")
Back to Journals » Clinical Ophthalmology » Volume 17
The Role of Preoperative Case Selection in the Training of Surgical Repair of Primary Rhegmatogenous Retinal Detachment
Authors William A, Kuehnel S, Dimopoulos S, Hillenkamp J, Goebel W
Received 7 July 2023
Accepted for publication 25 September 2023
Published 19 October 2023 Volume 2023:17 Pages 3113—3122
DOI https://doi.org/10.2147/OPTH.S425646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Antony William,1 Sophia Kuehnel,1 Spyridon Dimopoulos,2 Jost Hillenkamp,1 Winfried Goebel1
1Department of Ophthalmology, University Eye Hospital Würzburg, Würzburg, Germany; 2Department of Ophthalmology, University Eye Hospital Tübingen, Tübingen, Germany
Correspondence: Antony William, Department of Ophthalmology, University Hospital Würzburg, Josef–Schneider Straße 11, Würzburg, 97080, Germany, Tel +4993120120646, Email [email protected]
Purpose: To analyse single-operation anatomical success (SOAS) of primary rhegmatogenous retinal detachment (RRD) repair by junior vitreoretinal surgeons guided by preoperative individual case selection by an experienced mentor vitreoretinal surgeon.
Methods: Retrospective, single institute, observational study, included all patients who underwent standard pars plana vitrectomy (PPV) or combined encircling band (CB) and PPV and gas tamponade in the treatment of RRD from November 2021 to December 2022 were included. Preoperative selection for the surgery decision, whether standard PPV or combined CB & PPV was undertaken through the senior surgeon; according to the location and extensions of the RRD, number of retinal tears (RT) and lens status. We excluded patients with tractional retinal detachment, RD with proliferative vitreoretinopathy stage C, giant tears, trauma, previous scleral buckle, schisis RD and RD requiring silicone oil. The primary outcome measure was to evaluate the single-operation anatomic success (SOAS). Secondary outcome measures evaluated whether there was a statistical significant difference between both procedures.
Results: Eighty-two eyes were included in the study. Forty-five eyes were selected for combined CB&PPV and 37 eyes for standard PPV. SOAS was achieved in 40 eyes (88.8%) in combined group and 35 eyes (94.5%) in standard PPV group. There was no statistically significant difference in the success rate between both operations, p = 0.65.
Conclusion: Structured preoperative selection of standardized surgical techniques according to the degree of complexity of RD together with close supervision enables junior vitreoretinal surgeons in training to achieve re-attachment rates of more than 80% with both types of surgeries.
Keywords: primary rhegmatogenous retinal detachment, RRD, pars plana vitrectomy, PPV, encircling band, CB
Introduction
In the last two decades, numerous breakthrough advancements have emerged in treating primary rhegmatogenous retinal detachment (RRD), whether through development in viewing instrumentation, 3D viewing systems, or small gauge 25, 27-gauge vitrectomies.1–3 Furthermore, various prospective and retrospective studies helped evaluate the success and failure of various retinal surgical procedures in the treatment of retinal detachment.4–7 However, the fact remains that experience plays a significant role in achieving successful re-attachment of the retina.8–10 Nevertheless, experience requires a learning curve. Single studies have addressed the importance of experience and learning curve in vitreoretinal surgery.9–12 The learning curve in vitreoretinal surgery necessitates a high volume of RD surgeries ranging from at least 200 until to 500 surgeries, thus requiring a long duration of training.9,10 However, vitreoretinal fellowship programs are usually limited to a maximum of two years and therefore, achieving a high rate of surgical success within this period is challenging. Meanwhile, few studies have discussed the importance of the learning curve through continuous practice; however, none has discussed the importance of preoperative individual case selection, additive use of encircling band (CB) and status of the lens, which might play a role in the surgical success of RD by junior surgeons. Hence, the present study aims to evaluate whether preoperative individual case selection under the supervision of an experienced vitreoretinal surgeon could aid junior vitreoretinal surgeon in decision-making which type of surgery is the suitable for each case to enable favourable surgical success through a single operation. To date, the surgical repair of retinal detachment is based on a case-by-case fashion, and no consensus has yet been reached within the vitreoretinal community in to the superiority of either performing pars plana vitrectomy (PPV) as a standard procedure or combined surgery, i.e. encircling band (CB) and PPV.13
Methods
This is a retrospective, consecutive single-centre study of all patients with primary retinal detachment who underwent either standard PPV or combined CB and PPV by a single fellow of vitreoretinal surgery (AW) at the University Eye Hospital of Würzburg from November 1, 2021 to December 31, 2022 through preoperative selection under the supervision of an experienced vitreoretinal surgeon (WG).
