Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
The relationship of individual social activity and cognitive function of community Chinese elderly: a cross-sectional study
Authors Su X, Huang X, Jin Y, Wan S, Han Z
Received 16 December 2017
Accepted for publication 24 April 2018
Published 24 August 2018 Volume 2018:14 Pages 2149—2157
DOI https://doi.org/10.2147/NDT.S160036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Wai Kwong Tang
Xiufang Su,1 Xingbing Huang,2 Yu Jin,3 Shouwen Wan,4 Zili Han5
1Department of Psychiatry, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2The Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital), Guangzhou, People’s Republic of China; 3Faculty of Maternal and Child Health, School of Public Health, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 4Guangzhou Dr Su Health Industry (Group) Co., Ltd, Guangzhou, People’s Republic of China; 5Department of Psychiatry, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, People’s Republic of China
Background: The prevention of cognitive impairment is a crucial public health issue, and leisure activities have been studied as the strategy of the cognitive preservation. The aim of the study was to explore the possible relationship between social activity and cognitive function among community-dwelling Chinese elderly in two big cities of Southern China.
Participants and methods: Altogether, 557 nondemented older adults aged 60 years and older (73.4±6.5 years) were recruited in the social centers in Hong Kong and Guangzhou. A leisure activity questionnaire was used to measure the social activity participation. Cognitive function was examined using a neuropsychological battery. The association between social activity and cognitive function was analyzed using the multiple linear regression analysis.
Results: Social activities had a weak relationship with cognitive performance when measured in terms of overall participation. Attending an interest class had significant association with the Cantonese version of Mini Mental State Examination, the word list learning test, the delayed recall test, and the trail making test. Religious activity showed significant association with the word list learning test and the digit vigilance test. Singing had significant association with the Category Verbal Fluency Test (CVFT) and the trail making test.
Conclusion: Some individual social activity items may be associated with better cognitive function among the community Chinese elderly independently of other factors.
Keywords: social activity, cognitive function, Chinese elderly
Introduction
Cognitive impairment among older adults has long been a hot topic with population aging. It represents a tremendous burden on patients, families, and society. Cognitive function can be influenced by various factors, including age, gender, education level, marital status, and socioeconomic status. It is better to find an effective strategy for the prevention or delay of cognitive impairment. Increasing evidence has demonstrated that lifestyle leisure activity may have beneficial effect on the preservation of cognitive function.1–4
Social activity is considered to be another feature of an active lifestyle, alongside with physical and cognitive activities. It is demonstrated that social activity is beneficial for various health outcomes, including physical health status, mental health status, and quality of life.5–7 Individuals can improve their self-esteem, competence, and obtain meaningful social roles through participation in social activity.8,9 Social activity can improve cognitive reserve (CR) capacity by the effect of intellectual stimulation.10,11 Furthermore, it has the effect of emotional stimulation, which can reduce cognitive impairment.11
However, due to the heterogeneity in the measurement of social activity and cognitive function, the findings on social activity and cognitive function are not consistent. Some studies have found that social activity may have profound protective effect on cognitive function.12 A previous study12 estimated the association between social activity and cognitive decline in a sample of 1,138 nondemented older adults and the results showed that higher levels of social participation may be helpful for the prevention of cognitive decline, with 5.2 years of follow-up period. On the contrary, some studies showed that social activity might not have profound favorable effect on cognitive preservation.2,13 Iwasa et al2 found no significant association between social activity (volunteering and group activities for the elderly) and cognitive decline in 567 adults older than 70 years. Similarly, a 3-year longitudinal study failed to find the protective effect of social activity on the prevention of cognitive decline.13
Some investigators have suggested that the inconclusive results may be related to different statistical techniques. However, even those who use similar statistical methods tend to report inconsistent results. Brown et al14 analyzed four studies using a coordinated data analysis methods and found that baseline social activity was related to some specific cognitive domain and could not predict the rate of cognitive decline. Some researchers have argued that when estimating the possible effect of social activity on cognitive function, the interaction between physical, intellectual, and social activities should be considered, as many leisure activities contain all these three components. A study by Paillard-Borg et al15 revealed that each component (cognitive, physical, and social) was equally important in protecting against dementia. Hence, there is the possibility of the effects of social activity on cognitive function depending on the stage of cognitive decline: dementia16 or mild cognitive impairment.17
Some studies indicated that cultural background and natures of social activities should be considered when exploring the relationship of social activity and cognitive function, because it is possible that only some specific types of social activity have favorable effect on cognitive function. For example, in Asia, the tradition of piety culture and familism and the poor welfare system that makes the types of social activity benefit for cognitive preservation among the elderly are different from the western world. However, the evidence on the relationship of special types of social activity and cognitive function is limited. A Chinese study showed that playing mahjong, chess, or card games, meeting with friends, and joining a social center have more profound beneficial effect on the episodic memory than other types of social activity.18 A 20-year Swedish follow-up study manifested that prior political activities or mental activities are related to better late-life cognitive function, but activities in organization are not.19
Overall, these studies manifested that many questions on the special effect of social activity on cognitive preservation need to be answered. Most of the studies on social activity were limited to single measure of cognitive function. In the present study, we examined the association between social activity and different cognitive domains among the community-dwelling Chinese adults in the two biggest cities in southern China using a validated checklist. We also conducted the study to explore the characteristics of the relationship of individual social activity and cognitive function, with a view to find which types of social activity may have the advantages in the cognitive preservation among the Chinese elderly.
