Back to Journals » Risk Management and Healthcare Policy » Volume 19
The Role of Information Technology in Strengthening Vital Statistics in Public Health Institutions in Sana’a, Yemen
Authors Noman AS ![]() , Alshargabi K, Noman S
, Alshargabi K, Noman S
Received 15 March 2026
Accepted for publication 11 June 2026
Published 15 June 2026 Volume 2026:19 609380
DOI https://doi.org/10.2147/RMHP.S609380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Al-Safi Noman,1 Kassim Alshargabi,1,2 Sarah Noman3
1Center of Public Administration Development, Sana’a University, Sana’a, Yemen; 2Faculty of Commerce and Economics, Amran University, Amran, Yemen; 3Department of Community Health, Faculty of Medicine and Health Sciences, Taiz University, Taiz, Yemen
Correspondence: Al-Safi Noman, Center for Public Administration Development, Sana’a University, Sana’a, 13886, Yemen, Email [email protected] Sarah Noman, Department of Community Health, Faculty of Medicine and Health Sciences, Taiz University, Taiz, 6803, Yemen, Email [email protected]
Background: Reliable vital statistics are essential for evidence-based health planning, policy formulation, and population health monitoring. In fragile and conflict-affected settings, however, weak digital infrastructure and fragmented health information often compromise data quality, timeliness, and accessibility. These limitations restrict the availability of reliable information for effective decision-making. Strengthening information technology (IT) capacity may therefore play a critical role in improving the performance and reliability of vital statistics in resource-constrained health settings.
Methods: This study employed a quantitative cross-sectional design to examine the role of IT in enhancing vital statistics in public health institutions in Sana’a, Yemen. Data were collected from 119 administrative and technical staff across 32 public health institutions using a structured questionnaire measuring key IT dimensions (devices and equipment, software, human resources, and networks and communications) and vital statistics dimensions (registration and compilation, coverage and inclusiveness, data accuracy and quality, and publishing). Structural Equation Modeling (SEM) was applied to assess the relationship between IT capabilities and the performance of vital statistics. Due to the cross-sectional design, the results should be interpreted as associations rather than causal effects.
Results: The findings revealed a strong and statistically significant positive relationship between IT and vital statistics performance (β = 0.83, p < 0.001), with IT explaining a substantial proportion of the variation in system performance (R2 = 0.69). Descriptive results indicated moderate utilization of IT, alongside relatively high performance of vital statistics systems. This pattern suggests that even partial adoption of digital technologies contributes meaningfully to improving data availability, accuracy, and reporting efficiency in resource-constrained settings.
Conclusion: This study provides empirical evidence that IT capabilities are strongly associated with improved performance of vital statistics in fragile and conflict-affected contexts. By demonstrating how digital capacity supports data reliability and informed decision-making under constrained conditions, the findings highlight the critical role of IT in strengthening data systems and addressing operational challenges. Targeted investments in digital infrastructure, workforce capacity, and system integration are essential for building resilient and data-driven health systems in similar settings.
Keywords: information technology, vital statistics, health information systems, digital health, fragile health systems, Yemen
Introduction
Information technology (IT) has become an indispensable driver of institutional development and societal progress across diverse sectors, particularly within health systems, where digital transformation increasingly shapes organizational performance and service delivery.1 Beyond operational efficiency, digital technologies play a central role in improving data quality and supporting evidence-based decisionmaking within health institutions. Advances in digital technologies have enhanced the ability of institutions to collect, process, and disseminate data with greater efficiency and accuracy.2
Weak digital infrastructure often leads to delayed reporting, inaccurate records, and fragmented information flows, limiting the effectiveness of decision-making at institutional and policy levels. These challenges are further compounded in fragile contexts such as Yemen, where health system fragmentation and weak coordination mechanisms have been shown to disrupt information flows and limit the effectiveness of health data systems.3
These technological capabilities are not merely technical enhancements; they serve as mechanisms to mitigate data-related risks that can undermine health system performance and decision making across different levels. Digital health tools are also increasingly used to enhance knowledge dissemination and improve access to health information across diverse clinical fields, including innovative communication formats such as medical podcasting, which have been highlighted as emerging tools for education and health equity in specialized areas of healthcare practice.4
Within this context, vital statistics encompassing data on births, deaths, marriages, divorces, and other key life events constitute the backbone of population statistics and public health planning.5 Reliable and timely vital statistics are essential for understanding population dynamics, monitoring health indicators, designing effective social and economic policies, and evaluating development outcomes.
