Back to Journals » International Journal of Women's Health » Volume 18
The Ripple Effect: A Serial Mediation Analysis of Multimorbidity and Depressive Symptoms Among Women in Midlife in China
Authors Li Y, Feng J, Yang H, Zi D
Received 22 March 2026
Accepted for publication 3 June 2026
Published 8 June 2026 Volume 2026:18 611098
DOI https://doi.org/10.2147/IJWH.S611098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Yixin Li,1,2 Jianmin Feng,3 Hanlin Yang,2 Dan Zi2
1The First Clinical College, Zunyi Medical University, Zunyi, People’s Republic of China; 2Department of Gynecology, Guizhou Provincial People’s Hospital, Guiyang, People’s Republic of China; 3School of Public Health, Guizhou Medical University, Guiyang, People’s Republic of China
Correspondence: Dan Zi, Department of Gynecology, Guizhou Provincial People’s Hospital, No. 83, Zhongshan East Road, Nanming District, Guiyang City, Guizhou Province, 550002, People’s Republic of China, Email [email protected]
Purpose: Multimorbidity is a primary risk factor for depressive symptoms, particularly among women in midlife. Guided by stress process theory, this study investigated the underlying mechanisms of this association by testing a serial mediation model involving functional limitations, self-rated health, and life satisfaction.
Methods: This study conducted a secondary analysis using data from the fifth wave of the China Health and Retirement Longitudinal Study (CHARLS)-2020. The final analysis included 4,106 women aged 45– 60 years. Multimorbidity was defined as a self-reported diagnosis of two or more out of 14 chronic somatic conditions, and depressive symptoms were assessed using the Center for Epidemiological Studies-Depression (CES-D) scale. The serial mediation analysis was conducted in SPSS using the PROCESS macro via bootstrapping.
Results: The prevalence of multimorbidity and depressive symptoms among women in midlife was 10.35% and 41.50%, respectively. Our findings highlight a specific cascade of effects, where functional limitations, self-rated health, and life satisfaction serially and partially mediated the association between multimorbidity and depressive symptoms (total effect c=1.206, 95% CI=0.986 to 1.426; direct effect c′=0.421, 95% CI=0.220 to 0.622; total indirect effect ab=0.785, 95% CI=0.655 to 0.918). However, life satisfaction alone showed no significant mediating effect on the association between multimorbidity and depressive symptoms (a3b3=0.046, 95% CI: − 0.022 to 0.113). Among the seven mediation pathways, self-rated health accounted for the largest mediation effect of the total effect (30.60%), followed by functional limitations (14.26%) and a combination of self-rated health and life satisfaction (8.04%).
Conclusion: Our findings offer a comprehensive insight into the complex relationship between multimorbidity and depressive symptoms through various mediating mechanisms under a well-developed theoretical framework. These findings hold significant implications for the prevention and intervention efforts for depressive symptoms among women in midlife, underscoring the pivotal role of alleviating functional limitations, improving self-rated health, and enhancing life satisfaction.
Plain Language Summary: Why was this Study Done?
Women in midlife often face “multimorbidity”, a well-known risk factor for depression, yet we do not fully understand the step-by-step process of how physical illness leads to mental health challenges. Our team wanted to map the pathway between these conditions to identify where doctors and family members can best provide support.
What did the Researchers do and Find?
We analyzed data from over 4,100 women in China aged 45 to 60. We looked at how their chronic illnesses affected their daily physical abilities, how they viewed their own health, and how satisfied they felt with their lives.
Our study found that:Over 41% of the women experienced symptoms of depression.Physical illness does not just impact mood directly; it creates a “domino effect.” Chronic conditions often lead to functional limitations (difficulty with daily tasks), which causes women to view their health more poorly, eventually lowering their overall life satisfaction.How a woman feels about her health (her self-rated health) was the most powerful factor linking chronic illness to depression.
What do these Results Mean?
These findings show that supporting the mental health of women in midlife requires more than just treating physical symptoms. To prevent depression, healthcare providers and policy-makers should focus on:Helping women maintain their physical independence in daily life.Providing psychological support to improve how women perceive their own well-being.Creating programs that boost general life satisfaction.
By addressing these “middle steps”, we can help break the link between physical illness and emotional distress.
Keywords: multimorbidity, depressive symptoms, functional limitations, self-rated health, life satisfaction, serial mediation
Introduction
Multimorbidity, defined as the co-existence of two or more chronic conditions, is a prevalent and growing global health challenge.1 A recent meta-analysis of 126 studies from 54 countries showed that the pooled prevalence of multimorbidity was 37.2% (95% CI: 34.9–39.4%), with the disease burden varying significantly across different geographic regions, over time, and by factors such as age and gender.2 Multimorbidity results from the interaction and combination of multiple contributors, including biological and demographic factors, lifestyle and behavioral factors, and social and environmental factors.3 Multimorbidity not only negatively impacts an individual’s well-being through increased disability and decreased quality of life, but also imposes a significant social burden due to reduced productivity, increased health care utilization, and additional strain on caregivers.4
While multimorbidity is generally considered an aging disease, research suggests that it starts a decade earlier (around 45 years and older) in developing countries than in developed countries, steeply rising in midlife and plateauing in the elderly.5 Global systematic reviews estimate the pooled prevalence of multimorbidity in community settings at approximately 33.1%.6 Midlife women are especially vulnerable to multimorbidity, with prevalence rates exceeding 25% in the United States7 and reaching 29.8% in India—a figure that increases sharply with age.8 Hormonal shifts, including decreased estrogen, trigger metabolic changes that elevate the risk for osteoporosis, hypertension, diabetes, and cardiovascular disease.9 Additionally, socio-economic and cultural barriers, including financial strain and gendered societal roles (eg, housework and caregiving roles), exacerbate stress and impede healthcare access, further increasing their risk of multimorbidity.10
Multimorbidity is a major risk factor for depressive symptoms. Individuals with multimorbidity are two to three times more likely to experience depressive symptoms than those without chronic conditions, with prevalence rates estimated at 12.8–21% compared to just 3.9–4.7% in healthy populations.11,12 The risk of depressive symptoms from multimorbidity is significantly higher for women than for men, with approximately 35% to 43% of middle-aged women reporting elevated depressive symptoms.13 Furthermore, the presence of multimorbidity significantly increases the odds of both developing and worsening these symptoms.14 Women in midlife face a “window of vulnerability” where perimenopausal hormonal shifts and multimorbidity converge to drive a high prevalence of depressive symptoms.15 The cumulative physical and emotional burden of managing chronic conditions often leads to significant emotional distress.16 Biologically, multimorbidity-induced chronic inflammation can alter brain function and neurotransmitter systems, further elevating depressive risks.17 These physiological challenges are often compounded by concurrent psychosocial stressors, such as career transitions, financial strain, “empty nest syndrome,” and caregiving responsibilities.8
The link between multimorbidity and depressive symptoms can be explained by multiple biological and psychosocial drivers.18 Research indicates that functional limitations, including limitations in activities of daily living (ADLs) and instrumental ADLs (IADLs), act as significant mediators in the link between multimorbidity and depressive symptoms.19 Higher multimorbidity is associated with worsening disability and functional decline over time, which in turn increases the risk of depressive symptoms.20 Apart from functional limitations, multimorbidity also impacts an individual’s subjective perception of health and well-being, leading to decreased self-rated health and lower life satisfaction, which, in turn, contribute to more depressive symptoms.21 Living with multiple chronic conditions and managing the symptoms can alter a person’s self-perception from “healthy” to “ill,” negatively impacting their overall satisfaction with life.18,21 Such a decreased subjective sense of wellness further causes emotional exhaustion and psychological distress, leading to an increased risk of depressive symptoms.18,21
Although the association between multimorbidity and depressive symptoms is well-demonstrated, the underlying mechanism driving this relationship remains less understood. Guided by Stress Process Theory,22 this study posits that multimorbidity acts as a primary stressor that triggers a “cascade” of secondary stressors and psychological appraisals. Specifically, we examine the complex interactions between functional limitations (representing objective physical impact), self-rated health (the subjective perception of health), and life satisfaction (the global cognitive-evaluative appraisal). Most previous studies examined these relationships in isolation, without integrating all five variables in a single model. This fragmented approach may hinder a comprehensive understanding of the dynamic system encompassing physical, mental, objective, and subjective variables. Furthermore, while research often focuses on older adults or the general population, relatively less attention has been devoted to women in midlife. This understudied subgroup is at a particularly high risk of both multimorbidity and depressive symptoms.
