Back to Journals » Research and Reports in Urology » Volume 18
The Robosling Technique in Robotic Radical Prostatectomy Promotes Early and Sustained Return of Continence in Elderly Patients
Authors Yu V ![]() , Gibson D
, Gibson D ![]() , Cotte J, Amin A, Chan L, Ahmadi N, Jeffery N, Thanigasalam R, Leslie S
, Cotte J, Amin A, Chan L, Ahmadi N, Jeffery N, Thanigasalam R, Leslie S
Received 10 February 2026
Accepted for publication 5 March 2026
Published 2 July 2026 Volume 2026:18 599921
DOI https://doi.org/10.2147/RRU.S599921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Guglielmo Mantica
Victor Yu,1-3,* Damien Gibson,1-3,* Juliette Cotte,1-4 Amer Amin,1-3 Lewis Chan,5 Nariman Ahmadi,4,5 Nicola Jeffery,1 Ruban Thanigasalam,2,4-6 Scott Leslie,1-5
1Department of Urology, Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 2Institute of Academic Surgery, Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 3Surgical Outcomes Research Centre (SOuRCe), Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 4Department of Uro-Oncology, Chris O’Brien Lifehouse, Camperdown, NSW, Australia; 5Department of Urology, Concord Repatriation General Hospital, Concord, NSW, Australia; 6Faculty of Health and Medicine, Central Clinical School, The University of Sydney, Camperdown, NSW, Australia
*These authors contributed equally to this work
Correspondence: Victor Yu, Department of Urology, Royal Prince Alfred Hospital, Missenden Road, Camperdown, Sydney, 2050, Australia, Email [email protected]
Aim: The Robosling technique is a novel autologous fascial sling which supports the urethrovesical anastomosis in robotic radical prostatectomy (RARP) and has shown promise in improving early continence. Although curative surgery for prostate cancer is uncommonly offered to elderly patients aged ≥ 75, increase in active surveillance and overall life expectancy challenges this paradigm, though continence remains a challenge in this cohort. We sought to investigate the role of the Robosling technique in elderly patients to promote early return of continence.
Methods: Our prospective RARP database (2016– 2023) was analysed, recording demographic, surgical, pathological and functional outcomes. The primary endpoint was defined as pad-free continence, 1-year post-operatively. Patients aged ≥ 75 undergoing RARP with or without Robosling were compared using Chi-square/Fisher-exact and t-tests with p< 0.05 considered significant. Multinomial logistic regression was performed to account for confounders.
Results: 62 patients were included in the analysis (Robosling n=24). No significant differences were detected in surgical or pathological outcomes. Robosling was associated with improved pad-free continence rates from 6-months post-operatively (62.5% vs 30.0%, p=0.018) and sustained at 1-year (79.2% vs 30.0%, p< 0.01). Mean pad-use was lower in the Robosling cohort at all time points (0.21 vs 1.0 pads at 1-year, p< 0.05). On multivariate analysis, Robosling remained independently associated with improved pad-free continence (OR 0.11, 95% CI 0.03– 0.37, p< 0.001).
Conclusion: The Robosling technique is associated with significantly improved early and sustained pad-free continence rates in the elderly population in this single-surgeon study. While patient selection remains paramount, this intraoperative technique may mitigate a key quality-of-life concern in this cohort.
Keywords: prostate cancer, prostatectomy, elderly, procedure, robotic surgical, treatment outcome, urinary incontinence
Introduction
Curative surgery is uncommonly offered to elderly patients aged 75 and over for localised prostate cancer as traditionally, the survival benefits from a usually indolent disease are not considered to outweigh the significant adverse effects to quality-of-life following surgery.1 However, increasing overall life expectancy and advances in technical aspects of robotic-assisted radical prostatectomy (RARP) have challenged this paradigm.
Reported quality-of-life outcomes following RARP, particularly continence, have yielded discordant results, owing to differences in techniques, patient selection and inconsistencies in definition. However, cohorts examining elderly patients have consistently revealed higher rates of incontinence. Gondoputro et al reported only half of patients ≥75 years having pad-free continence 1-year post-operatively, significantly lower when compared with matched younger counterparts.2 Similarly, Mandel et al report continence rates of 86.5%, utilising a definition of continence as one safety pad per day, compared with over 90% in patients <70 years.3 Reducing the burden of incontinence in these patients can, therefore, be considered the rate-limiting step in considering proceeding with RARP.
