Back to Journals » OncoTargets and Therapy » Volume 12
The surgical perspective in precision treatment of diffuse gliomas
Authors Thon N, Tonn JC, Kreth FW
Received 16 May 2018
Accepted for publication 10 January 2019
Published 22 February 2019 Volume 2019:12 Pages 1497—1508
DOI https://doi.org/10.2147/OTT.S174316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Niklas Thon, Joerg-Christian Tonn, Friedrich-Wilhelm Kreth
Department of Neurosurgery, Ludwig-Maximilians-University Munich, Munich, Germany
Abstract: Over the last decade, advances in molecular and imaging-based biomarkers have induced a more versatile diagnostic classification and prognostic evaluation of glioma patients. This, in combination with a growing therapeutic armamentarium, enables increasingly individualized, risk-benefit-optimized treatment strategies. This path to precision medicine in glioma patients requires surgical procedures to be reassessed within multidimensional management considerations. This article attempts to integrate the surgical intervention into a dynamic network of versatile diagnostic characterization, prognostic assessment, and multimodal treatment options in the light of the latest 2016 World Health Organization (WHO) classification of diffuse brain tumors, WHO grade II, III, and IV. Special focus is set on surgical aspects such as resectability, extent of resection, and targeted surgical strategies including minimal invasive stereotactic biopsy procedures, convection enhanced delivery, and photodynamic therapy. Moreover, the influence of recent advances in radiomics/radiogenimics on the process of surgical decision-making will be touched.
Keywords: extent of resection, biomarker, metabolic imaging, molecular markers, personalized medicine, precision medicine, prognosis, stereotactic biopsy, cytoreductive surgery
Introduction
Diffuse gliomas make up about 80% of all malignant brain tumors with World Health Organization (WHO) grade IV glioblastoma being the most common and most aggressive tumor entity.1,2 The different WHO grades refer to the degree of malignant behavior and associated prognosis. Clinical outcome is highly variable and ranges from years of stable tumor formations to a rapid progression and fatal course, despite aggressive treatment.3 Notably, even “benign” grade II tumors are an incurable chronic disease; in here, malignant progression toward anaplastic glioma or glioblastoma represents the pivotal event in prognosis. Clinical complaints depend on the tumors size and localization, growth rate, degree of infiltration, and proximity of eloquent brain areas. A slow tumor growth frequently becomes symptomatic with epileptic seizures, whereas patients with fast growing tumors show acute deficits and a rapid clinical deterioration.4
Due to the increasing complexity of management algorithms, patients should be referred to specialized brain tumor centers with high case load, whose interdisciplinary team consists of experienced neurosurgeons, neurologists, medical and radiation oncologists, neuropathologists, neuroradiologists, palliative physicians, and specialized psycho-oncological care. Initial diagnosis is routinely based on magnetic resonance imaging (MRI), which is increasingly being supplemented by anatomical, functional, and metabolic imaging data in terms of differential diagnosis, identification of intratumoral heterogeneity, determination of tumor extension and spatial relation to function-relevant brain areas, and monitoring of the course of disease. Treatment considerations are based on clinical characteristics, conventional prognostic factors, and an increasing number of molecular, metabolic, and imaging biomarkers to fit tumor profiles to available treatment concepts, which should be adjusted each for its risk and possible benefit. Surgery, radiotherapy (RT), chemotherapy, and any combination thereof are the most important tumor-specific treatment modalities.
The neurosurgeon usually initiates the multidisciplinary treatment cascade. First, the question of open resection is evaluated. Imaging-defined complete resections improve outcome in glioma patients. The prognostic impact of complete resections may also to be seen in the relapse situation.5,6 The neurosurgeon must be aware, however, that total tumor removal cannot be achieved in the clear majority of patients, due to the highly infiltrative nature of the disease. Alternative options include biopsy procedures in high-risk patients which may occasionally be combined with sophisticated local treatment methods such as interstitial brachytherapy or photodynamic therapy for highly selected cases. As total tumor removal/local control does not exist, additional therapies are needed. Percutaneous RT plays a central role in glioma therapy. Over the past decade, significant advances in RT treatment and image-guidance technology have led to enormous improvements in the ability to optimize definitive and salvage treatment including re-irradiation protocols. An accurate and precise delineation of treatment volumes by molecular imaging in combination with conformal radiation strategies considering both the more or less heterogeneous composition of the disease and its relation to eloquent brain areas and neurovascular structures can be regarded as the hallmarks of modern RT.7 Systemic chemotherapy is of central importance at the time of first diagnosis and during the course of disease.8–10 Future protocols may be stratified according to the individual molecular characteristics (such as the protocol of the CeTeG-trial for O6-methylguanine-DNA-methyltransferase (MGMT) promoter methylated glioblastoma).11 Moreover, there is an increasing pursuit of targeted and immunomodulatory approaches, particularly in case of recurrent disease after conventional treatment.12 Tumor-treating fields (TTF) is a recently approved novel treatment modality that is referred to as the fourth modality of glioblastoma treatment.13 TTF is an antimitotic treatment modality that interferes with glioblastoma cell division and organelle assembly by delivering low-intensity (1–3 V/cm) intermediate frequency (200 kHz) alternating electrical fields to the tumor, which results in a significant improvement in progression-free survival and overall survival in glioblastoma patients with low treatment-associated side-effects.14 Last but not least, early psycho-oncological attendance and palliative care may additionally ameliorate the course of the disease.15 The overarching goals are to improve clinical prognosis while preserving the patients’ quality-of-life as long as possible which should also critically determine the activity of the neurosurgeon. This article aims to position the surgical procedures into this increasingly complex management of diffuse gliomas and to consolidate the neurosurgical perspective as an important component in a multidisciplinary treatment algorithm.
Classification of diffuse gliomas
According to the revised 2016 WHO classification of central nervous system tumors, diffuse gliomas are being categorized by integrated diagnoses considering both genetic and histological findings.2,4 A hierarchical structure of molecular biomarkers, namely the mutational status of the genes encoding the isocitrate dehydrogenasis (IDH) and loss of heterozygosity (LOH) on chromosomes 1 p and 19q (LOH 1 p/19q), have gained a powerful impact on both tumor classification and prognosis of the disease. 1 p/19q co-deleted IDH mutant tumors do better than IDH mutant tumors without LOH 1 p/19q, and IDH wildtype tumors bear the worst prognosis.16 The determination of the 1 p/19q chromosomal status sustainably has overcome uncertainties in the diagnosis of oligodendroglial tumors: an oligodendroglioma can now only be diagnosed in the case of a 1 p/19q co-deletion, whereas astrocytomas (typically harboring a loss of the histone chaparone protein ATRX) represent the glioma subgroup lacking this co-deletion.17,18 The new integrated diagnoses reflect the fact that prognosis depends primarily on molecular biomarkers and only secondarily on WHO grading. This also includes determination of the promoter methylation status of the gene encoding for the MGMT as it indicates a better response to alkylating chemotherapy and may serve as a basis for treatment decisions in selected patients with low- and high-grade gliomas.19–21 Moreover, mutations in the telomerase reverse transcriptase (TERT) have recently raised attention as important molecular events in IDH wildtype gliomas: It has been shown, for example, that IDH wildtype gliomas formally graded as WHO grade II, have glioblastoma-like characteristics in case of an additional TERT mutation.4,16,22 H3-K27 mutated midline gliomas represent a new aggressive subgroup of grade IV tumors, which frequently occur in the thalamus or brain stem area. Historically, a considerable number of these tumors had been grouped among low-grade brainstem gliomas. In summary, the introduction of integrated diagnoses in the revised WHO classification scheme has diminished diagnostic uncertainties, allows improved assessing of the prognosis, and provides a new basis for personalized treatment concepts. A representative viable tumor tissue sampling process (ie, avoidance of necrotic tissue samples) either by biopsy or resection is a prerequisite for proper molecular-genetic classification to avoid false negative results.23–25
Conventional and advanced glioma imaging
Magnetic resonance imaging (MRI) is the gold standard for diagnosis, characterization, and clinical management.26 Radiological findings in conventional MRI that can be indicative of a high-grade glioma include a bilateral pattern of growth, undefined margins with perifocal edema, mixed signal intensity, and significant contrast enhancement. However, a malignant phenotype must also be taken into account in non-enhancing lesions without pronounced edema.27,28 Determination of true tumor extensions can be challenging as single tumor cells invade into the surrounding brain tissue far beyond MRI-defined tumor margins.29 Particularly in non-enhancing lesions with a diffuse extension in FLAIR/ T2-weighted sequences, an extensive tumor cell spread, ie, along the U-fibers into the surrounding brain tissue, can be expected.30–33 In these patients, the benefit-risk profile should be critically assessed with regard to the surgical strategy, as complete resection is rarely achieved.30 In malignant gliomas the spatial extent is routinely defined by contrast enhancement in T1-weighted sequences. Signal alterations on T2-weighted sequences, however, can indicate tumor infiltration beyond contrast-enhancing tumor parts. This particularly concerns IDH mutant high-grade gliomas.34
Recent advances in radiomics/-genomics appear to offer a nearly limitless supply of potential imaging biomarkers that could support the suspected tumor diagnosis and the assessment of both prognosis and treatment response.35–40 Using large-scale data characterization algorithms and deep-learning methods, imaging based information might assess the patients’ individual prognosis (radiomics) and allow the prediction of distinct molecular-genetic textures (radiogenomics). Attention must be paid, however, that independent validation remains a concern. Hence, the quality of information should be ensured, eg, by blinded, preferably automatized imaging analyses.
