Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
The Role and Development of Advanced Clinical Practice Within Allied Health Professions: A Mixed Method Study
Authors Stewart-Lord A, Beanlands C ![]() , Khine R
, Khine R ![]() , Shamah S
, Shamah S ![]() , Sinclair N, Woods S
, Sinclair N, Woods S ![]() , Woznitza N
, Woznitza N ![]() , Baillie L
, Baillie L
Received 16 June 2020
Accepted for publication 3 August 2020
Published 25 November 2020 Volume 2020:13 Pages 1705—1715
DOI https://doi.org/10.2147/JMDH.S267083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Adéle Stewart-Lord,1 Clare Beanlands,2 Ricardo Khine,3 Shani Shamah,4 Noreen Sinclair,1 Sandie Woods,2 Nick Woznitza,5 Lesley Baillie6
1Therapeutic Radiography Allied Health Sciences School of Health and Social Care London South Bank University, London, UK; 2Occupational Therapy, Allied Health Sciences, London South Bank University, London, UK; 3Therapeutic Radiography, City University of London, London, UK; 4Service-User; Research (Public Patient Involvement) Consultant, Independent, London, UK; 5Diagnostic Radiography, Homerton University Hospital NHS Foundation Trust, London, UK; 6Adult Nursing, London South Bank University, London, UK
Correspondence: Adéle Stewart-Lord
Therapeutic Radiography Allied Health Sciences School of Health and Social Care London South Bank University, 103 Borough Road, London SE1 0AA, UK
Tel +44 207 815 7931
Fax +44 207 815 7933
Email [email protected]
Objective: To investigate the profiles of advanced clinical practitioners (ACPs) in the allied health professions (AHPs) and their skills, attributes, experiences and involvement in new models of care.
Methods: A 2 phase, cross sectional, mixed method survey of AHP ACPs across London was conducted in 2018– 2019. Online questionnaires were completed by 127 AHP ACPs and then semi-structured interviews were conducted with 15 AHP ACPs.
Results: The survey results gave a comprehensive overview of the attributes of AHPs in ACP roles across London. There was considerable variability between role titles, types and levels of qualification, and evolution of the roles. The respondents predominately worked in clinical practice, and less frequently in other ACP domains (research, leadership and management, education). The interview findings provided in-depth insights into the AHP ACP roles within four themes: being advanced, career pathways, outcomes of the advanced practitioner role and influencing and transforming. The “Being advanced” theme highlighted that expert practice comprised confident and autonomous practice, leadership, and applying specialist and expert decision-making skills. “Career pathways” highlighted the diversity within the participants’ roles, titles, career opportunities and development. In the “Outcomes of the advanced clinical practitioner role” theme, the ACPs described their services as prompter, more accessible and providing an improved patient journey. The “Influencing and transforming” theme highlighted networking and dissemination and ideas for innovation, influencing and transforming services.
Conclusion: This is the first comprehensive profile of ACP roles across AHPs and indicates that these roles are already having a positive impact on healthcare services and supporting new models of care. However, establishing the necessary infrastructure, standardization and governance for ACP roles across sectors, along with the career pathways, funding, sustainability and education, could increase impact in the future.
Keywords: allied health professionals, advanced practice, role development, expert practice, models of care, pathway configuration
Introduction
With a growing and aging population, new and emerging therapies and technologies, and chronic shortages of resources and workforce, healthcare in the United Kingdom (UK) is at a crossroad. One way to help meet rising service demand is by developing a workforce that can adapt and respond, maximizing existing roles and expanding the practice of nurses, midwives, health visitors and allied health professionals (AHPs). Health policies in England1,2 highlight the importance and need for change and to establish innovative new care models and develop new and enhanced roles, one key component being the formalization of advanced clinical practice.
In 2017, Health Education England (HEE)3 published the “Multi-professional framework for advanced clinical practice in England”, which aimed to provide clarity about advanced practice as a basis for good governance, enabling employers to “develop, enhance and deploy advanced clinical practice within their organizations” (p.4). The framework defined advanced clinical practice, to ensure a common understanding, and presented core capabilities, for all the health and care professions, across four pillars: clinical practice, leadership and management, education and research. HEE3 acknowledged that these capabilities may be demonstrated differently across varied professions and settings but emphasized that the core capabilities will enable standardization. Whilst there is considerable literature on advanced practice within nursing, publications relating to AHPs are more limited, especially in some professions.
NHS England4 proposed how AHPs could transform health, care and wellbeing across the sector. The effective use of AHPs could support integration, address variances in service quality and efficiency caused by historical service boundaries, duplication or fragmentation, and deliver evidence-based practice. The priorities for AHPs are therefore to meet the challenges of changing care needs through leadership further skill development, evaluating improvements, and evidencing impact of contribution. Case examples from “Allied Health Professionals into Action”4 demonstrated significant impact from AHPs addressing the challenges set by NHS England’s Five Year Forward View.1. A scoping review indicated the international interest in AHP ACP roles and examples of impact on service provision. However, there was a lack of profiling and evaluation of these roles. The current study aimed to investigate the profiles of AHP ACPs and their skills, attributes, experiences and involvement in new models of care, within one geographical area in England.
