")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
The Role of a Novel Generation of Emollients, ‘Emollients Plus’, in Atopic Dermatitis
Authors Araviiskaia E , Pincelli C , Sparavigna A , Luger T
Received 11 October 2022
Accepted for publication 26 November 2022
Published 14 December 2022 Volume 2022:15 Pages 2705—2719
DOI https://doi.org/10.2147/CCID.S389697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Elena Araviiskaia,1 Carlo Pincelli,2 Adele Sparavigna,3 Thomas Luger4
1Department of Dermatology and Venereal Diseases, First Pavlov State Medical University of St Petersburg, St Petersburg, Russia; 2DermoLab, Department of Surgical, Medical, Dental and Morphological Sciences, University of Modena and Reggio Emilia, Modena, Italy; 3Derming Clinical Research and Bioengineering Institute, Milan, Italy; 4Department of Dermatology, University of Munster, Munster, Germany
Correspondence: Thomas Luger, Dermatology Clinic, University of Münster, Von-Esmarch-Straẞe 58, Münster, 48149, Germany, Email [email protected]
Abstract: Emollients are the mainstay maintenance treatment for atopic dermatitis (AD). A novel generation of emollients, ‘emollients plus’, containing active, non-medicated substances, has softened the distinction between emollients and topical drugs. A literature search for selected key words was performed using PubMed. Additional papers were identified based on author expertise. Whilst the inclusion of five components of an ideal emollient has been proposed, no such consensus exists for emollients plus and they can vary markedly in their composition and modes of action for AD treatment. This could have a profound effect on their clinical efficacy. The efficacy of emollients plus in restoring and maintaining skin barrier function has been demonstrated on multiple levels, with evidence reported for their effects on the physical and biochemical, microbial, immunological, and neurosensory barriers. When selecting an appropriate AD treatment approach, the safety profiles of the available topical therapies must be carefully considered. There are several proposed treatment approaches for AD, including preventive, proactive, intermittent, and synergistic approaches. Emollients plus may be effective not only as maintenance therapy for AD, but also when used synergistically with anti-inflammatory pharmacological therapies.
Keywords: atopic dermatitis, atopic march, emollient, emollient plus, maintenance therapy, skin barrier
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by dry skin, intense itching, and inflammatory skin lesions, and can be highly heterogeneous in presentation.1–3 AD can present with frequent spontaneous flares and remissions.1,4,5 It is one of the most common non-communicable skin diseases, affecting up to 20% of children and 2–8% of adults.6
The skin is made up of multiple layers, and forms a physical, biochemical, microbial, immunological, and neurosensory barrier between the internal and external environments.7 The epidermis, comprising the stratum corneum, stratum granulosum, stratum spinosum, and the stratum basale, is the main component of the skin’s protective barrier.7 In AD, epidermal morphology and stratum corneum lipid composition are altered, and skin barrier function is impaired, with increased transepidermal water loss (TEWL) and increased percutaneous penetration. AD is also associated with T helper (Th)2-predominant inflammation.8–10
Emollients are the mainstay for AD management: maintenance of stable disease can be achieved with emollients after induction of remission with anti-inflammatory treatment.6 Emollients are topical formulations with vehicle-type substances lacking active ingredients,6 and act by providing a barrier for skin affected by AD, retaining moisture and protecting it from irritants.11 Emollients usually contain petrolatum, paraffin, glycerine, and plant-derived butter and oils.11 They can be classified as first, second, or third generation based on their composition and mode of action. First-generation emollients, such as petrolatum, paraffin oil, and fatty alcohols, are hygroscopic and occlusive; second-generation emollients, such as glycerol, sorbitol, and natural moisturizing factor substitutes, restore hydration and barrier function; third-generation emollients, such as physiological lipids, repair the skin barrier.12
The development of a novel generation of emollients containing active non-pharmacological ingredients, ‘emollients plus’, has softened the distinction between emollients and topical drugs.6 Dermoflan AD emollient plus cream (Meda Pharma, Solna, Sweden; herein referred to as EC) is an example of an emollient plus specifically formulated for skin affected by AD. It contains several active ingredients to target multiple mechanisms in AD pathophysiology: licorice extract (glycyrrhizinic acid) has anti-inflammatory properties;13 niacinamide, sterols, glycosphingolipid, and Linum seed oil act to restore barrier function;14–16 xylitol and galacto-oligosaccharide have selective antibacterial and prebiotic activity to maintain the skin microbiome;17–19 and laureth-9-polydocanol reduces itching.20
Given their integral role in AD management and the increase in commercially available products, this review aims to provide an overview of the composition and efficacy of emollients plus, with a particular focus on EC. We also provide an overview of the necessary safety considerations when selecting a treatment approach in AD.
Methods
A virtual focus meeting, attended by the authors, on dermocosmetics in AD was held in October 2021. The discussions resulting from that meeting formed the basis of this review. After agreeing the scope of this review, computerized searches were undertaken in PubMed, using the search term atopic dermatitis in combination with: Dermoflan AD, emollient, emollient plus, moisturizer, skin barrier, atopic march, flare, time to flare. Additional papers were identified based on author expertise. Only papers deemed directly relevant were included in this review.
Results
Emollients Plus
An emollient plus is a topical formulation with vehicle-type substances and active, non-medicated substances, such as saponins, flavonoids, and riboflavins from protein-free oat plantlet extracts, and bacterial lysates.6 Emollients plus can improve AD lesions through several synergistic modes of action, including preserving barrier lipid content,21 preventing TEWL, and moisturizing the skin,14,21 reducing inflammation,20,22 and reducing itch.20
Thirteen emollients plus of interest were identified. Below, their compositions and clinical efficacy have been compared.
The Composition of Emollients Plus
It has previously been suggested that the ideal emollient contains five key components: humectants, non-physiological lipids (eg, mineral or vegetable oil), physiological lipids (eg, ceramides, free fatty acids), anti-pruritics/soothing agents, and agents that support epidermal differentiation.23 This has recently been reviewed: the authors concluded that the concept of five components in an emollient for dry skin remains valid24 and highlighted the benefits of dexpanthenol to compensate for reduced hydration and enhance epidermal differentiation. They also recommended further exploration of substances targeting enzymes responsible for the synthesis or elongation of lipids. The need to develop different formulations for use in various environments (eg, by season/climate and skin site affected) was also emphasised.
Whilst the inclusion of five components has been proposed for emollients, no such consensus exists for emollients plus, which vary markedly in their composition and modes of action (Table 1).11,13,14,16–20,24–53 Given this heterogeneity, variability in the effects of emollients plus on AD is unsurprising.