We had previously demonstrated the possibility of equivalency in surgical, oncological and functional outcomes in elderly patients, with findings suggesting aspects of the technique serving a role in continence preservation.4 The Robosling, the primary continence technique utilised in this study, is a vascularised sling fascial flap, anchored to the pectineal ligaments bilaterally, to support the urethrovesical anastomosis (Figure 1). Robosling has been demonstrated to provide both early and sustained continence post-RARP in a non-randomised, prospective cohort setting.5
 |
Figure 1 The Robosling technique: (A) peritoneum is dissected off the posterior detrusor, (B) tunnelled underneath the bladder, (C) incorporated into the Rocco stitch and (D) tensioned laterally to the pectineal ligament. |
The aim of this study was to assess the utility and efficacy of the Robosling technique in reducing the burden of incontinence in elderly patients undergoing RARP.
Subjects and Methods
Study Design and Setting
Consecutive patients treated by four surgeons with RARP for localised prostate cancer at our two centres (Royal Prince Alfred Hospital, Chris O’Brien Lifehouse) between October 2016 to December 2023 were considered for the study. Data was analysed retrospectively from a prospectively maintained database RARP patients are routinely enrolled in. We performed subgroup analysis of the elderly population (≥75 years) to compare whether the use of the Robosling technique was associated with improved early and sustained continence. Robosling was performed by one surgeon, whilst all surgeons contributed to the control cohort.
Technique
All patients in the study underwent RARP with the da Vinci surgical robot system (da Vinci Xi, Intuitive Surgical Incorporation, Sunnyvale, CA) with a transperitoneal anterior, six-port technique. Surgeon discretion was employed to determine indication for nerve-sparing, bladder neck reconstruction and pelvic lymph node dissection. The Rocco suture re-approximation of Denonvillier’s, posterior detrusor and posterior sphincter was routinely incorporated in the Robosling technique.
The Robosling technique utilises an autologous vascularised fascial flap of peritoneum, harvested from the posterior aspect of the bladder prior to mobilisation. A broad base is maintained to ensure vascularity (Figure 1A). Following the prostatectomy, lymph node dissection (where relevant) and haemostasis, the peritoneal flap is transferred under the bladder (Figure 1B) and incorporated into the rectourethralis and bladder neck using a 3–0 V-Loc suture as the Rocco suture (Medtronic®, Minneapolis, USA) (Figure 1C). After vesico-urethral anastomosis, the corners of the fascial sling are then suture tensioned to the inguinal ligament of Cooper using a 3–0 V-Loc suture and secured with two Hem-o-lok clips (Teleflex®, Philadelphia, USA) (Figure 1D). As these sutures are tensioned, the anastomosis, posterior detrusor and sphincter are lifted upwards.
Variables and Study Outcomes
Patients were analysed for baseline demographic (age, body mass index [BMI], prostate-specific antigen [PSA], prostate volume), pathological (ISUP [International Society of Urological Pathology] Grade Group on biopsy, pathological T-score, positive surgical margin, pelvic lymph node dissection) and technical variables (bladder neck reconstruction, nerve sparing status, Robosling, use of Rocco suture).
Post-operatively, patients were followed up routinely at 6 weeks, 3, 6 and 12 months. The primary endpoint was complete continence at 1-year measured as zero-use of incontinence safety pads per 24-hours. Secondary endpoints included absolute number of incontinence pads per day, total operating time (min), blood loss (mL), 30-day complication rate (Clavien-Dindo classification I–IIIa/IIIb-IV), biochemical recurrence at 1-year (defined as PSA > 0.02ng/L).
Statistical Methods
Cohorts were compared with Chi-squared and Fisher-exact tests (categorical variables) and t-tests (continuous variables). Univariate logistic regression was performed to determine relationship between baseline and technical variables with pad-free continence at the 1-year endpoint. Variables with significant association on univariate analysis (p<0.1) were entered into a backward multivariate regression model to determine adjusted odds ratios (aOR) with p<0.05 considered statistically significant. Statistical analysis was performed using Statistical Package for Social Science (SPSS version 31.0, IBM, USA).