Methods
A cross-sectional, mixed method study was conducted in two phases: online questionnaires followed by individual semi-structured interviews. The project was conducted in partnership with NHS Trusts across North Central and East London. The scoping, development and delivery was achieved through a steering group, comprising the project lead, clinical partners and service user/care representation.
Data Collection Methods
The Phase 1 online self-completed questionnaire was administered through www.onlinesurveys.ac.uk. No standardized questionnaire existed; therefore the steering group designed a questionnaire, containing both open and closed questions, based on literature and expert opinion.5,6 The questionnaire was piloted with a small group (n=5) of AHP ACPs. Structured questions were used to collect data on demographic characteristics (age, gender, site of work), working practices, professional roles, length of employment and previous educational experiences. Attitudes and beliefs were measured using structured questions with a four-point Likert scale.
The Phase 2 interviews followed the questionnaire data analysis and provided an in-depth understanding of the ACP role. The interview guide contained mainly open-ended questions with follow-up probes used to elicit further detail (see Box 1, for questions). A pilot interview was conducted and no changes were needed. The pilot interview data were not included in analysis.
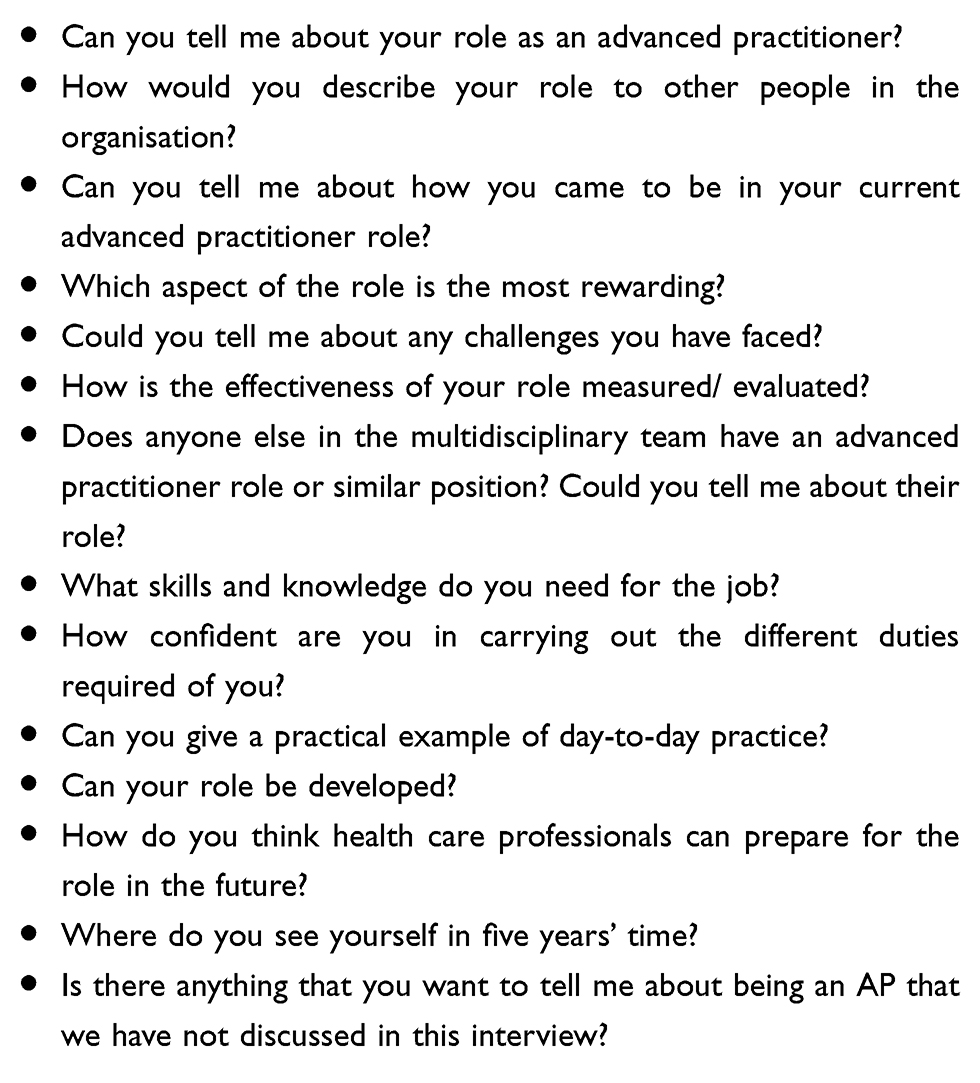 |
Box 1 Interview Questions |
Sample/Participants
There was no complete register of ACPs working in London and therefore it was difficult to determine a representative sample from the population of ACPs across AHP groups. Convenience sampling was used to access the maximum possible number of respondents to the Phase 1 questionnaire. An email invitation, containing a link to the online questionnaire, was sent via the HEE AHP network, with anticipation that the invitation would be shared amongst network members and others through snowballing. In addition, the steering group used social media to raise awareness of the project. The participant information sheet was included at the start of the questionnaire. The sample (n=127) who completed the questionnaire comprised: physiotherapists (n=40), diagnostic radiographers (n=34), paramedics (n=14), occupational therapists (n=12), art therapists (n=6), speech and language therapists (n=5), drama therapists (n=3), music therapists (n=3), therapeutic radiographers (n=2), dietetics (n=1), podiatrist (n=1), other (n=6).
