Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Social Problems of Morbidly Obese Patients on a Community Level: A Cross-Sectional Study in Saudi Arabia
Authors Kazim AH, Al-Ruwaybiah AM, Al-Naami MY, Aldohayan A, Binjaloud AA, Alarfaj MA
Received 24 March 2022
Accepted for publication 30 June 2022
Published 15 July 2022 Volume 2022:15 Pages 2061—2075
DOI https://doi.org/10.2147/DMSO.S366358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Albaraa H Kazim,1,* Afnan Mohammed Al-Ruwaybiah,2,* Mohammed Y Al-Naami,3 Abdullah Aldohayan,4 Ahmed A Binjaloud,4 Mosab A Alarfaj5
1Bariatric and Upper Gastro-Intestinal Surgery Unit, King Saud University, Riyadh, Saudi Arabia; 2Department of Social Studies, King Saud University, Riyadh, Saudi Arabia; 3Surgery Department, King Saud University, Riyadh, Saudi Arabia; 4Department of Surgery, King Saud University, Riyadh, Saudi Arabia; 5Department of Surgery, King Fahad Hospital of University, Imam Abdulrahman Bin Faisal University, Al-Khobar, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Albaraa H Kazim, Bariatric and Upper Gastro-Intestinal surgery Unit, King Saud University, Riyadh, Saudi Arabia, Tel +996 6555569875, Email [email protected]
Objective: To identify the predictors and social problems of obese patients in Saudi Arabia.
Methods: A cross-sectional study was conducted for the period between July 2016 and January 2017. The study population consisted of obese patients visiting the surgery clinics following the medical examinations required before obesity surgery. Patients were recruited from four main medical centres in Riyadh: King Fahad Medical City, University Medical City-King Khalid University Hospital, King Abdulaziz Medical City in the National Guard, and Prince Sultan Military Medical City. The study questionnaire tool was developed based on extensive literature. The questionnaire tool explored personal and demographic characteristics of obese patients and the social problems that morbidly obese patients suffer from at the community level. Logistic regression analysis was used to identify predictors of those facing social problems.
Results: A total of 374 patients completed the questionnaires. We found that having a bachelor’s degree, a body mass index (BMI) of 40 kg/m2 and above, and other comorbidities were important predictors that increased the likelihood of having social problems related to obesity on a community level (p< 0.05). On the other hand, having a high income (11,000 SR/per month and above) was a protective factor that was associated with lower odds of having social problems related to obesity on a community level (p< 0.05).
Conclusion: Obese patients with low socioeconomic status, having a bachelor’s degree, and those with comorbidities tend to have social problems. Future studies to investigate the predictors or social problems among obese patients on a larger scale are warranted.
Keywords: obese, problem, Saudi Arabia, social
Introduction
Obesity is one of the most widespread modern-day conditions that has affected many countries in the past decade.1 It is a multifactorial medical condition and can be considered a health problem of different dimensions.1 It is linked to an imbalance in energy intake and expenditure, as well as physical inactivity.2,3 The World Health Organization defines “overweight” as a condition in which the average body mass index (BMI) is 25 kg/m2 or more, and “obesity” is defined as a condition in which the average BMI is 30 kg/m2 or more.4 Obesity places huge pressure on public and specialised health institutions in terms of costs and the quality of services, which may lead to a deficiency in the services provided to society members in general.5 Obesity is a major public health challenge because it is linked to many other health problems, such as cancer. In addition, obesity is an independent risk factor for multiple comorbidities, including hypertension, type 2 diabetes, sleep disorders, breathing difficulties and heart diseases.6
The prevalence of obesity has nearly tripled since 1975, reaching a pandemic level with more than 1.9 billion adults in 2016 being either overweight or obese. It is estimated that by 2030, two-thirds of the world’s population will be overweight and 20% will be obese.7 As for the Kingdom of Saudi Arabia, despite the lack of accurate statistics on obesity, many recent studies have shown that the rate of obesity in Saudi society has increased rapidly enough to become a cause for concern.8 In a study in Jeddah, Saudi Arabia, the authors reported that the prevalence of overweight and obesity was 35.1% in males and 34.8% in females, and 30.1% in males and 35.6% in females, respectively.8 In another recent nationwide study, the authors reported that the national weighted prevalence of obesity (BMI≥30kg/m2) was 24.7%, and the prevalence in the sample (unweighted) was 21.7%.9
Obesity is also associated with social and psychological problems, including low self-esteem, low social competence, lack of adaptation, social isolation, unemployment, low socioeconomic status, and poor quality of life.10 Previous studies have reported increased social discrimination toward obese patients, especially those who are younger.11 Obese patients may face prejudice or discrimination in multiple settings, including in the job market, at school, or in other social situations, which may lead to mental health issues such as depression and anxiety.12 Most previous studies in the Middle East in general and in Saudi Arabia specifically focused on health problems associated with obesity, with limited focus on the social impact. Understanding the social impact on obese people is important to reducing obesity stigma. Previous studies investigating the social problems faced by obese people in Saudi Arabia are limited. Therefore, in this study, we aimed to identify the social problems faced by obese people in Saudi Arabia.