Participants and methods
Participants
The investigation was a part of one PhD project of the Chinese University of Hong Kong and conducted from August 2010 to October 2011. Altogether, 602 older adults aged 60 years and older were randomly selected and informed by the staffs of the neighborhood social centers in the two cities (322 adults in Guangzhou and 280 adults in Hong Kong) and 27 older adults refused to participate. Five hundred and seventy-five older adults finished the cognitive examination (307 adults in Guangzhou and 268 adults in Hong Kong), and 18 adults were screened as dementia (10 adults in Guangzhou and eight adults in Hong Kong). Finally, 557 older adults (297 adults in Guangzhou and 260 adults in Hong Kong) finished the whole interview (Figure 1).
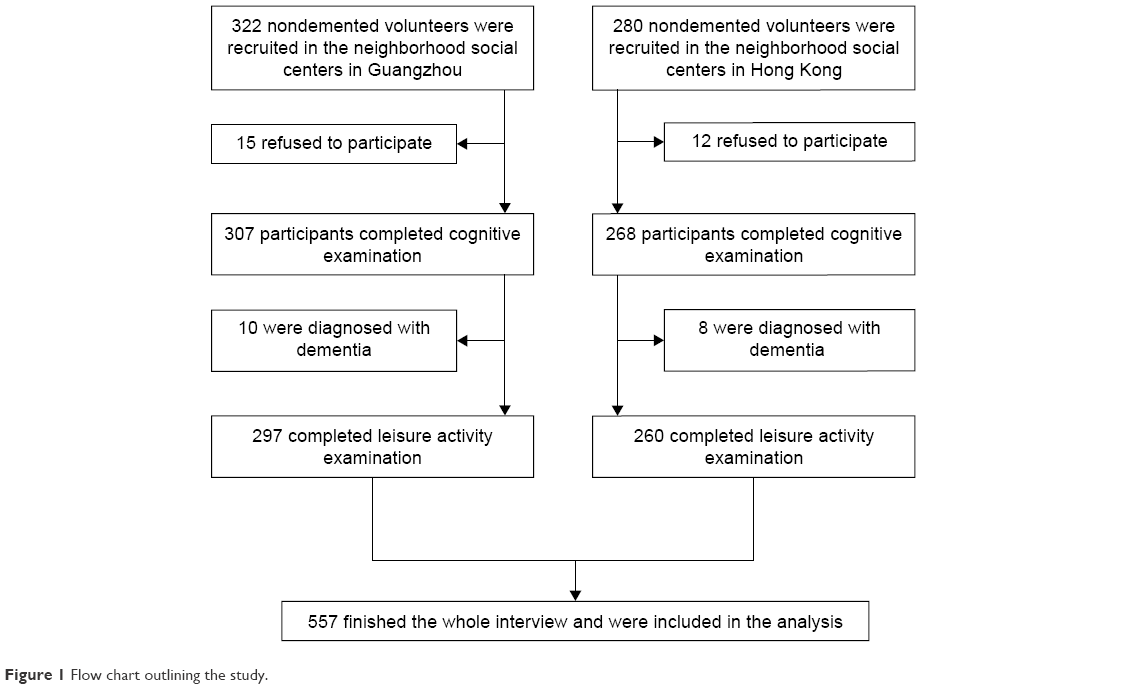 | Figure 1 Flow chart outlining the study. |
The exclusion criteria were as follows: dementia, living in old age homes, greatly impaired communication and language abilities, bed bound, unstable physical conditions, history of primary neurodegenerative disorder, known history of psychotic disorder, and substance misuse.20 The participants were invited to the community social centers and underwent the face-to-face interviews. Socio-demographic information was collected using a questionnaire, including age, gender, education, occupation, marital status, living arrangement, drinking status, and smoking status. Information on leisure activity participation and cognitive function was obtained using a standardized checklist and a battery of cognitive assessment tools. All the participants signed the written consent form before the interview. The study was approved by the Ethics Committees of the Chinese University of Hong Kong.