Ethics approval with a waiver of consent was approved for this manuscript by the institutional Human Research Ethics Committee (Sydney Local Health District Human Research Ethics Committee, approval number X23-0292). Waiver of consent was pursued due to the quantity of records and participation carrying no more than low risk. Patient confidentiality was maintained by de-identification of data. The study was conducted in accordance with the ethical principles stipulated by the Declaration of Helsinki.
Results
A total of 64 patients were included in the study (Robosling; n=24, control; n=40). Baseline demographic, intraoperative technical and pathological variables are compared in Table 1. Both cohorts displayed similar characteristics in terms of age, BMI, PSA and pathology although the Robosling group had an overall larger prostate volume (50.0 mL vs 29.3 mL, p=0.026) and fewer bladder neck reconstructions performed (0% vs 60%, p<0.001).
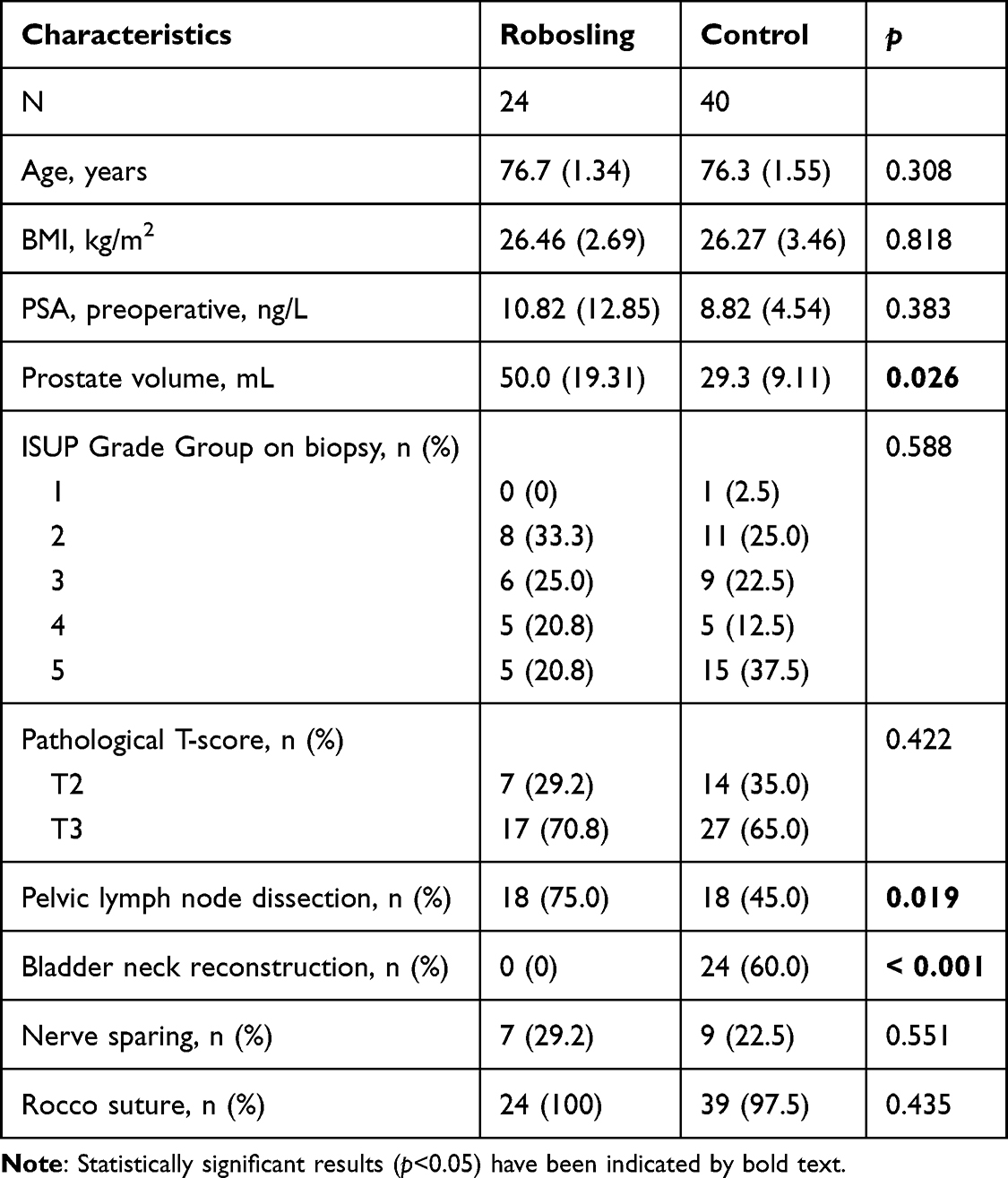 |
Table 1 Baseline Demographic, Intraoperative Technical and Pathological Variables Compared Between Cohorts |