The questionnaire included a question inviting respondents to identify willingness to participate in the Phase 2 interviews. Fifteen ACPs from varied professions volunteered. The research team contacted these respondents by email to explain the interview process and confirm their willingness to participate. Where possible, interviews were conducted face-to-face but, due to logistical constraints, some participants (n=4) were interviewed by telephone instead. The interview participants comprised: physiotherapists (n=7); radiographers (n=3); occupational therapists (n=2); paramedic (n=1); art therapist (n=1); drama therapist (n=1). Interviews were audio-recorded with the participants’ permission and then transcribed.
Data Analysis
Questionnaire data were entered into SPSS v21 for calculation of descriptive statistics using frequencies and percentages. Not all respondents answered every question. Due to limited response rates for some professional groups, the requirements for inferential statistical analysis were not met. Interview data were analyzed using Braun and Clarke7 six-phase approach to thematic analysis, which involves: 1) Familiarizing yourself with the data; 2) Generating initial codes; 3) Searching for themes; 4) Reviewing themes; 5) Defining and naming themes; 6) Producing the report. A team of three researchers coded the transcripts and searched for initial themes. They then reviewed these with the lead researcher and finalized the themes and sub-themes. Saturation was reached as analysis was completed, with the themes providing a comprehensive picture of the participants’ collective experiences, whilst also highlighting any differences between professions.
Ethical Issues
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from London South Bank University School of Health and Social Care Ethics Panel (HSCSEP17/20). Informed consent was inferred from the completed online questionnaires in Phase 1 and informed consent was obtained by the lead researcher prior to conducting the Phase 2 interviews. Informed consent included consent to publish quotes from participants. Participants were reminded of their right to withdraw and to ask any questions. All identifying information from the interview transcripts were removed or changed and participants are identified only by participant number. All data were stored on LSBU servers with password protected access. All data were managed in accordance with the University’s Code of Practice.
Results/Findings
The survey results gave a comprehensive overview of AHPs in ACP roles across London.
Geographical Location of Work and Healthcare Sector
There was a good spread of respondents from across primary and secondary NHS care, both acute and mental health, across London. A few respondents worked in other sectors, such as charity or private. The most common areas of work were Primary Care NHS (39%; n=49).
Current Post and Employment
Most respondents were appointed through either internal promotion (32%; n=47) or an externally advertised post (44%; n=64). They were most commonly employed at a senior level (band 8A Agenda for Change: 33%; n=42) but there were large variations across professional groups. Respondents worked in teams with a range of AHP skill mix levels. Role titles varied greatly and only 19% (n=24) respondents had titles that included “advanced”; a further 7% (n=9) had titles including “consultant”, which infers advanced practice. Respondents had been in their posts from <1 year to 15 years; the largest proportion had been in post 1–5 years (n=69; 57%). Respondents considered that they are always (24%; n=30) or frequently (60%; n=76) valued within their organisations.
Education and Preparation for Role
Eighty-eight (69%) respondents stated that it was a requirement to hold a further qualification (in addition to their registered qualification) for their current ACP position but this varied between professions. The types and levels of qualification that respondents held also varied, though post-graduate or master’s level was most likely. Most respondents considered that education/training adequately prepared them for their ACP role (74%; n=94). The respondents always (30%; n=38) or frequently (46%; n=57) considered their employers encouraged them to undertake further education and most had knowledge of funding sources available. Many respondents commented that, in addition to qualifications and education, experience was what had made them eligible for an ACP post.
The Domains of Advanced Practice and Scope of Practice
Respondents were asked how frequently they worked within each of the ACP domains: research/audit/service evaluation; clinical; education; management/leadership (see Table 1). The strong clinical focus of the roles was demonstrated by 73% (n=87) respondents working clinically on a daily basis, and a further 23% (n=27) worked clinically weekly. Just two respondents never worked clinically. In the other domains, respondents were much more likely to work weekly or monthly; fewer worked in these domains daily.
 |
Table 1 Frequency of Practice in the Domains of Advanced Clinical Practice |
Recognition, Confidence and Job Satisfaction
Most respondents considered it very important that they are recognized as ACPs (n=74; 58%), with only four respondents considering it not at all important. As regards their confidence in the ACP domains, there was variability (see Table 2). For example, in the clinical practice domain, there were high levels of confidence with 67% (n=80) who always felt confident; nearly all other respondents frequently felt confident (32%; n=38). However, in the research/audit/service evaluation domain, only 22% (n=26) always felt confident.
 |
Table 2 Confidence in the Domains of Clinical Practice |
The respondents were somewhat satisfied (51%; n=64) or satisfied (33%; n=41) with their roles, with 9% (n=11) being somewhat dissatisfied and one respondent feeling very dissatisfied with the role.
