Back to Journals » International Journal of General Medicine » Volume 14
The Sagittal Parameters and Efficacy of Pedicle Subtraction Osteotomy in Patients with Ankylosing Spondylitis and Kyphosis Under Different Lumbar Sagittal Morphologies
Authors Zhang PC, Deng Q ![]() , Sheng WB, Guo HL, Mamat M, Luo YX, Gao ST
, Sheng WB, Guo HL, Mamat M, Luo YX, Gao ST
Received 19 November 2020
Accepted for publication 14 January 2021
Published 5 February 2021 Volume 2021:14 Pages 361—370
DOI https://doi.org/10.2147/IJGM.S292894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Peng-Chao Zhang, Qiang Deng, Wei-Bin Sheng, Hai-Long Guo, Mardan Mamat, Yun-Xiao Luo, Shu-Tao Gao
Department of Spine Surgery, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, People’s Republic of China
Correspondence: Qiang Deng
Department of Spine Surgery, The First Affiliated Hospital of Xinjiang Medical University, No. 137 of Liyushan South Road, Xinshi District, Urumqi, 830054, People’s Republic of China
Tel +86 13325636562
Email [email protected]
Objective: This study aimed to compare the changes in sagittal parameters and the efficacy of pedicle subtraction osteotomy (PSO) in patients with ankylosing spondylitis (AS) and kyphosis under different lumbar sagittal morphologies and to explore the effect of sagittal morphology on the selection of PSO levels.
Methods: A total of 24 patients with AS and thoracolumbar kyphosis (TK) who were admitted to the First Affiliated Hospital of Xinjiang Medical University between 2008 and 2019 were enrolled in this study. They were divided into two groups: a lumbar lordosis group (n = 14) and a lumbar kyphosis group (n = 10). Changes in sagittal parameters, lumbar Japanese Orthopaedic Association (JOA) scores, and visual analog scale (VAS) scores for lumbar pain before and after operation were compared between the two groups to evaluate postoperative efficacy.
Results: The preoperative lumbar lordosis (LL) was − 29.29 ± 5.40 (lordosis) and 13.50 ± 3.65 (kyphosis) (P < 0.01), and the preoperative sagittal vertical axis (SVA) was 171.35 ± 25.46 (lordosis) and 223.58 ± 21.87 (kyphosis) (P < 0.01). Preoperative global kyphosis (GK) was 75.71 ± 5.26 (lordosis) and 86.30 ± 10.32 (kyphosis) (P < 0.05). All patients in the lordosis group underwent PSO surgery at the twelfth thoracic vertebra (T12) or the first lumbar spinal vertebra (L1), while all patients in the kyphosis group underwent the surgery at the second or third lumbar spinal vertebra (L2 or L3). The differences in postoperative GK, LL, and SVA between the two groups were not significant (P > 0.05). The JOA scores of the two groups increased from 13.00 ± 0.83 (lordosis) and 11.30 ± 0.93 (kyphosis) before surgery to 21.00 ± 0.67 and 19.70 ± 0.60 after surgery (P < 0.05).
Conclusion: Preoperative lumbar sagittal morphology needs to be considered when selecting the optimal osteotomy plane. An osteotomy can achieve the greatest success in patients with lumbar kyphosis at L2/L3; for patients with lumbar lordosis, it can achieve satisfactory outcomes at T12/L1.
