Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
The TBS-PALB-NLR Triad: A Novel Preoperative Prognostic System Guiding Therapeutic Decision-Making in Unresectable HCC Treated with Transarterial Chemoembolization
Authors Yu B ![]() , Xu L, Yang W, Yin Y, Yang J, Miao X
, Xu L, Yang W, Yin Y, Yang J, Miao X ![]() , Ni C
, Ni C
Received 15 September 2025
Accepted for publication 11 December 2025
Published 20 December 2025 Volume 2025:12 Pages 2859—2873
DOI https://doi.org/10.2147/JHC.S564976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Bin Yu, Lin Xu, Weihao Yang, Yu Yin, Jun Yang, Xiaoyun Miao, Caifang Ni
Department of Interventional Radiology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China
Correspondence: Caifang Ni, Department of Interventional Radiology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the predictive value of the Tumor Burden Score (TBS) combined with Serum Prealbumin (PALB) and the Neutrophil-to-Lymphocyte Ratio (NLR) for the long-term prognosis of patients with unresectable hepatocellular carcinoma (uHCC) following transcatheter hepatic artery chemoembolization (TACE) therapy, and to elucidate its significance in guiding treatment planning.
Patients and Methods: Clinical data from 940 patients with unresectable HCC who underwent TACE treatment at three hospitals in the Jiangsu Province between 2007 and 2018 were retrospectively analyzed. TBS was calculated using the formula: TBS2 = (maximum tumor diameter)2 + (number of tumors)2 (The diameter of the tumor is measured in centimeters). The optimal cutoff values for TBS and NLR were determined using R software. Patients were risk-stratified based on their TBS-PALB-NLR (TPN) score. Independent predictors associated with survival were identified using univariate and multivariate Cox proportional hazards regression analyses.
Results: Independent risk factors identified through univariate Cox analysis included age, cirrhosis, ascites, BCLC stage, vascular invasion, NLR, TBS, PALB, AFP, Bilirubin, AST, and ALT. Multivariate analysis revealed that BCLC stage, NLR, TBS, and PALB were significant independent risk factors affecting overall survival (P < 0.05). The TPN score was established based on TBS, PALB, and NLR, and patients were stratified into low-TPN, intermediate-TPN, and high-TPN groups.
Conclusion: The TPN score is a low-cost, readily available prognostic tool that can effectively risk-stratify patients with uHCC. It may guide personalized adjuvant therapy (eg, systemic therapy for high-risk patients), particularly in resource-limited medical centers.
Keywords: hepatocellular carcinoma, transarterial chemoembolization, tumor burden score, PALB, NLR, prognosis
Introduction
Hepatocellular carcinoma (HCC) is a highly heterogeneous malignant tumor characterized by high incidence and mortality rates.1 Since the majority of patients are diagnosed at intermediate or advanced stages, they are often unsuitable for surgical treatment. Only a small proportion of patients can undergo surgical resection or liver transplantation to achieve favorable therapeutic outcomes.2 TACE is typically the first-line treatment for patients with intermediate or advanced HCC.3 It aims to destroy tumor cells by embolizing the tumor-feeding vessels and locally releasing chemotherapeutic agents. This locoregional therapy has improved the survival rates of patients with advanced HCC.
However, due to the highly heterogeneous nature of HCC, there is significant variability in tumor burden and liver functional reserve among patients receiving TACE therapy. This inherent patient heterogeneity may lead to diverse therapeutic outcomes following TACE treatment.4 The prognosis of HCC patients after TACE is influenced by multiple factors, including tumor burden (tumor size and number), liver function, vascular invasion, and tumor biomarkers.5,6 Traditional HCC staging systems based on tumor burden, such as the BCLC staging system and the American Joint Committee on Cancer (AJCC) TNM staging system, are used to guide clinical practice.7,8 Nevertheless, commonly used prognostic models still assess tumor burden using dichotomous cutoff values. Studies have demonstrated that dichotomizing tumor size and number reduces statistical power, potentially diminishing the prognostic predictive ability for HCC patients.
Several prognostic models have been established to predict outcomes for HCC patients undergoing TACE, aiming to refine patient selection and personalize treatment strategies. Among them, the Albumin-Bilirubin (ALBI) grade has been widely adopted as a objective measure of liver function reserve. The ALBI grade, calculated solely from albumin and bilirubin levels, effectively stratifies patients based on hepatic dysfunction and has demonstrated prognostic value in the TACE setting.9 Furthermore, models that integrate both tumor burden and liver function have been developed. The Hepatoma Arterial-embolization Prognostic (HAP) score and its modified version (mHAP) are among the most recognized. The HAP score incorporates four pre-TACE parameters: albumin, bilirubin, alpha-fetoprotein (AFP), and tumor size.10 The mHAP score further refines this by including tumor number and replacing bilirubin with the ALBI grade, offering improved prognostic performance.11 While these models represent significant advances, they possess certain limitations. Firstly, they often assess tumor burden using dichotomous cut-offs for tumor size and number, which may reduce statistical power and fail to capture the continuous nature of tumor burden. Secondly, and crucially, these established models largely overlook the role of systemic inflammation, which is increasingly recognized as a key driver of tumor progression and poor prognosis in HCC.12,13 Parameters like the Neutrophil-to-Lymphocyte Ratio (NLR), a readily available marker of systemic inflammation, are not included in the ALBI, HAP, or mHAP systems. Therefore, a prognostic tool that synergistically integrates a continuous measure of tumor burden, a sensitive indicator of liver function and nutritional status, and a marker of systemic inflammation is lacking.
Recently, a novel scoring system termed the “Tumor Burden Score” (TBS) has been proposed for risk stratification of multifocal tumors.14 Sasaki et al were the first to incorporate tumor size and number as continuous variables, calculating TBS using a specific formula.15 They demonstrated that TBS could serve as an accurate tool for prognostic stratification in patients with colorectal liver metastases. Several studies have indicated the significant potential of TBS in predicting prognosis for patients undergoing surgical resection of liver metastases, HCC, and intrahepatic cholangiocarcinoma.16–18 Concurrently, prealbumin levels (PALB) and the NLR reflect liver function and inflammatory status, respectively. Compared to ALB, PALB has a considerably shorter half-life (approximately 2–3 days), while ALB has a longer half-life (approximately 21 days). Consequently, PALB serves as a more sensitive and timely indicator for detecting short-term changes in hepatic synthetic function and fluctuations in nutritional status.19,20 Relevant studies have consistently shown their strong association with the prognosis of HCC patients.21,22 However, no studies to date have investigated the prognostic impact of the combined assessment of tumor burden, liver function, and inflammatory status on patients with uHCC undergoing TACE therapy. Therefore, in our study, we developed a prognostic scoring system by integrating these three factors: TBS, PALB, and NLR to evaluate its prognostic significance for patients with uHCC receiving TACE treatment.
