Back to Journals » Patient Preference and Adherence » Volume 17
The Relationship Between Psychosocial Behavior and the Quality of Life of Male Gout Patients in Southwest China: A Cross-Sectional Study Based on an Information-Motivation-Behavioral Skills Model
Authors Wang Y ![]() , Guo X, Chen B, Chen H
, Guo X, Chen B, Chen H ![]() , Chen Y, Ma L, Liu H
, Chen Y, Ma L, Liu H
Received 27 September 2023
Accepted for publication 5 December 2023
Published 21 December 2023 Volume 2023:17 Pages 3503—3514
DOI https://doi.org/10.2147/PPA.S434875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ying Wang,1 Xin Guo,1 Bo Chen,2 Hong Chen,3 Yanling Chen,1 Ling Ma,1 Huan Liu2
1Department of Rheumatology and Immunology, West China Hospital of Sichuan University/West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Department of Rheumatology and Immunology, West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3West China School of Nursing/West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Hong Chen, West China School of Nursing/West China Hospital, Sichuan University, No. 37, Guoxue Alley, Wuhou District, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86 18980601733, Email [email protected]
Purpose: Gout is more severe in men, leading to a poor quality of life. Previous studies did not sufficiently pay attention to the quality of life and related factors in gout patients in Southwest China. This study aimed to investigate the quality of life of men with gout in Southwest China and explore the relationship between psychosocial factors and health-related quality of life from the perspective of an information-motivation-behavioral skill model.
Patients and Methods: This was a cross-sectional study conducted in the West China Hospital of Sichuan University located in Southwest China. In total, 230 male patients with gout were enrolled. The health-related quality of life of patients was assessed using the gout impact scale. The gout knowledge questionnaire was used to assess patients’ information. The positive psycap questionnaire was used to assess motivation. The gout patients’ self-management assessment scale was used to assess behavioral skills. Multiple linear regression was used to identify the factors associated with the health-related quality of life of patients.
Results: The overall mean gout impact scale score was 52.7± 15.3 (maximum possible = 100). Factors associated with the total gout impact scale score were tophi (β=0.138, P=0.050), pain (β=0.255, P< 0.001), and resiliency (β=− 0.282, P< 0.001). In addition, demographic characteristics (educational level, smoking and marital status), clinical characteristics (tophi, pain, number of attacks over half a year, and number of affected joints) and psychosocial behavior variables (resiliency, hope, disease treatment management, diet management) were associated with several dimensions of the gout impact scale.
Conclusion: The health-related quality of life of male patients with gout in Southwest China was at a medium level. We found that demographic characteristics, clinical characteristics, and psychosocial factors were associated with health-related quality of life of patients with gout. These findings can be used as a reference to improve health-related quality of life of patients with gout.
Keywords: gout impact scale, gout knowledge level, positive psycap, self-management
Introduction
Gout is a metabolic rheumatic disease caused by the deposition of urate crystals in the joints, tendons and other tissues due to continuously increasing serum uric acid levels.1 Worldwide, the prevalence of gout ranges from <1% to 6.8% and is increasing annually.1 Since 1990, the age-standardized disability-adjusted life years (DALY) rate, prevalence and incidence of gout have gradually increased in China.2 The DALY of gout in men was higher than that in women. The global male prevalence and incidence of gout increased by 5.81% and 4.52%, respectively. In the meantime, the prevalence and incidence of gout among men in China increased by 7.07% and 6.46%, respectively.2 Chinese men are more vulnerable to the effects of gout, which negatively affects their physical, psychological, and social life,3 and leads to poor health-related quality of life (HRQoL).3–5
The promotion of a good quality of life is important for everyone, and the first urgent task is to explore the factors associated with the quality of life in patients with gout and to implement an intervention for the variable factors involved. Recent studies have focused on the quality of life associated with demographic and clinical characteristics and unhealthy emotions,3–5 it provides some references for improving the health-related quality of life of gout patients. Some studies have reported on other factors associated with the chronic disease quality of life, such as the level of disease knowledge, self-efficacy, resilience, confidence, self-management, etc.6–11 However, we do not yet know whether these factors are also associated with HRQOL in patients with gout. In addition, Previous studies on the HRQOL in gout patients have focused on South and East China,4,5,12 while southwest China has unique geographical characteristics and food culture, but the current research in this region is still insufficient.
The information-motivation-behavioral skills model (IMB) is the classical theory of behavior change. The IMB indicates that information, motivation and behavioral skills are core elements of behavior building, and that the establishment of health behaviors and change in health outcomes needs to be based on disease-related knowledge or information as a theoretical ale, individual positive psychology and motivation to generate positive attitudes and maintain established positive behaviors.13 Recent studies have confirmed that IMB-based interventions can improve HRQoL in chronic conditions, such as diabetes,14 osteoarthritis,15 etc. Doherty et al also reported improved HRQoL of gout patients by providing information support interventions.16 Understanding HRQoL in patients with gout and whether it is associated with factors such as information, motivation, and behavioral skills is necessary to improve health outcomes. This study is based on IMB, we used the level of gout knowledge, positive psychological capital (PsyCap), information on self-management, motivation, and behavior, and analyzed whether these factors are associated with HRQoL of male patients with gout in Southwest China from the perspective of IMB (Figure 1).
 |
Figure 1 The research framework based on the information-motivation-behavioral skills model. |
Materials and Methods
Study Design and Participants
This study was a cross-sectional survey, following the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) principle.
