Back to Journals » Patient Preference and Adherence » Volume 20
Decision-Making Dilemmas Among Elderly Prostate Cancer Patients Receiving 177Lu-PSMA Therapy: A Qualitative Study
Authors Chen Y ![]() , Liu C, Li R, He Y
, Liu C, Li R, He Y ![]() , Li L
, Li L
Received 24 November 2025
Accepted for publication 13 March 2026
Published 23 March 2026 Volume 2026:20 584017
DOI https://doi.org/10.2147/PPA.S584017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ying Chen,1 Chunyu Liu,1 Ruilian Li,1 Yaping He,1 Li Li2
1School of Nursing, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 2Department of Nursing, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
Correspondence: Li Li, Department of Nursing, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China, Tel +86 13568624027, Email [email protected]
Objective: To explore the decision-making dilemmas experienced by elderly patients with advanced prostate cancer when considering 177Lu-PSMA therapy, and to provide evidence for the development of tailored decision-support strategies.
Methods: A qualitative descriptive design was adopted. Using purposive sampling, 20 elderly prostate cancer patients who had received 177Lu-PSMA therapy at a tertiary hospital in China between April and June 2025 were recruited for semi-structured interviews. Data were analyzed following Braun’s style of thematic analysis.
Results: Three overarching themes and nine subthemes were identified, reflecting multi-layered decision-making conflicts. (1) Decision-making triggers dilemma described information cognitive deficits, family value conflicts, and weak support systems that constrained patients’ understanding and autonomy. (2) Decision-conflicting perceptual dilemma captured uncertainty regarding treatment efficacy and emotional distress caused by disease progression and prior treatment experiences. (3) Coping-adaptive behavioral dilemma illustrated financial constraints, dependent decision tendencies, and varied coping strategies, alongside expressed needs for accessible and technology-supported tools. These findings reveal the complex interplay of cognitive, emotional, familial, and systemic factors influencing treatment decisions.
Conclusion: Effective resource support can help elderly prostate cancer patients cope with various dilemmas during the 177Lu-PSMA treatment decision-making process. Nursing staff should address the actual needs of patients, explore the clinical application of emerging age-appropriate decision-support interventions, and construct decision-support programs tailored to patient characteristics, thereby helping patients develop positive coping mechanisms and enhancing their active participation as well as rational decision-making abilities.
Keywords: elderly, prostate cancer, 177Lu-PSMA, dilemmas in decision-making, qualitative research, influencing factors
Introduction
Prostate cancer (prostate cancer, PCa) is one of the most prevalent malignancies among men worldwide, with increasing incidence in aging populations.1,2 A considerable proportion of patients are diagnosed at an advanced stage, with 60% diagnosed over the age of 65 and 20% diagnosed over the age of 75,3 and may progress to metastatic castration-resistant prostate cancer (mCRPC), which carries a poor prognosis and limited survival benefit from conventional therapies.4 Lutetium-177-labeled prostate-specific membrane antigen (177Lu-PSMA) therapy has emerged as a promising treatment for mCRPC, demonstrating survival benefits and manageable toxicity.5,6 However, its clinical application involves substantial uncertainty. Treatment response varies, adverse effects may occur, and access remains limited in China due to restricted institutional availability and high costs.7 Compared with established therapies, the novelty, complexity, and financial burden of 177Lu-PSMA therapy may intensify decisional challenges. Treatment decision-making in advanced PCa extends beyond medical considerations and encompasses emotional distress, value conflicts, family influence, and expectations regarding quality of life.8 Some qualitative research has confirmed decisional uncertainty, role transitions within families, and reliance on surrogate decision-makers among elderly cancer patients.9–11 Nevertheless, most existing research has focused on conventional treatments, with limited exploration of decision-making experiences related to novel, technology therapies such as radionuclide treatment.
In China, family-centered cultural norms further shape treatment decisions. Filial expectations, collective deliberation, and financial constraints may limit patient autonomy. Furthermore, patients’ limited understanding of nuclear medicine, coupled with information asymmetry between physicians and patients, particularly among older adults who may experience cognitive decline and heightened risk aversion, further exacerbates decision-making dilemmas.12 At present, research on 177Lu-PSMA has primarily focused on clinical efficacy and safety, qualitative evidence remains scarce regarding how informational barriers, emotional responses, family dynamics, and systemic constraints interact in shaping their decisions. This study employed a qualitative descriptive design to explore the decision-making dilemmas of elderly patients undergoing 177Lu-PSMA therapy. By examining triggering factors, perceptual conflicts, and coping behaviors, the study aims to provide insights for healthcare professionals to develop evidence-based decision-support strategies.
