Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
The subjective perception of past, present, and future time in patients with Alzheimer's disease: a qualitative study
Authors Shiromaru-Sugimoto A ![]() , Murakami H
, Murakami H ![]() , Futamura A
, Futamura A ![]() , Honma M, Kuroda T, Kawamura M, Ono K
, Honma M, Kuroda T, Kawamura M, Ono K ![]()
Received 1 September 2018
Accepted for publication 23 October 2018
Published 22 November 2018 Volume 2018:14 Pages 3185—3192
DOI https://doi.org/10.2147/NDT.S186081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Azusa Shiromaru-Sugimoto,1 Hidetomo Murakami,1 Akinori Futamura,1 Motoyasu Honma,2 Takeshi Kuroda,1 Mitsuru Kawamura,1,3 Kenjiro Ono1
1Division of Neurology, Department of Internal Medicine, Showa University School of Medicine, Tokyo 142-8666, Japan; 2Department of Physiology, Kyorin University School of Medicine, Tokyo 181-0004, Japan; 3Neurology, Okusawa Hospital and Clinics, Tokyo 158-0083, Japan
Background: The relationship between dementia and time perception impairment is unknown.
Aim: This study aims to explore subjective perception of the passage of time in patients with Alzheimer’s disease (AD).
Methods: We conducted semi-structured interviews with 11 AD patients. Grounded theory, a qualitative research methodology, was used for data analysis.
Results: Based on interview transcripts, five categories were designated: {Live according to a private clock}, {The past comes up}, {Move back and forth between the present and the past}, {Cannot imagine the future}, and {Bid farewell to this world as early as tomorrow}.
Discussion: Our results suggest that AD patients alternate past and present without complete awareness and cannot imagine a future other than one ending in death.
Keywords: dementia, grounded theory, neuropsychology, qualitative study, mind time, interview
Introduction
Time perception disorders have been observed in patients with dementia. For example, studies measuring time perception1 and disturbance of age awareness identified dementia patients with a fixed past reality and loss of ability to adjust to present circumstances.2 However, the symptoms and manifestation of time perception disorder are unclear.
Recent, animal and human research has increased understanding of psychological time perception. Human time perception has several features, including simultaneity and continuity, perceived timing and rhythm of movement, temporal order recognition, duration recognition, and time orientation. The symptoms of disorder include timing and calculation (anterograde, retrograde), time orientation and age awareness, and subjective anterograde/retrograde time flow perception.3 Episodic memory plays a prominent role in the perception of the passage of time; a given episodic memory contains elements of “what,” “where,” and “when.” It is unknown whether “when” is unique to humans or is present in other species. However, in humans, the “when” element of episodic memory allows individuals to “psychologically travel to the past” and supports the perception of self.4 In other words, episodic memory not only stores temporally bounded episodes, but also allows subjects to psychologically travel through subjective time, self-affecting consciousness, and perception of self.5 Episodic memory, therefore, not only defines experience of the past, but also influences the present and future based on the past.6
Due to a declining birth rate and a growing number of elderly individuals in super-aged societies, the care of dementia patients poses a significant challenge. Symptoms of dementia such as repetitive requests for food after eating, or the desire to go out for a walk immediately after returning home from a walk – activities that require caregiver assistance – cause problems in nursing-care situations. A subjective time flow perception disorder can in part explain these behavioral problems in dementia patients. The aim of this study is to evaluate subjective time flow perception in patients with Alzheimer’s disease (AD).
To assess the subjective passage of time in AD patients, we conducted exploratory interviews and constructed a model of the perceived flow of time using Grounded Theory (GT). Our aim was to explore the relevance of psychological time perception disorders in AD, to introduce time perception as a novel means of understanding the symptoms of dementia, and to provide a basis for therapeutic strategies.
Methods
Subjects
Eleven patients were diagnosed with AD according to revised NINCDS-ADRDA criteria 87 (February–May, 2015), and chosen as study subjects (Table 1). Written informed consent was obtained from all subjects and caregivers prior to study participation. The study was reviewed by the ethics committee of Showa University Hospital and conducted in accordance with the Declaration of Helsinki.