Primary Outcomes
Overall, the Robosling cohort was associated with significantly improved pad-free continence at 1-year post-operatively (79.2% vs 30.0%, p<0.001), with results displayed in Table 2. Significant differences in proportion of patients who were pad-free were detected from 6-months post-operatively. Mean pad usage over 24 hours was lower in the Robosling cohort at all post-operative timepoints (6-weeks; 1.42 vs 2.15, p=0.021, 1-year; 0.21 vs 1.03 pads, p=0.002).
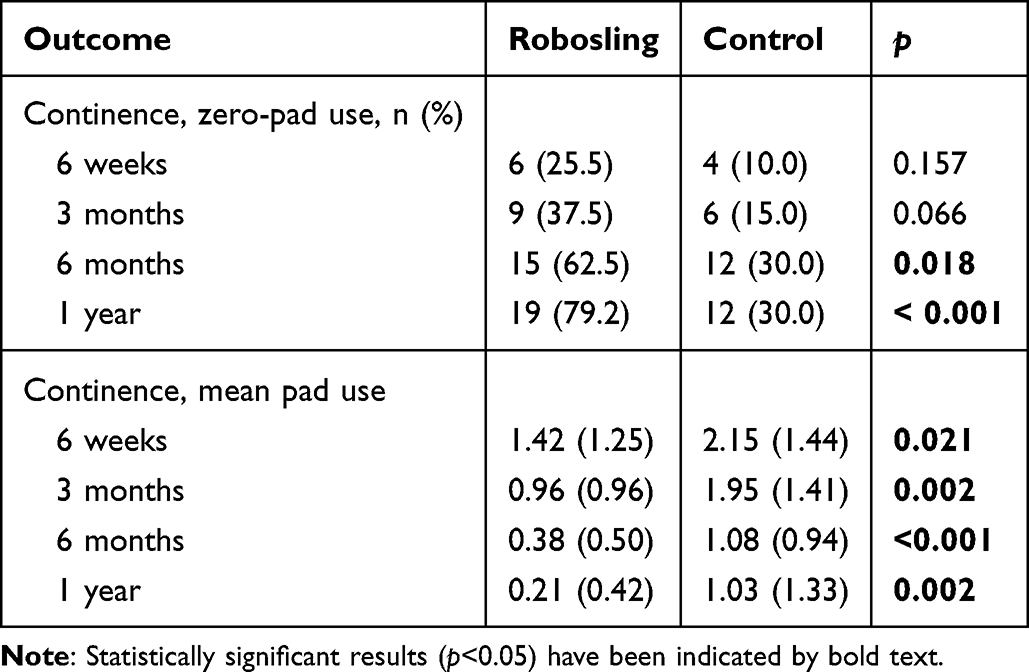 |
Table 2 Post-RARP Continence, Defined by Pad-Free Proportion and Pad-Use Rates Compared Between Cohorts |
Significant and relevant baseline demographic and technical characteristics of prostate volume, operating surgeon, nerve spare status, bladder neck reconstruction were included into the multivariate regression analysis to account for confounders (Table 3). Robosling was the only variable associated with pad-free continence at 1-year post-operatively (OR 0.11, 95% CI 0.03–0.37, p<0.001) on multivariable analysis.
