")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Role of Emotion Regulation for General Self-Efficacy in Adolescents Assessed Through Both Neurophysiological and Self-Reported Measures
Authors Lande NM, Ask TF , Sætren SS, Lugo RG, Sütterlin S
Received 15 February 2023
Accepted for publication 28 July 2023
Published 25 August 2023 Volume 2023:16 Pages 3373—3383
DOI https://doi.org/10.2147/PRBM.S406702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Einar Thorsteinsson
Natalie Marie Lande,1,* Torvald F Ask,2,3,* Sjur Skjørshammer Sætren,4,5,* Ricardo Gregorio Lugo,2,3,6 Stefan Sütterlin2,6,7
1Fontenehuset, Fredrikstad, Norway; 2Department of Health, Welfare and Organization, Østfold University College, Halden, Norway; 3Department of Information Security and Communication Technology, Norwegian University of Science and Technology, Gjøvik, Norway; 4Department for Child and Adolescent Research, Norwegian Centre for Violence and Traumatic Stress Studies, Oslo, Norway; 5TIPS Centre for Clinical Research in Psychosis, Stavanger University Hospital, Stavanger, Norway; 6Centre for Digital Forensics and Cybersecurity, Tallinn University of Technology, Tallinn, Estonia; 7Faculty of Computer Science, Albstadt-Sigmaringen University, Sigmaringen, Germany
*These authors contributed equally to this work
Correspondence: Torvald F Ask, Department of Health, Welfare and Organization, Østfold University College, Høgskolen i Østfold, B R A veien 4, NO-1757, Halden, Norway, Tel +47 696 08 607, Email [email protected]
Background: Self-efficacy, the belief in one’s ability and capacity to organize and execute actions required to achieve desired results, is associated with adolescent academic achievement and reduced risk for psychopathology. Adolescent emotion regulation represents an important component in the relationship between self-efficacy and developmental outcomes, but the underlying neurophysiological mechanisms are poorly understood. It is unclear how emotion regulation strategies, which change with experience, and emotion regulation capacity, which is largely determined by genetics, contribute to the development of self-efficacy.
Aim: The present study aims to explore the relationship between emotion regulation and self-efficacy in adolescents. We hypothesize that neurophysiological emotion regulation capacity moderates the relationship between emotion regulation strategies and self-efficacy.
Methods: The present study applied a cross-sectional design. A sample of high-school students (N = 45, nfemale = 31, age = 17– 18) provided answers on the General Self-Efficacy Questionnaire and the Emotion Regulation Questionnaire. Vagal tone was used as an indicator for emotion regulation capacity.
Results: In the initial correlational analysis, reappraisal, but not expressive suppression nor vagal tone was associated with self-efficacy. Vagal tone was not associated with any self-report measures of emotion regulation or self-efficacy. Contrary to our hypothesis, vagal tone did not moderate the relationship between emotion regulation and self-efficacy.
Conclusion: This is the first study assessing the relationship between neurophysiological indicators of emotion regulation and self-efficacy. Our results do not indicate that vagal tone moderates the relationship between emotion regulation strategies and general self-efficacy. Future studies should also assess the possible influence of metacognition and interoception on relationships.
Keywords: adolescent self-efficacy, vagally mediated heart rate variability, emotion regulation capacity, cognitive reappraisal, self-efficacy development, expressive suppression
Introduction
An individual’s beliefs in their own abilities and capacity to organize and execute the actions required to achieve a desired result constitute the concept of self-efficacy (SE).1 SE represents a positive youth developmental construct that has been found associated with reduced risk for adolescent psychopathology and higher academic achievement in several domains.2–4 If people believe they have a personal sense of control, they are prone to a more proactive approach in their life.5 This is reflected in individuals with a higher sense of SE, as they seem to utilize metacognitive strategies to a greater extent, which further enhances self-regulatory capabilities.2,6 Self-efficacious students appear to work harder, persist longer in challenging situations, and are less anxious.1 A great body of research suggests that adolescent emotion regulation (ER) represents an important component in the relationship between SE and developmental outcomes.7–11 However, the neurophysiological mechanisms underlying the relationship between ER and SE, and the development of adolescents’ SE beliefs in general, are still poorly understood.12
Studies on the relationship between SE and physiological measures has been conducted in conjunction with neuroanatomical studies on regional gray matter and mean diffusivity, and behavioral studies on phobias and fear conditioning.13–18 In the behavioral studies, it was found that individuals who believe they can exert control over aversive events show less autonomic arousal than those who believe that they have less control. While these studies indicate how SE may influence emotional responses to challenge in line with the concept of ER-SE, they do not explain the neurophysiological mechanisms facilitating the effective formation of general-domain SE beliefs.19 Given the relationship between SE and ER, it is of interest to determine if SE beliefs are influenced by neurophysiological processes involved in ER.12,15–17
SE beliefs are traditionally considered to be influenced in four different ways.15 The first three processes; mastery of experiences, role-modeling, and persuasion, are well researched and understood. The fourth process is less understood and concerns one’s own judgment about the experienced emotional and somatic states of arousal occurring in response to challenge exposure.1,20 Thus, being able to regulate one’s own emotions may prevent an individual from feeling overwhelmed by challenging tasks. ER may also allow for processing task-relevant features needed to ensure desired outcomes, thus ensuring the individual a sense of mastery.21,22 ER ability is influenced by factors such as ER strategies, ER-SE, and neurophysiological ER capacity, among others.19,23–26 While ER strategies and ER-SE are subject to change as a result of experience, the neurocognitive processes underlying ER capacity such as executive function and modulation of arousal are largely influenced by genetics.9,22,24,27–30 Thus, ER capacity represents a determinant of an individual’s absolute ER threshold, essentially serving as a psychophysiological constant that cuts across situations, potentially having a more chronic influence on the development of general SE beliefs.
Both ER and prospective and retrospective self-referential judgements of performance abilities are dependent on an overlapping set of prefrontal cortical structures, including the dorsolateral and the medial prefrontal cortex.22,31–33 Together, these prefrontal structures are intimately involved in brain networks coordinating internally and externally guided behaviors to reach desired outcomes.22,34,35 Vagally mediated heart rate variability (vmHRV), which refers to the difference in time intervals between heart beats resulting from vagal input, is considered an index for vagal tone and a proxy for the prefrontal activity that reflects ER capacity.24,25,36 A growing body of evidence suggests that vagal tone is influenced by dorsolateral prefrontal cortex activity.37–42 In a recent study, resting vagal tone was associated with functional connectivity between dorsolateral prefrontal- and medial prefrontal-related brain networks responsible for solving tasks and directing attention towards internal states, but this association diminished when participants were exposed to stress.39 Thus, ER capacity, indicated by vagal tone at rest, may be an indicator of the threshold for when coordination between internally and externally guided cognitions is no longer possible, serving as a possible modulator of processes influencing SE.