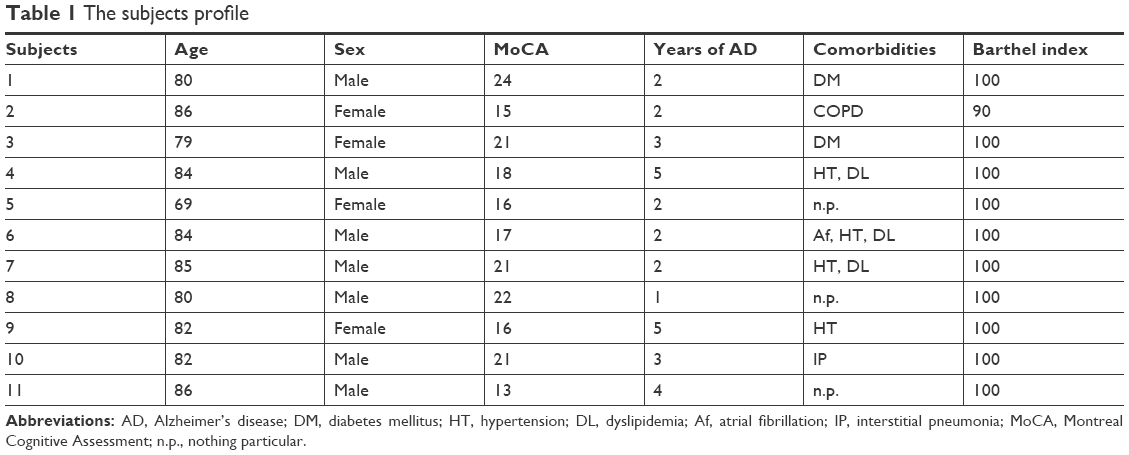 | Table 1 The subjects profile |
Data collection
An exploratory, semi-structured interview was held to assess subjects’ perception of time flow. Answers were recorded in response to the questionnaire shown in Supplementary materials, Appendix 1 for the past, present, and future. Interviews were recorded with the approval of subjects as well families, and conducted in a consulting room by an examiner with the subject, and, when present, subjects’ family members. There was no time limit for answering questions. However, if no voluntary answer was given after more than 30 seconds of silence, the following instruction was planned: “Now, I will repeat the question once again. However, if you cannot form an answer, you may instead answer ‘nothing in particular’.” In the event, we were able to obtain timely, voluntary answers in all cases and the instruction was unnecessary.
Data analysis
Methodology
In this study, recorded interviews were transcribed and we used a qualitative research methodology to achieve our primary study aim. Quantitative research, based on logical positivism, examines phenomena under controlled conditions to eliminate subjectivity.8 This is useful for verifying hypotheses. In contrast, qualitative research is useful for revealing the characteristics of phenomena previously overlooked, and for examining concepts that are not well studied.8 Therefore, a qualitative approach is useful to developing hypotheses prior to quantitative research.8 GT is an inductive methodology that leads to concept categories.9,10 Thus, we can combine GT with a semi-structured interview approach to see how patients with AD create subjective realities.7
Procedures
Data transcribed from interviews were encoded and categorized for analysis. A code was assigned based on the overall meaning of a given discourse, regardless of length. Relevant codes were grouped into categories for comparison.
Our study used trustworthiness, auditability, and appropriacy as quality indicators.
Results
Subjects
Of 11 subjects (four males and seven females), the average age was 81.5±4.2 years, and average cognitive function (as assessed by the Japanese version of the Montreal Cognitive Assessment) was 18.5±3.4 points. Single photon emission computed tomography revealed in all subjects hypoperfusion of the parietotemporal lobe and/or posterior cingulate gyrus for cerebral blood flow. The average interview duration was 67.4±27.1 minutes.
Category creation
During analysis, interview transcriptions for all 11 subjects were categorized, using GT, with attention paid to subjective perception of time flow when talking about present, past, and future. Supplementary materials, Appendix 2 shows the excerpt code book. As a result, five categories were identified: {Live according to a private clock}, {The past comes up}, {Move back and forth between the present and the past}, {Cannot imagine the future}, and {Bid farewell to this world as early as tomorrow}. These categories are described below. Note that, in this manuscript, curly brackets denote a category name, while round brackets represent interviewer statements. Our study did not identify one core category as being a comprehensive framework for all other categories.