Even though current data are immature and obtained mainly from retrospective analyses, interesting aspects have been described and may already be considered with respect to differential diagnosis, prognosis, and the process of surgical decision-making. For example, radiomic analyses have been shown to predict overall survival from baseline T1-weighted contrast-enhanced MRI in glioblastoma patients.41 Radiogenomic analyses suggest that IDH mutant grade II or III tumors tend to grow within a single lobe, are rarely found in deep-seated locations, are likely to have sharp tumor margins, a homogeneous signal intensity, and less contrast enhancement as compared to their IDH wildtype counterparts.42 The rare subgroup of IDH wildtype grade II gliomas are predominantly seen in the fronto-temporo-insular region presenting with larger tumor volumes as compared to IDH mutant grade II astrocytomas.43 IDH wildtype grade III and IV gliomas share poorly defined margins, mixed signal intensity, and pronounced enhancement.44 In IDH mutant high-grade gliomas, the tumor infiltration may be better visualized by T2-weighted sequences. The size of the hyperintense infiltration zone frequently extends beyond the contrast-enhanced tumor parts of the enhanced T1-weighted images.34 These data suggest a link between operative resectability of high-grade gliomas and the IDH mutation status: IDH mutant malignant gliomas seem to more often be suitable candidates for a gross total resection because of their relative sharp delineation on MRI. 1 p/19q co-deleted (oligo) tumors usually grow as well demarcated, sometimes cystic and/or calcified lesions in lobar location, which makes them more amenable for complete resection.45 Ill-defined tumor margins and intratumoral signal heterogeneity may indicate a worse prognosis in 1 p/19q co-deleted gliomas.46 Regarding the MGMT methylation status, only a few data in radiogenomic analyses have been described so far.44,45 Some ill-defined tumor margins may be seen more frequently in methylated glioblastomas.47 Other authors describe that MGMT unmethylated glioblastomas have a smaller volume on both T1-contrast enhanced and T2-FLAIR images than their methylated counterparts.48 The extent of perifocal edema seems to stratify survival in MGMT promoter methylated (but not in unmethylated) glioblastomas: patients with methylated tumors with little or no edema may exhibit particularly long survival.44 Supervised machine learning of MRI texture features might be used to predict MGMT methylation status in glioblastoma patients.45,49,50 Further genes potentially found to be correlated with respective imaging phenotypes in quantitative MRI analyses include EGFR, VEGF, PDGF, TP53, and PTEN.40,48,51 Transcriptomics, correlating transcriptome patterns with imaging features, revealed that glioblastomas exhibiting the proneural gene expression subtype most frequently occur in the frontal lobe.48 Zinn et al52 correlated imaging features with data from The Cancer Genome Atlas and found that tumors with high T2-/FLAIR volumes were enriched with genes and miRNAs involved in cellular migration and invasion and are associated with rapid tumor progression and short survival.
Over the last years, advanced imaging modalities such as MR spectroscopy, MR perfusion analysis, and amino acid positron emission tomography (PET) have been shown to improve diagnostic accuracy and are increasingly used for non-invasive glioma evaluation.33,53–56 These techniques can improve differential diagnosis and may detect infiltrative tumor tissue beyond conventional MRI-defined borders indicating “true” biological tumor volumes.57–59 They can be used to identify intratumoral heterogeneity, particularly in suspected low-grade gliomas, which gains impact for both biopsy planning and resective treatment.28,57,60,61 Moreover, earlier detection and a more precise characterization of glioma recurrence and their differentiation from pseudo-progression has been reported to be achieved using these advanced imaging techniques.62 MR spectroscopy might be useful for preoperative detection of IDH mutant gliomas.63,64 Correlations between apparent diffusion coefficient in diffusion-weighted imaging and the presence of MGMT promoter methylation seem to exist.65 The pattern of intratumoral radio tracer uptake in dynamic 18F-FET PET in non-enhancing gliomas has been found to be associated with both the IDH mutational and 1 p/19q co-deletion status.27,28 Evolving prospective data support the usefulness of dynamic 18F-FET PET as an imaging biomarker in suspected low-grade gliomas. In glioblastomas, the size of the biological tumor volume before RT as described by 18F-FET PET has been shown to be inversely correlated with the prognosis.28,59 The place of advanced imaging modalities within the framework of the prognostic evaluation and treatment decision process of gliomas must be further elucidated in future prospective studies. Up to now, radiomics/-genomics cannot be used as a substitute for molecular analyses of tumor tissue samples, and it is too early to announce guidelines for their use in everyday clinical practice.
The place of tumor resection and minimal-invasive biopsy in diffuse gliomas
Open tumor resection is recommended as the first step in the treatment of diffuse gliomas WHO grade II, III, and IV.10,66 At population level, prognostic favorable complete resection is achieved in about 40%–75% of surgical cases.4,8,67–75 In a selected series higher, complete resection rates might be observed.76 Still, there is a discrepancy between the number of patients selected for complete resection and the number of those for whom this goal has been achieved. It still remains true that the majority of patients selected for gross total surgery received an incomplete resection. Biopsy instead of resection is a relatively seldom used surgical strategy in glioma treatment concepts: in only 10%–20% of the patients, the glioma diagnosis has been obtained by open/stereotactic biopsy procedures alone.69,72 These figures derive from a rather conventional concept reserving biopsy procedures only for high-risk patients (older age, poor clinical condition, significant co-morbidity, deep-seated/eloquent tumor locations, such as the basal ganglia or brain stem). Due to the immanent poor clinical performance status and unfavorable prognostic profile, biopsied patients frequently undergo less invasive treatment regimens and are commonly excluded from large randomized controlled trials.10,77,78 However, recently published data have pointed out that biopsy only is a useful tool in not safely resectable high-grade glioma patients, even in the case of good clinical performance scores and low co-morbidity and not associated with a worse prognosis as compared to incomplete resections. Side-effects of the biopsy, however, were significantly seen less often than after incomplete resection.69,79,80 These data should be reconsidered indications in favor of biopsy in the case of not safely resectable tumors and to avoid therapeutic nihilism.
The challenge of accurate tissue sampling
An overriding goal of any surgical strategy is to obtain representative tissue samples for detailed histological and molecular genetic examination. In specialized neuro-oncological centers, a comprehensive neuropathological evaluation can routinely be obtained, even from tumor specimens which may be as small as the head of a match.24 In the majority of cases, tissue samples derive from open tumor resections or – if not safely feasible – from (stereotactic) biopsy procedures.81 Both microsurgical and stereotactic neurosurgeons have to ensure that tissue samples have been harvested from the biologically most active and prognostically most relevant parts of the tumor.28,82 The implementation of advanced functional and metabolic imaging data for the navigated precise tissue sampling procedure, minimizes the risk of undergrading, misdiagnosis, and undertreatment of heterogeneously composed gliomas.28,60 The fact that the so far clinically relevant molecular biomarker profiles do not differ throughout the tumor volume (as shown for the IDH, 1 p/19q, and MGMT status) shows that the risk of molecular-genetic misclassification is relatively low.23,25,28,83 However, contamination of the samples by a significant amount of necrotic and/or non-neoplastic tissue could easily result in false negative results. Thus, the selection of viable tumor tissue samples is a prerequisite for valid determination of the molecular-genetic profile of the glioma under consideration.23
Resectability
Any decision in favor of cytoreductive surgery should be based on a thorough assessment of the resectability, the associated risk profile, and the oncological benefit, considering both the individual prognosis and the therapeutic network, including alternative treatment options. Retrospective studies have shown that the rate of glioma patients with additional co-morbidity is relatively low. Brain tumor centers, however, are increasingly confronted with an aging patient population exhibiting significant comorbidity.84 Accordingly, differentiated management algorithms, particularly for the elderly, have been developed, and gross total resection is sometimes withheld.20,21,85,86 Treatment algorithms lacking open tumor resection include minimal-invasive biopsy procedures followed by early hypofractionated irradiation alone or in combination with concomitant and adjuvant temozolomid, and upfront tremozolomid treatment. Decisions in favor of a more or less invasive treatment strategy rely on the patients’ performance, their multidimensional quality-of-life scores, and the MGMT promoter methylation status.20,21,87 Older patients with unmethylated malignant gliomas, for example, are less likely to receive chemoradiation.