Methods
Study Design
This study adopted a qualitative descriptive design to conduct semi-structured interviews with elderly prostate cancer patients undergoing 177Lu-PSMA therapy. The study was reported in accordance with the Standards for Reporting Qualitative Research (SRQR) guidelines. The interview guide was based on existing literature concerning decision-making in patients with advanced cancer, research team discussions, and expert consultation with an oncology nurse, a nuclear medicine physician, and a nuclear medicine nurse. Three pilot interviews were conducted to refine question clarity and sequencing before formal data collection. Content includes: ① What are your primary sources of information about 177Lu-PSMA therapy? How did you choose your current treatment approach? ② What challenges did you encounter when selecting your treatment approach? ③ During discussions with your doctor about treatment options, were you able to understand the information, grasp the concepts, and express your thoughts? ④ Did family or friends offer advice during the decision-making process? ⑤ Do you wish to participate in discussions and choices regarding your treatment decisions? ⑥ What kind of assistance and support would you like to receive during the decision-making process? For example, visual aids, videos, or other resources?
Researcher Characteristics
Using purposive sampling and following the principle of maximum variation, participants were recruited from the Department of Nuclear Medicine at a tertiary hospital in Sichuan Province between April and June 2025. Variation was sought in age, education level, treatment experience, and geographic background to enhance data richness and transferability. The inclusion criteria were as follows: ① Age ≥ 60 years; ② Diagnosis of prostate cancer confirmed by histopathological or cytological examination; ③ History of ≥1 prior radionuclide therapy session; ④ No communication barriers; ⑤ Voluntary participation in this study. Exclusion Criteria: ① Concurrent severe comorbidities; ② Severe cognitive impairment. Data collection continued until thematic saturation was achieved. Saturation was considered to have occurred when no new codes, categories, or conceptual insights emerged from successive interviews. After the 18th interview, no substantially new themes were identified; therefore, two additional interviews were conducted to confirm informational redundancy. Ultimately, 20 elderly prostate cancer patients undergoing 177Lu-PSMA therapy from 11 provinces (municipalities) were included, as shown in Table 1.
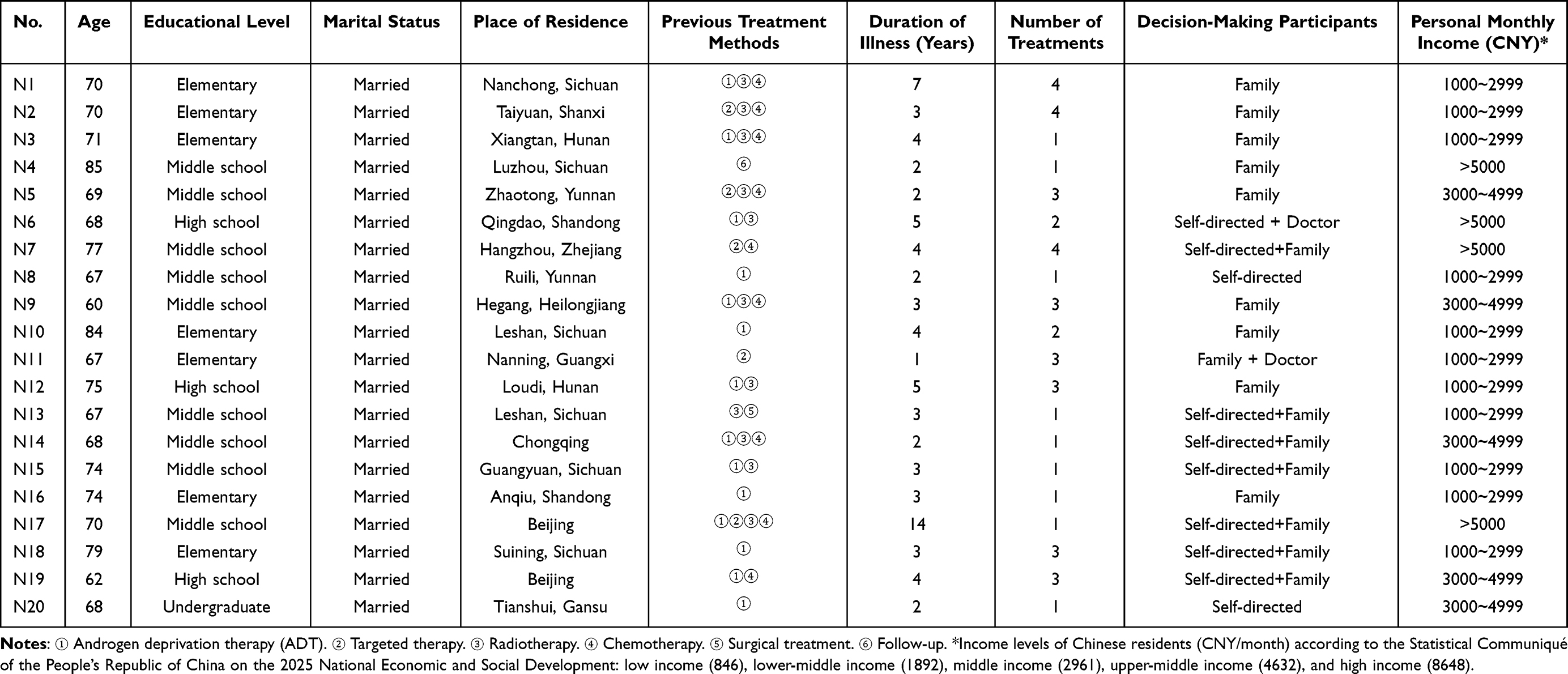 |
Table 1 The General Characteristics of the Respondents (n=20) |
Ethical Considerations
This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Southwest Medical University (KY2025421). Adhering to the principles of voluntary participation and confidentiality, all participants provided written informed consent prior to the interviews, which explicitly authorized the publication of anonymized responses and direct quotes. The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants were assigned unique identifier codes (eg N1, N2) to replace personal identifiers. Information concerning third parties within the interviews underwent de-identification prior to transcription and analysis. Personnel outside the research team had no access to raw data or unedited materials.