Materials and Methods
Patients
Clinical data from 940 patients with uHCC who underwent TACE treatment at three medical institutions in the Jiangsu Province between 2007 and 2018 were retrospectively collected. The primary ethical approval for this research, encompassing the use of data from all participating centers, was obtained from the Institutional Review Board (IRB) of The First Affiliated Hospital of Soochow University. For the other two participating hospitals, we did obtain official institutional data access and collaboration agreements from the respective administrative or research departments of these partner hospitals. Because this study was a retrospective analysis of anonymized patient data, the requirement for written informed consent was waived by the Institutional Review Board of The First Affiliated Hospital of Soochow University.
Inclusion criteria: (1) Pathologically confirmed diagnosis of HCC; (2) Patients deemed unsuitable for or refusing surgical resection; (3) No prior antitumor therapy received before the first TACE session; (4) Absence of diseases known to affect serum PALB levels, such as cardiovascular diseases, respiratory infections, or autoimmune disorders.
Exclusion criteria: (1) Concurrent other malignancies; (2) Pathologically confirmed non-HCC diagnosis; (3) History of other antitumor therapies prior to TACE; (4) Conditions affecting serum prealbumin levels or presence of severe underlying comorbidities; (5) Inconsistent follow-up, loss to follow-up, or incomplete clinical data.
Clinical Data Collection
The collected clinical data encompassed: gender, age, tumor characteristics, presence of liver cirrhosis, ascites, Hepatitis B virus (HBV) infection status, alanine aminotransferase (ALT), aspartate aminotransferase (AST), PALB, ALB, Bilirubin, alpha-fetoprotein (AFP), BCLC stage, vascular invasion, and NLR.
Definition of the Scoring System
The maximum tumor diameter and tumor number were determined based on preoperative CT/MRI imaging data. TBS is defined as the distance from the origin of the Cartesian plane and include two variables: maximum tumor size (x-axis) and number of tumors (y-axis). Its calculation formula is based on the Pythagorean theorem principle: TBS2 = (maximum tumor diameter)2 + (number of tumors)2 (The distribution of TBS across patients with different BCLC stages is illustrated in Figure 1). The NLR was calculated from preoperative neutrophil and lymphocyte counts. The optimal cutoff values for TBS and NLR were determined using the surv_cutpoint function in R software (Figure 2). High TBS was defined as ≥ 6.05, and high NLR was defined as ≥ 2.01. Low prealbumin level was defined as PALB < 170 mg/L. In this study, the TPN score was defined as follows: 1 point was assigned for each abnormal parameter (high TBS, low PALB, or high NLR). Consequently, patients were stratified into three risk groups based on their TBS-PALB-NLR score: low-risk (score 0–1), intermediate-risk (score 2), and high-risk (score 3).
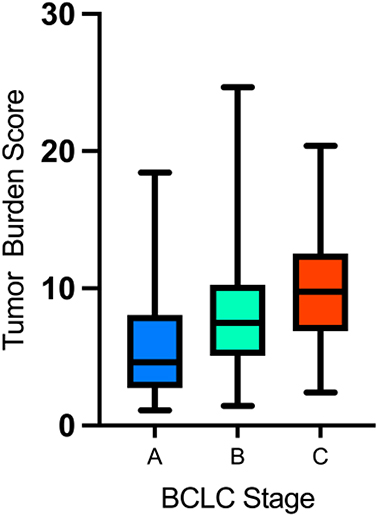 |
Figure 1 Distribution of TBS in patients with different BCLC stages. |
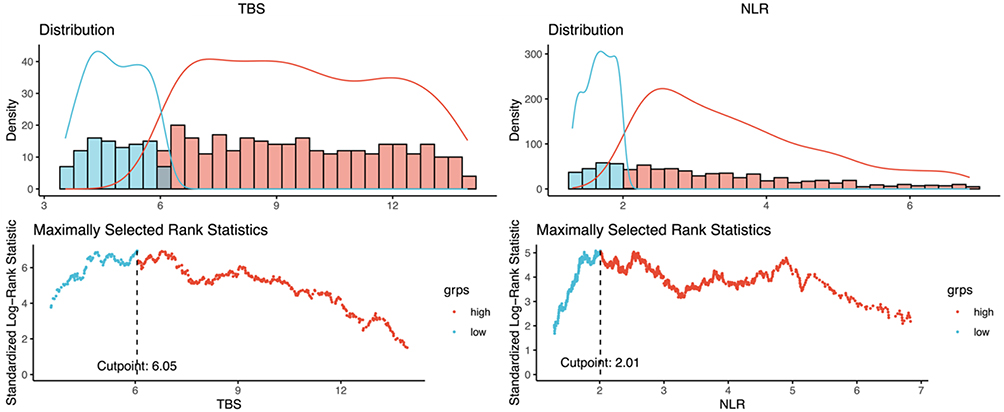 |
Figure 2 The optimal cutoff values for TBS and NLR were determined using the surv_cutpoint function in R software. |
TACE Procedure
Patients underwent conventional transarterial chemoembolization (cTACE). Under local anesthesia, an arterial sheath was placed using the Seldinger technique. Hepatic arteriography and cone-beam CT (CBCT) hepatic arteriography were performed using a 4F RH catheter, with contrast injection rates of 4–6 mL/s and 2–4 mL/s, respectively. Tumor-feeding arteries were identified with the assistance of embolization guidance software. A 2.7F microcatheter was superselectively advanced into the tumor-feeding artery. Chemoembolization was then performed using an emulsion consisting of oxaliplatin (85 mg/m2), epirubicin (10–20 mg), and lipiodol (10 mL). The specific embolization dose was determined by the operator based on tumor size. Embolization was reinforced using a small amount of gelatin sponge particles (350–560 μm). Embolization endpoints were defined as visualization of lipiodol in the portal vein segments and stasis of blood flow in the tumor-feeding artery.
Follow-Up and Assessment
The primary endpoint was patients overall survival (OS), defined as the time from the first TACE session to death. The follow-up period ended on December 31, 2020. Contrast-enhanced CT or MRI was performed at 1 month after the TACE procedure and subsequently at 3-month intervals to evaluate treatment response. The decision to perform additional TACE sessions was based on imaging assessment, the patient’s overall health status, and liver and kidney function.
Statistical Analysis
The optimal cutoff values for TBS and NLR were determined using the surv_cutpoint function in R software. Statistical analyses were performed using SPSS software (version 29.0), and graphs were generated using Prism software. Continuous variables were compared using the independent-samples t-test or non-parametric tests, as appropriate. Categorical variables were analyzed using the Chi-square test. Measurement data are presented as mean ± standard deviation (SD), and enumeration data are presented as frequencies. Survival rates were calculated using the Kaplan-Meier method. Prior to conducting the Cox regression modeling, a multicollinearity test was performed for all variables. The results indicated that all Variance Inflation Factor (VIF) values fell within the range of 1 to 2, demonstrating the absence of significant multicollinearity among the variables. Univariate and multivariate Cox proportional hazards regression analyses were performed, and forest plots were generated. A P-value < 0.05 was considered statistically significant.