In this study, vital statistics performance is operationally defined as the effectiveness of data registration and collection, coverage and comprehensiveness, data accuracy and quality, and dissemination and organization, consistent with established frameworks emphasizing completeness, timeliness, and quality of civil registration and vital statistics.6
When such systems are weak or fragmented, the consequences extend beyond data inaccuracies to misinformed policy decisions and inefficient resource allocation. Despite their critical importance, vital statistics in many developing countries continue to face persistent structural and operational challenges, including fragmented data collection processes, heavy reliance on manual tools, limited human capacity, and inadequate technological infrastructure.7
These challenges are further compounded by limited adoption of IT across public health institutions in developing contexts. As a result, deficiencies persist in the generation, management, and utilization of vital statistics data, restricting their effective use in planning and decision-making processes.8 Weak digital infrastructure and insufficient integration of information systems often undermine data quality, timeliness, and accessibility, thereby limiting the overall effectiveness of health information systems. Similar challenges have been documented in Yemen, where the performance of electronic health information systems has been constrained by limitations in data quality and reporting timeliness, particularly under fragile and conflict-affected conditions.9
Evidence from Risk Management and Healthcare Policy demonstrates that the implementation of clinical decision support and health information systems can enhance data utilization, improve system performance, and support safer and more efficient healthcare decision-making processes10 From a theoretical perspective, the relationship between IT and vital statistics performance can be explained by the DeLone and McLean information systems success model, which posits that system performance is shaped by the quality of information, technological systems, and their use within organizational contexts. Within this framework, IT capabilities act as enabling factors that enhance data quality, accessibility, and utilization, thereby improving overall performance of vital statistics.11
Yemen represents a particularly salient case within this broader landscape. Public health institutions in Sana’a operate under complex and fragile conditions characterized by severe resource constraints, damaged infrastructure, and administrative fragmentation resulting from prolonged conflict. Health information systems in Yemen rely heavily on traditional tools and lack clear technological policies, leading to delays, data inaccuracies, and limited use of statistical information for decision-making. Although vital statistics activities are formally conducted, their effectiveness, reliability, and long-term sustainability remain questionable.3
In such contexts, strengthening IT within vital statistics represents a critical strategy for improving data reliability and supporting more effective decision-making.
Strong digital systems can enhance data availability, accuracy, and transparency. However, while IT and vital statistics have been examined separately in prior research, empirical studies integrating these domains within fragile health systems remain scarce.12
This gap in the literature highlights the need for context-specific empirical evidence examining how IT can strengthen vital statistics in low-resource and fragile settings. In conflict-affected environments, weak digital infrastructure limits data availability, transparency, and the use of reliable information for evidencebased decision-making. A clearer understanding of how digital capacity contributes to improved data availability and institutional functioning is therefore essential. This study contributes primarily by providing empirical evidence from a fragile and underrepresented context rather than proposing a new theoretical relationship. Accordingly, this study addresses the following research question: What is the role of IT in enhancing the availability of vital statistics data in public health institutions in Sana’a, Yemen?
Materials and Methods
Study Design
This study adopted a quantitative, descriptive–analytical research design to examine the role of IT in enhancing vital statistics within public health institutions. A field-based survey approach was used to collect primary data from public-sector health institutions operating in Sana’a. The study was conducted during 2025, and data collection took place between 25 April 2025 and 3 June 2025. The quantitative design was appropriate for testing the hypothesized relationships between IT dimensions and vital statistics performance using statistical modeling techniques. This approach enables objective measurement of variables and empirical testing of theoretical assumptions. However, given the crosssectional nature of the study, the findings reflect associations observed at a single point in time and do not imply causal or temporal relationships between variables.
A multistage probability sampling strategy was implemented. At the institutional level, public health institutions were treated as clusters, and simple random sampling was applied to ensure representation across different facility types. At the respondent level, a census approach was adopted within selected institutions to obtain comprehensive data from relevant personnel.
Population and Sampling
The target population comprised 96 public health institutions operating in Sana’a, including hospitals, health centers, medical complexes, health units, and administrative offices. These institutions constitute the formal public health service delivery system in the study area. Due to the ongoing challenges affecting the health sector in Yemen, some institutions lacked sufficient technological infrastructure or specialized units related to vital statistics. Therefore, the study focused on institutions with functional IT-related activities and relevant vital statistics operations that aligned with the objectives of the research.
First Stage: Institutional Sampling
At the first stage, 32 institutions (33% of the total population) were selected using simple random sampling. A complete list of institutions served as the sampling frame, and each institution had an equal probability of selection. This method minimized selection bias and enhanced representativeness across service levels.
Second Stage: Respondent Selection
At the second stage, a census (complete enumeration) method was employed within each selected institution. All administrative and technical staff directly involved in IT operations and vital statistics activities were included. No eligible participants within the selected institutions were excluded from the study. This ensured that data were obtained from individuals with direct knowledge and practical experience relevant to the study constructs.