Interview Findings
Table 3 sets out the four themes, with sub-themes and numbers of participants contributing to each.
 |
Table 3 Themes and Sub-Themes with Participant Numbers |
Theme 1: Being Advanced
There are two sub-themes: expert practice, teamworking and collaboration.
Expert Practice
Expert practice comprised confident and autonomous practice, leadership, specialist clinical skills and expert decision-making. Participants identified that an important component of expert practice was the acquisition of specialist skills and experience in a specific area of practice:
If you were going down the advanced practitioner route, it would normally be for one part of the job, specifically: so, whether it be film reading, whether it be ultrasound or stereos. (P12, Diagnostic radiographer)
These specialist skills enabled the ACPs to work with complexity and to reason at an advanced level:
I’m able to conduct some complex patient assessment and make clinical decisions about onward referral or management or urgent referral for suspected serious illnesses. (P3, physiotherapist)
The ACPs led clinics, diagnosed and designed care pathways, with their roles crossing boundaries, whilst retaining their professional identity. Their autonomy enabled them to lead services, with ‘the freedom to manage the service the way that we see fit. (P7, occupational therapist).
Teamworking and Collaboration
An important part of being advanced was the ACPs’ role within the wider team, which included supporting more junior staff and collaboration. Teamworking also contributed to governance: ensuring the quality and safety of their practice. Many ACPs had a role in supporting junior staff:
I’m one of the senior members of staff in the team and I provide support and supervision to the junior members of the staff. (P9, drama therapist)
APs were able to role model, mentor and support others to realise their full potential:
As an advanced practitioner, we are expected to mentor and support and provide training for our physiotherapy colleagues. So we do a lot of coaching with them and even the new grads that come in sit in and watch clinics. (P13, physiotherapist)
Theme 2: Career Pathways
The interviews highlighted the diversity within the participants’ roles, titles, career opportunities and development. There were three sub-themes: routes to the advanced clinical practitioner role, education and training for the role, job titles and remuneration.
Routes to the Advanced Clinical Practitioner Role
Some participants described structured pathways to the role while for others, the posts evolved within their organisations. Progression to ACP was not an easy route for the drama therapist for various reasons: a lack of posts in the service, how others perceived the role, and the opportunity to use transferable skills in senior positions. Some participants described elements of “grow your own” with advanced roles reflecting the needs of the service and staff being flexible and responsive to service needs. Support from management was also important. Participants identified that training needed to be relevant to the roles and integrate clinical skills, management and research.
The importance of ensuring development of the necessary skills and establishing a framework or standards for the ACP role was identified:
I think there definitely needs to be time to develop these people, it can’t be done in a rush, and I think there needs to be standards and I think the standards need to be measured, need to be quite clear […] people in a way, at the moment, are pushing these roles without any specific standards or framework. (P3, physiotherapist)
Education and Training for the Role
Participants identified that training needed to be relevant to the roles and integrate clinical skills, management and research. There was however variation in how the participants developed in skills, knowledge and career opportunities. Budgets and workload affected opportunities for training and development, including funding for courses (P11, physiotherapist). Some discussed academic routes such as PhD or MSc programmes, while others discussed advanced clinical skills related to their profession which enabled them to become ACPs:
I’ve done post-grad training for different aspects of my work: so it might be vascular, it might be cardiac: whatever. (P12, radiographer)
Participants recognised the value of leadership development for the role, work-based learning and also joining professional networks:
I definitely recommend just joining a professional network, and being part of the committee, contributing, not just being passive but being active in being involved. (P3, physiotherapist)
Job Titles and Remuneration
The participants had a range of titles, which could affect salary and potentially impact on the public’s understanding and acceptance of the role. Some participants explained how they had removed the additional titles because they were not understood by service users, leading to confusion, for example:
the general public don’t know what an extended scope practitioner is, which is what I was first called, it means nothing, and they don’t really know what an advanced clinical practitioner is either. (P11, physiotherapist)
Participants discussed that there was diversity in their pay, even where roles and skills sets were similar, which affected their ability to change roles or work in other organisations.
Theme 3: Outcomes of the Advanced Clinical Practice Role
There were two sub-themes: benefits for direct patient care, measuring outcomes of the advanced clinical practitioner role.