Results
Patient Baseline Characteristics
Clinical data from a total of 940 patients with uHCC who underwent TACE were included in this study. The data encompassed gender, age, tumor characteristics (size, number), presence of liver cirrhosis, ascites, HBV infection status, ALT, AST, PALB, ALB, Bilirubin, AFP, BCLC stage, vascular invasion, and NLR. The specific baseline characteristics are presented in Table 1.
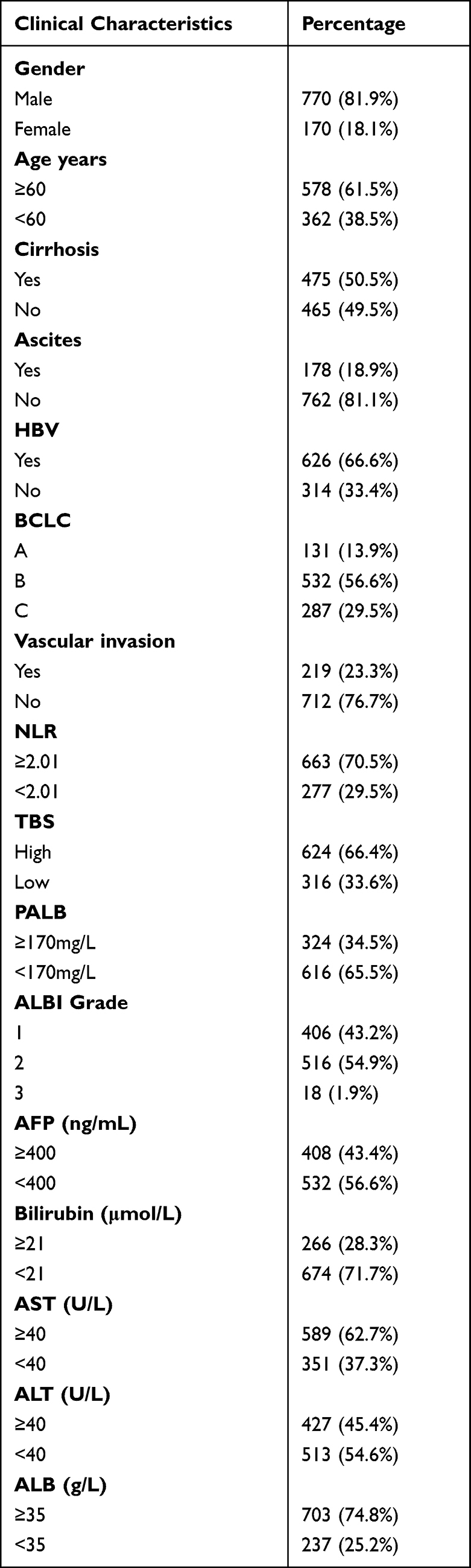 |
Table 1 Baseline |
Univariate and Multivariate Survival Analysis
The results of the univariate survival analysis demonstrated that covariates including age, cirrhosis, ascites, BCLC stage, vascular invasion, NLR, TBS, PALB, AFP, Bilirubin, AST, and ALT were significant risk factors influencing patients’ OS (P < 0.05). These significant factors identified in the univariate analysis were subsequently included in the multivariate survival analysis. The results revealed that BCLC stage, NLR, TBS, and PALB remained significant independent risk factors for OS (P < 0.05). A comprehensive overview of the results from both the univariate and multivariate survival analyses is detailed in Table 2 (The hazard ratio plots from the univariate and multivariate analyses of overall survival are presented in Figure 3).
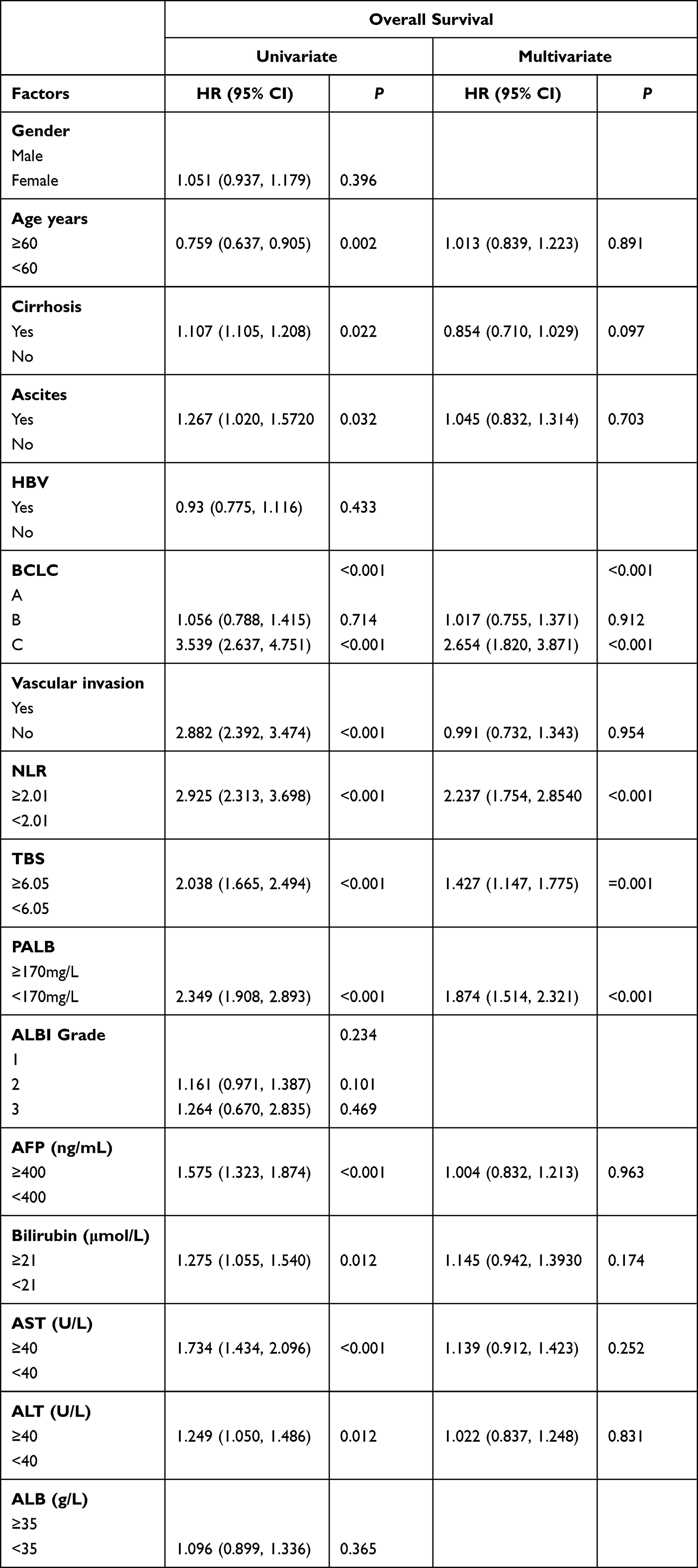 |
Table 2 The Results of Univariate and Multivariate Analysis |
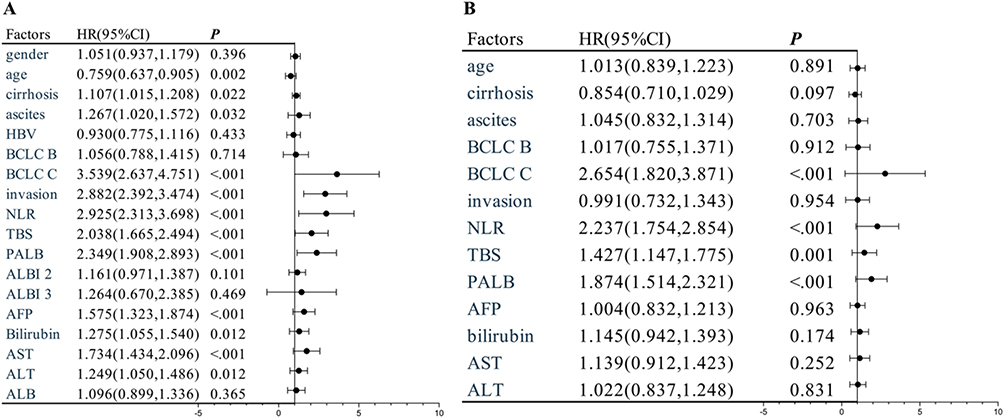 |
Figure 3 Univariate versus multivariate analysis of overall survival. (A) Results of the univariate Cox regression analysis. (B) Results of the multivariate Cox regression analysis. |
Survival Analysis
In this study, the median OS for all patients was 28.67 months (95% CI: 22.61, 34.72). The overall 1-, 3-, and 5-year survival rates were 69.6%, 47.4%, and 41.4%, respectively.
