Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Switch from Reference Biologic Medicines to Biosimilars in France: The Perspective of Patients and Prescribers on Barriers and Needs
Authors Gaujoux-Viala C, Tropé S ![]() , Buisson A, Lacombe F, Bocquet F, Languérand E, Cordurié L
, Buisson A, Lacombe F, Bocquet F, Languérand E, Cordurié L ![]() , Margulies G
, Margulies G ![]() , Le Berre C, Vittecoq O
, Le Berre C, Vittecoq O
Received 14 March 2025
Accepted for publication 23 July 2025
Published 14 October 2025 Volume 2025:18 Pages 6681—6698
DOI https://doi.org/10.2147/JMDH.S528370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Cécile Gaujoux-Viala,1,2 Sonia Tropé,3 Anne Buisson,4 Fabienne Lacombe,5 François Bocquet,6,7 Emeric Languérand,8 Laura Cordurié,9 Géraldine Margulies,10 Catherine Le Berre,11 Olivier Vittecoq12
1Inserm, IDESP, University of Montpellier, Montpellier, France; 2Rheumatology Department, CHU of Nîmes, Nîmes, France; 3French National Patient Organization Against Rheumatoid Arthritis (ANDAR), Paris, France; 4AFA Crohn RCH France, Paris, France; 5Association France Spondyloarthrites, Tulle, France; 6Data Factory & Analytics Department, Institut de Cancérologie de l’Ouest, Nantes-Angers, France; 7Law and Social Change Laboratory, Faculty of Law and Political Sciences, Nantes University, Nantes, France; 8Psychologist and Psychotherapist Cannes Sainte-Anne Hospital Paris, Paris, France; 9Consultant Access Strategy and Public Affairs Real World Solution, IQVIA France, Courbevoie, France; 10Marketing Biosimilars, Biogen France SAS, Puteaux, France; 11Institut des Maladies de l’Appareil Digestif, Hépato-Gastro-Entérologie et Assistance Nutritionnelle, CHU Nantes, Nantes, France; 12Rheumatology Department, CHU of Rouen, Rouen, France
Correspondence: Géraldine Margulies, Biogen France SAS, Tour Légende, 20 Place de la Défense, Puteaux, 92 800, France, Tel +33 1 41 37 95 95, Fax +33 1 41 37 24 00, Email [email protected]
Purpose: In France, the integration of biosimilars into medical practice in rheumatology and gastroenterology is well established. Despite a high penetration rate in hospitals, the adoption of biosimilars varies depending on the molecules. This adoption differs between new patients, for whom biosimilars are prescribed as initial biologic treatment, and those receiving these medications as part of a treatment switch from reference biologics. The objective of the COMPRENDRE study was to identify and understand the obstacles to switching from reference biologic products to their biosimilars by examining prescription practices and patient decisions. This study proposes recommendations to overcome these barriers.
Patients and Methods: A total of twelve rheumatology and gastroenterology prescribers and fourteen patients with rheumatologic and gastrointestinal disorders were interviewed for qualitative insights. Subsequently, one hundred prescribing physicians and one hundred ninety patients responded to a quantitative survey to validate and explore these findings. The study was supervised by a multidisciplinary expert committee.
Results: The results from the quantitative and qualitative surveys show similarities in the outcomes. In the qualitative study, 71% (10/14) of patients accepted the switch to a biosimilar. For half of them (7/14), trust in the physician-patient relationship was the main reason for acceptance. Key barriers identified by prescribers included the limited time available during consultations and patient anxiety due to their illness, both of which negatively impacted willingness to switch. In the quantitative study, 89% (89/100) prescribers reported prescribing biosimilars through switching from the reference biologic. However, only 33% (29/89) indicated that they systematically switch eligible patients. Overall, 55% (104/190) of the patients surveyed had never been offered a switch to a biosimilar.
Conclusion: Switching from a reference biologic to biosimilars is hampered by several factors, including the lack of systemic proposals in the practice of prescribers as well as the lack of information given to patients.
Keywords: biologic, biosimilar, gastroenterology, healthcare professional, patient satisfaction, rheumatology, shared decision making, switch
Introduction
The introduction of biosimilars to the European market starting in 2006 1 provided less costly but equally effective alternatives to reference biologic treatments. These more affordable medications, with equivalent efficacy and comparable pharmacokinetic, safety and immunogenicity profiles as their reference products, help to stimulate competition and contribute to alleviate the economic burden on healthcare systems. Biosimilars have gradually gained importance in the market, notably in the past five years, with the number of approvals doubling compared to the previous decade.2
Biosimilars have progressively penetrated markets in various therapeutic areas such as oncology, diabetes, rheumatology, dermatology, gastroenterology, and ophthalmology. This explains why biosimilar use is more established in some therapeutic areas than others. In France, the utilization of biosimilars is well integrated into the clinical practice of therapeutic areas such as rheumatology and gastroenterology; however, it is more recent in other areas such as ophthalmology. The first biosimilar used in rheumatology and gastroenterology, infliximab, was marketed in France in 2015,3 followed by other TNF-alpha inhibitors in 2016 (etanercept) and 2018 (adalimumab). Biosimilars of two TNF-alpha inhibitors are used in both rheumatology and gastroenterology.4
Despite a high hospital penetration rate, estimated at 90% in 2023, the adoption of biosimilars in community settings remains limited, with an average penetration rate of 31.9%.5 This observation is accompanied by significant heterogeneity between biosimilar molecules, with penetration rates in community settings ranging from 3% to 92.7%.5
The adoption of biosimilars also differs between naïve patients for whom the biosimilar is proposed as the initial prescription compared with switched patients who have had previous therapeutic exposure to the reference biologic. In 2021, the initiation rate of naïve patients to infliximab, etanercept, and adalimumab biosimilars was 94%, 67%, and 59%, respectively, contrasting with 48%, 20%, and 18% of patients treated with the reference biologic infliximab, etanercept, and adalimumab who transitioned to a biosimilar during their follow-up.4
According to the scientific literature, this limited adoption of biosimilars in switched patients is driven by multiple factors, primarily related to healthcare professionals ‘confidence and practices, as well as patient activation.
A lack of confidence in biosimilars among patients has been identified as a factor negatively influencing the perception of these medications and causing some reluctance to accept them.6 Patients have expressed concerns about a potential loss of efficacy or the appearance of side effects when switching from reference biologic to biosimilar treatment.7 Additionally, patients’ lack of understanding of the rigor of the approval process and health-economic benefits of biosimilars could reinforce their reluctance to accept biosimilars.8
Among healthcare professionals, a need for additional knowledge and experience regarding biosimilars has been observed, particularly among physicians and pharmacists.9,10 Limited knowledge and a lack of experience with biosimilars induced a lack of confidence and trust in biosimilars among healthcare professionals.8 Additionally, healthcare professionals’ reluctance to inform patients about biosimilars, due to fear of worrying them7 or time constraints during patient visits, has been identified as an additional barrier to the adoption of these medications.11
To better identify these mechanisms, the COMPRENDRE study, initiated in 2023, analysed the utilization of biosimilars, the barriers to their prescription, and their acceptance by patients. This study was conducted in two phases: qualitative interviews with prescribers and patients with rheumatologic and gastrointestinal disorders, and an electronic quantitative survey to validate and further explore the results with the same respondent profiles. A committee of experts supervised the entire process and participated in consolidating and validating the insights to formulate recommendations aimed at overcoming barriers to switching in France.
Materials and Methods
Establishment of an Expert Committee for the Utilization of Biosimilars
A multidisciplinary committee of experts was established to support the project throughout its development and at each stage. This committee comprised two rheumatologists, a gastroenterologist, a psychologist, a health economist, a public health expert and three representatives of patient associations.
Qualitative Study
Background
The qualitative study, conducted from June to July 2023 in mainland France, involved a series of semi-structured telephone interviews, each lasting approximately one hour. These interviews were conducted with prescribers of biologic medicines and patients treated with biologics. An interview guide, revised and validated by the members of the expert committee, was used to ensure all relevant themes were addressed. This guide was not shared with respondents prior to the interviews.
Methodological Considerations
To ensure the reliability and rigor of the interviews and facilitate the publication of the results the COREQ (Consolidated criteria for reporting qualitative research)12 checklist was used throughout all methodological decisions. This encompassed the development of the interview guide, selection of data collection and analysis methods, and the interpretation of the findings.
Inclusion and Exclusion Criteria
The recruitment process of prescribers and patients was established to ensure the representativeness and relevance of the respondents and was validated by the expert committee.
- Prescribers: Rheumatologists and gastroenterologists who prescribe biologic medicines. Participants were evenly distributed between the two specialties, practicing across the French territory and in clinical settings, with a target of 60% in hospital (regional and local) and/or mixed settings, and 40% in community settings.