Data Collection
Researchers explained the general treatment process to patients in their wards on the day of admission and maintained effective communication throughout the treatment to establish a relationship of trust. Interviews were conducted in a quiet and private environment. Prior to each interview, the purpose, content, methodology, and presentation format of the findings were clearly explained to participants. All interviews were audio-recorded. The interviewer employed active listening, probing questions, and clarification techniques to express their subjective experiences. Field notes were recorded to capture non-verbal cues and contextual observations. Each interview lasted approximately 20–40 minutes.
Data Analysis
Data were analyzed using Braun’s thematic analysis framework.13 Audio recordings were transcribed verbatim within 24 hours, with non-verbal cues such as body language and facial expressions annotated in the transcripts. Following transcription, the data were cross-checked for accuracy. Two researchers independently conducted initial coding using NVivo 11.0 software. Open coding was first performed to identify meaningful segments. Codes were then grouped into potential themes and subthemes through iterative comparison. Discrepancies in coding or theme interpretation were resolved through discussion until consensus was reached. When disagreements persisted, the research team engaged in collective discussion until consensus was achieved, thereby ensuring methodological rigour and consistency in coding and thematic analysis. The steps of the thematic analysis method are as follows: ① Reading all transcripts repeatedly to achieve data familiarity ② Conducting initial coding to extract meaningful data segments ③ Grouping initial codes into potential themes and subthemes ④ Reviewing and refining themes to ensure internal coherence and external distinction, splitting or revising themes when necessary ⑤ Defining and clearly naming each theme to capture its core essence ⑥ Structuring the research report around the identified themes.
Trustworthiness of Data
The researcher had clinical nursing experience in nuclear medicine and received formal training in qualitative research. By avoiding the use of leading, suggestive, or evaluative language, the researcher established a solid foundation for conducting effective interviews. Researchers consciously set aside prior experience through methods such as writing reflective journals and conducting research group discussions, striving to reconstruct patients’ genuine subjective experiences during the treatment decision-making process.
Results
This study identified 3 themes and 9 sub-themes, as shown in Figure 1.
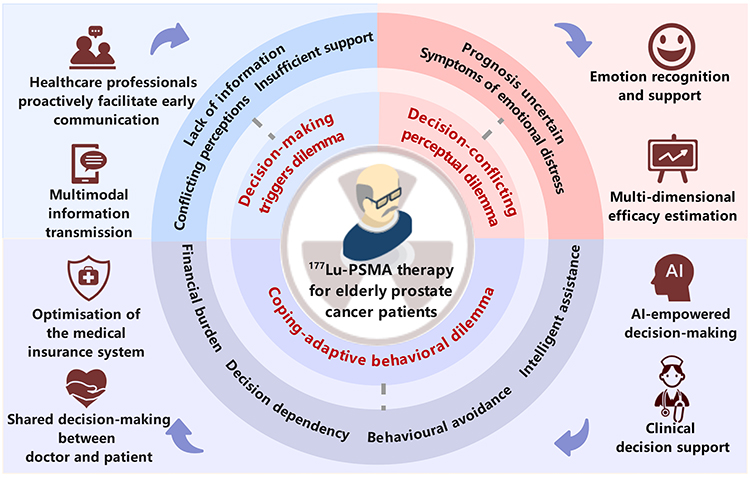 |
Figure 1 Core Dilemma Theme Extraction. |
Decision-Making Triggers Dilemma
Information Cognitive Deficit
Patients frequently encountered information gaps and comprehension barriers during the decision-making process for 177Lu-PSMA therapy, which limited both their willingness and capacity to engage in treatment choices. Many patients reported relying primarily on the internet or relatives for treatment-related information. The lack of authoritative sources and the predominance of medical jargon exacerbated difficulties in interpretation and heightened anxiety.
