Back to Journals » Infection and Drug Resistance » Volume 15
The Risk Factors of Carbapenem-Resistant Klebsiella pneumoniae Infection: A Single-Center Chinese Retrospective Study
Authors Wang L, Yuan XD, Pang T, Duan SH
Received 1 December 2021
Accepted for publication 11 March 2022
Published 5 April 2022 Volume 2022:15 Pages 1477—1485
DOI https://doi.org/10.2147/IDR.S352070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Lei Wang, Xiao-Dong Yuan, Ting Pang, Shu-Hong Duan
Department of Infectious Diseases, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Shu-Hong Duan, Department of Infectious Diseases, Beijing Shijitan Hospital, Capital Medical University, NO. 10 Tie Yi Road, Yang Fang Dian, Haidian District, Beijing, 100038, People’s Republic of China, Tel + 86 10 63926121, Email [email protected]
Objective: The present study aims to explore potential infection and death risk factors in patients infected with carbapenem-resistant Klebsiella pneumoniae (CRKP).
Methods: A retrospective case-control study was performed at Beijing Shijitan Hospital, China. The clinical and microbiological data of patients infected with K. pneumoniae (K.pn) were collected; the clinical characteristics of patients infected with carbapenem-susceptible K.pn and CRKP were analyzed using logistic regression analysis.
Results: CRKP infection was significantly associated with prior carbapenem use (odds ratio [OR] and 95% credibility interval [CI]: 5.161 [1.840– 32.233], P < 0.001), the use of more than three types of antibiotics for seven or more days (OR and 95% CI: 9.681 [2.662– 18.122], P < 0.001), tracheotomy (OR and 95% CI: 5.015 [2.343– 11.724], P < 0.001), and intensive care unit (ICU) stay (OR and 95% CI: 6.322 [2.02– 12.231], P < 0.001). The risk of death in patients with CRKP infection was significantly associated with older age (OR and 95% CI of 70– 80 years: 8.894 [1.972– 67.346], P < 0.001; ≥ 80 years: 15.234 [2.072– 93.452], P < 0.001), renal dysfunction (OR and 95% CI: 1.672 [1.104– 7.451], P = 0.016), tracheotomy (OR and 95% CI: 2.051 [1.217– 11.235], P = 0.002), and ICU stay (OR and 95% CI: 3.043 [2.174– 18.453], P < 0.001).
Conclusion: Prior to carbapenem use, older age, renal dysfunction, tracheotomy, and ICU stay were independent risk factors for death in patients infected with CRKP.
Keywords: Klebsiella pneumoniae, carbapenems, drug resistance, risk factors, antibiotics, Beijing
Introduction
Klebsiella pneumoniae (K.pn) is a Gram-negative bacteria and a major pathogen type that causes nosocomial infection, such as pyogenic liver abscess, urinary tract infection, bacteremia, and pneumonia.1 After Escherichia coli (E. coli),2 K.pn is the second most common pneumoniae cause (with occurrence rates of 29.9% and 19.8%, respectively) in Gram-negative organisms.
The incidence of K.pn in China is growing.2 Klebsiella pneumoniae isolates may be induced to express resistance phenotypes through carbapenemase (KPC) and/or cephalosporinase production, or outer membrane protein loss.3–5 The KPC gene is primarily plasmid-encoded; thus, it is disseminated among different K.pn clones and even among different bacterial species or genera.6 In clinical practice, an infection caused by enterobacterales (ENT) with extended-spectrum β-lactamases (ESBLs) was generally treated using carbapenem;7 however, the bacteria developed resistance to carbapenem.8
Carbapenem-resistant K.pn (CRKP) has been on the rise in most geographical areas since the 1990s, leading to increases in mortality, morbidity, hospitalization time, and medical costs.3,9 In China, the isolation rate of CRKP reached 3.5–5.9% in 2011–2012,10 6.4% in 2014,11 and 7.6% in 2015.2
Carbapenems belong to atypical β-lactam antibiotics with strong antimicrobial activity. As they are stable to is β-lactamases and have low toxicity, carbapenems serve as a major antibacterial agent in severe bacterial infection and have been considered the last line of treatment for infection caused by multi-drug resistant (MDR) Gram-negative pathogens. However, the dissemination of CR bacteria has become a global health problem.12 The emergence of CRKP has challenged carbapenem use.