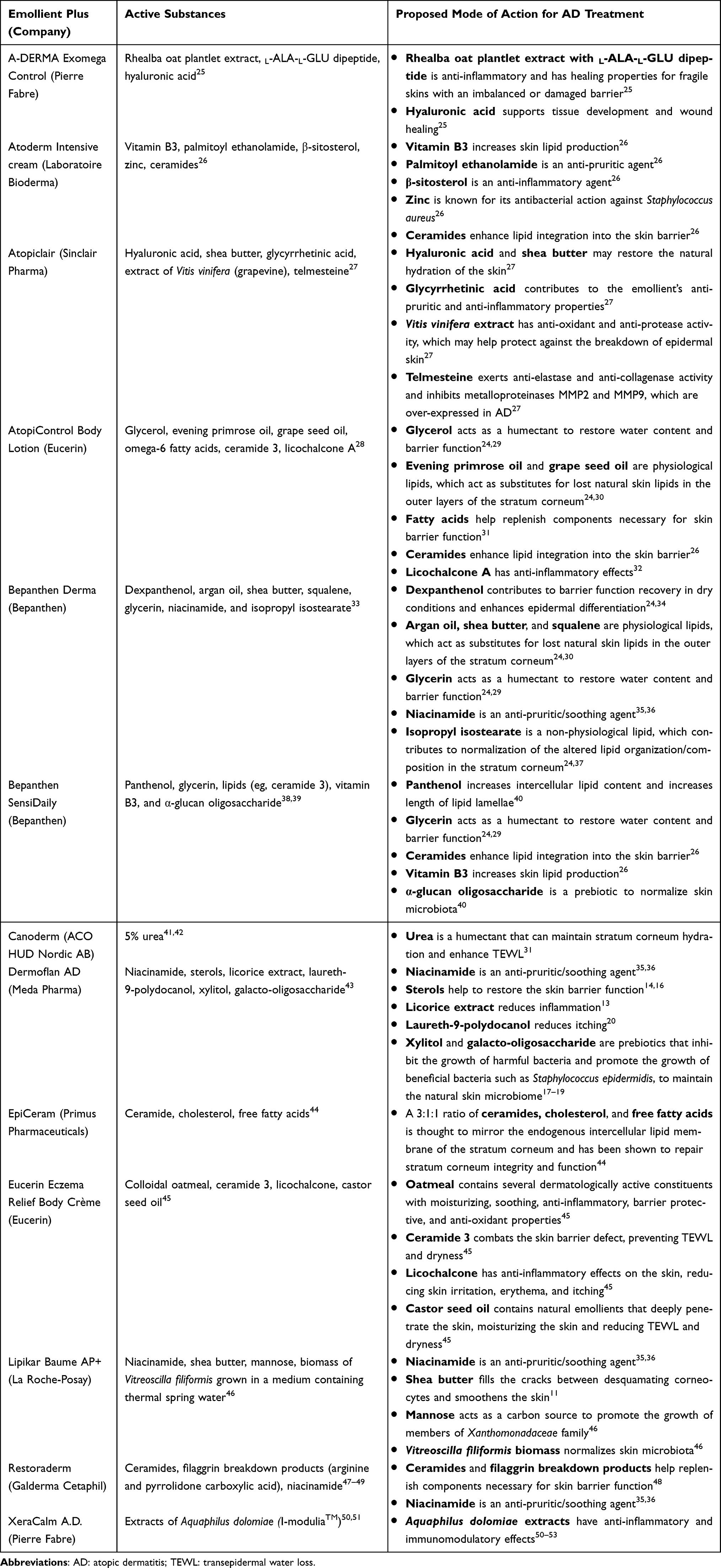 |
Table 1 Active Substances and Proposed Mode of Action of Commercially Available Emollients Plus |
Clinical Efficacy of Emollients Plus
Ten studies on nine emollients plus were identified, reporting data on average time to flare and/or flare-free period (Table 2).26,28,38,41,42,46,49,54–56
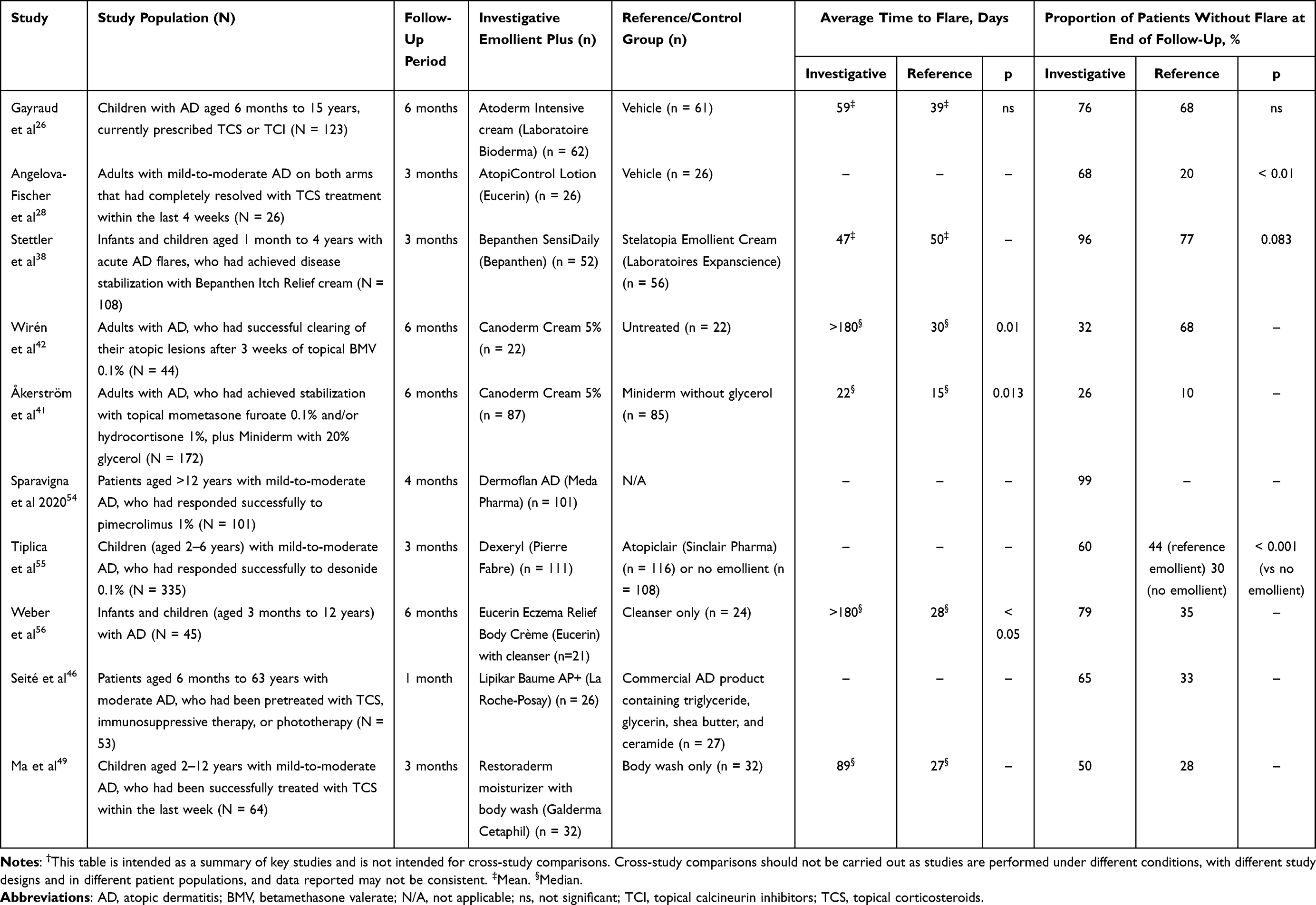 |
Table 2 Summary of Studies Reporting Time to Flare and Proportion of Flare-Free Patients for Commercially Available Emollients Plus† |
The longest average time to flare was reported with Eucerin Eczema Relief Body Crème plus cleanser (Eucerin, Hamburg, Germany) and Canoderm cream 5% (ACO HUD Nordic AB, Upplands Väsby, Sweden), with an average time to flare of >180 days for both (mean was reported for Eucerin Eczema Relief Body Crème; median was reported for Canoderm cream 5%).41,42,56 However, in a separate study, the median time to flare for Canoderm cream 5% was just 22 days.41
The highest percentage of patients without flare at the end of follow-up was with EC: 99% of patients were flare-free after 4 months of follow-up.54 A similarly high flare-free rate was with Bepanthen SensiDaily (Bepanthen, Bayer, Green Park, UK) at 96%, although with a shorter follow-up period (3 months). In comparison, use of the reference emollient in the same study (Stelatopia Emollient Cream [Laboratoires Expanscience, Courbevoie, France]) resulted in a flare-free rate of 77%, although this difference was not statistically significant (p = 0.083).38 Treatment with Eucerin Eczema Relief Body Crème plus cleanser and Atoderm Intensive cream (Laboratoire Bioderma, Aix en Provence, France) resulted in flare-free incidences of 79% and 76%, respectively, which, although lower than that of EC and Bepanthen SensiDaily, were reported after longer, 6-month follow-ups.26,56
In the studies identified, there was notable variability in the designs, populations, and types of data reported; thus, direct cross-study comparisons are not recommended. Standardization of reporting in emollient plus research may allow stronger conclusions to be drawn regarding efficacy. It should also be noted that this narrative review did not employ systematic review methodology; the publications listed may not represent an exhaustive list of available studies.