Assessment
Cognitive assessment
A cognitive test battery was adopted to assess the different cognitive domains of the elderly,20 including the Cantonese version of Mini Mental State Examination,21 the word list learning test and the delayed recall test from the Chinese version of the Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-Cog),22 the Category Verbal Fluency Test (CVFT),23 the trail making test,24 the digit vigilance test,25 and the Stroop test.26
Social activity assessment
Leisure activities were defined as activities in which individuals engage for enjoyment or well-being and are independent of work or the activities of daily living.27 A validated leisure checklist was adopted to assess social activity participation, which was developed by Leung et al.1 In the checklist, leisure activities were classified as physical, intellectual, social, and recreational categories. A focus group comprising elderly care professionals, an independent panel of occupational therapists in the field of geriatrics and psychiatry, and a convenience sample of community elderly has helped with the identification and categorization of leisure activity. The participants were asked whether they pursued any types of social activities in the past year (Table 1). Activities participated at the frequencies of less than monthly were excluded, as suggested by the previous studies.1,4 The levels of participation were measured in the following two ways: total hours per week and total number of individual items.20
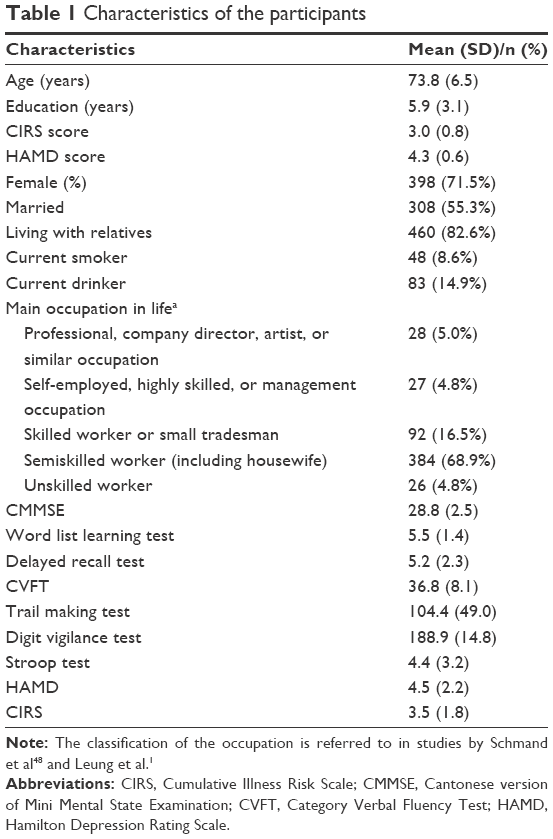 | Table 1 Characteristics of the participants |
Assessment of other variables
Participation in the other three categories of activities was examined using the same leisure activity checklist. These categories of leisure activities are intellectual activity (reading, writing, painting, calligraphy, using computer, playing mahjong or card games, gambling, participating in forums, handicraft, and playing a musical instrument), social activity (attending an interest class, joining a social center, participating in volunteer work, going to museums, exhibitions, theatres or concerts, meeting with relatives or friends, performing drama or Chinese opera, singing, and attending religious activities), and recreational activity (watching television and listening to the radio, listening to music, shopping, cooking for pleasure, fishing, keeping plants or pets, and facials or massage).20 The participation was assessed in terms of total hours per week and total number of individual items. Hamilton Depression Rating Scale (HAMD) was used to identify the depressive symptoms of the participants. The Cumulative Illness Risk Scale (CIRS)28 was adopted to assess chronic health burdens.
Statistical analyses
The correlation between leisure activity and cognitive performance was examined using Pearson’s correlation coefficient.
Multiple linear regression analyses were conducted to explore the association between social and cognitive functions. The dependent variables were the scores of cognitive examination. The independent variable was total number and total hours of social activity. The multiple linear regression models examined the independent association between total numbers of social activity, and total hours of social activity and cognitive function with engagement in the other three categories of activity were adjusted. Potential confounding factors were adjusted, including age, gender, education, occupation, marital status, living arrangement, drinking status, smoking status, HAMD score, and CIRS score.
Multiple linear regression analyses were implemented to examine the association between individual social activity items and cognitive function. The dependent variables were the scores of cognitive tests. The independent variables were individual social activity items. The individual items of the other three categories of activities and potential confounders mentioned earlier were adjusted as covariates.
The SPSS software, Version 17.0, was used to conduct the analysis. The level of statistical significance was set at P<0.05.
Results
All participants are Chinese elderly, and the demographics are given in Table 1, alongside with lifestyle factors, health status, and cognitive scores.20 Current smokers were defined as having smoked part or all of a cigarette during the past 30 days,29 and current drinkers were defined as having at least one drink of any kind of alcoholic beverage in the past year.30
Social activity profiles of the participants
Joining a social center (27.3%) and meeting with friends or relatives (25.1%) were the two most common social activities of the participants. Other activities reported less frequently attending an interest class (20.8%), volunteer work (17.8%), singing (16.5%), religious activity (8.6%), and Cantonese opera (1.3%) (Table 2).