Although several risk factors have been noted in existing studies, their conclusions have been inconsistent.13–15 To control nosocomial infection and improve empirical therapy efficacy, the present study attempted to identify the possible risk factors of CRKP-induced infection and death in hospitalized adults.
Methods
Study Design
A retrospective case-control study was performed to identify infection and death risk factors in patients infected with CRKP at Beijing Shijitan Hospital. Patients diagnosed with nosocomial K.pn infection between January 1, 2015, and June 30, 2018, were included in the present study. In cases of multiple K.pn infection episodes in one patient, only the first occurrence was included in the data analysis.
Inclusion criteria: (1) patients who were not infected with K.pn before admission; (2) patients with a hospital stay duration of ≥48 h; (3) patients aged ≥18 years. The patients were divided into two groups, ie, the case and control groups. Patients infected with CRKP were assigned to the case group, while patients infected with carbapenem-susceptible (CS) KP were assigned to the control group. The results of the two groups were subsequently compared.
Klebsiella pneumoniae infection: patients with fever, increased white blood cell count and/or neutrophil ratio, and whose specimen culture only isolated K.pn; K.pn was cultured in the specimen, but the patient had no inflammation and showed a K.pn value, which was excluded from this study.
Case-control data were matched according to the K.pn infection types, eg, respiratory tract infection, urinary system infection, thoracic and abdominal infection, bloodstream infection, and wound infection. The control and case groups were matched according to a 2–3:1 ratio. The patients received appropriate antibiotic treatment. In patients with CRKP infection, the death and survival groups were matched not only according to the type of infection but also based on the course of antibiotic treatment using a matching ratio of 1:2–3. This study complies with the Declaration of Helsinki. The ethics committee of Beijing Shijitan Hospital, Capital Medical University approved this study (No. Sjtky11-1x-2022(22)).
Data Collection
Data derived from medical records and microbiology were collected. Variables that were analyzed as potential risk factors included gender, age, medical unit, treatment, exposure to antibiotics, the length of hospital stay, comorbidities, and invasive procedures performed prior to infection. Exposure to antibiotics was defined as the use of antibiotics >48 h before K.pn infection.
Microbiological Examination
The antibiotics that were used in drug sensitivity tests were levofloxacin, ciprofloxacin, meropenem, imipenem, ceftazidime, ceftriaxone/sulbactam, cefepime, piperacillin/tazobactam, chloramphenicol, co-sulfamethoxazole, aztreonam, minocycline, ampicillin, and amikacin. Klebsiella pneumoniae isolate identification and drug susceptibility testing (AST) were carried out using the Vitek-2 Compact system. The AST results were interpreted in accordance with the Clinical and Laboratory Standards Institute criteria.16 In the case of CRKP, Hodge tests and combined disk tests using carbapenems with either ethylenediaminetetraacetic or boronic acid were performed.17,18 These experiments were phenotypic verification experiments of carbapenem drug resistance, as well as further verification of drug sensitivity results for meropenem, imipenem, and other carbapenem drugs using the minimal inhibitory concentration method. Quality control was conducted by testing Kpn ATCC 700603 and E. coli ATCC 25922. Quality control strains were used to monitor the accuracy and reliability of bacterial identification and drug sensitivity tests.
Statistical Analysis
Data were presented as n (%) or mean ± standard deviation (SD; range) and analyzed using the Statistical Package for Social Sciences 19.0 software. In the analysis of the risk factors for CRKP infection/colonization and mortality, a univariate logistic regression analysis was performed. To identify the independent risk factors, variables with P < 0.05 in the univariate analysis were included in the multivariate logistic regression model and analyzed using backward stepwise regression. Odds ratio (OR) and a 95% confidence interval (CI) were also calculated. For all statistical analyses, P < 0.05 indicated a statistical significance.
Results
A total of 333 patients with Kpn infection were included in this study, including 95 cases of CRKP infection (case group), and 238 cases of CSKP infection (control group). There were 207 male patients and 126 female patients in an age range of 39–97 years old (average age, 66.3 ± 11.3 years). Specimens were collected from 103 cases of respiratory tract infection, 78 cases of urinary tract infection, 64 cases of thoracic and abdominal infection, 54 cases of bloodstream infection, and 34 cases of wound infection.