- Patients: Participants had to be over 18 years old, without cognitive disorders, and diagnosed with a rheumatic or gastrointestinal disease. They must have been treated, or be currently treated, with the reference biologic medicine infliximab, etanercept, or adalimumab, with a proposal to switch to a biosimilar, regardless of whether they accepted or not. Participants were required to live and be treated in France either in a hospital, or mixed or community settings. Gender parity was sought as much as possible.
- Quotas of Respondents: Quotas of responses were determined in collaboration with the expert committee to ensure data saturation.
Participant Recruitment
Physicians were recruited by IQVIA France based on the inclusion and exclusion criteria. Patients were identified by the healthcare professionals participating in the interviews and by patient associations that are members of the expert committee.
Conducting the Interviews
Interviews were conducted in parallel to ensure consistency and avoid temporal biases in the collected information. Two members of the project team conducted to ensure continuity and limit interpretation biases.
Transcription of Insights
Insights from each interview were recorded in a transcription grid by the moderators.
Quantitative Study
Background
To further explore and validate the insights from the qualitative study, a quantitative study with a larger panel of respondents was conducted from November 2023 to January 2024. This study targeted prescribers of biologic medicines and patients treated with biologics. Two versions of online questionnaires were used, one for prescribers and one for patients. The questionnaires, composed of multiple-choice questions without open-ended responses, were revised and validated by the expert committee.
Inclusion and Exclusion Criteria
The recruitment process for prescribers and patients was established to ensure the representativeness and relevance of the respondents and was validated by the expert committee.
- Prescribers: Rheumatologists and gastroenterologists who prescribe biologic medicines. Participants were evenly distributed between the two specialties, practicing across the French territory and in clinical settings, with a target of 60% in hospital (regional and local) and/or mixed settings, and 40% in community settings.
- Patients: Participants had to be over 18 years old, without cognitive disorders, and diagnosed with a rheumatic or gastrointestinal disease. They must have been treated, or be currently treated, with the reference biologic medicine infliximab, etanercept, or adalimumab, with a proposal to switch to a biosimilar, regardless of whether they accepted or not. Participants were required to live and be treated in France either in a hospital, or mixed or community settings. Gender parity was sought as much as possible.
- Quotas of respondents: Quotas were determined in collaboration with the expert committee, targeting a total of 100 physicians. Initially, the quota was also set at 100 patients. However, due to a surge in participation, the collection period was extended by one month to accommodate a larger volume of responses.
Participant Recruitment
Physicians were recruited by IQVIA France based on the inclusion and exclusion criteria and received the survey link by email. Patients were recruited by healthcare professionals and representatives of patient associations who are members of the expert committee, through emails, newsletters, LinkedIn posts, or QR codes in services. Compliance with the inclusion criteria was ensured by preliminary questions at the beginning of the questionnaire.
GAD-7 Test
Responding patients who received a referral proposal could optionally complete a GAD-7 test reference. The GAD-7 is an anxiety assessment tool that assigns a score from 0 to 21, where a score of 0 indicates no anxiety about their disease and 21 indicates severe anxiety.
Data Collection and Analysis
The data collection period for the qualitative and quantitative studies of patients and prescribers were conducted in parallel to ensure consistency and avoid temporal bias. Data processing and analysis were performed by IQVIA France, using Excel. Qualitative variables were presented as percentages and quantitative variables were analyzed as mean, standard deviation, median, minimum, and maximum.
Elaboration of Recommendations
To formulate recommendations aimed at overcoming the barriers to switching to biosimilars identified during the qualitative and quantitative studies, three discussion groups were organized from February to March 2024. These groups comprised prescribing physicians and patients in the therapeutic areas of gastroenterology and rheumatology. The discussion themes were established to examine the primary outcomes of both the qualitative and quantitative studies. These sessions allowed the collection of participants’ perspectives on the identified barriers and prompted discussions, on potential solutions. Subsequently, recommendations were formulated, refined and validated by the multidisciplinary expert committee.
Results
Respondent Characteristics
Qualitative Study
A total of 12 prescribing physicians participated in the qualitative phase. Among them, 42% (5/12) were gastroenterologists and 58% (7/12) were rheumatologists. A total of 14 patients participated in the qualitative study. Of these, 43% (6/14) were treated in gastroenterology and 57% (8/14) in rheumatology. Out of 14 patients interviewed about the switch proposal, 71% (10/14) accepted the switch and 7% (1/14) refused it. 21% (3/14) accepted the switch to a biosimilar but were subsequently treated again with the reference biologic. The additional characteristics of these participants are presented in Table 1.
 |
Table 1 Socio-Demographic Data and Characteristics of Respondents of the Qualitative Study |
Quantitative Study
A total of 100 prescribing physicians, equally divided between rheumatologists (50) and gastroenterologists (50), participated in the quantitative phase. Among them, 86% (86/100) worked exclusively in a hospital setting, while 8% (8/100) practiced in a community setting and 6% (6/100) had a mixed practice. The results of this study primarily focus on the responses of prescribers involved in implementing treatment switches from reference biologic to biosimilar. The additional characteristics of the participating prescribers are presented in Table 2.
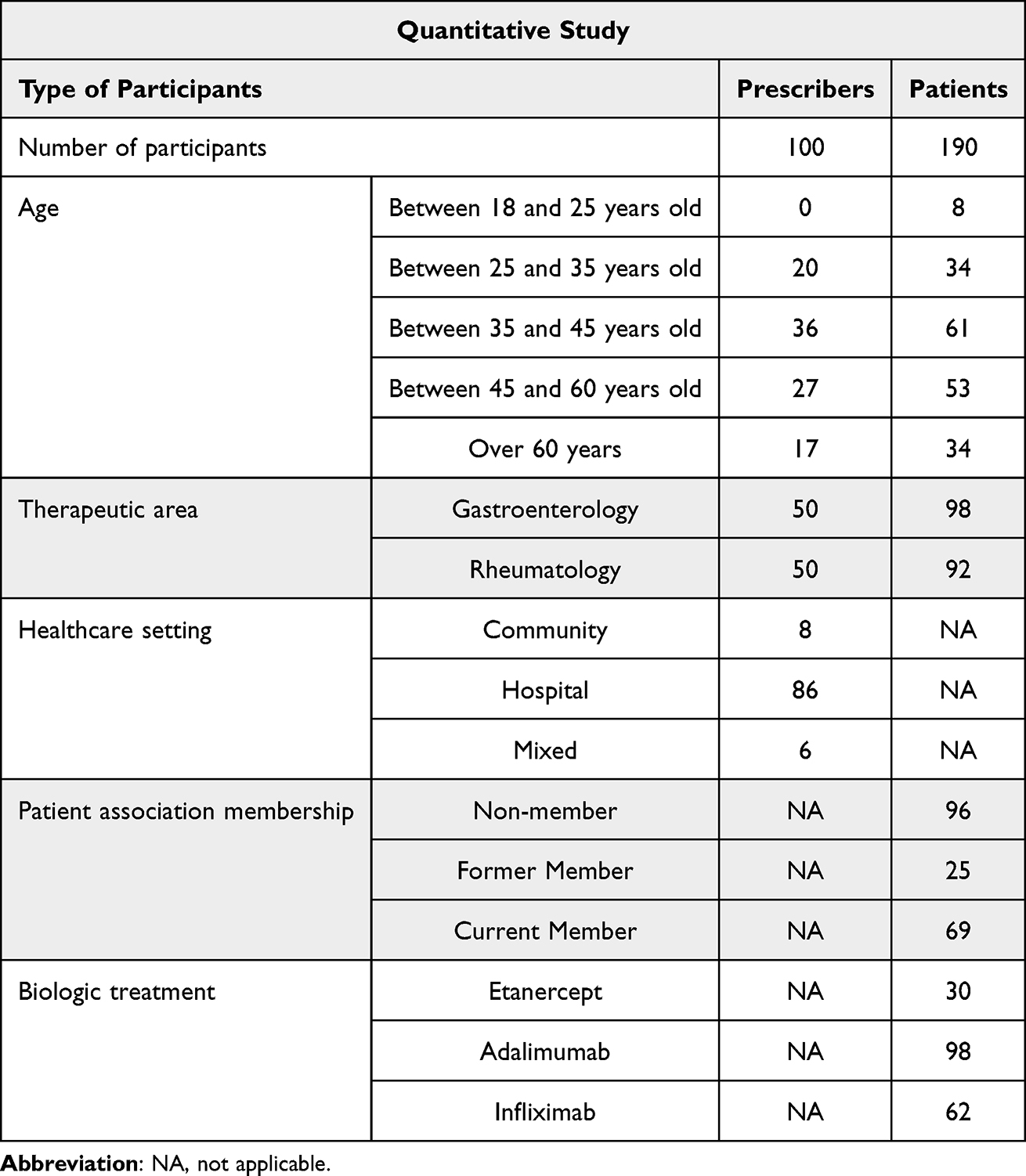 |
Table 2 Socio-Demographic Data and Characteristics of Respondents of the Quantitative Study |
Furthermore, a total of 190 patients participated in the quantitative study. Among them, 52% (98/190) were diagnosed with a gastrointestinal disease and 48% (92/190) with a rheumatic disease. The study results primarily rely on the responses of patients who received a proposal to switch from reference product to biosimilar (Figure 1). The additional characteristics of these participants are presented in Table 2.