Two of the most studied emotion regulation strategies are cognitive reappraisal and expressive suppression. Cognitive reappraisal is an antecedent- and goal-focused, flexible strategy aiming to modify the emotional impact of a situation by means of cognitive change, whereas expressive suppression is a response-focused strategy characterized by modulating current emotions through inhibiting the expression of them.23,43,44 When measured at rest, higher vagal tone is associated with various ER outcomes.21,26,45–47 This includes individual differences in daily reported affect in both challenging and everyday settings and more frequently using cognitive reappraisal as ER strategy in response to negative stimuli.21,46–48
The aim of this study is to assess the role of self-reported and neurophysiological indicators of ER on general SE in adolescents, thus covering a gap in the SE literature.12 SE beliefs are considered to be influenced by one’s own judgment about the experienced emotional and somatic states of arousal occurring in response to challenge exposure.1,20 A previous study found that vagal tone moderated the relationship between psychosocial stressors and psychopathology in adolescents.49 Because ER strategies arguably represent the steps to achieve a desired outcome, while ER capacity represents an individual’s neurophysiological threshold for when the strategies can no longer be successfully implemented, we hypothesize that vagal tone, as an indicator of prefrontal ER capacity, moderates the relationship between self-reported ER strategies and general SE beliefs (hypothesis: H).23,24,36,50
Materials and Methods
Ethics
The study was approved by the Norwegian Centre for Research Data. The study followed institutional guidelines when applying to the Norwegian Social Science Data Services (NSD) ethical guidelines for experimental studies. Approval was obtained by filling out the initial NSD online form. In accordance with NSD guidelines, informed consent from parents was not needed when all participants were 16 years or older. Only non-identifiable data was used, and all participants provided written informed consent and were debriefed about the purpose of the study after data collection. The present study complies with the Declaration of Helsinki, International Ethical Guidelines for Biomedical Research Involving Human Subjects and the International Guidelines for Ethical Review of Epidemiological Studies.
Sample Description
Forty-five healthy high school students (69% female, n = 31), 17–18 years of age at the time of data collection, were selected to participate in the present study. Four participants were excluded from data analysis due to invalid and missing results. Participants were recruited from high school classes, and everyone had chosen psychology as an optional subject.
Assessment, Design and Procedure
All self-report questionnaires were administered in paper format prior to recording of inter-beat intervals. Items on the questionnaires used to measure SE and ER were presented as statements and the participants used a pen to select the statements according to what fit them. There were no explicit options to leave items unanswered.
General Self-Efficacy Scale
SE beliefs are linked to distinct life domains of functioning and must be tailored to the specific situation of interest. However, some researchers have proposed a generalized sense of SE which is less context specific and explains a broader range of coping and performance.51,52 The present study was conducted utilizing a Norwegian translated version of the General Self-Efficacy Scale (GSE).3 The scale consists of ten Likert-scale items from 1 to 4, where higher scores indicate higher SE. GSE construct scores were generated from averaging all the scores of individual items. Construct validity has been shown in numerous domains and across cultures.53,54 Besides, according to Scholz et al, several research projects have yielded internal consistency (α = 0.75–0.91).3
Emotion Regulation Questionnaire
ER strategies were assessed through a Norwegian translated version of the Emotion Regulation Questionnaire (ERQ).54 ERQ consists of 10 Likert-scale items from 1 to 7 capturing habitual usage of cognitive reappraisal and expressive suppression. Higher scores indicate higher usage of the two emotion regulation strategies. ER construct scores were generated by averaging all the scores in each subscale. Psychometric evaluations of ERQ indicate high construct validity and high internal consistency for both reappraisal (Cronbach’s α = 0.91) and suppression (Cronbach’s α = 0.80).55–57
Days of Exercising
The participants were also asked to report how many days per week they engaged in physical exercising activities (days of exercising; DOE), as well as their usage of tobacco, caffeine, beta blockers, or other drugs that can cause disruptions in heart rate.
Vagally Mediated Heart Rate Variability
VmHRV was quantified from inter-beat intervals that were recorded for seven minutes with photoplethysmography by using the Alive Software (AliveTM by Somatic Vision, Inc.). Alive is used for recording inter-beat intervals in both clinical and non-clinical samples.58,59 The protocol was based on established recommendations for short-term recordings of inter-beat intervals for vmHRV quantification which suggests that five minutes of recording conducted at rest is required for quantifying reliable vmHRV indices.60 Thus, five minutes of the seven-minute recordings were intended for vmHRV analysis. Recordings were carried out after the participants had completed the self-report questionnaires, during school hours over four days in sound-attenuated rooms, with only one participant being recorded per room at any given time. Participants were asked to refrain from caffeine two hours before the assessment. Upon arrival, participants were seated, and some time was spent establishing rapport with each participant and confirming that they had abstained from coffee as agreed. Participants were then informed about the recording procedure and instructed to sit back in a comfortable position they could relax in. Three IOM finger sensors were then placed on the participant’s non-dominant hand. This was followed by instructions to relax by themselves for some minutes while breathing consistently at a natural pace, and to avoid bodily movements for the duration of the recording until the experimenter came back. Any participants that brought with them their phones to the site of recording were instructed to put their phone away after setting it to silent with vibration turned off. The participants were then left alone in the room for seven–eight minutes. Five minutes of highest quality, between the first 150 and the last 50 seconds of the inter-beat interval recordings were used for HRV quantification.
Data Reduction
Four participants were excluded due to missing participant code between self-report measure and recording of inter-beat intervals. There were no missing values in the remaining dataset. Five minutes of high-quality recording was selected from the middle parts of the seven minute recordings for vmHRV analysis, in line with established recommendations.60 R-peak extraction was used to detect inter-beat intervals and vmHRV was analyzed in the ARTiiFACT software.61 The detection of artifacts was done through the software, as well as by confirmatory visual inspection. Cubic spline interpolation was used to replace inaccurate IBIs.
The root mean square of successive differences (RMSSD) and the high-frequency component (HFms2; Fast-Fourier-Transformation, bandwidth 0.15 to 0.40 Hz), are the most commonly used indicators of vagal tone.60 We were mainly interested in RMSSD. HFms2 and RMSSD are usually highly correlated; thus, we included HFms2 in our initial analyses to test for this correlation.62 Mean HR and the percentage of successive NN intervals exceeding 50 ms (pNN50) were also quantified from the inter-beat interval recordings. Mean HR and pNN50 do not primarily indicate vagal mediation and were included for the possibility of comparison and replication with other studies. Normative data of vagal tone in healthy adolescents (non-athletes) with normal BMI indicate that RMSSD (ms) measures for girls are minimum 12.80 and maximum 256.30, and for boys, minimum 9.10 and maximum 350.40.63 Exclusion criteria followed the normative range as cut-off limits and was also compared to other studies.26 All participants were within the normal range.
Statistical Analysis
The means, standard deviations (SD), range, minimum, and maximum values were quantified for each variable and presented in Table 1. The relationships between GSE, ERQ, and vmHRV were initially explored through partial correlations controlling for DOE and sex. Results from all correlations are presented in Table 2.
