Back to Journals » International Journal of Women's Health » Volume 17
The Relationship Between Perceived Stress, Adult Attachment, and Dyadic Coping in Couples with Pregnancy: An Actor-Partner Interdependence Mediation Model
Authors Zhao J, An C, Liu S, Shen Q, He T, Hu S, Lei J, Liu D
Received 4 July 2025
Accepted for publication 17 October 2025
Published 4 November 2025 Volume 2025:17 Pages 4075—4090
DOI https://doi.org/10.2147/IJWH.S547870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Jinxin Zhao,1– 3 Chunyan An,3 Sihui Liu,3 Quan Shen,1,2 Tan He,1,2 Sijie Hu,1,2 Jun Lei,1 Dan Liu4
1Department of Obstetrics and Gynecology, The Third Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 2Xiangya School of Nursing, Central South University, Changsha, Hunan, People’s Republic of China; 3Department of Obstetrics and Gynecology, People’s Hospital of Ningxia Hui Autonomous Region, Yinchuan, Ningxia, People’s Republic of China; 4Department of Nursing, The Third Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Jun Lei, Department of Obstetrics and Gynecology, The Third Xiangya Hospital of Central South University, 138 Tongzipo Road, Yuelu District, Changsha, Hunan, 410013, People’s Republic of China, Email [email protected] Dan Liu, Department of Nursing, The Third Xiangya Hospital of Central South University, 138 Tongzipo Road, Yuelu District, Changsha, Hunan, 410013, People’s Republic of China, Email [email protected]
Purpose: The current study aims to analyze the relationships between perceived stress, adult attachment (attachment avoidance and attachment anxiety), and dyadic coping among Chinese couples during pregnancy. Additionally, it seeks to explore the mediating effects of adult attachment on these relationships.
Methods: A total of 701 heterosexual pregnant couples participated in this cross-sectional study, which was conducted at three tertiary hospitals in central and western China from September 2023 to July 2024. Participants’ mean age was 29.56± 4.15 years for pregnant women and 31.11± 4.33 years for their partners. They completed the Perceived Stress Scale, the Dyadic Coping Inventory, and the Experiences in Close Relationships Scale-Chinese Short Version. The actor-partner interdependence mediation model was employed to analyze the data derived from the dyadic relationships.
Results: The dyadic coping scores were recorded as 117.42± 16.63 for pregnant women and 117.75± 16.12 for their partners. The analysis revealed that individuals’ perceived stress was both directly and indirectly associated with their dyadic coping, as a mediator role of adult attachment (attachment avoidance and attachment anxiety). Furthermore, partners’ attachment avoidance was identified as a complete mediator of the partner effect. Partners’ attachment anxiety played a complete partner mediating role in the relationship between perceived stress on dyadic coping for pregnant women and their partners.
Conclusion: The present study examined the relationship between perceived stress, adult attachment (attachment avoidance and attachment anxiety), and dyadic coping. The findings indicate that interventions should consider the couple as a unit and take into account their adult attachment during pregnancy. Healthcare professionals may aim to reduce adult attachment insecurity in pregnant couples and enhance their dyadic coping abilities to improve psychological well-being.
Keywords: perceived stress, attachment avoidance, attachment anxiety, dyadic coping, the actor-partner interdependence model
Introduction
Pregnancy is a significant period in an individual’s life, providing profound joy to the family, while simultaneously introducing a range of challenges. The global demographic landscape is undergoing significant changes, characterized by an aging population1 and a consistent decline in the total fertility rate.2 This trend is particularly evident in China, where the recent implementation of a three-child policy,3 coupled with evolving societal attitudes towards parenthood. In traditional Chinese culture, the concept of family holds significant importance. The continuation and transmission of the family is regarded as a responsibility and a mission, underscoring the value of having a healthy child.4 Furthermore, prospective parents in China encounter substantial financial pressures. The costs associated with maternity checkups, delivery, and child education from birth represent a significant financial investment.5 All of these may increase perceived stress on prospective parents. Moderate levels of stress have been shown to provide protective benefits, while excessive psychosocial stress and inadequate coping adversely affects the well-being of pregnant women and their partners, potentially leading to depression and anxiety.6 The global prevalence of antenatal depression among pregnant women and their partners was reported at 20.7%7 and 9.76%,8 respectively, while prenatal anxiety rates were 22.2%9 and 10.69%.10 In China, the prevalence of antenatal depression stands at 19.7% for pregnant women11 and 11% for their partners,12 with anxiety rates at 17.4%13 and 2.6%,14 respectively. Inadequate management of negative emotions can adversely impact the health of expect parents, as well as to jeopardize fetal development,15,16 to strain couple relationships,17 and to disrupt family dynamics.18 In severe cases, this can lead to harmful behaviors towards infants19 and elevate the risk of suicidal tendencies.20 Therefore, it is crucial to implement positive stress coping during pregnancy to ensure well-being throughout this period and into parenthood.
Research indicates that the stressful coping mechanisms employed by one partner during pregnancy can have an impact on the other.21 According to the systemic transactional model (STM), which perceived stress and coping strategies are frames from a “we stress” perspective. This perspective emphasized the interdependence and mutual support inherent in a couple’s relationship.22 Thus, expecting a child, as a dyadic stress, impact both partners simultaneously, creating a shared experience. During this time, each partner must navigate their own stress while also addressing the needs and concerns of the other. Dyadic coping, the core content of the STM, refers to the collaborative efforts of both partners to manage stressful situations that affect either or both individuals. Dyadic coping encompasses both positive and negative aspects. The positive forms include supportive, delegated, and common dyadic coping, while the negative forms consist of hostile, ambivalent, and superficial dyadic coping.23 Research suggests that assessing dyadic coping during pregnancy is essential for enhancing both physical and mental well-being,24 as well as fostering the intimate relationship25 and enhancing the quality of life26 between expectant couples.