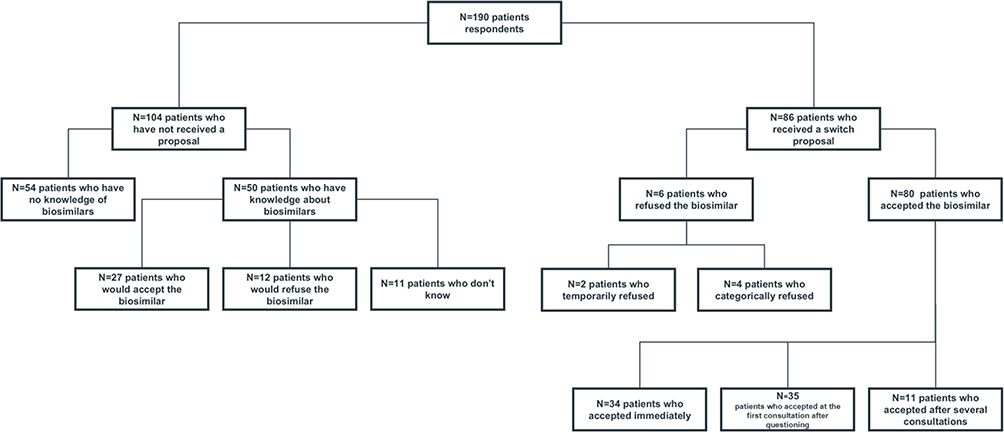 |
Figure 1 Sub-populations of patients according to questionnaire responses. |
Key Findings
The primary results of the study were categorized into three themes: 1) The relationship between the patient and the healthcare team, 2) The frequency of proposal and acceptance of the switch, and 3) The prescriber’s position regarding biosimilars and within the context of the proposal.
Relationship Between the Patient and Healthcare Team
During the qualitative interviews, patients were asked about the factors influencing their decision to accept the switch to a biosimilar. Half of the respondents (7/14) cited trust in their prescriber as a determining factor. Similarly, in the quantitative survey, prescribers were asked about the factors facilitating patient acceptance. Trust in the physician-patient relationship was the most frequently selected factor, reported by 54% of respondents (54/100). The second most common factor was having a stable disease activity, selected by 53% of prescribers (53/100) (Figure 2).
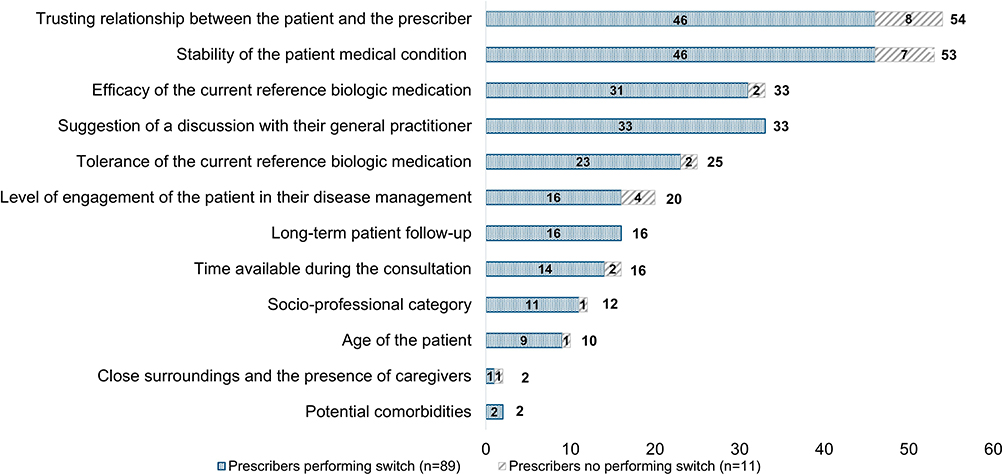 |
Figure 2 Factors that promote the acceptance of the switch according to prescribers. |
In the quantitative study, patients who accepted the switch to a biosimilar were also asked about the factors influencing their decision. Overall, 30% (24/80) identified feeling heard and supported as a determining factor (Figure 3).
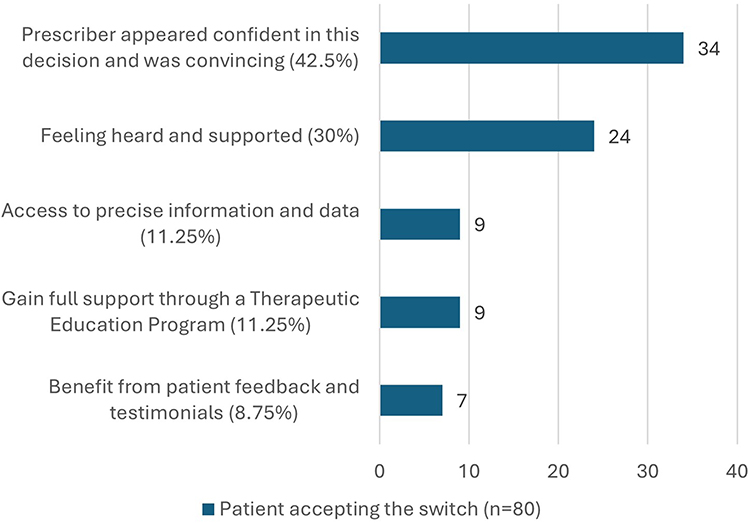 |
Figure 3 Factors that promote patient acceptance of switching to a biosimilar. |
To gain information about biosimilars, half of the patients in the qualitative study (7/14) indicated that the prescriber was their sole source of information, and the majority (9/14) identified the prescriber as one of their primary sources. Similarly, in the quantitative study, 51% (41/80) of patients who accepted the switch designated the prescriber as one of their main sources of information, reinforcing the findings of the qualitative survey (Figure 4).
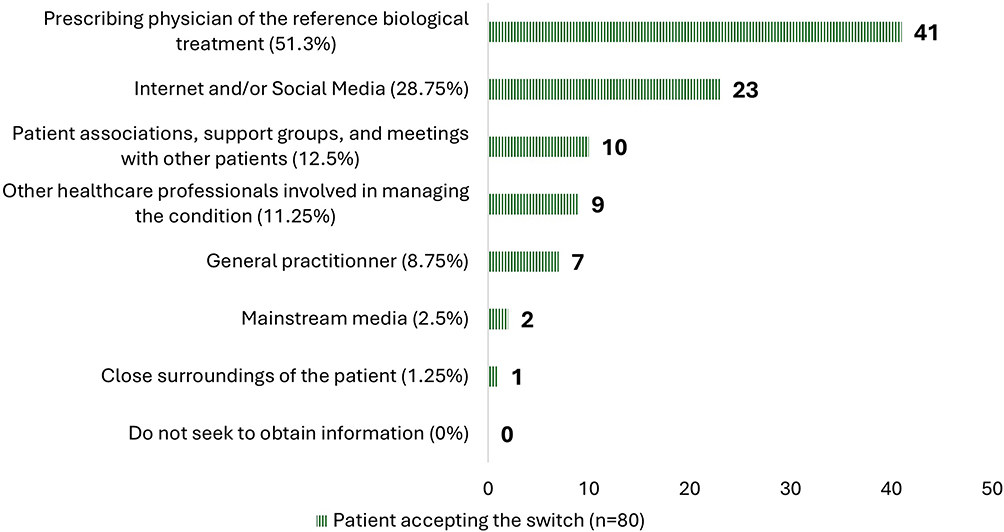 |
Figure 4 Sources of patient information about biosimilars. |
However, other healthcare professionals also played a role in providing information about biosimilars to patients. Among those who accepted to switch, 9% (7/80) identified their general practitioner, and 11% (9/80) reported other healthcare professionals involved in their care as primary sources of information (Figure 4). In the qualitative study, two prescribers considered that other healthcare professionals, particularly nurses and pharmacists, could also contribute to information dissemination and facilitate the acceptance of the proposal to switch.