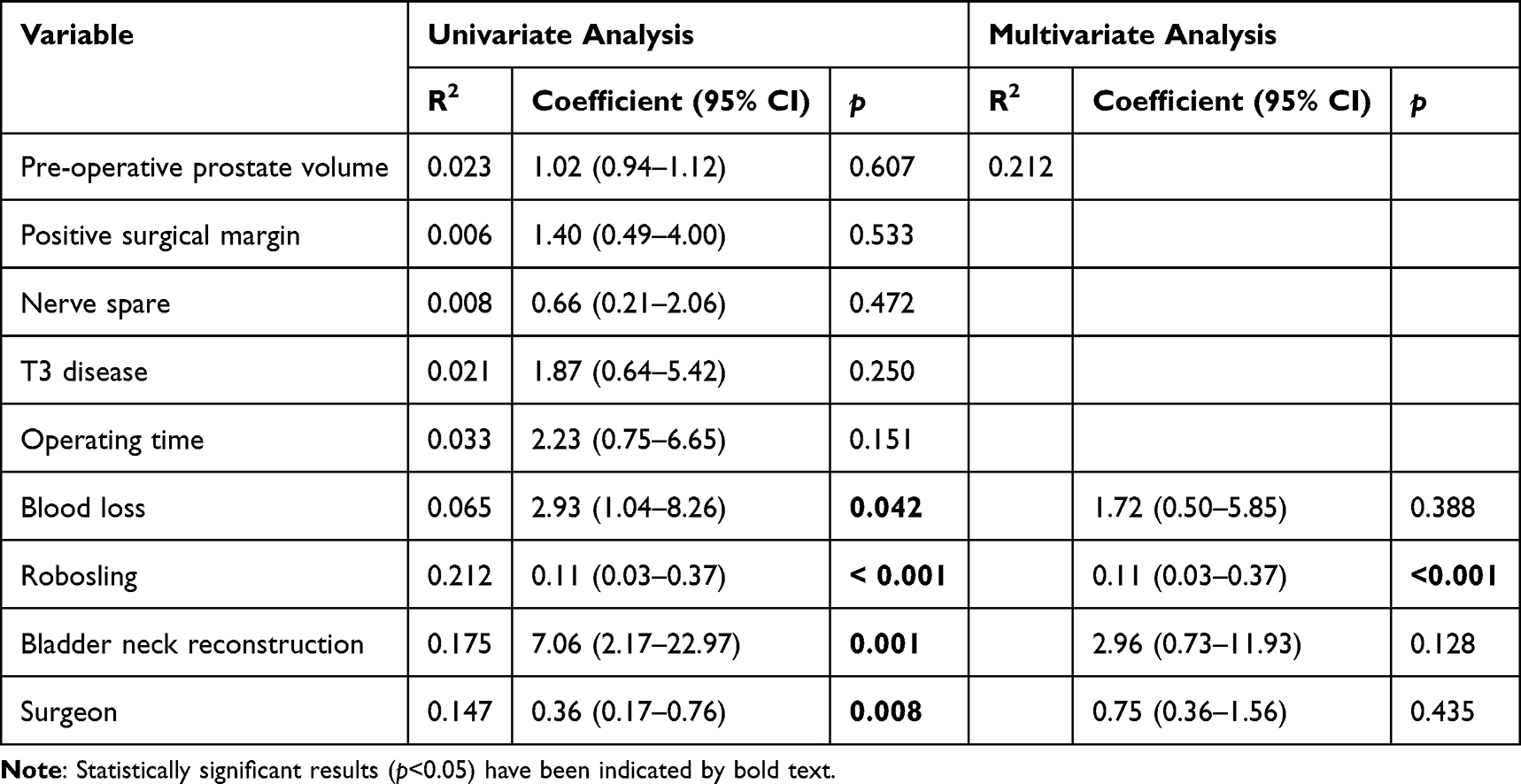 |
Table 3 Association Between Post-Operative Incontinence (Any Pad Usage) at 1-Year Post-Operatively with Baseline Characteristics from Logistic Regression Analysis |
Secondary Outcomes
Outcomes of surgical and oncological safety are summarised in Table 4. Operating time and blood loss were higher in the non-Robosling cohort. The non-Robosling cohort was also associated with increased overall length of stay (3.54 vs 2.32 days, p=0.007). Major complication (defined as Clavien-Dindo Grade III or higher) was higher in the Robosling cohort (8.3 vs 2.5%, p=0.551) but was not statistically significant as overall rates were low. No statistically significant differences were detected between the two cohorts in terms of surgical margin positivity (25% vs 37.5%, p=0.30) and biochemical (PSA) recurrence rates at 1-year post-operatively (8.3% vs 12.5%, p=0.48).