The experience of the fellow at the beginning of the study was limited to less than 50 pars plana Vitrectomy surgeries, which were done mainly for persistent vitreous hemorrhage and none of surgeries, were done for the treatment of retinal detachment.
We excluded patients with tractional retinal detachment, RD with proliferative vitreoretinopathy stage C, RD associated with macular hole, presence of giant retinal tear (more than 3 clock hours), history of a previous scleral buckle, retinoschisis RD and retinal detachment requiring silicone oil endotamponade. Patients with retinal detachment without vitreous detachment that were operated with scleral buckle or encircling band only were also excluded from the study.
At least a three-month follow-up minimum was required to assess for single-operation anatomic success (SOAS). The range of the fellow-up ranged from 3 to 9 months, since some of the patients required cataract surgery which was done postoperatively after 3 months from RD surgery. Patients with loss of postoperative follow-up were also excluded from this study.
We have recorded the following preoperative patient demographics; age, gender, laterality, best corrected visual acuity (BCVA) in LogMAR, myopia status (mild to moderate and high), lens status (phakic or pseudophakic or aphakic). Also, we recorded the location and extensions of the RD (in hours), the site of the RD (superior and inferior according to the 3-o’clock and 9-o’clock meridian), number of retinal tears (RT), macula status (macula on if the fovea was attached and macula-off if the fovea is detached). Patients’ demographics are listed in Table 1. Preoperative axial length measurement was performed in all patients who underwent CB with Swept Source Biometry (IOL Master® −700, Zeiss, Germany). The presence and stages of proliferative vitreoretinopathy were documented and assessed according to the Silicone study classification.14 We also reviewed the preoperative and postoperative documented retinal fundus drawing for all the patients to ensure the localisation and extension of RD and number of RT. At three months postoperative follow-up, we recorded BCVA, lens status, retinal attachment, presence of macular oedema, macular folds, subretinal perfluorodecalin, secondary cataract and secondary epiretinal membrane. The need for further surgeries, such as cataract surgery or revision due to re-retinal detachment was also recorded.
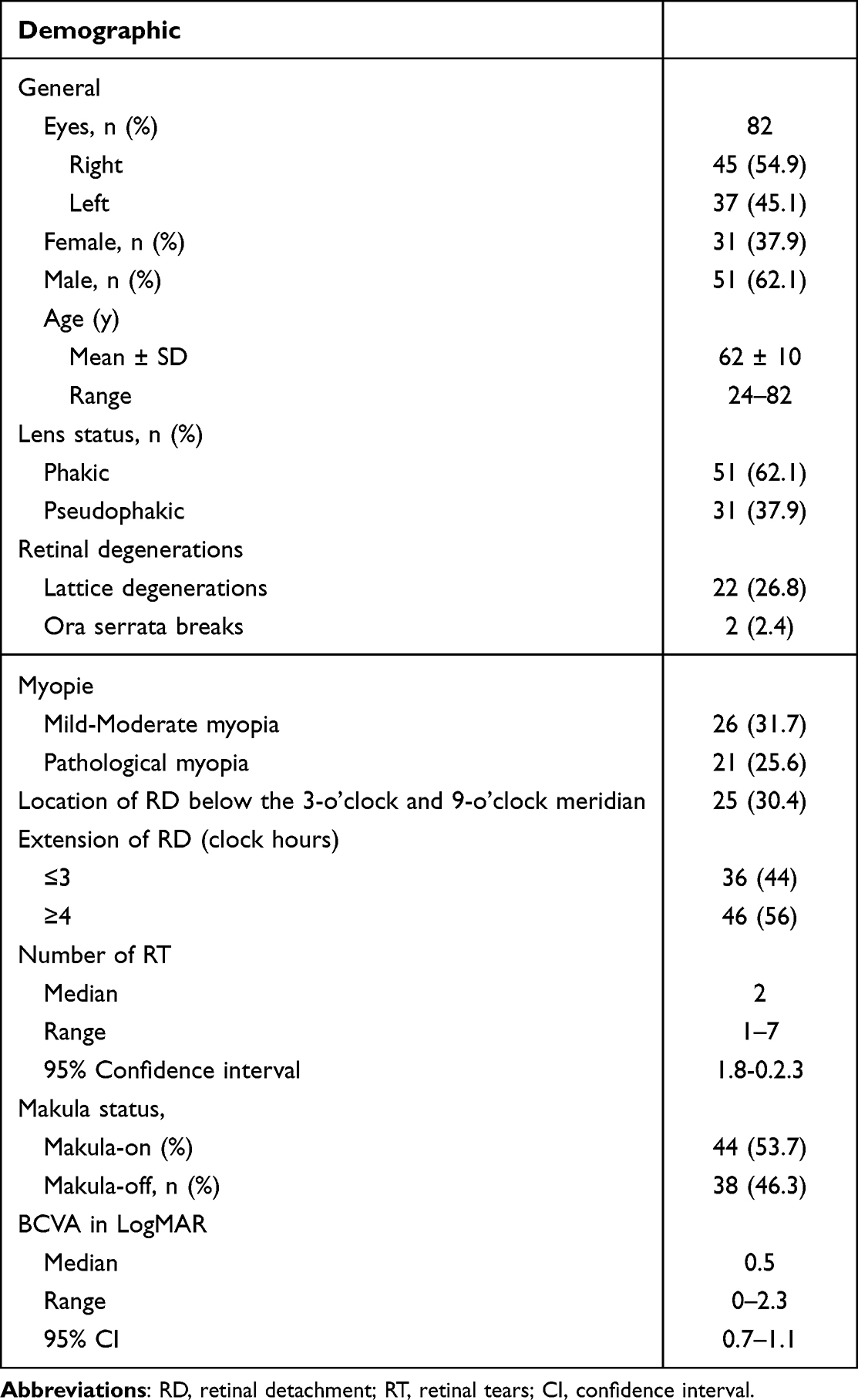 |
Table 1 Patient’s Demographics and Characteristics Preoperatively |
The surgical technique (standard PPV or combined CB & PPV) was chosen based on the location and extension of the retinal detachment, the number of retinal tears and lens status. The indication for standard PPV operation was employed when there was retinal detachment with retinal tears ≤3 or RD extensions up to four hours.