 | Table 2 Social activity profiles of participants |
Social activity and cognitive function
Correlation analyses of the leisure activity and cognitive test showed that total number of social activity had significant correlation with the word list learning test (P<0.001), the delayed recall test (P<0.01), and the CVFT (P<0.01). Total hours of social activity had significant correlation with the word list learning test (P<0.01), the delayed recall test (P<0.001) and the CVFT (P<0.0001) (Table 3). However, with adjustment for potential confounders (age, gender, education, occupation, marital status, living arrangement, smoking status, drinking status, CIRS score, and HAMD score) and participation in other types of leisure activities, the association between social activity and cognitive function became weak. Only the total number of social activity showed small association with digit vigilance test (adjusted beta =0.12, P=0.04, 95% CI: −2.71, 0.22) (Table 4).
 | Table 3 Correlation between leisure activity and cognitive performancea |
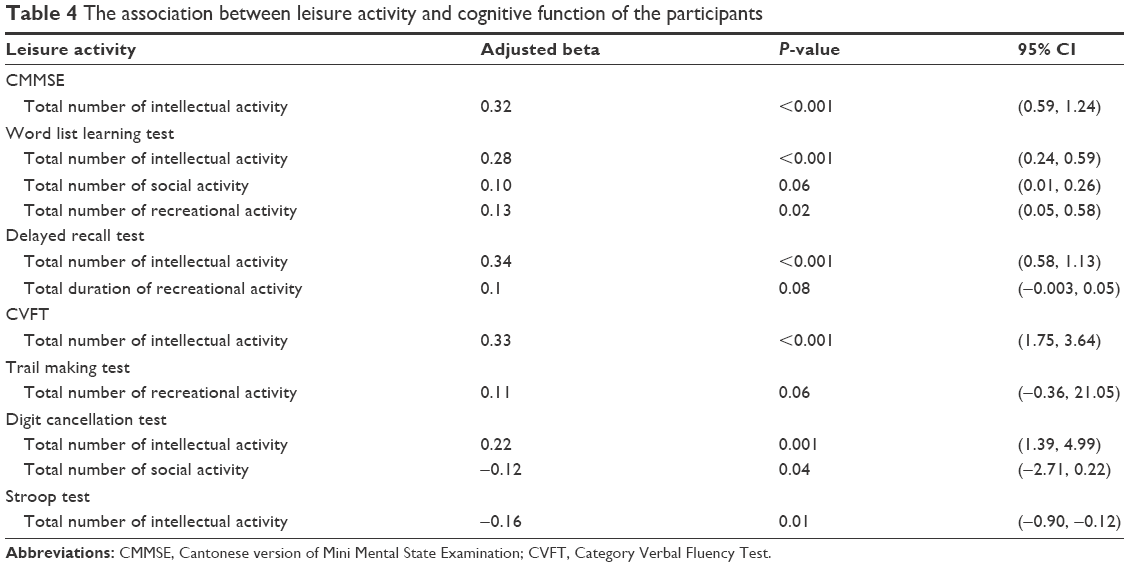 | Table 4 The association between leisure activity and cognitive function of the participants |
Multivariate linear regression showed that individual social activities, including attending an interest class, had consistent association with the cognitive tests, including the Cantonese version of Mini Mental State Examination (adjusted beta =0.19, P=0.002, 95% CI: −0.46, 1.97), the word list learning test (adjusted beta =0.17, P=0.005, 95% CI: −0.17, 1.95), the delayed recall test (adjusted beta =0.15, P=0.01, 95% CI: −0.23, 1.53), and the trail making test (adjusted beta =−0.15, P=0.01, 95% CI: −5.0, 31.39). Religious activity showed profound association with the word list learning test (adjusted beta =0.12, P=0.02, 95% CI: 0.08, 1.88) and the digit vigilance test (adjusted beta =0.20, P<0.001, 95% CI: −11.61, 3.32). Singing had statistically significant association with the CVFT (adjusted beta =0.15, P=0.02, 95% CI: −4.99, 1.55) and the trail making test (adjusted beta =−0.12, P=0.04, 95% CI: −30.84, 1.11) (Table 5).