Keywords: ankylosing spondylitis, kyphosis, sagittal parameters, PSO, osteotomy
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease characterized by invasion of the axial spine. Approximately 30% of sufferers will develop severe kyphosis1 and may go on to develop intra-abdominal complications.2–5 For patients with AS and kyphosis, the main purpose of surgical intervention is to reconstruct sagittal balance and restore horizontal gaze function.2–5 In recent years, pedicle subtraction osteotomy (PSO) has been used more frequently in clinical practice and has been found to achieve satisfactory correction and sagittal recovery results and to significantly improve the quality of life of these patients.6–10
Choosing the most suitable osteotomy plane is a key factor in achieving good results with PSO. Jackson et al11 reported that the osteotomy plane has a ⅔ angle focused on the fourth lumbar vertebra to the sacral base (L4–S1) for patients with AS and thoracolumbar kyphosis (TK). Roussouly et al12 studied four spinal features in healthy people and found that lumbar lordosis mainly relies on the third to fifth lumbar spinal vertebra (L3–L5). When considering the problem of upper and lower fixation of the osteotomy plane, it is more appropriate to undertake osteotomy at L3 or L4, as it can restore the physiological lordosis of the lumbar vertebrae. However, Qian13 and Chen et al6 have pointed out that when the apex of the kyphosis is located in the thoracolumbar segment, the osteotomy should be carried out at the apex of the kyphosis. The most successful corrective effect of osteotomy is usually achieved at the first lumbar spinal vertebra (L1). Moreover, Liu et al14 stated that osteotomy is not recommended at L3 because it reduces the patient’s standing function. Another study15 of PSO surgery for the treatment of AS with TK has indicated that a lower osteotomy level can achieve more effective sagittal correction due to the leverage.
Although PSO has been extensively discussed in previous literature, there is no definitive conclusion on the optimal osteotomy level of the surgery. Previous studies15 have revealed that surgical decision making as to the osteotomy level depends largely on preoperative lumbar sagittal morphology. However, it has also been reported that pelvic incidence (PI) becomes mismatched with lumbar lordosis (LL) after PSO surgery.16 The conclusions drawn in the literature are sometimes inconsistent; therefore, this study aimed to investigate the lumbar sagittal morphology of patients with AS, with emphasis on the effect of lumbar sagittal morphology on the selection of the most effective osteotomy plane for PSO surgery.
Patients and Methods
Inclusion and Exclusion Criteria
The cases of 24 patients with AS and TK who were admitted to the First Affiliated Hospital of Xinjiang Medical University between 2008 and 2019 were retrospectively analyzed. All AS diagnoses were based on the revised New York Standard.17
Inclusion criteria: (1) Patient had been diagnosed with AS and kyphosis by symptoms, signs, and imaging examination; (2) patient had undergone PSO; (3) patient had undergone an anteroposterior and lateral film of the whole spine before and after surgery; (4) patient had at least one year of follow-up.
Exclusion criteria: (1) Kyphosis was caused by other disease factors; (2) AS was complicated by pathological fractures; (3) AS was complicated by cervical or thoracic kyphosis (in patients with lumbar lordosis, the main pathology was thoracic); (4) patient had incomplete follow-up materials.
Grouping: The lumbar sagittal morphology in the whole-spine lateral radiographs was observed. The patients with different lumbar sagittal morphology were divided into two groups based on the LL Cobb angle: a lumbar lordosis group (LL < 0°; n = 14) and a lumbar kyphosis group (LL > 0°; n = 10).
The study was conducted in accordance with the Declaration of Helsinki (2013 revision) and approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (NO.K202010-17). Informed consent was obtained from all patients.
Procedure
Theoretically, in patients with AS and vertebral fusion up and down, setting is not easy to open; SPO bone cutting should not be used, as forcibly cutting the bone has a high risk of vascular complications, such as nerve damage. Three-dimensional reconstruction using CT scans showed lumbar anterior column ossification and incomplete fusion, so the front is a activity, through posterior column shortening can be finished in front of open, so we are in the L5 and S1, L4 and L5, L1 and L2 SPO osteotomy, use bit except to cut bone rongeur clearance of spinous process and ligament between the spine, spine, and remove the bilateral joints. Then, the lamina, ligamentum flavum and superior articular process were bit off with lamina osteotomy forceps, and the pedicle osteotomy was retained. Finally, the posterior column was compressed to open the front and the sagittal shape of the lumbar lordosis was corrected and restored.
Data Evaluation
Surgimap software was used to measure the preoperative and postoperative sagittal vertical axis (SVA), global kyphosis (GK), PI, pelvic tilt (PT), sacral slope (SS), LL (negative value: lordosis, positive value: kyphosis), and sagittal parameters in the lateral X-ray of the whole spine when standing up. Clinical data, including age, sex, lumbar Japanese Orthopaedic Association (JOA) scores, visual analog scale (VAS) scores for lumbar pain, and complications, were reviewed at the final follow-up.