The male gout participants were recruited from the outpatient department of West China Hospital of Sichuan University, a general hospital located in southwest China, between February and December 2021. Participants were included if (1) they were aged ≥18 years and fulfilled the 2015 Gout classification criteria suggested by the American College of Rheumatology/European League Against Rheumatism collaborative initiative;17,18 (2) they understood their disease status and volunteered to participate in this study; and (3) they were able to understand and complete the questionnaire. Participants who had other diseases, such as cognitive dysfunction or mental illness, were excluded from the study.
This study complied with the ethical guidelines of the 1975 Declaration of Helsinki, and ethical approval was obtained from the Medical Ethics Committee of the West China Hospital in 2020 (ID: 2020898). All participants were referred by two rheumatologists to participate in a 24-week self-management research project for patients with gout. Participants were first verbally informed about the research project, and if they showed interest, trained researchers informed participants of the purpose and the voluntary, anonymous nature of the study. All participants signed an informed consent form and they were asked to complete the questionnaire independently and were encouraged to seek help when needed.
The sample size of this study was estimated to be 5–10 times the number of variables according to the Kendall principle.19 There were 27 independent variables and dimensions in this study, and considering that 20% of the invalid questionnaires were included, the estimated sample size required was 169–338 cases.
Data Collection
Health-Related Quality of Life
The gout impact scale (GIS) was used to assess the HRQoL of the participants. The GIS compiled by Hirsch et al,20 and sinicized by Li et al in 2019 and its reliability and validity verified for use to assess HRQoL in patients with acute and chronic gout, and the Cronbach’s α coefficient of the total questionnaire was 0.928.21 The Chinese version of the GIS consists of 3 subscales, with 24 entries. It includes five dimensions, as follows: gout concern overall, gout medication side effects, unmet gout treatment requirements, gout concern during attacks, and well-being during attacks.21 The total scale is the average score of each item, with a full score of 100. Higher scores indicate a greater influence of disease and lower HRQoL.21 The Cronbach’s α of the GIS in this study was 0.900.
Questionnaire Based on the Three-Elements Questionnaire of IMB
The gout knowledge questionnaire (GKQ) was used to collect participants’ Information.22 The GKQ was developed by Zhang et al in 2011 and included 10 test questions with a total score of 0 to 10 points.22 Higher scores indicate a higher level of knowledge about the disease. The GKQ’s Flesch‒Kincaid grade level is 4.7, and the Flesch reading ease is 81.4%.22
In this study, we measured the participants’ motivation with a positive psycap questionnaire (PPQ). It includes four dimensions, namely, self-efficacy, resiliency, optimism and hope.23 The PPQ was developed by Luthans et al in 2007.24 Zhang et al standardized and verified the questionnaire, and the Cronbach’s α coefficient of the total questionnaire was 0.90.23 The scores ranged from 26 to 182, with higher scores representing more positive psychology.23 The Cronbach’s α of the PPQ in this study was 0.942.
The gout patient self-management assessment scale (GPSAS) was used to assess the participants’ behavioral skills. The GPSAS was developed by Yao et al in 2020, based on Lorig’s self-management theory.25 A Cronbach’s α coefficient of 0.962 and a content validity index of 0.905 were verified in China.25 The scale includes the four dimensions: disease treatment management, diet management, lifestyle management, and psychosocial management.25 The total GPSAS score was 41 to 205, with higher scores indicating better self-management behavior.25 The Cronbach’s α of the GPSAS in this study was 0.923.
Demographic and Clinical Characteristics of the Participants
Demographic variables that were assessed included age, body mass index (BMI), marital status, educational level, employment status, per capita monthly family income, gout-related expenses in the past year, and smoking and drinking status. Clinical characteristics included duration of symptoms, family history of gout, comorbidities, serum uric acid (SUA) levels in the most recent month, urate-lowering therapy (ULT), tophi, and pain [measured by a 10 cm horizontal visual analog scale (VAS) with a higher score indicating a higher level of pain], number of attacks over half a year and the number of affected joints.
Statistical Analysis
Data analysis was conducted using SPSS (version 25.0, IBM Corp). Suspicious errors, missing values, and outliers were filtered. The frequency and composition ratio of the categorical variables were selected, and the continuous variables underwent descriptive statistical analysis by using the median (interquartile range, IQR) or the mean ± standard deviation (SD). Independent sample t-tests, one-way ANOVA and correlation were used to analyze the relationship of GIS or dimensions with other variables. Variables with P <0.1 in univariate analysis were selected for multiple linear regression of factors associated with GIS or dimensions. The two-sided test level was α=0.05, with P≤0.05 indicating statistical significance.