Benefits for Direct Patient Care
The ACPs described a range of benefits. For example, they could ensure patients got the right advice at an early stage in their journey, offering a wider range of strategies, focused on individual needs:
We look at the effectiveness on their quality of life and we can start engaging the patient in self-management and looking at other strategies than just taking medication at a really early point, rather than the consultants who might rationalise the medication to some extent but don’t really offer the patient any alternative. (P8, physiotherapist)
An ACP who can prevent the patient being referred to multiple services or professionals potentially has real financial benefit as well as enhancing the patient experience. In addition, ACPs were taking on work that was traditionally the province of consultant doctors and reducing their workload:
If I’m not there, the workload would be increased for the consultants. That would be the difference. (P10, diagnostic radiographer)
The ACP role was seen as cost effective.
generally access to our services is quicker than the consultants as well, and less expense for commissioners that want to save money. (P13, physiotherapist)
Measuring Outcomes of the Advanced Clinical Practitioner Role
Most participants recognised the importance of measuring the outcomes associated with their role:
I think data is very important and I think any therapist who doesn’t keep data is a fool really, because at some point you’re going to have to prove your worth. (P11, physiotherapist)
Some participants were routinely measuring outcomes through audit and were able to measure the growth of their role within a service over time. However, in some services, establishing a baseline to measure from was not straight forward because of the complexity of patients and service provision:
We have mapped out some patient journeys and realised how incredibly complex it is, so in terms of patient outcomes we really struggle to capture it […] it just appears to be too complex for this system that we’re running to really know if whether they see a physio or whether they see a doctor has an impact on waiting lists. (P8 physiotherapist)
Sometimes the qualitative outcomes could be as valuable, or more valuable, than the quantitative ones:
When people are discharged from the service or moved on to something else, we ask for some feedback and it tends to be, rather than a tick box exercise, we ask for specific things like what’s been helpful and what hasn’t, and we do get quite a lot of really insightful feedback. (P2 occupational therapist)
Theme 4: Influencing and Transforming
There are two sub-themes: quality improvement and service developments, research and education.
Quality Improvements and Service Developments
Participants’ ideas to further develop services highlighted their energy, ideas and commitment to innovation, influencing and transforming services:
So we’re trying to design it so that it looks at structure, process and outcome across seven factors, so accessibility, sustainability, safety, client centeredness and how you can ensure that your service is meeting particular standards under those headings. We can’t predict an outcome but we can certainly set up a service using the best evidence. (P7, occupational therapist)
The different parts of the role (clinical, teaching, management and research) put the participants in a strong position to influence and change. They identified that there needed to be more working across sectors and services to fill current gaps in service provision.
Participant 6 (paramedic) shared ideas about developing the paramedic role and placing them in GP practices, which would be cost effective as patients are:
not being dealt with by the doctor, they’re being dealt with by paramedics who are used to going out to these patients anyhow, and it just moves some of the finances across to make it viable. (P6, paramedic)
Another participant also suggested how the ACP role in primary care, could be implemented more effectively through service redesign:
So I don’t think musculoskeletal patients need to see a GP – full stop. I think, if they come in with a back pain, I think they should be on a physio practitioner list. And I think the investment should be putting the physio practitioner in the GP practices. I think you would save an enormous amount of money: it would be a considerable reduction in secondary care referrals and also into primary care. (P4 physiotherapist)
Research and Education
Participants shared both the research work they were involved in and the design and development of educational programmes and services, for example:
I’ve also written up protocols, referral pathways and, also, manuals for training as well. (P10, radiographer)
Participant 14 (Art Therapist) outlined the development of a new course on Arts in Health for assistant practitioners, thus demonstrating development for different levels in the workplace. Some participants were writing for publication, some were engaged in audit projects and others were undertaking scoping studies and grant applications, including for doctoral studies:
I ran a small, local scoping study; I used that data to populate some grant applications. I got a doctoral fellowship from NIHR, as a clinical academic, conducted the study over four years and submitted the thesis. (P5, physiotherapist)
Discussion
This mixed method survey of ACPs in the allied health professions appears to be the first of its kind, providing a detailed profile of these roles and how they align with health policy and address current and future challenges in service delivery. The survey was based in London only but the results nevertheless provide a base line of these roles and their contribution in one area.
Through identifying core capabilities for ACPs, HEE3 established that the roles include clinical practice, leadership and management, education, and research, while acknowledging that the capabilities may be applied in different ways in different professions. In this survey, respondents confirmed the strong clinical practice focus of the roles. Most also worked within the other three domains, though less frequently; only a small proportion did not work in all domains. In a survey of UK radiographers who identified as advanced practitioners, the clinical practice role also dominated and most conducted research or service development; however, only just over half had a leadership role and just a fifth in education.8 However, it is possible that responses to both surveys might have been influenced by interpretations of these domains. For example, ACPs might have viewed working in education as being about formal teaching, and indeed Milner and Snaith8 referred to “expert education”. However, the HEE3 core capabilities for the education domain are much broader, including the ACP engaging in self-directed learning, enabling health literacy for service users, and supporting learning within their team while supporting an organizational learning culture. The interview participants gave rich examples of their roles in educational support, including mentoring and clinical supervision activities, which align with the HEE3 core capabilities for education. Overall, it is clearly important to establish a common understanding of what each of the domains for advanced clinical practice mean, as well as ensuring these are reflected in job descriptions and supported in practice.