Statistical Analysis
All data were calculated using SPSS v.22 software. A paired sample t-test was used to compare preoperative and postoperative data and final follow-up results. An independent sample t-test was used to determine the difference in radiological outcomes between the two groups. P < 0.05 was considered statistically significant.
Results
A total of 24 AS patients were enrolled from 2008 to 2019, including 14 patients in the lumbar lordosis group with a mean age of 39.2 years and ten patients in the lumbar kyphosis group with a mean age of 40.1 years. The follow-up time of patients in the two groups was 12 months. The PSO osteotomy was performed at T12 in seven patients and L1 in seven patients in the lordosis group. The PSO osteotomy was performed at L2 in five patients and at L3 in five patients in the kyphosis group (typical cases are shown in Figures 1–4). The postoperative sagittal parameters were significantly improved in both groups (Table 1). The mean SVA of the two groups changed from 171.35 ± 25.46 and 223.58 ± 21.87 before the operation to 55.46 ± 5.15 and 66.58 ± 5.81 after the operation, and the difference was not significant (P > 0.05) between the two groups. The GK was corrected to 51.43 ± 1.92 after the operation in the lordosis group from 75.71 ± 5.26 before the operation, and to 52.30 ± 3.17 (P < 0.05) from 86.30 ± 10.32 in the kyphosis group. All sagittal parameters (GK, LL, SVA, PT, and SS) were significantly improved (P < 0.05). No significant correction deletion was observed in the final follow-up. The difference in LL, SVA, and SS was not significant (P > 0.05) when comparing the imaging results between the two groups. The correction rate of LL and SVA in the kyphosis group was significantly higher than that in the lordosis group (P < 0.05). The mean postoperative JOA scores of the two groups increased from 11.30 ± 0.93 to 23.00 ± 0.68, and the VAS scores improved from 7.05 ± 0.39 to 1.87 ± 0.13, and the difference was not significant (P > 0.05) between the lordosis and kyphosis groups.
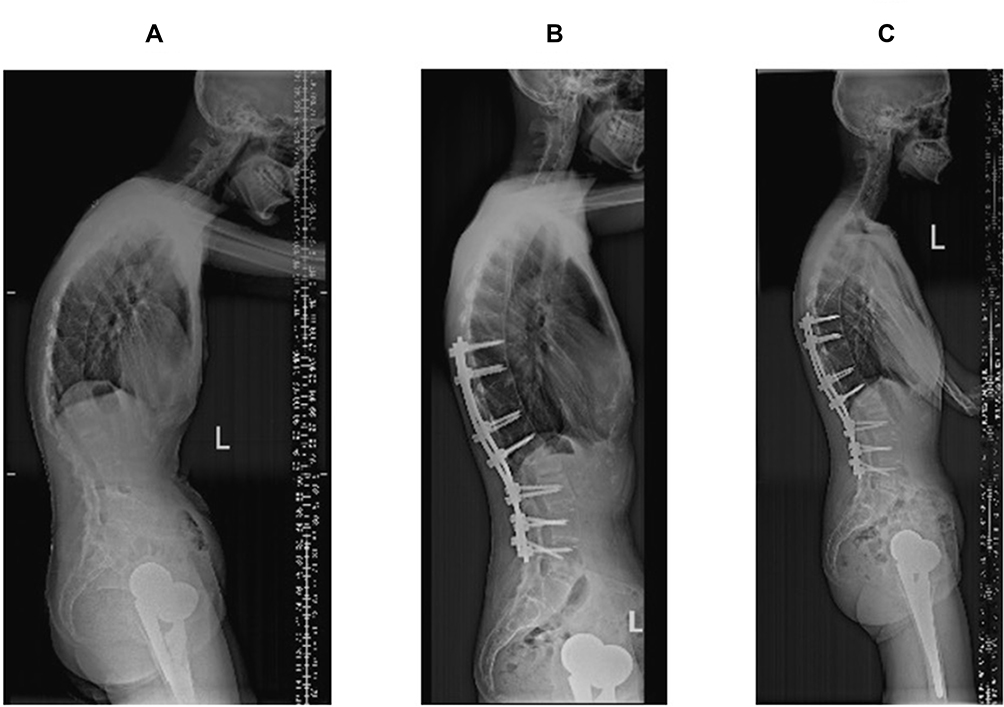 |
Figure 1 A 42-year-old female patient. (A) It shows the patient is allocated to the lumbar lordosis group before the operation. (B) Single segmental PSO surgery is performed at L1. The LL and SVA change to −59° and 38.26 mm from −24° and 148.73 mm, respectively. (C) During the follow-up, no obvious correction loss is observed in the final year. |
 |
Figure 2 A 49-year-old male patient. (A) It shows the disease is located at the apex of T11–12 before the operation, and the patient is allocated to the lumbar kyphosis group. (B) Single segmental PSO surgery is performed at T12. The GK and SVA are corrected to 61° and 72.31 mm from 93° and 274.29 mm, respectively. (C) During the follow-up, the GK increases to 57, and the LL is improved to −56° from −28° in the final year. No obvious correction loss is observed. |
 |
Figure 3 A 49-year-old male patient. (A) The patient is allocated to the lumbar kyphosis group before the operation. (B) Single segmental PSO surgery is performed at L2. The LL and SVA change to −56° and 63.06 mm from 8° and 312.84 mm, respectively (C). During the follow-up, no significant correction loss is observed in the final year. The LL and SVA are −56° and 70.35 mm, respectively. |
 |