I saw online that some people say this treatment causes skin ulcers, which looks pretty scary. (N1)
There’s too much information online, and most of it is in English, which I can’t understand. (N14)
Several patients also observed that healthcare providers were unfamiliar with this therapy, limiting their ability to provide systematic guidance.
The hospital I visited previously hadn’t even heard of this treatment, and the doctor couldn’t explain it clearly either, telling me to go home and search for the information myself. (N7)
In this study, the majority of patients demonstrated low levels of educational attainment. Some patients associated their limited health literacy with difficulties in comprehending treatment information and assessing treatment risks, frequently leaving them in a state of cognitive constraint and decision dependency.
My son discovered this treatment for me—I had no idea such a method even existed. (N11)
Family Value Conflict
Within the context of traditional Chinese culture, patients’ treatment decision-making is strongly shaped by the concept of filial piety (one of the core values in Chinese culture, referring to the moral code of respecting and caring for one’s parents and elders). For many families, particularly children, pursuing aggressive treatment is perceived as a demonstration of filial duty, whereas patients often experience a dual ethical and emotional conflict between “prolonging life” and “reducing family burden”. On one hand, some patients choose to forgo treatment due to concerns about imposing excessive financial strain on their families.
The treatment costs are just too high—I really don’t want to proceed. Everything is so expensive these days, and my child’s education is already costing a fortune. (N3)
My sons all urged me to seek treatment, but for me, finances are the top priority—medical care is simply unaffordable. (N10)
On the other hand, some patients passively accept treatment plans because they are unwilling to go against their children’s wishes.
Some people think that, at my age, it doesn’t matter whether I get treated or not. But my child believes that, as long as this medicine works, it’s worth it even if it only extends my life a little. (N4)
My family supports my treatment, so I’ll follow their advice. I’ll live one day at a time, and as long as I’m not too miserable, I’ll be satisfied. (N20)
Weak Support System
Some patients lack multidimensional support from family, healthcare providers, and the healthcare system during the treatment decision-making process, manifesting as insufficient emotional support, delayed doctor-patient communication, and limited access to resources. Patients find it difficult to confide in their relatives about the progression of their illness, leaving them in a state of prolonged emotional isolation.
I didn’t tell them about the progression of the illness, nor did I want to. (eyes welling up). (N2)
Young people have so much on their plates; they can’t spare the time for me. When the day comes that I can’t hold on any longer, I’ll just wait for death—I won’t burden my children. (N8)
In doctor-patient communication, some doctors lack professional guidance during treatment or employ terminology that is not sufficiently accessible, leaving patients to bear the burden of decision-making responsibilities while remaining in a state of partial comprehension.
Sometimes a doctor explains things quite clearly, yet I still find myself utterly baffled afterwards. It’s just like being in class: you think you understand while you’re listening, but come home and still can’t do the exercises. (N10)
Moreover, at the systemic level, constrained by the limited diagnostic capabilities of primary healthcare facilities and the uneven distribution of novel radionuclide therapy resources, some patients are compelled to seek treatment across regions, thereby missing the optimal window for disease intervention.
I went to the hospital with blood in my urine, but the doctor simply sent me home to monitor it. It wasn’t that no tests were done; rather, the doctor failed to diagnose the condition. (N9)
I’ve been seeking treatment everywhere for fear of missing the window of opportunity. The longer I wait, the more urgent it becomes—it’s like racing against time. (N17)
The absence of adequate support systems deprived patients of essential emotional connections, professional guidance, and coping resources, thereby amplifying both psychological distress and practical burdens in their healthcare decision-making.
Decision-Conflicting Perceptual Dilemma
Plagued by Fluctuating Efficacy
The efficacy of 177Lu-PSMA therapy varied substantially among individuals. Patients reported a lack of clear, staged criteria to evaluate treatment response, and recurrent disease further complicated outcome prediction, thereby contributing to hesitation in treatment decision-making.
After undergoing treatment, if I do not continue with medication, will I be prone to relapse? (N10)
The first treatment proved effective, but the second did not. My bones and lower back still hurt, and the effect did not last long. (N18)
Concurrently, patients expressed concerns regarding the frequent imaging examinations and potential radiation risks associated with 177Lu radionuclide therapy.
I feel that bone scans are performed too frequently during treatment, and they have quite a significant impact on people, with considerable side effects. (N1)
I understand that radionuclide therapy involves radiation. After treatment, will I still be able to live with my grandson? (N3)
Is the level of radiation in the body particularly high after radionuclide therapy, and could this affect living with family members? (N19)
Symptoms Emotional Distress
Several patients mentioned that the distress caused by symptoms of advanced prostate cancer significantly influenced their decision-making. The accumulation of negative emotions during the course of illness and prior treatments often left them more passive and reluctant when facing subsequent decisions.