The study results highlighted a lack of standardization in ACP roles, titles, career opportunities and development. Within nursing, where ACP roles have been implemented for many years, international studies continue to reveal variation in requirements for ACPs and a lack of role clarity.9–12 Previous studies have also highlighted the plethora of titles in use in AHP ACP roles8,13,14 and for nursing ACP roles too.15,16 HEE3 acknowledged the range of titles used and the confusion caused, but further raised that some posts with “advanced” in the title may not actually meet the criteria for ACP roles, thus highlighting a further issue to be addressed.
The importance of expert clinical practice in the ACP role has been identified in both dietetics17 and radiography.18 Interview participants discussed the leadership aspect of the ACP role, providing examples of how they applied leadership skills in service developments. In dietetics, Palermo et al19 identified leadership and influencing others, rather than specialist practice skills, as being the essential core of advanced practice. However, the HEE3 framework does not prioritize one part of the role over another but the capabilities for research, leadership and management, and education, are all applied to clinical practice too. The ACPs also discussed their skills in working with others in a team, collaboration with other professionals and across sectors, quality improvement, and mentoring and supervising colleagues. Whilst the ACPs applied their skills to crossing boundaries, they also considered that their professional specialty was an essential attribute that they needed to retain.
During the interviews, ACPs described the new models of care they were delivering. For example, in physiotherapy, ACPs described providing a “one-stop shop” for patients, who could see just one practitioner who offered a holistic approach with different strategies, rather than experiencing repeated appointments with different professionals. The ACPs identified that preventing patients being referred to multiple services or professionals has potential financial benefits as well as enhancing the patient experience. The international physiotherapy literature provides many examples of ACPs delivering new models of care, particularly in musculoskeletal services, and across different settings, including emergency, primary and secondary care.20–27 Many of these examples involved the physiotherapy ACPs assessing and treating patients for musculoskeletal conditions, instead of medical practitioners, both in routine clinics and emergency care. These models consistently evaluate well, providing not only an equivalent quality but also additional benefits, such as increased accessibility and wider range of strategies. While many of these examples come from the United States, some are from Ireland, Canada or Australia, where health systems are more similar to the UK. Outside physiotherapy, Bowles et al28 explained how paramedics are increasingly taking on varied operational roles to improve patient care and address gaps in an evolving and pressurised healthcare system. Similarly, ACPs in nursing have demonstrated comparable outcomes with medical practitioners, for example, in out of hours primary care29, emergency care30,31 and neurology.32
During interviews, the ACPs discussed the importance of measuring outcomes from the new models of care but they explained that, due to the complexity of patient pathways and interprofessional working, measuring direct impact of the ACP role within the services could be challenging. These experiences mirror findings from a review of advanced nursing practice, which revealed continued difficulties associated with accurate measurement of the impact of ACP roles on patient outcomes.33 HEE3 framework recommends that organisations implementing ACP roles need to identify the intended outcomes and how these will be measured, during preparation for the new roles.
The embedding of ACP roles in some professions places them in a good position to contribute to pathway reconfigurations and new models of care. However, art and drama therapist AP posts were few and the skills they could offer were not always recognized or understood by other professions, thus affecting opportunities to progress either in the service or elsewhere.
Lack of standardization in educational preparation for ACP roles has been previously highlighted in various professions, including podiatry,14 paramedics34 and nursing.35 The HEE3 definition of advanced clinical practice includes that the role is underpinned by a master’s level qualification or equivalent. Most survey respondents stated that it was a requirement to hold an additional qualification (in addition to their registered qualification) for their ACP position but types of qualification varied considerably.
Ongoing education within the role is also important, particularly so that ACPs can contribute to new and evolving pathway developments. While the majority of survey respondents had employers who were supportive to further education, around a quarter were not encouraged. During interviews, ACPs discussed the impact that budgets and workload had on opportunities for training and development, including funding for courses. In a previous study in physiotherapy, ACPs were found to be committed to further training and there were positive experiences reported, though opportunities varied.25 Similarly, in a study in radiography, barriers to implementation of ACP roles included funding and backfill for training.36 Within nursing, the availability of education has been identified as an enabler for the ACP role.37,38 Survey respondents also highlighted the importance of experience, as preparation for their ACP role. Therefore, the need for substantial experience during the career pathway to ACP roles also needs acknowledging.
During interviews, ACPs expressed that training needed to be relevant to the roles and integrate clinical skills, leadership and management, and research; these align with the domains of advanced practice, though preparation for education was not raised. There was a suggestion for a framework or standards for the ACP role, and this could promote standardization. The HEE3 aims that the core capabilities framework will meet this gap, though there will still need to be application to specific professions. As an example of individual professions taking advanced practice education forward, Crouch and Brown39 reported on the development of a UK-wide curriculum for emergency care ACPs.