During the interviews, one prescriber noted that the majority of community pharmacists did not have sufficient information to effectively inform patients about biosimilars. Similarly, some patients reported a lack of knowledge of biosimilars among community pharmacists, which hindered their ability to provide answers to their questions. Two prescribers also emphasized the importance of training other healthcare professionals in the care pathway, notably community pharmacists, to ensure the consistent transmission of accurate information beyond the hospital.
Patient associations were also frequently regarded by patients as sources of information. Among those patients who accepted to switch to a biosimilar, 12.5% (10/80) selected patient associations as one of their primary sources of information (Figure 4). During the interviews, several patients noted that sharing experiences from other patients could help facilitate the acceptance of the biosimilar. In the quantitative survey, 89 prescribers reported prescribing biosimilars through switching from the reference biologic. Thirty percent (27/89) of prescribers performing switch identified patient testimonials as a missing tool that could facilitate the acceptance of the switch (Figure 5).
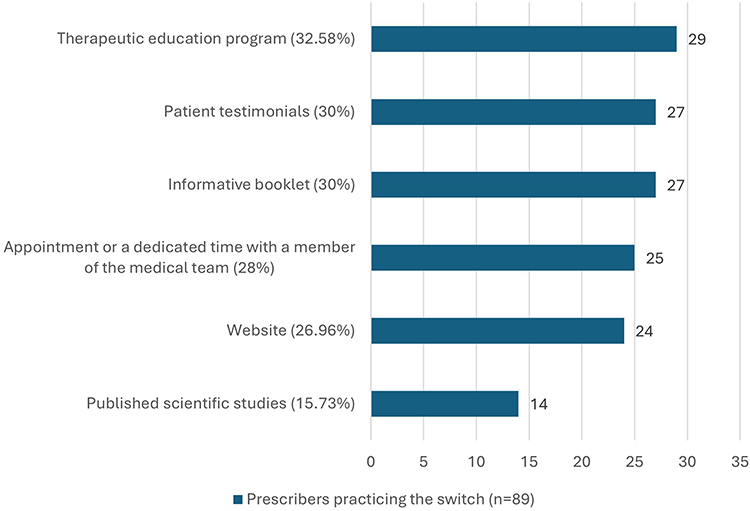 |
Figure 5 Missing tools identified by prescribers to support switching. |
The Frequency of Proposal and Acceptance of Switching from Reference Product to Biosimilar
Patient Response to the Switch Proposal
In the quantitative study, prescribers were asked how their patient reacted to the switch proposal. Each prescriber provided an estimate of the proportion of patients who accepted or refused to switch from reference biologic to a biosimilar, specifying whether acceptance was immediate, required additional information during the initial appointment, or several consultations. Similarly, refusals were categorized as potentially temporary or definitive. On average, prescribers who prescribe switches from reference product to biosimilar in their clinical practice (N=89) estimated that 82% of their patients accepted the switch: 40% immediately, 30% after asking questions, and 12% after several consultations. Among the 18% who refused, 8% were considered temporary refusals, while 10% were deemed categorical.
The patient acceptance rate for switching estimated by prescribers was slightly lower than that reported by the patients in the quantitative survey. Among the surveyed patients, 93% (80/86) indicated that they had accepted the switch, while 7% (6/86) had refused. Among those who accepted, 39.5% (34/86) did so immediately, 41% (35/86) after asking questions, and 13% (11/86) after several consultations. Among the patients who refused the biosimilar, 2% (2/86) indicated that their decision might change in the future.
Frequency of Switch Proposals
Among the 100 prescribers surveyed in the quantitative study, 89% (89/100) reported prescribing biosimilars through switching from the reference biologic. In contrast, 11% (11/100) indicated that they prescribe biosimilars only for biologic-naïve patients (initiation of biologic treatment) or in subsequent line therapy, but not through switching. Prescribers who practice switching were asked about the frequency with which they propose to switch from reference biologic to biosimilar to eligible patients. Only 33% (29/89) reported systematically proposing to switch to a biosimilar to eligible patients. Among the 67% (60/89) who did not always propose the switch, 28% (25/89) indicated that they rarely refrain from proposing it, 24% (21/89) occasionally refraining, 15% (13/89) stated that they often refrain, and 1% (1/89) reported very often refraining from proposing the switch.
Of the 190 patients who participated in the quantitative study, 55% (104/190) reported that they had never received a proposal to switch to a biosimilar.
Causes of Reluctance to Propose the Switch
Prescribers assessed the difficulty of using a biosimilar for patients who had already received a reference biologic treatment compared with treatment-naïve patients on biosimilars. This assessment was conducted using a five-point scale, where 1 indicated “the same level of effort”, and 5 represented an “extremely difficult” practice. Among the 100 prescribers surveyed, 67% (67/100) perceived switching to a biosimilar from the reference product as more challenging than prescribing in treatment-naïve patients. Among them, 43% (43/100) considered it slightly more difficult, 20% (20/100) rated it as quite difficult, and 4% (4/100) found it very difficult (Table 3). Conversely, 33% (33/100) of prescribers considered that switching required the same level of effort as prescribing biosimilars for treatment-naïve patients. Prescribers who do not practice switching (N=11) perceived the process as more challenging than others, assigning an average difficulty score of 2.5/5, compared to a score of 1.89/5 indicated by prescribers who practice switches. (Table 3).
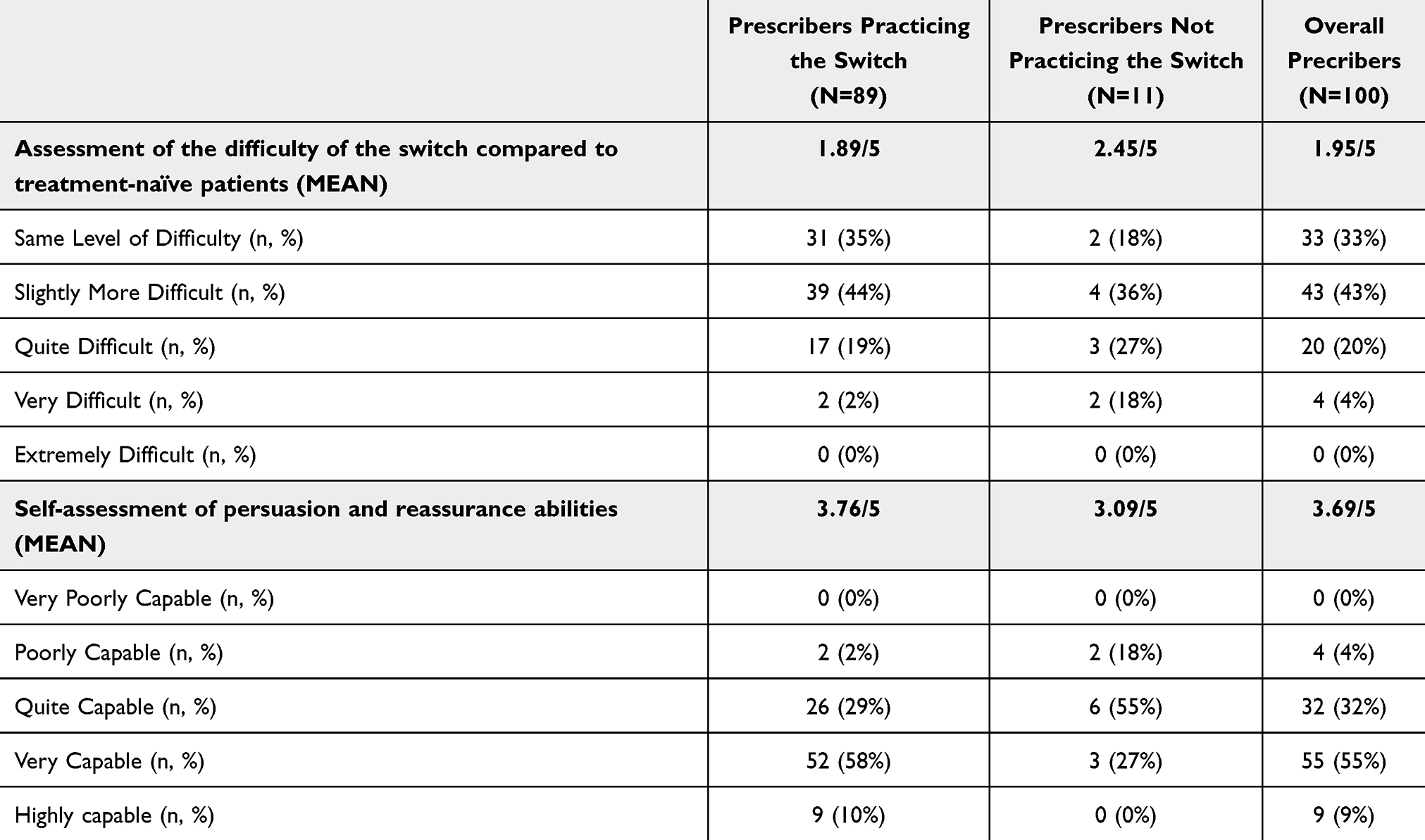 |
Table 3 Evaluation of the Difficulty of Switching to Biosimilars and Self-Assessment of the Ability to Convince Prescribers |
During the qualitative interviews, prescribers identified several factors contributing to their reluctance in proposing switches to biosimilars. One major obstacle was the limited duration of consultations, as the switch process was perceived as time-consuming and requiring significant discussion. Many prescribers reported prioritizing the medical follow-up of the patient during the consultations, often leaving insufficient time to introduce and offer to switch to a biosimilar. Additionally, some prescribers noted that patients with a long history of stable disease were more reluctant to change their treatment, further reducing the likelihood of accepting a switch proposal.