Figure 4 A 46-year-old female patient. (A) It shows the disease is located at the apex of L2–L3, and the patient is allocated to the lumbar kyphosis group. (B) The SPO osteotomy is performed at L1–L2, L4–L5, and L5–S1. The single segmental PSO osteotomy is performed at L3. The GK and SVA change to 59° and 56.36 mm from 103° and 261.49 mm, respectively. The LL is corrected to postoperative −44° from preoperative 41°. (C) During the follow-up, no significant correction loss is observed in the final year. The LL, GK, and SVA are −45°, 62°, and 48.82 mm, respectively. |
 |
Table 1 Comparison of Lordosis (A) and Kyphosis (B) Groups |
Table 2 shows the preoperative sagittal parameters of four groups (T12, L1, L2, and L3). The GK, LL, and SS of the preoperative L2 and L3 groups are significantly higher than those of the T12 and L1 groups (P < 0.05).
 |
Table 2 Preoperative Comparison of Four Subgroups (T12, L1, L2 and L3) |
Table 3 summarizes the clinical effects. The mean value of postoperative JOA increases to 22.39 from 11.15, and the VAS scores decrease to 1.72 from 7.99. There is no significant difference between subgroups (P < 0.05).
 |
Table 3 Efficacy Comparison of Four Subgroups (T12, L1, L2 and L3) |
Discussion
The key factor in surgical decision making for AS complicated with TK is restoring the sagittal balance of the patient. Previous studies15,18 have indicated that LL is correlated with PT, PI, and SS to some extent, while TK is not significantly correlated with them. Legaye et al19 proposed that LL and SS are most closely related to scoliosis (r = 0.80) and that pelvic parameters can be used to predict LL values. Gottfried et al20 found that the PI and PT values of patients with flatback deformity after spinal osteotomy were significantly higher than those of patients without flatback deformity. They speculated that the cause of flatback deformity may be related to a higher preoperative PI value in this group of patients. They also suggested that patients with high preoperative PI values may not be able to tolerate LL loss, which further suggests that PI and LL should be used as important reference indicators for the preoperative evaluation of adult patients with spinal deformities. Hence, it is necessary to study the sagittal morphology of the lumbar vertebrae, using LL as a guide.
Thomasen first proposed PSO as a method of correcting AS with severe kyphosis in 1985. The method can achieve a 30°–35° correction of deformity21,22 through a V-osteotomy of the pedicle, using the anterior cortical bone of the vertebral body as the correction axis and closing the posterior column to close the wedge gap at the osteotomy of the anterior middle column. Because the anterior column is not open, the tension of the anterior vertebrae tissue in the orthosis is small, thereby reducing the risk of anterior longitudinal ligament and abdominal aortic tear. Many studies have reported23,24 that PSO can effectively restore LL and SVA to reconstruct sagittal balance. However, the procedure is also associated with complications,23 such as nerve and vascular injuries. Despite this, it has become the most commonly used surgical method for correcting TK deformity in patients with AS. The present study found that the average correction degree of PSO in 24 patients with AS and TK was 30.3°, which is consistent with previous studies.