To fill the research gaps, this study aimed to test a serial mediation model of the association between multimorbidity and depressive symptoms, mediated by functional limitations, self-rated health, and life satisfaction, among women in midlife. We propose a serial mediation model grounded in the following evidence-based sequence. First, aligning with Verbrugge and Jette’s23 Disablement Process Model, somatic multimorbidity is conceptualized as the primary pathology that acts as an antecedent to functional limitations. Second, these functional restrictions are posited to drive self-rated health, as individuals primarily utilize their physical functioning capacity to formulate this cognitive summary of their health status.24 Third, drawing on the “Bottom-Up” Theory of Subjective Well-Being,25 we hypothesize that self-rated health represents a domain-specific evaluation that contributes directly to global life satisfaction. Finally, we frame the relationship between life satisfaction and depressive symptoms through the lens of resource erosion,26 where the depletion of global well-being serves as a proximal risk factor for depressive symptomatology. Based on this framework, we proposed the following hypotheses:
H1 (Total Effect): Multimorbidity was positively associated with depressive symptoms among women in midlife. H2 (Serial Mediation): Functional limitations, self-rated health, and life satisfaction serially mediated the link between multimorbidity and depressive symptoms.
Materials and Methods
Data Source and Participants
This study is a secondary analysis of data acquired from the fifth wave of the China Health and Retirement Longitudinal Study (CHARLS), 2020.27 CHARLS is a nationally representative survey of Chinese residents aged 45 and older conducted by Peking University to examine the health, economic, and social adjustments that the country’s aging population undergoes.27 The national baseline survey was conducted in 2011–2012, involving 17,708 participants from 150 county-level units across 28 provinces, using a multistage, stratified area-probability cluster sampling design. The follow-up surveys were conducted every two or three years, with wave 2 in 2013, wave 3 in 2015, wave 4 in 2018, and wave 5 in 2020. For this study, we used wave 5 data from two separate datasets: “demographic and background” (n = 19,395) and “health status and function” (n = 19,367). These datasets were merged, and information on 19,367 individuals was acquired. As this study focused on women in midlife, we excluded male participants (n = 3,903) and those aged younger than 45 or older than 60 years (n = 10,876), resulting in 4,588 eligible participants. We further excluded participants with missing data on multimorbidity (n=0), depressive symptoms (n=481), functional limitations (n=0), self-rated health (n=0), and life satisfaction (n=1), leading to a final analytic sample of 4,106 participants (Figure 1).
 |
Figure 1 Study Flowchart of Participant Selection. Notes: This flowchart illustrates the systematic selection process for study participants based on the China Health and Retirement Longitudinal Study (CHARLS) 2020 Survey. Starting with an initial sample of 19,367 participants, individuals were excluded if they were outside the target age range (younger than 45 or older than 59 years, n = 10,876) or identified as male (n = 3,903). Of the remaining 4,588 target participants, 482 individuals were further excluded due to missing data regarding depression (n = 481) and life satisfaction (n = 1). No participants were excluded for missing data on multimorbidity, functional limitations, or self-rated health. The final analytic sample consisted of 4,106 participants. |
Ethical Considerations
This study involves the secondary analysis of de-identified data from the CHARLS. Ethical approval for all CHARLS waves was granted by the Institutional Review Board at Peking University (IRB approval numbers: IRB00001052-11015 for the main household survey and IRB00001052-11014 for the biomarker collection). All participants were interviewed face-to-face by trained professional researchers using structured questionnaires, and informed consent was obtained from all participants. The data are publicly available to registered users, and details about the CHARLS data are available on its website (http://charls.pku.edu.cn/en).27 In accordance with the national legislation of China—specifically Items 1 and 2 of Article 32 of the “Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects” (issued February 18, 2023)28—the current secondary analysis is exempt from additional local institutional ethics committee review. This exemption applies because the research uses legally obtained, de-identified public data and poses no risk to subjects.
Measurements
Multimorbidity
Multimorbidity was assesses by a self-reported question (Code: DA003) “Have you been diagnosed with the following diseases by a doctor?” on a list of 15 chronic noncommunicable diseases: 1) hypertension, 2) dyslipidemia (elevation of low-density lipoprotein, triglycerides, and total cholesterol, or a low high density lipoprotein level, 3) diabetes or high blood sugar, 4) cancer or malignant tumor (excluding minor skin cancers), 5) chronic lung diseases, such as chronic bronchitis and emphysema (excluding tumors, or cancer), 6) liver disease (except fatty liver, tumors, and cancer), 7) heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems, 8) stroke, 9) kidney disease (except for tumor or cancer), 10) stomach or other digestive diseases (except for tumor or cancer), 11) emotional, nervous, or psychiatric problems, 12) memory-related disease (dementia and brain atrophy), 13) Parkinson’s disease, 14) arthritis or rheumatism, 15) asthma (excluding lung diseases). One point was assigned for a “yes” response and zero points for a “no” response to each disease question. To avoid conceptual overlap with the outcome variable (depressive symptoms), the item regarding “emotional, nervous, or psychiatric problems” was excluded from the multimorbidity count. The final score represents somatic multimorbidity, ranging from 0 to 14, with higher scores indicating greater multimorbidity. Participants were further classified into three subgroups based on the multimorbidity score: no morbidity (score=0), single morbidity (score=1), and multimorbidity (score≥2). Multimorbidity was defined as the simultaneous presence of two or more chronic non-communicable diseases. This threshold was chosen to align with the World Health Organization’s standard definition29 and is consistent with the methodology of prior studies using the CHARLS dataset.30 This ensures the comparability of our results with existing literature on the prevalence and burden of multimorbidity in China.
