Back to Journals » Advances in Medical Education and Practice » Volume 16
The Room of Errors as an Innovative Simulated Environment to Enhance the Management of Blood Exposure Accidents: A Tunisian Pre-Experimental Study
Authors Bouhoula M, Kacem I ![]() , Ghenim A, Ajmi M
, Ghenim A, Ajmi M ![]() , Mellouli A, Aloui A, Sridi C
, Mellouli A, Aloui A, Sridi C ![]() , Fki A, Maoua M, Naija W, Kahloul M
, Fki A, Maoua M, Naija W, Kahloul M
Received 28 April 2025
Accepted for publication 1 August 2025
Published 8 September 2025 Volume 2025:16 Pages 1641—1650
DOI https://doi.org/10.2147/AMEP.S530487
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Marwa Bouhoula,1,2 Imene Kacem,1,2 Amal Ghenim,2 Mohamed Ajmi,1,3 Amani Mellouli,1,3 Asma Aloui,1,2 Chaima Sridi,1,4 Amen Fki,1,4 Maher Maoua,1,4,5 Walid Naija,1,3,6 Mohamed Kahloul1,3,6
1University of Sousse, Faculty of Medicine of Sousse, Sousse, 4000, Tunisia; 2Occupational Medicine Department, Farhat Hached University Hospital, Sousse, Tunisia; 3Anesthesia and Intensive Care Department, Sahloul University Hospital, Sousse, Tunisia; 4Occupational Medicine Department, Sahloul University Hospital, Sousse, Tunisia; 5Laboratoire de Recherche (LR19SP03: Etude des risques et perspectives de prévention des maladies non transmissiblesen milieu professionnel), Sousse, Tunisia; 6Medical Simulation Center (CESIME), Faculty of Medicine Ibn El Jazzar of Sousse, University of Sousse Tunisia, Sousse, Tunisia
Correspondence: Imene Kacem, University of Sousse, Faculty of Medicine of Sousse, Occupational Medicine Department, Farhat Hached University Hospital, Sousse, 4000, Tunisia, Email [email protected]
Introduction: Blood exposure accidents (BEA) represent a significant risk for healthcare workers. To enhance safety awareness, particularly among medical students, the “Room of Errors” may offer an innovative and effective educational approach.
Objective: To assess the impact of the “Room of Errors” simulation on medical students’ knowledge regarding BEA management.
Methods: A pre-experimental study was conducted at the simulation center of the Faculty of Medicine of Sousse, including 63 students in the third level of the Second cycle of medical studies (SCMS3) who completed an internship in the occupational medicine department during the academic year2023/2024. Participants attended a simulation session of “room of errors” including seven intentional errors.An “error collection” sheet was used to identify these errors. A pre-test and post-test, each comprising 5 questions, evaluated participants’ knowledge. Answers were classified as correct or incorrect.
Results: All 63 students (100%) who participated to the simulation session were included in the study. Totally, 55.6% of participants were female, with a median age of 24 years. Participants have correctly identified an average of 5.8 errors (range: 3– 7) with a median of 6 [IQR: 5– 7]. Following the simulation, students demonstrated significant improvements in their knowledge compared to the median pre-simulation scores (4 [IQR: 4– 5] vs 2 [IQR: 1– 3]; p< 10− 3). The overall assessment of the tool indicated that all participants enjoyed and appreciate the error room: 64% found this learning method excellent and 22% found it good. The majority of the participants indicated that the debriefing was helpful, as it clarified specific elements, provided constructive feedback, and allowed a review of demonstrated technical skills, attitudes and behaviors.
Conclusion: The “Room of Errors” promotes reflective learning and enhances BEA prevention awareness. As an engaging and effective pedagogical tool, it may contribute to improving patient and professional safety.
Keywords: simulation, blood exposure accident, occupational injuries, medical student
Background
Blood exposure accidents (BEA) are defined by the Centers for Disease Control and Prevention (CDC) as percutaneous injuries or contact of mucous membranes or non-intact skin with blood, tissue, or other potentially infectious body fluids.1 BEA represents a significant occupational hazard in healthcare settings,2 with risks of transmitting life-threatening infections such as Human Immunodeficiency Virus (HIV), hepatitis B, and hepatitis C.3
Globally, the incidence of BEA remains alarmingly high. A systematic review revealed that more than half of healthcare workers have experienced needle stick injuries at some point in their careers.4 Despite the implementation of universal precautions, the persistent lack of awareness, inconsistent adherence to protective measures and underreporting of incidents continue to exacerbate the risks associated with BEA.5
These challenges are particularly pronounced among medical students and newly graduated professionals, who are more vulnerable due to their limited clinical experience and incomplete understanding of safety protocols.5
Given the significant magnitude and frequency of BEA, it is imperative to prioritize the training of students and future physicians. Such training should focus on fostering their ability to recognize risks in healthcare environments, equipping them with the knowledge and skills necessary to implement preventive measures, respond effectively to exposure incidents, and emphasize the critical importance of promptly reporting BEA. This approach is vital for ensuring proper incident management and reducing the likelihood of further complications.6,7 However, traditional teaching methods, often reliant on didactic lectures and written guidelines, fall short in cultivating the reflexive decision making and hands on skills required in real world clinical settings.8
In this context, simulation-based training (SBT) has emerged as an innovative and effective method for addressing these challenges. Recent advances in technology and research have significantly bolstered the integration of SBT into medical training.9,10 These innovations enable the development of realistic, and low-pressure environments where medical students can acquire foundational knowledge, apply scientific principles, and enhance their clinical skills across both pre-clinical and clinical settings.9–12
Despite the growing evidence supporting the use of simulation in medical education, there remains a notable gap in the literature regarding its application to occupational safety training, particularly for preventing BEA among medical students. Innovative educational tools tailored to this specific need are underexplored, highlighting the importance of developing and evaluating targeted simulation-based interventions.