Skin Barrier Function in AD Pathogenesis
The clinical efficacy of an emollient plus, as summarized above, may be determined by its ability to restore and maintain skin barrier function. The inflammatory, biochemical, microbial, and neurosensory changes seen in AD pathogenesis are described below.7
The inflammatory cascade in AD has been extensively reviewed.57,58 In brief, antigen penetration through damaged skin and presentation by antigen-presenting cells leads to a Th2 response, resulting in immunoglobulin E production. This can lead to degranulation of mast cells, a local inflammatory response, and recruitment of other inflammatory cells, such as eosinophils. Langerhans cells and inflammatory dendritic cells, activated by pathogen-derived antigens, promote Th1- and Th2-driven immune responses in acute AD lesions. However, as the understanding of the genetic contribution to AD has improved, the pathophysiology of AD is now recognized as being driven by an impaired skin barrier, rather than a purely immunological disorder.1,59
There is also evidence to suggest that skin pH regulation may be overlooked in AD disease pathogenesis. AD lesions have higher pH values than healthy skin,60 and a positive correlation was observed between severity of itch in children with AD and higher skin pH.61 This is supported by a phenome-wide association study that demonstrated a statistically significant association between AD and a single-nucleotide polymorphism (SNP) in G protein-coupled receptor (GPR) 65.62 GPR65 is an extracellular pH-sensing receptor widely expressed on immune cells.63 Normal signaling through GPR65 at low pH inhibits inflammatory cytokine release from immune cells;64,65 the SNP in AD reduces GPR65 signaling.62 Furthermore, GPR65 deficiency in a murine AD model resulted in exacerbated disease,62 demonstrating a mechanism by which the AD inflammatory cascade may be linked to skin pH.
The skin microbiome and presence of pathogens such as Staphylococcus aureus have also been implicated in AD pathogenesis.66 In healthy skin, the microbiome protects against colonization by pathogenic microbes via secretion of anti-microbial peptides and free fatty acids.66 However, in AD, the microbial community structure at sites of disease predilection is different compared with healthy controls. A correlation exists between decreased microbial diversity and increased severity of AD.67
Maintaining skin barrier integrity is central to AD management, and the capacity for treatment to restore and/or maintain skin barrier function as discussed above may be beneficial.
The Efficacy of Emollients Plus on Maintaining and Restoring the Skin Barrier
Below, we highlight recent evidence from pre-clinical and clinical studies for the capacity of emollients plus to restore barrier function at the physical and biochemical, microbial, immunological, and neurosensory levels of the skin barrier.
The Physical and Biochemical Barriers
The physical skin barrier consists of corneocytes, desmosomes, claudins and lipids, while the biochemical barrier is composed of molecules that contribute to hydration (eg, natural moisturizing factors) and prevention of infections (eg, anti-microbial peptides).7
In a recent in vitro study by Quadri et al, skin organ cultures were subject to tape stripping (100 repeated applications and subsequent removals of adhesive tapes to the skin surface) as a model for skin barrier damage. After incubation with either 100% or 50% EC solution or diluent alone, skin barrier recovery was assessed.43 Tape stripping resulted in complete removal of the epidermal stratum corneum and intercellular lipid component. Following culture with EC, epidermal thickness was significantly increased in organ cultures treated with 100% EC solution compared with those treated with diluent alone (p < 0.01).43 The application of 50% or 100% EC significantly increased lipid detection after only 24 hours compared with diluent, and after 120 hours restored lipid content to 99% and 93%, respectively, of that in unstripped tissue.43
Additionally, skin barrier restoration after tape stripping was assessed through expression of involucrin and caspase-14 (differentiation markers), claudin-1 (a tight junction protein normally homogenously expressed in the stratum granulosum), and keratin-16 (an intermediate filament cytoskeletal protein expressed in keratinocytes in response to epidermal barrier challenges).43 Compared with diluent, claudin-1 expression was significantly increased with both 50% and 100% EC solution (p < 0.05 and p < 0.01, respectively), involucrin expression was significantly increased with 100% EC only (p < 0.05), and caspase-14 expression was significantly increased with both 50% and 100% EC (p < 0.01 for both). Keratin-16 expression was significantly reduced with 100% EC only (p < 0.05) compared with diluent.43
A clinical study was performed to validate these findings. Patients with mild-to-moderate AD in clinical remission (N = 20) applied EC (n = 10) or placebo (n = 10) once a day for 2 consecutive months in the antecubital folds of the upper and lower limbs. Once-daily EC application reduced vascularization and epidermal thickness, and increased skin hydration in patients with mild-to-moderate AD in clinical remission, thus validating the in vitro findings, albeit with a small sample of patients.43
In a 2019 clinical study, 60 patients with mild AD applied EC or vehicle twice daily on their forearms for 28 days.68 Skin hydration, as measured by corneometry, was significantly improved by 19% after 28 days in patients treated with EC versus baseline (p < 0.05). Skin desquamation was also significantly decreased in patients treated with EC at the 14-day and 28-day timepoints, compared with baseline (p < 0.05). Skin barrier function, measured by TEWL, was significantly improved by 17% after 28 days in patients treated with EC versus baseline (p < 0.05). There was also a significant difference in skin hydration between the EC-treated and vehicle-treated groups at each timepoint (p < 0.05).
The capacity for EC to increase skin moisture levels and decrease TEWL was also shown in a small clinical study by Gasparri et al. In adults with AD (N = 10), skin moisture levels in treated areas were significantly higher at day 21 compared with baseline: mean skin moisture increased from baseline by 115.5% (corneometric units: 27.7 vs 13.1, respectively; p < 0.001), and TEWL was significantly reduced.69
The Microbial Barrier
Microbes contribute to the skin barrier by producing anti-microbial peptides and free fatty acids, and stimulating the innate immune system.7 Staphylococcus aureus colonization is a critical driver of AD inflammation.70 A study by Kong et al demonstrated that microbial diversity during AD flares depends on recent AD treatments, with even intermittent treatment (use of topical calcineurin inhibitors [TCI]/topical corticosteroids [TCS]/antibiotics in the past 7 days and/or consumption of oral antibiotics within 4 weeks before sampling) linked to reduction in Staphylococcus aureus and greater bacterial diversity compared with no recent treatment.67
Supporting these findings, Staphylococcus aureus growth and biofilm formation were assessed in vitro. EC rapidly (<3 hours) inhibited the growth and biofilm formation of two strains of Staphylococcus aureus.15 In clinical validation, patients predisposed to AD (N = 11) applied EC twice daily between the neck and shoulders. Microbial diversity significantly increased in EC-treated areas at day 28 versus baseline (p = 0.037).15
The microbiome maintenance action of EC is thought to be driven by the active ingredients galacto-oligosaccharides and xylitol. Galacto-oligosaccharides are a group of prebiotics.17 Prebiotics may promote the growth of beneficial commensal bacteria (eg, Staphylococcus epidermidis), thus preventing colonization by pathogenic bacteria (eg, Staphylococcus aureus).19,71 Xylitol has been shown to inhibit the formation of glycocalyx, a component of Staphylococcus aureus-associated biofilm.18
There is evidence for the capacity of another emollient plus, Lipikar Baume AP+ (La Roche-Posay, London, UK), in normalization of the skin microbiome.72 In a single-center study in patients with moderate AD (N = 49), patients applied Lipikar Baume AP+ twice daily to their entire body. Twice-daily application of Lipikar Baume AP+ improved symptoms in over 70% of patients and was associated with increased bacterial diversity and decreased Staphylococcus species. The abundance of Staphylococcus species was inversely related to microbial diversity.46,73
The Immunological Barrier
The immunological barrier involves components of the innate immune system (eg, anti-microbial peptides produced by keratinocytes) and the adaptive immune system (eg, dendritic cells and lymphocytes).7 Toll-like receptors (TLRs) are thought to play a role in AD susceptibility, and increased susceptibility to microbial infections in patients with AD may be attributed to TLR functional abnormalities.74 EC treatment is associated with increased expression of TLR-1 and TLR-2,43 indicating that EC may support the epidermal defense against pathogens.