Results
The demographic and clinical characteristics of the patients are listed in Table 1. We recruited 230 participants, and 225 (97.8%) validated questionnaires were included in the analysis. They aged between 18 and 75 years, mean 40.4±12.6 years. The mean BMI was 26.1±3.3 kg/m2, and SUA was 480.5±129.4 µmol/L. The average pain score was 5 points. Among the participants, 76.4% were married, 80.4% were in employment, 26.7% had tophi, and 46.7% had comorbidities.
 |
Table 1 Demographic and Clinical Characteristics of the Participants, and Univariate Analysis of GIS or Each GIS Dimension (N=225) |
The total GIS score was between 14.6 and 94.8, with an average of 52.7±15.3, and each dimension score from high to low were Gout concern overall (81.4±17.3), Gout medication side effects (66.6±21.3), Gout concern during attack (61.8±21.1), Unmet gout treatment needs (46.8±16.1), and Well-being during attack (38.1±23.4). The average GKQ score of the participants was 6.1±2.1. The PPQ and its four dimensions were scored as 133.0±23.6, 35.6±7.1, 33.3±7.7, 32.0±6.2, and 32.1±6.5, respectively. The GPSAS and its four dimensions scored were 144.9±26.9, 49.1±10.8, 41.8±9.2, 28.1±7.9, and 25.9±5.8, respectively.
The association between the GIS or scores in each dimension and demographic and clinical characteristics and levels of GKQ, PPQ, GPSAS are shown in Table 1 and Table 2. Factors associated with the total GIS score included age (P=0.008), marital status (P=0.028), educational level (P=0.038), BMI (P=0.031), SUA (P=0.042), symptom duration (P=0.010), number of attacks over half a year (P=0.003), number of affected joints (P=0.013), pain intensity (P<0.001), tophi (P=0.006), resiliency (P<0.001), diet management (P=0.035), lifestyle management (P=0.005) and psychosocial management (P=0.007). The following factors were associated with one or more of the five dimensions of the GIS. Demographic factors included age, marital status, employment status, BMI, smoking, and drinking. Clinical factors included symptom duration, SUA, number of attacks over half a year, number of affected joints, ULT, tophi, and pain intensity. Psychological behavioral characteristics included resiliency, hope, diet management, lifestyle management and psychosocial management. However, no relationships were found between per capita monthly family income, gout-related expenses in the past year, comorbidity, family history or GKQ scores with GIS or each GIS dimension score.
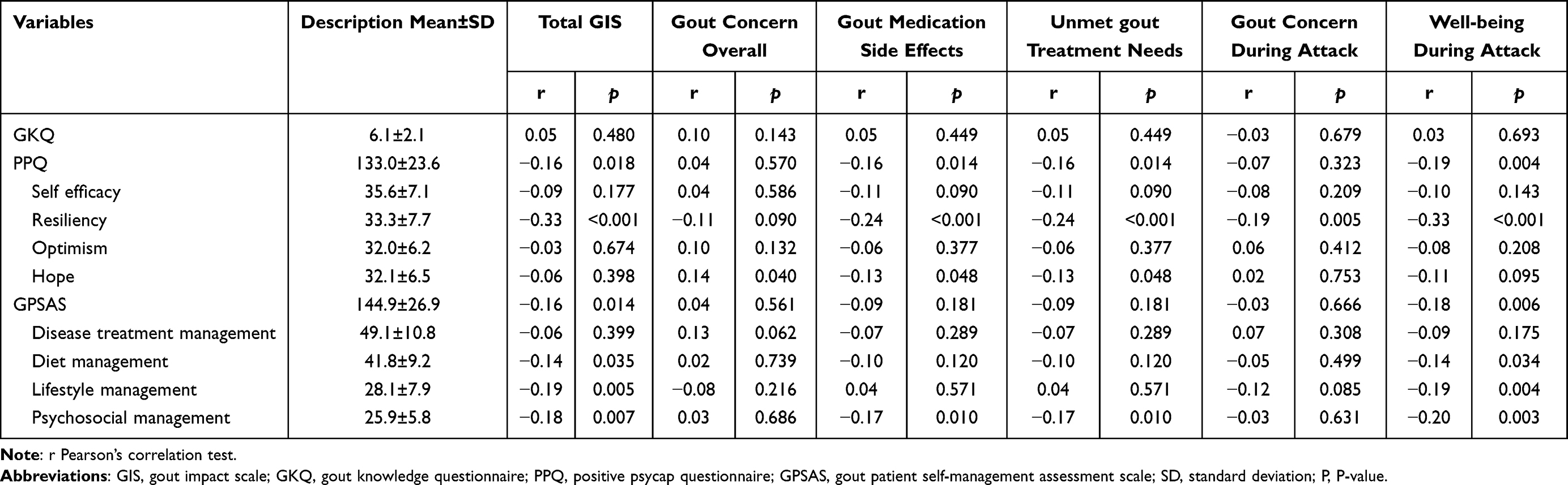 |
Table 2 Levels of GKQ, PPQ, GPSAS, and Univariate Analysis of GIS or Each GIS Dimension (N=225) |
The results of the univariate analysis affecting the GIS or scores in each dimension are shown in Table 1 and Table 2. Factors associated with the total GIS score included age (P=0.008), BMI (P=0.031), marital status (P=0.028), educational level (P=0.038), symptom duration (P=0.010), SUA (P=0.042), tophi (P=0.006), pain (P<0.001), number of attacks over half a year (P=0.003), number of affected joints (P=0.013), resiliency (P<0.001), diet management (P=0.035), lifestyle management (P=0.005),and psychosocial management (P=0.007). The following factors were associated with one or more of the five dimensions of the GIS. Demographic factors included age, BMI, marital status, employment status, smoking, and drinking. Clinical factors included symptom duration, SUA, ULT, tophi, pain, number of attacks over half a year, and number of affected joints. Psychological behavioral characteristics included resiliency, hope, diet management, lifestyle management and psychosocial management. However, no relationships were found between per capita monthly family income, gout-related expenses in the past year, comorbidity, family history or GKQ scores with GIS or each GIS dimension score.