Among the various techniques within SBT, the “Room of Errors” stands out as a particularly dynamic and engaging approach. By immersing learners in a simulated environment designed to identify and analyze deliberate errors, this approach not only fosters active learning and critical thinking but also promotes self-assessment and the development of practical problem-solving skills.13
This study aims to evaluate the effectiveness of the “Room of Errors” simulation method as a pedagogical tool to enhance knowledge and assess students’ satisfaction with this innovative learning experience.
Methods
Study Design and Setting
This pre-experimental study was conducted among Second cycle of medical studies 3 (SCMS3) trainees at the Simulation Center of the Faculty of Medicine of Sousse, Tunisia during the 2023–2024 academic year, after approval of the study protocol by the ethics committee of Sahloul Academic Hospital, Sousse, Tunisia (07/10/2023, Ref: HS 23–2023).The simulation sessions were conducted over five days: October the 9 th 2023, October the 29 th 2023, January the 16th 2024, January the 30 th 2024, and February the 13 th 2024.
Study Population
Inclusion Criteria
The students were recruited through an exhaustive sampling method, as all SCMS3 interns available during the five training periods were invited to participate in the study. The Faculty of Medicine organized the assignment of students into five internship groups according to its academic schedule. Each group participated in the simulation session during their respective internship period.
Non Inclusion Criteria
Students who were absent on the day of the simulation sessions or who submitted incomplete error logs or pre-test or post test questionnaires were excluded from the study.
Study Sample
The “Room of Errors” was integrated as part of a mandatory educational experience for Third-year medical students in the second cycle of medical education. It was implemented during their training in the Department of Occupational Medicine as a pedagogical tool for learning the BEA module. The educational sessions were conducted with a total of five groups. Four groups included 13 participants each, while one group comprised 11 students, resulting in a total of 63 participants.
Given that this was a pre-test/post-test educational intervention assessing changes in knowledge and performance, but responses were collected anonymously without individual linkage, the analysis was based on two independent groups. A sample size calculation was therefore conducted for independent means using Cohen’s d, assuming an expected effect size of 0.5,14 power of 80%, and an alpha level of 10%. The results indicated that a minimum of 42 participants per group would be needed to detect a significant difference.
The study was conducted as part of an educational session. In this context, participants were informed and made aware that their anonymized evaluation results could be used for scientific presentation.
Study Tool
“Error Form” (Appendix 1)
This tool was developed to assist participants in identifying seven errors intentionally introduced within the simulation room. The form was provided to participants, allowing them to document errors as they encountered them, while specifying the area where each error occurred: Zone 1 (patient), Zone 2 (healthcare provider), and Zone 3 (environment).As the form is anonymous, it encourages candidate reporting of the errors.
The errors to be identified in our study concerned the prevention of BEA, the immediate conduct to be taken following a BEA and the lack of asepsis rules.
“Pre-Test and Post-Test” (Appendix 2)
An assessment tool was designed, consisting of a pre-test administered before the session and a post-test conducted after the debriefing. The questionnaires were provided in paper format to all participants. They comprised 5 questions on infection risk following BEA, immediate measures required, standard precautions to prevent such incidents, and the reporting procedure for BEA. They aimed to evaluate the students’ progress.
The study questions were developed and validated by a staff of experts in occupational medicine and pedagogy. The correction of the questionnaires was done by a manager designated among the different members of this multidisciplinary staff. For single-choice questions, a response was classified as correct or incorrect based on whether it matched or not the correct answer. For multiple-choice questions, a response was considered correct only if all correct options were selected. If any correct option was missing or an incorrect option was selected, the entire question was marked as incorrect.