Method
Study Design
A cross-sectional study was conducted for the period between July 2016 and January 2017.
Study Population
The study population consisted of obese patients reviewing the surgery clinics following the medical examinations required before obesity surgery. Patients were recruited from four main medical centres in Riyadh: King Fahad Medical City, University Medical City-King Khalid University Hospital, King Abdulaziz Medical City in the National Guard, and Prince Sultan Military Medical City.
Study Sample
A purposive sampling technique was employed in this study to recruit the study participants to be involved in this study. Our sample was comprised of obese patients who were reviewing the surgery clinics to follow up on the medical examinations required to perform obesity operations during the study period.
The Questionnaire Tool
The study questionnaire tool was developed based on extensive literature. The questionnaire consisted of three parts. The first part dealt with the baseline sociodemographic characteristics of the study sample represented by gender, age, nationality, place of residence, educational level, marital status, occupational status, nature of work, and level of monthly income. The second part dealt with the personal characteristics of obese patients, which consisted of body mass index, the period of diagnosis with obesity, the presence of diseases associated with obesity, family members who have obesity, attempts to treat obesity before transferring to an obesity surgery clinic, attempts to treat obesity and the reason for performing surgery to treat obesity. The third part consisted of 20 items that explored the social problems that morbidly obese patients suffer from at the community level, particularly psycho-emotional features of the patients (feeling inferior, poor self-esteem, anxiety, isolation, frustration, sadness, pathological depression, and lack of self-confidence). Patients’ responses ranged from 1 to 5, where 1 means “never” and 5 means “always”. The total possible score for the social problems sub-scale ranged from 20 to 100. The higher the score, the more likely that the patient experienced social problems at the community level.
Instrument Reliability and Validity Procedures
Validity of the Tool
After preparation of the questionnaire, the researcher presented it in its initial form to a group of referees specialised in scientific research: professors, faculty members of the Department of Social Studies at King Saud University and Imam Muhammad bin Saud Islamic University, and social workers, to ensure the face validity of the tool. The arbitrators expressed their opinion on the clarity of the statements, their suitability for what they were measuring, and the appropriateness of the statements for the axis to which they belong. They also suggested amendments to the wording of the questionnaire phrases.
Questionnaire Internal Consistency, Validity, and Stability
After confirming the apparent validity of the study tool, the researcher applied the tool to 20 individuals from the study sample randomly to ensure the validity of the psychometric questionnaire in the field because it was not possible to conduct an exploratory sample before starting the study. Based on the sample data, the researcher calculated the Pearson correlation coefficient to find out the internal validity of the questionnaire, where the correlation coefficient was calculated between the degree of each of the terms of the study tool and the total degree of the social problems at the community level, as shown in the following Table 1:
 |
Table 1 Pearson Correlation Coefficients for the Questionnaire Items |
Sample Size
Using a 95% confidence interval, a 5.0% margin of error, and an estimated 35.0% obesity prevalence rate, the minimum required sample size is 349 participants.
The formula used to calculate sample size is given as:

Where Z = z- value; C = confidence interval; and p = percentage population (or prevalence)
Ethical Approval
Approval for this study was obtained from the ethics committee at King Saud University, Riyadh, Saudi Arabia and the participating healthcare centres (Ref: 005-08-2018-EM, 16/0304/IRB, IRB00010471, HAP-01-R-015). Informed consent was obtained from the study participants prior to study commencement. For participants under 18 years of age, approval was granted by their parents/caregivers. This study was conducted in compliance with the World Medical Association (WMA) Declaration of Helsinki.