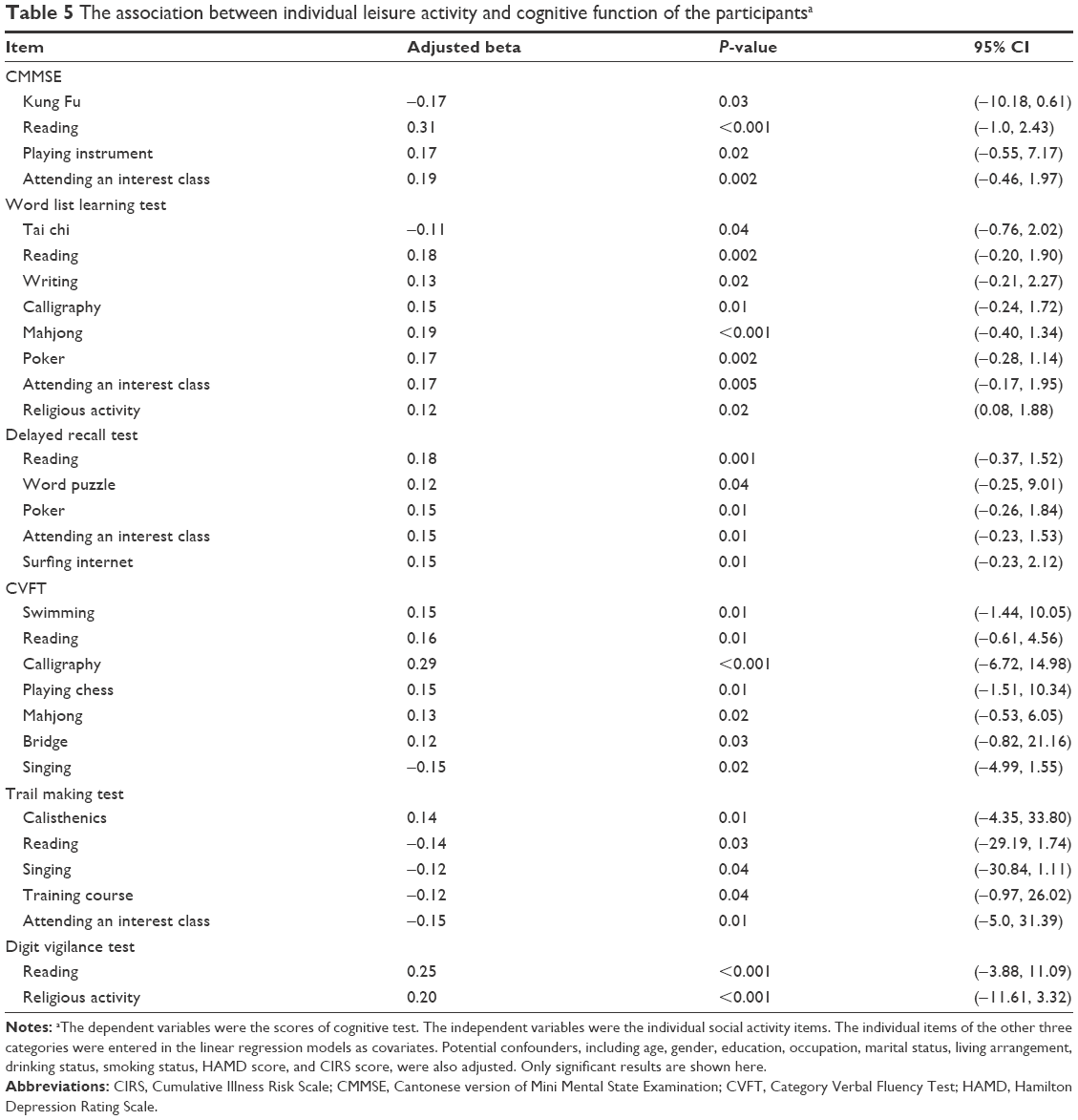 | Table 5 The association between individual leisure activity and cognitive function of the participantsa |
Discussion
This was a community-based, cross-sectional study, and all of the participants were nondemented. Our findings showed that social activities had significant relationships with the scores of some cognitive tests (word list learning test, delayed recall test, and CVFT). It seemed that the results were consistent with previous studies that social activities may be helpful for cognitive preservation.10,12 A study hypothesized that psychosocial pathways may play a role in the relationship.10 Participation in social activities may sustain the individual’s self-concept of usefulness and competence,31 which may lead to crucial health outcomes.32,33 Experimental studies on rodents also found that enriched social environment can improve the plasticity and thickness of the cerebral cortex of old rats.34 It is also possible that social active subjects may have received more material or emotional support.
However, the association became weak when potential confounders and participation in other types of activities were adjusted. Our results were consistent with the findings of some previous studies.1,2 Iwasa et al2 conducted a 5-year study among Japanese community-dwelling older adults and failed to found significant relationship. A cross-sectional study among Hong Kong community-dwelling Chinese elderly also showed that the total number of social activities only had significant association with CVFT after potential confounder and participation in other categories of activities were adjusted.1 These results implied that social activity may not have a substantial positive association with cognitive function on its own.
Some possible reasons may help to explain the soft association between social activity and cognitive function. First, intellectual activities might be confounding factors for the association between social activity and cognitive function, as there is some overlap between the components of social activities and intellectual activities. Some types of social activities may imply simultaneous cognitive activities and need to be implemented with explicit mental skills. For example, attending an interest class or training course can be cognitively demanding for older adults. A previous study manifested the confounding effect of other activities35 and revealed that the modest association between social activity and cognitive function was decreased by >50% when mental and physical activities were adjusted.