Based on the study results, recommendations include a standardized and coherent approach to AHP ACP career pathways, in particular those less well known such as drama and music therapy. It is important to promote understanding of ACP roles across the workforce and the public and ensure clarity about the role and titles that reflect both professional identity and advanced practice, with consistency across professions. To ensure sustainability of AHP ACPs, roles and new models of care, succession planning should be addressed and service reconfiguration should robustly be evaluated. Further research could include investigations across professional and geographical boundaries to examine how the core capabilities of advanced practice apply within these professions.
Conclusion
ACP roles within the allied health professions can help address the challenges faced across healthcare services globally. This project resulted in a comprehensive profile of AHP ACPs across London, illuminating the nature of their roles and how they are already delivering on new models of care. Furthermore, the ACPs could identify the potential for new models of care that could utilize these roles more effectively. However, there needs to be a consistent infrastructure, standardization and governance for ACP roles across sectors, along with career pathways, funding, sustainability and educational provision.
Acknowledgments
The authors would like to thank all Advanced Clinical Practitioner (ACP) participants for their valuable contributions during the survey and interviews.
Health Education England for Funding the Project.
North Central East London Allied Health Professions Network group for the project initiation and networking opportunities.
Mr. David Marston (Senior Strategic Programs, Planning and Performance Manager, Health Education England) for his role in initiating the project and contributions to the survey development.
Dr Lesley Baillie (Visiting Professor, LSBU) for finalizing the report.
All steering group members.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This project was funded by Health Education England.
Disclosure
Adéle Stewart-Lord reports grants from HEE, during the conduct of the study. Shani Shamah reports her involvement with the People's Academy at London South Bank University at the time of the project. The authors report no other potential conflicts of interest for this work.
References
1. NHS England. Five Year Forward view. 2014 Available from: https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf.
2. NHS England. Delivering the Five Year Forward View. 2015. Available from: https://www.england.nhs.uk/wp-content/uploads/2015/12/planning-guid-16-17-20-21.pdf.
3. Health Education England. Multi-professional framework for advanced clinical practice in England. 2017. Available from: https://www.hee.nhs.uk/our-work/advanced-clinical-practice/multi-professional-framework.
4. NHS England. Allied Health Professionals into Action: using allied health Professionals to transform health, care and well-being. 2017. Available from: https://www.england.nhs.uk/wp-content/uploads/2017/01/ahp-action-transform-hlth.pdf.
5. Boynton P, Greenhalgh T. Selecting, designing, and developing your questionnaire. Br Med J. 2004;328(7451):1312–1315. doi:10.1136/bmj.328.7451.1312
6. Oppenheim AN. Questionnaire Design, Interviewing and Attitude Measurement.
7. Braun V, Clark V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
8. Milner RC, Snaith B. Are reporting radiographers fulfilling the role of advanced practitioner? Radiography. 2017;23:48–54. doi:10.1016/j.radi.2016.09.001
9. King R, Tod A, Sanders T. Development and regulation of advanced nurse practitioners in the UK and internationally. Nurs Standard. 2017;32(14):43–50.
10. Casey M, O’Connor L, Cashin A, et al. Enablers and challenges to advanced nursing and midwifery practice roles. J Nurs Manag. 2019;27(2):271–277. doi:10.1111/jonm.12697
11. Halliday S, Hunter DJ, McMillan L. Ward staff perceptions of the role of the advanced nurse practitioner in a ‘hospital at day’ setting. Br J Nurs. 2018;27(2):92–97. doi:10.12968/bjon.2018.27.2.92
12. Heale R, Rieck Buckley C. An international perspective of advanced practice nursing regulation. Int Nurs Rev. 2016;2015(62):421–429.
13. Nightingale J, Hardy M, Snaith B. Embedding consultant radiographer roles within radiology departments: a framework for success. Radiography. 2018;24(4):289–297. doi:10.1016/j.radi.2018.06.007
14. Stuart L, McInnes A. Diabetes specialist podiatrists in the UK: ensuring a competent, adequate workforce. Diabetic Foot J. 2011;14(3):102–106.