In symptomatic patients with large tumor formations, tumor debulking may stabilize the patient for further treatment (see Figure 1). Upfront cortison treatment can help to differentiate between edema and tumor infiltration.88 Prospective assessment of the resectability of a glioma is still challenging: beyond conventional MRI, a multimodal workup, including fiber tracking in diffusion tensor imaging, metabolic PET data, and functional MRI, transcortical magnetic stimulation, electrophysiology, and complex neurocognitive testing, eg, for awake surgery, may improve resectability assessments preoperatively.59,89–91 Most of these preoperatively obtained structural and functional data can be integrated into the neuro-navigation device and used as a surgical guide in combination with intraoperative neuromonitoring to enable maximal safe resection (Figure 2). Prospective data elucidating factors associated with resectability are urgently needed to further improve the risk-benefit ratio of glioma surgery. The extent of resection (EOR) may be assessed online by means of routine ultrasound or intraoperative MRI.76,92 Both methods have their pros and cons. The introduction of fluorescence techniques such as use of 5-aminolevulin acid (5-ALA) has increased the rate of complete tumor resection.71,88 The rationale is that 5-ALA accumulates selectively in malignant glioma cells and can be visualized by blue light in the surgical microscope, enabling a better identification of tumor tissue in situ. Still, the surgeon has to keep in mind that a curative surgical treatment of grade II–IV gliomas is usually not possible due to the infiltrative character of the disease.93
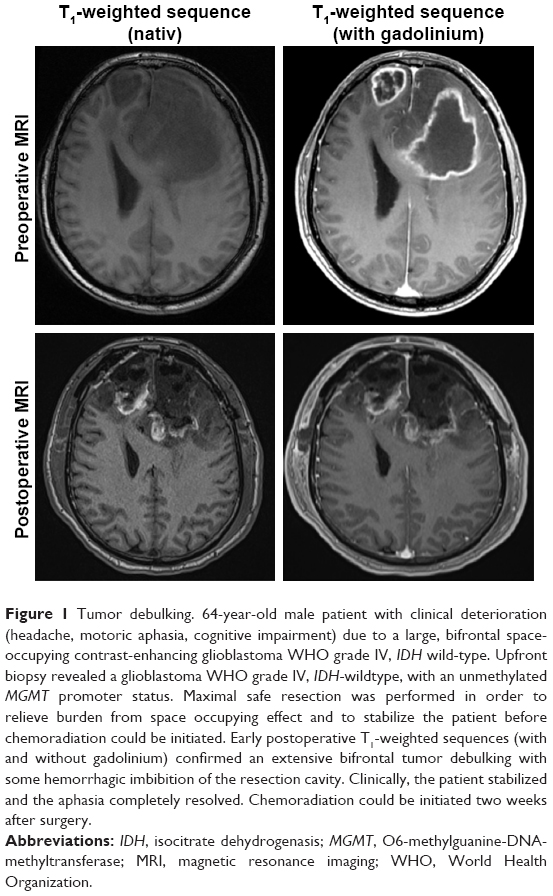 | Figure 1 Tumor debulking. 64-year-old male patient with clinical deterioration (headache, motoric aphasia, cognitive impairment) due to a large, bifrontal space-occupying contrast-enhancing glioblastoma WHO grade IV, IDH wild-type. Upfront biopsy revealed a glioblastoma WHO grade IV, IDH-wildtype, with an unmethylated MGMT promoter status. Maximal safe resection was performed in order to relieve burden from space occupying effect and to stabilize the patient before chemoradiation could be initiated. Early postoperative T1-weighted sequences (with and without gadolinium) confirmed an extensive bifrontal tumor debulking with some hemorrhagic imbibition of the resection cavity. Clinically, the patient stabilized and the aphasia completely resolved. Chemoradiation could be initiated two weeks after surgery. |
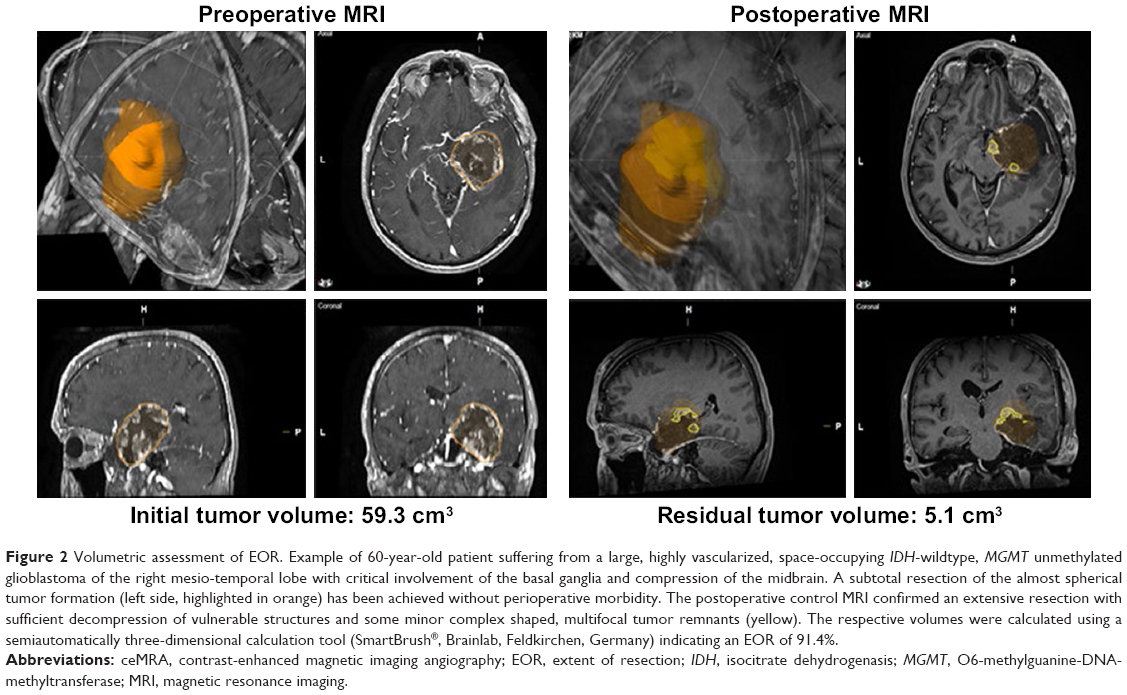 | Figure 2 Volumetric assessment of EOR. Example of 60-year-old patient suffering from a large, highly vascularized, space-occupying IDH-wildtype, MGMT unmethylated glioblastoma of the right mesio-temporal lobe with critical involvement of the basal ganglia and compression of the midbrain. A subtotal resection of the almost spherical tumor formation (left side, highlighted in orange) has been achieved without perioperative morbidity. The postoperative control MRI confirmed an extensive resection with sufficient decompression of vulnerable structures and some minor complex shaped, multifocal tumor remnants (yellow). The respective volumes were calculated using a semiautomatically three-dimensional calculation tool (SmartBrush®, Brainlab, Feldkirchen, Germany) indicating an EOR of 91.4%. |
EOR and prognosis
In malignant gliomas, the EOR is assessed by an early (within 72 hours) postoperative MRI. In low-grade gliomas, postoperative MRI 2–3 months after surgery is considered sufficient for EOR assessment.94 Qualitative descriptions of EOR such as “gross total resection”, “near total resection”, “subtotal resection”, “partial resection”, and “extended biopsy” are uncertain regarding their prognostic impact, and have been variably defined and used throughout the literature. Consensus exists, however, that patients undergoing gross total resections did better than the other ones. In glioblastomas, gross total resection refers to the complete removal of the contrast enhancing tumor parts. In WHO grade II gliomas, it refers to the complete removal of the tumor-associated hypointense areas as being depicted in T2-weighted/FLAIR sequences.94,95 Malignant enhancing gliomas also exhibit more or less often in additional non-enhancing tumor parts (a typical example is shown in Figure 1), which has been particularly seen in IDH mutant high-grade gliomas.34 Accordingly, the latest definition by the Revised Assessment in Neuro-oncology (RANO) criteria separates “complete resections of the contrast-enhancing tumor parts” from “complete resection of the detectable tumor” (including non-contrast-enhancing tumor parts), and the respective “incomplete (partial) resections” thereof.95