Functional Limitations
Functional limitations were measured using a custom measure combining ADL31 and IADL32 difficulties. The ADL scale included six items: dressing, bathing, eating, getting in/out of bed, using the toilet, and controlling urination/defecation. The IADL scale included six items: doing household chores, preparing hot meals, shopping for groceries, managing money, making phone calls, and taking medications. Each item was scored on a four-point Likert scale: 1 (“don’t have any difficulty”), 2 (“have difficulty but can still do it”), 3 (“have difficulty and need help”), and 4 (“can’t do it”) points. Scores were summed to create a composite index ranging from 12 to 48, with higher scores indicating more severe functional limitations. The scale demonstrated good internal consistency in the current study, with a Cronbach’s alpha coefficient of 0.85. Furthermore, item-total correlations were all above 0.40, supporting the unidimensionality of the combined ADL/IADL measure.
Self-Rated Health
Self-rated health was assessed using the single-item question from the CHARLS questionnaire (Code: DA001): “Would you say your health is very good, good, fair, poor, or very poor?” Participants responded on a 5-point scale: 1 (Very good), 2 (Good), 3 (Fair), 4 (Poor), to 5 (Very poor). For the analysis, these responses were reverse-coded so that higher scores indicate better self-rated health.
Life Satisfaction
Life satisfaction was assessed using the single-item question from the CHARLS questionnaire (Code: DC026):
Please think about your life as a whole. How satisfied are you with it? Are you completely satisfied, very satisfied, somewhat satisfied, not very satisfied, or not at all satisfied?
Responses were recorded on a 5-point scale: 1 (Completely satisfied), 2 (Very satisfied), 3 (Somewhat satisfied), 4 (Not very satisfied), and 5 (Not at all satisfied). For the analysis, these responses were reverse-scored (range: 1–5) and treated as a continuous variable, with higher values indicating greater life satisfaction.
Depressive Symptoms
Depressive symptoms were measured using the 10-item short form of the Center for Epidemiological Studies Depression Scale (CES-D10).33 The CES-D10 is a screening tool for current depressive symptomatology and does not constitute a clinical diagnosis. It includes 10 items asking participants about the frequency of symptoms or behaviors they experienced during the past week, eg., feeling bored, depressed, or fearful. Each item is rated on a four-point Likert scale ranging from 0 “rarely or none of the time,” to 3 “most or all of the time.” Two items (“I felt hopeful about the future” and “I was happy”) were reverse-scored. The total score ranges from 0 to 30, with a higher score indicating more depressive symptoms. Participants with a score of 10 and above were defined as having depressive symptoms. This threshold was chosen to align with the standard definition adopted by the developer and is consistent with the methodology of prior studies using the CHARLS dataset.34 The scale demonstrated good internal consistency in the current study, with a Cronbach’s alpha coefficient of 0.80.
Covariates
To ensure confounding was adequately addressed, we used a theory-driven approach to select covariates. We adjusted for a comprehensive set of potential confounders identified in prior literature, encompassing sociodemographic and lifestyle characteristics.3 Socio-demographic characteristics included age (years), marital status (not married/married), education (primary and below/middle and above), employment status (yes/no), and place of residence (rural/urban). Lifestyle characteristics included exercise (yes/no), insomnia with sleep length <6 hours (yes/no), alcohol use history (yes/no), and smoking history (yes/no).
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables were described using means ± standard deviations (SDs), while categorical variables were presented as frequencies (proportions). Correlations between multimorbidity, functional limitations, self-rated health, life satisfaction, and depressive symptoms were analyzed using Pearson’s correlations. The serial mediation model was tested using the SPSS PROCESS macro (Version 4.2, Model 6), which allows for the simultaneous estimation of multiple indirect effects with bootstrapped confidence intervals.35 We set multimorbidity (X) as the independent variable, depressive symptoms (Y) as the dependent variable, and functional limitations, self-rated health, and life satisfaction as three consecutive mediators, while accounting for all sociodemographic and lifestyle characteristics as covariables. To test the significance of the mediated effects, we utilized a non-parametric bootstrapping procedure with 5,000 resamples. This method generates bias-corrected confidence intervals (CIs) for the indirect effect and does not assume normality of the sampling distribution of the indirect effect.36 A random seed was set to ensure reproducibility of the bootstrap resampling. Both unstandardized (B) and standardized (β) coefficients were computed to report the magnitude of the effects. The mediation effect was considered significant if the 95% bootstrap confidence interval (CI) did not include zero. It is important to note that while the PROCESS macro allows for the estimation of direct and indirect associations using nonparametric bootstrapping, the cross-sectional design of this study precludes the determination of causality or temporal ordering among variables.
To ensure the independence of our mediators, we tested for multicollinearity using Variance Inflation Factors (VIF). All VIF values were below 5 (Range: 1.01–1.86), confirming that the mediators represent distinct constructs and that multicollinearity did not bias the model estimates. Prior to interpreting the mediation effects, we verified the assumptions of the general linear model for each constituent regression equation. Visual inspection of scatterplots of standardized residuals against standardized predicted values revealed random scatter with no evidence of nonlinearity or heteroscedasticity (non-constant variance). Normal P-P plots and histograms confirmed that the residuals were normally distributed. These diagnostics confirm that the model assumptions for the mediation analysis were met.
A p-value of less than 0.05 was used as the standard level of significance (two-sided tests). All estimates were reported by applying appropriate sampling weights.
Results
Sample Characteristics
As shown in Table 1, the final analytic sample of 4,106 participants was predominantly composed of women aged 50 and older (76.33%), the majority of whom were married (92.01%) and lived in rural areas (61.81%). Significant differences in depression scores were observed across nearly all sociodemographic and lifestyle categories. Specifically, higher depression scores were observed in individuals who were older (aged ≥ 50), not married, less educated, or living in rural areas (all p < 0.001). Regarding lifestyle factors, individuals reporting insomnia, non-alcohol use, and smoking exhibited substantially higher depression scores compared to their respective counterparts (all p < 0.01). Conversely, employment status and physical activity did not reach the threshold for statistical significance.