In this study, primary diseases did not include single diseases and most conditions coexisted with multiple illnesses. Table 1 indicates the concomitant diseases in this regard, which include 147 cases of lung disease, 91 cases of cardiac dysfunction, 107 cases of renal dysfunction, 37 cases of neurological disease, 77 cases of liver disease, 87 cases of diabetes mellitus, 169 cases of hypoalbuminemia, and 46 tumor cases.
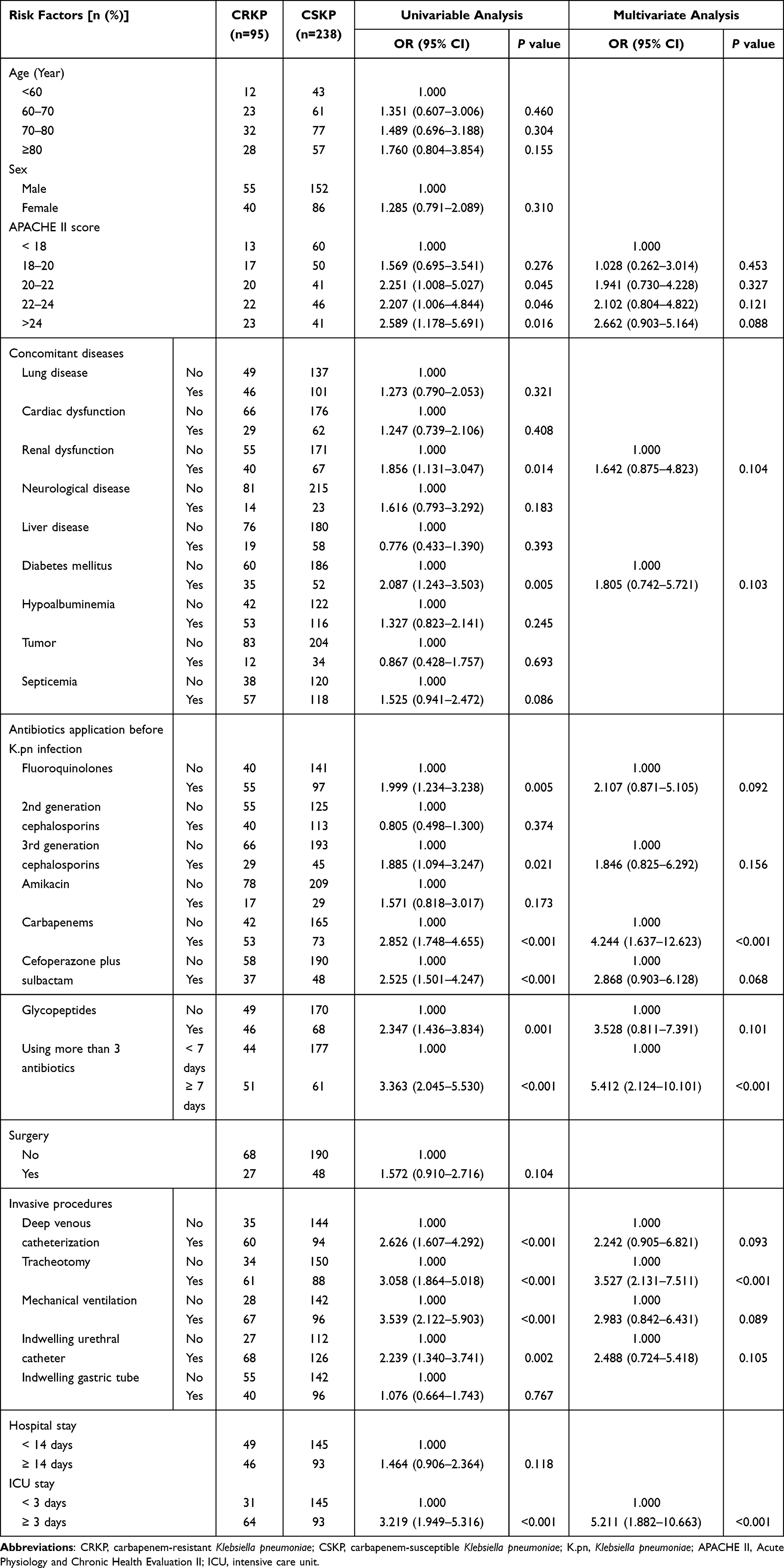 |
Table 1 Risk Factors for CRKP Infection |
In this study, the risk factors of carbapenem drug resistance to Kpn were primarily studied. Data concerning drug resistance of other antimicrobials were not collected. In addition, Kpn in this study was not included in the study because it was infected with other pathogens. The infection site was a matching factor and was not included in the risk factors. Mechanical ventilation and sepsis were added to the risk factor analysis, as shown in Tables 1 and 2.