Second, it is possible that the association between social activity and intellectual activity in older aged cognitive function is confounded by prior cognitive ability; ie, those who have higher cognitive ability throughout life are more likely to engage in these sorts of activities and still have higher cognitive ability in later life.36 However, one study showed that the association between intellectual activity and cognitive function remained significant after adjustment for age, education, baseline Mini Mental State Examination (MMSE) score, and participation in other categories of activities.1 In the present study, indexes of prior cognitive ability including education level and occupation have been adjusted and the relationship between intellectual activity and cognitive function was still significant. These results imply that cognitive activities undertaken in late life is crucial. Thus, it is likely that the beneficial effect of all types of leisure activities on cognitive function is worked through the mechanism of cognitive stimulation.
To further explore the relationship between social activities and cognitive function, we assessed the association between individual social activities and cognitive function. Some important findings have been revealed in our study. The results showed that some individual types of social activities had significant relationship with cognitive function, including attending an interest class, training course, religious activity, and singing. The association was independent of age, gender, education, marital status, chronic health burden, depression symptoms, and other types of leisure activity. The results were consistent with a previous study conducted among Korea’s elderly.37 The possible explanation for the findings is that social centers can provide social interaction services, education opportunities, and recreational activities for the elderly.18,38 Education is a well-known protective factor for cognitive function. Because of the historical reasons, Chinese elderly are less educated and most of them are engaged in less cognitively challenging social activities. We speculated that attending an interest class or training courses can provide the education opportunities for the elderly to learn reading and writing or master a special skill, which provide additional cognitive stimulation and increase CR. Randomized controlled trials are needed to explore the effect of interest class or training course on cognitive function. Music is often used as an intervention strategy in rehabilitation and care of the elderly. Previous studies showed that singing had beneficial effect on the mental health and oral function of the elderly39 and singing can improve cognitive efficacy of the individuals with dementia.40 It is possible that singing involves more positive process of combining a complex sequence of words and melody in a specific order, which the singer has to memorize and thus might also provide additional cognitive stimulation. Our results revealed that religion had positive relationship with the word list leaning test and the digit vigilance test. It seems that religious activities are becoming common among Chinese elderly. Religious activities may be helpful for the elderly to relax and cope with the effects of loneliness and isolation that are so prevalent among the elderly.41 Religious activities are related to more social support, better mental, and physical status.41
Previous evidence suggested that Asians’ social activities are likely to be family oriented.7 Our results also showed that the most common social activity was meeting with relatives or friends. Older individuals may receive more emotional support protecting against cognitive decline, whereas loneliness or social isolation can worsen cognitive decline among older adults.42,43 One interesting result of our study was that meeting with relatives or friends did not have significant relationship with better cognitive function. It is possible that meeting with relatives or friends may be less cognitively demanding than other activities. It is also possible that meeting with relatives or friends only had profound effect on the cognitive function among some special group of older adults, as a previous study found that profound relationship of meeting with children and cognitive decline was only found among older-old adults.37 Further studies are needed to identify the association between social activity and cognitive function of older adults.
This study has several advantages. First, this is a fairly large and community-based study and examined the possible relationship of social activity and cognitive function among the community Chinese elderly. Second, various potential confounders have been adjusted, including socio-demographics, physical and mental health-related factors, and other categories of leisure activity. Third, participants with dementia were excluded because impaired cognitive function can lead to less social interaction and recall bias of participation. Furthermore, our findings were based on the measurement of different cognitive domains. Thus, we can know which cognitive domains have specific associations with social activities. Depression symptoms have significant association with an increased risk of cognitive impairment in later life,44 and the association was independent of age, gender, follow-up periods, and base-line cognitive function.45 The confounding effect of depression symptoms was adjusted in our study by excluding the individuals with depression.
Limitations of the study should be mentioned. The cross-sectional design is the major limitation of the study, and we cannot draw causal conclusions. Furthermore, the accurate appraisals of social activity are limited by the retrospective evaluation. Third, it is suggested that the quality of social activities is more crucial for individual’s health than quantity.46 In our study, social activity was measured by the way of frequency and duration. The important dimensions of social activities such as satisfaction and burdens were not included in the assessment. More detailed social activity scales including quantity and quality should be adopted in future study, with a view to capture more important information on the association between social activity and cognitive function. Participants in social centers may be more social active than older adults outside, which limited the generalization of the results to the other population. Hence, large population-based, randomized controlled trials are needed to explore the effect of social activity on cognitive function.
Conclusion
Despite these limitations, our results support the hypothesis that participation in social activity may be benefit for cognitive function, providing cogent proof for the special types of social activity that may prevent cognitive impairment among Chinese elderly. A recent Asian study showed that some special activities had strong association with cognitive function, including religious activity, meeting with friends, joining clubs, meeting with relatives or classmates, volunteer work, and political organizations.47 The results combined with ours suggested that the relationship of social activity and cognitive function may be influenced by social or cultural background. Our findings suggested that some individual social items had positive association with better cognitive function. The population-based randomized case–control trials should be implemented to further explore the effect of these types of social activity on cognitive function. Social activity suitable for Chinese elderly should be explored and generalized with a view to find more strategy to prevent cognitive impairment.