Meanwhile, the decision for combined surgery, PPV and CB was utilised instead in inferior retinal detachment extending below the 3-o’clock and 9-o’clock meridian, inferior RD in phakic eyes, multiple retinal tears ≥4 or extensions of the RD of more than 4 hours. The presence of superior and inferior lattice degenerations, unclear retinal tear situation, ora serrata retinal tear was also an indication for combined surgery. This work conformed to the Declaration of Helsinki and was conducted with approvals from by the Ethic Committee of the University of Würzburg-Bayern-Germany, approval number 20230704 01. Informed consent was obtained from all the patients preoperatively and according to German legislation and the requirements of the local institutional review board, complete data anonymisation was performed in this study.
Surgical Technique
All patients that underwent standard PPV procedure underwent a standard 4-port 23-gauge PPV with a non-contact wide-angle viewing system, chandelier endo-illumination and combined with an image inverter (BIOM; Zeiss, Germany). Careful peripheral shaving was performed in all cases, Perfluorodecalin (DORC, Decalin, Netherlands) was used to reattach the retina in all eyes. Retinal Exo-cryopexy was applied externally at the retinal tear and to the basis for all the patients that were operated with standard PPV 23-gauge, followed by Endolaser-photocoagulation around the retinal breaks and 360° circumferentially at the periphery. A non-expansible concentration of perfluoropropane in air (16% C2F6) was used for tamponade.
A 360° encircling band (2.5 mm encircling band, Labtician Ophthalmics, Canada) was sutured to the sclera at the equator measured as half of the axial length of the eye using 4–0 Supramid non-absorbable surgical suture, (Resorba Medical GmbH, Nuremberg, Germany). The 360° encircling band tightened through a Watzke Sleeve without inducing choroidal folds. All patients that underwent a Pars Plana Vitrectomy combined with an encircling band underwent 3-port 20-gauge PPV with a non-contact wide-angle viewing system and combined with an image inverter (BIOM; Zeiss, Germany). Careful peripheral shaving was performed in all cases, Perfluorodecalin (Decalin, DORC, Zuidland, Netherland) was used to reattach the retina in all eyes. Endolaser-photocoagulation was applied around the retinal breaks and 360° circumferentially at the periphery. A non-expansible concentration of sulfur hexafluoride in air (20% SF6) was used for tamponade.
Outcomes Measures and Statistical Analysis
For statistical analysis, student two-tailed t-test, matched pairs test, one-way-ANOVA analysis and Fischer exact test analysis were calculated at a significance level of p < 0.05. For all parameters, ranges were given as standard deviations (SD). All statistical tests were performed using JMP® software (version 16.0, SAS Institute Inc., Cary, NC, USA).
Results
Preoperative Patients Demographics
From the period of November 2021 to December 2022, a total number of 119 eyes of 119 patients with RRD were operated by a single fellow in vitreoretinal surgery (AW) after preoperative selection under the supervision of an experienced vitreoretinal surgeon (GW).