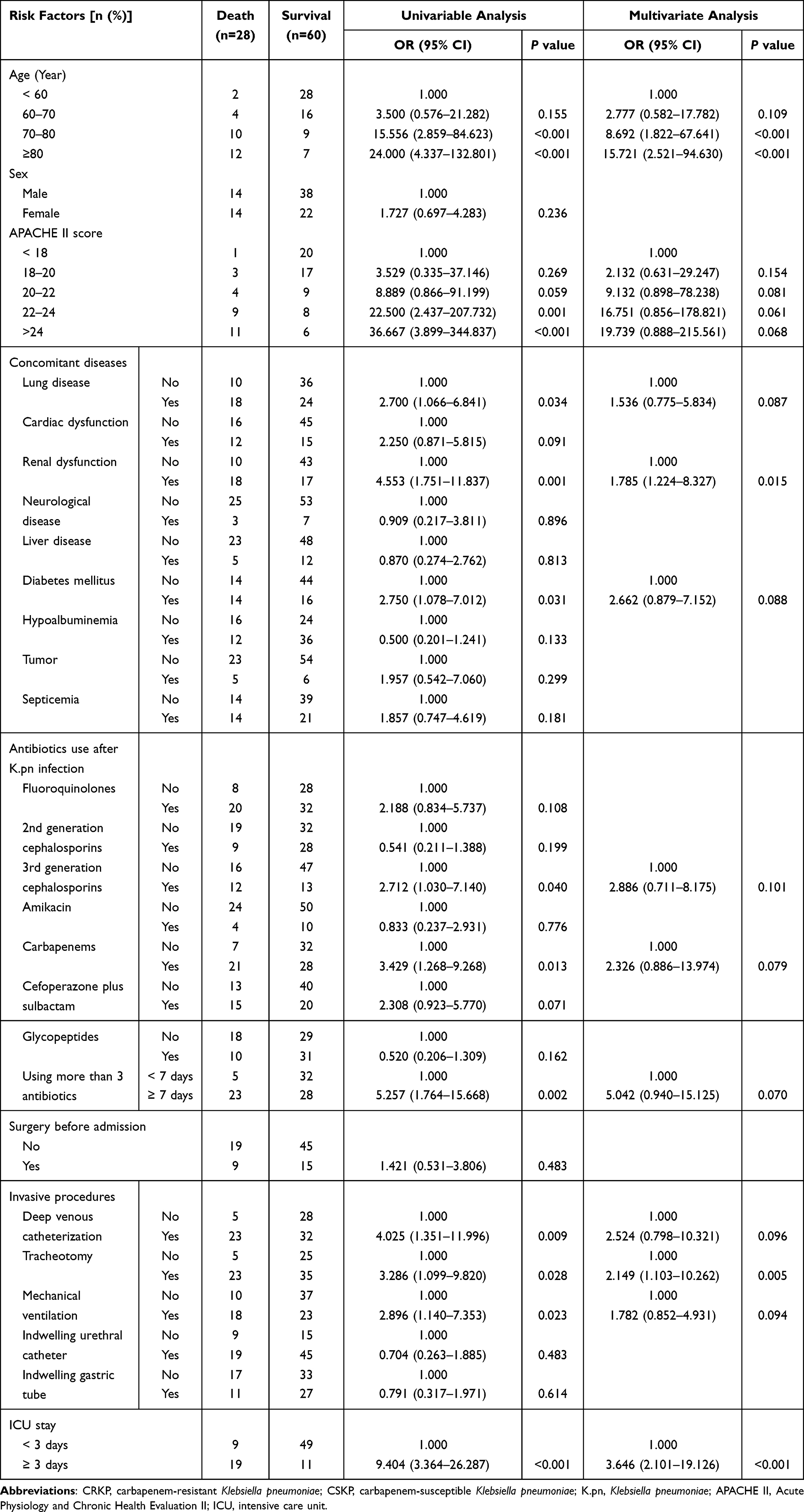 |
Table 2 Risk Factors for Death in Patients with CRKP Infection |
Carbapenem-Resistant Klebsiella pneumoniae Infection Risk Factors
In the univariate analysis, CRKP infection was significantly associated with a higher Acute Physiology and Chronic Health Evaluation II (APACHE II) score, prior exposure to fluoroquinolones, cefoperazone plus sulbactam and glycopeptides, the use of more than three types of antibiotics for seven or more days, deep venous catheterization, tracheotomy, indwelling urethral catheter, ICU stay, third-generation cephalosporins, and carbapenems (P < 0.05) (Table 1). The multivariable logistic regression analysis revealed significant associations between CRKP infection and prior carbapenem use (OR and 95% CI: 5.161 [1.840–32.233], P < 0.001), the use of more than three types of antibiotics for seven or more days (OR and 95% CI: 9.681 [2.662–18.122], P < 0.001], tracheotomy (OR and 95% CI: 5.015 (2.343–11.724], P < 0.001), and ICU stay (OR and 95% CI: 6.322 [2.02–12.231], P < 0.001) (Table 1).
Death Risk Factors in Patients Infected with Carbapenem-Resistant Klebsiella pneumoniae
The results of the univariate analysis showed that in patients infected with CRKP, death was significantly associated with older age, a higher APACHE II score, lung disease, renal dysfunction, prior carbapenem exposure, the use of more than three types of antibiotics for seven or more days, deep venous catheterization, tracheotomy, and ICU stay (P < 0.05) (Table 2).
The multivariable logistic regression analysis revealed significant associations between death and older age (OR and 95% CI of 70–80 years: 8.894 [1.972–67.346], P < 0.001; ≥80 years: 15.234 [2.072–93.452], P < 0.001), renal dysfunction (OR and 95% CI: 1.672 [1.104–7.451], P = 0.016), tracheotomy (OR and 95% CI: 2.051 [1.217–11.235], P = 0.002), and ICU stay (OR and 95% CI: 3.043 [2.174–18.453], P < 0.001) (Table 2).
Discussion