Evaluation Questionnaire (Appendix 3)
At the end of the course, students were invited to voluntarily complete a self-administered, anonymous evaluation questionnaire. The survey aimed to gather participants’ perceptions of the “Room of Errors” and collect their feedback on various aspects of the simulation session at different stages. Responses are presented using a 5-point Likert scale, which rates the simulation as: Inadequate, Insufficient, Adequate, Good, or Excellent.
Simulation Design
Preparations Before the Session
- Identification and Selection of Errors: Seven specific errors were purposefully selected to assess students’ ability to identify
Scenario Development
The “Room of Errors” scenario involved a medical student sustaining a needle stick injury while drawing blood from an HBsAg-positive patient (simulated using a Resusci Anne mannequin) during an emergency department internship. The injury occurred while she was recapping the needle, without wearing gloves. She left the needle on the patient’s bed. Following the injury, she made the wound bleed but did not perform any additional care and did not report or seek medical consultation for the occupational exposure to blood borne pathogens (OEBP).
Development of the Simulation Guide (Appendix 4)
In this guide, the objectives, target audience, training location, and all necessary documents for the implementation of the simulation session were outlined. This included the checklist for the materials and equipment required for simulating the room and staging the errors, the list of selected errors, and the instructors or facilitators involved.
Gathering of Necessary Materials
All required materials were collected and organized:
A mannequin placed in the bed to simulate a patient
Medical equipment
A monitoring sign indicating “HBs Ag-positive”
A sharps container
The patient’s medical file
Two Instructors Were Contacted to Lead the Training
Pre-briefing: Set up the materials and test the “Room of Errors.”
Preparations on the Day of the Session:
Step 1: The Briefing
- Introduction of the Workshop to Participants: Each simulation session begins with a briefing, which is prepared and structured by the facilitator.
- The facilitator presents the scenario to the learners, along with the instructions and guidelines to be followed during the session.
- The instructor introduces the environment, available materials, and the mannequin.The briefing is a crucial time for familiarizing the learners with the equipment.
- Group distribution: Group size is limited to 5–7 students, a capacity determined by the simulation room to optimize movement and facilitate observation.
Step 2: Scenario Implementation
The participants were provided with a form for error collection. They observed and filled out the form individually. The simulation ran for approximately 10 min.
Step 3: The Debriefing
- First, the participants’ feedback regarding their experience during the session and their overall impressions were collected. The scenario was then reviewed, instructions were reiterated, and the errors were corrected. The session concluded with a synthesis: What did we learn? What will we change in our practices? A review of best practices followed, with each error being addressed and discussed, emphasizing the expected responses.
- The debriefing is a critical component of simulation training, providing participants with an opportunity to reflect on their actions and thought processes, thereby promoting learning outcomes and improving future clinical performance.15
Statistical Analysis
The study data were entered and analyzed using SPSS version 25 (Statistical Package for the Social Sciences). Qualitative variables were presented as frequencies, and percentages. Quantitative variables were reported as means, standard deviations, and medians.
Data were assessed for normality using the Shapiro–Wilk test. For non-normally distributed continuous variables, the Wilcoxon signed-rank test was used to compare pre-test and post-test scores within groups. To evaluate changes in participants’ knowledge from pre-test to post-test, we used the two-tailed chi-square test for categorical variables. When the assumptions for the chi-square test were not satisfied, Fisher’s exact test was used as an alternative. A p-value of < 0.05 was considered statistically significant.
Ethical Consideration
This study adhered to the ethical principles of the Declaration of Helsinki. Before participation, students were fully informed about the study’s purpose, significance, and procedures. Oral informed consent was obtained, with assurances that their data would be used exclusively for research purposes and that participation was entirely voluntary, with no consequences for refusal.Confidentiality and privacy were strictly maintained throughout the study. All data were securely stored by the institution and accessible only to the primary researcher.
The ethics committee approved the use of oral consent, considering the pedagogical nature of the intervention and the methods employed for data collection. Verbal consent was obtained at the beginning of the simulation session, coinciding with the distribution of study materials. Prior to this, a standardized explanation of the study was provided, clearly outlining the voluntary nature of participation, the absence of any consequences for non-participation, and the option to decline involvement or withhold responses at any time. Students who accepted the materials and engaged in the activities were considered to have provided verbal consent. Those who chose not to participate were instructed to refrain from taking the materials or responding, with explicit reassurance that there would be no negative repercussions.
Results
All 63 students (100%) who participated to the simulation sessions were included in the study. Totally, 55.6% of participants were female, with a median age of 24 years.
Participants have correctly identified an average of 5.8 ± 1.5 errors (range: 3–7) with a median of 6 [IQR: 5–7]. Table 1 shows the percent of students who identified each of the 7 staged errors.