Another emollient plus compound, I-modulia (Pierre Fabre, Paris, France), an Aquaphilus dolomiae extract, has demonstrated anti-inflammatory and immunomodulatory effects. In vitro, I-modulia regulated keratinocyte inflammatory and lymphocyte immune responses, including thymic stromal lymphopoietin, interleukin (IL)-18, IL-4R, IL-8, monocyte chemoattractant protein-3, macrophage inflammatory protein-3a, and macrophage-derived chemokine.51,52 I-modulia has been suggested to activate TLR-2, TLR-4, and TLR-5, and subsequently induce anti-microbial peptides via TLR-5.53 I-modulia also displayed inhibition of human mast cell degranulation in vitro.50
The Neurosensory Barrier
Components of the neurosensory system function as sensors of external stimuli and include keratinocytes and ion channels expressed on cutaneous nerves. When activated, sensory nerve endings release neuropeptides such as substance P, mediating itch, pain, and inflammation.7 This is further compounded by the itch-scratch cycle: pruritis compels a patient to scratch AD lesions, resulting in a short-term neurological reward response but stimulating further dermatological inflammation.75,76
In the 2019 clinical study, in which 60 patients with mild AD used EC or vehicle twice daily on their forearms for 28 days, pruritus was significantly reduced by 89% in patients treated with EC versus baseline (p < 0.05).68 Patient self-evaluation showed a reduction in pruritus after just 4 days treatment with EC versus vehicle, which continued steadily and progressively. Desquamation was significantly reduced by 83% after 28 days in patients treated with EC versus baseline (p < 0.05), although there was no significant difference in desquamation between the EC- and vehicle-treated groups at any timepoint.
The capacity for EC to improve desquamation and decrease itching was shown in a small clinical study: in adults with AD (N = 10), desquamation in treated areas significantly improved from moderate at baseline (mean rating 3.1) to largely absent by day 7 (mean rating 1.1 at days 7 and 21; p < 0.005 vs baseline at all time points). Most (9/10) patients reported improvements in itching after 24 hours.69
AD Topical Treatment Approaches: Guidelines and Supporting Evidence
The European guidelines for AD treatment recommend liberal and frequent use of emollients (minimum amount of 250 g per week for adults), and the American Academy of Dermatology advises that moisturizers should be the primary treatment for mild disease and part of the regimen for moderate/severe disease.6,77 A recently published algorithm to inform clinical decision-making recommends regular use of emollients for early AD control.78 However, the European guidelines note that direct sole use of emollients on inflamed skin is poorly tolerated, and so induction of remission with TCS or TCI is required before application of the emollient.6
For long-term AD management, an alternative to TCS is required;79 prolonged use of TCS can cause skin atrophy, barrier impairment, increased infection risk, and tachyphylaxis.6,80–82 Additionally, corticophobia is an issue in patients receiving TCS: over 80% of patients and caregivers have concerns about TCS and 36% of patients are nonadherent to TCS treatment.83
TCI, namely pimecrolimus and tacrolimus, are favorable over TCS for topical long-term management as they do not impair the epidermal barrier function or cause skin atrophy.6,84 In an evaluation of a pimecrolimus-based regimen in patients at least 3 months old, a high percentage of patients were clear or almost clear of AD signs at the end of treatment.85 Pimecrolimus treatment also reduced TCS use: 47% of patients never used TCS over the 6-month study period, indicating that pimecrolimus has a steroid-sparing effect.85 Pimecrolimus has an improved safety profile versus TCS, with lower systemic exposure.86 Although the JOELLE study reported a possible increased risk of lymphoma with tacrolimus and pimecrolimus, the low incidence rates implied that even if the increased risk is causal, it represents a small excess risk for individual patients. Residual confounding by AD severity, increased monitoring of severe patients, and reverse causation could have affected the results.87 Previous reports have found no evidence to suggest an increased risk of lymphoma with TCI.79,88,89
Regular emollient use may decrease the need for TCS while maintaining efficacy in AD treatment.90–92 In 108 children with moderate AD (aged 6 months to 6 years) treated with an oat-based sterile emollient plus cream for 3 months, the number of flares and use of TCS significantly decreased by month 3 (both p < 0.001).93 Additionally, in 2456 patients with mild-to-moderate AD treated with an emollient plus containing N-palmitoylethanolamine, TCS were omitted by 56% of patients at the end of the study. The average weekly application rate of TCS decreased by 62% from 7.9 ± 6.0 to 3.0 ± 5.1 (p < 0.001).94
Compared with other topical therapies, emollients are rarely associated with health hazards, even when used on large body surface areas over an extended period.31 Some emollients may cause contact irritation, although this is rare. Specific emollient components require extra attention regarding safety: occlusive oils are associated with cosmetic acne, while preservatives such as sorbic acid, fragrances, or balsam of Peru may cause contact urticaria.31
With regard to emollients plus specifically, tolerability is generally good with few adverse events (AEs) reported. One study investigating an emollient plus containing vitamin B3, palmitoyl ethanolamide, β-sitosterol, zinc, and ceramides reported that 4/62 patients (6.5%) experienced symptoms possibly or definitely related to treatment, including warm sensation, pruritus, stinging, pain, erythema, and flare-ups.26 Another study reporting on an emollient plus containing 5% urea reported that 5/87 patients (6%) experienced at least one treatment-related adverse event (TRAE) and one patient experienced a severe TRAE.41 Three further studies investigating different emollients plus (including a panthenol-containing emollient plus, a niacinamide-containing emollient plus, and a ceramide 3-containing emollient plus) all reported good tolerability with no AEs related to treatment.38,49,56
With EC to date, no AEs have been reported in patients with AD.43,54,68 In one study, investigators judged EC tolerability as good or excellent in 100% of treated patients.54 In a patient assessment of EC, the majority of patients rated EC as good or excellent in terms of cosmetic acceptability.68
Safety implications must be considered when selecting an AD topical treatment approach. Various emollient treatment approaches have been recommended: from prophylactic use in neonates and infants to prevent AD occurrence, to proactive, intermittent, and synergistic treatments.
The Preventative Approach
Emollients for the Prevention of AD
Evidence suggests that prophylactic use of emollients can prevent AD flares. In a study evaluating a body wash and moisturizer regimen (Cetaphil Restoraderm Skin Restoring Body Wash and Cetaphil Restoraderm Skin Restoring Moisturizer [Galderma Laboratories, L.P., Fort Worth, USA]) for infants and toddlers (aged 3–36 months) with a history of AD (N = 56), the percentage of subjects with no erythema increased from 33.9% to 50.0% by week 4.47 The percentage of subjects with no scaling/dryness increased from 58.9% to 85.2% at week 4.
In a randomized controlled trial in 124 neonates at high risk for AD, Simpson et al investigated whether skin barrier enhancement with emollients (an oil, cream/gel, or ointment) from birth represents a feasible strategy for reducing AD incidence.95 Daily emollient use significantly reduced the cumulative incidence of AD at 6 months (43% vs 22% for control vs emollient, respectively), with a relative risk (RR) reduction of 50% (RR: 0.50; 95% confidence interval [CI]: 0.28–0.90; p = 0.017).