Quantitative EOR assessment also remains a controversial issue. It relies on different methods such as the product of the maximal diameter, the sum of areas on consecutive sequences, and three-dimensional, software-based calculations, etc. None of these methods has been validated in prospective studies.96 The volumetric calculation of complex shaped and/or multifocal tumor remnants is challenging and might be prone to biased estimations (a typical example is shown in Figure 3). Unspecific postoperative signal alterations (such as perifocal edema), bleedings, hemostatic agents, and/or surgically induced disturbances of the blood–brain barrier might also bias volumetric calculations.95 Relative EOR assessments indicating the relative reduction of the preoperative tumor volume have been performed in glioblastoma patients, and a linear correlation between distinct relative EOR levels and survival was assumed. For example, an EOR of 70% was better than a 50% EOR, which again was better than a 10% vol reduction and biopsy only strategies.68,70 These analyses, however, were not adjusted for the effects of the molecular biomarkers and modern adjuvant treatment concepts, and should not be used to revitalize the concept of incomplete resections in glioblastoma patients. Other studies have referred to absolute measurements of the residual tumor volume.97,98 Some recent data suggest that the prognostic relevance of EOR in high-grade glioma may depend on the molecular profile.80,99 For example, in IDH wildtype high-grade gliomas the prognostic decisive step is the complete removal of the contrast-enhancing tumor, whereas in IDH mutant high-grade gliomas best outcome may result if resection of both the contrast-enhancing and non-enhancing tumor parts has been achieved.34
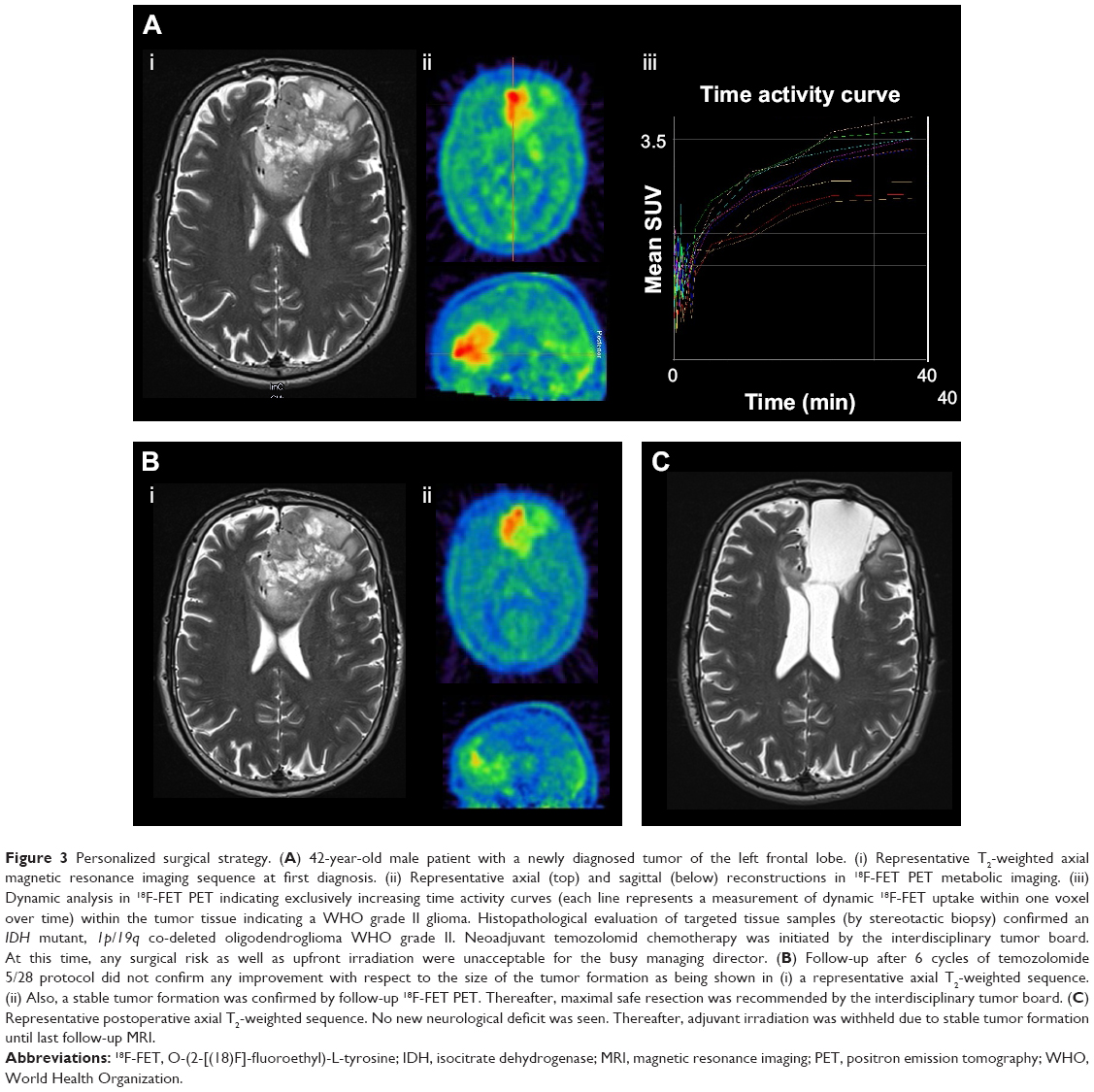 | Figure 3 Personalized surgical strategy. (A) 42-year-old male patient with a newly diagnosed tumor of the left frontal lobe. (i) Representative T2-weighted axial magnetic resonance imaging sequence at first diagnosis. (ii) Representative axial (top) and sagittal (below) reconstructions in 18F-FET PET metabolic imaging. (iii) Dynamic analysis in 18F-FET PET indicating exclusively increasing time activity curves (each line represents a measurement of dynamic 18F-FET uptake within one voxel over time) within the tumor tissue indicating a WHO grade II glioma. Histopathological evaluation of targeted tissue samples (by stereotactic biopsy) confirmed an IDH mutant, 1p/19q co-deleted oligodendroglioma WHO grade II. Neoadjuvant temozolomid chemotherapy was initiated by the interdisciplinary tumor board. At this time, any surgical risk as well as upfront irradiation were unacceptable for the busy managing director. (B) Follow-up after 6 cycles of temozolomide 5/28 protocol did not confirm any improvement with respect to the size of the tumor formation as being shown in (i) a representative axial T2-weighted sequence. (ii) Also, a stable tumor formation was confirmed by follow-up 18F-FET PET. Thereafter, maximal safe resection was recommended by the interdisciplinary tumor board. (C) Representative postoperative axial T2-weighted sequence. No new neurological deficit was seen. Thereafter, adjuvant irradiation was withheld due to stable tumor formation until last follow-up MRI. |
The role of molecular imaging for critical assessment of EOR as compared to structural imaging should be addressed in further prospective studies. Notably, a correlative analysis of MRT and 18F-FET PET in newly diagnosed glioblastomas showed larger tumor volumes according to the applied PET criteria as compared to conventional MRI in the majority of the tumors.59 Limitations of prognostic EOR measurements in glioblastomas also concerns estimations in low-grade gliomas.100,101 Even though some retrospective data supported a favorable impact of EOR on the malignant transformation rate of low-grade gliomas67,68,102–104 and even argue in favor of “supramarginal” resections guided by “functional” boarders,105 significant selection bias by tumor location, molecular-genetic profiles, and tumor size could not be excluded.106 Other studies did not report correlations between EOR and the risk of malignant transformation. Prospective data are necessary to define standardized EOR measurements associated with the prognosis and the respective molecular-genetic profiles of the disease.