A total of 125 questionnaires were distributed, of which 119 valid responses were returned, yielding a response rate of 95.2%. The final sample size (n = 119) was considered adequate for Structural Equation Modeling (SEM) given the relative simplicity of the proposed model, which included a limited number of latent constructs and structural paths. Previous methodological literature suggests that SEM can be appropriately applied in models with moderate complexity when sample sizes exceed 100 participants.13 Nevertheless, the absence of a formal statistical power analysis should be acknowledged as a methodological limitation, and future studies are encouraged to employ larger samples and formal power estimation procedures.
Study Tool
Data were collected using a structured questionnaire developed specifically for the objectives of this study. The instrument consisted of 34 items designed to measure the key constructs of information technology (IT) and vital statistics. IT was operationalized as a multidimensional construct comprising four dimensions: devices and equipment, software, human resources, and networks and communications. Vital statistics were similarly conceptualized as a multidimensional construct, including registration and compilation, coverage and inclusiveness, data accuracy and quality, and publishing. The measurement items were developed based on a review of relevant literature on health information systems and vital statistics and were adapted to suit the context of public health institutions in Yemen. Responses were recorded using a five-point Likert scale, ranging from strongly disagree (1) to strongly agree (5). To ensure content clarity and relevance, the questionnaire was reviewed and validated by a panel of subject-matter experts in health information systems and public health research, and minor revisions were made based on their feedback.
Reliability and Validity
The reliability and validity of the measurement instrument were rigorously assessed. Internal consistency validity was evaluated by examining the correlations between individual items and their corresponding dimensions, as well as between dimensions and the overall study constructs. All correlation coefficients were statistically significant, indicating satisfactory construct validity. Internal consistency reliability was evaluated using Cronbach’s Alpha, with all constructs exceeding the recommended threshold, indicating strong reliability. Composite Reliability (CR) values ranged between 0.70 and 0.95, while Average Variance Extracted (AVE) values exceeded the acceptable threshold, confirming convergent validity and the stability of the latent constructs. These results demonstrate that the instrument possesses adequate psychometric properties suitable for SEM analysis.
Statistical Analysis
Data analysis was conducted using SPSS version 24 to generate descriptive statistics, including means and standard deviations. Structural Equation Modeling (SEM) was applied using AMOS version 24 to test the hypothesized relationship between IT and vital statistics (IT → Vital Statistics). SEM was selected because it enables the simultaneous estimation of relationships among latent constructs measured by multiple indicators while assessing the explanatory power of IT on vital statistics performance.
Confirmatory factor analysis (CFA) was conducted to evaluate the measurement model prior to structural analysis. Model fit was assessed using multiple fit indices, including the chi-square/degrees of freedom ratio (CMIN/df), Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Tucker–Lewis Index (TLI). The obtained fit-index values, indicated acceptable model fit according to recommended thresholds (CMIN/df = 1.784, CFI = 0.977, TLI = 0.966, and RMSEA = 0.071).
Prior to SEM analysis, data normality was assessed using skewness and kurtosis statistics. The obtained values fell within the recommended acceptable ranges, indicating that the data were approximately normally distributed and suitable for SEM estimation. The alpha level of significance was set at a value of less than 0.05.
Ethical Approval and Informed Consent
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of Sana’a University, Center for Public Administration Development (CPAD) [Ref No. CPAD (KXM16) P952]. Written informed consent was obtained from all participants prior to their involvement in the study. To ensure confidentiality, participants were assigned unique identification codes and no personal identifiers were recorded. All results are presented in aggregated form to maintain participant anonymity and protect the privacy of the respondents.
Results
Characteristics of the Study Sample
A total of 125 questionnaires were distributed to staff members across 32 public health institutions in Sana’a. Of these, 119 valid responses were received and included in the analysis, resulting in a high response rate of 95.2%, which indicates strong engagement and data reliability. The participating institutions represented various levels of the public health system, including hospitals, health centers, medical complexes, health units, and administrative offices.
Health centers constituted the majority of institutions (76.47%), followed by hospitals (12.61%) and other public health facilities (10.92%), reflecting the structural composition of primary healthcare services in the study area. Regarding job roles, most respondents occupied administrative positions (68.07%), while technical staff accounted for 31.93%. This distribution suggests that the data were primarily provided by personnel directly involved in management, IT oversight, and vital statistics processes. In terms of professional experience, a substantial proportion of respondents (62.18%) reported more than 10 years of service, indicating a mature and experienced workforce. Concerning educational attainment, 47.06% held a bachelor’s degree, while diploma holders represented 26.05% and postgraduate degree holders accounted for 26.89%. This educational profile reflects an adequately qualified respondent group capable of providing informed responses on institutional information systems and performance (Table 1).