At the same time, individual differences in adult attachment play a critical role in shaping how stress is experienced and how coping is enacted. According to attachment theory, whether an individual engages in dyadic coping behaviors might vary according to the degree of insecure attachment toward the romantic partner.27 Adult attachment is assessed as per two dimensions representing attachment insecurities: anxiety and avoidance.28 Individuals with higher levels of avoidance tend to keep both behavioral and cognitive distance from stressful events. They often avoid expressing distress to their partners, seeking support, or offering assistance to their distressed partners during challenging times.29 As a result, these individuals may not see dyadic coping strategies as helpful for alleviating distress, primarily due to negative expectations about their partner’s availability.30 On the other hand, individuals with higher attachment anxiety often feel increased perceived pressure and become overwhelmed by their own distress.29 This focus on their attachment needs might lead to less effective dyadic coping or result in coping strategies that do not align well with their partner’s actual needs.30
The Attachment Diathesis-Stress Process Model suggests that stress—such as that experienced during pregnancy—can activate threat perceptions and trigger the attachment system, thereby intensifying maladaptive coping strategies.31 Thus, in the context of pregnancy, perceived stress may operate as a key activator of attachment-related vulnerabilities, which in turn disrupt adaptive dyadic coping processes.
However, a limited number of studies have explored whether individual perceptions of stress or adult attachment are associated with couple coping, but there is still a lack of overall focus on the relationship between the variables.32–36 As a result, our understanding of the dyadic relationships among these variables in the specific context of pregnancy remains limited. Several longitudinal studies have examined the evolution of perceived stress, dyadic coping and adult attachment during the transition to parenthood. While these studies emphasize the importance of temporal factors and individual predispositions, they tend to focus either on the relationship between two variables or on pregnant women. Even when partner data is incorporated, it is often analyzed separately or treated as a covariate. This approach inherently overlooks dyadic interaction, whereby partners’ psychological states influence one another continuously and reciprocally.
Our study aims to bridge this gap by employing a dyadic analytical framework. The actor-partner interdependence mediation model (APIMeM) is proposed for use in analyzing the path relationships among perceived stress, adult attachment, and dyadic coping in pregnant women and their partners. APIMeM emphasizes the importance of strong interpersonal interactions within intimate relationships while simultaneously examining how the independent variable affects the dependent variable through mediation analysis.37 In this context, an individual’s dependent variable is shaped not only by their own independent variable (actor effect) but also by their partner’s independent variable (partner effect). The independent variable has both a direct impact on the outcome variable and an indirect influence through a mediating variable. Given the study’s research objectives, APIMeM’s approach goes beyond individual-level analysis by examining how an individual’s dyadic coping is affected by perceived stress from both the individual and their partner. It also explores the role of adult attachment as a mediator in the relationship between perceived stress and dyadic coping.
Based on the theoretical framework, the following hypotheses were proposed and tested using the APIMeM:
H1: Perceived stress will be negatively associated with dyadic coping, demonstrating both: (H1a) actor effects (an individual’s own perceived stress will negatively predict their own dyadic coping), and (H1b) partner effects (an individual’s perceived stress will negatively predict their partner’s dyadic coping). H2: Adult attachment (attachment avoidance and attachment anxiety) will be negatively associated with dyadic coping, demonstrating both: (H2a) actor effects, and (H2b) partner effects. H3: Adult attachment will mediate the relationship between perceived stress and dyadic coping. Specifically: (H3a) The actor effect of perceived stress on dyadic coping will be mediated by the individual’s own adult attachment (actor-mediation). (H3b) The partner effect of perceived stress on dyadic coping will be mediated by the partner’s adult attachment (partner-mediation).
The objectives of this study are threefold: (i) to examine sex differences in the levels of perceived stress, adult attachment, and dyadic coping between pregnant women and their partners; (ii) to assess the impact of perceived stress and adult attachment on the dyadic coping of both pregnant women and their partners; and (iii) to explore the mediating role of adult attachment in the relationship between perceived stress and dyadic coping. The study aims to elucidate the relational pathways of dyadic coping interactions between prenatal couples and to provide a theoretical foundation for clinical interventions designed to enhance the dyadic coping of these couples.
Materials and Methods
Study Design and Participants
A cross-sectional study design using convenience sampling was performed, and the STROBE checklist was followed to report the findings of this study. This cross-sectional study was carried out between September 2023 to July 2024 at three local tertiary hospitals in central and western China. Potential participants were approached during antenatal clinic visits and invited to participate in the study. The inclusion criteria stipulated that couples must be legally married, with fathers being biologically related to the fetus. Pregnant women were required to be at least 20 years old and free from severe pregnancy complications, while partners needed to be a minimum of 22 years of age. All participating couples were cisgender and heterosexual. Specifically, the pregnant partners were female and the non-pregnant partners were male, based on sex assigned at birth. The exclusion criteria for either member of the couple included having a mental or psychiatric disorder, as well as a refusal to participate in the study.
Assuming a medium actor and partner effect size of 0.16, with a two-tailed type I error rate of 5% and a statistical power of 80%, the calculated sample size was determined to be a minimum of 320 dyads.38,39 To address the possibility of incomplete data, an additional 15% was incorporated into the sample size, culminating in a total requirement of 368 dyads (368 pregnant women and 368 partners).
Measures
Perceived Stress
The Chinese version of Perceived Stress Scale (PSS) was used to measure the perceived stress in the present study.40 This scale consists of 14 items. Each item is scored on a 5-point Likert scale from 1 to 5. The total scores range from 14 to 70, with higher scores indicating higher perceived stress. In our study, the Cronbach’s alpha coefficient was 0.779 and 0.777 for pregnant women and their partners, respectively.
Dyadic Coping
The Dyadic Coping Inventory (DCI) was used to measure dyadic coping in pregnant women and their partners.41 The DCI includes six dimensions of stress communication, supportive coping, delegated coping, joint coping, negative coping, and coping quality evaluation, with 37 items. Each item is scored on a 5-point Likert scale from 1 to 5. The total score on the DCI ranged from 35 to 175, with higher scores indicating higher levels of dyadic coping. The Cronbach’s alpha coefficient of DCI in this study for pregnant women and their partners was 0.913 and 0.919, respectively.
Adult Attachment
The Experiences in Close Relationships Scale-the Chinese Short Version (ECR-CS) was used to measure adult attachment in pregnant women and their partners.42 The ECR-CS consists of 11 items on two dimensions: attachment anxiety and attachment avoidance. Each item is scored on a 7-point Likert scale ranging from 1 to 7, with 1 representing “strongly disagree” and 7 representing “strongly agree”. Note that four questions are reverse scored. The ECR-CS is a tool for measuring trait attachment style; it calculates scores for each dimension rather than the total score. The Cronbach’s alpha coefficient of ECR-CS in this study for pregnant women and their partners was 0.767 and 0.753, respectively.