Category descriptions
{Live according to a private clock}
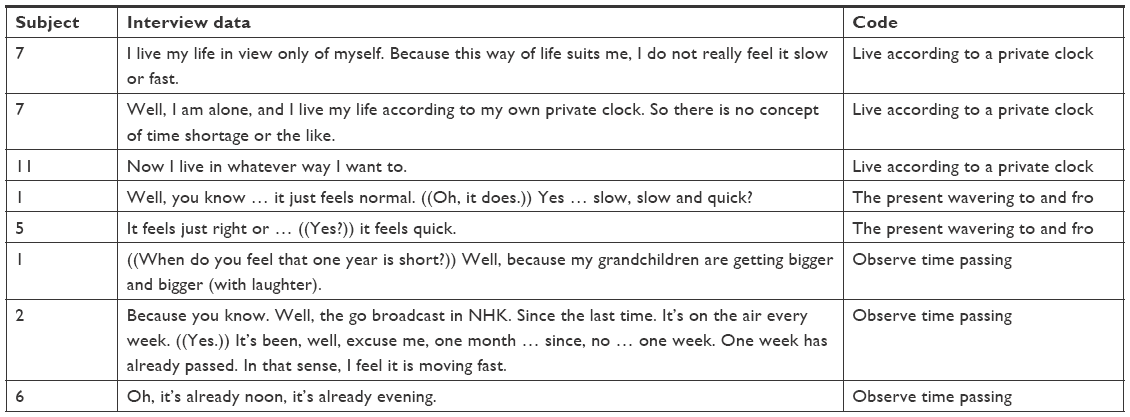
This describes those subjects who live everyday in response to the circumstances of their medical condition. As the subjects were elderly with dementia, many had difficult comorbidities. On the other hand, from a social point of view, the necessity of paying attention to people around them had declined with retirement and a diminishing family role. For example, subject no 7 described the passage of present time as “I live my life according to my own needs. Because this way of life suits me, I do not really feel it is slow or fast.” Furthermore, she said, “Well, I am alone, and I live my life according to my own private clock. So there is no concept of time shortage or the like.” In contrast, subject no 5 stated that “It feels just right or … ((Yes?)) it feels quick” in reference to the present passage of time, indicating that it felt unstable. Subject no 5 provided a reason for this perception, saying, “Listen. After all, I was not able to do what I thought I was going to do … I think that means it passed quickly.”
Subject no 1 explained his inability to grasp the present passage of time in a coherent manner: “Well, you know … it just feels normal. ((Oh, it does.)) Yes … slow, slow and quick?” Then he provided a reason for quickness in reference to the passage of time as reported by others, saying, “Well, because my grandchildren are getting bigger and bigger (with laughter).”
Thus, the present passage of time – perceived according to an internal clock – was fluctuating and witnessing rapid change.
{The past comes up}
Subjects could talk about the past vividly and in-depth, as if it were the present. For example, subject no 5 talked about how memories of the past come to mind, saying, “Sometimes, it comes back to me … gradually in this manner … as if it … it were a story.” Subject no 11 (female) said that, “The memory just … bursts vividly” and talked about the remembered past in detail saying, “Listen. Well … the so-called dotera (a Japanese, traditional full-length garment) in old days? ((Hmm …)) They kindly made a sort of dotera for … for children. ((Oh, yes.)) I carried a baby piggyback, and then put my arms through the sleeve in this manner.”
The past was an experience remembered with intimacy for some subjects. Subject no 1 understood the past as close to him, saying, “It seems I’ve been reminded of it for quite some time. So it might be close.” Thus, subjects were able to remember the details of past memories, although their objective correctness was not evaluated. The past did not feel distant from the present and was recollected in a way that allowed the subjects to reveal themselves to the interviewer.