Patients were stratified into low-, intermediate-, and high-risk groups based on the previously defined TPN score (TPN scores of 0–1, 2, and 3 points, respectively). Low-TPN group: The median OS was not reached. The 1-, 3-, and 5-year survival rates were 91.4%, 69.5%, and 59.8%, respectively. Intermediate-TPN group: The median OS was 37.77 months (95% CI: 18.91, 56.62). The 1-, 3-, and 5-year survival rates were 71.3%, 50.5%, and 44.9%, respectively. High-TPN group: The median OS was 12.50 months (95% CI: 9.23, 15.77). The 1-, 3-, and 5-year survival rates were 51.8%, 28.1%, and 24.1%, respectively. There were statistically significant differences in the 1-, 3-, and 5-year survival rates among the low-TPN, intermediate-TPN, and high-TPN groups (P < 0.0001)(The survival curves for patients with different TPN scores are shown in Figure 4).
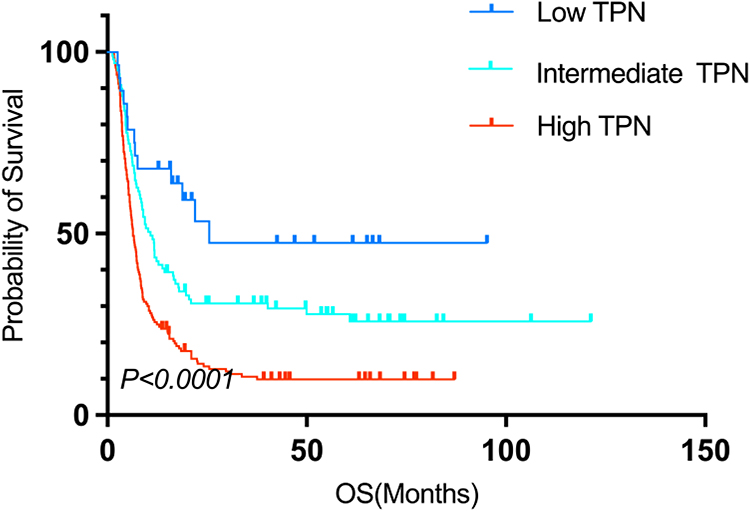 |
Figure 4 Overall survival curves for low, intermediate, and high TPN. |
Stratified Survival Analysis by BCLC Stage
Given that BCLC stage was also identified as a significant risk factor for OS in this study, we performed a survival analysis stratified by TPN score within each BCLC stage category.
Patients with BCLC stage A/B disease: The median OS was 70.20 months (95% CI: 41.86, 98.55), with 1-, 3-, and 5-year survival rates of 84.5%, 59.0%, and 50.8%, respectively. When stratified by TPN score: Low-TPN group: Median OS not reached; 1-, 3-, and 5-year survival rates: 94.3%, 72.1%, 61.2%. Intermediate-TPN group: Median OS not reached; 1-, 3-, and 5-year survival rates: 82.6%, 58.5%, 51.8%. High-TPN group: Median OS: 24.17 months (95% CI: 17.50, 30.84); 1-, 3-, and 5-year survival rates: 74.7%, 43.5%, 36.5%. Statistically significant differences in 1-, 3-, and 5-year survival rates were observed among the three TPN groups (P < 0.0001).
Patients with BCLC stage C disease: The median OS was 7.83 months (95% CI: 6.82, 8.85), with 1-, 3-, and 5-year survival rates of 35.9%, 21.1%, and 19.6%, respectively. When stratified by TPN score: Low-TPN group: Median OS not reached; 1-, 3-, and 5-year survival rates: 67.9%, 47.4%, 47.4%. Intermediate-TPN group: Median OS: 10.80 months (95% CI: 8.45, 13.15); 1-, 3-, and 5-year survival rates: 43.4%, 30.8%, 27.8%. High-TPN group: Median OS: 6.40 months (95% CI: 5.47, 7.33); 1-, 3-, and 5-year survival rates: 25.6%, 10.6%, 9.90%. Statistically significant differences in 1-, 3-, and 5-year survival rates were observed among the three TPN groups (P < 0.0001)(The survival curves of patients based on TPN score, stratified by BCLC stage, are shown in Figure 5).