When the bones ache, one becomes irritable and miserable, and I feel compelled to decide quickly whether to seek treatment. (N1)
The pain was so intense I couldn’t sit still or stand upright; it was truly unbearable, forcing me to switch treatment methods. (N6)
Undergoing radiotherapy and chemotherapy proved quite gruelling, yet the outcome was negligible—barely even achieving a delay in the progression of the disease. (N8)
For decades, I’ve hardly ever been ill or taken any medication, so how did I suddenly develop cancer? I used to think it was something that only happened to other people, but now it’s happened to me. I simply can’t accept it and don’t know what to do. (N14)
Coping-Adaptive Behavioral Dilemmas
Economic Burden Constraints
The substantial of treatment coupled with inadequate health insurance coverage presents a significant barrier in patients’ treatment decisions, with many finding themselves torn between financial constraints and the necessity of treatment.
When will radionuclide therapy be covered by medical insurance ? We could breathe a sigh of relief, but without medical insurance coverage, the financial burden is simply too heavy. (N5)
The cost of further treatment is simply too high, so I’ve no choice but to abandon it. (N8)
Some patients have also indicated that the number of medical institutions offering radionuclide therapy is limited, necessitating frequent cross-regional travel and long-term treatment. This requires carers to take frequent leave or suspend work, thereby further exacerbating the financial burden.
Each follow-up requires traveling back and forth from our hometown to Beijing, followed by treatment in Luzhou after recovery. This constant back-and-forth has left us utterly exhausted. (N9)
Not everyone can take time off freely. Even if leave is granted, protecting long-term job security remains a pressing concern. (N11)
Dependent Decision-Making Tendency
In this sample, patients aged 70 and above predominantly exhibit family-dominated or collaborative decision-making patterns, whereas those under 70 showed a greater tendency toward autonomous decision-making.
This reflects a shift in decision-making patterns from individual-led to family-involved or family-dominated approaches. With advancing age, older patients may face limitations in cognitive comprehension and financial capacity, resulting in an insufficient ability to make active decisions. Some patients expressed difficulties in comprehending treatment information during interviews and a reliance on family members’ opinions, thereby transferring decision-making authority to their family members.
I’m not entirely clear on the treatment arrangements; it’s all been handled by my son, who has been keeping abreast of the situation and making the decisions. (N2)
Radioactive isotope therapy is far too expensive. I’ve never encountered such high costs before, and I simply cannot afford it. It’s all down to my sons making the decisions. (N3)
My son knows more about the treatment than I do. When it comes to hospital procedures on the phone, he’s the one liaising with the doctors. I can’t make head nor tail of it. (N5)
I’ve no other thoughts either. I’ll just go with the flow. Wherever my son-in-law tells me to go for treatment, that’s where I’ll go. (N11)
Coping Behavioral Strategies
Confronted with decision-making pressures stemming from incomplete information, insufficient support, and treatment uncertainty, some patients demonstrated significant decision-making incapacity and marginalization. They often resorted to emotional reassurance or conservative strategies as a means to mitigate or avoid the conflict and anxiety associated with decision-making.
Though death is inevitable, I still wish to linger a few more days. I can only console myself that if nothing else works, I will resort to conservative treatment, taking each day as it comes. (N15)
If I could live a few more years, perhaps treatment options that now seem unattainable might gradually become a reality. (N17)
The worsening of my condition has left me feeling rather anxious, so I thought I’d give it one more try, hoping that radionuclide therapy might actually prove effective. (N18)
On the surface, I appear calm, but internally, I experience considerable distress. When illness strikes, no one can escape it; one must simply accept it. (N19)
Intelligent Decision-Making
Some patients, whose limited digital literacy restricted their ability to access and evaluate information during treatment decision-making, expressed a need for straightforward and accessible information-support tools. This highlights the urgent need for effective interventions employing alternative communication formats and assistive technologies.
I keep forgetting things these days, and I’m not very adept at mobile phones either. It would be much easier if we could just communicate directly, like making a phone call. (N8)
The department has promotional materials and case studies, but I don’t know how to search for them on my phone, and I can’t remember what the doctor explained. (N12)
The text on my phone is too small to read, and I don’t understand it either. If there were a video explanation, I would grasp it much better. (N14)
Some patients also expressed acceptance of and anticipation for AI-assisted communication tools.