Sociodemographic and Obstetric Features
The study was designed by the researcher and included the following variables: age, education level, employment status, current residence, monthly household income, pregnancy status, complications of pregnancy, marital status, and marrying age.
Data Analysis
SPSS version 26.0 and AMOS version 24.0 were utilized for data analysis. Descriptive statistical analysis was used to calculate means and standard deviations for all variables. Paired sample t-tests were used to analyze sex differences in perceived stress, adult attachment, and dyadic coping scores. Pearson correlation analysis was used to test the relationship between pregnant women and their partners on perceived stress, adult attachment, and dyadic coping. The associations of age, duration of marriage and monthly household income were entered as covariates in the APIMeM.
To examine the impact of perceived stress on the couples’ dyadic coping and the mediating role of adult attachment, dyad data were analyzed using the APIMeM model.37 Before proceeding with the analysis, empirical distinguishability was verified by imposing constraints to ensure that each effect was equivalent across the two groups. Each constrained model was tested separately.37
When P>0.20, it indicates that there was no significant difference in the goodness-of-fit between the two models. The results of the dyad data discriminability test utilized several metrics, including χ2, Tucker-Lewis Index (TLI), Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Residual (SRMR), to evaluate the fit of the dyadic model hypothesis in this study. The criteria for a well-fitted model were established as χ2/df < 3, CFI and TLI ≥ 0.90, and RMSEA and SRMR ≤ 0.08.43 To assess mediation, indirect effects were estimated through bootstrapping with 5000 iterations.44 If the 95% confidence interval does not include 0, it indicates that the indirect effects are significant. p < 0.05 was considered to represent acceptable statistical significance.
Results
Features of Participants
A summary of the sociodemographic characteristics of pregnant women and their partners was presented Table 1. Out of 750 couples who were initially contacted and eligible, a total of 701 dyads provided complete and valid data, constituting the final analytical sample. The average age of the pregnant women was 29.56 years (SD = 4.15), while the average age of their partners was 31.11 years (SD= 4.33). The duration of marriage averaged 3.81 years (SD= 3.20). More than half of pregnant women (51.78%) and their partners (55.92%) had education levels below a college degree. A significant proportion of pregnant women (84.74%) and partners (95.15%) were employed. Additionally, over eighty percent of the couples (83.88%) resided in the city, and more than half (61.77%) reported a monthly household income of less than ¥8,000, which is below the national monthly household income of urban households.45 Furthermore, over half of the pregnant women (63.62%) were primiparous.
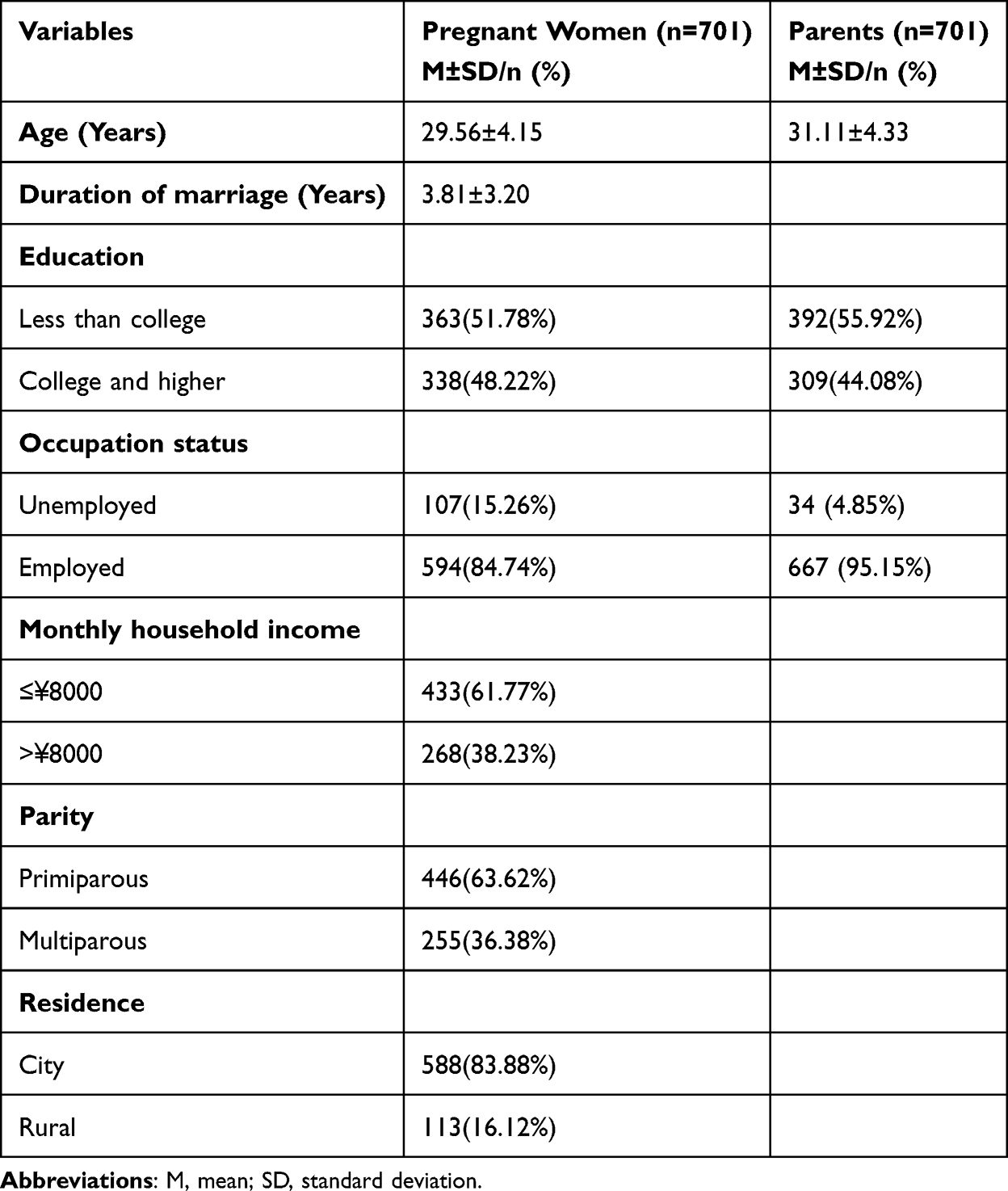 |
Table 1 Sociodemographic and Obstetric Features of the Pregnant Women and Their Partners (n=701 Couples) |
The differences in perceived stress, adult attachment (attachment avoidance and attachment anxiety), and dyadic coping between pregnant women and their partners was presented Table 2. The results of the paired sample t-tests indicate that there were no significant differences between couples in terms of attachment avoidance and dyadic coping. Pregnant women reported higher perceived stress scores than their partners (t=5.572, p<0.001, Cohen’s d=0.307). Additionally, pregnant women exhibited higher scores on attachment anxiety than their partners (t=3.053, p=0.002, Cohen’s d=0.163).