After applying the inclusion and exclusion criteria mentioned above, eighty-two eyes of eight two patients were identified, who underwent either standard PPV operation or combined CB & PPV for primary RRD. Preoperative patient’s demographics are listed in Table 1.
The mean age of the patients was 62.4 years, with a standard deviation, 9.8 years, range from 24 to 82 years. Phakic eyes were seen in 51 eyes (62.2%) and pseudophakic in 31 eyes (37.8%). Lattice degeneration were documented in 22 eyes (26.8%) and in Ora serrata tears in 2 eyes (2.4%). Pathological myopia (defined as axial length 26.5 mm or more and a spherical equivalent >-6 diopters) was found in 21 eyes (25.6%). At presentation of RRD; the macula was attached in 44 eyes (53.7%) and macula off in 38 eyes (46.3%). The median number of the RT was 2 (95% CI 1.8–2.3, range 1–7) and the median extensions of the RD was 5 hours (95% CI 4.1–5.2, range 2–10 hours). Proliferative vitreoretinopathy stage B was found in all of patients at the presentation. The median BCVA in LogMAR preoperative was 0.5 (95% CI 0.7–1.1, range 0–2.3).
Intraoperative Demographics
The intraoperative demographics for all the patients are illustrated in Table 2. Forty-five eyes underwent combined CB and PPV, from which 21 eyes were phakic and 24 eyes were pseudophakic. Similarly, 37 eyes underwent standard PPV procedure from which 28 eyes were phakic and 9 eyes pseudophakic. Pseudophakic eyes were statistically significant lower in the PPV group in comparison to the combined group, p = 0.001. However, retinal tears > 3 were statistically significantly more prevalent in the combined group than the PPV group, p = 0.001. RD extending 4 hours and more were significantly more observed in the combined group in comparison to the PPV group, p = 0.0001. Nevertheless, inferior RD was more seen in the combined group than the PPV group, p = 0.001. In two eyes in PPV group, silicone oil was instilled and removed after three months due to re-detachment of the retina under gas during the operation. Phacoemulsification was combined in one eye in the SB & PPV group due to the presence of significant cataract obliterating fundus view. Scleral perforation in the CB & PPV group occurred in two eyes that was directly treated through adjustment of the CB onto the perforation site. Intraoperative lens touch occurred in two eyes which required further surgical treatment of traumatic cataract after three months. The duration of the surgery was statistically significantly longer in the combined CB & PPV compared to standard PPV (135 ± 4.5 minutes versus 92.4± 5 minutes), p < 0.001 respectively, Figure 1.
 |
Table 2 Intraoperative Patient’s Demographics |
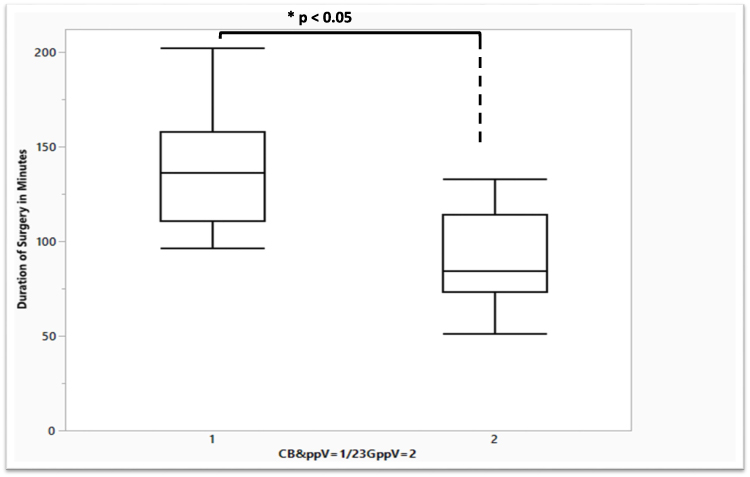 |
Figure 1 Boxplot diagram showing the duration of the surgery in minutes in combined CB & PPV (1) and in PPV (2) alone. The whiskers indicate minimum and maximum values, the length of boxes represents the interquartile range, and the horizontal line in the boxes shows the median time. Combined CB& PPV were associated with a statistical significant longer operation duration than compared to PPV alone, *p-value 0<0.05. |
Anatomical Surgical Outcomes
Single-operation anatomic success was achieved in 40 eyes in the combined group and 35 eyes in the PPV group (88.8% and 94.5%, respectively). There was no statistically significant difference in the success rate between both operations, p = 0.65, Table 3. Five eyes in the combined CB & PPV underwent reoperation due to retinal re-detachment requiring 360° retinectomy and 360° circumferential laser-retinopexy and silicone oil endotamponade. Two eyes in the PPV group underwent reoperation, one due to retinal re-detachment and the other due to expulsive choroidal bleeding that required cutting drainage and silicone oil endotamponade. The median postoperative BCVA was LogMAR 0.4, 95% CI (0.4–0.7, range 0–2.3), which was statistically significant compared to the preoperative BCVA median LogMAR 0.5 (95% CI (0.7–1.1, range 0–2.3), P = 0.0013, Figure 2. Postoperatively, in 46.4% of the patients were having a reading visual acuity. The main postoperative complication observed was the development of secondary cataract in both groups, followed by cystoid macular edema and secondary epiretinal membrane. After combined CB & PPV, phacoemulsification was required in eight eyes versus five eyes in the PPV group. The presence of subretinal Perfluorodecalin was reported in only a single eye in the CB & PPV.