{Go back and forth between the past and the present}
During the interviews, we observed some subjects alternating between the past and present in their responses to questions that were focused either on the past or the present. For example, although subject no 2 had frequently enjoyed traveling overseas with her partner, she had ceased to travel overseas about 10 years prior due to health concerns. She remembered her time abroad as the past and said, “Well, I cannot say it is close, but it is not so distant either … because even now, I would love to go if I had a chance to.” This suggested that subject’s concept of the present and past was interchangeable. Afterward, the subject described an outbound trip to a destination as distant but an inbound trip from a destination as close; then she returned to discussing her past memory for the remainder of the interview.
On the other hand, subject no 7 talked about the past and emphasized its proximity, saying, “You see. Well … my home has not changed. Naturally, many things also … well, my neighbors also have not changed. At every turn of events, the memory flashes across my mind.” Thus, the past and present were experiences that were not felt in the context of the passage of time (flowing in a unidirectional fashion), but rather as points between which the subjects could move at will.
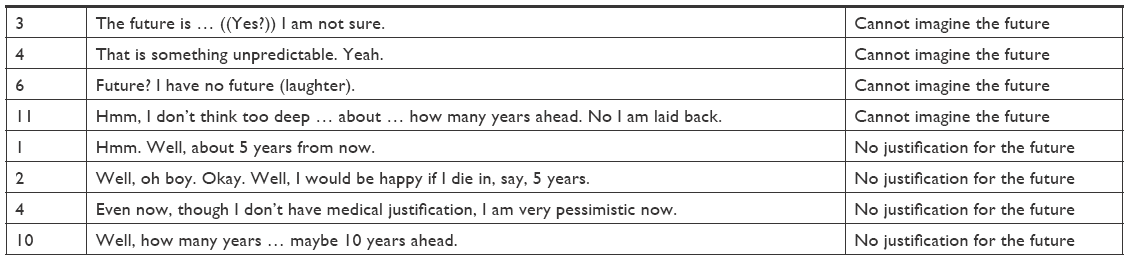
{Cannot imagine the future}
The flow of time toward the future did not feel realistic for subjects and could not be described by subjects in detail. Subject no 3 simply stated, “The future is … ((Yes?)) I am not sure.” Subject no 6 talked about her inability to imagine the future, saying, “Future? I have no future (laughter).” Furthermore, when asked to imagine a future event and tell the interviewer how many years from the present it would take place, subject no 10 replied, “Well, how many years … maybe 10 years ahead,” without suggesting a reason for “10 years” in the context of her speech.
For subject no 4, the future was also unimaginable and something that seemed to persist for a tragically short period without a clear reason, even after trying to remember it. She said, “That is something unpredictable. Yeah. ((Hmm …)) It’s just a feeling I have. To put it into words … ((Yes?)) For some reason, my life, it seems, has come to an end. ((Hmm. Roughly when?)) I am probably too old to say such a thing. Yes. ((Okay. Roughly when do you think it will be?)) Well. ((From your current guess.)) My current … even now, though I don’t have medical justification, I am very pessimistic now. ((Yes.)) Well, my life may not be long. ((Hmm …)) Well, it’s sort of like … no. Uh … is … is this okay? Only just that feeling. It seems that feeling puts me back where I started.”
As seen above, it was difficult for subjects to imagine the future, and they replied to the interviewer’s questions without certainty or strong justifications for their answers. This category shows disturbance of time flow from the present to the future.
{Bid farewell to this world as early as tomorrow}
In this category, subjects experienced the progression of time as an imminent journey to death rather than the passage of time from the present to the future. For example, subject no 5 said, “Oh, but I am going to bid farewell to this world … well, without … without living too long. ((I see.)) I’ve thought about leaving the world as early as tomorrow.” In addition, subject no 9 talked about her life nearing the end rather than continuing into the future, saying, “Moving forward! ((Yes, the future.)) You know. I am short-lived (laughter).” Thus, {bid farewell to this world as early as tomorrow} refers to the experience indicated by subjects during interviews; of readiness to promptly travel to the end of their lives rather than into the living future.