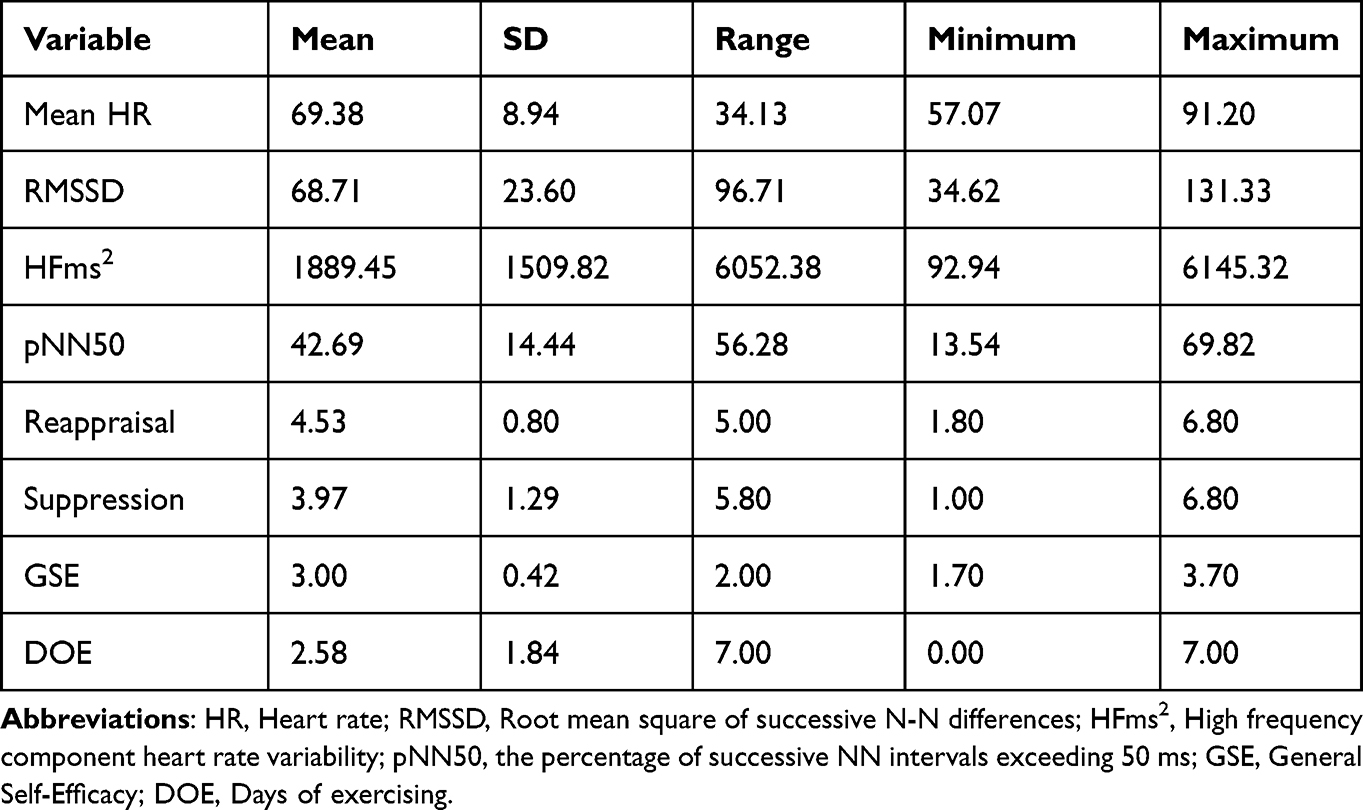 |
Table 1 Descriptive Statistics (N = 41) |
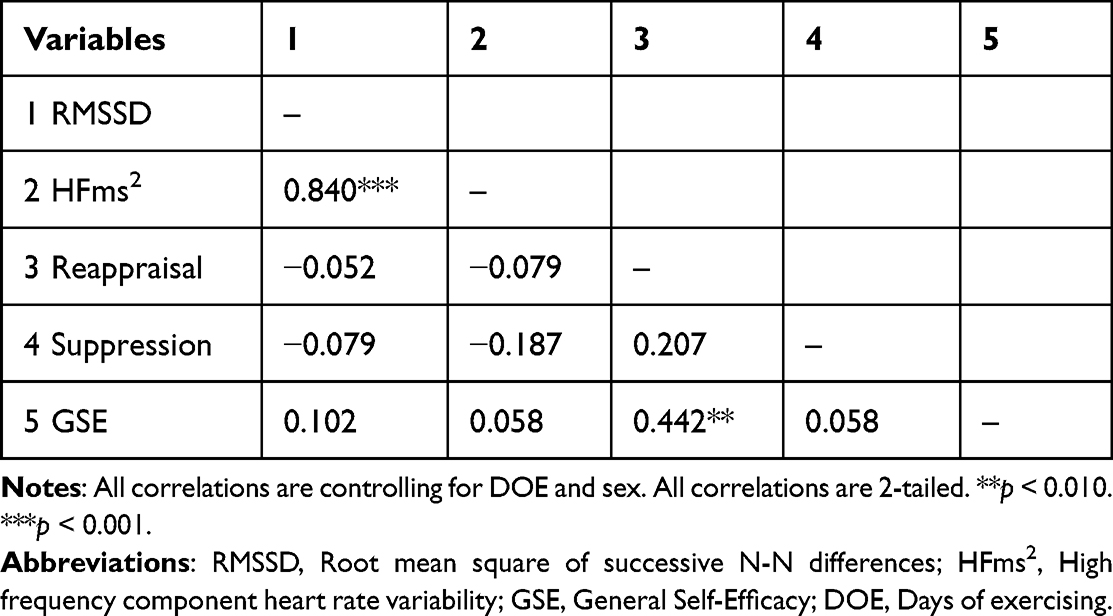 |
Table 2 Partial Correlations Controlling for DOE and Sex (N = 41) |
Hierarchical multiple linear regression analyses controlling for the effect of sex and DOE were conducted using RMSSD, HFms2, and ERQ subscales as predictors of GSE. First, sex and DOE were entered as predictors of GSE in the first model (model 1), reappraisal was included as predictor in the second model (model 2), and RMSSD was included as predictor in the third model (model 3). Results of the regression analysis are presented in Table 3.