I’m comfortable with how rapidly AI is advancing. I often use it when I’m unsure about something. If hospitals offered this kind of service, it would save us the trouble of bothering doctors. (N13)
The images in the examination report would be more comprehensible if accompanied by explanatory text, or if the report could be interpreted via voice narration. (N20)
Discussion
Bridge Information Gaps, Enhance Resource Support, and Advance Shared Decision-Making Practices
This study indicates that elderly prostate cancer patients undergoing 177Lu-PSMA therapy frequently face information gaps and insufficient support systems during the decision-making process, consistent with the findings of Kawasaki.14 As a novel radioligand therapy, its technical attributes and implementation conditions are unique. During the decision-making process, patients must not only confront the clinical complexity and uncertainty of treatment efficacy but also weigh additional concerns, including radiation safety, the limited availability of specialized medical resources in China, and the significant financial pressure resulting from its exclusion from national health insurance. These factors collectively constitute a decisional pressure specific to 177Lu-PSMA therapy, distinguishing it from other emerging treatments, which require timely and effective decision-related information and support systems to inform their choices. Currently, the information provided by clinical healthcare professionals is predominantly unidirectional, lacking both specificity and accessibility. Online resources are also constrained by delayed timeliness and high professional barriers. For 177Lu-PSMA therapy, patients require precise guidance on the treatment protocol and the risk-benefit balance. Therefore, healthcare professionals should advance the point of communication, using plain language and multimodal communication strategies such as illustrated guides, educational videos, leveraging internet platforms to promote the sharing and understanding of information. Strengthening family and social support provides important protection against decision-making pressures. This study found that some patients experience isolation in decision-making due to limited family understanding and involvement, which may be associated with filial piety and collectivist values in the Chinese cultural context.15 Notably, such cultural factors do not solely support; they may also restrict patient autonomy and limit access to information. Some scholars have suggested,16 convening a family meeting upon admission to enhance cohesion and communication. The uneven distribution of 177Lu-PSMA treatment resources and its high cost make accessibility and financial burden key factors influencing treatment uptake. Healthcare professionals should refrain from making substitute decisions, instead guiding families towards shared decision-making aligned with the patient’s genuine wishes, thereby avoiding excessive medical interventions. At the societal level, efforts should focus on optimizing the allocation of medical resources and accelerating improvements to the health insurance system, reduce disparities in treatment accessibility, and ease patients’ decision-making burden. Moreover, patients often struggle to clearly express their preferences when faced with complex options and limited information. The emergence of shared decision-making represents an effective pathway to enhance both the quality of decision-making and patient satisfaction.17 Nurses, as facilitators of shared decision-making,18 should act as bridges and guides in practice, dynamically assessing patients’ health literacy and psychological state, and implementing compassionate, tailored support to foster active participation in decision-making.
Prioritise Patient Emotional Wellbeing, Foster Effective Communication, and Enhance Decision-Making and Coping Capabilities
Within outpatient settings characterized by fast-paced clinical workflows and limited communication resources, patients are often required to make critical treatment decisions within a very short timeframe. Insufficient absorption of information, restricted opportunities for expression, and difficulties in emotional adjustment make them highly susceptible to anxiety and decision-making dilemmas. This study indicates that patients face dual pressures during treatment decision-making: the rapid progression of disease and the uncertainty of therapeutic outcomes. Furthermore, because 177Lu-PSMA therapy is a novel treatment modality, patients often lack sufficient time, knowledge, and emotional preparation. Consequently, decision-making is frequently accompanied by negative emotional fluctuations, leaving them prone to experiences of anxiety, fear, and uncertainty. On the one hand, patients are often required to make multiple high-stakes treatment decisions concerning quality of life and financial burden within a limited period. This frequent decision-making significantly increases their cognitive load and diminishes their capacity to allocate cognitive resources;19 On the other hand, the accumulation of negative emotions may induce avoidance behaviors, leading patients to make decisions inconsistent with their true intentions, ultimately undermining decision quality and treatment adherence.20 Consistent with prior studies, the combined effects of time pressure and anxiety substantially reduce elderly patients’ willingness to participate in decision-making and their perceived cognitive efficacy.21,22 Consequently, nursing staff should promptly identify patients’ emotional responses, enhance communication skills, and make effective use of visual and multimodal resources to convey knowledge about 177Lu-PSMA therapy. This approach aims to improve patient comprehension, encourage the expression of genuine feelings, and identify and address emotional distress. Emotional support may be provided through complementary methods such as mindfulness-based stress reduction and music therapy. Concurrently, ward-based discussion sessions and multidisciplinary support groups can promote belief reinforcement and psychological resonance, thereby enhancing their decision-making confidence and capacity. Additionally, a multidimensional efficacy prediction model is established based on biological, psychological, and social indicators—including laboratory tests, PSA assessments, imaging metrics, and patient-reported outcomes (eg FACT-RNT),23,24 enhance the effectiveness of doctor-patient communication, facilitate precise decision support, and improve communication efficiency and trust in treatment plans.