Summary of the results
Table 2 shows frequency of each category as observed for each subject. Furthermore, the normal subjective passage of time experienced by healthy individuals in Figure 1 is contrasted with a model for the subjective passage of time in AD patients proposed in Figure 2.
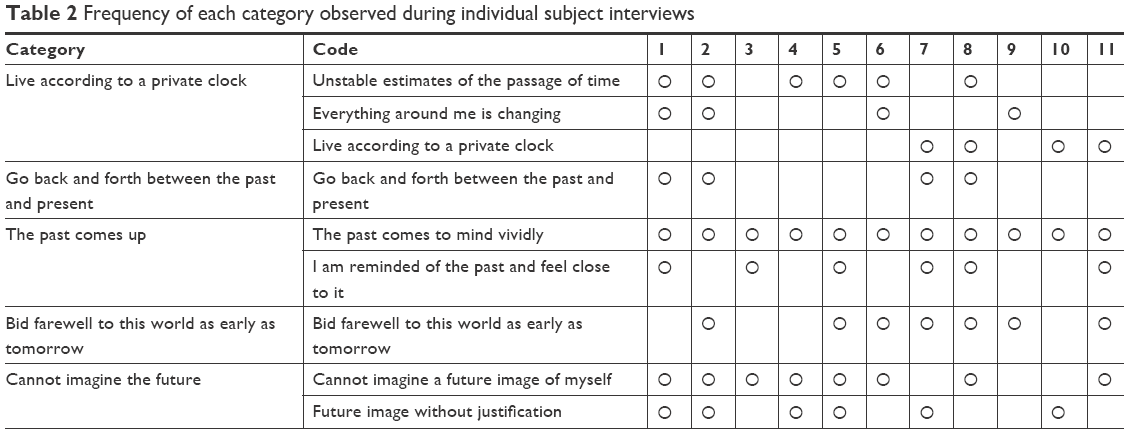 | Table 2 Frequency of each category observed during individual subject interviews |
 | Figure 1 A model of subjective time in normal individuals. |
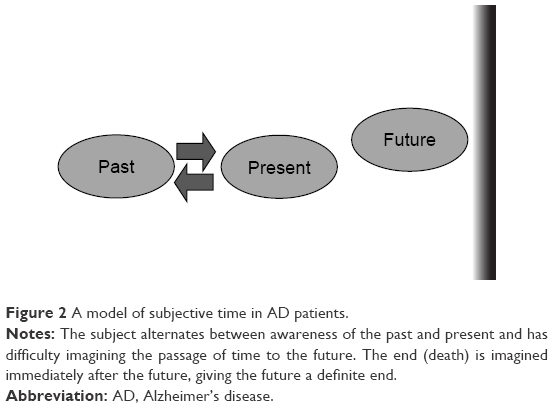 | Figure 2 A model of subjective time in AD patients. |
Discussion
This study was designed to describe alteration of time perception as a symptom of dementia. It is necessary to consider the effects of various AD-related cognitive impairments on the ability of subjects to express their narratives. However, in order to understand patients with dementia and their symptoms, we believe that our results offer an important and novel perspective on the subjective passage of time as experienced by AD patients.
Previous studies have shown that imagining the future vs past events produces activation in the same brain areas, including the medial prefrontal area, precuneus, retrosplenial cortex, medial temporal lobe, lateral temporal lobe, and lateral parietal lobe.9 In this study, completely different processes were observed in AD patients when they imagined the past vs the future. That is, while the past was imagined vividly and as if it were the present, subjects found it difficult to imagine the future. Vivid recollections of the past may also have differed from objective facts due to AD memory impairment. Nevertheless, difficulty describing a concrete image of the future may have been related to a lack of reference, AD-related, or other age-related problems. Importantly, our study does not exclude the possibility that AD patients may not be able to imagine the future. Additional studies are required to evaluate future visualization as a novel symptom of AD-specific time perception.