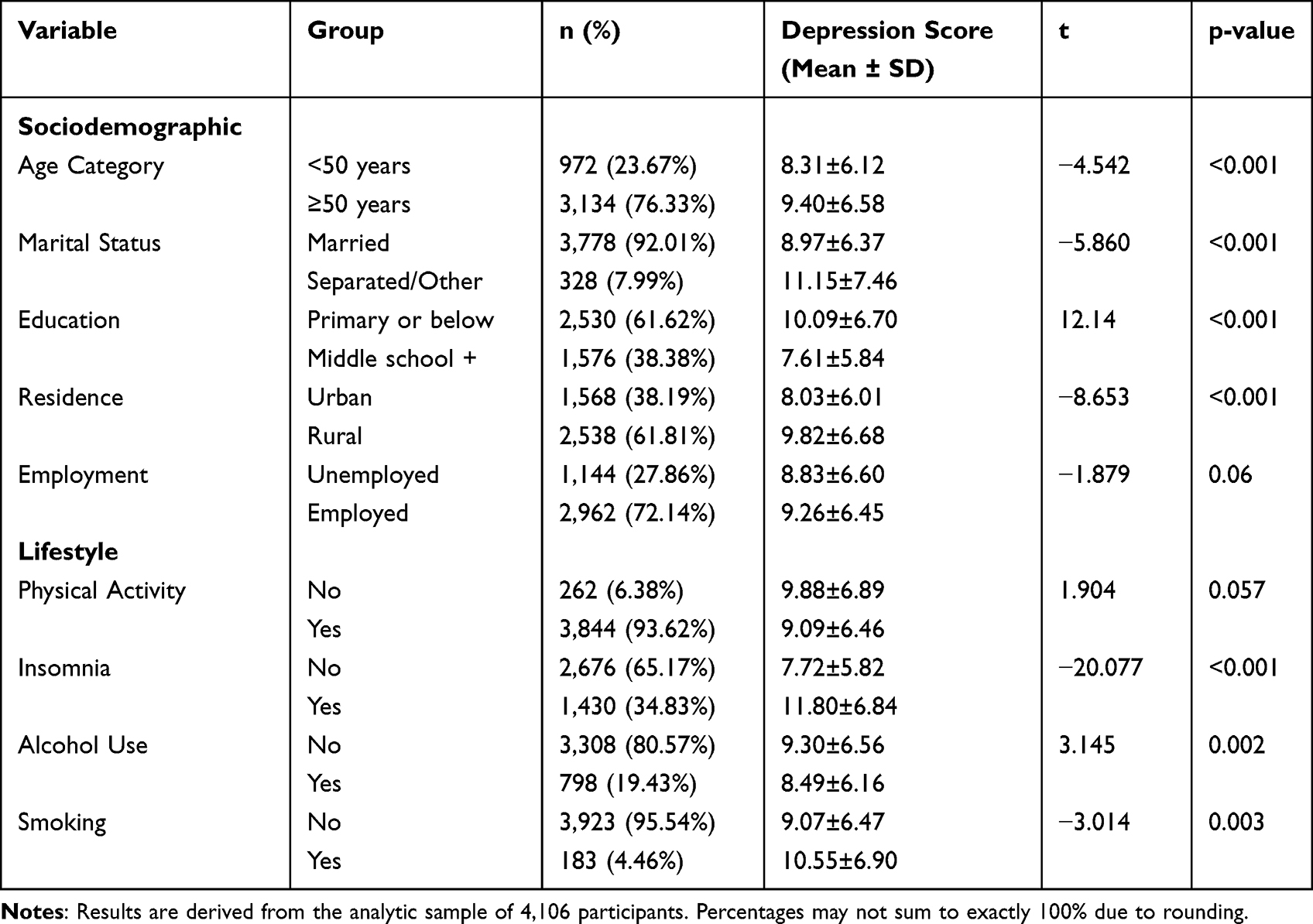 |
Table 1 Depression Scores Stratified by Sociodemographic and Lifestyle Characteristics (n = 4,106) |
Table 2 shows the prevalence of individual somatic conditions and distribution of multimorbidity scores. Among the 14 somatic conditions, the top four most prevalent conditions were dyslipidemia (8.79%), arthritis (7.45%), hypertension (6.26%), and stomach diseases (6.14%). Regarding disease burden, 66.05% reported no somatic conditions, 23.60% had a single somatic condition, and 10.35% had multimorbidity.
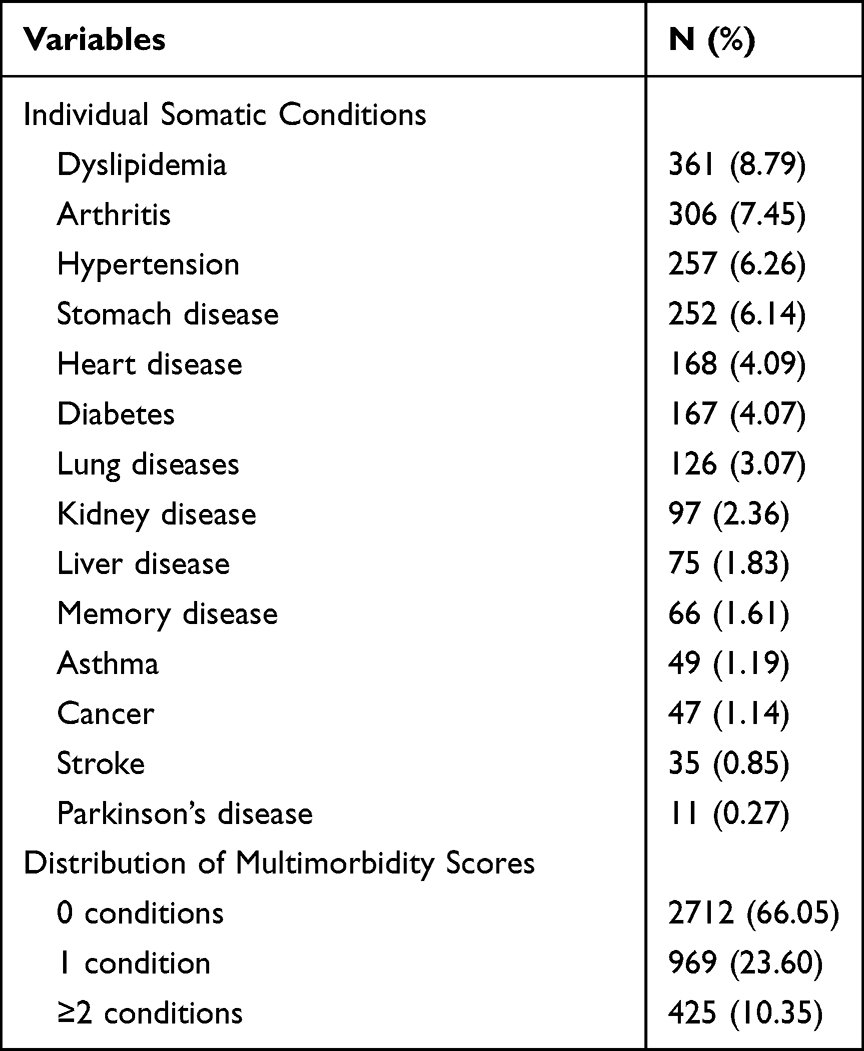 |
Table 2 Prevalence of Individual Somatic Conditions and Distribution of Multimorbidity Scores |
Correlation Analysis
Table 3 shows the descriptive statistics and correlation analysis of the key study variables. In this sample, the average CES-D10 score was 9.14 ± 6.49, with 41.50% of participants scoring 10 or higher, indicating elevated depressive symptoms. The mean scores for multimorbidity, functional limitations, self-rated health, and life satisfaction were 0.49 ± 0.83, 12.89 ± 2.56, 3.08 ± 1.02, and 3.22 ± 0.80, respectively. All four variables demonstrated significant correlations with each other. Specifically, multimorbidity was positively correlated with depressive symptoms (r=0.18, p<0.001) and functional limitations (r=0.15, p<0.001), while negatively correlated with self-rated health (r=−0.27, p<0.001) and life satisfaction (r=−0.10, p<0.001). Depressive symptoms were positively correlated with multimorbidity (r=0.18, p<0.001) and functional limitations (r=0.33, p<0.001), while negatively correlated with self-rated health (r=−0.41, p<0.001) and life satisfaction (r=−0.38, p<0.001). In addition, the three mediators — functional limitations, self-rated health, and life satisfaction — were significantly correlated with each other (r = −0.17, −0.32, 0.27, all p < 0.001).