Focusing on Geriatric Characteristics and Integrating Artificial Intelligence to Achieve Precision-Tailored Decision Support
This study reveals that the treatment decision dilemma surrounding 177Lu-PSMA therapy exhibits significant population specificity among elderly prostate cancer patients. The patients in this study were aged 60–80 years. Patients under 70 years demonstrated greater decision-making autonomy, patients aged 70 and above exhibited more pronounced differences in cognitive function and support requirements. Due to varying degrees of cognitive decline and digital literacy, many elderly patients particularly those of advanced age struggle to independently comprehend complex treatment mechanisms, these differences result in unique characteristics regarding information acquisition, technology reliance, and treatment objectives. They are prone to comprehension barriers and decision fatigue in fragmented, jargon-laden information environments, and show strong reliance on explanations that are clear, repetitive, and visually supported. Furthermore, the majority of patients in this study had limited educational backgrounds, which further intertwined with their age to exacerbate difficulties in assessing treatment risks and increased their dependence on physicians or family members. The relationship between individual characteristics and decision-making tendencies determines their preferences and receptiveness toward decision support methods. Relying solely on traditional educational and communication approaches is insufficient to fully meet their practical needs. Artificial intelligence (AI), as a vital tool for advancing healthcare, has demonstrated its advantages in complex data analysis, predicting medical outcomes, and optimizing treatment decisions through deep learning algorithms and large-scale data training;25 The application of AI health assistants,26 can efficiently identify patients’ characteristics in emotional preferences, and value orientations. However, although some patients express interest in technological tools such as AI, their acceptance remains constrained by factors including operational complexity and a weak foundation of trust.27 Therefore, future research may emphasise age-friendly features in the design of AI and other digital assistive tools, such as simplified interfaces, enhanced voice interaction, and visual guidance.28 Leveraging AI tools to translate complex radionuclide therapy information into verbal explanations and visual representations, while strengthening healthcare professionals’ role in guiding and connecting patients during technical procedures. Consequently, it alleviates digital barriers and communication difficulties. Nevertheless, their practical effectiveness and acceptability among older adults require further empirical validation. Subsequent studies may be based on the characteristics of the elderly population, integrating value orientation, family collaboration, and healthcare empowerment. This approach would advance the realisation of precision decision support tailored to the needs of older adults.
Limitations
This study has several limitations that should be acknowledged. The findings may have been influenced by the availability of healthcare resources, as participants were recruited from a single hospital. Furthermore, the absence of longitudinal follow-up precluded capturing the dynamic evolution of decision conflict. The relatively low educational attainment of the participants may restrict the generalizability of these results to more highly educated groups or populations with different sociocultural backgrounds.
Conclusion
This study elucidates the complex interplay between practical, emotional, familial and treatment-related factors encountered by elderly prostate cancer patients undergoing 177Lu-PSMA therapy during their decision-making process. Therefore, a comprehensive assessment of the patient’s needs is paramount, taking into account not only medical factors but also the socio-psychological and family circumstances that influence decision-making. Healthcare professionals should enhance both the capacity and quality of patient participation by identifying determinants of involvement and developing tailored decision-support tools based on patient characteristics and information needs. Future research should prioritize multi-center, large-sample longitudinal studies to track the dynamic evolution of decision conflicts. Developing age-friendly AI tools represents a promising future direction. Further exploration is needed to evaluate the feasibility and effectiveness of AI-assisted decision-making applications in addressing the stage-specific challenges faced by elderly patients, thereby providing a robust basis for tailored support solutions.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the 2024 Science and Technology Strategic Cooperation Project between Luzhou Municipal People’s Government and Southwest Medical University (Grant No. 2024LZXNYDJ067), the 2024 Special Research Fund for Clinical Medicine at Southwest Medical University (Grant No. 2024LCYXZX65), and the 2025 Scientific Research Fund of Southwest Medical University (Grant No. 2025SKYB01).
Disclosure
The authors declare no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Zheng RS, Chen R, Han BF, et al. [cancer incidence and mortality in China, 2022]. Zhonghua Zhong Liu Za Zhi. 2024;46(3):221–231. (in Chinese). doi:10.3760/cma.j.cn112152-20240119-00035
3. Graham LS, Lin JK, Lage DE, et al. Management of prostate cancer in older adults. Am Soc Clin Oncol Educat Book. 2023;43:e390396. doi:10.1200/EDBK_390396
4. Wang SH, Gu YF, Xu S. Advances in radionuclide therapy for metastatic castration-resistant prostate cancer. Chin J Androl. 2023;2023(3):275–281. (in Chinese).