This study investigated the different sagittal patterns of the lumbar vertebrae in patients with AS and TK. Satisfactory correction was achieved in all 24 patients after surgery. The 14 patients in the lumbar lordosis group underwent PSO at the twelfth thoracic vertebra (T12) or the first lumbar spinal vertebra (L1), while the 10 in the lumbar kyphosis group underwent PSO at the second or third lumbar spinal vertebra (L2 or L3). A slight loss (1.4°–2.7°) of correction degree was identified in both groups at the last follow-up. This is similar to the results of Liu14 and Qian.25
For the calculation of osteotomy angles, Surgimap software was used for preoperative simulation (Figure 5) in all patients in the present study. Osteotomy angle = preoperative maxillary eyebrow angle + preoperative PT-tPT-10 (tPT is an ideal PT value; tPT = 0.37 × PT − 7). The preoperative theoretical osteotomy degree was between 31.5° and 33° in the lumbar lordosis group and between 32.5° and 82.5° in the kyphosis group. Previous studies have reported an average corrective degree of 16°,26 35°,24 and 38°27 for single-segmental PSO in patients with AS and an improvement of 30–130 mm28 after surgery. The results of the present study are consistent with these findings: the average GK and LL correction values were 37.53° and 29.51°, respectively, and the SVA correction was about 116.96 mm. There was also no obvious loss within a one-year follow-up period, which is largely consistent with the calculation of preoperative theoretical values. The preoperative SVA and GK of patients in the kyphosis group were obviously worse when comparing the preoperative radiological parameters of the two groups, and the postoperative JOA and VAS scores of patients in the kyphosis group were lower than those in the lordosis group.
 |
Figure 5 Simulated selection of osteotomy plane and PSO angle before operation. Simulated osteotomy angle = preoperative mandibular eyebrow angle + preoperative PT-tPT-10, tPT = 0.37 × PT-7. |
In addition, five patients with lumbar kyphosis underwent total hip arthroplasty (THA) before PSO. There is still controversy about the order of surgery for patients with AS and TK: should THA be undertaken first to address AS hip joint deformity, or should spinal orthopedic surgery be undertaken first to treat kyphosis deformity? Le et al29 believed that performing a spinal osteotomy first, following by THA, allows more accurate determination of the acetabular anterior inclination and abduction angles. Guan et al30 stated that undertaking spinal posture surgery after THA surgery is more convenient because the spinal orthopedic surgery can be performed with the patient prone. Vaz and Roussouly et al31 found that PT and TK values decreased after THA when AS affected the hip joints, while SS and LL values increased. As previous findings suggest that spinal and pelvic parameters are improved by undertaking THA first, five of the patients in the present study underwent THA before spinal surgery.
In this study, all patients in the kyphosis group underwent PSO surgery at L2 or L3. The osteotomy at L3 could provide a larger range of bone resection and longer PSO leverage than the upper lumbar vertebrae and achieve maximum correction of LL and SVA. However, such patients often require sacral base (S1) fixation. For precise control in PSO surgery, orthodontic, in drawing up bone cutting cone and two sections near the cone into long segmental pedicle screws and install a temporary fixed rod (that is, the four fixed adjacent cones in order to maintain the stability of the spine). Longer segmental internal fixation can effectively maintain the protrusion deformity after correction, so AS patients often experience vertebral osteoporosis. Strong fixation of the long segmental pedicle screw can avoid loosening and emergence of the postoperative screw and prevent the need for postoperative convex deformity correction after failure. To formulate the cone, a V-shaped cut is made on the bone according to the required angle of bone cutting. Titanium rods are bent to the shape of the reset bone and the bed is slowly adjusted to reset the spine. Gradually closed bone cutting clearance, maintaining the dural sac and nerve-root compression, evoked potential amplitude detection continuously. In order to address abnormal situations in a timely manner, a closed complete intraoperative X-ray should be taken to confirmed reset and no significant deviation.