Another key barrier was patient anxiety, which prescribers perceived as negatively impacting willingness to switching. Indeed, 58% (7/12) of the interviewed prescribers identified anxious patients as the most resistant to the switch. This finding was reinforced by the quantitative survey, where 65% (65/100) of prescribers reported that patient anxiety was a significant factor reducing the likelihood of switch acceptance.
In the quantitative survey, 61 patients who received a proposal to switch agreed to take the optional GAD-7 anxiety test. Among the patients who accepted to switch, those who accepted immediately (26/61) had the highest mean anxiety score although it was still considered in the range of mild anxiety symptoms <10 (Table 4). Conversely, patients who accepted to switch after asking questions (25/61) had the lowest score (score <10) (Table 4). The sample of patients who refused to switch either temporarily (2/61) or categorically (3/61) was too small to allow for meaningful interpretation of their anxiety scores.
 |
Table 4 Patient’s Average GAD-7 Anxiety Score Based on Their Responses to Switch Proposal |
Prescribers’ Position on Biosimilars and Their Approach to Proposing the Switch from Reference Product
Prescribers’ Adoption of Biosimilars
In the quantitative study, 80 patients who accepted to switch from a reference biologic to a biosimilar were asked about the factors influencing their decision. The most frequently mentioned factor, chosen by 42.5% (34/80) of them, was the prescriber’s conviction in favor of biosimilars and the presentation of convincing arguments (Figure 3).
Prescribers assessed their level of knowledge about biosimilar medicines on a scale from 1 to 5, where 1 represented “low knowledge” and 5 indicated “extensive knowledge”. The mean score across all prescribers was 4.5/5, and 93% (93/100) of prescribers rated their knowledge as at least “good”. Despite this, four prescribers expressed the need for additional training on biosimilars, and three prescribers indicated a lack of documentation on biosimilars. Additionally, two prescribers voiced concerns about the evidence on efficacy of certain biosimilars, particularly regarding the use of indication extrapolated indications within their therapeutic area.
Communication and Trust in the Prescriber-Patient Relationship
In the quantitative study, prescribers were asked to evaluate their ability to convince and reassure patients about biosimilars on a scale from 1 to 5 where 1 indicated “very little” and 5 indicated “extremely capable”. The majority of prescribers, 64% (64/100) felt they were either very capable or extremely capable of reassuring their patients during the switch proposal. A further 32% (32/100) rated themselves as moderately capable, while 4% (4/100) felt less capable (Table 4). Prescribers who rated their convincing ability as good (3/5) or very good (4/5) were more likely to systematically propose biosimilars to their eligible patient population compared to the overall group (Table 5). This highlights the significant role of communication in fostering trust and facilitating the decision to switch to a biosimilar.
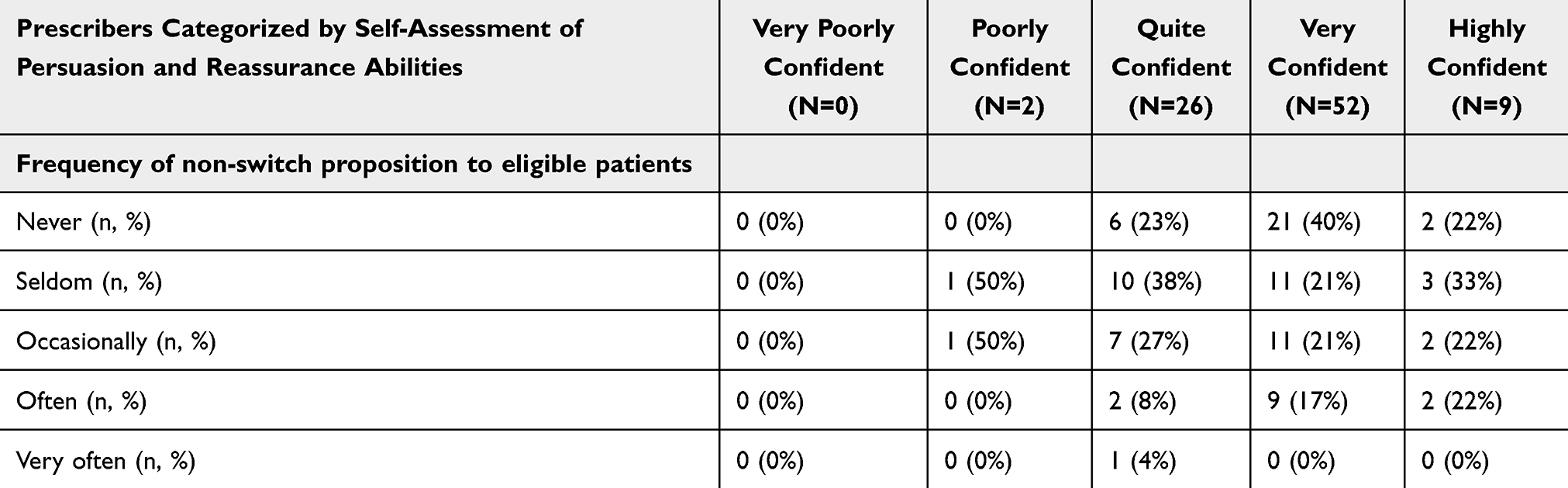 |
Table 5 Frequency of Non-Proposal of Switch of Eligible Patients According to Self-Assessment of Prescribers’ Persuasive Capacity |
Similarly, the 11 prescribers who do not practice switching patients from reference biologics to biosimilars rated their ability to convince and reassure patients at a lower level than the entire panel (3.1/5 compared to 3.8/5).
Furthermore, the quantitative study examined prescribers’ responses in cases where a patient refused the switch proposal. In this situation, 29% (26/89) of prescribers stated that they systematically repeat the proposal at the next consultation. 29% (26/89) indicated that they discontinued efforts to switch in such cases. 39% (35/89) indicated that they provide documentation or share additional information sources with the patient after a refusal (Figure 6).
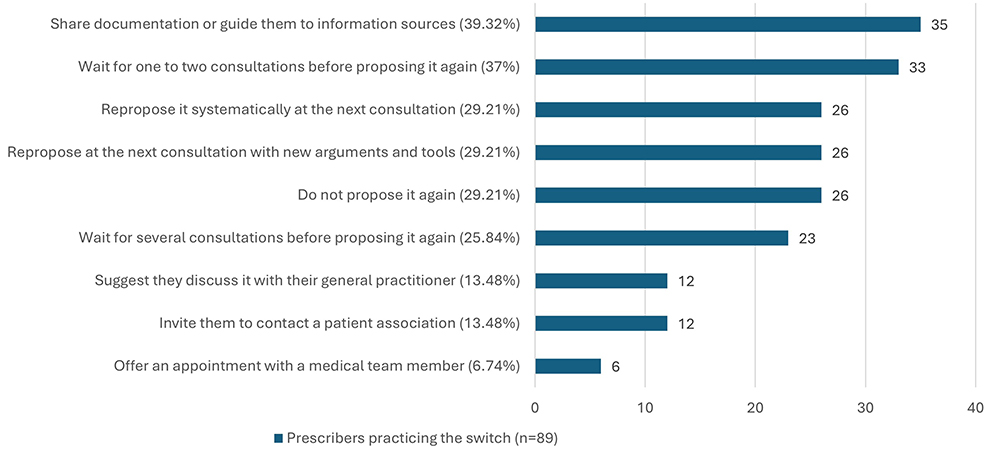 |
Figure 6 Prescriber reactions to rejection following the proposal switch to switch. |
Tools and Information to Support the Proposal to Switch
In the quantitative study, prescribers were asked about the main tools they rely on when proposing patients to switch from reference biologic to biosimilar. Among them, 60% (53/89) indicated that they provide brochures, 26% (23/89) encouraged participation in therapeutic education programs, and 22% (20/89) shared scientific studies as part of their approach.