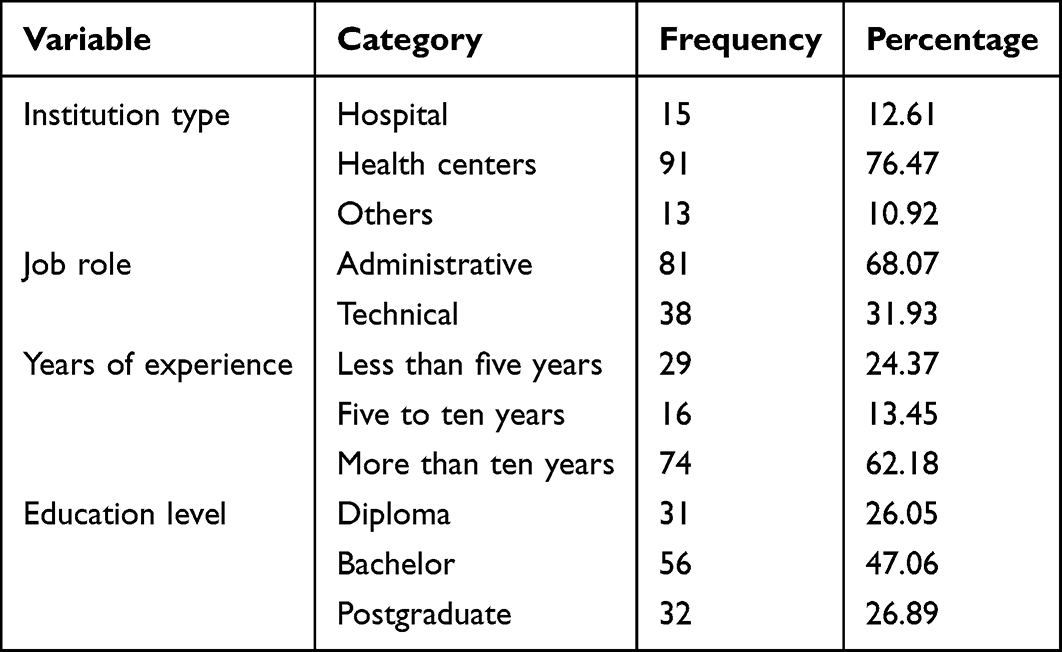 |
Table 1 Demographic and Institutional Characteristics of Respondents (n=119) |
Descriptive Statistics of the Main Study Variables
Descriptive analysis was conducted to assess the overall level of IT utilization and the availability of vital statistics in public health institutions. The results indicate that the overall level of IT utilization was moderate, with a mean score of 3.189. This suggests that while basic technological resources and capabilities are present, there remains substantial room for improvement in digital infrastructure and system integration. In contrast, the overall level of vital statistics performance was rated as high, with a mean score of 3.600, indicating relatively strong performance in registration, coverage, data accuracy, and dissemination processes (Table 2).
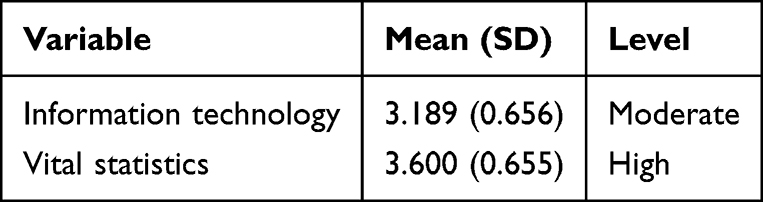 |
Table 2 Descriptive Statistics of the Main Study Variables |
Structural Equation Modeling and Hypothesis Testing
Structural Equation Modeling was employed to test the hypothesized relationship between IT and vital statistics. The model exhibited acceptable fit indices, indicating a good overall fit between the proposed theoretical framework and the observed data.
The results demonstrate a strong, positive, and statistically significant effect of IT on vital statistics (β = 0.83, t = 12.401, p < 0.001). The coefficient of determination (R2 = 0.69) indicates that 67.3% of the variance in the performance of vital statistics is explained by IT, underscoring the critical role of digital capabilities in supporting effective health information management (Table 3).
 |
Table 3 Structural Equation Modeling Results |
To visually summarize these findings, Figure 1 illustrates the structural model depicting the influence of IT on vital statistics.
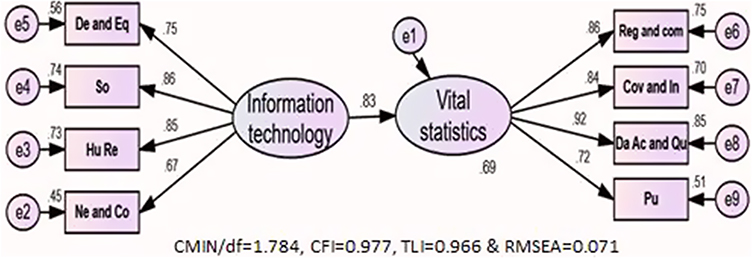 |
Figure 1 Effect of Information Technology on Vital Statistics. Information Technology is measured by four indicators: devices and equipment (De and Eq), software (So), human resources (Hu Re), and networks and communications (Ne and Co). Vital Statistics is measured by four indicators: registration and compilation (Reg and Com), coverage and inclusiveness (Cov and In), data accuracy and quality (Da Ac and Qu), and publishing (Pu). The model shows a positive structural relationship between Information Technology and Vital Statistics (β = 0.83), with R2 = 0.69, indicating that Information Technology explains 69% of the variance in Vital Statistics. Model fit indices indicate a good fit to the data (CMIN/df = 1.784, CFI = 0.977, TLI = 0.966, and RMSEA = 0.071). |
As shown in Figure 1, IT exerts a substantial and statistically significant impact on vital statistics performance. The path diagram clearly demonstrates the magnitude of this effect and highlights the central role of IT in enhancing the availability, accuracy, and dissemination of vital statistics in public health institutions in Sana’a, Yemen.