For patients with severe kyphosis, when the required correction exceeds 60°, two-stage PSO or PSO + Smith-Peterson osteotomy (SPO) should be considered to obtain a larger range of correction. In the present study, a 46-year-old woman (Figure 4) presented a typical folding-knife back. Her chin-brow vertical angle (CBVA) was −58°, and her SVA was approximately 300 mm. Her lumbar spine was kyphotic, and her LL was 45°. An osteotomy angle of 86.5° was required before the operation. PSO + SPO was performed for this patient, using Surgimap software to simulate every individual segment that could provide a 15° correction from osteotomy. Single-segmental PSO can provide a 40° correction at most, while the combined surgery can provide a total of 85° correction. Therefore, the SPO osteotomy was undertaken at L5–S1 and L4–L5.
In three-dimensional reconstruction from CT scans, the patient showed lumbar anterior column ossification and incomplete fusion, so the front is an activity, through the posterior column of shortening are able to do in front of open, so we are in the L5 and S1, L4 and L5, L1 and L2 SPO osteotomy, use bit except to cut bone rongeur clearance of spinous process and ligament between the spine, spine, and remove the bilateral joints, reoccupy lamina rongeur bite in addition to the part of the lamina, yellow ligament and articular process, retain pedicle bone cutting, finally open the front, compressed column to achieve correct the restoration of lumbar lordosis sagittal morphology and L1–L2 and PSO osteotomy at L3, respectively. Fixed segments were at T9–S1. The postoperative CBVA was improved to 8°, SVA to 48.4 mm, and LL to −44°. One year after the operation, no correction loss was observed in this patient. From the patient’s point of view, satisfactory sagittal shape and good quality of life were achieved.
Previous studies6,22 have reported that PSO should be performed at the apex of kyphosis. However, the present study suggests that the patient’s preoperative sagittal morphology needs to be evaluated if the osteotomy plane is close to the kyphotic apex. Based on the results of this study, it appears that patients with lumbar kyphosis usually present with kyphosis in the thoracolumbar segments. T12 or L1 are therefore recommended as the osteotomy plane because they are relatively close to the kyphotic apex and can therefore achieve a better correction of TK. Owing to the reduction of fixed segments, the risk of postoperative PJK can be reduced.
For patients with lumbar kyphosis, PSO is recommended at L2 or L3. The preoperative sagittal imbalance is often severe in such patients, which means a greater correction is needed to achieve a satisfactory outcome. The adult spinal cones terminate at L2, and a lower level of osteotomy can reduce the risk of spinal cord injury. However, S1 fixation is often required at L3 in patients with osteotomy, which may result in a poor quality of life.32 However, taking into consideration a better correction of LL and SVA, this is an acceptable option. Therefore, the osteotomy position of patients with lumbar kyphosis should be either L2 or L3.
Conclusion
The present study has some limitations. Firstly, it was a retrospective study. Secondly, its sample size was small, especially for patients with lumbar kyphosis. Moreover, none of the enrolled patients underwent PSO at L4. As such, larger cohort studies are needed to improve the classification of lumbar sagittal morphology in patients with AS. Lastly, the conclusion of this study is relatively preliminary because both groups lacked a control group for comparison. Further prospective cohort studies are needed to determine the optimal osteotomy level for single-level PSO.
Acknowledgments
We are particularly grateful to all the people who have given us help in this article.
Funding
This study was funded by the Research on TGF-β2 in regulating the apoptotic signaling pathways of Fluoride-stained Cells Project (No.2018D01C158). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no competing interest.