This is supported by a study by Horimukai et al: daily application of an emulsion-type emollient (2e [Douhet] emulsion) during the first 32 weeks of life reduced AD risk in infants considered to be at high risk for the condition (N = 118).96 Approximately 32% fewer neonates who received the emollient had AD by week 32 compared with control subjects (p = 0.012). In 100 neonates (recruited as newborns within 21 days), McClanahan et al also found a trend for a protective effect of daily Restoraderm moisturizer full-body application compared with application of control emollient to dry skin only. A trend for reduced AD incidence was observed with Restoraderm moisturizer compared with control at 12 months (13.2% vs 25.0%, respectively; p = 0.204) and 2 years (19.4% vs 31.0%, respectively; p = 0.296), but did not reach statistical significance.97
However, there is conflicting evidence on the preventative use of emollients for AD. In the Barrier Enhancement for Eczema Prevention (BEEP) multicenter, randomized, controlled trial, 1394 newborns at high risk of developing AD were assigned to receive either daily emollient (either Diprobase cream [Bayer, Barmen, Germany] or DoubleBase gel [Dermal Laboratories Ltd., Hitchin, UK]) or control for the first year of life.98 At two years of age, AD was present in 23% of infants in the emollient group and 25% of infants in the control group (adjusted RR: 0.95 [95% CI: 0.78–1.16], p = 0.61; adjusted risk difference –1.2% [95% CI: –5.9 to 3.6]), suggesting that daily emollient use during the first year of life does not prevent AD in high-risk children. There was also evidence to suggest that daily emollient use in the first year of life may increase infection risk.
Emollients for the Prevention of Atopic March
The ‘atopic march’ is a clinical sequence that begins with AD and progresses to food allergy followed by development of respiratory allergies, such as asthma and allergic rhinitis.99 It remains unclear whether regular emollient application to the skin of neonates can decrease the risk of AD progression to food allergies.99 The ‘Prevention of AD By a Barrier Lipid Equilibrium Strategy’ (PEBBLES) pilot study showed a trend for decreased food sensitization at 6 and 12 months of age when emollients were used preventatively from birth, particularly when the lipid-rich emollient was introduced early (<2 weeks after birth) and used frequently (≥5 days per week). However, this study was not powered to detect differences or measure true food allergy outcomes.100
Conversely, in the BEEP trial, food allergies to milk, egg, or peanut were confirmed in 7% of infants in the emollient group and 5% in the control group (adjusted RR: 1.47; 95% CI: 0.93–2.33), and the proportion of infants with allergic rhinitis, wheezing, and allergic sensitization to cat dander, grass pollen, and dust mites was similar between groups.98 The Preventing Atopic Dermatitis and ALLergies in Children (PreventADALL) trial aimed to determine if either regular emollient application from 2 weeks of age, or early complementary feeding introduced between 12 and 16 weeks of age, reduced AD development by 12 months in the general population (N = 2397). Neither emollients nor early complementary feeding reduced AD development, with a risk difference of 3.1% (95% CI: –0.3 to 6.5) for skin intervention and 1.0% (95% CI: –2.1 to 4.1) for food intervention, in favor of control.101
Evidence for the use of emollients in the prevention of AD and atopic march is conflicting. This is perhaps unsurprising given the heterogeneous compositions of commercially available emollients (Table 1); it is possible that the specific composition of different emollients and/or emollients plus can impact their effects.
In the BEEP trial, participants could choose between Doublebase Gel or Diprobase Cream. Doublebase Gel is composed of two emollients: isopropyl myristate and liquid paraffin.102 There are a range of creams in the Diprobase range with differing compositions, and it is not clear which was used in the BEEP trial. In the PreventADALL trial, the skin intervention consisted of baths with emulsified oil (paraffinum liquidum and trilaureth-4-phosphate) and Ceridal cream (GSK, London, UK), whose key ingredients are petrolatum, paraffinum liquidum, and glycerin.103 The emollients used in the BEEP and PreventADALL trials were not emollients plus containing additional active ingredients. Hypothetically, an emollient plus may be more effective at preventing AD and atopic march; prospective trials are required to confirm this hypothesis.
In future AD studies, the choice of emollient or emollient plus (and its composition) should be carefully considered. Publications should not only incorporate transparent reporting of the choice of emollient or emollient plus, but also discuss the impact of any active ingredients on results. Head-to-head trials are required to determine the most effective composition for emollients plus.
The Proactive Approach
For established disease, a proactive approach to long-term AD management has been suggested, where flares are treated with anti-inflammatory therapy (TCI or TCS) until the affected areas are almost clear.104 Anti-inflammatory treatment on previously affected skin areas should subsequently continue once or twice per week (depending on disease severity) in combination with an emollient, regardless of AD signs or symptoms.6,105 Tacrolimus 0.03% twice daily for treatment of flares for a maximum of 6 weeks, followed by proactive use of tacrolimus 0.03% twice weekly to all affected areas for 1 year was shown to increase median time to flare from 36 days in the vehicle control group to 217 days in the proactive tacrolimus group.106
The Intermittent Approach
Conversely, an intermittent approach to long-term AD management involves applying TCS or TCI at the first signs (ie, erythema) or symptoms (ie, pruritus) of AD to prevent progression to flare. This was trialed in a study where 713 patients with AD (aged 2–17 years) were randomized to either a pimecrolimus-based regimen (emollients with pimecrolimus at the first early signs and symptoms of flare) or a conventional regimen (emollients with vehicle at the first early signs and symptoms of flare). Intermittent use of pimecrolimus was associated with a significantly longer flare-free period compared with the conventional regimen (p < 0.001). The proportion of patients with no flares after 6 and 12 months was approximately twice as high in the group treated with pimecrolimus plus emollient compared with those treated with emollient alone (61.0% vs 34.2%, respectively, at 6 months; 50.8% vs 28.3%, respectively, at 12 months).107
The Synergistic Approach
In an open-label, multi-center study on EC use for maintaining disease regression after pimecrolimus therapy in mild-to-moderate AD, EC after pimecrolimus maintained regression of flare for at least 4 months in almost all patients: 98% of patients at the end of the study were clear or almost clear of signs and symptoms at 4 months.54 Improvement was observed in all other efficacy outcomes, including Investigator’s Global Assessment, SCORing Atopic Dermatitis, and Visual Analog Scale.54 A synergistic approach, with pharmacological intervention for flare treatment and emollient cream for maintenance therapy, may be useful in management of mild-to-moderate AD, as illustrated in Figure 1. Using pimecrolimus and EC, this approach allows patients to avoid the use of rescue medication (topical anti-inflammatory treatment) for up to 4 months.54
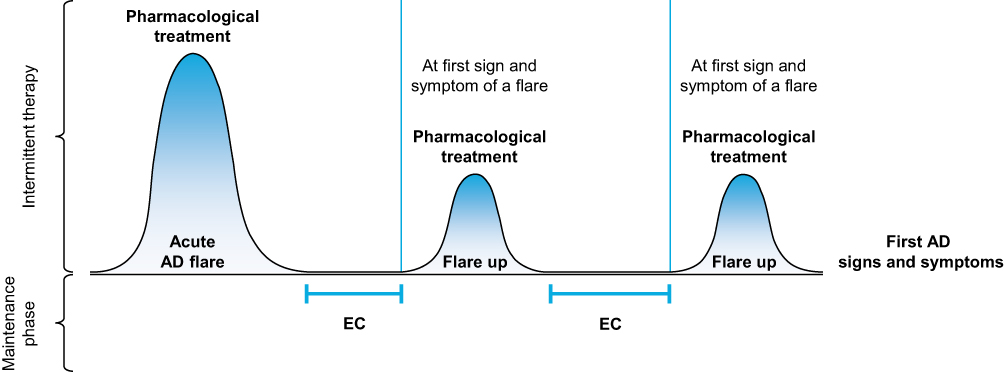 |
Figure 1 The synergistic approach to long-term AD management. Figure developed as a result of the expert panel’s discussions, in line with treatment labels and previous data.54,108 Abbreviations: AD, atopic dermatitis; EC, emollient cream. |
Conclusion
Based on the evidence summarized in this review, the authors recommend the novel generation of emollients, emollients plus, for AD maintenance therapy. However, not all emollients plus are created equal: their composition can vary widely with a profound impact on clinical efficacy. This should not be overlooked when interpreting results. Despite a wealth of evidence supporting the clinical efficacy of emollients plus in AD and their ability to restore and maintain skin barrier function, head-to-head trials are required to determine their most effective composition for AD treatment.