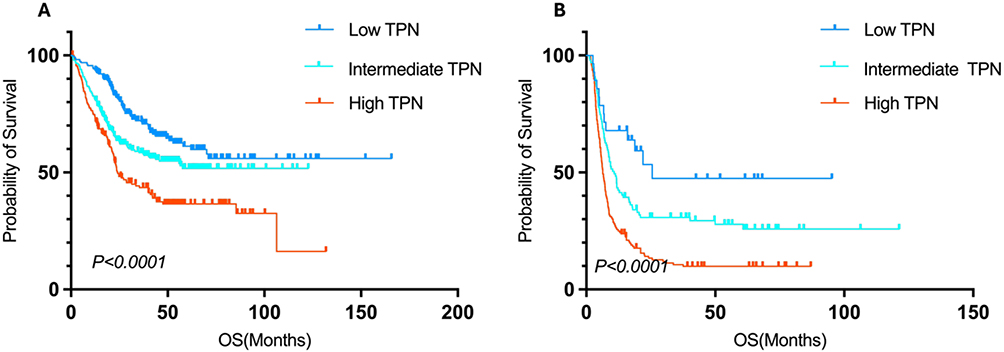 |
Figure 5 Survival curves of patients with different TPN scores based on BCLC staging. (A) Stratified results of patients with BCLC stage A/B based on TPN scores. (B) Stratified results of patients with BCLC stage C based on TPN scores. |
Furthermore, the TPN score demonstrated its ability to stratify HCC patients based on liver function status and underlying disease etiology. As shown in the Figure 6, the TPN score effectively stratified patient survival regardless of the presence or absence of cirrhosis or HBV infection, indicating its broad applicability.
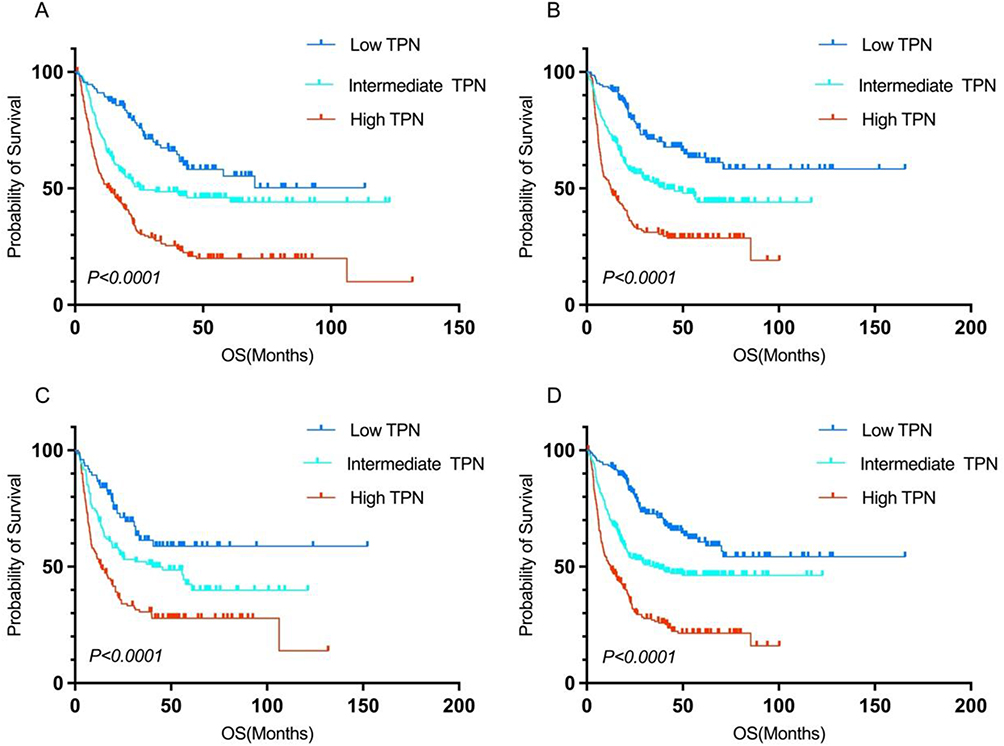 |
Figure 6 Stratification of OS using the TPN Score according to Liver Function and Etiology. (A) Patients with cirrhosis. (B) Patients without cirrhosis. (C) HBV-infected patients. (D) Non-HBV-infected patients. |
Predictive Performance of the TPN Score
As shown in Figure 7, the TPN score demonstrated the highest AUC value (AUC = 0.721) compared to the risk factors identified by the multivariate Cox regression analysis. We performed internal bootstrap validation for the TPN score model using R software. The results demonstrated that for the time-dependent ROC curves at 1, 3, and 5 years, the AUC values for the TPN score system remained stable, with mean values consistently exceeding 0.7 (Figure 8). This indicates a stable predictive performance of the TPN score. Furthermore, decision curve analysis and calibration curves were plotted to evaluate the predictive accuracy of the TPN score (Figure 9). The results showed that the decision curves for 1, 3, and 5 years were above the None line and the All line. Additionally, the calibration curves for predicting OS at 1, 3, and 5 years showed high concordance between predicted and observed outcomes. These findings collectively indicate that the TPN score system possesses stable and accurate predictive performance.
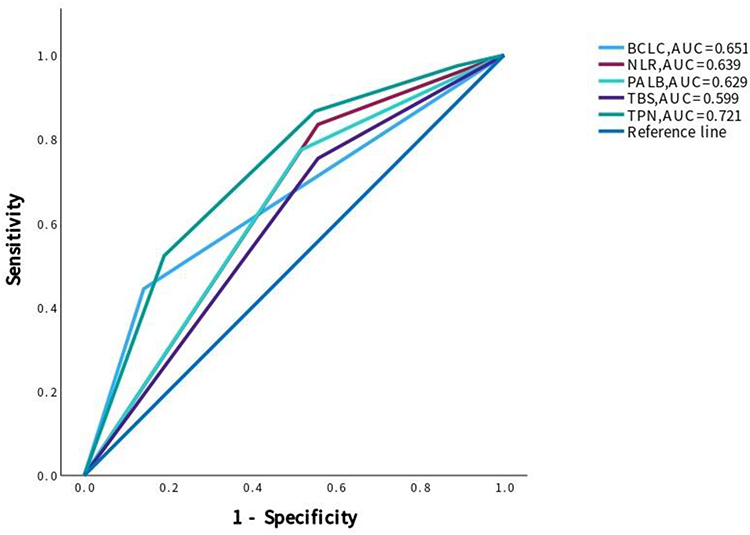 |
Figure 7 AUC of TPN and other risk factors on overall patient survival. |
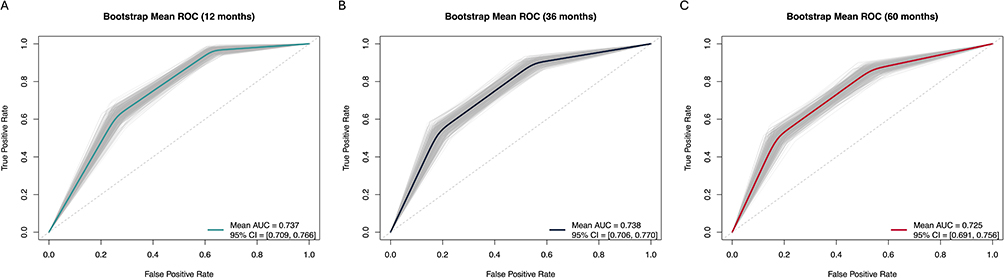 |
Figure 8 Internal bootstrap validation of the TPN score model was performed using R software. (A) ROC curve for predicting 1-year patient survival. (B) ROC curve for predicting 3-year patient survival. (C) ROC curve for predicting 5-year patient survival. |
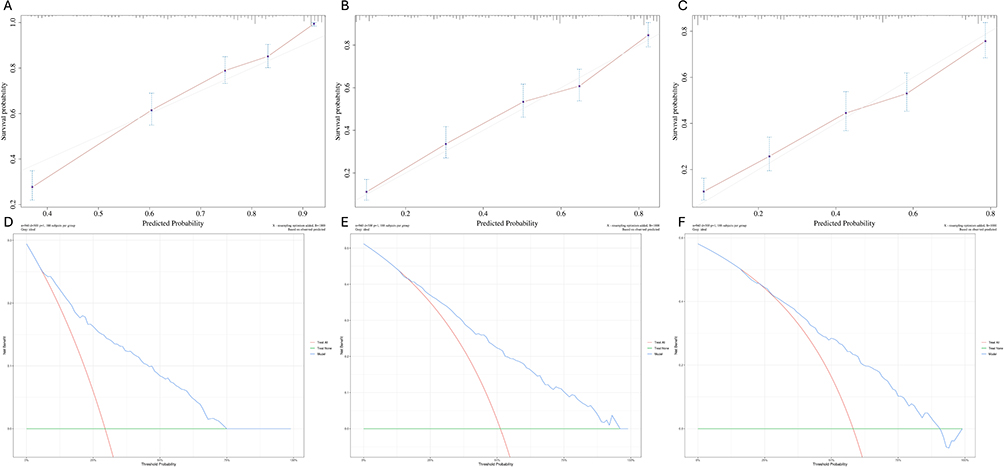 |
Figure 9 Calibration and Decision Curve Analysis (DCA) of the TPN Score. (A–C) Calibration curves for the TPN score at 1, 3, and 5 years. (D–F) Decision curve analysis (DCA) curves for the TPN score at 1, 3, and 5 years. |
Discussion
Despite advancements in diagnostic techniques and treatment options leading to continuous improvements in the clinical management of HCC patients, HCC remains a significant global healthcare challenge. The clinical prognosis of HCC patients continues to exhibit high heterogeneity.23 For patients with intermediate to advanced uHCC, TACE serves as a first-line treatment option.7 However, due to variations in tumor burden and liver functional reserve among HCC patients, heterogeneous responses to TACE therapy may occur, leading to diverse outcomes following TACE treatment in this patient population.4 Consequently, accurate prognostic stratification is crucial for optimizing treatment strategies and improving survival rates.
In this study, we developed a novel preoperative triple score, the TPN score, by integrating the patient’s preoperative TBS, PALB level, and NLR. We demonstrated its robust capability in predicting long-term survival for patients with uHCC following TACE treatment. Our findings underscore the value of integrating tumor morphology, liver functional reserve, and inflammatory status into a single, easily applicable clinical decision-making tool.