 |
Table 3 Single Operation Anatomical Success (SOAS) |
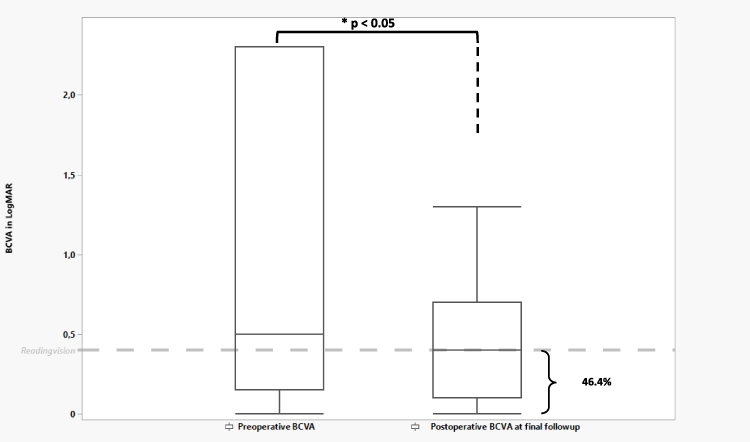 |
Figure 2 Boxplot diagram showing the BCVA in LogMAR preoperatively and postoperatively. The whiskers indicate minimum and maximum values, the length of boxes represents the interquartile range. The dashed line in the boxes shows the reading vision 0.4LogMAR, 46.4% of the patients were having a reading vision. There was statistically significant difference in the BCVA postoperative, *p-value <0.05. |
Discussion
Experience is known to play a major role in achieving successful re-attachment of the retina and preserving the visual acuity after RRD.15,16 However, experience can be obtained through supervision, the ability to learn different surgical techniques and a senior surgeon’s advice. The experience of senior vitreoretinal surgeon is of a significant importance in guiding junior vitreoretinal surgeons in decision-making which type of retinal surgery is suitable for each individual case. The preoperative discussion between the senior and the junior surgeon is of crucial importance in the learning process. Different clinical findings that might be of important surgical relevance in the decision-making of the surgery such as the presence of PVR, the localization of the RT, and whether RT are located anterior or posterior to the equator. Since multifactorial factors such as age, lens status (phakic or pseudophakic), attachment or detachment of vitreous, location and extensions of the RD, number of RT, stage of the PVR, plays an important role in the decision of surgery.7,13,17–21
Another fact of similar importance is that the learning curve in vitreoretinal surgery requires a certain number of RD surgeries, skill advancement towards surgical refinement occur after at least 200 surgeries and require a longer duration of practice.10,11 In a recent study that investigated the learning curve in ten vitreoretinal surgeons at the beginning of their training in RD surgery, from which more than 75% of the RD surgeries were operated with PPV; the anatomical success in treatment of primary non-complicated RD reached 80% within the first 200 surgeries.10 However, the variability between individual learning curve was relatively high, especially in the first 100 surgeries, where some surgeons experienced a re-detachment rate ranging from 25% to 40%.10 Another study that discussed the relationship between surgical experience and success rate in unexperienced retinal surgeons operating non-complicated RD with either scleral buckle or combined PPV & CB concluded that experience is indeed an essential factor influencing the outcome of RD surgery, mainly at the beginning of the training period and requiring 500 surgeries and a duration of four years of training.9
Furthermore, another study that evaluated the learning curve in primary vitrectomy without scleral buckling in non-complicated pseudophakic retinal detachment in unexperienced retinal surgeons showed that the success rate increased significantly from 66.7% after one year to 80% after two years.11 The study concluded that; to reach approximately the same success rate as an experienced surgeon, a less experienced surgeon probably requires between 2 and 3 years or approximately 180 surgical procedures for RD.11
However, in clinical practice, vitreoretinal fellowship programs worldwide are usually offered by a limited number of institutions and are usually confined to two years. Hence, surgical teaching on the background of medical-based evidence is essential to achieve higher competency within this period in terms of higher success and quality. Senior guidance is paramount to junior surgeons in the decision-making and other aspects; advice regarding viewing system, additive exocryopexy, combing RD surgery with cataract surgery and CB suturing techniques in cases of thin sclera as seen with pathological myopia. The acquisition of psychomotor skills and the ability to master different surgical skills and techniques is of decisive importance but should be based on an ample knowledge background.