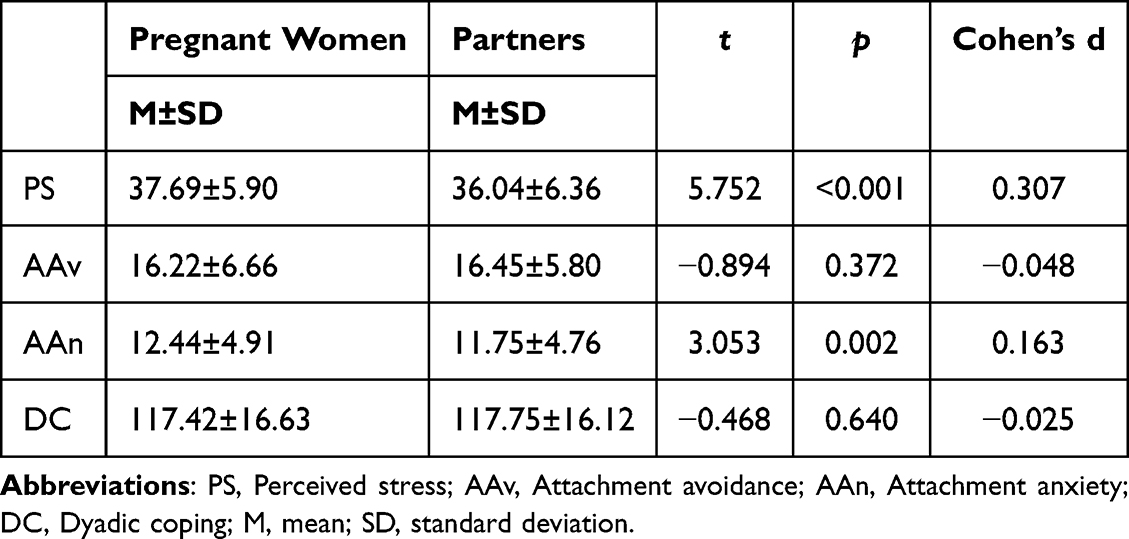 |
Table 2 The Mean Values, and Differences of the Study Variables Between the Pregnant Women and Their Partners (N =701couples) |
All variables were correlated with each other (p<0.05), as shown in Table 3. Notably, perceived stress in both pregnant women and their partners showed a significant positive correlation with adult attachment (attachment avoidance and attachment anxiety), while demonstrating a significant negative correlation with dyadic coping. Adult attachment (attachment avoidance and attachment anxiety) was significantly negatively correlated with dyadic coping. Additionally, perceived stress, adult attachment, and dyadic coping were significantly positively correlated between both partners.
 |
Table 3 Pearson Correlation Analysis of the Study Variables (N = 701 Couples) |
Analysis for the APIMeM
With attachment avoidance as the mediator, the results of the empirical distinguishability test showed that there was no significant difference between partners on any path (p=0.496>0.20). Therefore, treating pregnant women and their partners as indistinguishable dyad data by constraints in APIMeM facilitates simulation and computation using a more parsimonious model. Model fit indicators of χ2(6) =5.382, P=0.496, TLI=1.003, CFI=1.000, RMSEA=0.000, and SRMR=0.017 indicated that the model fit the data well. The model simplified by the constraints is shown in Figure 1. Individuals’ perceived stress positively predicted their own (β=0.325, p<0.001) and their partner’s (β=0.225, p<0.001) attachment avoidance. At the same time, individuals’ attachment avoidance negatively predicted their own (β=−0.156, p<0.001) and their partner’s (β=−0.057, p=0.042) dyadic coping. However, individuals’ perceived stress only negatively predicted their own dyadic coping (β=−0.058, p=0.040), indicating that there was only an actor effect between perceived stress and dyadic coping.
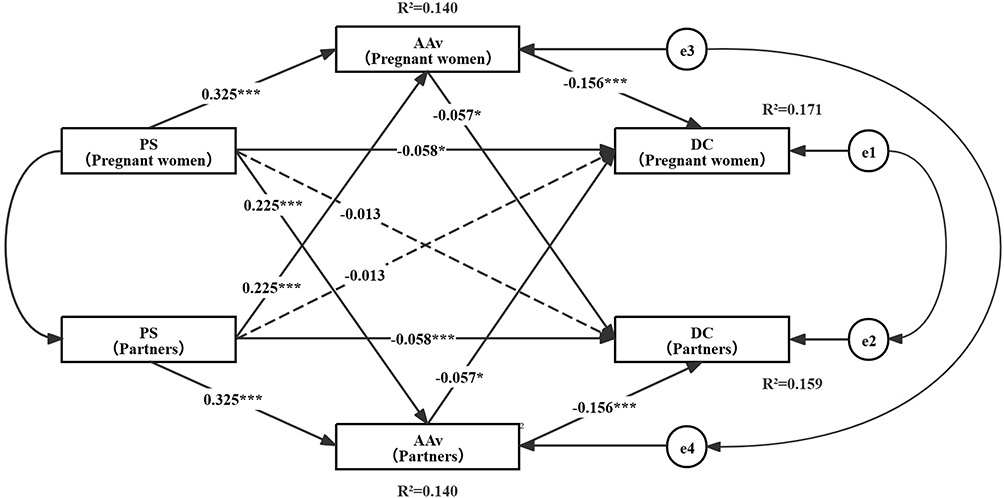 |
Figure 1 APIMeM of PS on DC through AAv with standardized coefficients. Lines represent significant paths, and dotted lines represent nonsignificant paths. *p <0.05, ***p <0.001. Abbreviations: PS, Perceived stress; AAv, Attachment avoidance; DC, Dyadic coping. |
With attachment anxiety as the mediator, the results of the empirical distinguishability test showed that there was a significant difference between partners on each path (p=0.015<0.20). Therefore, treating pregnant women and their partners as distinguishable dyad data. The model simplified by the constraints is shown in Figure 2. Pregnant women’s perceived stress positively predicted their own (β=0.324, p<0.001) and their partners’ (β=0.128, p<0.001) attachment anxiety, while partners’ perceived stress could only positively predict their own attachment anxiety (β=0.179, p<0.001), indicating that there was only actor effect between partners’ perceived stress and attachment anxiety. Partners’ attachment anxiety negatively predicted their own (β=−0.087, p=0.023) and pregnant women’s (β=−0.083, p=0.024) dyadic coping, while pregnant women’s attachment anxiety could only negatively predicted their own dyadic coping (β=−0.222, p<0.001). Partners’ perceived stress could only negatively predict their own dyadic coping (β=−0.098, p=0.011), indicating that there was only actor effect between partners’ perceived stress and dyadic coping.