Patients who agreed to switch were also questioned about their main sources of information. The internet and social media, selected by 29% (23/80), was the second most cited source (Figure 4).
In the qualitative study, both prescribers and patients were asked about the potential tools and measures that could facilitate patient acceptance. During the interviews, five patients expressed the need for written materials on biosimilars, such as brochures. Three patients indicated a desire for more detailed instructions on self-administration of the biosimilar treatment. One patient expressed the need for more digital content.
Discussion
Biologic medicines provide significant therapeutic benefits for patients, improving clinical outcomes, while stopping or delaying disease progression; however, their costs can be substantial. Biosimilars offer a more cost-effective alternative while maintaining comparable efficacy and safety to the reference biologic. Despite these advantages, the patient acceptance of switching from the reference product to the corresponding biosimilar remains a key challenge.13 Based on this analysis, supported by available literature, three strategic axes are recommended to improve patient acceptance and biosimilar adoption in a context of switching.
Implement a Structured Framework for the Prescription of Biosimilars
This study highlights the crucial role of prescribing physicians in facilitating patients to accept the switch to biosimilars. Evidence suggests that patients with a better understanding of biosimilars demonstrate higher adherence to these treatments.7 Given that prescribers serve as the primary source of information, it is essential that they provide clear, evidence-based, and convincing communication. Additionally, introducing a proposal to switch to a biosimilar within an established trust-based relationship fosters a more reassuring environment, which may enhance patient acceptance.7 To further optimize this process, prescribers should tailor their communication strategies to individual patient profiles,14 particularly by incorporating active listening techniques.
Despite the high overall acceptance rate among patients, the study reveals that only half of eligible patients receive a switch proposal. This suggest that the switching process is not yet fully integrated into routine clinical practice. Indeed, only one-third of prescribers systematically propose switching to eligible and stable patients. Time constraints during consultations, coupled with the absence of standardized protocols, appear to hinder the widespread adoption of this practice.11 Additionally, factors such as disease history, patient anxiety, and prescriber-related barriers may contribute to a reluctance to propose switching to biosimilars, even to patients who meet the eligibility criteria.
The analysis of the average GAD-7 anxiety scores indicates that mild anxiety is prevalent among patients,15 which can be attributed to the impact of their chronic condition on daily life.16 Nevertheless, the results reveal that patients who refuse the switch proposal do not exhibit higher anxiety scores than those who accept it. This finding suggests that prescribers may overestimate the influence of anxiety on patient’s decision and that anxiety may not be a significant barrier to biosimilar acceptance. Furthermore, more than half of the patients who have never been offered a switch indicate that they would accept it if proposed. This underscores the fact that the absence of a switch proposal to eligible patients represents a major barrier to the broader adoption of biosimilars.
The study highlights that over 10% of patients require multiple consultations to accept switching to a biosimilar. This reflects the need for time to gather information and reflect on their decision. For certain patient profiles, a gradual approach could be beneficial and should be systematically considered in cases of initial refusal. The concept of a biosimilar could be introduced during a first consultation, at the end of which the prescriber would provide documentation to the patient. The following consultation could allow addressing patient’s questions or concerns. The proposal to switch would be made at the end of this consultation, or during a third consultation if the patient needs further time to reflect. However, the study reveals that only half of the prescribers renew the proposal after an initial refusal. This means that half of the patients who require additional time may never receive another opportunity to reconsider the switch.
To bridge the gap between patient needs and prescriber practices, it is essential to implement a structured operational process for biosimilar switching. For community settings, a structured process would simplify the steps involved in proposing a switch, reducing its perceived complexity. By providing a clear framework or protocol, prescribers can be guided through the entire transition process, ensuring that eligible patients receive consistent well-structured communication about biosimilars. This comprehensive tool, designed for all healthcare professionals involved in the patient’s care pathway, should cover all stages of the switch proposal: identification of eligible patients, guidance on proposing the switch, and post-switch follow-up to ensure treatment adherence and address patients concerns.
A clearly defined protocol would ensure access to a system that provides a detailed list of followed patients, the nature of their current treatment, their eligibility for a treatment change, and the date of their next consultation. This systematic tracking of patients would help medical teams and private specialists to identify eligible patients and set up the most suitable approach for each profile before the consultation. This could allow, in some cases, an extension of the consultation duration, the adoption of an appropriate posture, a pre-interview with a hospital nurse, or the preparation of arguments and tools. In cases of refusal, notes could be recorded to adjust the physician’s approach in future visits or involve other team members and provide supporting materials between appointments. Post-consultation support should also be included, allowing patients to ask questions and express concerns. To implement this effectively, a biosimilar referent should be appointed to coordinate the process and serve as the main contact for community physicians and pharmacists. Monitoring a dashboard would help track the protocol’s impact.
A structured protocol for proposing to switch to a biosimilar was implemented and tested in the rheumatology department of Cochin Hospital between April 2019 and March 2020.17 This process involved the use of a pharmacy software to identify eligible patients, followed by telephone communication with these patients to propose a multidisciplinary consultation. During the consultation, patients first met with a care coordinator to assess the progression of their disease, followed by a meeting with a pharmacist who explained the concept of a biosimilar and initiated a discussion about a potential switch. Finally, the patient consulted with the rheumatologist, who would decide whether to propose the switch based on the reports provided by the care coordinator and pharmacist.
To evaluate the impact of this switching protocol, a retrospective study was conducted to compare a group of patients who participated in this multidisciplinary consultation with a control group who only consulted the rheumatologist. The results demonstrated a positive impact of this structured approach, with a switch rate of 69.4% (59/85) in the intervention group compared to 41.1% (23/56) in the control group.18
The successful implementation of this protocol encourages its replication. However, it is essential to ensure that this organizational approach can be adapted to the specific needs of each hospital department and private practice. The process may therefore vary depending on factors such as the size of the department or practice, the experience of healthcare professionals, available resources, and the current management of switch proposals.
Enhancing Knowledge and Awareness Among Healthcare Professionals and Patients on the Value of Biosimilars
Not all prescribers show the same level of initiative or confidence when proposing the switch to biosimilars, as some do not engage in this process. The analysis of the subpopulation of prescribers who never switch patients to biosimilars revealed a lower self-assessment of their ability to convince patients and greater perception of the challenges associated with this process.
A prescriber’s level of knowledge about biosimilars can significantly influence their approach to switching. Some prescribers show reluctance to use biosimilars, fearing a loss of efficacy, adverse events, or inferior quality, despite evidence confirming their equivalent efficacy and comparable pharmacokinetic, safety and immunogenicity profiles.8 Concerns about efficacy are partly driven by indication extrapolation. However, this reluctance may also stem from a lack of comprehensive knowledge about biosimilars, which can contribute to their hesitation.
The level of knowledge about biosimilars reported by prescribers in this study contrasts with findings from a previous French study conducted before the introduction of incentives for prescribing biosimilars.19,20 A 2015 study found that 55.2% of rheumatologists surveyed rated knowledge of biosimilars as low,9 whereas only 7% of prescribers in the COMPRENDRE study, including both rheumatologists and gastroenterologists, reported having limited knowledge. The available scientific evidence and successful experience with TNF inhibitors biosimilars in clinical practice over the years in rheumatology and gastroenterology may partially explain this difference. Nevertheless, the COMPRENDRE study results, the sample of prescribers consisted of only 8% of exclusively community practitioners, compared to 32.8% in the considered study. In that sense, prior to April 2024, the majority of biologic medicines had to be initially prescribed in the hospital,21 which allowed hospital prescribers to accumulate more experience with biologics – and by extension, biosimilars – compared to private prescribers. Considering that in 2023, 36% of gastroenterologists and 40% of rheumatologists practiced exclusively privately,22 the prescribers in this study might, on average, have better experience with biosimilars. Therefore, the average level of knowledge among prescribers in this study might be slightly higher than the national average.
Furthermore, healthcare professionals involved in the patient’s care pathway, particularly those practicing in the community such as pharmacists, general practitioners, and nurses among others, may not all be fully knowledgeable about biosimilars,10 limiting their ability to answer patients’ questions.8 However, ensuring consistent information conveyed to the patient throughout patient care, both in the community and in the hospital, is key to promoting patient acceptance. Therefore, it is crucial to ensure that all these healthcare professionals have access to clear and reliable information about biosimilars. To address these disparities in knowledge and ability to communicate the value of biosimilars, new tools could be developed to support healthcare professionals who need assistance with these aspects. These tools would compile reliable and compelling data on biosimilars, including scientific studies on their clinical value, economic benefits, and positive impacts on the healthcare system. Based on this information, clear and comprehensive support measures could be created and disseminated. These would equip healthcare professionals with the necessary responses to provide before, during, and after the proposal to switch. Such tools could improve prescribers’ understanding and confidence in biosimilars, particularly among private practitioners, and encourage them to initiate the switch more frequently and confidently.