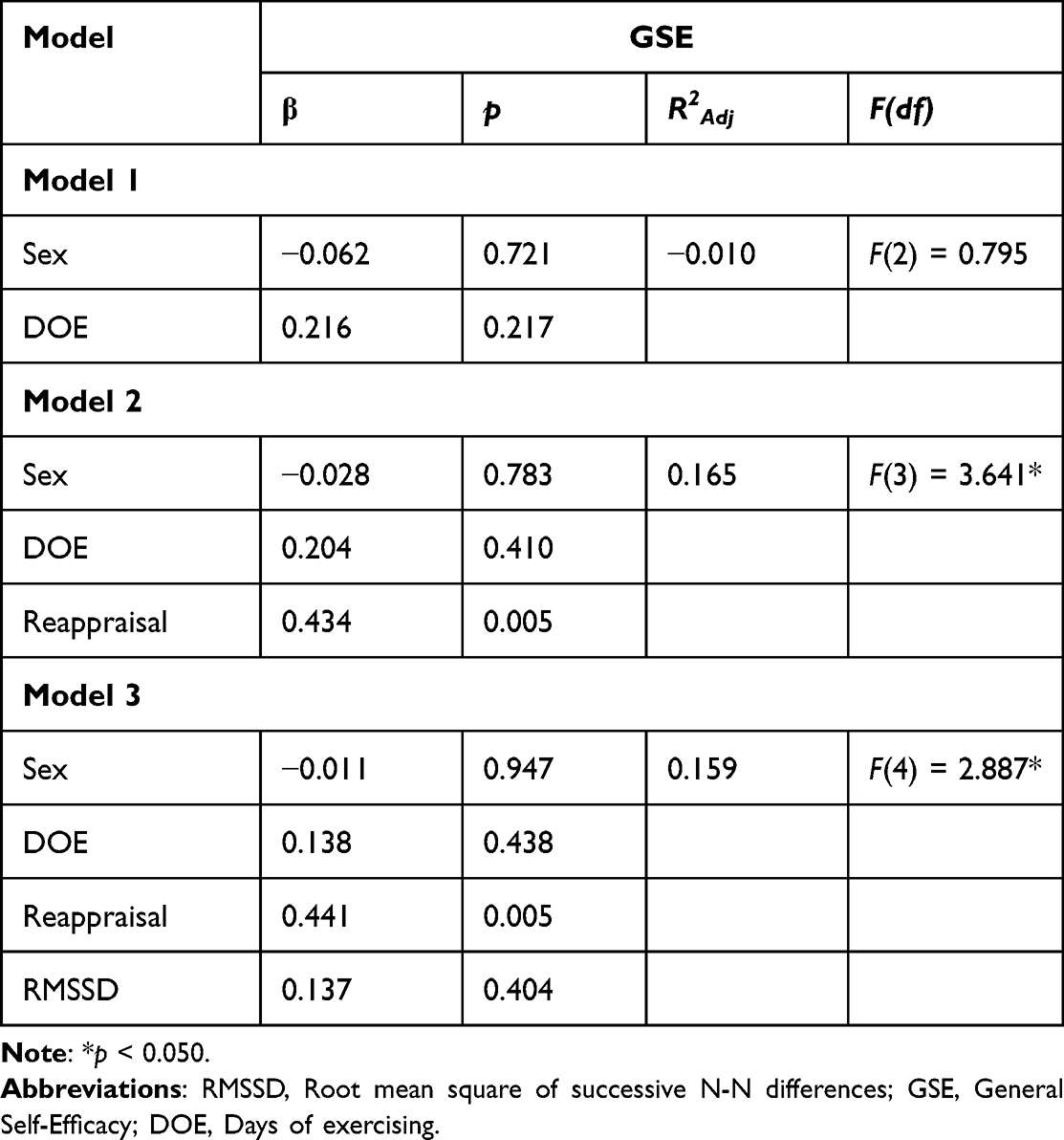 |
Table 3 Hierarchical Linear Regressions Predicting GSE (N = 41) |
To test the hypothesis that ER capacity moderates the relationship between self-reported ER strategies and general SE beliefs, moderation regression analyses were conducted using ERQ scores as independent variable, RMSSD as moderator variable, and GSE as dependent variable to assess if RMSSD influenced change in the relationship between ER and SE. Moderation analysis was conducted with the PROCESS macro-version 3.5 for SPSS.64
How an individual judges their ability to perform the actions needed to reach desired outcomes is influenced by metacognition, where favorable estimations can be due to overconfidence rather than metacognitive accuracy.21,65 The accuracy to which one judges one’s own performance abilities and vagal tone are influenced by the same prefrontal structures.32,33,37,39,42 Vagal tone is negatively associated with overconfidence and positively associated with metacognitive accuracy.21,66 As we use self-report measures of ER strategies and GSE, it is possible that metacognition is a confounding variable in the present analysis. In a follow-up analysis, and because we did not measure metacognition, this possibility was explored by plotting the quadratic relationship between the z-transformed RMSSD variable (predictor) and the z-transformed GSE and Reappraisal variables (dependent variables). The plots are presented in Figure 1.
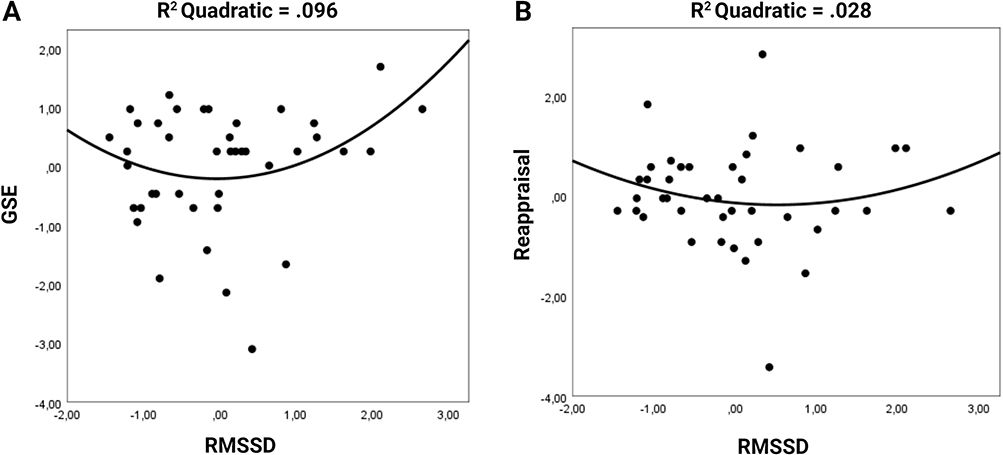 |
Figure 1 Scatter plots for relationships between RMSSD and GSE, and RMSSD and reappraisal with quadratic regression line. (A) GSE and RMSSD. There is a trend in the quadratic regression towards individuals with both lower and higher values of RMSSD to report high GSE. (B) Reappraisal and RMSSD. There is a slight trend in the quadratic regression towards individuals with both lower and higher values of RMSSD to report more use of reappraisal as emotion regulation strategy. Abbreviations: RMSSD, Root mean square of successive N-N differences; GSE, General Self-Efficacy. |
All analyses were conducted using the SPSS software package (version 26).67
Results
Descriptive Statistics
Table 1 provides descriptive statistics for mean HR, vagal tone indices RMSSD and HFms2, pNN50, scores on ERQ subscales, GSE, and DOE.
Gender differences in RMSSD measures were non-significant (t(39) = −0.404, p = 0.688). This must, however, be considered in light of the fact that the sample size for the male group is small (nmale = 12).
Results from Correlation Analysis
Results from the partial correlations controlling for DOE and sex are shown in Table 2. HFms2 and RMSSD were highly correlated (p < 0.001) indicating good quality of indices.62
When controlling for sex and DOE, RMSSD was not significantly correlated with reappraisal (p = 0.751), suppression (p = 0.632), or GSE (p = 0.539). HFms2 was not significantly correlated with reappraisal (p = 0.632), suppression (p = 0.255), or GSE (p = 0.725). Reappraisal was not significantly correlated with suppression (p = 0.205). Reappraisal was significantly correlated with GSE (p = 0.004). Suppression was not significantly correlated with GSE (p = 0.996). Due to RMSSD and HFms2 being highly correlated, only RMSSD was used in subsequent analyses.