It has been suggested that the insula is involved in conceptualization of the past, present, and future. Somatosensory information about the body is conveyed to the posterior insula cortex; the latter is transferred to the frontal area and permits momentary self-awareness and the emergence of self-consciousness. When emotions reminiscent of the past are added to this momentary self-awareness, the duration of self-awareness is extended.11 Spiegel et al12 reported thalamic chronotaraxis symptoms associated with lesions in the nucleus dorsomedialis of thalamus, including time disorientation, overstatement or understatement of time duration, and a distorted sense of the passage of time. Time perception is thought to be facilitated by a broad neural network related to other cognitive functions. This network may include the insula and nucleus dorsomedialis of thalamus as well as the medial temporal lobe, and these regions may be affected independently or in tandem with memory deficits in AD.
With regard to the present, AD subjects in this study gave unstable estimates of the current passage of time, described the passage of time in accordance with their own condition, and indicated that they lived according to a private clock. From a psychological perspective, a private clock may function as a buffer between life and perception of self, and as a coping mechanism for enduring memory loss.
Tsukiura suggests that for episodic memory, tagging serves roles that he refers to as “combining” and “distinguishing,” which are important for day-to-day time perception.13 Contextual information, such as time and location in episodic memory, provides multiple elements for tagging and subsequent “combining.”13 The second role that contextual information plays in episodic memory is to distinguish between multiple episodic memories as discrete events in an ordered time series.13 Confabulation is sometimes observed in amnesia caused by lesions in the basal forebrain regions, and may lead to inability to process “time tags” for discrete events in a time series.14,15 In functional brain imaging studies of young healthy adults, basal forebrain has been implicated in the processing of time context in memory, and in using “time tags” to distinguish multiple discrete episodes in a time series.16,17 We hypothesize that AD patients also have impaired tagging functions for “combining” and “distinguishing” episodic memories. There is a disconnection of objective and subjective time, epitomized by “living according to a private clock.” Furthermore, altered tagging functions for “combining” and “distinguishing” the past and present may underlie the categories of {The past comes up} and {Go back and forth between the past and the present}; that is, conflation of, or alternation between, the past and present.
Iwata18 uses the term “kronos time” to discuss the objective passage of time (eg, chronological or sequential time), and “kairos time” to discuss the subjective passage of time (eg, a period or season). While time keeping devices record kronos time, subjective time keeping is kairos time. As kairos time changes with dementia, similar disturbances may also occur in perception of kronos time. Furthermore, disturbances in kairos time and kronos time are, to some degree, correlated. However, establishing a method for directly assessing kairos time as opposed to kronos time is challenging.
Finally, this qualitative research can be discussed in terms of trustworthiness, auditability, and appropriateness. As for trustworthiness, we engaged in the medical treatment of dementia patients and determined a research plan and its details according to this. Notably, we were not able to provide the results of our interview analyses as feedback due to the nature of the outpatient clinic where this research was conducted, because of progressive cognitive impairment in the AD patients. As for auditability, the criteria for subjects and the structure of interviews are clearly outlined in our methods. Furthermore, we provided actual examples for the process of generating categories from codes. For appropriateness, we discussed the present study results in the context of preceding quantitative studies on time perception. To further improve the quality of future studies related to this work, data collection and interpretation might be improved by the creation of a questionnaire based on our findings and their implementation and validation in a clinical context. Moreover, increasing the number of study subjects is critical to future studies.19 In a larger sample, some correlations between the qualitative categories and clinical and/or socio-demographic characteristics of subjects could be analyzed.
Understanding dementia in terms of dysfunctional time perception is a novel idea, and we hope our study leads to better care strategies for patients with dementia.
Acknowledgments
This study was supported by Grant-in-aids for Scientific Research (KAKENHI) for Innovative Areas “The science of Mental Time” (25119006), JSPS KAKENHI grant number 26860677, and KAKENHI 18H05525.
Disclosure
The authors report no conflicts of interest in this work.