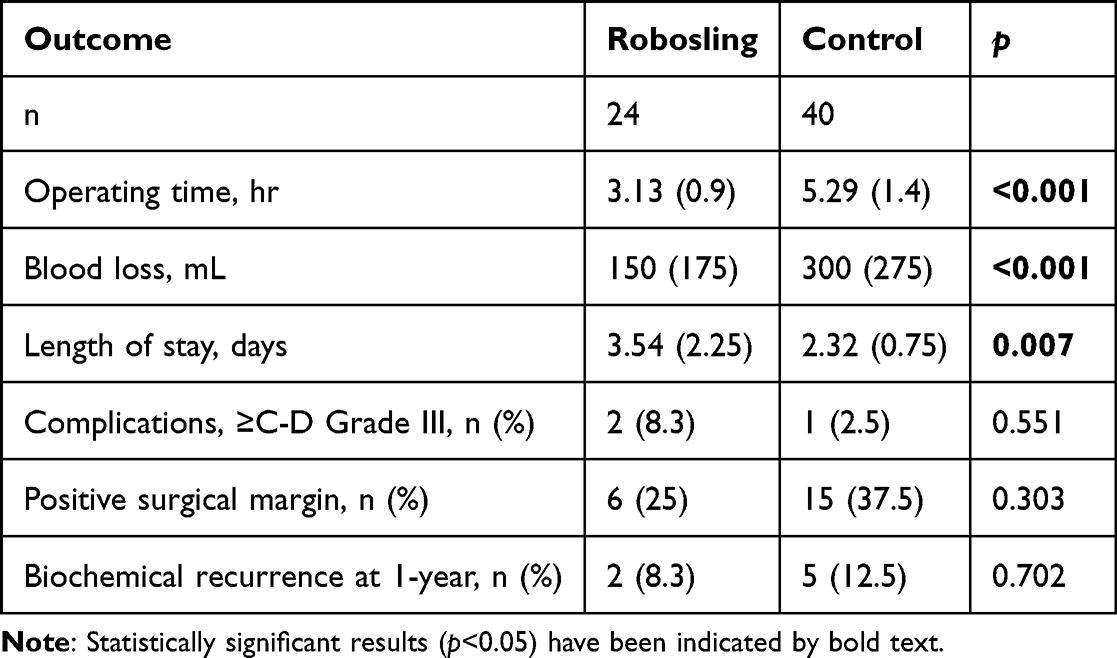 |
Table 4 Secondary Outcomes (Surgical and Pathological) Compared Between Cohorts |
Discussion
Our results demonstrate minor alterations to surgical technique can result in significant improvements in the short- and longer-term continence of elderly men undergoing RARP. The odds of incontinence requiring any pad use were nearly 90% lower following RARP with Robosling compared to without, accounting for covariates.
Importantly, we have demonstrated that this technique does not compromise on the primary objective of RARP in oncological safety, illustrated by the equivalence in surgical margin positivity and biochemical recurrence rates, at least in the short term. Disease severity in this study population was relatively high, with T3 or higher disease in around two-thirds of the patients in both cohorts (Robosling 70.8 vs control 65.0%, p=0.422). This is likely primarily a consequence of patient selection, given that most elderly men with low or intermediate risk prostate cancer may opt for surveillance or watchful waiting approaches to management.
From a technical standpoint, the Robosling technique has been demonstrated to have no significant repercussions to intraoperative complexity. Operating time is not meaningfully extended, with the step requiring an additional 16 min, on average to complete, with no significant differences detected in blood loss or complication rate in prior trials.5 The longer operating time and increased blood loss in our control cohort in this subgroup analysis is likely secondary to the proportion of patients who underwent bladder neck reconstruction; overall, neither factor showed association with continence endpoints.