The risk of surgery
Perioperative morbidity of microsurgical glioma resection has been reported to be highly variable, currently lying in the range of 5%–20% or even higher.69,88,107 Even though risk factors of glioma surgery are poorly defined, frequent inclusion of older patients and/or those with an eloquent tumor location might have increased the complication rate in some studies.87,108 The overall proportion of safe gross total resections, however, has been increased by utilization of elaborate imaging and functional diagnostics before and during surgery.71,73,89,109–111 More recent data have suggested that pre- and intraoperative functional assessments, neuro-navigation, and in-situ imaging techniques have the potential to improve both the risk profile of resective treatment (morbidity below 5%) and the proportion of complete resections in the overwhelming number of patients.30,73 To which extent patient selection has contributed to these favorable results remains unknown. Intraoperative neurophysiological mapping, including awake craniotomy with language monitoring, has been shown to be helpful to maximize safe EOR and to maintain/improve functional scores postoperatively in eloquently located glioma surgery. However, all these imaging and monitoring techniques could not adequately control for the neurovascular risks of resective treatment. Symptomatic ischemic events are expected to occur in 6%–10% of patients, particularly if surgery is performed within areas of small perforating arteries supplying highly eloquent areas such as the insula or crus cerebri.112
The risk of stereotactic biopsy has been shown to be also highly variable, presumably depending on the applied biopsy technique and the biopsy frequency per year in the respective centers.113,114 In experienced hands, the risk has been shown to lie in the range of 1% and was not influenced by tumor size, number of biopsies taken, and tumor location.24,69,78
In general, risk assessment is of fundamental relevance for treatment decisions and prognosis of the patient under consideration. Those with significant postoperative morbidity have a worse prognosis and are less often eligible for adjuvant treatment.107 Risk-adapted surgical concepts are one of the cornerstones of individualized glioma treatment concepts.115
Toward individualized surgical strategies
The overwhelming contribution of molecular markers for diagnostic classification, prognosis, and treatment decision requires a reassessment of surgical strategies in the context of increasingly complex, risk, and benefit-optimized management strategies. Microsurgical resection should be performed if a complete removal of the entire tumor volumes can be safely achieved. In the case of unclear differential diagnosis and/or an unfavorable risk-benefit ratio for microsurgery, molecular stereotactic biopsy technique represents an useful alternative.24 If the molecular profile indicates increased chemo- and/or radiation resistance, surgical resection may become even more important for the improvement of the overall prognosis. Conversely, delayed resection might be considered for residual eloquently located tumors when upfront chemotherapy/irradiation had successfully been applied (Figure 3).116 Individualized modification of the place of surgery within the treatment network of requires further evaluation. In complex located low-grade glioma patients suffering from pharmacoresistant epilepsy, a sophisticated electrophysiological evaluation in highly specialized epilepsy centers may be indicated.117–119 Invasive monitoring, eg, with stereotactically implanted deep electrodes, could be performed for identification of the epileptogenic focus and to guide targeted resections.
Alternative local therapies
Besides surgical resection, alternative local treatment strategies can be applied in addition to resective treatment or instead of that. Most of these therapies are currently under investigation.
Local chemotherapy
Outcome after partial resection may be ameliorated by the use of local chemotherapy using biodegradable polymers as a carrier matrix. These compounds are placed into the resection cavity (preferentially attached to the resection walls), which allows the drug to be delivered directly to the tumor cells left behind after surgery. Carmustine (BCNU) wafers are the only ones who have been evaluated in two controlled phase III trials for recurrent120 and newly diagnosed121 high grade glioma. Due to positive study results, carmustine wafers have become part of many guidelines and recommendations in clinical neuro-oncology. The effectiveness, however, depends on EOR with best results in the case of complete resections and MGMT promoter methylated tumors.122 As the formulations release most of the BCNU within the first 2 weeks after application it is considered a “gab-treatment” in newly diagnosed glioblastoma before conventional chemoradiation is initiated.
Convection enhanced delivery (CED) represents another highly attractive technique for intratumoral drug delivery. This technique can be used to deliver small bioactive molecules within the tumor, thereby overcoming limitations due to the blood–brain barrier. CED is achieved by stereotactically placed catheters and a constant low pressure infusion.123 Targeted toxins, which are chimeric molecules binding to a selectively overexpressed cell surface molecule, include transforming growth factor-alpha, interleukin-4 and -13 linked to pseudomonas exotoxin and others.124 First results were promising, however, a clear indication and criteria for patient selection have not yet established. Further investigations are needed to implement CED in glioma therapy.
Interstitial brachytherapy
For patients with well-demarcated, complex located low-grade gliomas with a maximum diameter of 3.5 cm, interstitial brachytherapy poses an alternative, minimally-invasive, highly-localized treatment option.125 A versatile neuropathological diagnosis must be obtained upfront, eg, by means of minimal invasive stereotactic biopsy procedures.24 The stereotactic implantation of low-energy radioactive Iodine-125 seeds enables the application of a high, necrotizing dose within the tumor, whereas the steep decline of dose at the tumor boundaries enables a continual, low-dose “hyperfractionated” irradiation of the tumor margin under protection of the surrounding brain parenchyma.126 Due to these favorable radiobiological characteristics, external beam radiation may still be performed in the case of a local tumor recurrence without an increase of radiogenic complications. For larger and/or eloquently located low-grade gliomas, a combination of a planned partial resection followed by interstitial brachytherapy may be a reasonable treatment recommendation within the framework of personalized surgical therapy.127 The place of interstitial brachytherapy for circumscribed high-grade gliomas needs to be determined.125 Moreover, we do not know whether molecular profiles influence responses to interstitial brachytherapy.
Photodynamic therapy
Oral application of 5-ALA leads to a highly specific accumulation in malignant glioma cells. Besides its use for fluorescence guided resections, the cytotoxic properties of 5-ALA in conjunction with high energy light application leads to apoptosis and subsequent cell death, which can be used for local therapy. Tumor cell illumination can be effectively obtained from stereotactically placed light fibers. Typically, after interstitial photodynamic therapy (iPDT) there is a complete decrease of the local contrast agent uptake in the tumor. In contrast, the diffusion-weighted sequences show a massive restriction in the treatment volume. First studies show that photodynamic therapy for highly selected patients with localized malignant glioma up to 4 cm in diameter (first diagnosis or recurrence) significantly prolongs survival. These first observations should be evaluated in future prospective trials.128 From a pathophysiological perspective, the remarkable results after iPDT may be due to long-lasting immunological processes specifically triggered by this method. Accordingly, cortison treatment should be avoided not to interfere with these processes.
Outlook
Mostly due to ethical considerations it seems to be rather unlikely that class I evidence will be available on the impact of EOR on outcome measurements in glioma patients. However, an improved prognostic evaluation that also includes the emerging field of molecular, metabolic, and imaging-based biomarkers will certainly help to identify the surgical procedure that fits most to the needs and limits of the individual patient within a multimodal risk-/benefit-optimized oncological management concept. Recent developments in targeted therapy will also push treatment concepts toward “molecular neurosurgery”, for example, using conjugated immunotoxins that specifically bind to characteristic surface markers for glioma cells. Emerging experimental therapies will certainly influence future management consideration and re-adjust the place of surgery in diffuse gliomas. Moreover, multimodal imaging systems with existing and new contrast agents, molecular tracers, technological advances, and advanced data analysis will serve as disease relevant biomarkers that will improve disease management and patient care.
Disclosure
The authors report no conflicts of interest in this work.