The results of multiple linear regression analysis are shown in Table 3. Pain intensity (β=0.255) with tophi (β=0.138) were positively correlated with the total GIS score, whereas resiliency (β=−0.282) was negatively associated with the total GIS score (R2=0.312, indicating that approximately 31.2% of the changes in the GIS could be explained by these variables). Tophi (β=0.178) and hope (β=0.198) were positively correlated with the dimension of gout concern overall, while the resiliency (β=−0.219) score was negatively associated with this dimension (R2= 0.191, indicating that an approximately 19.1% change in this dimension score can be explained by these variables). Pain (β=0.142) was positively correlated with the dimension of gout medication side effects, while resiliency (β=−0.220) was negatively correlated with it (R2=0.101, indicating that approximately 10.1% of the change in this dimension score can be explained by these variables). Educational level (β=0.235), number of attacks over half a year (β=0.155), number of affected joints (β=0.240), were all positively correlated with the dimension of unmet gout treatment needs, while smoking (β=−0.178) and disease treatment management (β=−0.178) were negatively correlated with this (R2=0.171, indicating that an approximately 17.1% change in this dimension score can be explained by these variables). Smoking status (β=0.131), number of attacks over half a year (β=0.146), tophi (β=0.140), and pain (β=0.141) were all positively associated with the dimension of gout concern during attacks, and marital status (β=−0.168) and diet management (β=−0.138) were negatively associated (R2=0.178, indicating that a 17.8% change in this dimension score can be explained by these variables). Finally, pain was positively correlated with the dimension of well-being during attacks (β=0.271), while resiliency (β= −0.325) was negatively correlated (R2=0.283, indicating that an approximately 28.3% change in this dimension score can be explained by these variables.
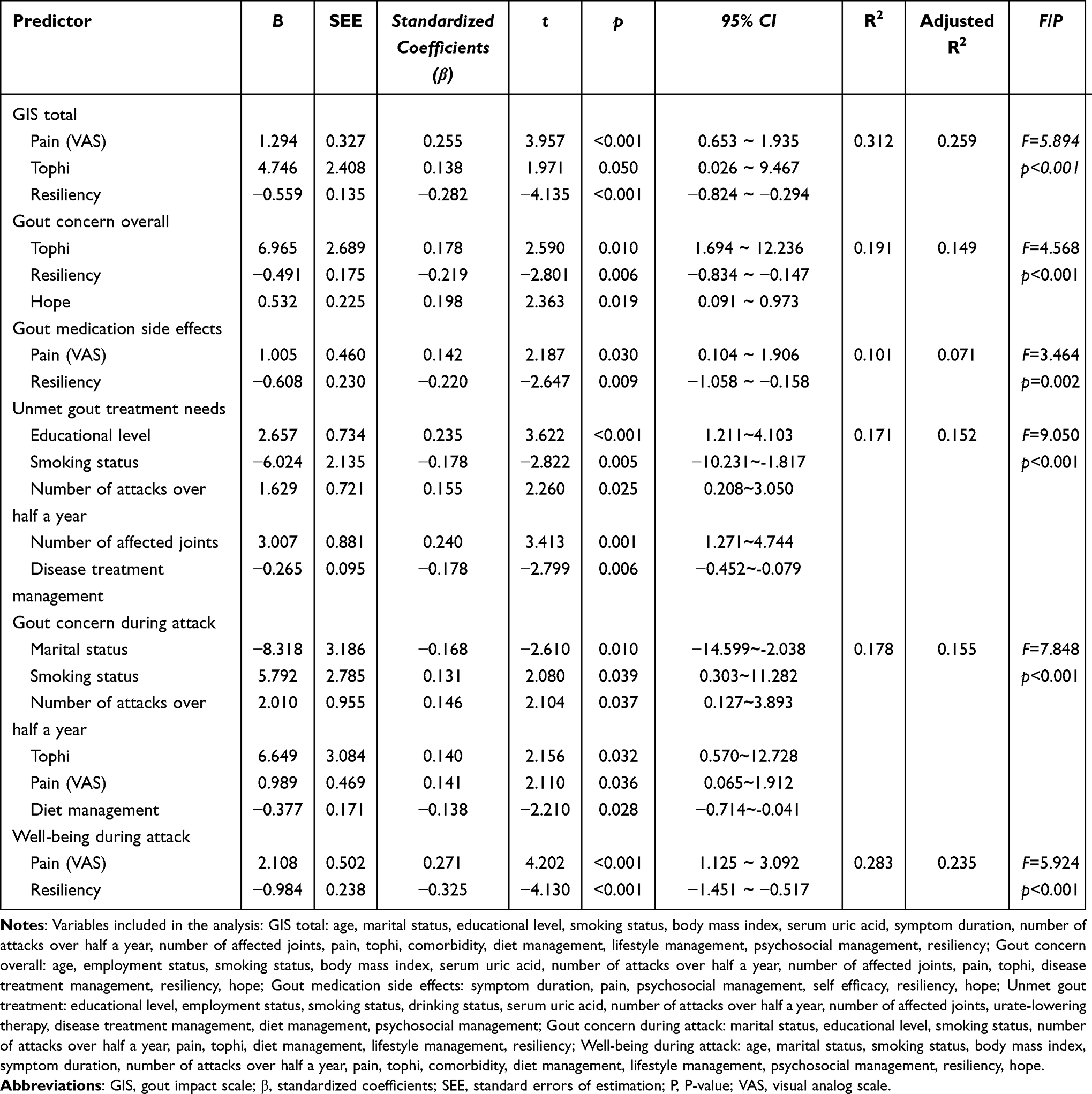 |
Table 3 Multiple Linear Regression of Factors Associated with GIS and GIS Dimension Scores |
Discussion
In this study, we assessed the HRQoL in 225 Chinese male gout patients using the GIS. The participants had a GIS score of 52.7±15.3, which represents a moderate level, slightly better than in the previous study of Zhou et al in North China (56.79±15.45).12 It may be relevant for explaining this difference that the participants had different regional and demographic characteristics.12 The dimension with the highest participant score was gout concern overall (81.4±17.3), meaning that this dimension was the most influential, whereas the least influential dimension was well-being during attacks (38.1±23.4). The ranking of the five dimensions found here is consistent with that reported by Zhou et al.12 We found that among the total GIS score and the five GIS dimensions, meaningful demographic variables included marital status, educational level, and smoking; clinical characteristics included the number of attacks over half a year, number of affected joints, pain and tophi; and finally, social and behavioral variables included resiliency and hope, disease treatment management and diet management.