Statistical Analysis
The SPSS software, version 27, was used to analyze the data. For quantitative variables, descriptive analysis was reported as mean (standard deviation [SD]). Both tests yielded statistically insignificant results (p > 0.5), indicating that the data were normally distributed. Categorical data were presented in the form of percentages and frequencies. Patients’ social problems scores were interpreted as a continuous scale based on the scale midpoint, where a score above the midpoint identified a greater degree of the social problem encountered by the patient. The Student’s t-test/ANOVA were used to compare the mean scores between different demographic groups. Logistic regression was used to estimate odds ratios (ORs) with 95% confidence intervals (CIs) for predictors of social problems at a community level. Logistic regression was carried out using the mean social problem score of the study sample as a cut-off point (57.1). A confidence interval of 95% (p<0.05) was applied to represent the statistical significance of the results, and the level of significance was assigned as 5%. The Pearson correlation coefficient calculates the validity of the internal consistency of the study tool.
Results
Characteristics of Study Participants
A total of 374 patients participated in this study, of which 59.1% were females. The majority of them (72.7%) were aged under 40 years. The majority (79.4%) were living in the capital of the Kingdom of Saudi Arabia, Riyadh. Around half of them (47.6%) had a bachelor’s degree. A total of 65.5% were married, of which 81.2% reported having children. More than half of them (54.0%) were employed. More than one-quarter (27.3%) of the study sample reported that they work in administrative work, with a similar percentage (23.8%) reporting that their work is mainly office-based. Around 31.0% of the patients reported that their income category was less than 3000 Saudi Riyal (SR) per month. For further details on the demographic characteristics of study participants, refer to Table 2.
 |
Table 2 Demographic Characteristics of Study Participants |
Participants’ Clinical Profile
The majority of the study participants (70.1%) reported that they have a family member who suffers from obesity, of which around 50.0% reported that their brother/sister suffers from obesity. The vast majority of the study participants (80.2%) reported that their BMI was 40 kg/m2 or above. Around 60.0% of the participants reported that they were diagnosed with obesity more than 5 years ago. Around 27.0% of the participants reported that they had difficulty with movement. The most commonly reported comorbidities were diabetes mellitus, hypertension, and sleep apnoea. For further details on the clinical profile of the study participants, refer to Table 3.
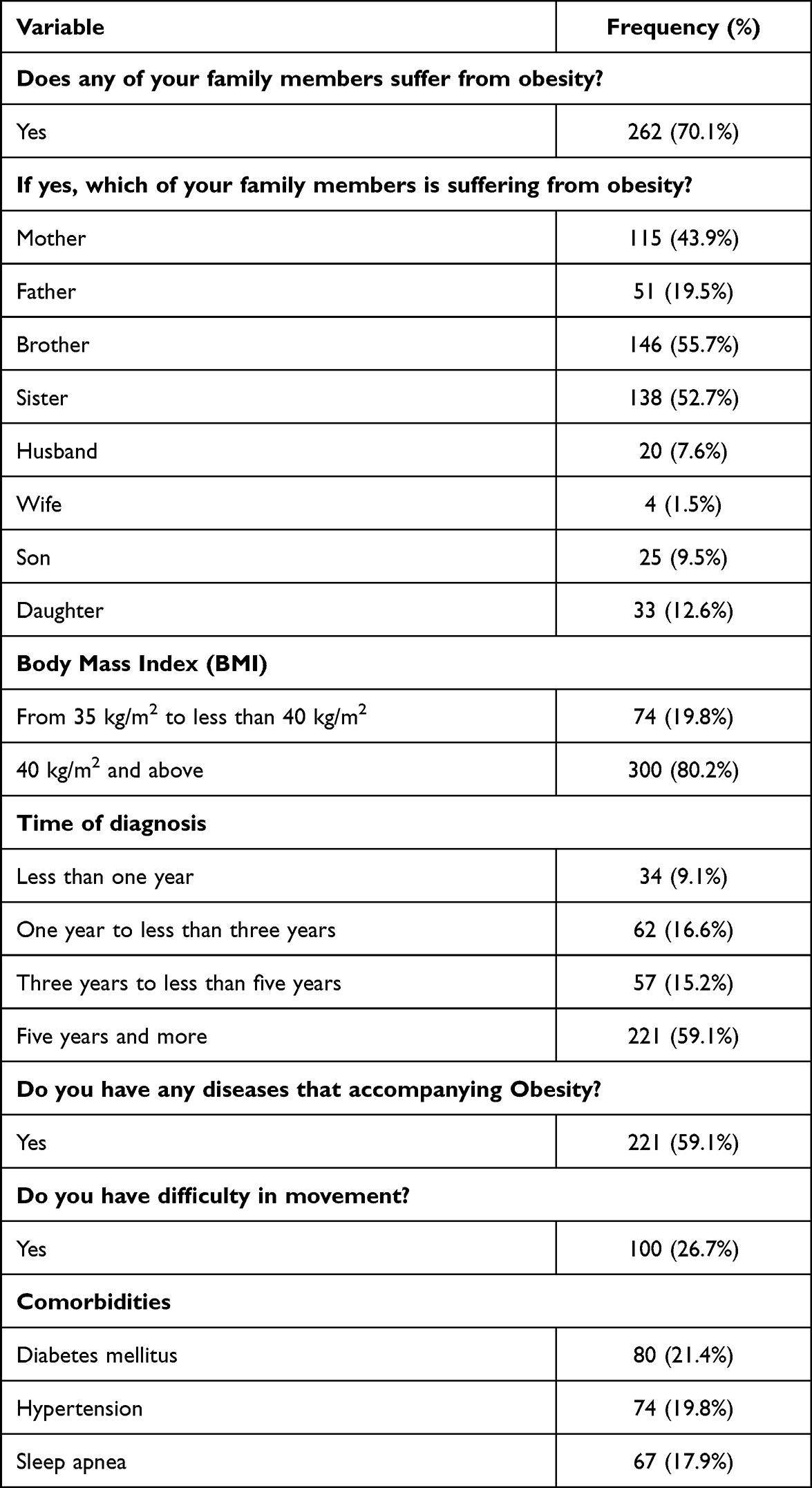 |
Table 3 Participants’ Clinical Profile |
Attempts to Treat Obesity Before Being Referred to an Obesity Surgery Clinic