Sasaki et al were the first to propose calculating TBS by treating tumor size and number as continuous variables, their research established TBS as an accurate tool for prognostic stratification in patients with colorectal cancer liver metastases. Furthermore, subsequent studies have shown that TBS holds significant potential for predicting outcomes in patients undergoing surgical resection for colorectal liver metastases, HCC, and intrahepatic cholangiocarcinoma.24,25 Studies have also demonstrated that the TBS serves as a significant prognostic indicator for HCC patients undergoing TACE treatment.14,26,27 PALB levels and the NLR reflect liver function and systemic inflammatory status, respectively, and associated research indicates their strong correlation with prognosis in HCC patients. The nutritional status of cancer patients significantly impacts their prognosis, in current clinical practice, albumin levels are commonly monitored to assess both nutritional status and liver function. However, research indicates that PALB demonstrates higher specificity and sensitivity, serving as a valuable biomarker for evaluating nutritional status and predicting prognosis.19,20 Furthermore, a heightened systemic inflammatory state contributes to increased levels of VEGF and PDGF. This, in turn, induces tumor-associated angiogenesis, thereby promoting tumor progression and recurrence.12,13 Related studies have shown that inflammatory cells, including neutrophils, platelets, and monocytes, play crucial roles in various stages of cancer development, encompassing tumor initiation, malignant transformation, promotion, invasion, and metastasis.28–30 However, no prior study has investigated the combined prognostic impact of tumor burden, liver function, and inflammatory status on unresectable HCC patients undergoing TACE therapy. Therefore, our study explored the predictive value of the TBS-PALB-NLR triple score system for outcomes in uHCC patients receiving TACE treatment.
The TPN score developed in this study provides a simple and practical prognostic tool for enabling personalized clinical management of patients with uHCC. Based on the significantly different survival outcomes observed in our study, we propose a potential pathway for TPN score-guided treatment intensification and follow-up planning: For patients in the low-TPN group, who have a favorable prognosis, standard cTACE protocol can be followed. Given their good prognosis, aggressive initial combination with expensive systemic therapies might be unnecessary, thereby avoiding unnecessary toxicity and financial burden for patients. Furthermore, considering their relatively stable disease course, follow-up intervals could potentially be extended after confirmed disease stability to reduce healthcare resource utilization and patient inconvenience. For patients in the intermediate-TPN group, who have a moderate prognosis, close monitoring of their response to the first TACE session is crucial. If the initial response is suboptimal, earlier consideration should be given to combining systemic therapy (eg, Tyrosine Kinase Inhibitors [TKIs] or Immune Checkpoint Inhibitors [ICIs]) to overcome TACE resistance.31–33 For patients in the high-TPN group, who have a very poor prognosis characterized by high tumor burden, compromised liver function, and strong systemic inflammatory response, the benefit from TACE alone is limited. Therefore, for these patients, aggressive combination therapy regimens should be actively considered from the very beginning of treatment. Our data showed that even high-TPN patients within BCLC A/B stages had a poor prognosis, strongly supporting the early introduction of systemic therapy in this subgroup to improve survival. Additionally, due to their high risk of disease progression, more intensive and frequent follow-up is mandatory. This follow-up should not be limited to imaging assessments but should also include dynamic monitoring of liver function and inflammatory markers to facilitate the timely detection of disease progression or liver function deterioration, allowing for rapid adjustment of treatment strategies.
All parameters comprising the TPN score are readily available and low-cost, making this scoring system particularly suitable for resource-limited medical centers. Through a simple calculation, physicians can quickly identify those high-risk patients with a very poor prognosis who urgently require referral to higher-level medical centers for intensive combination therapy, while also enabling the safe and more cost-effective management of low-risk patients.