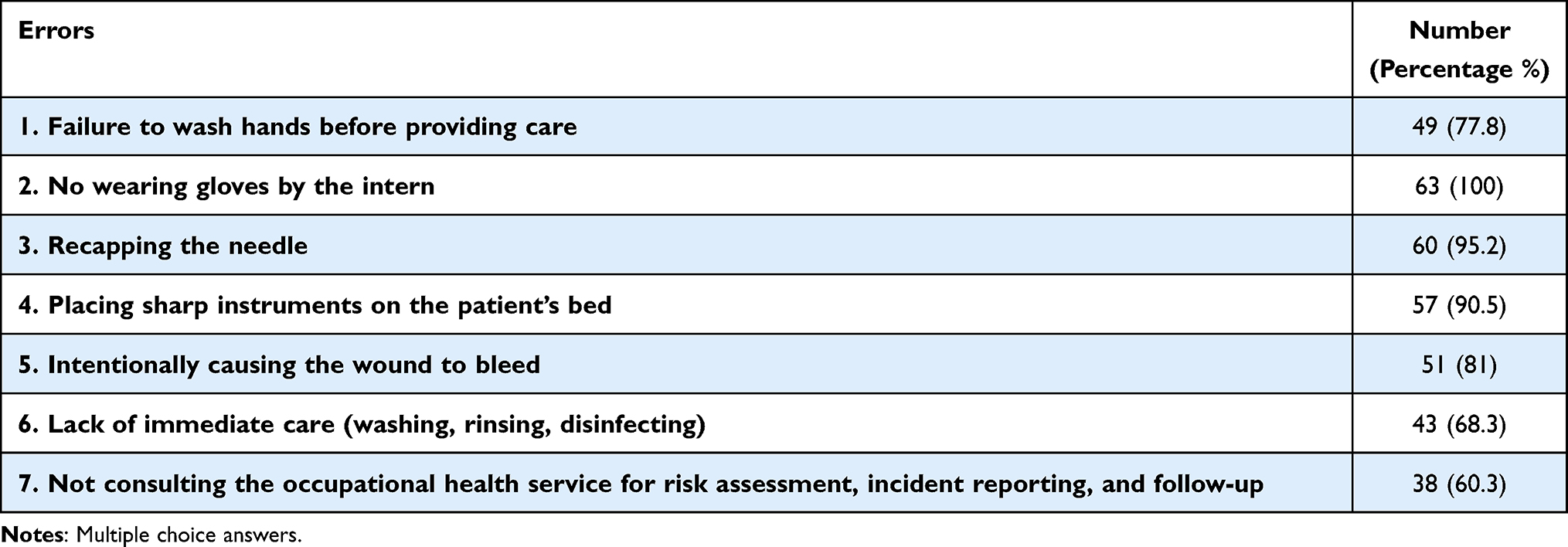 |
Table 1 Errors Correctly Identified by Students |
All medical students identified that the simulated patient did not wear gloves before performing the blood draw and that she recapped the needle. However, 60.3% did not recognize that the victim of the BOA must consult the occupational health department for risk assessment, incident reporting, and follow-up.
Some participants recorded additional errors on their lists that were neither intended nor simulated. The most commonly identified items were: lack of hygiene and asepsis, noted by 5 students (7.9%), and poor communication with the patient, identified by 8 students (12.6%).
After analyzing the pre- and post-test answers, a substantial improvement in correct response rates was observed across all questions. The most improvement rates were recorded regarding the risk factors for contamination with blood borne pathogens, but the difference was not statistically significant (6.3% versus 41.3%; p=0.06) (Table 2).
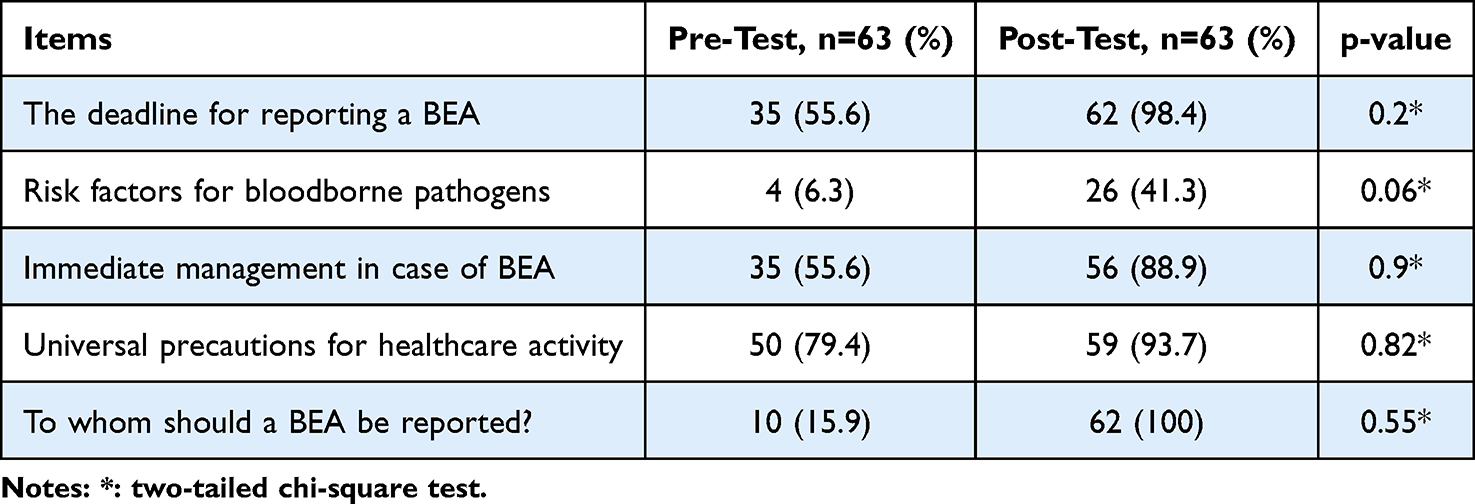 |
Table 2 Comparison of Correct Knowledge Related to BEA Between Pre-Test and Post-Test Among SCMS3 Students, Sousse Tunisia 2023–2024 |
Following the simulation, students demonstrated significant improvements in their knowledge compared to the median pre-simulation scores (4 [IQR: 4–5] vs 2 [IQR: 1–3]; p<10−3) (Table 3).