When the participants were asked whether they had attempted to treat obesity before being referred to obesity surgery clinics, the vast majority (88.5%) of them confirmed that they had tried to do so. The most commonly reported obesity management procedure was dieting under medical supervision. When the participants were asked about the reason for choosing surgery for obesity treatment, the vast majority (84.2%) of the participants reported that this was due to health problems related to obesity. For further details on obesity treatment attempts and reasons for choosing surgery as a management option, refer to Table 4.
 |
Table 4 Obesity Treatment Attempts and Reasons for Choosing Surgery as a Management Option |
Obesity and Social Problems
When the patients were asked about the social problems that they face at the community level, a wide variety of problems were reported, of which the most common were: being exploited in advertisements as a marketing method for consumable products and restaurants, lacking suitable places in which to do sports, being annoyed by a negative image of obese patients’ personalities in series and programmes. For further details on social problems that patients face at the community level, refer to Figure 1.
 |
Figure 1 Social problems that patients face at the community level. |
Predictors of Social Problems at the Community Level
The overall level of social problems among the study participants on the community level was moderate, with a mean social problem score of 57.1 out of 100, representing 57.1%. The total social problem score among the study participants ranged from 20 to 100. The mean social problem scores significantly differed between study participants based on income category, BMI level, and whether the patients reported having difficulty in movement (p<0.05). For further details on the mean social problem score stratified by participants’ characteristics, refer to Table 5.
 |  |  |
Table 5 Mean Social Problem Score Stratified by Participants Characteristics |
Using binary logistic regression analysis, we identified that having a bachelor’s degree, a BMI of 40 kg/m2 or above, and other comorbidities were important predictors that increased the likelihood of having social problems related to obesity on the community level (dependent variable) (p<0.05). On the other hand, having a high income (11,000 SR/per month and above) was a protective factor that was associated with lower odds of having social problems related to obesity at the community level (p<0.05). For further details on the binary logistic regression analysis findings, please refer to Table 6.
 |  |  |
Table 6 Binary Logistic Regression Analysis |
Discussion
In this cross-sectional survey, we investigated the social problems among obese patients in a surgery clinic in Saudi Arabia. We found that having a bachelor’s degree, a BMI of 40 kg/m2 or above, and other comorbidities were important predictors that increased the likelihood of having social problems related to obesity at the community level (p<0.05). On the other hand, having a high income (11,000 SR/per month and above) was a protective factor that was associated with lower odds of having social problems related to obesity at the community level (p<0.05).