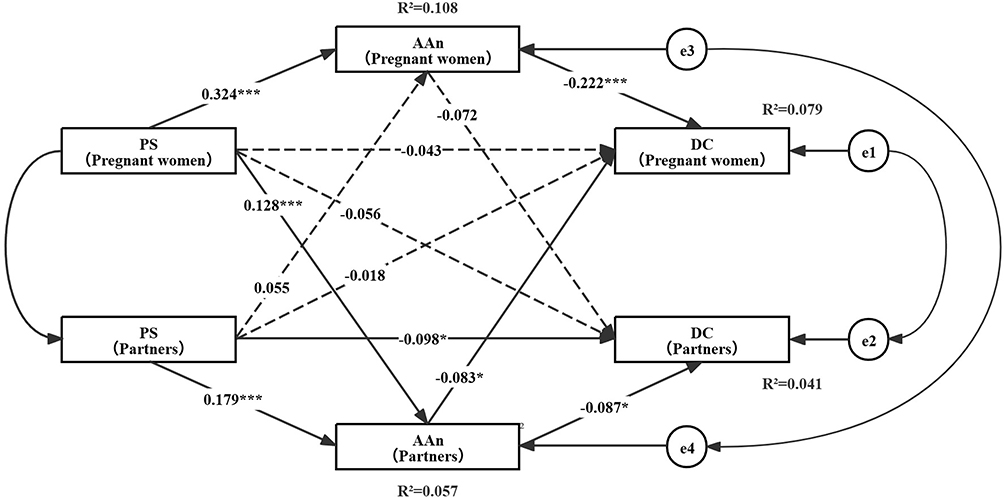 |
Figure 2 APIMeM of PS on DC through AAn with standardized coefficients. Lines represent significant paths, and dotted lines represent nonsignificant paths. *p <0.05, ***p <0.001. Abbreviations: PS, Perceived stress; AAn, Attachment anxiety; DC, Dyadic coping. |
Tables 4 and 5 present the total, direct, and indirect effects of pregnant women and their partners in the APIMeM. Attachment avoidance mediated the effect of perceived stress on dyadic coping, with a statistically significant actor indirect (β=−0.063, 95% CI [−0.089, −0.039]) and partner indirect effects (β=−0.054, 95% CI [−0.080, −0.029]). In other words, attachment avoidance completely mediated the actor effect and the partner effect of perceived stress on dyadic coping in pregnant couples. Furthermore, attachment anxiety was found to mediate the effect of perceived stress on dyadic coping for both pregnant women (β=−0.083, 95% CI [−0.116, −0.054]) and their partners (β=−0.020, 95% CI [−0.041, −0.004]), with a statistically significant actor indirect effect. The study also revealed a statistically significant mediator effect of perceived stress on dyadic coping for both pregnant women (β=−0.027, 95% CI [−0.058, −0.004]) and their partners (β=−0.034, 95% CI [−0.064, −0.009]), with a statistically significant partner indirect effect.
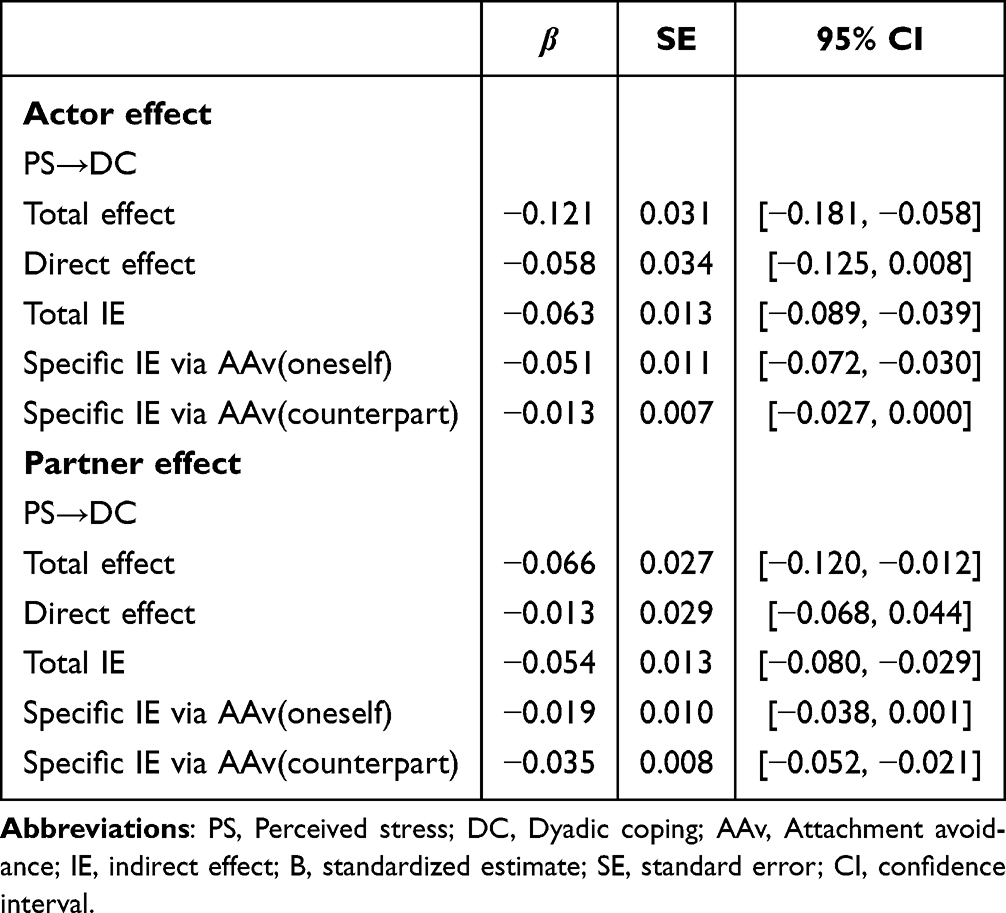 |
Table 4 Total, Direct, and Indirect Effects of AAv in the APIMeM |
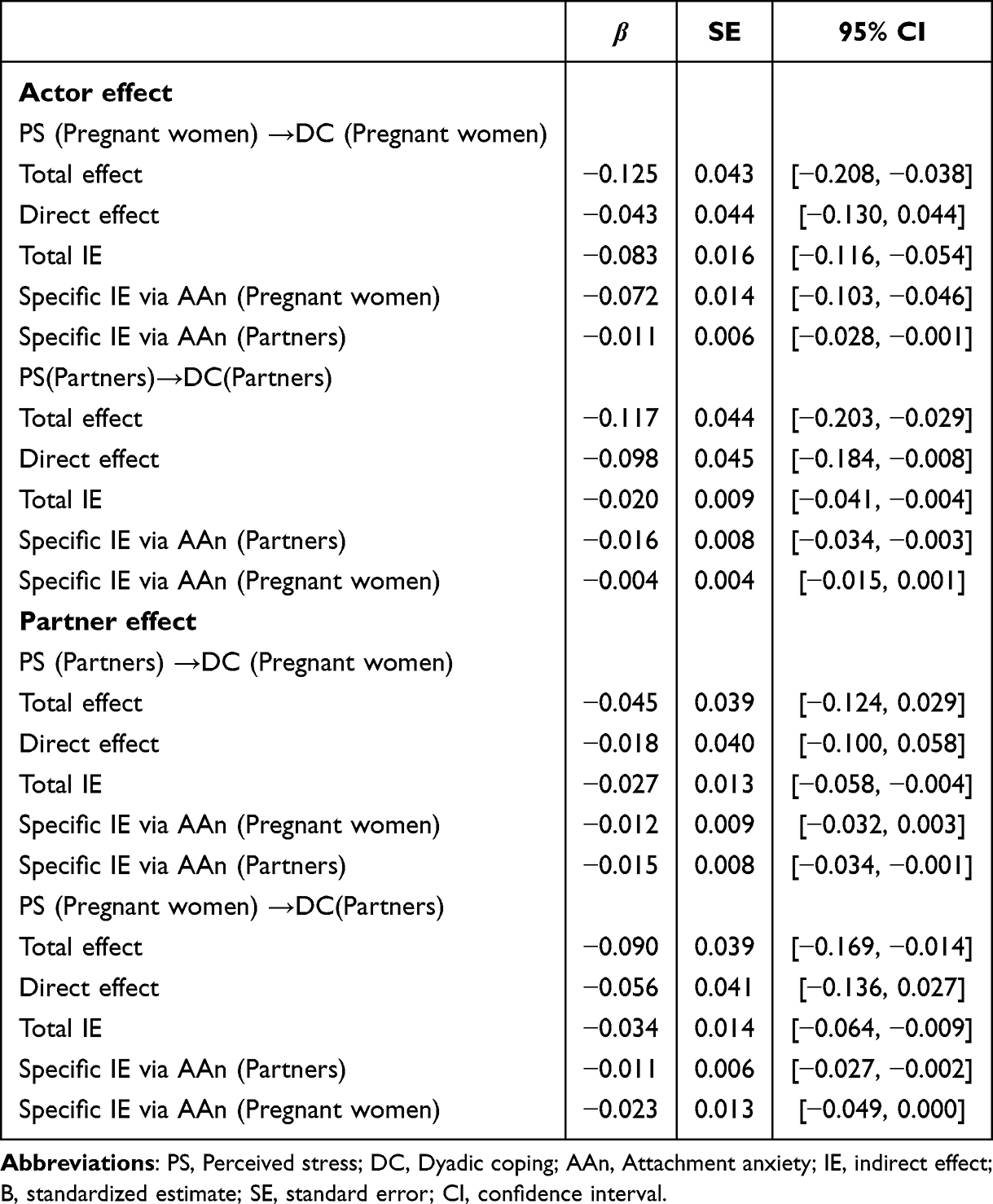 |
Table 5 Total, Direct, and Indirect Effects of AAn in the APIMeM |
Discussion
The present study revealed significant correlations among perceived stress, adult attachment, and dyadic coping in couples during pregnancy. The previous hypotheses were also tested, and the results indicated that the prenatal couple’s perceived stress negatively predicted their own dyadic coping, and adult attachment mediated the negative effects