Performing RARP in elderly men has been controversial, given that many patients may not have any significant survival benefits and risk severe impacts to quality-of-life. Therefore, the ability to maintain continence in this population, more than their younger counterparts, is of utmost importance. It has been traditionally suggested that elderly men are at higher risk of severe incontinence following radical prostatectomy,3 however the utilisation of RARP has been potentially shown to limit these adverse effects.6–9 The aetiology of post-prostatectomy incontinence is still poorly understood and almost certainly multifactorial, though a number of processes have been associated, including bladder denervation,10 loss of urethral length11 and damage to the native urinary sphincteric complex.12,13 Several hypotheses have been suggested to account for the differences that elderly men in particular face, which include loss of support structures around the male urethral complex14 and age-related atrophy of the rhabdosphincter.15 It is therefore logical that preservation or and attempt at reconstruction of native supportive structures would improve continence, and this has been shown in other techniques including the “Rocco stitch”.16
The paramount consideration in RARP in elderly men remains to be patient selection. Clearly, not every patient will derive benefit from operative intervention and meaningfully less so if the alternative is the potential for intractable incontinence. It is not within the scope of this study to guide this decision-making pathway, however, these results do offer promise in reducing the burden of morbidity associated with intervention and may therefore swing the balance in decision-making. Furthermore, trends in life expectancy and management of localised prostate cancer predict a growing proportion of elderly men pursuing active surveillance and eventual radical treatment,17 reinforcing the needs to address worse continence outcomes in this cohort following RARP.
The major limitation of this study is in its methodology as a non-randomised, retrospective, single-surgeon study. There is, therefore, significant risk of bias, particularly in the context of a control group with heterogeneity and results may not be generalisable until validated in a multi-surgeon and ideally randomised setting. Of note, surgeon discretion was utilised in terms of nerve-sparing, lymph node dissection and bladder neck reconstruction, which have debated impact on overall continence post-RARP. Rates of these differed between study and control cohorts and potentially significantly confound our results. We attempted to account for these factors, including surgeon experience with multivariate analysis, which demonstrated no significant association (OR 0.75, 95% CI 0.36–1.56, p=0.435), but ultimately this would not completely account for all confounders. Furthermore, our data did not assess other functional outcomes of this technique, including erectile function or other patient-reported quality-of-life metrics which play a significant role, particularly when considering RARP in elderly men. Overall, our results are in keeping with a prior prospective, non-randomised cohort study on Robosling, which demonstrated favourable continence outcomes in both objective and patient-reported measures.5
The Robosling technique is associated with significantly improved early and sustained pad-free continence rates in the elderly population in this single-surgeon retrospective study. While patient selection remains paramount, this intraoperative technique may mitigate a key quality-of-life concern in this cohort.
Abbreviations
ASA, American Society of Anaesthesiologists; BMI, Body mass index; OR, Odds ratio; PSA, Prostate-specific antigen; RARP, Robotic assisted radical prostatectomy.
Data Sharing Statement
De-identified data associated with this manuscript is available on request from the authors.
Ethics Statement
Waiver of consent was approved by local ethics board (Sydney Local Health District Huma Research Ethics Committee, approval number X23-0292). Patient data was de-identified to maintain confidentiality.
Funding
No funding was obtained for the production of this manuscript.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Cornford P, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer-2024 update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2024;86(2):148–8.
2. Gondoputro W, Thompson J, Evans M, et al. How does age affect urinary continence following robot-assisted radical prostatectomy? A prospective multi-institutional study using independently collected, validated questionnaires. J Urol. 2022;207(5):1048–1056.
3. Mandel P, Graefen M, Michl U, Huland H, Tilki D. The effect of age on functional outcomes after radical prostatectomy. Urol Oncol. 2015;33(5):203.e11–e18.
4. Yu V, Treacy P-J, Thanigasalam R, et al. Robotic-assisted radical prostatectomy in the elderly patient—a study of functional, surgical, and oncological outcomes in an australian cohort. Prostate. 2026;86(2):158–166.