In our study, remarkably, we were able to attain a surgical success rate of more than 85% in treatment of primary non-complicated RD either with standard PPV procedure or combined CB & PPV in a duration of one year of training through preoperative case selection under supervision of experienced retinal surgeon and with two different surgical approaches. Case selection was bases according to the site of the RD (above or below the 3-o’clock and 9-o’clock meridian), number of the RT, RD extensions, retinal degenerations and lens status. To the best of our knowledge, this is the first study that considered preoperative case selection as an essential tool for deciding RD surgery.
Interestingly, Heimann et al discussed previously that due to the broad spectrum of the different anatomical RD situations, a tailored approach with different methods for diverse situations seems to be more reasonable than a ʽʽone method for all concept”.22 A recently published retrospective study that discussed the outcomes of PPV alone versus combined CB & PPV; determined a higher surgical success rate after combining CB & PPV compared to PPV alone, 92.2% versus 81.1%, respectively.13 Nevertheless, combined CB & PPV achieved higher surgical success in phakic eyes than in pseudophakic eyes (92.9% versus 68.6%).13 We achieved similar results to the above-mentioned study; however, with a slightly higher rate in PPV alone, 94.5%, than combined CB & PPV, 88.8%. This is explicable given that the PPV group had RD with a limited number of RT (≤3) and RD extensions (≤4 hours); however, the RD in the combined CB & PPV group were more complicated cases in terms of multiple RT (≥4), RD extension (≥4 hours) and with inferior RD.
The lens status in RD surgery has always been of substantial importance in the decision of RD surgery. Previously, Heimann et al demonstrated that scleral buckling was better than PPV in treating phakic RD.5 The results of the VIPER study demonstrated that PPV alone is non-inferior when compared to combined CB & PPV (87.7% versus 87.7%) in the treatment of pseudophakic inferior RD.7 On the contrary, results by Starr et al comparing PPV alone versus PPV combined with CB in treating inferior RD in phakic eyes showed a significantly higher surgical success in phakic eyes in the latter compared to PPV alone, 85.2% versus 68.6%, respectively.20 In our study, a combined CB & PPV approach was utilised for all patients with inferior RD. Inferior RD in phakic eyes are difficult to manage for various reasons; complete removal and shaving of the vitreous base is usually impossible without touching the lens and the left behind vitreous strands remains as a cornerstone for PVR-reactions, consequently leading to new retinal holes. This is of even greater importance for junior vitreoretinal surgeons as their surgical technique is still under development and the duration of surgery is usually longer. Another problem with inferior RD is that sufficient retinal tamponade is difficult to achieve leading to failure to close the RT or re-opening of a closed RT.23 CB is for junior vitreoretinal surgeon very helpful in complex cases as; multiple retinal tears, missed retinal tear or in cases with bad fundus contrast view as seen for instance with high myopic patients. This because in the case of a missed tear or not full treated tear the CB will support the tear. A recent study, have shown that 34% of the retinal re-detachment occurring with unexperienced surgeon operated primarily with standard PPV occurs due to untreated tears or missed tears.22
Numerous studies had evaluated the success of primary PPV as standalone procedure in the treatment of RD in experienced retinal surgeon.7,22,24,25 The single surgical success rate ranged from 72% to 92% through the different surgical approach such as 20, 23 and 25 gauge vitrectomy. One of the essential factors leading to retinal re-detachment was the undiagnosed retinal break, followed by the combination of new breaks and PVR.22
Furthermore, a recent study discussing the surgical success of PPV using 23 and 25-gauge vitrectomy performed by an unexperienced retinal surgeon showed that retinal re-detachment occurred due to untreated retinal breaks in 34% and breaks in the treated area in 26%.8 Consequently, in our study, the PPV approach was performed using 4-port vitrectomy with chandelier endoillumination and under circular 360° scleral indentation to avoid and decrease the incidence of missed retinal breaks. The benefit of chandelier endoillumination and 360° scleral indentation in decreasing the risk of retinal re-detachment has also been recently evaluated by Wakili et al, where chandelier endoillumination with external indentation was associated with a lower incidence of retinal re-detachment when compared with external indentation and external illumination.26
Moreover, in our study, meticulous consideration was given to the fundus drawing preoperatively to ensure the location and number of the RT and extensions of the RD according to the 3-o’clock and 9-o'clock meridian. It is worth mentioning that the fundus drawing was the most crucial examination tool for the inclusion criteria in the SPR study; anatomical details established the criteria of medium RD severity.18
Although we utilised both types of surgeries in our study and a higher SSOS was achieved with both types, however, combined CB & PPV approach was associated with a statistically significant and more prolonged operation duration compared to PPV alone, p < 0.001.