Overall, the results provide strong empirical evidence that IT is a key determinant of the effectiveness and reliability of vital statistics, confirming the study hypothesis and reinforcing the importance of investing in digital infrastructure and capabilities within resource-constrained health settings.
Summary of Key Findings
The results of this study provide clear empirical evidence that IT plays a pivotal role in enhancing the performance and availability of vital statistics in public health institutions in Sana’a, Yemen. Descriptive analysis indicated that while IT utilization is moderate, vital statistics perform relatively well, suggesting that current digital capabilities are contributing positively but have room for improvement.
Structural Equation Modeling confirmed a strong and statistically significant impact of IT on vital statistics performance, with 67.3% of the variance explained by IT. This high explanatory power highlights the central role of digital tools and resources in supporting data collection, accuracy, dissemination, and overall management of vital statistics, even within fragile and resource-constrained health systems. Figure 1 visually illustrates this relationship, emphasizing the substantial effect of IT on vital statistics performance. The findings underscore that investments in IT infrastructure, human capacity, and system integration are essential for strengthening health information systems and ensuring the reliability, timeliness, and accessibility of vital statistics in Yemen.
In summary, this study demonstrates that enhancing IT capabilities is a key strategy for improving vital statistics, providing evidence-based insights for policymakers, health administrators, and stakeholders seeking to strengthen health information management in fragile contexts.
Discussion
This study examined the role of IT in enhancing vital statistics in public health institutions in Sana’a, Yemen. Using SEM, the results demonstrated a strong and statistically significant positive effect of IT on vital statistics performance, with IT explaining a large proportion of the variation in vital statistics performance. These results indicate that digital capacity is a central determinant of institutional data performance and overall system quality. While this relationship is consistent with existing literature, the contribution of this study lies in validating it within a fragile, conflict-affected context.
From a risk management perspective, the findings suggest that weak IT increase vulnerability by exposing institutions to data inaccuracies, reporting delays, and fragmented information flows. This is particularly relevant in the Yemeni context, where health system fragmentation and weak institutional coordination have been identified as key factors contributing to inefficiencies and disruptions in information flow, ultimately affecting system performance and decision-making.3
Such weaknesses increase the likelihood of poor decision-making and may result in policy inefficiencies or misallocation of scarce resources. Conversely, stronger IT capabilities appear to improve transparency, reliability, and responsiveness within health information.
The descriptive analysis revealed that the overall level of IT utilization in public health institutions in Sana’a was moderate (mean = 3.189), while the performance of vital statistics was rated as high (mean = 3.600). This pattern suggests that although basic technological tools and capacities exist, IT integration remains incomplete, whereas vital statistics functions are comparatively more established.
The finding of moderate IT utilization aligns with broader evidence from developing country contexts where information systems are present but not fully integrated or optimized. For example, a narrative review of health information systems in developing countries found that adoption is often constrained by cultural, social, economic, political, and geographical barriers.8 Other studies reported socioeconomic constraints,14–17 lack of private sector participation; and lack of a clear institutional vision.18–22 Similarly, a study in Indonesia reported fragmentation, infrastructure limitations, and workforce disparities restricting optimal digital system usage.23
Overall, these findings suggest that IT adoption challenges in low-resource settings are typically structural and organizational rather than purely technical, limiting full system integration despite the availability of basic technologies.
These same factors likely contribute to the moderate IT utilization observed in Sana’a’s health institutions where resource constraints and fragmented system development complicate sustained IT integration.8 The relatively higher performance of vital statistics may reflect the longstanding institutional role of these systems in public health administration. However, such systems may still be vulnerable to delays and inaccuracies when digital support is limited.24
In summary, the descriptive findings reflect a common pattern in developing countries: moderate IT adoption alongside relatively more established routine data functions, although both remain constrained by system-level limitations.
The SEM analysis provides empirical support for the hypothesis that IT positively influences vital statistics performance (β = 0.83, p< 0.001), with strong explanatory power (R2 = 0.69). However, this effect should be interpreted cautiously, as it may be influenced by contextual factors, measurement limitations, and the cross-sectional design, which does not allow causal inference.