5. Leslie S, Jackson S, Broe M, et al. Improved early and late continence following robot-assisted radical prostatectomy with concurrent bladder neck fascial sling (RoboSling). BJUI Compass. 2023;4(5):597–604.
6. Labanaris AP, Witt JH, Zugor V. Robotic-assisted radical prostatectomy in men ≥75 years of age. Surgical, oncological and functional outcomes. Anticancer Res. 2012;32(5):2085–2089.
7. Ubrig B, Boy A, Heiland M, Roosen A. Outcome of robotic radical prostatectomy in men over 74. J Endourol. 2018;32(2):106–110. doi:10.1089/end.2017.0512
8. Togashi K, Hatakeyama S, Okamoto T, et al. Oncologic and patient-reported outcomes after robot-assisted radical prostatectomy in men aged ≥75 years. Urol Oncol. 2021;39(10):729.e17–e25. doi:10.1016/j.urolonc.2020.12.001
9. Basto MY, Vidyasagar C, te Marvelde L, et al. Early urinary continence recovery after robot-assisted radical prostatectomy in older Australian men. BJU Int. 2014;114(Suppl 1):29–33. doi:10.1111/bju.12800
10. Egawa S, Minei S, Iwamura M, Uchida T, Koshiba K. Urinary continence following radical prostatectomy. Jpn J Clin Oncol. 1997;27(2):71–75.
11. Matsushita K, Kent MT, Vickers AJ, et al. Preoperative predictive model of recovery of urinary continence after radical prostatectomy. BJU Int. 2015;116(4):577–583.
12. Giannantoni A, Mearini E, Di Stasi SM, et al. Assessment of bladder and urethral sphincter function before and after radical retropubic prostatectomy. J Urol. 2004;171(4):1563–1566.
13. Groutz A, Blaivas JG, Chaikin DC, Weiss JP, Verhaaren M. The pathophysiology of post-radical prostatectomy incontinence: a clinical and video urodynamic study. J Urol. 2000;163(6):1767–1770. doi:10.1016/S0022-5347(05)67538-6
14. van der Poel HG, de Blok W, Joshi N, van Muilekom E. Preservation of lateral prostatic fascia is associated with urine continence after robotic-assisted prostatectomy. Eur Urol. 2009;55(4):892–900. doi:10.1016/j.eururo.2009.01.021
15. Strasser H, Frauscher F, Helweg G, Colleselli K, Reissigl A, Bartsch G. Transurethral ultrasound: evaluation of anatomy and function of the rhabdosphincter of the male urethra. J Urol. 1998;159(1):100–4; discussion 4–5. doi:10.1016/S0022-5347(01)64025-4
16. Rocco F, Carmignani L, Acquati P, et al. Restoration of posterior aspect of rhabdosphincter shortens continence time after radical retropubic prostatectomy. J Urol. 2006;175(6):2201–2206. doi:10.1016/S0022-5347(06)00262-X
17. Liu Y, Hall IJ, Filson C, Howard DH. Trends in the use of active surveillance and treatments in Medicare beneficiaries diagnosed with localized prostate cancer. Urol Oncol. 2021;39(7):432.e1–e10.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
What are the Most Important Objectives of Patients Undergoing Radical Prostatectomy? A Narrative Review
Virk A, Treacy PJ, Thanigasalam R, Leslie S
Research and Reports in Urology 2023, 15:563-569
Published Date: 19 December 2023
The Prognostic Value of Perioperative Factors on Biochemical Recurrence in Patients Undergoing Radical Prostatectomy
Pyrgidis N, Weinhold P, Schulz GB, Chaloupka M, Berg E, Westhofen T, Rodler S, Keller P, Jokisch F, Stief CG, Marcon J, Bischoff R
Research and Reports in Urology 2025, 17:185-194
Published Date: 27 May 2025
Decision-Making Dilemmas Among Elderly Prostate Cancer Patients Receiving 177Lu-PSMA Therapy: A Qualitative Study
Chen Y, Liu C, Li R, He Y, Li L
Patient Preference and Adherence 2026, 20:584017
Published Date: 23 March 2026