of individual perceived stress on dyadic coping. The current study validated the interplay between both partners’ perceived stress and their dyadic coping from a dyadic perspective. The study also revealed the mechanisms by which adult attachment may act as a mediator in the effects of perceived stress and dyadic coping in couples with pregnancy.
Sex Differences in Perceived Stress, Adult Attachment, and Dyadic Coping in Couples with Pregnancy
The present study found that there was no statistically significant difference between sexual for dyadic coping scores. This may be due to the factor that pregnant women and their partners share a common goal during pregnancy: ensuring the health of the pregnant woman and the fetus for a smooth pregnancy. In order to achieve this goal, they collaborate and implement various coping mechanisms. This common goal engenders greater consistency in their dyadic coping without significant differences.46 However, the score was lower than that reported in other related studies.47–49 This may be because lower dyadic coping scores may be associated with the number of pregnancies. Molgora et al50 found that first-time parents may exhibit lower dyadic coping in late pregnancy due to reasons such as fear of labor and delivery during their first delivery. More than half of the participants in this study were first-time parents. In addition, research indicates that education level and monthly income are influential factors in the dyadic coping.47 The study, which was conducted in central and western China, found that the region’s economic and educational development was relatively lagging. More than half of the couples had a monthly household income below the national average, and less than a college degree. As a result, pregnant women and their partners may lack sufficient economic resources, as well as adequate knowledge and skills to cope with the challenges of pregnancy.