Following the findings of existing reports,14,19 completing a stay in the ICU before Kpn infection was a risk factor for CRKP infection. Patients in the ICU are typically in a serious condition with relatively severe complications; accordingly, they may be treated with a combination of different antibiotics with a longer usage duration. They may also undergo more invasive procedures compared with patients in other wards. These factors may be beneficial for reducing CRKP dissemination and screening.
Carbapenems are highly effective antibacterial agents in the treatment of infections caused by MDR-ENT bacteria that produce ESBLs and/or the ampicillinase C enzyme.20 Thus, a relationship between CRKP infections and carbapenem use can be anticipated. In the present study, prior carbapenem use was an independent risk factor of CRKP-induced infections. This result was consistent with the results of existing studies.14,21,22 In a different study, carbapenem use was not an independent risk factor in the multivariate analysis.23
CRKP infection was associated with the use of more than three types of antibiotics for seven or more days. Although the long-term combined application of several antibacterial agents could significantly inhibit bacterial growth, it may also cause bacterial mutation and drug resistance due to the selective antibiotic pressure imposed on the microorganism environment. If more than one antibiotic type is present in microbial communities, the pressure caused by these antibiotics may lead to bacteria employing multiple drug resistance mechanisms. Thus, the bacteria will select one optimized drug resistance mechanism or increase mutational events to survive in bacterial stress situations.22,24,25
The results of the present study showed a significant association between CRKP infection and tracheotomy; frequent invasive operations may result in respiratory tract mucosal injury, increasing bacterial infection susceptibility.