When considering AD treatment, the safety profiles of topical therapies must be carefully examined. There are data to support several treatment approaches for emollients in AD, including preventative, proactive, intermittent, and synergistic approaches. Although there is conflicting evidence on the use of emollients for preventing atopic march, regular, synergistic use of emollients is effective for AD disease control and reduces the need for anti-inflammatory treatment. This reduces the risk of adverse reactions associated with TCS.
The ability of emollients plus to repair and maintain the skin barrier places them not only as suitable maintenance therapies for AD, but also as effective treatment options when used synergistically with anti-inflammatory pharmacological therapies.
Acknowledgments
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Bonnie Nicholson, PhD, and Molly Macpherson, BSc, of Ashfield MedComms, an Inizio company, and funded by Meda Pharma S.p.A., a Viatris company.
Author Contributions
All authors made significant contributions to the work reported; took part in drafting, revising and critically reviewing the article; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Medical writing support for the development of this manuscript was funded by Meda Pharma S.p.A., a Viatris company.
Disclosure
EA has received honorarium as advisor or speaker from the following companies: Bayer Health Care, Bioderma, Galderma SA, Glenmark, La Roche Posay, L’Oreal, Meda Pharma S.p.A. (a Viatris company), Merz Aesthetics, Pierre Fabre Dermo-Cosmétique, Uriage, and Vichy. CP has received research fees from Meda Pharma S.p.A. (a Viatris company). AS has received research fees from Meda Pharma S.p.A. (a Viatris company). TL has participated as Principal Investigator in clinical trials, advisory boards and has given lectures, sponsored by Janssen, La Roche Posay, Lilly, Novartis, Pfizer and Sanofi. He has received consultancy/speaker honoraria from Abbvie, Galderma, Janssen, La Roche Posay, Meda Pharma S.p.A. (a Viatris company), Novartis and Sanofi, and has acted as a scientific advisory board member for Abbvie, Celgene, Galderma, Janssen, La Roche Posay, Lilly, Meda Pharma S.p.A. (a Viatris company), Menlo, Pfizer and Symrise. He has received research grants from: Celgene, Janssen-Cilag, Leo, Meda Pharma S.p.A. (a Viatris company) and Pfizer.
References
1. Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109–1122.
2. Andersen RM, Thyssen JP, Maibach HI. Qualitative vs. quantitative atopic dermatitis criteria - in historical and present perspectives. J Eur Acad Dermatol Venereol. 2016;30(4):604–618.
3. Bieber T. Atopic dermatitis. N Engl J Med. 2008;358(14):1483–1494.
4. Bos JD, Brenninkmeijer EE, Schram ME, Middelkamp-Hup MA, Spuls PI, Smitt JH. Atopic eczema or atopiform dermatitis. Exp Dermatol. 2010;19(4):325–331.
5. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338–351.
6. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657–682.
7. Luger T, Amagai M, Dreno B, et al. Atopic dermatitis: role of the skin barrier, environment, microbiome, and therapeutic agents. J Dermatol Sci. 2021;102(3):142–157.
8. Tsakok T, Woolf R, Smith CH, Weidinger S, Flohr C. Atopic dermatitis: the skin barrier and beyond. Br J Dermatol. 2019;180(3):464–474.
9. Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1):1.
10. De Benedetto A, Rafaels NM, McGirt LY, et al. Tight junction defects in patients with atopic dermatitis. J Allergy Clin Immunol. 2011;127(3):773–786.e771–777.
11. Hon KL, Kung JSC, Ng WGG, Leung TF. Emollient treatment of atopic dermatitis: latest evidence and clinical considerations. Drugs Context. 2018;7:212530. doi:10.7573/dic.212530
12. Galli E, Neri I, Ricci G, et al. Consensus conference on clinical management of pediatric atopic dermatitis. Ital J Pediatr. 2016;42:26. doi:10.1186/s13052-016-0229-8
13. Saeedi M, Morteza-Semnani K, Ghoreishi MR. The treatment of atopic dermatitis with licorice gel. J Dermatolog Treat. 2003;14(3):153–157.
14. Bissett D. Topical niacinamide and barrier enhancement. Cutis. 2002;70(6 Suppl):8–12.
15. Gasparri F, Lupieri Sinibaldi T. Skin microbiome changes after treatment with a topical emollient plus in subjects predisposed to atopic dermatitis.
16. Offerta A, Bonina F, Gasparri F, Zanardi A, Micicche L, Puglia C. In vitro percutaneous absorption of niacinamide and phytosterols and in vivo evaluation of their effect on skin barrier recovery. Curr Drug Deliv. 2016;13(1):111–120.
17. Davani-Davari D, Negahdaripour M, Karimzadeh I, et al. Prebiotics: definition, types, sources, mechanisms, and clinical applications. Foods. 2019;8(3):92.
18. Katsuyama M, Ichikawa H, Ogawa S, Ikezawa Z. A novel method to control the balance of skin microflora. Part 1. Attack on biofilm of Staphylococcus aureus without antibiotics. J Dermatol Sci. 2005;38(3):197–205.
19. Krutmann J. Pre- and probiotics for human skin. J Dermatol Sci. 2009;54(1):1–5.
20. Freitag G, Höppner T. Results of a postmarketing drug monitoring survey with a polidocanol-urea preparation for dry, itching skin. Curr Med Res Opin. 1997;13(9):529–537.
21. Tanno O, Ota Y, Kitamura N, Katsube T, Inoue S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability barrier. Br J Dermatol. 2000;143(3):524–531.
22. Ishida T, Mizushina Y, Yagi S, et al. Inhibitory effects of glycyrrhetinic acid on DNA polymerase and inflammatory activities. Evid Based Complement Alternat Med. 2012;2012:650514. doi:10.1155/2012/650514
23. Proksch E, Lachapelle JM. The management of dry skin with topical emollients--recent perspectives. J Dtsch Dermatol Ges. 2005;3(10):768–774.
24. Proksch E, Berardesca E, Misery L, Engblom J, Bouwstra J. Dry skin management: practical approach in light of latest research on skin structure and function. J Dermatolog Treat. 2020;31(7):716–722.
25. Saint Aroman M, Guillot P, Dahan S, et al. Efficacy of a repair cream containing Rhealba oat plantlets extract l-ALA-l-GLU dipeptide, and hyaluronic acid in wound healing following dermatological acts: a meta-analysis of >2,000 patients in eight countries corroborated by a dermatopediatric clinical case. Clin Cosmet Investig Dermatol. 2018;11:579–589. doi:10.2147/ccid.S177614
26. Gayraud F, Sayag M, Jourdan E. Efficacy and tolerance assessment of a new type of dermocosmetic in infants and children with moderate atopic dermatitis. J Cosmet Dermatol. 2015;14(2):107–112.
27. Patrizi A, Capitanio B, Neri I, et al. A double-blind, randomized, vehicle-controlled clinical study to evaluate the efficacy and safety of MAS063DP (ATOPICLAIRTM) in the management of atopic dermatitis in paediatric patients. Pediatr Allergy Immunol. 2008;19(7):619–625.
28. Angelova-Fischer I, Rippke F, Richter D, et al. Stand-alone emollient treatment reduces flares after discontinuation of topical steroid treatment in atopic dermatitis: a double-blind, randomized, vehicle-controlled, left-right comparison study. Acta Derm Venereol. 2018;98(5):517–523.
29. Fluhr JW, Darlenski R, Surber C. Glycerol and the skin: holistic approach to its origin and functions. Br J Dermatol. 2008;159(1):23–34.
30. Lin TK, Zhong L, Santiago JL. Anti-inflammatory and skin barrier repair effects of topical application of some plant oils. Int J Mol Sci. 2017;19(1):70.
31. Purnamawati S, Indrastuti N, Danarti R, Saefudin T. The role of moisturizers in addressing various kinds of dermatitis: a review. Clin Med Res. 2017;15(3–4):75–87.
32. Phan HTL, Kim HJ, Jo S, Kim WK, Namkung W, Nam JH. Anti-inflammatory effect of licochalcone a via regulation of ORAI1 and K(+) channels in t-lymphocytes. Int J Mol Sci. 2021;22(19):10847.