Table 3 presents the result from the hierarchical multiple regression analysis control for DOE and sex.
As indicated from the initial correlation analyses, RMSSD (p = 0.404) was not a significant predictor of GSE when controlling for sex and DOE. Reappraisal (p = 0.005) significantly predicted GSE when controlling for sex and DOE.
H: VmHRV moderates the relationship between self-reported ER strategies and general SE beliefs
Due to the non-significant relationship between suppression and GSE, only reappraisal was included in the moderation analysis. The relationship between reappraisal and general SE beliefs was not moderated by vagal tone (reappraisal x RMSSD: B = 0.005, p < 0.279).
Post-Hoc Exploratory Quadratic Regression Analysis
Figure 1 shows the quadratic relationship between RMSSD and GSE, and RMSSD and Reappraisal. As shown in Figure 1, results indicated a bidirectional relationship between RMSSD and GSE and reappraisal, where both higher and lower RMSSD resulted in higher scores on GSE (p > 0.05) and reappraisal (p > 0.05), but this was not statistically significant.
Discussion
The aim of the present study was to investigate ER capacity, indicated by vagal tone, as a potential moderator in the relationship between self-reported ER strategies and general SE in a sample of high school students. ER is an important component in the relationship between SE and developmental outcomes but the neurophysiology underlying this relationship is poorly understood.12 Our hypothesis was that vagal tone as an indicator of ER capacity would moderate the relationship between self-reported ER strategies and general SE beliefs. In our initial analyses, we found that cognitive reappraisal, but not expressive suppression, was significantly and positively associated with SE. The significant association between cognitive reappraisal and general self-efficacy was expected, given that cognitive reappraisal allows an individual to find ways of contextualizing situational outcomes in ways that are conducive for motivation towards desired outcomes.68–70 As opposed to cognitive reappraisal, expressive suppression has traditionally been considered a maladaptive strategy.23,43,44,71 This is arguably a far too static view on ER, and the more recent view is that expressive suppression increases resilience if applied flexibly and appropriately.72–74 For instance, a recent study found that both the flexible suppression and enhancement of emotion expression were positively associated with general self-efficacy beliefs.74 Because expressive suppression is also associated with psychopathology, which is negatively associated with SE, the flexibility to which individuals apply expressive suppression may have been a bidirectional confounder in the relationship between expressive suppression and SE in our results. Nevertheless, expressive suppression was excluded from subsequent analyses.75–78
Vagal tone was not significantly associated with either self-reported SE beliefs nor any of the self-reported ER measures. A growing body of evidence suggests that the relationship between vagal tone and measures of ER depends on whether ER strategies are inferred from measures conducted at rest (eg, using the ERQ as in the present study) or from measuring daily emotional states or responses to emotional stimuli.21,46–48 Follow-up regression analyses confirmed that vagal tone did not predict cognitive reappraisal.
Contrary to our hypothesis, we did not find evidence in support of ER capacity moderating the relationship between ER strategies and general SE beliefs. Several factors could explain these results. As ER strategies and SE beliefs are considered to be modified by experience, while vagal tone is largely determined by genetics, it could be that genetic factors play a lesser role in the development of SE.9,27,29,30 This interpretation, however, is in stark contrast to evidence from genetic research suggesting that adolescent SE is mostly determined by genetics.78 Thus, another and perhaps more plausible interpretation of our results, may be that the relationship between ER capacity and SE beliefs is influenced by the degree to which participants are able to use experience to develop an accurate understanding of their abilities to master various tasks. Another possible moderator of this relationship can be interoception. Previous studies suggest interoception as a central mechanism in neurological and self-reported processing of emotions, emotion regulation, and neural activity and performance in emotional and counter-intuitive decision-making tasks.26,48,79–85 In counter-intuitive decision-making tasks, interoception was found to moderate the relationship between SE and performance.82 Vagal tone has also been found related to emotion regulation during decision-making tasks.83 Thus, future research should test the influence of interoception on the relationship between ER and SE.
Whether self-reported ER strategies correspond to actual ER strategies, and whether a high score on self-reported SE represents overconfidence or an accurate assessment of an individual’s ability to master the environment, will arguably depend on the metacognitive accuracy of the respondent. Metacognitive accuracy is dependent on the dorsolateral prefrontal cortex.32,33 A growing body of evidence suggests that vagal tone is influenced by dorsolateral prefrontal cortex activity.37–42 Vagal tone, in turn, is positively associated with prospective metacognitive accuracy for performance estimations, and negatively associated with overconfidence.21,66 Thus, individuals with low vagal tone may have high SE due to overconfidence resulting from lower dorsolateral prefrontal cortex function, while individuals with high vagal tone may have high SE due to increased dorsolateral prefrontal capacity for 1) metacognitive judgements of their abilities, 2) metacognitive ER, and 3) applying metacognitive learning strategies.2,21,31–33,47,48,66 To explore this possible confounder, and because we did not include a measure of metacognition in our study, we conducted quadratic regression analyses on the relationship between vagal tone and SE, and vagal tone and ER in a follow-up exploratory analysis. The findings (Figure 1) revealed a u-shape indicative of the suspected interference of metacognition. The relationship was more pronounced for SE than for reappraisal, although none of the relationships were significant, which could be due to the modest sample size.
Limitations and Future Directions
The results should be interpreted in light of several limitations. Our sample size is relatively modest; a post hoc power analysis showed that with a sample size of 41 achieved test power was 1-β = 0.77. We needed a sample size of N = 44 to achieve a test power above the normative level of 80%, thus we cannot exclude the possibility of type two error. The sample population consisted of healthy high school students, which means that we already include participants who have experienced some sense of mastery, and that are on track for academic achievement. Furthermore, almost 70% of our sample consisted of females, while research indicates that adolescent males tend to have higher SE than adolescent females.86–88 Although we controlled for the effect of sex in the present study, generalizing our findings to a broader context should be done with caution.
While both RMSSD and HFms2 are accepted indicators of vagal tone, and both indicators are associated with prefrontal cortex activity, research indicates that RMSSD is also influenced by sympathetic activity.37–42,60,89,90 Thus, it can be argued that the choice of index could have slightly impacted results, especially considering our modest sample size.
All limitations considered, future studies should repeat measurements in a larger sample of adolescents, with a more balanced distribution of males and females, preferably with a greater age distribution, and include interoceptive and metacognitive measurements. Future studies should also consider including measurements of daily affect or an emotion regulation task, and both RMSSD and HFms2 in analyses.21,46 Utilizing other methods (eg, electroencephalogram, functional near-infrared spectroscopy, or functional magnetic resonance imaging) for measuring neurophysiological correlates of ER capacity, such as dorsolateral prefrontal cortex activity and connectivity with other prefrontal structures and amygdala during ER tasks, may serve as more objective indicators of ER capacity thus more appropriate predictors of self-efficacy than vagal tone in isolation.31,91
Conclusion
This is the first study to assess whether emotion regulation capacity, indicated by vagal tone, moderates the relationship between emotion regulation and general self-efficacy beliefs in adolescents. Using both psychological and neurophysiological measures is a first step towards filling a neuroscience gap in the research on self-efficacy. While we did find an association between emotion regulation and self-efficacy in the present study, we did not find evidence for neurophysiological emotion regulation capacity moderating the influence of emotion regulation on self-efficacy beliefs. While we controlled for the influence of both sex and exercise in our analyses, we cannot account for the possible role that metacognition or interoception may have had on our results. Thus, the study should be repeated while including those variables in a larger and more representative sample before findings can be generalized.