References
Ostrom QT, Gittleman H, Liao P, et al. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2010–2014. Neuro Oncol. 2017;19(suppl_5):v1–v88. | ||
Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. | ||
Dunn GP, Andronesi OC, Cahill DP. From genomics to the clinic: biological and translational insights of mutant IDH1/2 in glioma. Neurosurg Focus. 2013;481(2):E2. | ||
Weller M, van den Bent M, Tonn JC, et al. European association for neuro-oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017;18(6):e315–e329. | ||
Ringel F, Pape H, Sabel M, et al. Clinical benefit from resection of recurrent glioblastomas: results of a multicenter study including 503 patients with recurrent glioblastomas undergoing surgical resection. Neuro Oncol. 2016;18(1):96–104. | ||
Suchorska B, Weller M, Tabatabai G, et al. Complete resection of contrast-enhancing tumor volume is associated with improved survival in recurrent glioblastoma – results from the director trial. Neuro Oncol. 2016;18(4):549–556. | ||
Mann J, Ramakrishna R, Magge R, Wernicke AG. Advances in radiotherapy for glioblastoma. Front Neurol. 2017;8:748. | ||
Weller M, van den Bent M, Hopkins K, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014;15(9):e395–e403. | ||
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. | ||
Stupp R, Brada M, van den Bent MJ, Tonn J-C, Pentheroudakis G; Group EGW; ESMO Guidelines Working Group. High-grade glioma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(suppl 3):iii93–iii101. | ||
Herrlinger U, Tzaridis T, Mack F, et al. ACTR-58. Phase III trial of CCNU/Temozolomide (TMZ) combination therapy vs. standard TMZ therapy for newly diagnosed MGMT-METHYLATED glioblastoma patients: the CeTeg/NOA-09 trial. Neuro Oncol. 2017;19(suppl_6):vi13–vi14. | ||
Weiss T, Weller M, Roth P. Immunotherapy for glioblastoma: concepts and challenges. Curr Opin Neurol. 2015;28(6):639–646. | ||
Mun EJ, Babiker HM, Weinberg U, Kirson ED, von Hoff DD. Tumor-Treating fields: a fourth modality in cancer treatment. Clin Cancer Res. 2018;24(2):266–275. | ||
Stupp R, Taillibert S, Kanner A, et al. Effect of tumor-treating fields plus maintenance temozolomide vs maintenance temozolomide alone on survival in patients with glioblastoma. JAMA. 2017;318(23):2306–2316. | ||
Ford E, Catt S, Chalmers A, Fallowfield L. Systematic review of supportive care needs in patients with primary malignant brain tumors. Neuro Oncol. 2012;14(4):392–404. | ||
Eckel-Passow JE, Lachance DH, Molinaro AM, et al. Glioma groups based on 1p/19q, IDHIDH, and TERTTERT promoter mutations in tumors. N Engl J Med. 2015;372(26):2499–2508. | ||
Cairncross G, Jenkins R. Gliomas with 1p/19q codeletion: a.k.a. oligodendroglioma. J Clin Oncol. 2008;14(6):352–357. | ||
Cairncross G, Wang M, Shaw E, et al. Phase III trial of chemoradiotherapy for anaplastic oligodendroglioma: long-term results of RTOG 9402. J Clin Oncol. 2013;31(3):337–343. | ||
Hegi ME, Diserens A-C, Gorlia T, et al. MGMTMGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352(10):997–1003. | ||
Malmström A, Grønberg BH, Marosi C, et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial. Lancet Oncol. 2012;13(9):916–926. | ||
Wick W, Platten M, Meisner C, et al. Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: the NOA-08 randomised, phase 3 trial. Lancet Oncol. 2012;13(7):707–715. | ||
Wijnenga MMJ, Dubbink HJ, French PJ, et al. Molecular and clinical heterogeneity of adult diffuse low-grade IDH wild-type gliomas: assessment of TERT promoter mutation and chromosome 7 and 10 copy number status allows superior prognostic stratification. Acta Neuropathol. 2017;134(6):957–959. | ||
Grasbon-Frodl EM, Kreth FW, Ruiter M, et al. Intratumoral homogeneity of MGMT promoter hypermethylation as demonstrated in serial stereotactic specimens from anaplastic astrocytomas and glioblastomas. Int J Cancer. 2007;121(11):2458–2464. | ||
Eigenbrod S, Trabold R, Brucker D, et al. Molecular stereotactic biopsy technique improves diagnostic accuracy and enables personalized treatment strategies in glioma patients. Acta Neurochir (Wien). 2014;156(8):1427–1440. | ||
Thon N, Eigenbrod S, Grasbon-Frodl EM, et al. Novel molecular stereotactic biopsy procedures reveal intratumoral homogeneity of loss of heterozygosity of 1p/19q and TP53 mutations in World Health organization grade II gliomas. J Neuropath Exp Neur. 2009;68(11):1219–1228. | ||
Henson JW, Gaviani P, Gonzalez RG. MRI in treatment of adult gliomas. Lancet Oncol. 2005;6(3):167–175. | ||
Thon N, Kunz M, Lemke L, et al. Dynamic 18F-FET PET in suspected WHO grade II gliomas defines distinct biological subgroups with different clinical courses. Int J Cancer. 2015;136(9):2132–2145. | ||
Kunz M, Thon N, Eigenbrod S, et al. Hot spots in dynamic18FET-PET delineate malignant tumor parts within suspected WHO grade II gliomas. Neuro Oncol. 2011;13(3):307–316. | ||
Sahm F, Capper D, Jeibmann A, et al. Addressing diffuse glioma as a systemic brain disease with single-cell analysis. Arch Neurol. 2012;69(4):523–526. | ||
Ius T, Isola M, Budai R, et al. Low-grade glioma surgery in eloquent areas: volumetric analysis of extent of resection and its impact on overall survival. A single-institution experience in 190 patients. J Neurosurg. 2012;42(6):1039–1052. | ||
Lang FF, Olansen NE, Demonte F, et al. Surgical resection of intrinsic insular tumors: complication avoidance. J Neurosurg. 2001;7(4):638–650. | ||
Mandonnet E, Capelle L, Duffau H. Extension of paralimbic low grade gliomas: toward an anatomical classification based on white matter invasion patterns. J Neurooncol. 2006;78(2):179–185. | ||
Ius T, Turella L, Pauletto G, et al. Quantitative diffusion tensor imaging analysis of low-grade gliomas: from preclinical application to patient care. World Neurosurg. 2017;97:333–343. | ||
Beiko J, Suki D, Hess KR, et al. IDH1 mutant malignant astrocytomas are more amenable to surgical resection and have a survival benefit associated with maximal surgical resection. Neuro Oncol. 2014;16(1):81–91. | ||
O’Connor JPB, Aboagye EO, Adams JE, et al. Imaging biomarker roadmap for cancer studies. Nat Rev Clin Oncol. 2017;14(3):169–186. | ||
Gillies RJ, Kinahan PE, Hricak H. Radiomics: images are more than pictures, they are data. Radiology. 2016;278(2):563–577. | ||
Kerns SL, L West CM, Andreassen CN, et al. Radiogenomics: the search for genetic predictors of radiotherapy response. Future Oncol. 2014;10(15):2391–2406. | ||
Pallud J, Capelle L, Taillandier L, et al. Prognostic significance of imaging contrast enhancement for WHO grade II gliomas. Neuro Oncol. 2009;11(2):176–182. | ||
Pallud J, Mandonnet E, Duffau H, et al. Prognostic value of initial magnetic resonance imaging growth rates for World Health organization grade II gliomas. Ann Neurol. 2006;60(3):380–383. | ||
Diehn M, Nardini C, Wang DS, et al. Identification of noninvasive imaging surrogates for brain tumor gene-expression modules. Proc Natl Acad Sci U S A. 2008;105(13):5213–5218. | ||
Ingrisch M, Schneider MJ, Nörenberg D, et al. Radiomic analysis reveals prognostic information in T1-weighted baseline magnetic resonance imaging in patients with glioblastoma. Invest Radiol. 2017;52(6):360–366. | ||
Delfanti RL, Piccioni DE, Handwerker J, et al. Imaging correlates for the 2016 update on WHO classification of grade II/III gliomas: implications for IDH, 1p/19q and ATRX status. J Neurooncol. 2017;135(3):601–609. | ||
Metellus P, Coulibaly B, Colin C, et al. Absence of IDH mutation identifies a novel radiologic and molecular subtype of WHO grade II gliomas with dismal prognosis. Acta Neuropathol. 2010;120(6):719–729. | ||
Carrillo JA, Lai A, Nghiemphu PL, et al. Relationship between tumor enhancement, edema, IDHIDH1 mutational status, MGMTMGMT promoter methylation, and survival in glioblastoma. AJNR Am J Neuroradiol. 2012;33(7):1349–1355. | ||
Drabycz S, Roldán G, de Robles P, et al. An analysis of image texture, tumor location, and MGMT promoter methylation in glioblastoma using magnetic resonance imaging. NeuroImage. 2010;49(2):1398–1405. | ||
Jansen RW, van Amstel P, Martens RM, et al. Non-invasive tumor genotyping using radiogenomic biomarkers, a systematic review and oncology-wide pathway analysis. Oncotarget. 2018;9(28):20134–20155. | ||