33. Stettler H, de Salvo R, Olsavszky R, Nanu EA, Dumitru V, Trapp S. Performance and tolerability of a new topical dexpanthenol-containing emollient line in subjects with dry skin: results from three randomized studies. Cosmetics. 2021;8(1):18.
34. Proksch E, de Bony R, Trapp S, Boudon S. Topical use of dexpanthenol: a 70th anniversary article. J Dermatolog Treat. 2017;28(8):766–773.
35. Otte N, Borelli C, Korting HC. Nicotinamide - biologic actions of an emerging cosmetic ingredient. Int J Cosmet Sci. 2005;27(5):255–261.
36. Wohlrab J, Kreft D. Niacinamide - mechanisms of action and its topical use in dermatology. Skin Pharmacol Physiol. 2014;27(6):311–315.
37. Caussin J, Gooris GS, Bouwstra JA. FTIR studies show lipophilic moisturizers to interact with stratum corneum lipids, rendering the more densely packed. Biochim Biophys Acta. 2008;1778(6):1517–1524.
38. Stettler H, Kurka P, Kandzora J, Pavel V, Breuer M, Macura-Biegun A. A new topical panthenol-containing emollient for maintenance treatment of childhood atopic dermatitis: results from a multicenter prospective study. J Dermatol Treat. 2017;28(8):774–779.
39. Stettler H, Kurka P, Wagner C, et al. A new topical panthenol-containing emollient: skin-moisturizing effect following single and prolonged usage in healthy adults, and tolerability in healthy infants. J Dermatol Treat. 2017;28(3):251–257.
40. Stettler H, Kurka P, Lunau N, et al. A new topical panthenol-containing emollient: results from two randomized controlled studies assessing its skin moisturization and barrier restoration potential, and the effect on skin microflora. J Dermatolog Treat. 2017;28(2):173–180.
41. Åkerström U, Reitamo S, Langeland T, et al. Comparison of moisturizing creams for the prevention of atopic dermatitis relapse: a randomized double-blind controlled multicentre clinical trial. Acta Derm Venereol. 2015;95(5):587–592.
42. Wirén K, Nohlgård C, Nyberg F, et al. Treatment with a barrier-strengthening moisturizing cream delays relapse of atopic dermatitis: a prospective and randomized controlled clinical trial. J Eur Acad Dermatol Venereol. 2009;23(11):1267–1272.
43. Quadri M, Lotti R, Bonzano L, et al. A novel multi-action emollient plus cream improves skin barrier function in patients with atopic dermatitis: in vitro and clinical evidence. Skin Pharmacol Physiol. 2021;34(1):8–18.
44. Kircik LH, Del Rosso JQ. Nonsteroidal treatment of atopic dermatitis in pediatric patients with a ceramide-dominant topical emulsion formulated with an optimized ratio of physiological lipids. J Clin Aesthet Dermatol. 2011;4(12):25–31.
45. Weber TM, Herndon JH
46. Seité S, Zelenkova H, Martin R. Clinical efficacy of emollients in atopic dermatitis patients - relationship with the skin microbiota modification. Clin Cosmet Investig Dermatol. 2017;10:25–33. doi:10.2147/ccid.S121910
47. Simpson E, Trookman NS, Rizer RL, et al. Safety and tolerability of a body wash and moisturizer when applied to infants and toddlers with a history of atopic dermatitis: results from an open-label study. Pediatr Dermatol. 2012;29(5):590–597.
48. Brandt S, Meckfessel MH, Lio PA. Tolerability and cosmetic acceptability of a body wash in atopic dermatitis-prone subjects. J Drugs Dermatol. 2014;13(9):1108–1111.
49. Ma L, Li P, Tang J, et al. Prolonging time to flare in pediatric atopic dermatitis: a randomized, investigator-blinded, controlled, multicenter clinical study of a ceramide-containing moisturizer. Adv Ther. 2017;34(12):2601–2611.
50. Nguyen T, Chol B, Maitre M, et al. Additional pharmacological activity of I-modulia and generation of two newly designed extracts of Aquaphilus dolomiae culture for dermocosmetic actives. J Eur Acad Dermatol Venereol. 2020;34(Suppl 5):27–29.
51. Aries MF, Hernandez-Pigeon H, Vaissière C, et al. Anti-inflammatory and immunomodulatory effects of Aquaphilus dolomiae extract on in vitro models. Clin Cosmet Investig Dermatol. 2016;9:421–434. doi:10.2147/ccid.S113180
52. Aries MF, Vaissière C, Delga H, Castex-Rizzi N, Bessou-Touya S, Nguyen T. Antiinflammatory and immunomodulatory effects of I-modulia, an Aquaphilus dolomiae extract, on atopic dermatitis in vitro. J Am Acad Dermatol. 2014;70(5 Suppl 1):AB61.
53. Aries MF, Duplan H, Hernandez-Pigeon H, Galliano MF, Bessou-Touya S, Nguyen T. I-modulia, an Aquaphilus dolomiae extract, stimulates innate immune response through Toll-like receptor activation. J Am Acad Dermatol. 2014;70(5 Suppl 1):AB63.
54. Sparavigna A, Trischitta A. Open multi-centre study on the use of a novel emollient plus cream (EC) for maintaining eczema regression after pimecrolimus therapy in atopic dermatitis. J Plast Pathol Dermatol. 2020;16(3):1–14.
55. Tiplica GS, Boralevi F, Konno P, et al. The regular use of an emollient improves symptoms of atopic dermatitis in children: a randomized controlled study. J Eur Acad Dermatol Venereol. 2018;32(7):1180–1187.
56. Weber TM, Samarin F, Babcock MJ, Filbry A, Rippke F. Steroid-free over-the-counter eczema skin care formulations reduce risk of flare, prolong time to flare, and reduce eczema symptoms in pediatric subjects with atopic dermatitis. J Drugs Dermatol. 2015;14(5):478–485.
57. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. 2021;21(1):21–40.
58. Wollenberg A, Thomsen SF, Lacour JP, Jaumont X, Lazarewicz S. Targeting immunoglobulin E in atopic dermatitis: a review of the existing evidence. World Allergy Organ J. 2021;14(3):100519.
59. Palmer CN, Irvine AD, Terron-Kwiatkowski A, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38(4):441–446.
60. Eberlein-König B, Schäfer T, Huss-Marp J, et al. Skin surface pH, stratum corneum hydration, trans-epidermal water loss and skin roughness related to atopic eczema and skin dryness in a population of primary school children. Acta Derm Venereol. 2000;80(3):188–191.
61. Sparavigna A, Setaro M, Gualandri V. Cutaneous pH in children affected by atopic dermatitis and in healthy children: a multicenter study. Skin Res Technol. 1999;5(4):221–227.
62. Xie L, McKenzie CI, Qu X, et al. pH and proton sensor gpr65 determine susceptibility to atopic dermatitis. J Immunol. 2021;207(1):101–109.
63. Robert R, Mackay CR. Gαs-coupled GPCRs GPR65 and GPR174. Downers for immune responses. Immunol Cell Biol. 2018;96(4):341–343.
64. Jin Y, Sato K, Tobo A, et al. Inhibition of interleukin-1β production by extracellular acidification through the TDAG8/cAMP pathway in mouse microglia. J Neurochem. 2014;129(4):683–695.
65. Mogi C, Tobo M, Tomura H, et al. Involvement of proton-sensing TDAG8 in extracellular acidification-induced inhibition of proinflammatory cytokine production in peritoneal macrophages. J Immunol. 2009;182(5):3243–3251.
66. Chen YE, Tsao H. The skin microbiome: current perspectives and future challenges. J Am Acad Dermatol. 2013;69(1):143–155.
67. Kong HH, Oh J, Deming C, et al. Temporal shifts in the skin microbiome associated with disease flares and treatment in children with atopic dermatitis. Genome Res. 2012;22(5):850–859.