Previous studies reported that the effect of marital status on HRQoL in gout patients is inconsistent.3,5,12 Chandratre et al found that married people had better HRQoL than single people.3 However, this was not the case for Chinese gout patients.5,12 No statistical significance was found concerning marital status and GIS total score in this study, but further analysis suggested that married people had lower scores for gout concern during attacks than singles (β=−0.168), ie single people have more concerns during gout attacks than married people. During gout attacks, patients not only need to endure severe pain but also face changes in physical movement barriers, medical treatment, work, life and social interaction.26,27 Patients with gout have an increased need for family and intimate relationship support,26 while these needs in single people are less likely to be met. Therefore, healthcare providers should focus on single patients and assist them in predesigning responses to attacks of gout to mitigate their impact.
Although previous studies have not found an association between educational level and HRQoL in gout patients, it is evident that such an association exists in other chronic diseases27,28 Interestingly, the present study found that the educational level of gout patients did have a significant impact on the GIS dimension of unmet gout treatment needs (β=0.235). This finding is not in agreement with some other studies.28,29 A possible reason for this is that people with high educational levels may have access to better health-related knowledge and skills,30,31 while information may have a negative impact on healthcare utilization.32 Therefore, healthcare providers are advised to guide gout patients to correctly access and utilize information resources to best meet their treatment needs.
The relationship between smoking and gout is also inconclusive.33,34 Here, we found that smokers scored higher for the GIS dimension of gout concern during attacks (β=0.131) but lower in the dimension of unmet gout treatment needs (β=−0.178). Studies have shown that the effect of smoking on quality of life is related to the number of cigarettes smoked,35 duration of the habit,36 and age of the smokers.37 Currently, the effect of smoking on HRQoL and its mechanisms in gout patients still needs further investigation.
The correlation between clinical characteristics and HRQoL in gout patients has received more attention. The findings in this study had similar results to previous studies.5,38,39 Clinical features associated with the total GIS score included tophi (β=0.138) and pain intensity (β=0.255). In addition, tophi was associated with two GIS dimensions including gout concern overall (β =0.178) and gout concern during attacks (β =0.140).Tophi is a specific sign of chronic gout, which not only causes changes in body structure and joint movement restrictions, but also exerts negative effects on psychological and social participation, and increases the burden to healthcare systems.38,40 Treatment to target (T2T) is an effective way to prevent and reduce tophi.41 Therefore, the implementation of standard treatment should be considered in the management of gout patients.