15. Gardner G, Duffield C, Doubrovsky A, Adams M. Identifying advanced practice: a national survey of a nursing workforce. Int J Nurs Stud. 2016;55:60–70. doi:10.1016/j.ijnurstu.2015.12.001
16. Newall F, Twomey B, Lima S. Advanced practice nursing–Promoting organisation clarity and connectedness: a mixed methods approach. Collegian. 2018;25:97–103. doi:10.1016/j.colegn.2017.04.003
17. Brody RA, Byham-Gray L, Touger-Decker R, et al. What clinical activities do advanced-practice registered dietitian nutritionists perform? Results of a Delphi study. J Acad Nutr Diet. 2014;114(5):718–733. doi:10.1016/j.jand.2014.01.013
18. Thom SE. Does advanced practice in radiography benefit the healthcare system? A literature review. Radiography. 2018;24(1):84–89. doi:10.1016/j.radi.2017.08.002
19. Palermo C, Capra S, Beck EJ, Dart J, Conway J, Ash S. Development of advanced practice competency standards for dietetics in Australia. Nutr Diet. 2017;74(4):327–333. doi:10.1111/1747-0080.12338
20. Desmeules F, Toliopoulos P, Roy JS, et al. Validation of an advanced practice physiotherapy model of care in an orthopaedic outpatient clinic. BMC Musculoskelet Disord. 2013;14:162. doi:10.1186/1471-2474-14-162
21. Ó Mír M, O’Sullivan C. Advanced practice physiotherapy in paediatric orthopaedics: innovation and collaboration to improve service delivery. Irish J Med Sci. 2018;187(1):131–140. doi:10.1007/s11845-017-1611-2
22. Sayer JM, Kinsella RM, Cary BA, Burge AT, Kimmel LA, Harding P. Advanced musculoskeletal physiotherapists are effective and safe in managing patients with acute low back pain presenting to emergency departments. Aust Health Rev. 2018;42(3):321–326. doi:10.1071/AH16211
23. Hurtubise K, Shanks R, Benard L. The design, implementation, and evaluation of a physiotherapist-led clinic for orthopedic surveillance for children with cerebral palsy. Phys Occup Ther Pediatr. 2017;37(4):399–413. doi:10.1080/01942638.2017.1280869
24. Fennelly O, Blake C, Desmeules F, Stokes D, Cunningham C. Patient‐reported outcome measures in advanced musculoskeletal physiotherapy practice: a systematic review. Musculoskel Care. 2018;16(1):188–208.
25. Fennelly O, Blake C, FitzGerald O, et al. Advanced musculoskeletal physiotherapy practice in Ireland: a National Survey. Musculoskel Care. 2018;1557–1681.
26. Chang AT, Gavaghan B, O’Leary S, McBride L-J, Raymer M. Do patients discharged from advanced practice physiotherapy-led clinics re-present to specialist medical services? Aust Health Rev. 2018;42(3):334–339. doi:10.1071/AH16222
27. Kinsella R, Collins T, Shaw B, et al. Management of patients brought in by ambulance to the emergency department: role of the advanced musculoskeletal physiotherapist. Aust Health Rev. 2018;42(3):309–315. doi:10.1071/AH16094
28. Bowles RR, van Beek C, Anderson GS. Four dimensions of paramedic practice in Canada: defining and describing the profession. AJP. 2017;14(3):1–11.
29. Collins D. Assessing the effectiveness of advanced nurse practitioners undertaking home visits in an out of hours urgent primary care service in England. J Nurs Manag. 2019;27:450–458. doi:10.1111/jonm.12680
30. Griffin M, McDevitt J. an evaluation of the quality and patient satisfaction with an advanced nurse practitioner service in the emergency department. J Nurse Pract. 2016;12(8):553–559. doi:10.1016/j.nurpra.2016.05.024
31. Woo BJY, Jasmine Xin Yu Lee JXL, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: a systematic review. Hum Resour Health. 2017;15:63. doi:10.1186/s12960-017-0237-9
32. Leahy T, Counihan TJ. Physician and advanced nurse practitioner decision-making in the management of multiple sclerosis. Br J Neurosci Nurs. 2018;14(5):240–248. doi:10.12968/bjnn.2018.14.5.240
33. Casey M, O’Connor L, Cashin A, et al. An overview of the outcomes and impact of specialist and advanced nursing and midwifery practice, on quality of care, cost and access to services: a narrative review. Nurse Educ Today. 2017;56:35–40. doi:10.1016/j.nedt.2017.06.004
34. Halter M, Ellison G Evaluation of the Emergency Care Practitioner Role in London: a study of the processes and outcomes of clinical decision-making. London: Faculty of Health and Social Care Sciences, University of London. 2008. Available from: https://core.ac.uk/download/pdf/90501.pdf.
35. King R, Tod A, Sanders T. Development and regulation of advanced nurse practitioners in the UK and internationally. Nurs Standard. 2017;32(14):43–50. doi:10.7748/ns.2017.e10858
36. Henderson I, Mathers SA, McConnell J, Minnoch D. Advanced and extended scope practice of radiographers: the Scottish perspective. Radiography. 2016;22(2):185–193. doi:10.1016/j.radi.2015.12.002
37. Fealy GM, Casey M, O’Leary DF, et al.Developing and sustaining specialist and advanced practice roles in nursing and midwifery: a discourse on enablers and barriers. J Clin Nurs. 2018;27:3797–3809. doi:10.1111/jocn.14550
38. Wisur-Hokkanen C, Glasberg A-L, Mäkelä C, Fagerström L. Experiences of working as an advanced practice nurse in Finland – the substance of advanced nursing practice and promoting and inhibiting factors. Scand J Caring Sci. 2015;29:793–802. doi:10.1111/scs.12211
39. Crouch R, Brown R. Advanced clinical practitioners in emergency care: past, present and future. Brit J Hosp Med. 2018;79(9):511–515. doi:10.12968/hmed.2018.79.9.511
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.