Acknowledgments
A preprint of this article is available at PsyArXiv.92
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
2. Hayat AA, Shateri K, Amini M, Shokrpour N. Relationships between academic self-efficacy, learning-related emotions, and metacognitive learning strategies with academic performance in medical students: a structural equation model. BMC Med Educ. 2020;20:76. doi:10.1186/s12909-020-01995-9
3. Scholz U, Doña BG, Sud S, Schwarzer R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur J Psychol Assess. 2002;18(3):242–251. doi:10.1027//1015-5759.18.3.242
4. Urdan T, Pajares F. Self-Efficacy Beliefs of Adolescents. IAP; 2006.
5. Schwarzer R. Self-Efficacy: Thought Control of Action. Taylor & Francis; 2014.
6. Efklides A. Metacognition: defining its facets and levels of functioning in relation to self-regulation and co-regulation. Eur Psychol. 2008;13:277–287. doi:10.1027/1016-9040.13.4.277
7. Bassi M, Delle Fave A, Steca P, Caprara GV. Adolescents’ regulatory emotional self-efficacy beliefs and daily affect intensity. Motiv Emot. 2018;42(2):287–298. doi:10.1007/s11031-018-9669-3
8. Caprara GV, Gerbino M, Paciello M, Di Giunta L, Pastorelli C. Counteracting depression and delinquency in late adolescence: the role of regulatory emotional and interpersonal self-efficacy beliefs. Eur Psychol. 2010;15(1):34–48. doi:10.1027/1016-9040/a000004
9. Caprara GV, Alessandri G, Barbaranelli C, Vecchione M. The longitudinal relations between self-esteem and affective self-regulatory efficacy. J Res Pers. 2013;47:859–870. doi:10.1016/j.jrp.2013.08.011
10. Di Giunta L, Lunetti C, Gliozzo G, et al. Negative parenting, adolescents’ emotion regulation, self-efficacy in emotion regulation, and psychological adjustment. Int J Environ Res Public Health. 2022;19(4):2251. doi:10.3390/ijerph19042251
11. Tamir M, John OP, Srivastava S, Gross JJ. Implicit theories of emotion: affective and social outcomes across a major life transition. J Pers Soc Psychol. 2007;92:731–744.
12. Caprara M, Gerbino M, Mebane ME, Ramirez-Uclés IM. Self-efficacy beliefs in managing positive emotions: associations with positive affect, negative affect, and life satisfaction across gender and ages. Front Hum Neurosci. 2022;16:927648. doi:10.3389/fnhum.2022.927648
13. Nakagawa S, Takeuchi H, Taki Y, et al. Lenticular nucleus correlates of general self-efficacy in young adults. Brain Struct Funct. 2017;222(7):3309–3318. doi:10.1007/s00429-017-1406-2
14. Sugiura A, Aoki R, Murayama K, et al. Regional gray matter volume in the posterior precuneus is associated with general self-efficacy. Neuroreport. 2016;27(18):1350–1353. doi:10.1097/WNR.0000000000000702
15. Bandura A. Self-efficacy mechanism in human agency. Am Psychologist. 1982;37(2):122.
16. Bandura A, Reese L, Adams NE. Microanalysis of action and fear arousal as a function of differential levels of perceived self-efficacy. J Pers Soc Psychol. 1982;43(1):5.
17. Wiedenfeld SA, O’Leary A, Bandura A, Brown S, Levine S, Raska K. Impact of perceived self-efficacy in coping with stressors on components of the immune system. J Pers Soc Psychol. 1990;59(5):1082.
18. Zlomuzica A, Preusser F, Schneider S, Margraf J. Increased perceived self-efficacy facilitates the extinction of fear in healthy participants. Front Behav Neurosci. 2015;9:270. doi:10.3389/fnbeh.2015.00270
19. Caprara GV, Di Giunta L, Eisenberg N, Gerbino M, Pastorelli C, Tramontano C. Assessing regulatory emotional self-efficacy in three countries. Psychol Assess. 2008;20:227–237. doi:10.1037/1040-3590.20.3.227
20. Bandura A. Guide for constructing self-efficacy scales. Self Efficacy Beliefs Adolesc. 2006;5(1):307–337.
21. Ask TF, Knox BJ, Lugo R, Helgetun I, Sütterlin S. Neurophysiological and emotional influences on team communication and metacognitive cyber situational awareness during a cyber engineering exercise. Front Hum Neurosci. 2023;16:1092056. doi:10.3389/fnhum.2022.1092056
22. Friedman NP, Robbins TW. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology. 2022;47(1):72–89. doi:10.1038/s41386-021-01132-0
23. Gross JJ. The emerging field of emotion regulation: an integrative review. Rev General Psychol. 1998;2(3):271.
24. Appelhans BM, Luecken LJ. Heart rate variability as an index of regulated emotional responding. Rev General Psychol. 2006;10(3):229–240. doi:10.1037/1089-2680.10.3.229
25. Thayer JF, Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. 2000;61(3):201–216.
26. De Witte NA, Sütterlin S, Braet C, Mueller SC. Getting to the heart of emotion regulation in youth: the role of interoceptive sensitivity, heart rate variability, and parental psychopathology. PLoS One. 2016;11(10):e0164615. doi:10.1371/journal.pone.0164615
27. McRae K, Rhee SH, Gatt JM, Godinez D, Williams LM, Gross JJ. Genetic and environmental influences on emotion regulation: a twin study of cognitive reappraisal and expressive suppression. Emotion. 2017;17(5):772–777. doi:10.1037/emo0000300
28. Friedman NP, Miyake A, Young SE, DeFries JC, Corley RP, Hewitt JK. Individual differences in executive functions are almost entirely genetic in origin. J Exp Psychol Gen. 2008;137(2):201–225. doi:10.1037/0096-3445.137.2.201
29. Golosheykin S, Grant JD, Novak OV, Heath AC, Anokhin AP. Genetic influences on heart rate variability. Int j Psychophysiol. 2017;115:65–73. doi:10.1016/j.ijpsycho.2016.04.008
30. Wang X, Ding X, Su S, et al. Genetic influences on heart rate variability at rest and during stress. Psychophysiology. 2009;46(3):458–465. doi:10.1111/j.1469-8986.2009.00793.x
31. Golkar A, Lonsdorf TB, Olsson A, et al. Distinct contributions of the dorsolateral prefrontal and orbitofrontal cortex during emotion regulation. PLoS One. 2012;7(11):e48107. doi:10.1371/journal.pone.0048107
32. Fleur DS, Bredeweg B, van den Bos W. Metacognition: ideas and insights from neuro-and educational sciences. NPJ Sci Learn. 2021;6:13. doi:10.1038/s41539-021-00089-5
33. Jiang K, Wu S, Shi Z, et al. Activations of the dorsolateral prefrontal cortex and thalamus during agentic self-evaluation are negatively associated with trait self-esteem. Brain Res. 2018;1692:134–141. doi:10.1016/j.brainres.2018.05.017
34. Menon V, D’Esposito M. The role of PFC networks in cognitive control and executive function. Neuropsychopharmacology. 2022;47:90–103. doi:10.1038/s41386-021-01152-w
35. Nee DE. Integrative frontal-parietal dynamics supporting cognitive control. eLife. 2021;10:e57244. doi:10.7554/eLife.57244
36. Thayer JF, Åhs F, Fredrikson M, Sollers Iii JJ, Wager TD. A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neurosci Biobehav Rev. 2012;36(2):747–756.