References
1. Koller H, Koller J, Mayer M, Hempfing A, Hitzl W. Osteotomies in ankylosing spondylitis: where, how many, and how much? Eur Spine J. 2018;27(Suppl 1):70–100. doi:10.1007/s00586-017-5421-z
2. Campochiaro C, Caruso PF. Ankylosing spondylitis and axial spondyloarthritis. N Engl J Med. 2016;375(13):1302. doi:10.1056/NEJMc1609622
3. Uckun A, Sezer I. Ankylosing spondylitis and balance. Eurasian J Med. 2017;49(3):207–210. doi:10.5152/eurasianjmed.2017.17116
4. QQian BP, Huang JC, Qiu Y, et al. Complications of spinal osteotomy for thoracolumbar kyphosis secondary to ankylosing spondylitis in 342 patients: incidence and risk factors. J Neurosurg Spine. 2018;30(1):91–98. doi:10.3171/2018.6.SPINE171277
5. Tominaga R, Fukuma S, Yamazaki S, et al. Relationship between kyphotic posture and falls in community-dwelling men and women: the locomotive syndrome and health outcome in Aizu cohort study. Spine (Phila Pa 1976). 2016;41(15):1232–1238. doi:10.1097/BRS.0000000000001602
6. Chen IH, Chien JT, Yu TC. Transpedicular wedge osteotomy for correction of thoracolumbar kyphosis in ankylosing spondylitis: experience with 78 patients. Spine (Phila Pa 1976). 2001;26(16):E354–E360. doi:10.1097/00007632-200108150-00010
7. Xu H, Zhang Y, Zhao Y, Zhang X, Xiao S, Wang Y. Radiologic and clinical outcomes comparison between single- and two-level pedicle subtraction osteotomies in correcting ankylosing spondylitis kyphosis. Spine J. 2015;15(2):290–297. doi:10.1016/j.spinee.2014.09.014
8. Kim KT, Park DH, Lee SH, Lee JH. Results of corrective osteotomy and treatment strategy for ankylosing spondylitis with kyphotic deformity. Clin Orthop Surg. 2015;7(3):330–336. doi:10.4055/cios.2015.7.3.330
9. Yıldız F, Akgül T, Ekinci M, Dikici F, Şar C, Domaniç Ü. Results of closing wedge osteotomy in the treatment of sagittal imbalance due to ankylosing spondylitis. Acta Orthop Traumatol Turc. 2016;50(1):63–68. doi:10.3944/AOTT.2016.14.0059
10. Hua WB, Zhang YK, Gao Y, et al. Analysis of sagittal parameters in patients undergoing one- or two-level closing wedge osteotomy for correcting thoracolumbar kyphosis secondary to ankylosing spondylitis. Spine (Phila Pa 1976). 2017;42(14):E848–E854. doi:10.1097/BRS.0000000000001984
11. R P Jackson, Mcmanus AC. Pelvic lordosis and pelvic incidence: the relationship of pelvic parameters to sagittal spinal profile. Curr Opin Orthop. 2004;15(3):150–153. doi:10.1097/01.bco.0000120643.46244.8a
12. Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976). 2005;30(3):346–353. doi:10.1097/01.brs.0000152379.54463.65
13. Qian BP, Wang XH, Qiu Y, et al. The influence of closing-opening wedge osteotomy on sagittal balance in thoracolumbar kyphosis secondary to ankylosing spondylitis: a comparison with closing wedge osteotomy. Spine (Phila Pa 1976). 2012;37(16):1415–1423. doi:10.1097/BRS.0b013e318250dc95
14. Liu C, Zheng G, Guo Y, et al. Two-level osteotomy for correcting severe ankylosing spondylitis kyphosis: radiologic outcomes of different osteotomy position-selection strategy for different type of patients. Spine Deform. 2018;6(3):273–281. doi:10.1016/j.jspd.2017.10.011
15. Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002;27(6):612–618. doi:10.1097/00007632-200203150-00010
16. Liu ZJ, Qian BP, Qiu Y, Mao SH, Jiang J, Wang B. Does postoperative PI-LL mismatching affect surgical outcomes in thoracolumbar kyphosis associated with ankylosing spondylitis patients? Clin Neurol Neurosurg. 2018;169:71–76. doi:10.1016/j.clineuro.2018.04.006