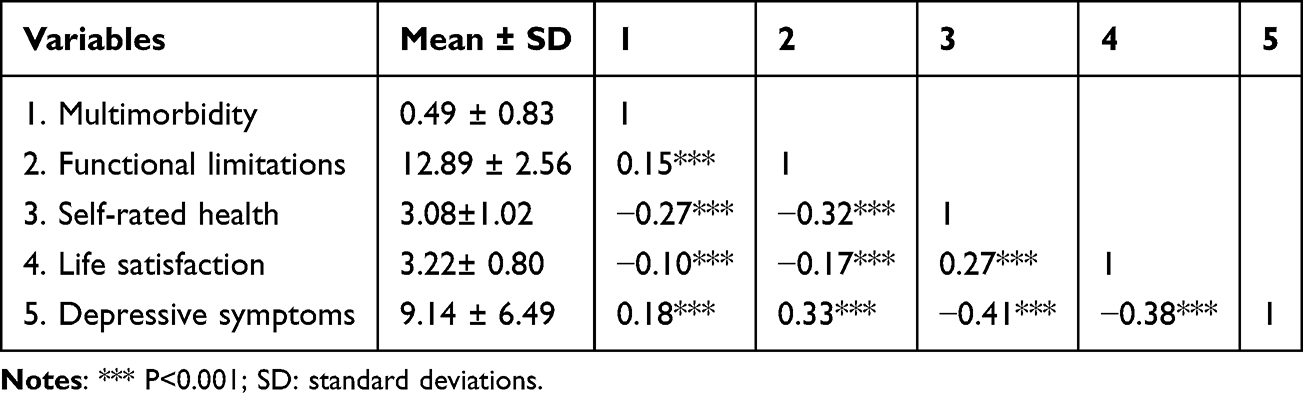 |
Table 3 Descriptives and Correlation Analysis of Key Variables |
Serial Mediation Analysis
Figure 2 and Table 4 outline the total, direct, and indirect effects of multimorbidity on depressive symptoms, which are mediated through functional limitations, self-rated health, and life satisfaction. The total effect of multimorbidity on depressive symptoms was significant (c=1.206, 95% CI=0.986 to 1.426). When three mediators were added, the direct effect of multimorbidity on depressive symptoms decreased but remained significant (c′=0.421, 95% CI=0.220 to 0.622). Functional limitations, self-rated health, and life satisfaction serially mediated the association between multimorbidity and depressive symptoms, with a total indirect effect of 0.785 (95% CI=0.655 to 0.918). Two mediators, functional limitations and self-rated health, mediated the association between multimorbidity and depressive symptoms, as represented by corresponding mediator paths (a1b1=0.172, 95% CI: 0.106 to 0.246; a2b2=0.369, 95% CI: 0.299 to 0.443). Notably, life satisfaction alone showed no significant mediation effect in the association between multimorbidity and depressive symptoms (a3b3=0.046, 95% CI: −0.022 to 0.113), primarily because the direct link from multimorbidity to life satisfaction was not statistically significant. However, life satisfaction did serve as a significant indirect mediator as part of a serial chain. Specifically, significant indirect effects were observed for pathways through functional limitations followed by life satisfaction (a1d31b3=0.024, 95% CI: 0.012 to 0.039), and through self-rated health followed by life satisfaction (a2b32b3=0.097, 95% CI=0.076 to 0.122). Higher multimorbidity was associated with more functional limitations, which further led to lower self-rated health and then lower life satisfaction, thus contributing to depressive symptoms. Among the seven mediation pathways, self-rated health accounted for the largest proportion of the total effect (30.60%), followed by functional limitations (14.26%) and a combination of self-rated health and life satisfaction (8.04%).
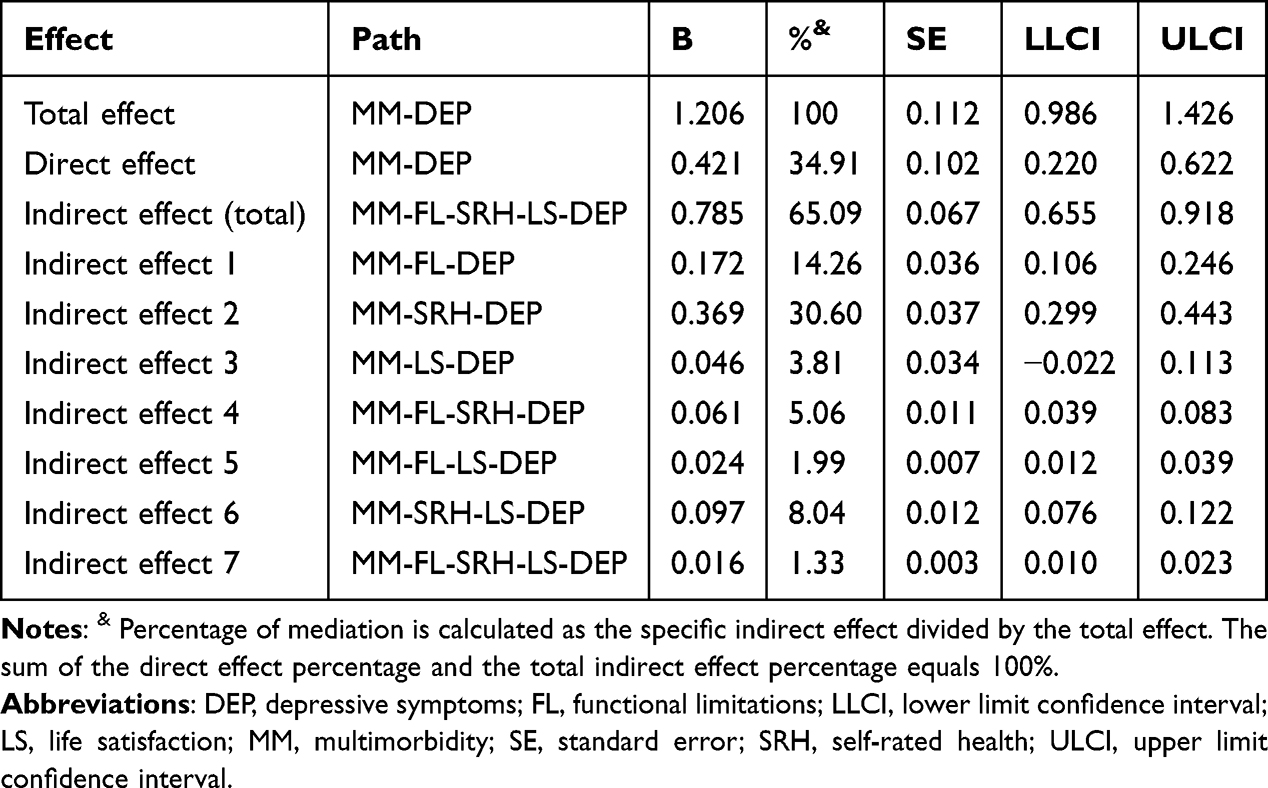 |
Table 4 Total, Direct, and Indirect Effects of the Serial Mediation Model |
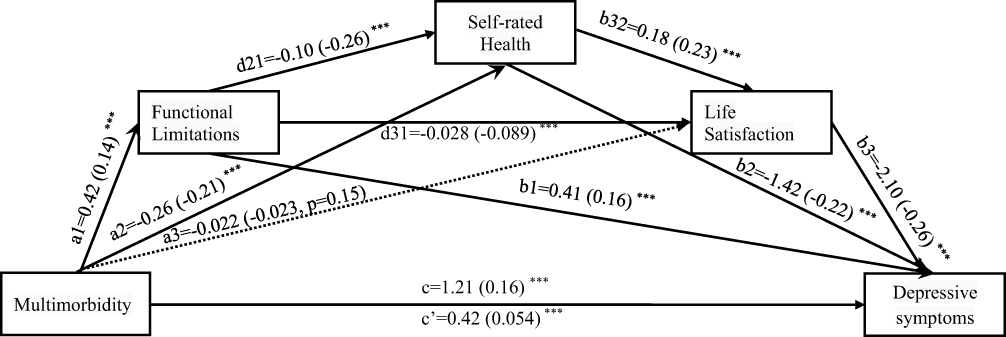 |
Figure 2 Serial Mediation Model of the Relationship Between Multimorbidity and Depressive Symptoms. Notes: This schematic diagram illustrates the direct and indirect effects of multimorbidity on depressive symptoms, with functional limitations, self-rated health, and life satisfaction acting as serial mediators. The numbers on the paths represent the unstandardized coefficients, with standardized coefficients provided in parentheses. Solid lines indicate statistically significant paths (***p < 0.001), while dashed lines indicate non-significant paths (e.g., the path from multimorbidity to life satisfaction, p = 0.15). The total effect is represented by c, and the direct effect after controlling for mediators is represented by c′. All models are adjusted for relevant covariates. |
Discussion
Summary of the Findings
Using a nationally representative sample and driven by the stress process theory, our study examined the association between multimorbidity and depressive symptoms among women in midlife and the serial mediating roles of functional limitations, self-rated health, and life satisfaction. We found that 10.67% of participants had multimorbidity, while 41.50% had depressive symptoms. Multimorbidity was positively associated with depressive symptoms both directly and indirectly through functional limitations, self-rated health, and life satisfaction, with self-rated health accounting for the largest mediation effect. Our findings suggest that multimorbidity and depressive symptoms are complexly linked through a range of objective and subjective pathways. Objective pathways relate to tangible physical effects, such as functional limitations, while subjective pathways involve a person’s perceptions and emotional responses, including self-rated health and life satisfaction. These findings provide important implications for future comprehensive and targeted interventions to integrate mental and physical healthcare to decrease the negative impacts of multimorbidity and prevent depressive symptoms among women in midlife.
Multimorbidity and Depressive Symptoms
Our study showed a prevalence of 10.35% for multimorbidity, which was lower than most previous studies reporting rates of 30% to over 70% among women in their mid-to-late 40s and 60s.6 The observed lower estimate in our study is likely an artifact of the “diagnosed by a doctor” criterion used in the survey. Given that 61.81% of our sample resides in rural areas where healthcare access is often limited, it is probable that a significant number of chronic conditions remain undiagnosed. Previous research comparing self-reported data with objective biomarkers has consistently demonstrated that reliance on medical diagnosis underestimates the true prevalence of chronic conditions, particularly in populations with lower healthcare utilization.37 Therefore, our reported figure should be explicitly interpreted as the prevalence of diagnosed multimorbidity, which likely underestimates the true biological burden of disease in this population.