To effectively disseminate this information, training programs for healthcare professionals, both hospital-based and private, could be implemented. These programs should be tailored to all stakeholders in the healthcare pathway, including nurses, general practitioners, and pharmacists. Such training sessions would raise awareness among all involved parties and create a reliable and functional source of information for patients. This could also support prescribers in improving their approach and the value arguments they present to patients during the switch proposal. This would improve their confidence in convincing patients while reducing the perceived challenges associated with the proposal. Patient associations could also leverage these training sessions to allow a biosimilar expert, identified within their organization, to enhance their knowledge and address questions beyond the strictly medical framework.
These training sessions can be delivered through various formats, including modules, symposia, seminars, or interactive workshops, and can be complemented by interactive digital tools to assist prescribers in the prescription of biologic treatments. Prioritizing young physicians for these sessions may be particularly relevant, as many may not have studied or experienced biosimilar switching during their academic training. Additionally, with the gradual expansion of therapeutic areas incorporating biosimilars, it is essential to extend this opportunity to specialists whose fields have recently adopted or are expected to adopt biosimilars. This would enable them to initiate the switch process more efficiently and with greater confidence. Finally, with the removal of the initial hospital prescription requirement in April 2024,20,21 it is essential to encourage private practitioners – who generally have less experience with biosimilars – to participate in these training sessions.
Improving Access to Reliable, Relevant, and Patient-Tailored Content Through a Multichannel Approach
A limited understanding of biosimilars among patients is often linked to increased concerns about their efficacy and safety,7 as well as confusion about the reasons for switching treatments. Providing clear and accurate information is therefore essential to fostering patient confidence and adherence to treatment. According to the COMPRENDRE study, addressing patients’ questions during consultations increases the likelihood of switch acceptance for more than half of the patients. To further support patient acceptance, it is important to dedicate time during consultations to answer their concerns and guide them toward reliable sources of information.
Providing patients with written materials during the switch proposal can enhance both the clarity and impact of the message.8 However, findings from the COMPRENDRE study suggest that this practice is not systematically adopted. While the prescriber remains a key source of information for most patients, they may also seek additional details outside of medical consultations, which are often infrequent and time limited. In these cases, patients may turn to online resources, patient associations, or other healthcare professionals in their care. However, community-based professionals (community pharmacists, general practitioners, and nurses, among others), often lack specialized training on biosimilars,10 making it difficult for them to provide accurate and consistent information. According to the COMPRENDRE study, patients rely more on the internet and social media than on non-prescribing healthcare professionals for information. Notably, those who conduct online research tend to develop more negative perceptions regarding the safety and efficacy of biosimilars.23
To reinforce patient adherence, it is important to provide accessible and reliable information beyond medical consultations. This can be achieved through trusted digital platform or websites, ensuring that patients receive clear, educational, and tailored content. Such resources not only offer reassurance but also empower patients by granting them access to verified information.
The use of educational tools is an integral part of the shared medical decision-making process.24 These tools help patients explore different treatment options and communicate their preferences to physicians,24 ultimately enhancing patient engagement in their treatment.24
Given the wide range of diseases treated with biologic treatments25 and the diverse patient population in terms of age and autonomy, it is essential to offer multiple communication channels tailored to individual needs. A combination of printed materials provided by healthcare professionals and digital resources can help a wider audience. Some content, such as informational websites or brochures, already exists but could be more widely disseminated. Digital tools, such as mobile applications17 or serious games,26 have already been tested in certain diseases to improve treatment understanding and disease management, demonstrating a positive impact on patient adherence.27 These resources address clinical and practical aspects of different biosimilars, but could also include patient testimonials, videos, and tutorials on the use of biosimilars.
Additionally, organizing through patient associations, in collaboration with healthcare professionals, could allow patients to feel supported and have access to reliable information on biosimilars outside the traditional medical setting. The goal of all these initiatives is to provide answers both before and after the switch proposal, ensuring that patients feel supported at every stage and addressing their main concerns.
Study Limitations
This study presents several limitations to consider when interpreting the results. It was conducted from June 2023 to January 2024. The experimental incentive on biosimilars in hospitals (Article 51) ended in late December 2022.19 On the other hand, the experiment of Amendment 9 on the prescription of biosimilars in the community, which began in January 2022, and ended in December 2024.26 These incentives aimed at changing prescriber practices may have influenced the study results.
The recruitment method resulted in a substantial proportion of patients – 49% (94/190) – being members or former members of patient associations. Additionally, the territorial distribution of patients was uneven, which could introduce a bias related to disparities in access to care and healthcare professionals.
The distribution of prescribers according to their mode of practice was very uneven, with only 8% practicing exclusively privately, which does not reflect the national distribution.22 Therefore, the generalization of the results to all prescribers in France should be done with caution.
Important to notice the study was carried out before the publication of the decree1 authorizing substitution by the dispensing pharmacist (Decree of 20 February 2025 establishing the list of similar biological groups that can be substituted by pharmacist and the conditions for substitution).
Conclusion
The COMPRENDRE study has identified key barriers to the acceptance of biosimilars when switching from a reference biologic in France. Currently, this process is not systematically implemented by prescribers, resulting in a limited number of switch proposals, despite a high rate of patient acceptance when offered. The identified barriers in the study allowed the expert committee to develop levers to bridge the gap and provide therapeutic education for patients and support physicians to adopt switches from reference biologic to biosimilar. The qualitative and quantitative studies highlighted that physicians perceive switching from reference biologic to its biosimilar more challenging than prescribing a biosimilar to treatment-naïve patients. The qualitative patient study identified patient trust in their physicians to significantly influence their acceptance to switch. This highlights the critical role of shared decision-making between prescribers and patients, which is built on a foundation of trust established with the treating specialist. This was corroborated in the quantitative study of patients which highlighted that the main source of information for patients was their physician. Even if this study suggests that patients would accept the switch if offered, only half of the eligible patients received a switch proposal. This study also indicates that the switching process is not yet fully integrated into routine clinical practice due to limited time during consultations and prescriber reluctance to propose a switch due to perceived patient anxiety about changes in therapy. The study shed light on the differences in perception between patients and doctors, as well as the gap that exists between the needs of patients and clinical practice. Implementing an organized and structured switch proposal protocol could help integrate this practice more consistently within the relevant services. Additionally, it would ensure that the proposal is tailored to the diverse profiles and needs of patients, promoting a more inclusive and effective approach.
The study highlighted that a large majority of physicians rate their level of knowledge about biosimilars as very good, whereas most patients have limited knowledge of biosimilars. One of the solutions proposed by the expert committee to improve patients’ knowledge of biosimilars is to widely disseminate information regarding biosimilars, to have a multi-channel approach through healthcare professionals, and to collaborate cross-functionally with patient associations. Training all healthcare professionals involved in the patient care pathway on biosimilars would facilitate a smoother switch process and enable them to provide consistent, reliable information to patients, both in hospital and community settings. Additionally, ensuring that patients have access to accurate and reliable information about biosimilars, even outside the clinical environment, is essential. A coordinated, cross-disciplinary approach involving different stakeholders is important to strengthen the switch process and enhance patient acceptance.
The recommendations from this study are relevant to all therapeutic areas utilizing biosimilars, particularly those where biosimilars have been recently introduced. These insights may help promote best practices and improve the overall adoption of biosimilars.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki.
In accordance with the French Jardé Law (Law No. 2012-300 of March 5, 2012, and Decree No. 2017-884 of May 9, 2017), this study does not fall under the category of research involving human subjects that requires ethical review or informed consent. The study did not involve any interventional procedures, collection of sensitive personal data, or biological sampling, and therefore was not subject to approval by a research ethics committee.
Acknowledgments
The authors would like to thank the patients and physicians who participated in this survey. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published. Biogen and IQVIA France reviewed the article for medical accuracy and provided feedback to the authors.
Funding
This study was organized by IQVIA France and funded by Biogen France SAS. This article was funded by Biogen France.