Studies found that pain was a predictor of low HRQoL in the Chinese gout population.4,5 The correlation of pain with GIS and its different dimensions was also reported by Pao et al.42 Our study focused on the effect of the intensity of pain on gout patients. We found that pain intensity affected the total GIS score (β=0.255) and the three dimensions including gout medication side effects (β=0.142), gout concern during attacks (β=0.141), and well-being during attacks (β=0.271). As one of the indicators of the patient-reported outcome (PRO) of gout,43 pain is the main symptom in acute gout attacks, it is also an important feature of chronic gout, which is also the most direct impact and the main cause of seeking medical treatment in gout patients.43 Moreover, pain carries a burden of treatment, decreased mobility, productivity and mood.44 Therefore, healthcare providers should take measures to actively control inflammation to reduce pain.
The two variables, the number of gout attacks and the number of affected joints, were not significantly associated with the GIS total score but were associated with some GIS dimensions. Gout attacks are one of the main reasons why patients seek medical treatment,44 and they often present with severe joint swelling and pain, having serious impacts on daily life.26,44 Frequent attacks and more joints affected mean that treatment is not satisfactory. While actively controlling acute attacks, medical staff should also pay attention to the standard treatment and T2T of gout to reduce the number of acute attacks and the number of affected joints and reduce the impact of the disease.
Resiliency is the ability of individuals to adapt to change in an appropriate and lasting manner, and their ability to choose the best way to address challenges in the face of adversity to maintain physical and mental health.45 Previous studies have found that psychological capital plays a protective role in maintaining the quality of life.46 We found that in all dimensions of the PPQ, psychological resiliency was negatively correlated with the total GIS score (β= −0.282), gout concern overall (β= −0.219), gout medication side effects (β= −0.220), and well-being during attacks (β= −0.325). This implies people with high resiliency have a more positive adaptation and more willpower to more effectively accept and adapt to psychological impairment and manage the effects of the disease.45,46 Therefore, it is recommended that healthcare personnel conduct active psychological interventions to improve the level of resilience of gout patients to help them improve their quality of life. Hope refers to the individual’s belief in achieving the goal and the power to adjust the path accordingly.46 Hope is an important psychological and spiritual resource that can protect against perceived stress, and people with higher hope levels can adopt a more positive coping approach.47,48 We found that hope was positively correlated with the score for the GIS dimension Gout concern overall (β=0.198), meaning that hope has a negative impact on the quality of life of this dimension. This result differs from previous studies,10,47 and the reasons for this phenomenon need to be further investigated.
Studies have confirmed the benefit of self-management interventions in improving the quality of life of patients with chronic diseases.11,49 The present study found that in all GPSAS dimensions, only disease treatment management was negatively correlated with unmet gout treatment needs (β= −0.178), and diet management was negatively correlated with gout concern during attacks (β= −0.138). This implies that active disease treatment and diet management can help to improve the HRQoL in gout patients. Such results are similar to those of Quon et al.11 Hence, the present study supports a relationship between self-management behaviors and the HRQoL of gout patients, suggesting that the HRQoL can be improved through aggressive self-management interventions.
Although existing studies confirm that the level of disease knowledge is closely related to quality of life,6 this study did not confirm this association, which requires further investigation.
This study has some deficiencies. First, it is a cross-sectional study that may be limited in explaining causality. Second, we did not recruit healthy controls synchronously, weakening the strength of the conclusions. This study only analyzed the relationship of the three elements of the IMB model with HRQoL, and did not further analyze the mediating role of self-management behaviors. Finally, we did not distinguish the degree of diagnosis in gout patients, which may be detrimental to the practical application of the findings.
Conclusion
In this study, we adopted the IMB model and investigated the relationship of psychosocial behavior with HRQoL in patients with gout. We found that HRQoL in patients with gout in Southwest China was not only associated with demographic factors and clinical characteristics but also associated with resilience, hope, disease treatment management behaviors, and diet management behaviors. The results indicated that healthcare providers should choose intervention strategies with variable factors, actively monitor clinical symptoms, and pay more attention to psychosocial factors to improve the quality of life of patients with gout.
Acknowledgments
The authors acknowledge gout patients who were involved in this study for providing feedback and data. The authors would like to express their gratitude to EditSprings for the expert linguistic services provided.