This study found that pregnant women reported higher levels of perceived stress compared to their partners, which aligns with prior research.51 Biological factors contribute to this elevated stress, including increased cortisol secretion through the hypothalamic-pituitary-adrenal (HPA) axis during pregnancy.52 In traditional Chinese culture, women typically assume a greater role in child-rearing. This can lead to concerns among some women that they are not meeting the expectations of their role as mothers, or that their parenting style does not align with traditional norms.46 Furthermore, concerns regarding the health and safety of the fetus, apprehensions about postnatal body shape and activity contribute to heightened perceived stress levels in pregnant women.53
In accordance with the findings of preceding studies, which indicated heightened levels of attachment anxiety in pregnant women in comparison to their partners, the present study corroborated this observation.54 The observed discrepancy may be attributed to a range of physiological and psychological factors associated with pregnancy. These include physical symptoms such as nausea, vomiting, fatigue, and sleep disorders, as well as concerns about the health of the fetus and the pressure of identity change. These factors make pregnant women more eager to obtain a sense of security and support from their partners and other significant others.55 This may result in heightened levels of attachment anxiety in pregnant women. These findings underscore the importance of sex difference and the implementation of tailored interventions to improve dyadic coping levels in affected populations.
Perceived Stress, Adult Attachment, and Dyadic Coping in APIMeM
Intra-Individual Perceived Stress and Adult Attachment on Dyadic Coping
The results of the present study partly supported hypotheses H1a and H2a, indicating that individuals’ perceived stress had a direct negative effect on their own dyadic coping, with the exception of pregnant women, where perceived stress had no effect on dyadic coping when added to the attachment anxiety as a mediator. This finding aligns robustly with the Conservation of Resources (COR) theory,56 which posits that individuals strive to retain and protect valued resources, and that stress arises when these resources are threatened or lost. Individuals experiencing elevated stress may become depleted of personal psychological resources, thereby leaving them with fewer resources to invest in supportive dyadic interactions, such as providing emotional support or engaging in shared problem-solving with their partner.23 Martos et al57 demonstrated that high stress levels can impair an individual’s ability to provide responsive support to their partner. The present findings are consistent with the research showing that in recent decades, changing attitudes to parenthood, coupled with significant economic pressures, have resulted in Chinese fathers taking on more responsibility for childcare and housework, while more women are entering the workforce.58 These changes are contributing to an increase in perceived stress among expectant parents. Research by Ogan et al59 concluded that partners’ stress contagion effects can create a cyclical pattern of resource drain, undermining mutual support processes.
Attachment avoidance is defined as an individual’s tendency to avoid intimacy and dependence on others in close relationships. Individuals with high attachment avoidance typically show distrust of intimate relationships and prefer independence and self-protection.60 The present study has determined that individuals’ attachment avoidance has a detrimental effect on their own dyadic coping (actor direct effect). According to a study by Wendołowska et al,61 individuals with high attachment avoidance tend to be more independent problem solvers in the face of stress and less likely to seek support from their partners, which may lead them to adopt a more negative dyadic coping approach.
Attachment anxiety is an individual’s excessive desire to be loved and cared for in intimate relationships and concerns about the stability of the relationship.62 The present study also found that individuals with high attachment anxiety negatively affected themselves dyadic coping (actor direct effect). According to Mikulincer and Shaver,63 individuals with high attachment anxiety frequently encounter difficulties in emotion regulation. When confronted with various challenges during pregnancy, pregnant women and their partners may overreact to negative emotions and conflict with their partner, rather than maintaining composure and adopting appropriate dyadic coping. Research has shown that levels of attachment anxiety during pregnancy are associated with levels of relationship insecurity. This has been demonstrated to influence the interaction and cooperation between pregnant women and their partners.64 Individuals with high attachment anxiety have been observed to hold diminished evaluations of their own worth and abilities, exhibiting reduced self-efficacy. This may result in a perception that they are unable to effectively cope with the challenges associated with pregnancy, potentially leading to a negative attitude towards dyadic coping.65
Intra-individual resource issues (elevated stress and insecure attachment) have a significant impact on an individual’s ability to contribute to the couple’s shared coping process. These findings underscore a key practical implication: taking individual perceived stress and attachment insecurities into consideration should be a fundamental prerequisite before intervening in the more complex interpersonal dynamics between partners during pregnancy.
High Correlations of Perceived Stress, Adult Attachment and Dyadic Coping Between Couples with Pregnancy
Our findings did not support the hypothesized partner effects (H1b). Specifically, an individual’s perceived stress did not have a direct negative impact on their partner’s dyadic coping in the APIMeM. It is worth noting, however, that correlational analyses showed a significant negative association between one partner’s perceived stress and the other’s dyadic coping. This is a critical finding. It indicates that while an individual’s perceived stress is correlated with their partner’s dyadic coping, this association is not a direct effect. Instead, it is fully accounted for by other variables in the model—most likely, the mediation through attachment (as partially seen in H3b). This underscores the necessity of mediation models like APIMeM to move beyond simple associations and identify the precise mechanisms at play.