68. Sparavigna A, Tenconi B, La Penna L. Efficacy of a novel emollient plus in atopic dermatitis: a randomized, vehicle-controlled, double-blind study. J Plast Pathol Dermatol. 2019;15(2):85–93.
69. Gasparri F. Effects of a novel emollient cream on skin moisture, epidermal barrier function and atopic dermatitis signs and symptoms: results from a clinical study.
70. Wollina U. Microbiome in atopic dermatitis. Clin Cosmet Investig Dermatol. 2017;10:51–56. doi:10.2147/ccid.S130013
71. Bockmühl D, Jassoy C, Nieveler S, Scholtyssek R, Wadle A, Waldmann-Laue M. Prebiotic cosmetics: an alternative to antibacterial products. Int J Cosmet Sci. 2007;29(1):63–64.
72. Seite S, Flores GE, Henley JB, et al. Microbiome of affected and unaffected skin of patients with atopic dermatitis before and after emollient treatment. J Drugs Dermatol. 2014;13(11):1365–1372.
73. Gueniche A, Knaudt B, Schuck E, et al. Effects of nonpathogenic gram-negative bacterium Vitreoscilla filiformis lysate on atopic dermatitis: a prospective, randomized, double-blind, placebo-controlled clinical study. Br J Dermatol. 2008;159(6):1357–1363.
74. Lai Y, Gallo RL. Toll-like receptors in skin infections and inflammatory diseases. Infect Disord Drug Targets. 2008;8(3):144–155.
75. Rinaldi G. The itch-scratch cycle: a review of the mechanisms. Dermatol Pract Concept. 2019;9(2):90–97.
76. Murota H, Katayama I. Exacerbating factors of itch in atopic dermatitis. Allergol Int. 2017;66(1):8–13.
77. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116–132.
78. Luger T, Adaskevich U, Anfilova M, et al. Practical algorithm to inform clinical decision-making in the topical treatment of atopic dermatitis. J Dermatol. 2021;48(8):1139–1148.
79. Sigurgeirsson B, Boznanski A, Todd G, et al. Safety and efficacy of pimecrolimus in atopic dermatitis: a 5-year randomized trial. Pediatrics. 2015;135(4):597–606.
80. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol. 2006;54(1):1–15; quiz 16–18.
81. Wong VK, Della Croce C, Schonfeld S, Mastrangelo AM, Lebwohl M. Use and abuse of topical corticosteroids in infections of the skin and related structures. J Drugs Dermatol. 2003;2(3):268–276.
82. Danby SG, Chittock J, Brown K, Albenali LH, Cork MJ. The effect of tacrolimus compared with betamethasone valerate on the skin barrier in volunteers with quiescent atopic dermatitis. Br J Dermatol. 2014;170(4):914–921.
83. Aubert-Wastiaux H, Moret L, Le Rhun A, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. 2011;165(4):808–814.
84. Jensen JM, Pfeiffer S, Witt M, et al. Different effects of pimecrolimus and betamethasone on the skin barrier in patients with atopic dermatitis. J Allergy Clin Immunol. 2009;123(5):1124–1133.
85. Lübbe J, Friedlander SF, Cribier B, et al. Safety, efficacy, and dosage of 1% pimecrolimus cream for the treatment of atopic dermatitis in daily practice. Am J Clin Dermatol. 2006;7(2):121–131.
86. Billich A, Aschauer H, Aszódi A, Stuetz A. Percutaneous absorption of drugs used in atopic eczema: pimecrolimus permeates less through skin than corticosteroids and tacrolimus. Int J Pharm. 2004;269(1):29–35.
87. Castellsague J, Kuiper JG, Pottegård A, et al. A cohort study on the risk of lymphoma and skin cancer in users of topical tacrolimus, pimecrolimus, and corticosteroids (Joint European Longitudinal Lymphoma and Skin Cancer Evaluation - JOELLE study). Clin Epidemiol. 2018;10:299–310. doi:10.2147/clep.S146442
88. Carr WW. Topical calcineurin inhibitors for atopic dermatitis: review and treatment recommendations. Paediatr Drugs. 2013;15(4):303–310.
89. Luger TA, Lahfa M, Fölster-Holst R, et al. Long-term safety and tolerability of pimecrolimus cream 1% and topical corticosteroids in adults with moderate to severe atopic dermatitis. J Dermatolog Treat. 2004;15(3):169–178.
90. Grimalt R, Mengeaud V, Cambazard F. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214(1):61–67.
91. Lucky AW, Leach AD, Laskarzewski P, Wenck H. Use of an emollient as a steroid-sparing agent in the treatment of mild to moderate atopic dermatitis in children. Pediatr Dermatol. 1997;14(4):321–324.
92. Msika P, De Belilovsky C, Piccardi N, Chebassier N, Baudouin C, Chadoutaud B. New emollient with topical corticosteroid-sparing effect in treatment of childhood atopic dermatitis: SCORAD and quality of life improvement. Pediatr Dermatol. 2008;25(6):606–612.
93. Mengeaud V, Phulpin C, Bacquey A, Boralevi F, Schmitt AM, Taieb A. An innovative oat-based sterile emollient cream in the maintenance therapy of childhood atopic dermatitis. Pediatr Dermatol. 2015;32(2):208–215.
94. Eberlein B, Eicke C, Reinhardt HW, Ring J. Adjuvant treatment of atopic eczema: assessment of an emollient containing N-palmitoylethanolamine (ATOPA study). J Eur Acad Dermatol Venereol. 2008;22(1):73–82.
95. Simpson EL, Chalmers JR, Hanifin JM, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134(4):818–823.
96. Horimukai K, Morita K, Narita M, et al. Application of moisturizer to neonates prevents development of atopic dermatitis. J Allergy Clin Immunol. 2014;134(4):824–830.e826.
97. McClanahan D, Wong A, Kezic S, et al. A randomized controlled trial of an emollient with ceramide and filaggrin-associated amino acids for the primary prevention of atopic dermatitis in high-risk infants. J Eur Acad Dermatol Venereol. 2019;33(11):2087–2094.
98. Chalmers JR, Haines RH, Bradshaw LE, et al. Daily emollient during infancy for prevention of eczema: the BEEP randomised controlled trial. Lancet. 2020;395(10228):962–972.
99. Lowe AJ, Leung DYM, Tang MLK, Su JC, Allen KJ. The skin as a target for prevention of the atopic march. Ann Allergy Asthma Immunol. 2018;120(2):145–151.
100. Lowe AJ, Su JC, Allen KJ, et al. A randomized trial of a barrier lipid replacement strategy for the prevention of atopic dermatitis and allergic sensitization: the PEBBLES pilot study. Br J Dermatol. 2018;178(1):e19–e21.
101. Skjerven HO, Rehbinder EM, Vettukattil R, et al. Skin emollient and early complementary feeding to prevent infant atopic dermatitis (PreventADALL): a factorial, multicentre, cluster-randomised trial. Lancet. 2020;395(10228):951–961.
102. Dermal. Doublebase gel package leaflet; 2020. Available from: https://www.medicines.org.uk/emc/files/pil.1325.pdf.
103. ApoPro.dk. Ceridal Crème; 2021. Available from: https://apopro.dk/ceridal-creme-150-g-216917.
104. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: section 4. Prevention of disease flares and use of adjunctive therapies and approaches. J Am Acad Dermatol. 2014;71(6):1218–1233.
105. Bieber T. Atopic dermatitis. Ann Dermatol. 2010;22(2):125–137.
106. Reitamo S, Allsopp R. Treatment with twice-weekly tacrolimus ointment in patients with moderate to severe atopic dermatitis: results from two randomized, multicentre, comparative studies. J Dermatolog Treat. 2010;21(1):34–44.
107. Wahn U, Bos JD, Goodfield M, et al. Efficacy and safety of pimecrolimus cream in the long-term management of atopic dermatitis in children. Pediatrics. 2002;110(1 Pt 1):e2.
108. Mylan. Elidel 10mg/G cream package leaflet: information for the user; 2019. Available from: https://www.medicines.org.uk/emc/files/pil.4966.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.