Funding
This study was supported by the SCST (Science and Technology of Sichuan Province) (Grant No.2018FZ0110).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. 2020;16(7):380–390. doi:10.1038/s41584-020-0441-1
2. Tang YM, Zhang L, Zhu SZ, et al. Gout in China, 1990–2017: the global burden of disease study 2017. Public Health. 2021;191:33–38. doi:10.1016/j.puhe.2020.06.029
3. Chandratre P, Mallen C, Richardson J, et al. Health-related quality of life in gout in primary care: baseline findings from a cohort study. Semin Arthritis Rheu. 2018;48(1):61–69. doi:10.1016/j.semarthrit.2017.12.005
4. Yang P, Chen Z, Chen YT, et al. Use of the gout impact scale to evaluate quality of life in Chinese subjects with gout: a cross-sectional study. Med Sci Monit. 2020;26:e925593-1–e925593–8. doi:10.12659/MSM.925593
5. Fu T, Cao H, Yin R, et al. Associated factors with functional disability and health-related quality of life in Chinese patients with gout: a case-control study. BMC Musculoskel Dis. 2017;18:429. doi:10.1186/s12891-017-1787-7
6. Alikari V, Matziou V, Tsironi M, et al. Patient knowledge, adherence to the therapeutic regimen, and quality of life in hemodialysis: knowledge, adherence, and quality of life in hemodialysis. Adv Exp Med Biol. 2021;1337:259–272. doi:10.1007/978-3-030-78771-4_29
7. Suh CH, Lee K, Kim JW, Boo S. Factors affecting quality of life in patients with rheumatoid arthritis in South Korea: a cross-sectional study. Clin Rheumatol. 2022;41(2):367–375. doi:10.1007/s10067-021-05944-9
8. Hashimoto A, Sonohata M, Mawatari M. The use of oral analgesics and pain self-efficacy are independent predictors of the quality of life of individuals with rheumatoid arthritis. Pain Res Manag. 2020;2020:7409396. doi:10.1155/2020/7409396
9. Liu X, Yang X, Yao L, et al. Prevalence and related factors of depressive symptoms in hemodialysis patients in northern China. BMC Psychiatry. 2017;17(1):128. doi:10.1186/s12888-017-1294-2
10. Zhang Y, Cui C, Wang Y, Wang L. Effects of stigma, hope and social support on quality of life among Chinese patients diagnosed with oral cancer: a cross-sectional study. Health Qual Life Out. 2020;18(1):112. doi:10.1186/s12955-020-01353-9
11. Quon R, Andrew A, Schmidt S, et al. Self-management practices associated with quality of life for adults with epilepsy. J Neurol. 2019;266(11):2821–2828. doi:10.1007/s00415-019-09503-w
12. Zhou W, Zhu J, Guo J, et al. Health-related quality of life assessed by Gout Impact Scale (GIS) in Chinese patients with gout. Curr Med Res Opin. 2020;36(12):2071–2078. doi:10.1080/03007995.2020.1840341
13. Fassier JB, Sarnin P, Rouat S, et al. Interventions developed with the intervention mapping protocol in work disability prevention: a systematic review of the literature. J Occup Rehabil. 2019;29(1):11–24. doi:10.1007/s10926-018-9776-8
14. Yao X, Zhang L, Du J, Gao L. Effect of information-motivation-behavioral model based on protection motivation theory on the psychological resilience and quality of life of patients with type 2 DM. Psychiatr Q. 2021;92(1):49–62. doi:10.1007/s11126-020-09783-w
15. Kim JS, Kim CJ. Effect of a physical activity promoting program based on the imb model on obese-metabolic health outcomes among obese older adults with knee osteoarthritis. J Korean Acad Nurs. 2020;50(2):271–285. doi:10.4040/jkan.2020.50.2.271
16. Doherty M, Jenkins W, Richardson H, et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: a randomised controlled trial. Lancet. 2018;392(10156):1403–1412. doi:10.1016/S0140-6736(18)32158-5
17. Neogi T, Jansen TLTA, Dalbeth N, et al. 2015 Gout classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2015;74(10):1789–1798. doi:10.1136/annrheumdis-2015-208237
18. Chinese Rheumatology Association. 2016 China gout clinical practice guideline. Chin J Intern Med. 2016;55(11):892–899. Chinese. doi:10.3760/cma.j.issn.0578-1426.2016.11.019
19. Ni P, Chen JL, Li N. Sample size estimates for quantitative studies in nursing studies. Chin J Nurs. 2010;45(04):378–380. Chinese. doi:10.3761/j.issn.0254-1769.2010.04.037
20. Hirsch JD, Lee SJ, Terkeltaub R, et al. Evaluation of an instrument assessing influence of gout on health-related quality of life. J Rheumatol. 2008;35(12):2406–2414. doi:10.3899/jrheum.080506
21. Li Y, Liu T, Miao XX, et al. Reliability and validity of the Chinese version of gout impact scale. Chin Nurs Manag. 2019;19(10):1472–1477.Chinese. doi:10.3969/j.issn.1672-1756.2019.10.009
22. Zhang LY, Schumacher HR, Su HH, et al. Development and evaluation of a survey of gout patients concerning their knowledge about gout. Jcr-j Clin Rheumatol. 2011;17(5):242–248. doi:10.1097/RHU.0b013e318228b4e2
23. Zhang K, Zhang S, Dong YH. Positive psychological capital: measurement and relationship with mental health. Stud Psych Behav. 2010;8(1):58–64. Chinese.
24. Luthans F, Avolio BJ, Avey JB, Norman SM. Positive psychological capital: measurement and relationship with performance and satisfaction. Pers Psychol. 2007;60(3):541–572. doi:10.1111/j.1744-6570.2007.00083.x
25. Yao XY, Liu T, Li Y, et al. Development and psychometric testing of a gout patient self-management assessment scale. Chin J Nurs. 2020; 55:261–265. Chinese. doi:10.3761/j.issn.0254-1769.2020.02.018
26. Singh JA. The impact of gout on patient’s lives: a study of African-American and caucasian men and women with gout. Arthritis Res Ther. 2014;16(3):R132. doi:10.1186/ar4589
27. The experience and impact of living with gout: a study of men with chronic gout using a qualitative grounded theory approach - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/21169857/.