Limitations of the present study include its retrospective design, a single surgeon and a relatively follow-up period of 3 months. Nonetheless, we were able to demonstrate in our study, as compared to previous studies, that a high surgical success does not necessarily require a higher volume of RD surgeries and a longer duration of practice but can be accomplished within one year of training via supervision, guidance in decision making and the ability to learn different surgical approaches in the treatment of RD such as PPV alone and combined PPV & CBV. The discussions of every case preoperatively between senior and junior surgeons are of crucial importance for junior surgeons in both gaining clinical and surgical experience.
Vigilant observation of the postoperative outcomes during the entire training period is indispensable, not only to assist the success rates but also to monitor other elements that could influence the outcome given that a successful retinal re-attachment is not an exclusive means of success; for instance, the absence of retinal folds or subretinal perfluorodecalin is vital.
In conclusion, we elaborated that junior retinal surgeons can accomplish a high surgical success rate of more than 85% with PPV as a standalone procedure or a combined CB & PPV approach in treating RD. Learning different retinal surgical approaches, especially the ability of mastering encircling band surgery (CB) helps junior vitreoretinal surgeons to perform complex RD surgery for example with multiple retinal tears and inferior retinal detachment in phakic eyes with a high success rate.
Key Messages
- Preoperative case selection under supervision of an experienced vitreoretinal surgeon can aid junior vitreoretinal surgeons achieve more than 85% surgical success defined as retinal re-attachment after one operation in surgical repair of rhegmatogenous retinal detachment either with pars plana vitrectomy (PPV) alone or PPV combined with encircling band.
Ethical Approval
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This work conformed to the Declaration of Helsinki and was conducted with approvals from by the Ethic Committee of the University of Würzburg, approval number 20230704 01. Informed consent were obtained from all the patients preoperatively.
Funding
No funding was received for this research.
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grant); participation in speaker’s bureaus; membership, employment or other equity interest, or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in subject matter or materials discussed in the manuscript.
References
1. Eckardt C, Eckert T, Eckardt U. 27-gauge Twinlight chandelier illumination system for bimanual transconjunctival vitrectomy. Retina. 2008;28(3):518–519. doi:10.1097/IAE.0b013e3181607a0f
2. Oshima Y, Awh CC, Tano Y. Self-retaining 27-gauge transconjunctival chandelier endoillumination for panoramic viewing during vitreous surgery. Am J Ophthalmol. 2007;143(1):166–167. doi:10.1016/j.ajo.2006.07.051
3. Romano MR, Cennamo G, Ferrara M, et al. Twenty-Seven-Gauge Versus 25-Gauge Vitrectomy for Primary Rhegmatogenous Retinal Detachment. Retina. 2017;37(4):637–642. doi:10.1097/IAE.0000000000001215
4. Feltgen N, Heimann H, Hoerauf H, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR study): risk assessment of anatomical outcome. SPR study report no. 7. Acta Ophthalmol. 2013;91(3):282–287. doi:10.1111/j.1755-3768.2011.02344.x
5. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142–2154. doi:10.1016/j.ophtha.2007.09.013
6. Heimann H, Bornfeld N, Bartz-Schmidt U, et al. Analysis of the surgeon factor in the treatment results of rhegmatogenous retinal detachment in the “scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study”. Klin Monbl Augenheilkd. 2009;226(12):991–998. doi:10.1055/s-0028-1109873
7. Mazinani B, Baumgarten S, Schiller P, et al. Vitrectomy with or without encircling band for pseudophakic retinal detachment: a multi-centre, three-arm, randomised clinical trial. VIPER Study Report No. 1--design and enrolment. Br J Ophthalmol. 2016;100(3):405–410. doi:10.1136/bjophthalmol-2015-306732