This finding aligns with literature showing that health IT improves data quality, timeliness, and accessibility.25,26 In low‑ and middle‑income countries (LMICs), IT has been associated with improved data management and reporting outcomes when properly implemented.27
These findings are consistent with evidence from Yemen, where electronic disease surveillance systems have improved data availability but continue to face challenges related to data quality and reporting timeliness, particularly in fragile and conflict-affected settings.9
In developing country contexts, studies also report that fragmented infrastructure and limited integration constrain the full benefits of IT, although improvements are still observed when systems are effectively implemented.24,28
However, it is important to note that the strong statistical association observed in this study does not exclude the influence of other contextual or organizational factors, such as workforce capacity, governance arrangements, and infrastructure constraints, which may also shape vital statistics performance. Another challenge identified in LMIC literature is that inadequate infrastructure, interoperability issues, and skill gaps often reduce the effectiveness of IT interventions.29
The high R2 observed in this study may reflect the relative importance of IT in a context with limited baseline digital infrastructure. Similar findings have been reported where incremental improvements in IT produce measurable gains in data performance.30
In summary, while the results confirm a strong positive association between IT and vital statistics performance, the findings should be interpreted as indicating an association rather than a standalone explanatory mechanism, given the influence of broader system and contextual factors.
Strengths of the Study
This study makes an important contribution to the literature by providing empirical evidence from a fragile and conflict-affected context that remains underrepresented in health information systems research. By focusing on public health institutions in Sana’a, the research offers context-specific insights into how digital technologies influence vital statistics performance in resource-constrained environments. The use of SEM enhances methodological rigor by allowing simultaneous assessment of latent constructs and explanatory relationships. Additionally, the high response rate strengthens data credibility and reduces the likelihood of non-response bias. The multistage probability sampling approach further enhances institutional representativeness, while the strong reliability and validity indicators confirm the robustness of the measurement model. Together, these strengths increase the internal validity and analytical reliability of the findings.
Limitations of the Study
Despite its contributions, several limitations should be acknowledged. First, the cross-sectional design limits the ability to draw definitive causal conclusions and to assess temporal effects, as relationships were examined at a single point in time. Accordingly, the findings should be interpreted as associations rather than evidence of causality or system improvement over time. Longitudinal or repeated crosssectional studies would provide stronger evidence regarding the sustained and causal impact of IT on vital statistics performance. Second, the study was geographically confined to public health institutions in Sana’a, which may limit generalizability to other regions of Yemen or to different national contexts. Third, the use of self-reported, perception-based data collected from a single source at one point in time may introduce implicit bias, including perception bias or social desirability bias, as responses may reflect subjective assessments rather than objective measures of system performance. This may influence the interpretation and strength of the observed relationships between variables. In addition, the high internal consistency values (Cronbach’s alpha > 0.90) may indicate potential redundancy among some measurement items. Furthermore, the model did not include control variables (eg, organizational or contextual factors), which may limit the robustness of the estimated relationships. Finally, although IT explained a substantial proportion of variance in vital statistics performance, other organizational, financial, and institutional factors were not included in the structural model and may also influence the effectiveness of vital statistics systems.
Recommendations
The findings underscore the urgent need to strengthen digital infrastructure within public health institutions in Yemen as a strategic risk management priority. Investment in interoperable systems, reliable connectivity, and centralized databases is essential to reduce data fragmentation and improve institutional accountability. Strengthening IT infrastructure should be viewed not only as a technological upgrade but as a structural reform aimed at improving data quality and reducing the risks associated with inaccurate or delayed vital statistics. Capacity building must accompany infrastructure investments. Continuous professional training in digital data management, analytical reporting, and system utilization is critical to ensure that technological improvements translate into measurable reductions in decisionmaking risk.
Establishing clear IT frameworks is equally important. Standardized protocols, data security regulations, interoperability standards, and accountability mechanisms should be institutionalized to enhance transparency and minimize institutional weaknesses. In fragile contexts, clarity in these frameworks reduces the risk of parallel systems and inconsistent reporting practices. In alignment with international digital health strategies, including the WHO Global Strategy on Digital Health, Yemen’s health sector should adopt a phased and context-sensitive digital transformation roadmap. Such a strategy can strengthen institutional resilience, improve data management practices, and support evidence-based policymaking in conflict-affected environments.
Future Research Directions
Future research should expand the geographical scope of investigation to include multiple regions within Yemen and comparative analyses across other LMICs to enhance generalizability. Longitudinal studies are needed to assess the long-term sustainability and causal effects of digital health investments on vital statistics. Further research could also incorporate additional explanatory variables, such as organizational culture, leadership support, and funding mechanisms, to develop more comprehensive models of health information system performance. Mixed-method approaches integrating qualitative insights may provide deeper understanding of implementation barriers and contextual dynamics that shape digital transformation in fragile health systems.