 |
Table 3 Comparison Between Pre-Test and Post-Test Scores Among SCMS3 Students, Sousse Tunisia 2023–2024 |
The results of the evaluations showed that the learning method was highly appreciated by the students. The overall assessment of the tool indicated that all participants enjoyed and appreciate the error room: 64% found this learning method excellent and 22% found it good. The majority of the participants indicated that the debriefing was helpful, as it clarified specific elements, provided constructive feedback, and allowed for a review of both demonstrated technical skills and attitudes and behaviors. Items that were judged inadequate and/or insufficient were essentiallyReview of the trigger video, Mannequin quality, Overallrealism of the simulation environment and Realism of auditory cues (Table 4).
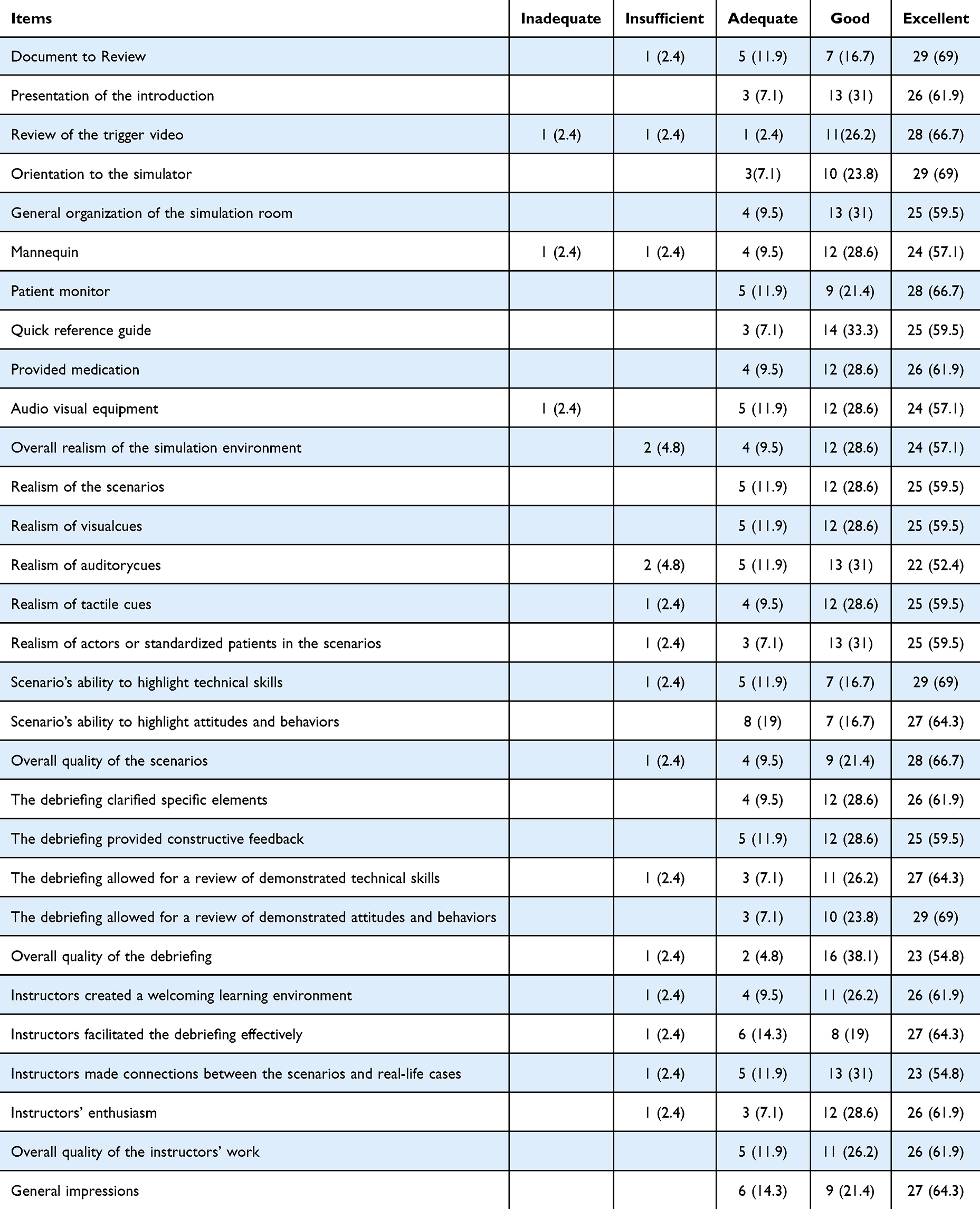 |
Table 4 Evaluation of the Simulation Session Using a 5-Point Likert Scale by Participants (n=42) |
Discussion
This study evaluated medical students’ ability to identify errors related to BEA using the “Room of Errors” simulation. It also assessed the SBT impact on knowledge improvement and measured student satisfaction with the learning experience.