Previous studies have linked poor socioeconomic status with health outcomes. People with lower educational levels and low income are associated with a worse quality of life and health status.13–15 Recent results from a study in Saudi Arabia reported that people with a low income were associated with obesity.8 In our study, we used the same methodology and a similar population, and our results were consistent with the previous study. We found that people with a low income were associated with a poorer social life. In another study in Denmark, the authors investigated the socioeconomic impact of obesity by estimating the associated direct and indirect costs at the individual level. They found that one BMI unit above 30 kg/m2 was associated with a 2% reduction in income.16 These findings can be explained by the fact that people with low socioeconomic status tend to have poor lifestyle behaviours, including drinking, smoking, lack of exercise, and poor sleep quality.17,18 These are all risk factors for poor quality of life and poor health outcomes, including obesity and other chronic comorbidities. Another noteworthy finding from our research was that people with bachelor’s degrees were more likely to suffer social problems related to obesity in their communities. Bachelor’s degree holders are more likely to interact with other professionals and educated individuals. This makes individuals more conscious of their appearance in public, and obesity becomes a stressful factor for them, resulting in social problems.
This study showed that the presence of comorbidities is associated with a poorer quality of life among patients with obesity. It is well known that comorbidities are associated with a worse quality of life and health status.19 Obesity has been linked as a risk factor to the development of multiple comorbidities, and it often coexists with other diseases, including metabolic syndromes, which include diabetes, dyslipidemia, and obesity.20 Patients with two or more diseases and patients with metabolic syndrome have a higher risk of developing cardiac diseases and hospital admissions.21 In addition, the quality of life of these patients is sometimes restricted due to mobility problems, which may also affect their social life.
Despite that 42.2% of the population in Saudi Arabia is females and the majority are males,22 most of the patients who went for bariatric surgery in our study were females. Our study also showed that around 60% of the study sample were females. A previous study that conducted a retrospective analysis of data on bariatric surgery in the United States from 1998–2010 reported that 80% of the patients who went for bariatric surgery were females. The authors also reported that sociodemographic and cultural factors could be related to this difference in proportion.23 Females tend to have better awareness, perception, and knowledge of the complications of obesity, which may be a reason for this difference. However, our study did not investigate this finding, and we urge future studies to investigate this gap in knowledge. The results of this study may help healthcare providers identify those obese patients at a higher risk of developing social problems. Providing awareness, support, and health services for this category of patients may be necessary to avoid future social or psychological complications.
To the best of our knowledge, this study is the first in Saudi Arabia that has investigated the social problems among patients with obesity. We included patients from four main hospitals in the city of Riyadh, which has a population of more than 8 million. Therefore, we assume that the results of our study can be generalised to the population of Saudi Arabia. However, our study also has some limitations. Due to the nature of the study design of this cross-sectional survey, we were not able to determine any causality between the study variables. In addition, there are no other studies that investigate the social problems among patients with obesity in Saudi Arabia; so we were not able to compare our findings with a population with similar characteristics. Finally, we tested our newly constructed (non-standardized) questionnaire instrument on a small set of participants from the target population without any further validation processes. As a result, our findings should be interpreted carefully.
Conclusion
This is the first study to investigate the social problems among patients with obesity. Obese patients with low socioeconomic status, those with a bachelor’s degree, and those with comorbidities tend to have social problems. Future studies to investigate the predictors of social problems among obese patients on a larger scale are warranted.