Moon W-J, Choi JW, Roh HG, Lim SD, Koh Y-C. Imaging parameters of high grade gliomas in relation to the MGMT promoter methylation status: the CT, diffusion tensor imaging, and perfusion MR imaging. Neuroradiology. 2012;54(6):555–563. | ||
Ellingson BM, Lai A, Harris RJ, et al. Probabilistic radiographic atlas of glioblastoma phenotypes. AJNR Am J Neuroradiol. 2013;34(3):533–540. | ||
Korfiatis P, Kline TL, Coufalova L, et al. MRI texture features as biomarkers to predict MGMT methylation status in glioblastomas. Med Phys. 2016;43(6 Part 1):2835–2844. | ||
Levner I, Drabycz S, Roldan G, de Robles P, Cairncross JG, Mitchell R. Predicting MGMT methylation status of glioblastomas from MRI texture. Med Image Comput Comput Assist Interv. 2009;12(Pt 2):522–530. | ||
Seow P, Wong JHD, Ahmad-Annuar A, Mahajan A, Mahajan A, Abdullah NA. Quantitative magnetic resonance imaging and radiogenomic biomarkers for glioma characterisation: a systematic review. Br J Radiol. 2018;91(1092):20170930. | ||
Zinn PO, Majadan B, Sathyan P, et al. Radiogenomic mapping of edema/cellular invasion MRI-phenotypes in glioblastoma multiforme. PLoS One. 2011;6(10):e25451. | ||
Abrigo JM, Fountain DM, Provenzale JM, et al. Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation. Cochrane Database Syst Rev. 2018;1:CD011551. | ||
Falk Delgado A, Nilsson M, van Westen D, A FD, Falk Delgado A. Glioma grade discrimination with MR diffusion Kurtosis imaging: a meta-analysis of diagnostic accuracy. Radiology. 2017;287(1):119–127. | ||
Liang J, Liu D, Gao P, et al. Diagnostic values of DCE-MRI and DSC-MRI for differentiation between high-grade and low-grade gliomas: a comprehensive meta-analysis. Acad Radiol. 2018;25(3):338–348. | ||
Yang Y, He MZ, Li T, Yang X. MRI combined with PET-CT of different tracers to improve the accuracy of glioma diagnosis: a systematic review and meta-analysis. Neurosurg Rev. Epub 2017 Sep 16. | ||
Arbizu J, Tejada S, Marti-Climent JM, et al. Quantitative volumetric analysis of gliomas with sequential MRI and 11C-methionine PET assessment: patterns of integration in therapy planning. Eur J Nucl Med Mol Imaging. 2012;39(5):771–781. | ||
la Fougere C, Suchorska B, Bartenstein P, Kreth F-W, Tonn J-C. Molecular imaging of gliomas with PET: opportunities and limitations. Neuro Oncol. 2011;13(8):806–819. | ||
Suchorska B, Jansen NL, Linn J, et al. Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM. Neurology. 2015;84(7):710–719. | ||
Pauliah M, Saxena V, Haris M, Husain N, Rathore RKS, Gupta RK. Improved T1-weighted dynamic contrast-enhanced MRI to probe microvascularity and heterogeneity of human glioma. Magn Reson Imag. 2007;25(9):1292–1299. | ||
Ah J, Thomas A, Kracht LW, et al. 18F-fluoro-L-thymidine and 11C-methylmethionine as markers of increased transport and proliferation in brain tumors. J Nucl Med. 2005;46(12):1948–1958. | ||
Chiang GC, Kovanlikaya I, Choi C, Ramakrishna R, Magge R, Shungu DC. Magnetic resonance spectroscopy, positron emission tomography and radiogenomics – relevance to glioma. Front Neurol. 2018;9:33. | ||
Choi C, Ganji SK, Deberardinis RJ, et al. 2-Hydroxyglutarate detection by magnetic resonance spectroscopy in IDH-mutated patients with gliomas. Nat Med. 2012;18(4):624–629. | ||
Elkhaled A, Jalbert LE, Phillips JJ, et al. Magnetic resonance of 2-hydroxyglutarate in IDH1-mutated low-grade gliomas. Sci Transl Med. 2012;4(116):116ra5. | ||
Rundle-Thiele D, Day B, Stringer B, et al. Using the apparent diffusion coefficient to identifying MGMT promoter methylation status early in glioblastoma: importance of analytical method. J Med Radiat Sci. 2015;62(2):92–98. | ||
Jakola AS, Unsgård G, Myrmel KS, et al. Surgical strategy in grade II astrocytoma: a population-based analysis of survival and morbidity with a strategy of early resection as compared to watchful waiting. Acta Neurochir (Wien). 2013;155(12):2227–2235. | ||
Smith JS, Chang EF, Lamborn KR, et al. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J Clin Oncol. 2008;26(8):1338–1345. | ||
Shaw EG, Berkey B, Coons SW, et al. Recurrence following neurosurgeon-determined gross-total resection of adult supratentorial low-grade glioma: results of a prospective clinical trial. J Neurosurg. 2008;72(98):835–841. | ||
Kreth F-W, Thon N, Simon M, et al. Gross total but not incomplete resection of glioblastoma prolongs survival in the era of radiochemotherapy. Ann Oncol. 2013;24(12):3117–3123. | ||
Lacroix M, Abi-Said D, Fourney DR, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg. 2001;34(2):190–198. | ||
Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. 2006;7(5):392–401. | ||
Chinot OL, de La Motte Rouge T, Moore N, et al. AVAglio: phase 3 trial of bevacizumab plus temozolomide and radiotherapy in newly diagnosed glioblastoma multiforme. Adv Therapy. 2011;28(4):334–340. | ||
De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, Berger MS. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: a meta-analysis. J Clin Oncol. 2012;30(20):2559–2565. | ||
Jiang B, Chaichana K, A V, Chang SD, Black KL, Patil CG. Biopsy versus resection for the management of low-grade gliomas. Cochrane Database Syst Rev. 2017;4:CD009319. | ||
Veeravagu A, Jiang B, Ludwig C, Chang SD, Black KL, Patil CG. Biopsy versus resection for the management of low-grade gliomas. Cochrane Database Syst Rev. 2013;4:CD009319. | ||
Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Intraoperative MRI guidance and extent of resection in glioma surgery: a randomised, controlled trial. Lancet Oncol. 2011;12(11):997–1003. | ||
Laws ER, Parney IF, Huang W, et al; Glioma Outcomes Investigators. Survival following surgery and prognostic factors for recently diagnosed malignant glioma: data from the glioma outcomes project. J Neurosurg. 2003;48(3):467–473. | ||
Ragel BT, Ryken TC, Kalkanis SN, Ziu M, Cahill D, Olson JJ. The role of biopsy in the management of patients with presumed diffuse low grade glioma: a systematic review and evidence-based clinical practice guideline. J Neurooncol. 2015;125(3):481–501. | ||
Thon N, Thorsteinsdottir J, Eigenbrod S, et al. Outcome in unresectable glioblastoma: MGMT promoter methylation makes the difference. J Neurol. 2017;264(2):350–358. | ||
Thon N, Eigenbrod S, Grasbon-Frodl EM, et al. Predominant influence of MGMT methylation in non-resectable glioblastoma after radiotherapy plus temozolomide. J Neurol Neurosurg Psychiatr. 2011;82(4):441–446. | ||
Rachinger W, Grau S, Holtmannspotter M, Herms J, Tonn J-C, Kreth FW. Serial stereotactic biopsy of brainstem lesions in adults improves diagnostic accuracy compared with MRI only. J Neurol Neurosurg Psychiatr. 2009;80(10):1134–1139. | ||
Kim BYS, Jiang W, Beiko J, et al. Diagnostic discrepancies in malignant astrocytoma due to limited small pathological tumor sample can be overcome by IDH1 testing. J Neurooncol. 2014;118(2):405–412. | ||
Kreth S, Limbeck E, Hinske LC, et al. In human glioblastomas transcript elongation by alternative polyadenylation and miRNA targeting is a potent mechanism of MGMT silencing. Acta Neuropathol. 2013;125(5):671–681. | ||
Sasaki T, Fukai J, Kodama Y, et al. Characteristics and outcomes of elderly patients with diffuse gliomas: a multi-institutional cohort study by Kansai molecular diagnosis network for CNS tumors. J Neurooncol. 2018;140(2):329–339. | ||
Ironside S, das S, Sahgal A, Moroney C, Mainprize T, Perry JR. Optimal therapies for newly diagnosed elderly patients with glioblastoma. Curr Treat Options in Oncol. 2017;18(11):66. | ||
Perry JR, Laperriere N, O’Callaghan CJ, et al; Trial Investigators. Short-course radiation plus temozolomide in elderly patients with glioblastoma. N Engl J Med. 2017;376(11):1027–1037. | ||
Heiland DH, Haaker G, Watzlawick R, et al. One decade of glioblastoma multiforme surgery in 342 elderly patients: what have we learned? J Neurooncol. 2018;140(2):385–391. | ||
Stummer W, Tonn J-C, Mehdorn HM, et al. Counterbalancing risks and gains from extended resections in malignant glioma surgery: a supplemental analysis from the randomized 5-aminolevulinic acid glioma resection study. J Neurosurg. 2011;25(3):613–623. | ||
