their clinical practices? Int J Environ Res Public Health. 2018;15(6):1210. doi:10.3390/ijerph15061210
30. Pronk R, Willems DL, de Vathorst S V. Do doctors differentiate between suicide and physician-assisted death? A qualitative study into the views of psychiatrists and general practitioners. Cult Med Psychiatry. 2021;45:268–281. doi:10.1007/s11013-020-09686-2
31. Osafo J, Asante KO, Akotia CS. Suicide prevention in the African region. Crisis. 2020;41(Supplement 1):S53–S71. doi:10.1027/0227-5910/a000668
32. Green B, Colucci E. Traditional healers’ and biomedical practitioners’ perceptions of collaborative mental healthcare in low-and middle-income countries: a systematic review. Transcult Psychiatry. 2020;57(1):94–107. doi:10.1177/1363461519894396
33. Frick MG, Butler SA, deBoer DS. Universal suicide screening in college primary care. J Am Coll Health. 2021;69(1):17–22. doi:10.1080/07448481.2019.1645677
34. Spillane A, Matvienko-Sikar K, Larkin C, Corcoran P, Arensman E. How suicide-bereaved family members experience the inquest process: a qualitative study using thematic analysis. Int J Qual Stud Health Well-Being. 2019;14(1):1563430. doi:10.1080/17482631.2018.1563430
35. Zygo M, Pawłowska B, Potembska E, Dreher P, Kapka-Skrzypczak L. Prevalence and selected risk factors of suicidal ideation, suicidal tendencies and suicide attempts in young people aged 13–19 years. Ann Agric Environ Med. 2019;26(2):329–336. doi:10.26444/aaem/93817
36. Leah S, Eyal G, Nirit Y, Ariel B-Y, Yossi L-B. Suicide among Ethiopian origin soldiers in the IDF-A qualitative view of risk factors, triggers, and life circumstances. J Affect Disord. 2020;269:125–133. doi:10.1016/j.jad.2020.03.034
37. Arensman E, Scott V, De Leo D, Pirkis J. Suicide and suicide prevention from a global perspective. Crisis. 2020;41(Supplement 1):S3–S7. doi:10.1027/0227-5910/a000664
38. Gordon JA, Avenevoli S, Pearson JL. Suicide prevention research priorities in health care. JAMA psychiatry. 2020;77(9):885–886. doi:10.1001/jamapsychiatry.2020.1042
39. Comtois KA, Kerbrat AH, DeCou CR, et al. Effect of augmenting standard care for military personnel with brief caring text messages for suicide prevention: a randomized clinical trial. JAMA psychiatry. 2019;76(5):474–483. doi:10.1001/jamapsychiatry.2018.4530
40. Platt S, Arensman E, Rezaeian M. National Suicide Prevention Strategies–Progress and Challenges. Hogrefe Publishing; 2019.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.