Comparison of the TPN Score with Existing Prognostic Models
The BCLC staging system is an internationally recognized guideline for HCC management. It integrates tumor burden, liver function, and performance status to guide initial treatment decisions for liver cancer patients. However, substantial heterogeneity exists within BCLC stages, particularly stages B and C, meaning patients classified under the same BCLC B or C stage can have significantly different prognoses. Furthermore, its assessment of tumor burden relies on categorical variables rather than continuous variables, which may reduce its statistical power. In our study, although BCLC stage itself was a risk factor for patient OS, our TPN score further enabled effective risk stratification within each BCLC stage. This finding indicates that the TPN score can compensate for the limitations of the BCLC staging system in patient risk stratification, thereby providing a valuable supplement and refinement to the BCLC framework. The ALBI grade is another predictive model used for HCC patients.34 It utilizes objective indicators (albumin and bilirubin) to assess liver function more precisely. However, it focuses solely on liver function, overlooking two other critical prognostic factors: tumor burden and systemic inflammatory status. Moreover, in our multivariate Cox regression analysis, the ALBI grade did not emerge as an independent predictor of overall survival (P = 0.234), whereas all three components of the TPN score (TBS, PALB, NLR) were independent predictors. This suggests that the TPN score may possess superior prognostic predictive capability compared to the ALBI grade for uHCC patients undergoing TACE. The HAP score and its modified version (mHAP) are prognostic models specifically designed for TACE patients. They attempt to integrate tumor-related factors and liver function factors. However, the assessment of tumor size and number in the HAP/mHAP scores often relies on dichotomous categorization. This categorical approach can lead to loss of information and diminished statistical power. In contrast, the TPN score utilizes the TBS, which treats tumor size and number as continuous variables, providing a more precise quantification of tumor burden. Additionally, the HAP/mHAP scores do not incorporate systemic inflammatory markers. The NLR, an easily obtainable and low-cost inflammatory marker, has been demonstrated by numerous studies to be associated with HCC prognosis and was an independent prognostic factor for OS in our study. Therefore, we integrated it into the TPN score. Concurrently, we included PALB instead of ALB; PALB has a short half-life and is considered a more sensitive indicator of nutritional status and hepatic synthetic function than ALB. Although this study did not perform a direct statistical comparison with the HAP/mHAP scores, the TPN score, through its continuous quantification of tumor burden, inclusion of inflammatory status, and utilization of a more sensitive nutritional marker, offers conceptual and methodological refinements.
Limitations
This study has several limitations. First, the primary inherent limitation of this study lies in its retrospective design. Although we included a large patient sample from three centers and applied strictly uniform inclusion and exclusion criteria, the retrospective analysis remains susceptible to selection bias and the influence of unmeasured confounding factors. Consequently, our conclusions require further validation through prospective studies. Second, the proposed TPN score currently lacks external validation. Both model development and performance evaluation in this study were based on the same patient cohort, which may lead to an overoptimistic estimation of the model’s predictive performance. The generalizability of the TPN score and its performance in settings with different practice patterns and patient populations from our centers remain unclear. Therefore, a critical next step is to conduct multi-center, multi-regional external validation, preferably involving patient cohorts from different countries with varying healthcare practices, to rigorously assess the TPN score’s generalizability and clinical applicability. Third, the geographical homogeneity and etiological composition of the study cohort represent a significant limitation. All patients were recruited from three hospitals in China, where HBV infection is the predominant etiology. This contrasts sharply with HCC patient populations in Western countries, where alcoholic liver disease (ALD) and non-alcoholic steatohepatitis (NASH) are the leading causative factors. HCCs of different etiologies may differ in tumor biology, underlying liver disease background, and treatment response. Therefore, the prognostic predictive efficacy of the TPN score in non-HBV predominant populations may require recalibration. Future studies are urgently needed to validate the TPN score in international cohorts with diverse etiological compositions to determine if it is a truly universal prognostic tool. Finally, it is important to note that the data collection period for this study predates the era where immune checkpoint inhibitors and modern tyrosine kinase inhibitors became first-line standard treatments for unresectable HCC. Our findings were established within a treatment context dominated by cTACE. While we recommend intensified combination therapy for high-TPN score patients, the specific regimens for such intensification in current clinical practice, and the predictive value of the TPN score in patients receiving TACE combined with these modern systemic therapies, remain to be explored in future prospective clinical trials.
Conclusion
The TPN score is a novel, low-cost prognostic tool that integrates tumor burden, liver function, and systemic inflammatory status. It can predict long-term survival in uHCC patients receiving TACE therapy and holds clinical value, particularly in resource-limited medical settings. This score refines risk stratification within the BCLC staging system and demonstrates potential for assisting in the development of personalized treatment strategies based on BCLC stages. However, future multi-center prospective studies are required to validate these findings and to aid clinicians in patient risk stratification and treatment decision-making.
Ethical Statement
The primary ethical approval for this research, encompassing the use of data from all participating centers, was obtained from the Institutional Review Board (IRB) of The First Affiliated Hospital of Soochow University (Ethical Approval Number: [2024641]). For the other two participating hospitals, we did obtain official institutional data access and collaboration agreements from the respective administrative or research departments of these partner hospitals, and was conducted in strict accordance with the principles of the Declaration of Helsinki. As this study was retrospective, the committee waived the requirement of informed consent. All patient-related data used in this study complied with privacy protection regulations.
Acknowledgments
The authors would like to acknowledge the following member of the grant project for his contributions and support: Caifang Ni (The First Affiliated Hospital of Soochow University).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China Project [grant number 82272094].
Disclosure
The authors have all declared that they do not have any conflicts of interest.