Rasmussen I-A, Lindseth F, Rygh OM, et al. Functional neuronavigation combined with intra-operative 3D ultrasound: initial experiences during surgical resections close to eloquent brain areas and future directions in automatic brain shift compensation of preoperative data. Acta Neurochir (Wien). 2007;149(4):365–378. | ||
Sollmann N, Wildschuetz N, Kelm A, et al. Associations between clinical outcome and navigated transcranial magnetic stimulation characteristics in patients with motor-eloquent brain lesions: a combined navigated transcranial magnetic stimulation-diffusion tensor imaging fiber tracking approach. J Neurosurg. 2018;21(1):800–810. | ||
Suchorska B, Giese A, Biczok A, et al. Identification of time-to-peak on dynamic 18F-FET-PET as a prognostic marker specifically in IDH1/2 mutant diffuse astrocytoma. Neuro Oncol. 2017;20(2):279–288. | ||
Coburger J, Merkel A, Scherer M, et al. Low-grade glioma surgery in intraoperative magnetic resonance imaging: results of a multicenter retrospective assessment of the German Study Group for intraoperative magnetic resonance imaging. Neurosurgery. 2016;78(6):775–786. | ||
Cavaliere R, Lopes MBS, Schiff D. Low-grade gliomas: an update on pathology and therapy. Lancet Neurol. 2005;4(11):760–770. | ||
van den Bent MJ, Wefel JS, Schiff D, et al. Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol. 2011;12(6):583–593. | ||
Vogelbaum MA, Jost S, Aghi MK, et al. Application of novel response/progression measures for surgically delivered therapies for gliomas: response assessment in neuro-oncology (RANO) Working Group. Neurosurgery. 2012;70(1):234–243; discussion 243–244. | ||
Kubben PL, Postma AA, Kessels AGH, van Overbeeke JJ, van Santbrink H. Intraobserver and interobserver agreement in volumetric assessment of glioblastoma multiforme resection. Neurosurgery. 2010;67(5):1329–1334. | ||
Grabowski MM, Recinos PF, Nowacki AS, et al. Residual tumor volume versus extent of resection: predictors of survival after surgery for glioblastoma. J Neurosurg. 2014;36(5):1115–1123. | ||
Keles GE, Chang EF, Lamborn KR, et al. Volumetric extent of resection and residual contrast enhancement on initial surgery as predictors of outcome in adult patients with hemispheric anaplastic astrocytoma. J Neurosurg. 2006;12(1):34–40. | ||
Stewart LA. Chemotherapy in adult high-grade glioma: a systematic review and meta-analysis of individual patient data from 12 randomised trials. Lancet. 2002;359(9311):1011–1018. | ||
Sanai N, Polley M-Y, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011;16(1):3–8. | ||
Chaichana KL, Jusue-Torres I, Navarro-Ramirez R, et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro Oncol. 2014;16(1):113–122. | ||
Ahmadi R, Rezvan A, Dictus C, Hartmann C, et al. Long-term outcome and survival of surgically treated supratentorial low-grade glioma in adult patients. Acta Neurochir (Wien). 2009;151(11):1367–1365. | ||
Chaichana KL, McGirt MJ, Laterra J, Olivi A, Quiñones-Hinojosa A. Recurrence and malignant degeneration after resection of adult hemispheric low-grade gliomas. J Neurosurg. 2010;112(1):10–17. | ||
McGirt MJ, Chaichana KL, Attenello FJ, et al. Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas. Neurosurgery. 2008;63(4):700–708; author reply 707–708. | ||
Yordanova YN, Moritz-Gasser S, Duffau H. Awake surgery for WHO Grade II gliomas within “noneloquent” areas in the left dominant hemisphere: toward a “supratotal” resection. Clinical article. J Neurosurg. 2011;115(2):232–239. | ||
Marko NF, Weil RJ, Schroeder JL, Lang FF, Suki D, Sawaya RE. Extent of resection of glioblastoma revisited: personalized survival modeling facilitates more accurate survival prediction and supports a maximum-safe-resection approach to surgery. J Clin Oncol. 2014;32(8):774–782. | ||
Gulati S, Jakola AS, Nerland US, Weber C, Solheim O. The risk of getting worse: surgically acquired deficits, perioperative complications, and functional outcomes after primary resection of glioblastoma. World Neurosurg. 2011;76(6):572–579. | ||
Satoer D, Visch-Brink E, Dirven C, Vincent A. Glioma surgery in eloquent areas: can we preserve cognition? Acta Neurochir (Wein). 2016;158(1):35–50. | ||
Berman JI, Berger MS, Chung SW, Nagarajan SS, Henry RG. Accuracy of diffusion tensor magnetic resonance imaging tractography assessed using intraoperative subcortical stimulation mapping and magnetic source imaging. J Neurosurg. 2007;107(3):488–494. | ||
Guggisberg AG, Honma SM, Findlay AM, et al. Mapping functional connectivity in patients with brain lesions. Ann Neurol. 2008;63(2):193–203. | ||
Jenkinson MD, Barone DG, Bryant A, et al. Intraoperative imaging technology to maximise extent of resection for glioma. Cochrane Database Syst Rev. 2018;1:CD012788. | ||
Dützmann S, Geßler F, Bink A, et al. Risk of ischemia in glioma surgery: comparison of first and repeat procedures. J Neurooncol. 2012;107(3):599–607. | ||
Kulkarni AV, Guha A, Lozano A, Bernstein M. Incidence of silent hemorrhage and delayed deterioration after stereotactic brain biopsy. J Neurosurg. 1998;89(1):31–35. | ||
Kreth FW, Muacevic A, Medele R, Bise K, Meyer T, Reulen HJ. The risk of haemorrhage after image guided stereotactic biopsy of intra-axial brain tumours – a prospective study. Acta Neurochir (Wein). 2001;143(6):539–546; discussion 545–546. | ||
Vogelbaum MA. Towards a genomic definition of completeness of resection? Neuro Oncol. 2014;16(1):2–3. | ||
Taal W, van der Rijt CC, Dinjens WN, et al. Treatment of large low-grade oligodendroglial tumors with upfront procarbazine, lomustine, and vincristine chemotherapy with long follow-up: a retrospective cohort study with growth kinetics. J Neurooncol. 2015;121(2):365–372. | ||
Soffietti R, Baumert BG, Bello L, et al. Guidelines on management of low-grade gliomas: report of an EFNS-EANO Task Force. Eur J Neurol. 2010;17(9):1124–1133. | ||
Avila EK, Chamberlain M, Schiff D, et al. Seizure control as a new metric in assessing efficacy of tumor treatment in low-grade glioma trials. Neuro Oncol. 2017;19(1):12–21. | ||
Ius T, Pauletto G, Isola M, et al. Surgery for insular low-grade glioma: predictors of postoperative seizure outcome. J Neurosurg. 2014;120(1):12–23. | ||
Brem H, Piantadosi S, Burger PC, et al. Placebo-controlled trial of safety and efficacy of intraoperative controlled delivery by biodegradable polymers of chemotherapy for recurrent gliomas. The Polymer-brain tumor treatment Group. Lancet. 1995;345(8956):1008–1012. | ||
Westphal M, Hilt DC, Bortey E, et al. A phase 3 trial of local chemotherapy with biodegradable carmustine (BCNU) wafers (Gliadel wafers) in patients with primary malignant glioma. Neuro Oncol. 2003;5(2):79–88. | ||
Gutenberg A, Bock HC, Brück W, et al. MGMT promoter methylation status and prognosis of patients with primary or recurrent glioblastoma treated with carmustine wafers. Br J Neurosurg. 2013;27(6):772–778. | ||
Bobo RH, Laske DW, Akbasak A, Morrison PF, Dedrick RL, Oldfield EH. Convection-enhanced delivery of macromolecules in the brain. Proc Natl Acad Sci U S A. 1994;91(6):2076–2080. | ||
Kunwar S, Chang S, Westphal M, et al. Phase III randomized trial of CED of IL13-PE38QQR vs Gliadel wafers for recurrent glioblastoma. Neuro Oncol. 2010;12(8):871–881. | ||
Schwarz SB, Thon N, Nikolajek K, et al. Iodine-125 brachytherapy for brain tumours – a review. Radiat Oncol. 2012;7:30. | ||
Kreth FW, Thon N, Siefert A, Tonn JC. The place of interstitial brachytherapy and radiosurgery for low-grade gliomas. Adv Tech Stand Neurosurg. 2010;35:183–212. | ||
Schnell O, Schöller K, Ruge M, Siefert A, Tonn JC, Kreth FW. Surgical resection plus stereotactic 125I brachytherapy in adult patients with eloquently located supratentorial WHO grade II glioma – feasibility and outcome of a combined local treatment concept. J Neurol. 2008;255(10):1495–1502. | ||
Stummer W, Beck T, Beyer W, et al. Long-sustaining response in a patient with non-resectable, distant recurrence of glioblastoma multiforme treated by interstitial photodynamic therapy using 5-ALA: case report. J Neurooncol. 2008;87(1):103–109. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.