37. Brunoni AR, Vanderhasselt MA, Boggio PS. Polarity- and valence-dependent effects of prefrontal transcranial direct current stimulation on heart rate variability and salivary cortisol. Psychoneuroendocrinology. 2013;38(1):58–66. doi:10.1016/j.psyneuen.2012.04.020
38. Carnevali L, Pattini E, Sgoifo A, Ottaviani C. Effects of prefrontal transcranial direct current stimulation on autonomic and neuroendocrine responses to psychosocial stress in healthy humans. Stress. 2020;23(1):26–36. doi:10.1080/10253890.2019.1625884
39. Chand T, Li M, Jamalabadi H, et al. Heart rate variability as an index of differential brain dynamics at rest and after acute stress induction. Front Neurosci. 2020;14:645. doi:10.3389/fnins.2020.00645
40. Era V, Carnevali L, Thayer JF, Candidi M, Ottaviani C. Dissociating cognitive, behavioral and physiological stress-related responses through dorsolateral prefrontal cortex inhibition. Psychoneuroendocrinology. 2020;124:105070. doi:10.1016/j.psyneuen.2020.105070
41. Gu Z, Chen W, Lu Q, et al. Anodal high-definition transcranial direct current stimulation reduces heart rate and modulates heart-rate variability in healthy young people: a randomized cross-controlled trial. Front Cardiovascular Med. 2022;9:1070157. doi:10.3389/fcvm.2022.1070157
42. Nikolin S, Boonstra TW, Loo CK, Martin D. Combined effect of prefrontal transcranial direct current stimulation and a working memory task on heart rate variability. PLoS One. 2017;12(8):e0181833. doi:10.1371/journal.pone.0181833
43. Butler EA, Egloff B, Wlhelm FH, Smith NC, Erickson EA, Gross JJ. The social consequences of expressive suppression. Emotion. 2003;3(1):48.
44. Ochsner KN, Ray RD, Cooper JC, et al. For better or for worse: neural systems supporting the cognitive down-and up-regulation of negative emotion. Neuroimage. 2004;23(2):483–499.
45. Geisler FCM, Vennewald N, Kubiak T, Weber H. The impact of heart rate variability on subjective well-being is mediated by emotion regulation. Pers Individ Dif. 2010;49(7):723–728.
46. Koval P, Ogrinz B, Kuppens P, Van den Bergh O, Tuerlinckx F, Sütterlin S. Affective instability in daily life is predicted by resting heart rate variability. PLoS One. 2013;8(11):e81536. doi:10.1371/journal.pone.0081536
47. Volokhov RN, Demaree HA. Spontaneous emotion regulation to positive and negative stimuli. Brain Cogn. 2010;73(1):1–6. doi:10.1016/j.bandc.2009.10.015
48. Pinna T, Edwards DJ. A systematic review of associations between interoception, vagal tone, and emotional regulation: potential applications for mental health, wellbeing, psychological flexibility, and chronic conditions. Front Psychol. 2020;11:1792. doi:10.3389/fpsyg.2020.01792
49. McLaughlin KA, Rith-Najarian L, Dirks MA, Sheridan MA. Low vagal tone magnifies the association between psychosocial stress exposure and internalizing psychopathology in adolescents. J Clin Child Adolesc Psychol. 2015;44(2):314–328. doi:10.1080/15374416.2013.843464
50. Hildebrandt LK, McCall C, Engen HG, Singer T. Cognitive flexibility, heart rate variability, and resilience predict fine-grained regulation of arousal during prolonged threat. Psychophysiology. 2016;53(6):880–890. doi:10.1111/psyp.12632
51. Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: construction and validation. Psychol Rep. 1982;51(2):663–671.
52. Skinner EA, Chapman M, Baltes PB. Control, means-ends, and agency beliefs: a new conceptualization and its measurement during childhood. J Pers Soc Psychol. 1988;54(1):117.
53. Luszczynska A, Gutiérrez‐Doña B, Schwarzer R. General self‐efficacy in various domains of human functioning: evidence from five countries. Int j Psychol. 2005;40(2):80–89.
54. Lazić M, Jovanović V, Gavrilov-Jerković V. The general self-efficacy scale: new evidence of structural validity, measurement invariance, and predictive properties in relationship to subjective well-being in Serbian samples. Curr Psychol. 2021;40:699–710. doi:10.1007/s12144-018-9992-6
55. Gouveia VV, de Moura HM, de Oliveira ICV, Ribeiro MGC, Rezende AT, Brito TRS. Emotional regulation questionnaire (ERQ): evidence of construct validity and internal consistency. Psico-USF. 2018;23(3):461–471. doi:10.1590/1413-82712018230306
56. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348.
57. Vuorela M, Nummenmaa L. Experienced emotions, emotion regulation and student activity in a web-based learning environment. Eur J Psychol Educ. 2004;19(4):423–436.
58. Schuman DL, Lawrence KA, Boggero I, et al. A pilot study of a three-session heart rate variability biofeedback intervention for veterans with posttraumatic stress disorder. Appl Psychophysiol Biofeedback. 2023;48:51–65. doi:10.1007/s10484-022-09565-z
59. Sætren SS, Sütterlin S, Lugo RG, Prince-Embury S, Makransky G. A multilevel investigation of resiliency scales for children and adolescents: the relationships between self-perceived emotion regulation, vagally mediated heart rate variability, and personal factors associated with resilience. Front Psychol. 2019;438. doi:10.3389/fpsyg.2019.00438
60. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation. 1996;93(5):1043–1065.
61. Kaufmann T, Sütterlin S, Schulz SM, Vögele C. ARTiiFACT: a tool for heart rate artifact processing and heart rate variability analysis. Behav Res Methods. 2011;43(4):1161–1170.
62. Goedhart AD, Van Der Sluis S, Houtveen JH, Willemsen G, De Geus EJC. Comparison of time and frequency domain measures of RSA in ambulatory recordings. Psychophysiology. 2007;44(2):203–215. doi:10.1111/j.1469-8986.2006.00490.x
63. Sharma VK, Subramanian SK, Arunachalam V, Rajendran R. Heart rate variability in adolescents–normative data stratified by sex and physical activity. J Clin Diagnostic Res. 2015;9(10):CC08.
64. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: a Regression-Based Approach. Guilford Publications; 2017.
65. Sütterlin S, Lugo RG, Ask TF, et al. The role of IT background for metacognitive accuracy, confidence and overestimation of deep fake recognition skills. Lecture Notes Comput Sci. 2022:13310. doi:10.1007/978-3-031-05457-0_9
66. Meessen J, Sütterlin S, Gauggel S, Forkmann T. Learning by heart-the relationship between resting vagal tone and metacognitive judgments: a pilot study. Cogn Process. 2018;19(4):557–561. doi:10.1007/s10339-018-0865-6
67. IBM Corp. IBM SPSS Statistics for Windows, Version 24.0 [Computer Software]. Amonk, NY: IBM Corp; 2016.
68. Kelley NJ, Glazer JE, Pornpattananangkul N, Nusslock R. Reappraisal and suppression emotion-regulation tendencies differentially predict reward-responsivity and psychological well-being. Biol Psychol. 2019;140:35–47. doi:10.1016/j.biopsycho.2018.11.005
69. Staudinger MR, Erk S, Abler B, Walter H. Cognitive reappraisal modulates expected value and prediction error encoding in the ventral striatum. NeuroImage. 2009;47(2):713–721. doi:10.1016/j.neuroimage.2009.04.095
70. Staudinger MR, Erk S, Walter H. Dorsolateral prefrontal cortex modulates striatal reward encoding during reappraisal of reward anticipation. Cerebral Cortex. 2011;21(11):2578–2588. doi:10.1093/cercor/bhr041
71. Gross JJ. Emotion regulation in adulthood: timing is everything. Curr Dir Psychol Sci. 2001;10(6):214–219.
72. Burton CL, Bonanno GA. Measuring ability to enhance and suppress emotional expression: the Flexible Regulation of Emotional Expression (FREE) Scale. Psychol Assess. 2016;28(8):929–941. doi:10.1037/pas0000231
73. Chen SQ, Chen T, Bonanno GA. Expressive flexibility: enhancement and suppression abilities differentially predict life satisfaction and psychopathology symptoms. Pers Individ Dif. 2018;126:78–84. doi:10.1016/j.paid.2018.01.010
74. Gonzalez-Escamilla G, Dörfel D, Becke M, Trefz J, Bonanno GA, Groppa S. Associating flexible regulation of emotional expression with psychopathological symptoms. Front Behav Neurosci. 2022;16:924305. doi:10.3389/fnbeh.2022.924305
75. Moore SA, Zoellner LA, Mollenholt N. Are expressive suppression and cognitive reappraisal associated with stress-related symptoms? Behav Res Ther. 2008;46(9):993–1000. doi:10.1016/j.brat.2008.05.001
76. Schönfeld P, Brailovskaia J, Zhang XC, Margraf J. Self-efficacy as a mechanism linking daily stress to mental health in students: a three-wave cross-lagged study. Psychol Rep. 2019;122(6):2074–2095. doi:10.1177/0033294118787496
77. Tak YR, Brunwasser SM, Lichtwarck-Aschoff A, Engels RC. The prospective associations between self-efficacy and depressive symptoms from early to middle adolescence: a cross-lagged model. J Youth Adolesc. 2017;46(4):744–756. doi:10.1007/s10964-016-0614-z
78. Waaktaar T, Torgersen S. Self-efficacy is mainly genetic, not learned: a multiple-rater twin study on the causal structure of general self-efficacy in young people. Twin Res Hum Genet. 2013;16(3):651–660. doi:10.1017/thg.2013.25
79. Terasawa Y, Fukushima H, Umeda S. How does interoceptive awareness interact with the subjective experience of emotion? An fMRI study. Hum Brain Mapp. 2013;34(3):598–612. doi:10.1002/hbm.21458
80. Lugo RG, Helkala K, Knox BJ, Jøsok Ø, Lande NM, Sütterlin S. Interoceptive sensitivity as a proxy for emotional intensity and its relationship with perseverative cognition. Psychol Res Behav Manag. 2017;11:1–8. doi:10.2147/PRBM.S139790
81. Wiens S. Interoception in emotional experience. Curr Opin Neurol. 2005;18(4):442–447. doi:10.1097/01.wco.0000168079.92106.99
82. Lugo RG, Sütterlin S, Knox BJ, Jøsok Ø, Helkala K, Lande NM. The moderating influence of self-efficacy on interoceptive ability and counterintuitive decision making in officer cadets. J Mil Stud. 2016;7(1):44–52. doi:10.1515/jms-2016-0005
83. Sütterlin S, Schulz SM, Stumpf T, Pauli P, Vögele C. Enhanced cardiac perception is associated with increased susceptibility to framing effects. Cogn Sci. 2013;37(5):922–935. doi:10.1111/cogs.12036
84. Werner NS, Schweitzer N, Meindl T, Duschek S, Kambeitz J, Schandry R. Interoceptive awareness moderates neural activity during decision-making. Biol Psychol. 2013;94(3):498–506. doi:10.1016/j.biopsycho.2013.09.002
85. Wölk J, Sütterlin S, Koch S, Vögele C, Schulz SM. Enhanced cardiac perception predicts impaired performance in the Iowa Gambling Task in patients with panic disorder. Brain Behav. 2014;4(2):238–246. doi:10.1002/brb3.206
86. Céspedes C, Rubio A, Viñas F, Cerrato SM, Lara-órdenes E, Ríos J. Relationship between self-concept, self-efficacy, and subjective well-being of native and migrant adolescents. Front Psychol. 2021;11:620782. doi:10.3389/fpsyg.2020.620782
87. Spence JC, Blanchard CM, Clark M, Plotnikoff RC, Storey KE, McCargar L. The role of self-efficacy in explaining gender differences in physical activity among adolescents: a multilevel analysis. J Phys Act Health. 2010;7(2):176–183. doi:10.1123/jpah.7.2.176
88. Trost SG, Pate RR, Dowda M, Saunders R, Ward DS, Felton G. Gender differences in physical activity and determinants of physical activity in rural fifth grade children. J Sch Health. 1996;66(4):145–150. doi:10.1111/j.1746-1561.1996.tb08235.x
89. Berntson GG, Lozano DL, Chen YJ. Filter properties of root mean square successive difference (RMSSD) for heart rate. Psychophysiology. 2005;42:246–252. doi:10.1111/j.1469-8986.2005.00277.x
90. Williams DP, Koenig J, Carnevali L, et al. Heart rate variability and inflammation: a meta-analysis of human studies. Brain Behav Immun. 2019;80:219–226. doi:10.1016/j.bbi.2019.03.009
91. Berboth S, Morawetz C. Amygdala-prefrontal connectivity during emotion regulation: a meta-analysis of psychophysiological interactions. Neuropsycholog. 2021;153:107767. doi:10.1016/j.neuropsychologia.2021.107767
92. Lande NM, Ask TF, Sætren SS, Lugo RG, Sütterlin S. The role of emotion regulation for general self-efficacy in adolescents assessed through both neurophysiological and self-reported measures. PsyArXiv. 2023. doi:10.31234/osf.io/abxfn
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.