Acknowledgment
SW is the co-first author.
Disclosure
The authors report no conflicts of interest in this work.
References
Leung TY, Fung WT, Tam WC, et al. Examining the association between participation in late-life leisure activities and cognitive function in community-dwelling elderly Chinese in Hong Kong. Int Psychogeriatr. 2010;22(1):1–13. | ||
Iwasa H, Yoshida Y, Kai I, Suzuki T, Kim H, Yoshida H. Leisure activities and cognitive function in elderly community-dwelling individuals in Japan: a 5-year prospective cohort study. J Psychosom Res. 2012;72(2):159–164. | ||
Wang JY, Zhou DH, Li J, et al. Leisure activity and risk of cognitive impairment: the Chongqing aging study. Neurology. 2006;66(6):911–913. | ||
Niti M, Yap KB, Kua EH, Tan CH, Ng TP. Physical, social and productive leisure activities, cognitive decline and interaction with APOE-ε4 genotype in Chinese older adults. Int Psychogeriatr. 2008;20(2):237–251. | ||
James BD, Boyle PA, Buchman AS, Bennett DA. Relation of late-life social activity with incident disability among community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2011;66(4):467–473. | ||
Park HK, Chun SY, Choi Y, Lee SY, Kim SJ, Park EC. Effects of social activity on health-related quality of life according to age and gender: an observational study. Health Qual Life Outcomes. 2015;13:140. | ||
Lee SH, Kim YB. Which type of social activities decrease depression in the elderly? An analysis of a population-based study in South Korea. Iran J Public Health. 2014;43(7):903–912. | ||
Kim YB. Type of social activity and morale in later life: a comparison between male and female. Asian Women. 2009;25(4):69–85. | ||
Holtzman RE, Rebok GW, Saczynski JS, Kouzis AC, Wilcox Doyle K, Eaton WW. Social network characteristics and cognition in middle-aged and older adults. J Gerontol B Psychol Sci Soc Sci. 2004;59(6):278–284. | ||
Wang HX, Karp A, Winblad B, Fratiglioni L. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: a longitudinal study from the Kungsholmen project. Am J Epidemiol. 2002;155(12):1081–1087. | ||
Fratiglioni L, Wang HX, Ericsson K, Maytan M, Winblad B. Influence of social network on occurrence of dementia: a community-based longitudinal study. Lancet. 2000;355(9212):1315–1319. | ||
James BD, Wilson RS, Barnes LL, Bennett DA. Late-life social activity and cognitive decline in old age. J Int Neuropsychol Soc. 2011;17(6):998–1005. | ||
Green F, Rebok G, Lyketsos CG. Influence of social network characteristics on cognition and functional status with aging. Int J Geriatr Psychiatry. 2008;23(9):972–978. | ||
Brown CL, Gibbons LE, Kennison RF, et al. Social activity and cognitive functioning over time: a coordinated analysis of four longitudinal studies. J Aging Res. 2012;2013:287438. | ||
Paillard-Borg S, Fratiglioni L, Winblad B, Wang HX. Leisure activities in late life in relation to dementia risk: principal component analysis. Dement Geriatr Cogn Disord. 2009;28(2):136–144. | ||
Woods B, Aguirre E, Spector AE, Orrell M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst Rev. 2012;2:CD005562. | ||
Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr. 2013;25(4):587–595. | ||
Yuqing H, Xiaoyan L, James PS, Yaohui Z. Aging in Asia: Findings from New and Emerging Data Initiatives. Effects of Social Activities on Cognitive Functions: Evidence from CHARLS. Washington, DC: National Academies Press (US); 2012. | ||
Kåreholt I, Lennartsson C, Gatz M, Parker MG. Baseline leisure time activity and cognition more than two decades later. Int J Geriatr Psychiatry. 2011;26(1):65–74. | ||
Su XF, Lin YQ, Zhang SL, Leung GT, Chiu H, Lam LC. Physical activity and cognitive function of the community elderly Chinese in Hong Kong and Guangzhou. Int Psychogeriatr. 2015;27(6):959–966. | ||
Chiu HFK, Lee HCB, Chung WS, Kwong PK. Reliability and validity of the Cantonese version of the mini-mental state examination: a preliminary study. Hong Kong J Psychiatry. 1994;4(suppl 2):25–28. | ||
Chu LW, Chiu KC, Hui SL, Yu GK, Tsui WJ, Lee PW. The reliability and validity of the Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) among the elderly Chinese in Hong Kong. Ann Acad Med Singapore. 2000;29(4):474–485. | ||
Lam LC, Ho P, Lui VW, Tam CW. Reduced semantic fluency as an additional screening tool for subjects with questionable dementia. Dement Geriatr Cogn Disord. 2006;22(2):159–164. | ||