In addition, older age, renal dysfunction, tracheotomy, and ICU stay were independent death risk factors in patients infected with CRKP. Older age and severe concomitant diseases lead to a decline in immunity, thereby increasing the risk of CRKP infection and even death.15
Although several independent risk factors of CRKP-induced infection and death were identified, the present study has limitations. (1) The number of included patients was relatively small; (2) risk factor omissions may be present; (3) as the present report was a single-center case-control study, selection bias was inevitable and the presented data were limited. Thus, a multicenter, large-scale study should be conducted in the future; (4) only prior infection by Kpn was tested, whereas prior colonization by such Kpn was not screened for. This study analyzed the risk factors of CSKP or CRKP infection for the first time; it did not, however, analyze the risk factors of CRKP isolated after the initial CSKP isolation. We aim to address this aspect in follow-up research. Nonetheless, according to the risk factors of CRKP infection, the long-term use of more than three antibiotics, the long-term use of carbapenems, long-term endotracheal intubation, and long-term ICU stay (for the same patient) may promote the transformation of CSKP to CRKP. Therefore, the rational use of antibiotics should be based on drug sensitivity results in clinical treatment. In addition, its use time should be shortened as much as possible, and do a good job in maintaining sterile conditions to avoid secondary CRKP infection.
Conclusion
The present study provided evidence that prior carbapenem use, the use of more than three types of antibiotics for seven or more days, tracheotomy, and ICU stay increased the risk of CRKP infection, while older age, renal dysfunction, tracheotomy, and ICU stay increased the risk of death in patients infected with CRKP. In this respect, the present findings are significant for clinicians controlling CRKP infections.
Ethics Statement
All procedures performed in the study involving human participants were in accordance with the ethical standards of the ethics committee of Beijing Shijitan Hospital, Capital Medical University (No: Sjtky11-1x-2022(22)). All patients provided written informed consent.
Acknowledgments
The authors would like to thank the patients enrolled in the study, and Dr Pan-Pan Sun and Hao Zhu for the identification and DST of pathogens.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Keynan Y, Rubinstein E. The changing face of Klebsiella pneumoniae infections in the community. Int J Antimicrob Agents. 2007;30(5):385–389. doi:10.1016/j.ijantimicag.2007.06.019
2. Singh S, Sharma A, Nag VL. Bacterial pathogens from lower respiratory tract infections: a study from Western Rajasthan. J Family Med Prim Care. 2020;9(3):1407–1412. doi:10.4103/jfmpc.jfmpc_994_19
3. MacKenzie FM, Forbes KJ, Dorai-John T, Amyes SG, Gould IM. Emergence of a carbapenem-resistant Klebsiella pneumoniae. Lancet. 1997;350(9080):783. doi:10.1016/S0140-6736(05)62567-6
4. Shanthi M, Sekar U, Arunagiri K, Sekar B. Detection of Amp C genes encoding for beta-lactamases in Escherichia coli and Klebsiella pneumoniae. Indian J Med Microbiol. 2012;30(3):290–295. doi:10.4103/0255-0857.99489
5. Sun K, Xu X, Yan J, Zhang L. Evaluation of six phenotypic methods for the detection of carbapenemases in gram-negative bacteria with characterized resistance mechanisms. Ann Lab Med. 2017;37:305–312.
6. Munoz-Price LS, Quinn JP. The spread of Klebsiella pneumoniae carbapenemases: a tale of strains, plasmids, and transposons. Clin Infect Dis. 2009;49:1739–1741. doi:10.1086/648078
7. Orsi GB, García-Fernández A, Giordano A, et al. Risk factors and clinical significance of ertapenem-resistant Klebsiella pneumoniae in hospitalised patients. J Hosp Infect. 2011;78(1):54–58. doi:10.1016/j.jhin.2011.01.014
8. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect Dis. 2009;9(4):228–236. doi:10.1016/S1473-3099(09)70054-4
9. Hussein K, Sprecher H, Mashiach T, Oren I, Kassis I, Finkelstein R. Carbapenem resistance among Klebsiella pneumoniae isolates: risk factors, molecular characteristics, and susceptibility patterns. Infect Control Hosp Epidemiol. 2009;30:666–671. doi:10.1086/598244
10. Li Y, Lv Y, Xue F, et al. [Antimicrobial susceptibility surveillance of gram-negative bacterial from Mohnarin 2011–2012]. Chin J Clin Pharmacol. 2014;30:260–277. In Chinese.