During the simulation session, participants demonstrated a strong ability to identify staged errors, with a median of seven errors correctly identified (IQR: 5–7). In comparison, a study conducted in Virginia among third-year medical students during their surgical clerkship orientation reported that students identified between 2% and 93% of 33 staged errors.16 Similarly, a study conducted across 13 Swiss hospitals using a Room of Errors simulation revealed that healthcare professionals failed to correctly identify even half of the intentionally implemented hazards.13 This detection rate aligns with findings from two additional studies conducted in the United States.17,18
In our study, 46.6% of participants failed to recognize the necessity for the victim of the BOA to consult the occupational health department for risk assessment and follow-up. This finding highlights a significant gap in participants’ understanding of post-exposure protocols, which are crucial for ensuring timely evaluation and preventing potential infections following a BOA. Wiest et al19 suggest that the findings from the Room of Errors simulation could serve as a valuable tool for health leaders and educators in identifying critical areas requiring attention to ensure high-quality and safe care.
Similar shortcomings have been observed in other studies. For example, a recent study conducted at the University of Bangui found that only 37% of students who were victims of a BOA reported the incident.19 Likewise, a study among nursing students during their clinical internship revealed that 25% of participants failed to report the occupational accident.5 Furthermore, research conducted in six nursing schools and six hospitals in Lorraine among 964 nurses showed that approximately half of all BOA cases were not reported (51.5%).20
These findings underscore the persistent issue of underreporting among healthcare professionals and trainees. This knowledge gap highlights the urgent need for targeted educational initiatives to address deficiencies in understanding post-exposure protocols, which are crucial for ensuring timely evaluation and preventing potential complications.21 The SBT and particularly the Room Of Errors provide an excellent platform for initiating discussions on systemic challenges in clinical practice, paving the way for targeted and timely improvement initiatives.19
A key strength of this educational approach lies in its capacity to provide a safe and controlled environment where learners can practice repeatedly and learn from their own mistakes without the pressure of real-life consequences.22 SBT establishes a safe environment where making mistakes poses no harm to patients or healthcare providers but rather serves as a powerful learning opportunity for learners, ultimately contributing to a reduction in errors in clinical practice. Research confirms that practicing and learning from mistakes in a simulated setting significantly enhances both competency and long-term retention among students and professionals.23
Interestingly, some participants identified unintended errors that were not part of the simulated scenarios, such as lack of hygiene and asepsis (11.9%) and poor communication with the patient (9.52%). This observation underscores the participants’ heightened attention to detail, suggesting that the simulation not only improved their ability to identify the staged errors but also encouraged a broader critical assessment of clinical practices.
Analysis of the pre- and post-test responses revealed a notable improvement in the accuracy of answers across all topics. However, the area of risk factors for contamination with blood borne pathogens showed a more modest increase in correct responses compared to other topics (45.2%). This suggests that while overall knowledge improved, certain topics, particularly those related to associated factors of BOA, may require more focused attention in training.
After the simulation, students demonstrated a significant enhancement in their knowledge, with a marked increase in median scores from 2 [IQR: 1–3] to 4 [IQR: 4–5] (p<10−3). These findings underline the effectiveness of the simulation in improving general knowledge, although specific areas still present challenges and need to be addressed through targeted educational efforts.
Comparable findings have been reported in other studies. For instance, a study conducted at the Clinical Skills Training Center at Xiangya Hospital, Central South University, assessed medical students’ performance during simulation-based training for asthma exacerbation.15 The study revealed a significant post-simulation knowledge improvement, with scores markedly higher than pre-simulation values. Similarly, an observational study among medical students demonstrated enhanced professional knowledge of basic pulmonary physiology following simulation training, with participants achieving higher scores compared to lecture-based education alone.24 These findings collectively emphasize the role of simulation in bridging knowledge gaps and fostering skill acquisition.