17. Mathies H. Diagnostische Kriterien der Spondylitis ankylosans [Diagnostic criteria in ankylosing spondylitis]. Dtsch Med Wochenschr. 1984;109(10):382–385. doi:10.1055/s-2008-1069200
18. Chang KW, Chen YY, Lin CC, Hsu HL, Pai KC. Closing wedge osteotomy versus opening wedge osteotomy in ankylosing spondylitis with thoracolumbar kyphotic deformity. Spine (Phila Pa 1976). 2005;30(14):1584–1593. doi:10.1097/01.brs.0000170300.17082.49
19. Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99–103. doi:10.1007/s005860050038
20. Gottfried ON, Daubs MD, Patel AA, Dailey AT, Brodke DS. Spinopelvic parameters in postfusion flatback deformity patients. Spine J. 2009;9(8):639–647. doi:10.1016/j.spinee.2009.04.008
21. Kim YJ, Bridwell KH, Lenke LG, Cheh G, Baldus C. Results of lumbar pedicle subtraction osteotomies for fixed sagittal imbalance: a minimum 5-year follow-up study. Spine (Phila Pa 1976). 2007;32(20):2189–2197. doi:10.1097/BRS.0b013e31814b8371
22. Zhu Z, Wang X, Qian B, et al. Loss of correction in the treatment of thoracolumbar kyphosis secondary to ankylosing spondylitis: a comparison between Smith-Petersen osteotomies and pedicle subtraction osteotomy. J Spinal Disord Tech. 2012;25(7):383–390. doi:10.1097/BSD.0b013e318224b199
23. Enercan M, Ozturk C, Kahraman S, Sarıer M, Hamzaoglu A, Alanay A. Osteotomies/spinal column resections in adult deformity. Eur Spine J. 2013;22(Suppl 2):S254–S264. doi:10.1007/s00586-012-2313-0
24. Kim KT, Lee SH, Suk KS, Lee JH, Jeong BO. Outcome of pedicle subtraction osteotomies for fixed sagittal imbalance of multiple etiologies: a retrospective review of 140 patients. Spine (Phila Pa 1976). 2012;37(19):1667–1675. doi:10.1097/BRS.0b013e3182552fd0
25. Diao WY, Qian BP, Qiu Y, Zhu ZZ, Wang B, Yu Y. Does the preoperative lumbar sagittal profile affect the selection of osteotomy level in pedicle subtraction osteotomy for thoracolumbar kyphosis secondary to ankylosing spondylitis? Clin Neurol Neurosurg. 2018;172:39–45. doi:10.1016/j.clineuro.2018.06.026
26. Park YS, Kim HS, Baek SW, Oh JH. Preoperative computer-based simulations for the correction of kyphotic deformities in ankylosing spondylitis patients. Spine J. 2014;14(10):2420–2424. doi:10.1016/j.spinee.2014.02.022
27. Arun R, Dabke HV, Mehdian H. Comparison of three types of lumbar osteotomy for ankylosing spondylitis: a case series and evolution of a safe technique for instrumented reduction. Eur Spine J. 2011;20(12):2252–2260. doi:10.1007/s00586-011-1894-3
28. Xin Z, Zheng G, Huang P, Zhang X, Wang Y. Clinical results and surgery tactics of spinal osteotomy for ankylosing spondylitis kyphosis: experience of 428 patients. J Orthop Surg Res. 2019;14(1):330. doi:10.1186/s13018-019-1371-y
29. Le Huec JC, Leijssen P, Duarte M, Aunoble S. Thoracolumbar imbalance analysis for osteotomy planification using a new method: FBI technique. Eur Spine J. 2011;20(Suppl 5):669–680. doi:10.1007/s00586-011-1935-y
30. Guan M, Wang J, Zhao L, Xiao J, Li Z, Shi Z. Management of hip involvement in ankylosing spondylitis. Clin Rheumatol. 2013;32(8):1115–1120. doi:10.1007/s10067-013-2278-3
31. Roussouly P, Transfeldt E, Schwender J, et al. 7:58 Sagittal morphology and equilibrium of pelvis and spine in normals. Spine J. 2002;2(5):61–62. doi:10.1016/S1529-9430(02)00299-1
32. Abe H, Matsunaga A, Watanabe H, et al. Relationship between the severity of osteoarthritis of the knee and spino-pelvic alignment in Japanese patients with knee osteoarthritis. Physiotherapy. 2015;101:e29–e30. doi:10.1016/j.physio.2015.03.139
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.