Acknowledgment
Albaraa H. Kazim and Afnan Mohammed Al-Ruwaybiah have equal contribution in this study and should be considered joint first author.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10. doi:10.1016/j.metabol.2018.09.005
2. Vandevijvere S, Chow CC, Hall KD, et al. Increased food energy supply as a major driver of the obesity epidemic: a global analysis. Bull World Health Organ. 2015;93(7):446–456. doi:10.2471/BLT.14.150565
3. Theodorou M, Kabir R. Exploring the effects of cold-water swimming on obese population: a systematic review. J Appl Sports Sci. 2019;2(December):3–21. doi:10.37393/jass.2019.02.1
4. World Health Organization. Obesity and overweight. 2020 [
5. Grundy SM. Multifactorial causation of obesity: implications for prevention. Am J Clin Nutr. 1998;67(3):563s–572s. doi:10.1093/ajcn/67.3.563S
6. Larsson U, Karlsson J, Sullivan M. Impact of overweight and obesity on health-related quality of life—a Swedish population study. Int J Obes. 2002;26(3):417–424. doi:10.1038/sj.ijo.0801919
7. Hruby A, Hu FB. The epidemiology of obesity: a big picture. PharmacoEconomics. 2015;33(7):673–689. doi:10.1007/s40273-014-0243-x
8. Al-Qahtani AM. Prevalence and predictors of obesity and overweight among adults visiting primary care settings in the southwestern region, Saudi Arabia. Biomed Res Int. 2019;2019:1–6. doi:10.1155/2019/8073057
9. Althumiri NA, Basyouni MH, AlMousa N, et al. Obesity in Saudi Arabia in 2020: prevalence, distribution, and its current association with various health conditions. Healthcare. 2021;9(3):1–8.
10. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–298. doi:10.1038/s41574-019-0176-8
11. Puhl R, Brownell KD. Bias, discrimination, and obesity. Obes Res. 2001;9(12):788–805. doi:10.1038/oby.2001.108
12. Wellman N, Friedberg B. Causes and consequences of adult obesity: health, social and economic Impacts in the United States. Asia Pac J Clin Nutr. 2002;11(Suppl 8):S705–S709. doi:10.1046/j.1440-6047.11.s8.6.x
13. Wang J, Geng L. Effects of socioeconomic status on physical and psychological health: lifestyle as a mediator. Int J Environ Res Public Health. 2019;16(2):1–9.
14. Adler NE, Newman K. Socioeconomic disparities in health: pathways and policies. Health Aff. 2002;21(2):60–76. doi:10.1377/hlthaff.21.2.60
15. Signorello LB, Cohen SS, Williams DR, et al. Socioeconomic status, race, and mortality: a prospective cohort study. Am J Public Health. 2014;104(12):e98–e107. doi:10.2105/AJPH.2014.302156
16. Kjellberg J, Tange Larsen A, Ibsen R, et al. The socioeconomic burden of obesity. Obes Facts. 2017;10(5):493–502. doi:10.1159/000480404
17. Kushner RF. Weight loss strategies for treatment of obesity: lifestyle management and pharmacotherapy. Prog Cardiovasc Dis. 2018;61(2):246–252. doi:10.1016/j.pcad.2018.06.001
18. Kurth T, Moore SC, Gaziano JM, et al. Healthy lifestyle and the risk of stroke in women. Arch Intern Med. 2006;166(13):1403–1409. doi:10.1001/archinte.166.13.1403
19. Xuan J, Kirchdoerfer LJ, Boyer JG, et al. Effects of comorbidity on health-related quality-of-life scores: an analysis of clinical trial data. Clin Ther. 1999;21(2):383–403. doi:10.1016/S0149-2918(00)88295-8
20. Canale MP, Manca Di Villahermosa S, Martino G, et al. Obesity-related metabolic syndrome: mechanisms of sympathetic overactivity. Int J Endocrinol. 2013;2013:1–13. doi:10.1155/2013/865965
21. Han TS, Lean ME. A clinical perspective of obesity, metabolic syndrome and cardiovascular disease. JRSM Cardiovasc Dis. 2016;5:1–13. doi:10.1177/2048004016633371
22. Blogger GMI. Saudi Arabia population statistics 2022. 2022; Available from: https://www.globalmediainsight.com/blog/saudi-arabia-population-statistics/#:~:text=In%20Saudi%20Arabia%2C%20the%20male%20population%20is%2020.70,UAE%20and%20Saudi%20Arabia.%20Saudi%20Population%20by%20Age.
23. Fuchs HF, Broderick RC, Harnsberger CR, et al. Benefits of bariatric surgery do not reach obese men. J Laparoendosc Adv Surg Tech A. 2015;25(3):196–201. doi:10.1089/lap.2014.0639
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.