Despite low multimorbidity, participants in our study presented a high prevalence of depressive symptoms at 41.50%, higher than the range of 26% to 35.6% in various global and regional contexts.6,38 While the timing of data collection during the COVID-19 pandemic likely contributed to elevated stress,39 methodological factors must also be considered. First, the CES-D 10 is a screening tool based on a 1-week recall period, designed to capture current psychological distress rather than diagnose clinical depression; such screening tools typically yield higher prevalence rates than diagnostic interviews.40 Second, the use of listwise deletion to handle missing data may have introduced selection bias, potentially retaining a sample with distress profiles that differ from those excluded due to incomplete responses.41 Importantly, our study consistently demonstrated a robust positive association between multimorbidity and depressive symptoms among women in midlife, further confirming the well-documented relationship supported by substantial research.12,42,43 A meta-analysis concluded that people with multimorbidity were two to three times more likely to become depressed than those with no chronic physical conditions, and each additional chronic condition increased the risk of depressive symptoms by 45%.12 Our findings underscore the importance of routine depressive symptoms screenings for women in midlife with multimorbidity to initiate timely and effective interventions and advocate for integrated care that addresses both physical and mental health.
The Serial Mediating Effect of Functional Limitations, Self-Rated Health, and Life Satisfaction
Our study supports a serial mediation model and identified a specific pathway explaining how multimorbidity was associated with depressive symptoms among women in midlife.22 The statistical model suggests that functional limitations, self-rated health, and life satisfaction may serve as intermediary factors in the relationship between somatic multimorbidity and depression, though longitudinal data are required to confirm this temporal sequence. Our findings support the trajectory proposed by the stress process theory, where the impact of multimorbidity (primary stressor) cascades through functional limitations (secondary stressor) and self-rated health (subjective appraisal) to life satisfaction and depressive symptoms. This suggests that the physical restrictions imposed by multiple chronic conditions shape how individuals perceive their general health, which in turn dictates their overall psychological well-being. Our findings indicate that multimorbidity acts as a primary stressor for women in midlife, who often face the complex task of managing multiple diseases, symptoms, treatments, and side effects.16 Consistent with the Stress Process Theory,22 chronic stress from multimorbidity is associated with functional limitations, which prevent individuals from performing daily activities due to physical or mental impairments, creating a primary source of subjective stress. Furthermore, the experience of functional decline and the accumulating burden of disease may contribute to a negative self-assessment of one’s overall health and poorer self-rated health.44 As observed in our model, this decline in health perception is associated with a negative overall assessment of one’s life and lower life satisfaction. Finally, the erosion of life satisfaction due to the cascading effect of multimorbidity, functional decline, and poor self-rated health is a significant driver of depressive symptoms.21
Notably, among the multiple mediation pathways, self-rated health was identified as exerting the largest mediation effect in the association between multimorbidity and depressive symptoms. This finding was consistent with a previous study showing that self-rated health acted as a potent mediator between physical health conditions and depressive symptoms.45 Self-rated health captures both objective and subjective health factors that influence mental well-being.46 These findings underscore that how people feel about their health—their subjective perception—can be a more immediate and powerful driver of depressive symptoms than objective clinical diagnoses alone.47 Self-rated health provides a holistic measure that reflects the cumulative burdens of multimorbidity on a person’s mental state, including financial strain, caregiver burden, and decreased social participation.48 In addition, self-rated health is influenced by psychosocial factors, such as personality traits, resilience, and coping, which also directly affect individuals’ vulnerability to depressive symptoms.49 This finding underscores the crucial importance of a patient-centered approach to managing multimorbidity. Clinicians may use self-reported health as a routine and cost-effective screening tool to identify high-risk patients to initiate early, targeted psychosocial interventions for depressive symptoms.
By identifying the sequential steps in the association between multimorbidity and depressive symptoms, our study provides a more comprehensive and nuanced understanding of the psychological toll of multimorbidity. It reveals the complex interrelationships between multimorbidity and depressive symptoms through both objective (functional limitations) and subjective (self-rated health and life satisfaction) pathways. Our findings regarding the association between multimorbidity and psychological well-being align with a growing body of literature identifying psychosocial resources as key mechanisms in this pathway. Recent research utilizing robust empirical designs has begun to unpack these mediating processes. For instance, internal psychological resources, such as positive affect, has been identified as a key mediator of the link between multimorbidity and depressive symptoms.50 Taken together with our current results, this suggests that interventions targeting both objective and subjective pathways may be effective in mitigating the adverse mental health effects of multimorbidity.