References
El Haj M, Moroni C, Samson S, Fasotti L, Allain P. Prospective and retrospective time perception are related to mental time travel: evidence from Alzheimer’s disease. Brain Cogn. 2013;83(1):45–51. | ||
Kuroda T, Futamura A, Sugimoto A, Midorikawa A, Honma M, Kawamura M. Autobiographical age awareness disturbance syndrome in autoimmune limbic encephalitis: two case reports. BMC Neurol. 2015;15:238. | ||
Sugimoto A, Futamura A, Kawamura M. “Kokoro no jikan” no noukairo (Brain circuit in mind’s time). Brain Medical. 2014;26:19–23. | ||
Tulving E. Episodic and semantic memory. Organization of Memory, Tulving E, Donaldson W, editors. New York: Academic Press; 1972:381–403. | ||
Tulving E. Episodic memory: from mind to brain. Annu Rev Psychol. 2002;53:1–25. | ||
Igarashi H, Nomura H, Ikegaya Y. Kako to genzai o tsunagu kioku no kikou. [Memory mechanism that links between the past and the present]. Brain Nerve. 2013;65:933–940. Japanese. | ||
Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007;6(8):734–746. | ||
Glaser B, Strauss A. The Discovery of Grounded Theory. Chicago: Aldine Publishing Co; 1967. | ||
Schacter DL, Addis DR, Buckner RL. Remembering the past to imagine the future: the prospective brain. Nat Rev Neurosci. 2007;8(9):657–661. | ||
Iwakabe S. Rinsho-shinrigaku no shituteki-kenkyu (Qualitative research in clinical psychology). Tokyo: Iwasaki Academic Publisher; 2010. | ||
Craig AD. How do you feel – now? The anterior insula and human awareness. Nat Rev Neurosci. 2009;10(1):59–70. | ||
Spiegel EA, Wycis HT, Orchinik C, Freed H. Thalamic chronotaraxis. Am J Psychiatry. 1956;113(2):97–105. | ||
Tsukiura T. Kioku ni okeru jikan-bunmyaku no shori wo ninau nounai-kikou to sono shogai. [Brain mechanism that processes time context in memory and its deficits]. Shinkei Chiryo-gaku. 2015;32:373–377. Japanese. | ||
Eichenbaum H. Memory on time. Trends Cogn Sci. 2013;17(2):81–88. | ||
Tranel D, Jones RD. Knowing “what” and knowing “when”. J Clin Exp Neuropsychol. 2006;28(1):43–66. | ||
Fujii T, Suzuki M, Okuda J, et al. Neural correlates of context memory with real-world events. Neuroimage. 2004;21(4):1596–1603. | ||
Schnider A, Treyer V, Buck A. Selection of currently relevant memories by the human posterior medial orbitofrontal cortex. J Neurosci. 2000;20(15):5880–5884. | ||
Iwata M. Kanjiru jikan to hakaru jikan: Jikan no kenkyu shoshi. [Time that is felt and time that is measured: Short history of study on time]. Brain Medical. 2014;26:57–63. Japanese. | ||
Morrow SL, Susan L. Quality and trustworthiness in qualitative research in counseling psychology. J Couns Psychol. 2005;52(2):250–260. |
Supplementary materials
Appendix 1: Interview instructions and the questionnaire
1. Instruction
Now, I would like to ask you several questions about your present, past, and future. Please feel free to express your current feelings.
2. Questionnaire
1) I will ask you about your present.
Do you find the current flow of time to be slow or fast?
How about the time passing in a day (sleep–wake cycle and diet intervals, etc.)?
How about the time passing in a year (ceremonies and seasonal transitions)?
Or, is there anything that you feel about the present passage of time other than that it is slow or fast?
When do you have this feeling?
2) I would like to ask you about the past.
Please recall the past. What comes to your mind? When did it happen?
Do you feel that the past is distant or close?
3) I would like to ask you about the future.
Please imagine your future. What do you imagine? When will it happen?
Do you feel that the future is distant or close?
If no voluntary response is given after more than 30 seconds of continued silence, or if the response is off-topic:
“Now, I will repeat the question once again. However, if you cannot form an answer, you may instead answer ‘nothing in particular’.”
Appendix 2: The excerpt code book
 | 1. {Live according to a private clock} |
 | 2. {The past comes up} |
 | 3. {Go back and forth between the past and the present} |
 | 4. {Cannot imagine the future} |
 | 5. {Bid farewell to this world as early as tomorrow} |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.