5. Cao J, Chen Y, Hu M, et al. 177Lu-PSMA-RLT of metastatic castration-resistant prostate cancer: limitations and improvements. Ann Nucl Med. 2021;35(8):861–870. doi:10.1007/s12149-021-01649-w
6. Sartor O, de Bono J, Chi KN, et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. New Engl J Med. 2021;385(12):1091–1103. doi:10.1056/NEJMoa2107322
7. Mehrens D, Kramer KKM, Unterrainer LM, et al. Cost-effectiveness analysis of 177Lu-PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer. J Natl Compr Canc Netw. 2023;21(1):43–50.e2. doi:10.6004/jnccn.2022.7070
8. Gartrell BA, Phalguni A, Bajko P, et al. Influential factors impacting treatment decision-making and decision regret in patients with localized or locally advanced prostate cancer: a systematic literature review. Eur Urol Oncol. 2024;7(6):1216–1227. doi:10.1016/j.euo.2024.04.016
9. Dijkman BL, Luttik ML, Paans W, et al. Exploring family perspectives in geriatric oncology: a triadic approach to shared decision-making - a qualitative study. BMC Geriatr. 2025;26(1):123. doi:10.1186/s12877-025-06744-5
10. Su Y, Yuki M, Hirayama K. The experiences and perspectives of family surrogate decision-makers: a systematic review of qualitative studies. Patient Educ Couns. 2020;103(6):1070–1081. doi:10.1016/j.pec.2019.12.011
11. Yu T, Li Y, Hu Z, et al. Family members’ experiences of surrogate decision-making in hospice care: a systematic review of qualitative studies. Int J Nurs Stud. 2025;162:104987. doi:10.1016/j.ijnurstu.2024.104987
12. Wilson RS, Yu L, Stewart CC, et al. Change in decision-making analysis and preferences in old age. J Gerontol Ser B. 2023;78(10):1659–1667. doi:10.1093/geronb/gbad037
13. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Wellbeing. 2014;9:26152. doi:10.3402/qhw.v9.26152
14. Kawasaki Y, Hirai K, Nii M, et al. Factors involved in shared decision-making regarding treatment selection by patients with cancer. Cancer Diagn Progn. 2024;4(1):57–65. doi:10.21873/cdp.10286
15. Li MN, Yan YY, Fu G, et al. Clinical shared decision-making: the “collision” between Western theory and Chinese culture. Chin Med Ethics. 2025:1–9. (in Chinese).
16. Qi CH, Kang FY, Zhao WF, et al. Phenomenological study on family members’ decision-making dilemmas in continuous renal replacement therapy for ICU patients with acute kidney injury. Mil Nurs. 2023;2023(3):41–44. (in Chinese).
17. Waddell A, Lennox A, Spassova G, et al. Barriers and facilitators to shared decision-making in hospitals from policy to practice: a systematic review. Implement Sci. 2021;16(1):74. doi:10.1186/s13012-021-01142-y
18. Zhan YX, Yu JH, Liu YF, et al. Qualitative study on nurses’ cognition of shared decision-making practice. J Nurs Sci. 2021;2021(1):56–59. (in Chinese).
19. Guo ZN, Ling KY, Chen SF, et al. Qualitative study on surrogate decision-making dilemmas of families of patients with severe stroke. Chin J Nurs. 2024;59(14):1746–1751. (in Chinese).
20. Soshi T, Nagamine M, Fukuda E, et al. Pre-specified anxiety predicts future decision-making performances under different temporally constrained conditions. Front Psychol. 2019;10:1544. doi:10.3389/fpsyg.2019.01544
21. Wieringa TH, León-García M, Espinoza Suárez NR, et al. The role of time in involving patients with cancer in treatment decision making: a scoping review. Patient Educ Couns. 2024;125:108285. doi:10.1016/j.pec.2024.108285
22. Pang TY, Yuan L, Wu LG, et al. Qualitative study on decision-making experiences of family members in palliative care for advanced cancer patients. Chin J Nurs. 2023;58(13):1559–1564. (in Chinese).
23. Chinese Society of Clinical Oncology Committee of Nuclear Medicine, Chinese Medical Doctor Association Branch of Nuclear Medicine Physicians. Expert consensus on clinical practice of 177Lu-PSMA radioligand therapy for prostate cancer (2024 edition). China Oncology. 2024;34(7):702–714. (in Chinese).
24. Gudenkauf LM, Chavez MN, Maconi ML, et al. Developing a patient-reported outcome measure for radionuclide therapy for prostate cancer. J Nucl Med. 2023;64(6):869–872. doi:10.2967/jnumed.122.264946
25. Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23(1):689. doi:10.1186/s12909-023-04698-z
26. Curtis RG, Bartel B, Ferguson T, et al. Improving user experience of virtual health assistants: scoping review. J Med Internet Res. 2021;23(12):e31737. doi:10.2196/31737
27. Rezaeian O, Bayrak AE, Asan O. Explainability and AI confidence in clinical decision support systems: effects on trust, diagnostic performance, and cognitive load in breast cancer care. Int J Hum Comput Interact. 2025;41:149–160. doi:10.1080/10447318.2023.2295725
28. Cho H, Oh O, Greene N, et al. Engagement of older adults in the design, implementation, and evaluation of artificial intelligence systems for aging: a scoping review. J Gerontol A Biol Sci Med Sci. 2025;80(5):glaf024. doi:10.1093/gerona/glaf024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Robosling Technique in Robotic Radical Prostatectomy Promotes Early and Sustained Return of Continence in Elderly Patients
Yu V, Gibson D, Cotte J, Amin A, Chan L, Ahmadi N, Jeffery N, Thanigasalam R, Leslie S
Research and Reports in Urology 2026, 18:599921
Published Date: 2 July 2026