Reiran RM, Wolfson D. Category test and trail making test as measures of frontal lobe functions. Clin Neuropsychol. 1995;9(1):50–56. | ||
Kelland DZ, Lewis RF. The digit vigilance test: reliability, validity, and sensitivity to diazepam. Arch Clin Neuropsychol. 1996;11(4):339–344. | ||
Lee TMC, Chan CCH. Stroop interference in Chinese and English. J Clin Exp Neuropsychol. 2000;22(4):465–471. | ||
Verghese J, LeValley A, Derby C, et al. Leisure activities and the risk of amnestic mild cognitive impairment in the elderly. Neurology. 2006;66(6):821–827. | ||
Conwell Y, Forbes NT, Cox C, Caine ED. Validation of a measure of physical illness burden at autopsy, the Cumulative Illness Rating Scale. J Am Geriatr Soc. 1993;41(1):38–41. | ||
Substance Abuse and Mental Health Services Administration. National Survey on Drug Use and Health, 2008: Codebook. Rockville, MD: SAMHSA, Office of Applied Studies; 2009. Available from: http://www.gmhc.org/files/editor/file/a_pa_nat_drug_use_survey.pdf | ||
Clark WB, Hilton ME, editors. Alcohol in America: Drinking Practices and Problems. Albany, NY: State University of New York Press; 1991. | ||
Herzog AR, Franks MM, Markus HR, Holmberg D. Activities and well-being in older age: effects of self-concept and educational attainment. Psychol Aging. 1998;13(2):179–185. | ||
Mendes de Leon CF, Seeman TE, Baker DI, Richardson ED, Tinetti ME. Self efficacy, physical decline, and change in functioning in community-living elders: a prospective study. J Gerontol. 1996;51(4):S183–S190. | ||
Orth-Gomér K, Rosengren A, Wilhelmsen L. Lack of social support and incidence of coronary heart disease in middle-aged Swedish men. Psychosom Med. 1993;55(1):37–43. | ||
Powell D. Profiles in Cognitive Aging. Cambridge, MA: Harvard University Press; 1994. | ||
Krueger KR, Wilson RS, Kamenetsky JM, Barnes LL, Bienias JL, Bennett DA. Social engagement and cognitive function in old age. Exp Aging Res. 2009;35(1):45–60. | ||
Deary IJ, Gow AJ, Taylor MD, et al. The Lothian Birth Cohort 1936: a study to examine influences on cognitive ageing from age 11 to age 70 and beyond. BMC Geriatr. 2007;7:28. | ||
Lee SH, Kim YB. Which type of social activities may reduce cognitive decline in the elderly? A longitudinal population-based study. BMC Geriatr. 2016;16:165. | ||
Turner AW. Senior citizens centers: what they offer, who participates, and what they gain. J Gerontol Soc Work. 2004;43(1):37–49. | ||
Sakano K, Ryo K, Tamaki Y, et al. Possible benefits of singing to the mental and physical condition of the elderly. Biopsychosoc Med. 2014;8:11. | ||
Satoh M, Yuba T, Tabei K, et al. Music therapy using singing training improves psychomotor speed in patients with Alzheimer’s disease: a neuropsychological and fMRI study. Dement Geriatr Cogn Dis Extra. 2015;5(3):296–308. | ||
Koenig HG, George LK, Titus P. Religion, spirituality, and health in medically ill hospitalized older patients. J Am Geriatr Soc. 2004;52(4):554–562. | ||
Holtzman RE, Rebok GW, Sacynski JS, Kouzis AC, Wilcox Doyle K, Eaton WW. Social network characteristics and cognition in middle-aged and older adults. J Gerontol B Psychol Sci Soc Sci. 2004;59(6):278–284. | ||
Zunzunegui MV, Alvarado BE, Del Ser T, Otero A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J Gerontol B Psychol Sci Soc Sci. 2003;58(2):S93–S100. | ||
Erten-Lyons D, Silbert L. Depressive symptoms are associated with late life cognitive decline independent of common age-related pathologies. Evid Based Ment Health. 2015;18(2):50. | ||
Gllagher D, Kiss A, Lanctot K, Herrmann N. Depressive symptoms and cognitive decline: a longitudinal analysis of potentially modifiable risk factors in community dwelling older adults. J Affect Disord. 2106;190:235–240. | ||
Volis CI, Allaire JC, Olsen MK, Steffens DC, Hoyle RH, Bosworth HB. Five-year trajectories of social networks and social support in older adults with major depression. Int Psychogeriatr. 2007;19(6):1110–1124. | ||
Choi Y, Park S, Cho KH, Chun SY, Park EC. A change in social activity affect cognitive function in middle-aged and older Koreans: analysis of a Korean longitudinal study on aging (2006–2012). Int J Geriatr Psychiatry. 2016;31(8):912–919. | ||
Schmand B, Smit JH, Geerlings MI, Lindeboom J. The effects of intelligence and education on the development of dementia: a test of brain reserve hypothesis. Psychol Med. 1997;27(6):1337–1344. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.