28. Zhang H, Wang Y, Cai X, Tang N, Wei S, Yang Y. Family functioning and health-related quality of life of inpatients with coronary heart disease: a cross-sectional study in Lanzhou city, China. BMC Cardiovasc Disord. 2022;22(1):397. doi:10.1186/s12872-022-02844-x
29. Illness perception and quality of life in patients with migraine and tension-type headache - pubmed. Available from: https://pubmed.ncbi.nlm.nih.gov/36413440/.
30. Pollitt RA, Swetter SM, Johnson TM, Patil P, Geller AC. Examining the pathways linking lower socioeconomic status and advanced melanoma. Cancer-Am Cancer Soc. 2012;118(16):4004–4013. doi:10.1002/cncr.26706
31. Ng CY, Lee ZS, Goh KS. Cross-sectional study on knowledge of chronic kidney disease among medical outpatient clinic patients. Med J Malaysia. 2016;71(3):99–104.
32. Schmid C. Consumer health information and the demand for physician visits. Health Econ. 2015;24(12):1619–1631. doi:10.1002/hec.3117
33. Fanning N, Merriman TR, Dalbeth N, Stamp LK. An association of smoking with serum urate and gout: a health paradox. Semin Arthritis Rheu. 2018;47(6):825–842. doi:10.1016/j.semarthrit.2017.11.004
34. Jee Y, Jeon C, Sull JW, Go E, Cho SK. Association between smoking and gout: a meta-analysis. Clin Rheumatol. 2018;37(7):1895–1902. doi:10.1007/s10067-018-4118-y
35. Goldenberg M, Danovitch I, IsHak WW. Quality of life and smoking. Am J Addict. 2014;23(6):540–562. doi:10.1111/j.1521-0391.2014.12148.x
36. Dotlic J, Markovic N, Gazibara T. Patterns of smoking and menopause-specific quality of life: smoking duration matters more. Behav Med. 2023;49(1):29–39. doi:10.1080/08964289.2021.1958739
37. Jing Z, Li J, Wang Y, et al. Association of smoking status and health-related quality of life: difference among young, middle-aged, and older adults in Shandong, China. Qual Life Res. 2021;30(2):521–530. doi:10.1007/s11136-020-02645-9
38. Khanna PP, Nuki G, Bardin T, et al. Tophi and frequent gout flares are associated with impairments to quality of life, productivity, and increased healthcare resource use: results from a cross-sectional survey. Health Qual Life Out. 2012;10:117. doi:10.1186/1477-7525-10-117
39. Chandratre P, Roddy E, Clarson L, Richardson J, Hider SL, Mallen CD. Health-related quality of life in gout: a systematic review. Rheumatology. 2013;52(11):2031–2040. doi:10.1093/rheumatology/ket265
40. Cellular characterization of the gouty tophus: a quantitative analysis - pubmed. Available from: https://pubmed.ncbi.nlm.nih.gov/20131281/.
41. Kiltz U, Smolen J, Bardin T, et al. Treat-to-target (T2T) recommendations for gout. Ann Rheum Dis. 2017;76(4):632–638. doi:10.1136/annrheumdis-2016-209467
42. Pao CH, Ko Y. An assessment of the psychometric properties of the Chinese version of the gout impact scale. Curr Med Res Opin. 2020;36(1):17–21. doi:10.1080/03007995.2019.1662990
43. Singh JA, Taylor WJ, Simon LS, et al. Patient-reported outcomes in chronic gout: a report from OMERACT 10. J Rheumatol. 2011;38(7):1452–1457. doi:10.3899/jrheum.110271
44. Coulshed A, Nguyen AD, Stocker SL, Day RO. Australian patient perspectives on the impact of gout. Int J Rheum Dis. 2020;23(10):1372–1378. doi:10.1111/1756-185X.13934
45. Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol. 2002;58(3):307–321. doi:10.1002/jclp.10020
46. Li MY, Yang YL, Liu L, Wang L. Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: a cross-sectional study. Health Qual Life Out. 2016;14:73. doi:10.1186/s12955-016-0481-z
47. Klein DE, Winterowd CL, Ehrhardt MD, Carter JC, Khan O, Mayes S. The relationship of self-compassion and hope with quality of life for individuals with bleeding disorders. Haemophilia. 2020;26(3):e66–e73. doi:10.1111/hae.13959
48. Fong TCT, Lo TLT, Ho RTH. Indirect effects of social support and hope on quality of life via emotional distress among stroke survivors: a three-wave structural equation model. Front Psychiatry. 2022;13:919078. doi:10.3389/fpsyt.2022.919078
49. A conceptual model for quality of life among people with type 2 diabetes in the Philippines - pubmed. Available from: https://pubmed.ncbi.nlm.nih.gov/30962745/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Status Quo and Influencing Factors of Self-Management Behavior in Patients with Recurrent Gout in China: A Cross-Sectional Study
Hao X, Wang A
Patient Preference and Adherence 2025, 19:1793-1806
Published Date: 19 June 2025