Limitations
This study has several limitations. First, a cross-sectional study design cannot establish causal relationships among variables, and previous research suggests bidirectional interrelationships among these variables.51,52 Future longitudinal study designs are needed to clarify temporal relationships further and understand the dynamic nature of how variables interact over time. Second, the use of single-item questions for complex, multidimensional concepts, such as self-rated health and life satisfaction, can compromise the reliability and validity of the findings. Future studies should use validated multi-item questionnaires to obtain a more robust and comprehensive assessment of these concepts. Third, the reliance on self-reported data is subject to recall and social desirability biases, which may affect the reliability of the findings. Future research should consider combining self-report with objective measures, such as direct observation, tracking devices, or biomarkers, to achieve a more accurate assessment. Fourth, our study only included three mediators in the link between multimorbidity and depression, and there may be other potential factors playing a role in their association. Future studies can explore alternative mediating variables across biological, psychological, social, and functional domains to build a more comprehensive model of the relationship.
Conclusions
Our findings offer a comprehensive insight into the complex relationship between multimorbidity and depressive symptoms among women in midlife through various mediating mechanisms under a well-developed theoretical framework. Multimorbidity was positively associated with depressive symptoms both directly and indirectly through functional limitations, self-rated health, and life satisfaction. These findings yield critical insights for clinical, research, and political endeavors to address the negative impacts of multimorbidity and alleviate depressive symptoms among women in midlife, emphasizing the crucial role of mitigating functional limitations, improving self-rated health, and enhancing life satisfaction. Future longitudinal studies with more comprehensive assessments, including objective measures and alternative variables, are needed to validate our models further.
Data Sharing Statement
The CHARLS study data are publicly available and open to researchers worldwide. Our study is a secondary analysis conducted using the CHARLS public data. The CHARLS dataset is accessible at http://charls.pku.edu.cn/.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki, and ethical approval for CHARLS was granted by the Institutional Review Board at Peking University. The IRB approval number for the main household survey, including anthropometrics, is IRB00001052-11015; the IRB approval number for biomarker collection is IRB00001052-11014. All participants provided informed consent at the time of participation and were informed about and consented to the secondary analysis of the survey results. In accordance with the national legislation of China—specifically Items 1 and 2 of Article 32 of the “Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects” (issued February 18, 2023)—the current secondary analysis is exempt from additional local institutional ethics committee review. This exemption applies because the research uses legally obtained, de-identified public data and poses no risk to subjects.
Acknowledgments
The authors are grateful to the China Health and Retirement Longitudinal Study (CHARLS) for assembling and publishing nationally representative data on a range of high-quality public micro-databases from socioeconomic status to health conditions, to serve the needs of scientific research on the elderly. The authors are also grateful to CHARLS’s partner, the Institute of Social Science Survey of Peking University, Beijing, China, for data collection and fieldwork. The authors would also express their sincere thanks to all the participants and families involved in the study for their time and for sharing their life experiences and feelings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by a grant from the Guizhou Provincial Science and Technology Plan Project, Guizhou Science and Technology Foundation-ZK (2024)-452; ZK (2022)-270; ZK (2024)-465, and Guizhou Provincial Health Commission Science and Technology Fund Project (2024GZWJKJXM1253), in support of the corresponding author, Dr. Dan Zi.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Chua YP, Xie Y, Lee PSS, Lee ES. Definitions and prevalence of multimorbidity in large database studies: a scoping review. Int J Environ Res Public Health. 2021;18(4):1673. doi:10.3390/ijerph18041673
2. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
3. Alvarez-Galvez J, Ortega-Martin E, Carretero-Bravo J, et al. Social determinants of multimorbidity patterns: a systematic review. Front Public Health. 2023;11:1081518. doi:10.3389/fpubh.2023.1081518
4. Cabral GG, Dantas de Souza AC, Barbosa IR, Jerez-Roig J, Souza DLB. Multimorbidity and its impact on workers: a review of longitudinal studies. Saf Health Work. 2019;10(4):393–14. doi:10.1016/j.shaw.2019.08.004
5. Mohanty SK, Rodgers J, Singh RR, et al. Morbidity compression or expansion? A temporal analysis of the age at onset of non-communicable diseases in India. Geroscience. 2021;43(1):409–422. doi:10.1007/s11357-020-00296-9
6. Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorb. 2019;9:2235042X19870934. doi:10.1177/2235042X19870934
7. Watson KB, Wiltz JL, Nhim K, et al. Trends in multiple chronic conditions among US adults, by life stage, Behavioral Risk Factor Surveillance System, 2013-2023. Prev Chronic Dis. 2025;22:E15. doi:10.5888/pcd22.240539
8. Puri P, Sinha A, Mahapatra P, Pati S. Multimorbidity among midlife women in India: well-being beyond reproductive age. BMC Womens Health. 2022;22(1):117. doi:10.1186/s12905-022-01693-2
9. Jeong HG, Park H. Metabolic disorders in menopause. Metabolites. 2022;12(10):954. doi:10.3390/metabo12100954
10. Temkin SM, Barr E, Moore H, Caviston JP, Regensteiner JG, Clayton JA. Chronic conditions in women: the development of a National Institutes of Health framework. BMC Womens Health. 2023;23(1):162. doi:10.1186/s12905-023-02319-x
11. Pundhir A, Naveen K, Harbishettar V, et al. A systematic review and meta-analysis of the global prevalence of depression in older adults with multi-morbidity. Indian J Psychol Med. 2025. doi:10.1177/02537176251403605
12. Read JR, Sharpe L, Modini M, Dear BF. Multimorbidity and depression: a systematic review and meta-analysis. J Affect Disord. 2017;221:36–46. doi:10.1016/j.jad.2017.06.009
13. Jia Y, Zhou Z, Xiang F, Hu W, Cao X. Global prevalence of depression in menopausal women: a systematic review and meta-analysis. J Affect Disord. 2024;358:474–482. doi:10.1016/j.jad.2024.05.051
14. Zheng Y, Lin P, Zhao L, et al. Multimorbidity is significantly associated with higher prevalence of depressive symptoms in middle-aged and older Chinese adults. Prev Med Rep. 2025;60:103289. doi:10.1016/j.pmedr.2025.103289
15. Sassarini DJ. Depression in midlife women. Maturitas. 2016;94:149–154. doi:10.1016/j.maturitas.2016.09.004
16. Bobo WV, Grossardt BR, Virani S, et al. Association of depression and anxiety with the accumulation of chronic conditions. JAMA Network Open. 2022;5(5):e229817. doi:10.1001/jamanetworkopen.2022.9817
17. Jiang C, Yin H, Liu A, et al. Dietary inflammatory index and depression risk in patients with chronic diseases and comorbidity. J Affect Disord. 2022;301:307–314. doi:10.1016/j.jad.2022.01.008
18. Triolo F, Harber-Aschan L, Belvederi Murri M, et al. The complex interplay between depression and multimorbidity in late life: risks and pathways. Mech Ageing Dev. 2020;192:111383. doi:10.1016/j.mad.2020.111383
19. Ansari S, Anand A, Hossain B. Multimorbidity and depression among older adults in India: mediating role of functional and behavioural health. PLoS One. 2022;17(6):e0269646. doi:10.1371/journal.pone.0269646
20. Wang S, Yu M, Huang W, Wang T, Liu K, Xiang B. Longitudinal association between ADL disability and depression in middle-aged and elderly: national cohort study. J Nutr Health Aging. 2025;29(2):100450. doi:10.1016/j.jnha.2024.100450
21. Garcia Perez A, Villanueva Gutierrez T. Multimorbidity and depressive symptoms and their association with self-reported health and life satisfaction among adults aged ≥ 50 years in Mexico. J Cross Cult Gerontol. 2025;40(1):107–121. doi:10.1007/s10823-025-09521-4
22. Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. J Health Soc Behav. 1981;22(4):337–356. doi:10.2307/2136676
23. Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38(1):1–14. doi:10.1016/0277-9536(94)90294-1
24. Idler EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997;38(1):21–37. doi:10.2307/2955359
25. Diener E. Subjective well-being. Psychol Bull. 1984;95(3):542–575. doi:10.1037/0033-2909.95.3.542
26. Hobfoll SE. Conservation of resources. A new attempt at conceptualizing stress. Am Psychol. 1989;44(3):513–524. doi:10.1037/0003-066X.44.3.513
27. Zhao Y, Strauss J, Chen X, et al. China Health and Retirement Longitudinal Study Wave 4 User’s Guide. Beijing: National School of Development, Peking University; 2020.