11. National Bacterial Resistance Monitoring Network, Expert Committee on Rational Drug Use, National Health and Family Planning Commission. [China Antimicrobial Resistance Surveillance System Report 2014]. China Licensed Pharm. 2016;14:3–8. In Chinese.
12. Richet HM, Mohammed J, McDonald LC, Jarvis WR. Building communication networks: international network for the study and prevention of emerging antimicrobial resistance. Emerg Infect Dis. 2001;7(2):319–322. doi:10.3201/eid0702.010235
13. Akgul F, Bozkurt I, Sunbul M, Esen S, Leblebicioglu H. Risk factors and mortality in the Carbapenem-resistant Klebsiella pneumoniae infection: case control study. Pathog Glob Health. 2016;110(7–8):321–325. doi:10.1080/20477724.2016.1254976
14. Vardakas KZ, Matthaiou DK, Falagas ME, Antypa E, Koteli A, Antoniadou E. Characteristics, risk factors and outcomes of carbapenem-resistant Klebsiella pneumoniae infections in the intensive care unit. J Infect. 2015;70(6):592–599. doi:10.1016/j.jinf.2014.11.003
15. Jiao Y, Qin Y, Liu J, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization and predictors of mortality: a retrospective study. Pathog Glob Health. 2015;109:68–74. doi:10.1179/2047773215Y.0000000004
16. Thol F, Ganser A. Treatment of relapsed acute myeloid leukemia. Curr Treat Options Oncol. 2020;21(8):66. doi:10.1007/s11864-020-00765-5
17. Tsakris A, Kristo I, Poulou A, et al. Evaluation of boronic acid disk tests for differentiating KPC-possessing Klebsiella pneumoniae isolates in the clinical laboratory. J Clin Microbiol. 2009;47:362–367. doi:10.1128/JCM.01922-08
18. Franklin C, Liolios L, Peleg AY. Phenotypic detection of carbapenem-susceptible metallo-beta-lactamase-producing gram-negative bacilli in the clinical laboratory. J Clin Microbiol. 2006;44(9):3139–3144. doi:10.1128/JCM.00879-06
19. Gregory CJ, Llata E, Stine N, et al. Outbreak of carbapenem-resistant Klebsiella pneumoniae in Puerto Rico associated with a novel carbapenemase variant. Infect Control Hosp Epidemiol. 2010;31(05):476–484. doi:10.1086/651670
20. Ghebremedhin B. Extended-Spectrum-Betalaktamasen (ESBL): gestern ESBL - heute ESBL, Carbapenemase-Bildner und multiresistente Bakterien [Extended-spectrum of beta-lactamases (ESBL): yesterday ESBL: and today ESBL, carbapenemase-producing and multiresistant bacteria]. Dtsch Med Wochenschr. 2012;137(50):2657–2662. In German. doi:10.1055/s-0032-1327341
21. Orsi GB, Bencardino A, Vena A, et al. Patient risk factors for outer membrane permeability and KPC-producing carbapenem-resistant Klebsiella pneumoniae isolation: results of a double case–control study. Infection. 2013;41(1):61–67. doi:10.1007/s15010-012-0354-2
22. Gómez Rueda V, Zuleta Tobón JJ. Risk factors for infection with carbapenem-resistant Klebsiella pneumoniae: a case-case-control study. Colomb Med. 2014;45:54–60. doi:10.25100/cm.v45i2.1417
23. Candevir Ulu A, Kurtaran B, Inal AS, et al. Risk factors of carbapenem-resistant Klebsiella pneumoniae infection: a serious threat in ICUs. Med Sci Monit. 2015;21:219–224. doi:10.12659/MSM.892516
24. Baquero F, Negri MC, Morosini MI, Blázquez J. Antibiotic-selective environments. Clin Infect Dis. 1998;27(Suppl 1):S5–11. doi:10.1086/514916
25. Sacks D, Baxter B, Campbell BCV, et al.; From the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of Interventional Radiology (SIR), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO). Multisociety consensus quality improvement revised consensus statement for endovascular therapy of acute ischemic stroke. Int J Stroke. 2018;13(6):612–632. doi:10.1177/1747493018778713.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.