In this study, the evaluation results highlighted that students not only highly valued the learning method but also greatly appreciated the debriefing process conducted immediately after the Room of Errors session. Debriefing is a vital component of SBT, serving as a structured opportunity to consolidate knowledge, clarify key concepts, and reflect on performance. Studies have shown that debriefing is among the most effective methods for enhancing learning outcomes in SBT.25 It allows participants to compare their performance with others, recognize their strengths and weaknesses, and receive immediate, constructive feedback from instructors.13 In a study conducted by Antila et al,26 reflective writings from 208 fourth-year medical students, collected after a communication skills course, revealed that students placed significant emphasis on the role of feedback in their learning process. They expressed a clear preference for honest, constructive feedback, which they found to be instrumental in improving their skills. Additionally, feedback from professional actors was particularly valued, as it enriched the learning experience.
However, Liu et al15 reported that 0.66% of students found the SBT experience stressful. For these students, educators could offer additional debriefing sessions and extended practice opportunities to maximize their benefit from SBT and address specific needs.15
By integrating reflective and structured debriefing sessions following simulation exercises, participants are encouraged to explore additional observations, engage in meaningful discussions, and learn from their mistakes.27,28 Immediate feedback and structured debriefing are key components of SBT, helping to reinforce learning, correct errors, and promote reflective practice.29
This study has several notable strengths. It employed an innovative and interactive learning approach, the Room of Errors, which actively engaged participants in identifying and reflecting on simulated errors. This method effectively enhanced knowledge retention while fostering critical thinking and self-assessment, essential skills for future healthcare professionals. Furthermore, the study resulted in the development of a comprehensive pedagogical guide for the Room of Errors, designed to serve as a valuable training resource for healthcare professionals in managing BEAs in the future.
However, the study also has certain limitations. First, the sample size was relatively small, which may limit the generalizability of the findings to broader populations of medical students or healthcare professionals. Second, the study was conducted in a single institution, and the results may not fully reflect the experiences of learners in different educational or clinical settings. Third, the assessment focused primarily on knowledge improvement without fully exploring the long-term impact of the intervention on clinical practice or patient outcomes. Finally, self-reported data on error recognition and participant evaluations may be subject to bias, potentially affecting the accuracy of some findings.
Future studies should aim to address these limitations by including larger, more diverse samples, exploring the long-term effects of the intervention, and evaluating its impact on real-life clinical performance and patient safety. Despite these limitations, the study highlights the value of simulation-based education in fostering a culture of safety and improving the training of healthcare professionals.
Conclusion
This study highlights the value of the “Room of Errors” as an innovative and effective SBT tool for improving medical students’ knowledge and awareness of BEA. This method could enhance learners’ ability to identify errors, promote critical thinking, and foster self-assessment skills that are essential for preparing future healthcare professionals to navigate the complexities of clinical practice. Furthermore, integrating BEA-related scenarios into this framework provides a valuable opportunity to reinforce best practices, promote adherence to safety protocols, and develop a culture of vigilance and prompt reporting in clinical settings.
Ethics Statement
Ethical approval was obtained from the ethics committee of the Sahloul University Hospital, Sousse, Tunisia (07/10/2023, Ref: HS 23–2023).
Acknowledgments
The authors would like to thank all participants for their time and cooperation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Hbibi A, Kasouati J, Charof R, et al. Evaluation of the knowledge and attitudes of dental students toward occupational blood exposure accidents at the end of the dental training program. J Int Soc PrevCommunity Dent. 2018;8(1):77–86. doi:10.4103/jispcd.JISPCD_282_17
2. Bouya S, Balouchi A, Rafiemanesh H, et al. Global prevalence and device related causes of needlestick injuries among health care workers: a systematic review and meta-analysis. Ann GlobHealth. 2020;86(1):35.
3. Reis RK, Gir E, Canini SR. Accidents with biological material among undergraduate nursing students in a public Brazilian university. Braz J Infect Dis. 2004;8(1):18–24. doi:10.1590/S1413-86702004000100003
4. Mengistu DA, Tolera ST. Prevalence of occupational exposure to needle-stick injury and associated factors among healthcare workers of developing countries: systematic review. J Occup Health. 2020;62(1):e12179. doi:10.1002/1348-9585.12179
5. El Bouazzi O, Toujami Z, Raoui SM, et al. Occupational exposure to blood and body fluids among nursing studentshv in clinical internship. J Public Health Afr. 2023;14(6):2336. doi:10.4081/jphia.2023.2336
6. Ippolito G, Puro V, De Carli G. The risk of occupational human immunodeficiency virus infection in health care workers. Arch Intern Med. 1993;153(12):1451–1458. doi:10.1001/archinte.1993.00410120035005
7. Trim JC, Elliott TSJ. A review of sharps injuries and preventative strategies. J Hosp Infect. 2003;53(4):237–242. doi:10.1053/jhin.2002.1378
8. Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Medical Teacher. 2005;27(1):10–28. doi:10.1080/01421590500046924