Conclusion
This study provides empirical evidence on the important role of IT in supporting vital statistics within public health institutions in Sana’a, Yemen. The findings indicate a strong and statistically significant positive association between IT and vital statistics performance, suggesting that digital capabilities are closely associated with improvements in data availability, quality, and reporting processes.
Although IT utilization was found to be moderate, vital statistics performance was relatively high. This suggests that while traditional mechanisms of registration and reporting remain functional, their efficiency and sustainability may be enhanced through greater integration of digital systems. In fragile and resource constrained contexts such as Yemen, strengthening IT infrastructure and capacity may support improvements in institutional data systems and decision-making processes.
The findings align with global policy directions emphasizing digital transformation in health systems. The World Health Organization, through the Global Strategy on Digital Health,31 highlights the importance of digital technologies in strengthening health information systems and improving data use. Similarly, the World Health Organization’s Health Metrics Network Framework emphasizes the role of integrated information systems in supporting reliable vital statistics.32 The present study provides context-specific empirical evidence that supports these global perspectives within a conflict-affected setting. Overall, the findings suggest that IT represents an important enabling factor for strengthening vital statistics systems. However, given the cross-sectional and perception-based nature of the data, these findings should be interpreted as associations rather than causal effects. In addition, the results are context-specific to public health institutions in Sana’a and may not be directly generalizable to other settings. Further research using longitudinal or multi-source data is recommended to better understand the long-term impact of digital investments in similar contexts.
Institutional Review Board Statement
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board of Sana’a University, Center for Public.
Administration Development (CPAD) [Ref No. CPAD (KXM16) P952].
Data Sharing Statement
The data that support the findings of this study are available from Al-Safi Noman upon reasonable request.
Acknowledgments
The authors would like to express their sincere appreciation to the administrative and technical staff working in public health institutions in Sana’a, Yemen, for their cooperation and valuable participation in this study. Their willingness to share their experiences and insights regarding IT and vital statistics greatly contributed to the successful completion of this research. The authors also acknowledge the support of the relevant public health authorities and institutions that facilitated data collection for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stoumpos AI, Kitsios F, Talias MA. Digital transformation in healthcare: technology acceptance and its applications. Int J Environ Res Public Health. 2023;20(4):3407. doi:10.3390/ijerph20043407
2. Organization WH. Digital Implementation Investment Guide (DIIG): Integrating Digital Interventions Into Health Programmes. World Health Organization; 2020.
3. Dureab F, Hussain T, Sheikh R, Al-Dheeb N, Al-Awlaqi S, Jahn A. Forms of health system fragmentation during conflict: the case of Yemen. Front Public Health. 2021;9:659980. doi:10.3389/fpubh.2021.659980
4. Richardson EM, Provencher LM. Podcasting in ophthalmology: advancing education, knowledge dissemination, and implications for health equity. Clin Ophthalmol. 2026;20:596945. doi:10.2147/OPTH.S596945
5. Jackson D, Wenz K, Muniz M, et al. Civil registration and vital statistics in health systems. Bull World Health Org. 2018;96(12):861. doi:10.2471/BLT.18.213090
6. Muñoz DC, Abouzahr C, de Savigny D. The ‘Ten CRVS Milestones’ framework for understanding civil registration and vital statistics systems. BMJ Global Health. 2018;3(2):1.
7. Cobos Muñoz D, de SavignyD, Sorchik R, et al. Better data for better outcomes: the importance of process mapping and management in CRVS systems. BMC Med. 2020;18(1):67. doi:10.1186/s12916-020-01522-z
8. Bagherian H, Sattari M. Health information system in developing countries: a review on the challenges and causes of success and failure. Med J Islamic Republic Iran. 2022;36:111. doi:10.47176/mjiri.36.111
9. Dureab F, Ahmed K, Beiersmann C, Standley CJ, Alwaleedi A, Jahn A. Assessment of electronic disease early warning system for improved disease surveillance and outbreak response in Yemen. BMC Public Health. 2020;20(1):1422. doi:10.1186/s12889-020-09460-4
10. Chen H, Peng J, Xu X, Li Y, Tong Z, Gao C. Development and application of a unplanned extubation assessment and clinical decision support information system. Risk Manag Healthc Policy. 2026;19:594033. doi:10.2147/RMHP.S594033
11. DeLone WH, McLean ER. The DeLone and McLean model of information systems success: a ten-year update. J Manage Inf Syst. 2003;19(4):9–11.