28. National Health Commission of the People’s Republic of China. Measures for ethical review of life science and medical research involving human subjects.
29. World Health Organization. Multimorbidity: Technical Series on Safer Primary Care. Geneva: World Health Organization; 2016.
30. Zhong Y, Qin G, Xi H, et al. Prevalence, patterns of multimorbidity and associations with health care utilization among middle-aged and older people in China. BMC Public Health. 2023;23(1):537. doi:10.1186/s12889-023-15412-5
31. Wade DT, Collin C. The Barthel ADL Index: a standard measure of physical disability? Int Disabil Stud. 1988;10(2):64–67. doi:10.3109/09638288809164105
32. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. doi:10.1093/geront/9.3_Part_1.179
33. Kohout FJ, Berkman LF, Evans DA, Cornoni-Huntley J. Two shorter forms of the CES-D (Center for Epidemiological Studies Depression) depression symptoms index. J Aging Health. 1993;5(2):179–193. doi:10.1177/089826439300500202
34. Li H, Liu X, Zheng Q, Zeng S, Luo X. Gender differences and determinants of late-life depression in China: a cross-sectional study based on CHARLS. J Affect Disord. 2022;309:178–185. doi:10.1016/j.jad.2022.04.059
35. Hayes AF. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
36. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. doi:10.3758/brm.40.3.879
37. Vellakkal S, Subramanian SV, Millett C, et al. Socioeconomic inequalities in non-communicable diseases prevalence in India: disparities between self-reported diagnoses and standardized measures. PLoS One. 2013;8(7):e68219. doi:10.1371/journal.pone.0068219
38. Ps A, Das S, Philip S, et al. Prevalence of depression among middle aged women in the rural area of Kerala. Asian J Psychiatr. 2017;29:154–159. doi:10.1016/j.ajp.2017.05.016
39. Wang Y, Kala MP, Jafar TH. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: a systematic review and meta-analysis. PLoS One. 2020;15(12):e0244630. doi:10.1371/journal.pone.0244630
40. Thombs BD, de Jonge P, Coyne JC, et al. Depression screening and patient outcomes in cardiovascular care: a systematic review. JAMA. 2008;300(18):2161–2171. doi:10.1001/jama.2008.667
41. Little RJ. Missing data analysis. Annu Rev Clin Psychol. 2024;20(1):149–173. doi:10.1146/annurev-clinpsy-080822-051727
42. Zhang Y, Cheng Y, Carrillo-Larco RM, et al. Postpartum depression in relation to chronic diseases and multimorbidity in women’s mid-late life: a prospective cohort study of UK Biobank. BMC Med. 2025;23(1):24. doi:10.1186/s12916-025-03853-1
43. Chen XY, Zhou Y, Qing LX, et al. Multimorbidity incidence among middle-aged and elderly Chinese women with depression in CHARLS 2020: interaction of urban-rural differences (STROBE). Medicine. 2025;104(26):e43083. doi:10.1097/MD.0000000000043083
44. Straatmann VS, Vetrano DL, Fratiglioni L, Calderon-Larranaga A. Disease or function? What matters most for self-rated health in older people depends on age. Aging Clin Exp Res. 2020;32(8):1591–1594. doi:10.1007/s40520-020-01507-1
45. Jang Y, Yoon H, Li M, et al. Self-rated health as a mediator between physical health conditions and depressive symptoms in older Chinese and Korean Americans. PLoS One. 2021;16(1):e0245136. doi:10.1371/journal.pone.0245136
46. Jung NH, Lee CY. Subjective and objective health according to the characteristics of older adults: using data from a national survey of older Koreans. Medicine. 2024;103(47):e40633. doi:10.1097/MD.0000000000040633
47. Boehme S, Geiser C, Renneberg B. Functional and self-rated health mediate the association between physical indicators of diabetes and depressive symptoms. BMC Fam Pract. 2014;15:157. doi:10.1186/1471-2296-15-157
48. Ando T, Nishimoto Y, Hirata T, et al. Association between multimorbidity, self-rated health and life satisfaction among independent, community-dwelling very old persons in Japan: longitudinal cohort analysis from the Kawasaki Ageing and Well-being Project. BMJ Open. 2022;12(2):e049262. doi:10.1136/bmjopen-2021-049262
49. Kang W. Personality predicts self-rated health: considering age differences. Front Psychol. 2023;14:1143077. doi:10.3389/fpsyg.2023.1143077
50. Demirer I, Kuhhirt M, Karbach U, Pfaff H. Does positive affect mediate the association of multimorbidity on depressive symptoms? Aging Mental Health. 2022;26(1):65–76. doi:10.1080/13607863.2020.1870209
51. Qiao Y, Liu S, Zhang Y, et al. Bidirectional association between depression and multimorbidity in middle-aged and elderly Chinese adults: a longitudinal cohort study. Aging Mental Health. 2022;26(4):784–790. doi:10.1080/13607863.2021.1877609
52. Joshanloo M, Blasco-Belled A. Reciprocal associations between depressive symptoms, life satisfaction, and eudaimonic well-being in older adults over a 16-year period. Int J Environ Res Public Health. 2023;20(3):2374. doi:10.3390/ijerph20032374
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Perceived Community Services for the Elderly on Self-Rated Health: An Analysis Utilizing a Mediated Latent Growth Model
Jiang M, Yao Y, Xia X, Kong Y, Zhang N
Journal of Multidisciplinary Healthcare 2024, 17:4383-4396
Published Date: 7 September 2024
Relieving Depressive Symptoms Through Chinese Relational Culture Among Older Adults with Multimorbidity: Evidence from CHARLS
Duan XY, Sun T, Lu F, Yang XJ, Yin HY, Cao DP, Zhang SE
Psychology Research and Behavior Management 2024, 17:4331-4344
Published Date: 17 December 2024