References
1. Huang DQ, Singal AG, Kanwal F, et al. Hepatocellular carcinoma surveillance - utilization, barriers and the impact of changing aetiology. Nat Rev Gastroenterol Hepatol. 2023;20(12):797–809. doi:10.1038/s41575-023-00818-8
2. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
3. Zhong BY, Jin ZC, Chen JJ, Zhu HD, Zhu XL. Role of transarterial chemoembolization in the treatment of hepatocellular carcinoma. J Clin Transl Hepatol. 2023;11(2):480–489. doi:10.14218/JCTH.2022.00293
4. Pinero F, Dirchwolf M, Pessoa MG. Biomarkers in hepatocellular carcinoma: diagnosis, prognosis and treatment response assessment. Cells. 2020;9(6):1370. doi:10.3390/cells9061370
5. Hung YW, Lee IC, Chi CT, et al. Radiologic patterns determine the outcomes of initial and subsequent transarterial chemoembolization in intermediate-stage hepatocellular carcinoma. Liver Cancer. 2024;13(1):29–40. doi:10.1159/000530950
6. Muller L, Stoehr F, Mahringer-Kunz A, Hahn F, Weinmann A, Kloeckner R. Current strategies to identify patients that will benefit from TACE treatment and future directions a practical step-by-step guide. J Hepatocell Carcinoma. 2021;8:403–419. doi:10.2147/JHC.S285735
7. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
8. Moris D, Martinino A, Schiltz S, et al. Advances in the treatment of hepatocellular carcinoma: an overview of the current and evolving therapeutic landscape for clinicians. CA Cancer J Clin. 2025;75(6):498–527. doi:10.3322/caac.70018
9. Li J, Feng T, Cui C, et al. Post-TACE ALBI-score trajectory in intermediate and advanced hepatocellular carcinoma: prognostic implications and influencing factors analysis. J Hepatocell Carcinoma. 2025;12:865–878. doi:10.2147/JHC.S503581
10. Zhu Y, Wang E, Zhao S, et al. Identify optimal HAP series scores for unresectable HCC patients undergoing TACE plus sorafenib: a Chinese multicenter observational study. Front Oncol. 2022;12:983554. doi:10.3389/fonc.2022.983554
11. Jia K, Yin W, Gao Z, et al. Recommendation of mHAP and ABCR scoring systems for the decision-making of the first and subsequent TACE session in HCC patients. Eur J Gastroenterol Hepatol. 2023;35(4):461–470. doi:10.1097/MEG.0000000000002515
12. Chen S, Shen B, Wu Y, et al. The relationship between the efficacy of thermal ablation and inflammatory response and immune status in early hepatocellular carcinoma and the progress of postoperative adjuvant therapy. Int Immunopharmacol. 2023;119:110228. doi:10.1016/j.intimp.2023.110228
13. Prieto J, Melero I, Sangro B. Immunological landscape and immunotherapy of hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2015;12(12):681–700. doi:10.1038/nrgastro.2015.173
14. Ho SY, Liu PH, Hsu CY, et al. Tumor burden score as a new prognostic marker for patients with hepatocellular carcinoma undergoing transarterial chemoembolization. J Gastroenterol Hepatol. 2021;36(11):3196–3203. doi:10.1111/jgh.15593
15. Sasaki K, Morioka D, Conci S, et al. The tumor burden score: a New “Metro-ticket” prognostic tool for colorectal liver metastases based on tumor size and number of tumors. Ann Surg. 2018;267(1):132–141. doi:10.1097/SLA.0000000000002064
16. Moris D, Shaw BI, McElroy L, Barbas AS. Using hepatocellular carcinoma tumor burden score to stratify prognosis after liver transplantation. Cancers. 2020;12(11):3372. doi:10.3390/cancers12113372
17. Endo Y, Tsilimigras DI, Munir MM, et al. Prognostic significance of postoperative complications for patients with hepatocellular carcinoma relative to alpha-feto protein and tumor burden score. HPB. 2024;26(8):998–1006. doi:10.1016/j.hpb.2024.04.013
18. Qiu ZC, Wu YW, Qi WL, Li C. PIVKA-II combined with tumor burden score to predict long-term outcomes of AFP-negative hepatocellular carcinoma patients after liver resection. Cancer Med. 2024;13(1):e6835. doi:10.1002/cam4.6835
19. Ranasinghe RN, Biswas M, Vincent RP. Prealbumin: the clinical utility and analytical methodologies. Ann Clin Biochem. 2022;59(1):7–14. doi:10.1177/0004563220931885
20. Watanabe T, Shibata M, Nishiyama H, et al. Serum levels of rapid turnover proteins are decreased and related to systemic inflammation in patients with ovarian cancer. Oncol Lett. 2014;7(2):373–377. doi:10.3892/ol.2013.1735
21. Xu L, Zhao D, Tian P, et al. Development and validation of a prognostic model for transarterial chemoembolization in unresectable hepatocellular carcinoma based on preoperative serum prealbumin. J Hepatocell Carcinoma. 2023;10:2239–2250. doi:10.2147/JHC.S433245
22. Wang D, Bai N, Hu X, et al. Preoperative inflammatory markers of NLR and PLR as indicators of poor prognosis in resectable HCC. PeerJ. 2019;7:e7132. doi:10.7717/peerj.7132
23. Wang Q, Xia D, Bai W, et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: a multicentre observational study. J Hepatol. 2019;70(5):893–903. doi:10.1016/j.jhep.2019.01.013
24. Lima HA, Endo Y, Alaimo L, et al. Tumor burden score and serum alpha-fetoprotein subclassify intermediate-stage hepatocellular carcinoma. J Gastrointest Surg. 2022;26(12):2512–2521. doi:10.1007/s11605-022-05469-9
25. Ding HF, Yang T, Lv Y, Zhang XF, Pawlik TM. International Hepatocellular Carcinoma Study G. development and validation of an alpha-fetoprotein tumor burden score model to predict postrecurrence survival among patients with hepatocellular carcinoma. J Am Coll Surg. 2023;236(5):982–992. doi:10.1097/XCS.0000000000000638
26. Xia D, Wang Q, Bai W, et al. Optimal time point of response assessment for predicting survival is associated with tumor burden in hepatocellular carcinoma receiving repeated transarterial chemoembolization. Eur Radiol. 2022;32(9):5799–5810. doi:10.1007/s00330-022-08716-4
27. Muller L, Hahn F, Auer TA, et al. Tumor burden in patients with hepatocellular carcinoma undergoing transarterial chemoembolization: head-to-head comparison of current scoring systems. Front Oncol. 2022;12:850454. doi:10.3389/fonc.2022.850454
28. Li N. Platelets in cancer metastasis: to help the “villain” to do evil. Int J Cancer. 2016;138(9):2078–2087. doi:10.1002/ijc.29847
29. Salmaninejad A, Valilou SF, Soltani A, et al. Tumor-associated macrophages: role in cancer development and therapeutic implications. Cell Oncol. 2019;42(5):591–608. doi:10.1007/s13402-019-00453-z
30. Zhang X, Zhang W, Yuan X, Fu M, Qian H, Xu W. Neutrophils in cancer development and progression: roles, mechanisms, and implications (Review). Int J Oncol. 2016;49(3):857–867. doi:10.3892/ijo.2016.3616
31. Xue M, Wu Y, Tang Y, et al. Efficacy and safety of TACE combined with lenvatinib and PD-1 Inhibitor in intermediate-stage HCC exceeding the up-7 criteria: a retrospective cohort study. Front Immunol. 2025;16:1560750. doi:10.3389/fimmu.2025.1560750
32. Guo Y, Pan Z, Kan X, et al. Immunotherapy improved the efficacy of TACE or TACE plus MTTs in HCC patients: a meta-analysis. Int Immunopharmacol. 2025;147:114006. doi:10.1016/j.intimp.2024.114006
33. Xiao CL, Zhong ZP, Lu C, et al. Physical exercise suppresses hepatocellular carcinoma progression by alleviating hypoxia and attenuating cancer stemness through the Akt/GSK-3beta/beta-catenin pathway. J Integr Med. 2023;21(2):184–193. doi:10.1016/j.joim.2023.01.002
34. Hiraoka A, Kumada T, Michitaka K, Kudo M. Newly proposed ALBI grade and ALBI-T score as tools for assessment of hepatic function and prognosis in hepatocellular carcinoma patients. Liver Cancer. 2019;8(5):312–325. doi:10.1159/000494844
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.