12. Kumar M, Gotz D, Nutley T, Smith JB. Research gaps in routine health information system design barriers to data quality and use in low‐and middle‐income countries: a literature review. Int J Health Plann Manag. 2018;33(1):e1–e9. doi:10.1002/hpm.2447
13. Hair JJF, Black WC, Babin BJ, Anderson RE. Multivariate data analysis. 2010;785.
14. Ishijima H, Mapunda M, Mndeme M, Sukums F, Mlay VS. Challenges and opportunities for effective adoption of HRH information systems in developing countries: national rollout of HRHIS and TIIS in Tanzania. Human Res Health. 2015;13(1):48. doi:10.1186/s12960-015-0043-1
15. Othman M, Hayajneh JA, Ali N, Ali N. An integrated success model for an electronic health record: a case study of Hakeem Jordan. Procedia Econ Finance. 2015;23:95–103. doi:10.1016/S2212-5671(15)00526-2
16. Kpobi L, Swartz L, Ofori-Atta AL. Challenges in the use of the mental health information system in a resource-limited setting: lessons from Ghana. BMC Health Serv Res. 2018;18(1):98. doi:10.1186/s12913-018-2887-2
17. Afrizal SH, Handayani PW, Hidayanto AN, Eryando T, Budiharsana M, Martha E. Barriers and challenges to Primary Health Care Information System (PHCIS) adoption from health management perspective: a qualitative study. Inf Med Unlocked. 2019;17:100198. doi:10.1016/j.imu.2019.100198
18. Tilahun B, Fritz F. Modeling antecedents of electronic medical record system implementation success in low-resource setting hospitals. BMC Med Inf Decis Making. 2015;15(1):61. doi:10.1186/s12911-015-0192-0
19. Verbeke F, Karara G, Nyssen M. Human factors predicting failure and success in hospital information system implementations in Sub-Saharan Africa. In: MEDINFO. Vol. 2015. eHealth-enabled Health: IOS Press; 2015:482–486.
20. Deriel E, Puttkammer N, Hyppolite N, et al. Success factors for implementing and sustaining a mature electronic medical record in a low-resource setting: a case study of iSanté in Haiti. Health Policy Plann. 2018;33(2):237–246. doi:10.1093/heapol/czx171
21. Sahay S, Nielsen P, Latifov M. Grand challenges of public health: how can health information systems support facing them? Health Policy Technol. 2018;7(1):81–87. doi:10.1016/j.hlpt.2018.01.009
22. Edoh TO, Pawar PA, Loko LY. Challenges facing health service delivery in developing countries and solution approaches: the case of Benin, a West-African developing country. In: Handbook of Research on Emerging Perspectives on Healthcare Information Systems and Informatics. IGI Global Scientific Publishing; 2018:515–559.
23. Aisyah DN, Setiawan AH, Mayadewi CA, Lokopessy AF, Kozlakidis Z, Manikam L. Understanding health information systems utilization across public health centers in Indonesia: cross-sectional study. JMIR Med Informat. 2025;13(1):e68613. doi:10.2196/68613
24. Koumamba AP, Bisvigou UJ, Ngoungou EB, Diallo G. Health information systems in developing countries: case of African countries. BMC Med Inf Decis Making. 2021;21(1):
25. Jamal A, McKenzie K, Clark M. The impact of health information technology on the quality of medical and health care: a systematic review. Health Inform Manag J. 2009;38(3):26–37. doi:10.1177/183335830903800305
26. Belardi P, Corazza I, Bonciani M, Manenti F, Vainieri M. Evaluating Healthcare performance in Low-and middle-income countries: a pilot study on selected settings in Ethiopia, Tanzania, and Uganda. Int J Environ Res Public Health. 2022;20(1):41. doi:10.3390/ijerph20010041
27. Ndabarora E, Chipps JA, Uys L. Systematic review of health data quality management and best practices at community and district levels in LMIC. Inf Dev. 2014;30(2):103–120. doi:10.1177/0266666913477430
28. Getachew N, Erkalo B, Garedew MG. Data quality and associated factors in the health management information system at health centers in Shashogo district, Hadiya zone, southern Ethiopia, 2021. BMC Med Inf Decis Making. 2022;22(1):154. doi:10.1186/s12911-022-01898-3
29. Moucheraud C, Schwitters A, Boudreaux C, et al. Sustainability of health information systems: a three-country qualitative study in Southern Africa. BMC Health Serv Res. 2017;17(1):23. doi:10.1186/s12913-016-1971-8
30. Hung YW, Hoxha K, Irwin BR, Law MR, Grépin KA. Using routine health information data for research in low-and middle-income countries: a systematic review. BMC Health Serv Res. 2020;20(1):790. doi:10.1186/s12913-020-05660-1
31. Organization WH. Global Strategy on Digital Health 2020-2027. World Health Organization; 2025.
32. Network HM. Framework and standards for country health information systems. 2008.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Effectiveness of DHIS2 and FAIR Data Approaches for Privacy-Preserving Health Data Analytics in Uganda: A Systematic Review
Basajja M, Paul-Chima UO
ClinicoEconomics and Outcomes Research 2025, 17:849-864
Published Date: 18 November 2025