Disclosure
Cécile Gaujoux-Viala reports serving as a consultant and on a speaker’s bureau for AbbVie, Alfasigma, Amgen, Biogen, Biocon, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion HealthCare, Chugai, Eli Lilly, Fresenius Kabi, Galapagos, Gilead, Janssen, Medac, Merck-Serono, Mylan, Nordic Pharma, Novartis, Pfizer, Sandoz, Sanofi, UCB and Viatrix. Sonia Tropé is employee of an organization receiving sponsorship from Abbvie, Amgen, Allfa Sigma, Galapagos, Bristol-Myers Squibb, Celltrion, Biogen, Boehringer,Lilly, Fresenius Kabi, Nordic, Chugai, Pfizer, outside the submitted work. Anne Buisson is member of an organization sponsored by AbbVie, Adacyte, Amgen, Alfasigma, Biogen, Celltrion, Ferring, Janssen, Eli Lilly, MSD, Nordic Pharma, Pfizer, Pilèje, Sandoz, Takeda and Tillots Pharma. Emeric Languérand reports personal fees from IQVIA. Laura Cordurié is employee of IQVIA France and may hold company stock. Géraldine Margulies is employee of Biogen France and may hold company stock or stock options. Oliver Vittecoq has received research funding, consulting, speaker fee, and sponsorship from Bristol Myers-Squibb, AbbVie, Galapagos, Alfasigma, Janssen, Biocon Biologics, Biogen, Sandoz, Novartis, Pfizer, UCB, MSD, Eli Lilly, Medac, Roche and Viatris. Catherine Le Berre reports personal fees from Abbvie, Amgen, Celltrion, Ferring, Fresenius Kabi, Galapagos, Janssen, Lilly, MSD, Nordic Pharma, Pfizer, Takeda, outside the submitted work. The remaining authors have no conflicts of interest in this work.
References
1. Assurance Maladie. Définition et caractéristiques des médicaments biosimilaires. 2024. Available from: https://www.ameli.fr/paris/etablissement/exercice-professionnel/prescriptions/medicaments-biosimilaires/definition-et-caracteristiques.
2. Troein P, Newton M, Stoddart K, Arias A. The Impact of Biosimilar Competition in Europe. Available from: https://www.iqvia.com/-/media/iqvia/pdfs/library/white-papers/the-impact-of-biosimilar-competition-in-europe-2022.pdf.
3. Jourdain H, Hoisnard L, Sbidian E, Zureik M. Persistence and safety of anti-TNF biosimilars versus originators in immune-mediated inflammatory diseases: an observational study on the French National Health Data System. RMD Open. 2024;10(1):e003531. doi:10.1136/rmdopen-2023-003531
4. Jourdain H, Hoisnard L, Sbidian E, Zureik M. TNF-alpha inhibitors biosimilar use in France: a nationwide population-based study using the French National Health Data System. Sci Rep. 2022;12(1):19569. doi:10.1038/s41598-022-24050-7
5. Améliorer La Qualité Du Systéme De Santé Et Maîtriser Les Dépenses, Propositions de l’Assurance Maladie pour 2025. 2024. Available from: https://www.assurance-maladie.ameli.fr/sites/default/files/2024-07_rapport-propositions-pour-2025_assurance-maladie.pdf.
6. Sigaux J, Semerano L, Boissier MC. Faut-il substituer un traitement en cours par un biosimilaire coûte que coûte ? Rev Rhum. 2019;86(1):1–4. doi:10.1016/j.rhum.2018.09.004
7. Frantzen L, Cohen JD, Tropé S, et al. Patients’ information and perspectives on biosimilars in rheumatology: a French nation-wide survey. Joint Bone Spine. 2019;86(4):491–496. doi:10.1016/j.jbspin.2019.01.001
8. Scherlinger M, Pellegrin JL, Germain V, Lazaro E, Duffau P, Schaeverbeke T. Les biosimilaires en France, bien en comprendre les enjeux pour bien les utiliser. Rev Médecine Interne. 2019;40(1):5–8.
9. Beck M, Michel B, Rybarczyk-Vigouret MC, et al. Rheumatologists’ perceptions of biosimilar medicines prescription: findings from a french web-based survey. BioDrugs. 2016;30(6):585–592. doi:10.1007/s40259-016-0202-5
10. Beck M, Michel B, Rybarczyk-Vigouret MC, et al. Knowledge, behaviors and practices of community and hospital pharmacists towards biosimilar medicines: results of a French web-based survey. mAbs. 2017;9(2):384–391. doi:10.1080/19420862.2016.1267087
11. Cohen JD, Tropé S, Paubel P, Munos A, Bocquet F. Preconceived notions about biosimilars—a French experience. Clin Rheumatol. 2020;39(8):2251–2254. doi:10.1007/s10067-020-05229-7
12. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
13. Jourdain H, Hoisnard L, Weill A, Sbidian E, Zureik M. Utilisation Des Biosimilaires Des Anti-Tnf-Alpha En France: Une Étude À Partir Des Données Du SNDS. Annales de Dermatologie et de Vénéréologie-FMC. 2022;2:A266–7.
14. Gasteiger C, Jones ASK, Kleinstäuber M, et al. Effects of message framing on patients’ perceptions and willingness to change to a biosimilar in a hypothetical drug switch. Arthritis Care Res. 2020;72(9):1323–1330. doi:10.1002/acr.24012
15. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092. doi:10.1001/archinte.166.10.1092
16. Scott AJ, Correa AB, Bisby MA, Dear BF. Depression and anxiety trajectories in chronic disease: a systematic review and meta-analysis. Psychother Psychosom. 2023;92(4):227–242. doi:10.1159/000533263
17. Belo-Kibabu S, Bottois C, Dumas S, et al. Mise en place de consultations pluridisciplinaires pour des patients atteints de rhumatisme inflammatoire chronique et traités par biothérapie sous-cutanée: bilan à un an et perspectives. Ann Pharm Fr. 2023;81(2):370–379. doi:10.1016/j.pharma.2022.08.011
18. Levivien C, López Medina C, Bottois C, et al. Impact of a clinical pharmacist in a multidisciplinary consultation on the switch to a biosimilar for inflammatory rheumatic diseases. Joint Bone Spine. 2022;89(3):105322. doi:10.1016/j.jbspin.2021.105322
19. Maladie A. Dispositif d’intéressement à la prescription de médicaments biosimilaires: ce qu’il faut savoir. 2024. Available From: https://www.ameli.fr/paris/medecin/exercice-liberal/facturation-remuneration/dispositif-interessement-prescription-biosimilaires.
20. de la Santé Et de la Prévention M. Rapport au parlement 2022 sur les expérimentations innovantes en santé, Article 51 de la loi de financement de la sécurité sociale pour 2018. Available from: https://sante.gouv.fr/IMG/pdf/rapport_parlement_article_51_2022.pdf#:~:text=du%20syst%C3%A8me%20de%20sant%C3%A9%20post-Covid,%20les%20exp%C3%A9rimentations%20article.
21. ANSM. Modification des conditions de prescription et de délivrance de certaines biothérapies utilisées dans le traitement de maladies inflammatoires chroniques. 2024. Available from: https://ansm.sante.fr/actualites/modification-des-conditions-de-prescription-et-de-delivrance-de-certaines-biotherapies-utilisees-dans-le-traitement-de-maladies-inflammatoires-chroniques.
22. DREES. Démographie des professionnels de santé en 2023 par spécialité et mode d’exercice; 2023.
23. Gasteiger C, Lobo M, Dalbeth N, Petrie KJ. Patients’ beliefs and behaviours are associated with perceptions of safety and concerns in a hypothetical biosimilar switch. Rheumatol Int. 2021;41(1):163–171. doi:10.1007/s00296-020-04576-7
24. Elwyn G, Laitner S, Coulter A, Walker E, Watson P, Thomson R. Implementing shared decision making in the NHS. BMJ. 2010;341(oct14 2):c5146. doi:10.1136/bmj.c5146
25. Maladie A. Tout savoir sur les biothérapies. 2024. Available from: https://www.ameli.fr/paris/assure/sante/medicaments/comprendre-les-differents-medicaments/tout-savoir-sur-les-biotherapies#:~:text=Les%20bioth%C3%A9rapies%20sont%20des%20traitements%20utilisant%20des#:~:text=Les%20bioth%C3%A9rapies%20sont%20des%20traitements%20utilisant%20des.
26. Maurin KD, Girod C, Consolini JL, et al. Use of a serious game to strengthen medication adherence in euthymic patients with bipolar disorder following a psychoeducational programme: a randomized controlled trial. J Affect Disord. 2020;262:182–188. doi:10.1016/j.jad.2019.10.008
27. Magnol M, Eleonore B, Claire R, et al. Use of eHealth by patients with rheumatoid arthritis: observational, cross-sectional, multicenter study. J Med Internet Res. 2021;23(1):e19998.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Therapeutic Potential of Tralokinumab in the Treatment of Atopic Dermatitis: A Review on the Emerging Clinical Data
Kelly KA, Perche PO, Feldman SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1037-1043
Published Date: 3 June 2022