8. Keller J, Haynes RJ, Sparrow JM. Sequential Hypothesis Testing to Characterise the Learning Curve and Monitor Surgical Performance in Retinal Detachment Surgery. Ophthalmologica. 2016;235(3):157–162. doi:10.1159/000443749
9. Mazinani BA, Rajendram A, Walter P, et al. Does surgical experience have an effect on the success of retinal detachment surgery? Retina. 2012;32(1):32–37. doi:10.1097/IAE.0B013E3182411CD2
10. Radeck V, Helbig H, Barth T, et al. The learning curve of retinal detachment surgery. Graefes Arch Clin Exp Ophthalmol. 2021;259(8):2167–2173. doi:10.1007/s00417-021-05096-1
11. Dugas B, Lafontaine P-O, Guillaubey A, et al. The learning curve for primary vitrectomy without scleral buckling for pseudophakic retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2009;247(3):319–324. doi:10.1007/s00417-008-0997-y
12. Schimel AM, Grand MG, H.w. F Jr. Surgery for retinal detachment: does experience matter? Retina. 2012;32(1):1–3. doi:10.1097/IAE.0B013E3182411D04
13. Echegaray JJ, Vanner EA, Zhang L, et al. Outcomes of Pars Plana Vitrectomy Alone versus Combined Scleral Buckling plus Pars Plana Vitrectomy for Primary Retinal Detachment. Ophthalmol Retina. 2021;5(2):169–175. doi:10.1016/j.oret.2020.09.013
14. Lean JS, Stern WH, Irvine AR, et al. Classification of proliferative vitreoretinopathy used in the silicone study. The Silicone Study Group. Ophthalmology. 1989;96(6):765–771. doi:10.1016/S0161-6420(89)32821-1
15. Miki D, Hida T, Hotta K, et al. Comparison of scleral buckling and vitrectomy for retinal detachment resulting from flap tears in superior quadrants. Jpn J Ophthalmol. 2001;45(2):187–191. doi:10.1016/S0021-5155(00)00377-4
16. Oshima Y, Yamanishi S, Sawa M, et al. Two-year follow-up study comparing primary vitrectomy with scleral buckling for macula-off rhegmatogenous retinal detachment. Jpn J Ophthalmol. 2000;44(5):538–549. doi:10.1016/S0021-5155(00)00205-7
17. Agarkar S, Gokhale VV, Raman R, et al. Incidence, Risk Factors, and Outcomes of Retinal Detachment after Pediatric Cataract Surgery. Ophthalmology. 2018;125(1):36–42. doi:10.1016/j.ophtha.2017.07.003
18. Feltgen N, Weiss C, Wolf S, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study (SPR Study): recruitment list evaluation. Study report no. 2. Graefes Arch Clin Exp Ophthalmol. 2007;245(6):803–809. doi:10.1007/s00417-006-0399-y
19. Gonzalez MA, Flynn HW, Smiddy WE, et al. Surgery for retinal detachment in patients with giant retinal tear: etiologies, management strategies, and outcomes. Ophthalmic Surg Lasers Imaging Retina. 2013;44(3):232–237. doi:10.3928/23258160-20130503-04
20. Starr MR, Obeid A, Ryan EH, et al. RETINAL DETACHMENT WITH INFERIOR RETINAL BREAKS: primary Vitrectomy Versus Vitrectomy With Scleral Buckle (PRO Study Report No. 9). Retina. 2021;41(3):525–530. doi:10.1097/IAE.0000000000002917
21. Walter P, Hellmich M, Baumgarten S, et al. Vitrectomy with and without encircling band for pseudophakic retinal detachment: VIPER Study Report No 2-main results. Br J Ophthalmol. 2017;101(6):712–718. doi:10.1136/bjophthalmol-2016-309240
22. Heimann H, Zou X, Jandeck C, et al. Primary vitrectomy for rhegmatogenous retinal detachment: an analysis of 512 cases. Graefes Arch Clin Exp Ophthalmol. 2006;244(1):69–78. doi:10.1007/s00417-005-0026-3
23. Ziemssen F, Bartz-Schmidt KU. Vitrectomy with or without cerclage in the treatment of retinal detachment. Ophthalmologe. 2004;101(6):554–562. doi:10.1007/s00347-004-1041-1
24. Susskind D, Neuhann I, Hilgers R-D, et al. Primary vitrectomy for rhegmatogenous retinal detachment in pseudophakic eyes: 20-gauge versus 25-gauge vitrectomy. Acta Ophthalmol. 2016;94(8):824–828. doi:10.1111/aos.13133
25. Tsang CW, TZE-ON CHEUNG B, LAM RF, et al. Primary 23-gauge transconjunctival sutureless vitrectomy for rhegmatogenous retinal detachment. Retina. 2008;28(8):1075–1081. doi:10.1097/IAE.0b013e31817b98ba
26. Wakili P, Boden KT, Szurman P, et al. Influence of the scleral indentation technique on the re-detachment rate following retinal detachment surgery. Int J Retina Vitreous. 2022;8(1):12. doi:10.1186/s40942-022-00362-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.