9. Al-Elq AH. Simulation-based medical teaching and learning. J FamilyCommunity Med. 2010;17(1):35–40.
10. Alluri RK, Tsing P, Lee E, Napolitano J. A randomized controlled trial of highfidelity simulation versus lecture-based education in preclinical medical students. Med Teach. 2016;38(4):404–409. doi:10.3109/0142159X.2015.1031734
11. Owen H. Early use of simulation in medical education. Simul Healthc. 2012;7(2):102–16.5. doi:10.1097/SIH.0b013e3182415a91
12. Gordon JA, Hayden EM, Ahmed RA, Pawlowski JB, Khoury KN, Oriol NE. Early bedside care during preclinical medical education: can technologyenhanced patient simulation advance the Flexnerianideal? Acad Med. 2010;85(2):370–377. doi:10.1097/ACM.0b013e3181c88d74
13. Zimmermann C, Fridrich A, Schwappach DLB. Training situational awareness for patient safety in a room of errors: an evaluation of a low-fidelity simulation method. J Patient Safet. 2021;17(8):e1026. doi:10.1097/PTS.0000000000000806
14. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation training for internal medicine and emergency medicine procedural skills: a systematic review and meta-analysis. Acad Med. 2011;86(9):1172–1184.
15. Liu Z, Chen Q, Wu J, Li X, He Y, Yu Q. Simulation-based training in asthma exacerbation for medical students: effect of prior exposure to simulation training on performance. BMC Med Educ. 2022;22(1):223. doi:10.1186/s12909-022-03300-2
16. Turrentine FE, Schroen AT, Hallowell PT, et al. Enhancing medical students’ interprofessional teamwork through simulated room of errors experience. J Surg Res. 2020;251:137–145. doi:10.1016/j.jss.2020.02.001
17. Farnan JM, Gaffney S, Poston JT, et al. Patient safety room of errors: a novel method to assess medical students and entering residents’ ability to identify hazards of hospitalisation. BMJ QualSaf. 2016;153–158.
18. Clay AS, Chudgar SM, Turner KM, et al. How prepared are medical and nursing students to identify common hazards in the intensive care unit? Ann Am Thorac Soc. 2017;14(4):543–549. doi:10.1513/AnnalsATS.201610-773OC
19. Mossoro-Kpinde HD, Koyambenguia C, Mangbé YK, Diemer SCH. Incidence and management of occupational blood exposure (OBE) among medical students at the university of Bangui. Occup Dis Environ Med. 2024;12(2):68–77.
20. Rabaud C, Zanea A, Mur JM, et al. Occupational exposure to blood: search for a relation between personality and behavior. Infect Control Hosp Epidemiol. 2000;21(9):564–574.
21. Bun RS, Bouziad KA, Daouda OS, et al. Identifying individual and organizational predictors of accidental exposure to blood (AEB) among hospital healthcare workers: a longitudinal study. Infect Control Hosp Epidemiol. 2024;45(4):491–500.
22. Datta R, Upadhyay K, Jaideep C. Simulation and its role in medical education. Med J Armed Forces India. 2012;68(2):167–172. doi:10.1016/S0377-1237(12)60040-9
23. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
24. Meyers L, Mahoney B, Schafernocker T, et al. The effect of supplemental high Fidelity simulation training in medical students. BMC Med Educ. 2020;20(1):421. doi:10.1186/s12909-020-02322-y
25. Dhar E, Upadhyay U, Huang Y, et al. A scoping review to assess the effects of virtual reality in medical education and clinical care. Digit Health. 2023;9:20552076231158022. doi:10.1177/20552076231158022
26. Antila AK, Lindblom S, Louhiala P, Pyörälä E. Creating a safe space: medical students’ perspectives on using actor simulations for learning communication skills. BMC Med Educ. 2024;24(1):1225. doi:10.1186/s12909-024-06184-6
27. Jiang H, Vimalesvaran S, Wang JK, Lim KB, Mogali SR, Car LT. Virtual reality in medical students’ education: scoping review. JMIR Med Educ. 2022;8:e34860.
28. Gunn T, Rowntree P, Starkey D, Nissen L. The use of virtual reality computed tomography simulation within a medical imaging and a radiation therapy undergraduate programme. J Med Radiat Sci. 2021;68(1):28–36. doi:10.1002/jmrs.436
29. Mallik R, Patel M, Atkinson B, Kar P. Exploring the role of virtual reality to support clinical diabetes training-a pilot study. J Diabetes Sci Technol. 2022;16(4):844–851. doi:10.1177/19322968211027847
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.