The results partly supported the hypothesized partner effects (H2b), indicating that an individual’s adult attachment negatively predicted their partner’s dyadic coping, with the exception of partners, where attachment anxiety had no effect on dyadic coping when added to the attachment anxiety as a mediator. This finding emphasizes that adult attachment influences not only an individual’s own functioning, but also has a tangible cross-over effect on their partner’s ability to engage in constructive dyadic coping.27
This significant partner effect (H2b) stands in contrast to the non-significant direct partner effect of perceived stress on dyadic coping (H1b). This discrepancy suggests that while a partner’s perceived stress may not directly impact one’s coping, it is the manifestation of that stress through the lens of adult attachment that ultimately exerts the negative cross-partner influence, aligning with the Attachment Diathesis-Stress Process Model.31
Moreover, correlational analyses demonstrated that maternal and paternal perceived stress, adult attachment and dyadic coping were positively correlated. These findings imply that clinical psychological interventions for prenatal couples should not be employed in isolation. Although the levels of perceived stress and attachment anxiety were higher in pregnant women than in their partners, suggesting that the focus of intervention should be on the pregnant woman, according to our findings and the STM, this highlights the critical need for couple-focused interventions during pregnancy.22 Screening for and addressing adult attachment in both partners is essential, as improving one partner’s attachment security could enhance dyadic coping quality for prenatal couples.66
Mediating Roles and Dyadic Interactions in Adult Attachment
The present study found that the individual’s own attachment avoidance played a mediating role in the actor effects of perceived stress on dyadic coping in couples with pregnancy. The results supported hypotheses H3a. According to the Attachment Diathesis-Stress Process Model, individuals who exhibit high levels of attachment avoidance activate the attachment system when confronted with stress and employ distancing/deactivating avoidant/deactivating coping strategies, adopting a negative attitude toward dyadic coping.31 Research has corroborated these findings, demonstrating that higher levels of attachment avoidance are associated with poorer dyadic coping.67
It is noteworthy that dyadic coping is not directly influenced by the perceived stress of the partner. However, it can exhibit an indirect partner effect that is mediated by partners’ attachment avoidance. The results supported hypotheses H3b. These findings aligned with the Attachment Diathesis-Stress Process Model. The attachment behavioral system activates when an individual is in distress. Distress stirs attachment motivations to seek closeness, support or reassurance from romantic partners. These motivations then prompt attachment behaviors that ease distress and influence how one perceives the partner and the situation. Also, the partner’s behavior in the situation affects such perceptions.68 Empirical studies have reached the same conclusion. Partners who are highly attachment avoidance may not be able to respond adequately when the pregnant woman needs emotional comfort, which can affect dyadic coping between couples.64 The presence of a partner with elevated levels of attachment avoidance has the potential to influence the other partner’s involvement and motivation in dyadic coping strategies. This is due to the possibility that the partner who avoids dependence on the other may experience feelings of rejection or unappreciation, which in turn could affect their dyadic coping ability.61 Georgiadis et al also reported that partners may choose to cope alone with the stress of pregnancy rather than working with the pregnant woman to solve the problem. This behavior can make the pregnant woman feel neglected, which can affect the couple’s intimacy and dyadic coping.69
The present study found that attachment anxiety played a mediating role in the actor effects of perceived stress on dyadic coping for pregnant women and their partners. The results supported hypotheses H3a. According to the Attachment Diathesis-Stress Process Model, individuals who exhibit high levels of attachment anxiety activate the attachment system when confronted with stress and employ emotion-focused/hyperactivating coping strategies. These strategies sustain or escalate their worries and maintain their attachment system activated. As a result, they are unable to provide positive and effective dyadic coping.68 According to Kardatzke,70 attachment anxiety has a negative impact on positive dyadic interactions during stress coping in pregnant couples. Individuals with higher attachment anxiety tend to focus on (or be overwhelmed by) their own distress rather than their partner’s. They may be less inclined to use dyadic coping to help their partner relieve stress.
The present study revealed a noteworthy discovery: partners’ attachment anxiety plays a partner mediating role in two significant relationships. The results partly supported hypotheses H3b. These relationships include the association between pregnant women’s perceived stress and their partners’ dyadic coping, and partners’ perceived stress and pregnant women’s dyadic coping. Previous studies have concluded that, in the context of stress management, women may be more inclined to express emotions and seek support, and their attachment anxiety may be more likely to manifest in dyadic coping behaviors.69
The study’s findings differ from those of previous studies. In context of pregnancy, socio-cultural norms generally assign the role of “primary caregiver” to the partners, while the pregnant woman is regarded as the “cared-for” individual. In addition, the traditional Chinese culture, with its emphasis on subtlety and introversion, appears to influence men’s tendency to be independent and less emotional.71 This expectation requires men to conceal their vulnerability in stressful situations and prioritize practical support rather than emotional expression.72 Chae found that partners’ attachment anxiety may exhibit overprotective or overcontrolling behaviors, which can lead to resentment in the pregnant woman and further strain the relationship.73 These behaviors can hinder the effectiveness of dyadic coping, potentially resulting in conflict and tension between partners. The present study has revealed a strong correlation between pregnant women’s attachment anxiety and their partners’ attachment anxiety. However, the correlation may obscure the mediating effect of pregnant women’s attachment anxiety, which could be masked by the impact of their partners’ attachment anxiety.74 These reasons may be contributing factors to partners’ attachment anxiety playing such mediating roles.
Implications
The present study is of some theoretical significance, since, as far as we are aware, it is the first to investigate the relationship between perceived stress, adult attachment and dyadic coping for prenatal couples from the dyadic perspective. Based on the systematic transaction model, the present study explored the intrapersonal and interpersonal interaction of perceived stress, adult attachment, and dyadic coping. The findings enrich and expand the applicability of this model to the field of prenatal couple’s relationships. In addition, the Attachment Diathesis-Stress Process Model highlights the impact of adult attachment on stress coping processes in romantic partnerships. Further analysis of the proposed mediation model supports the view and enriches the Attachment Diathesis-Stress Process Model.
The present study is of practical significance in that it could provide references for conducting interventions and practices. Research has demonstrated that enhancing dyadic coping during pregnancy is crucial for improving both physical and mental health, as well as for promoting the intimate bond and enhancing the quality of life for expectant couples.47 According to previous study, insecure attachment influences dyadic coping in the face of stress and challenges.36 Hence, our findings underscore the important of interventions intended to improve dyadic coping should treat the couple as an integral unit. In particular, couples where one or both partners show insecure attachment (eg, avoidance or anxiety) are more likely to use negative coping strategies, which may reduce their effectiveness in dealing with stress during pregnancy and even the perinatal period.
Therefore, we propose the following concrete recommendations: First, routine antenatal educational programs for pregnant women and their partners should take into account their adult attachment. Identifying couples with insecure attachment enables tailored psychoeducation and counselling—such as through Emotionally Focused Therapy (EFT)66—to help develop more secure relational patterns and reinforce constructive coping skills. Second, healthcare providers should receive training to facilitate couple-centered communication and mutual understanding, thereby enabling couples to better navigate stress together. Brief screening tools could be administered during prenatal visits to identify at-risk couples. Lastly, healthcare institutions and policymakers should support the integration of couple-based counseling into standard perinatal care. Systemic support at this level encourages participation in relationship-strengthening interventions and promotes long-term family well-being. In conclusion, these findings will assist health professionals in delivering precise and effective psychological support to couples during pregnancy, thereby promoting their physical and mental well-being and enhancing family harmony.
Limitations
The limitations of the present study are as follows. Firstly, the participants were recruited from only three hospitals in central and western China. As a result, the sample may not be sufficiently representative, which could limit the generalizability of the findings to eastern regions. Future studies should employ a national multicenter design to enhance the external validity of the results. Secondly, our cross-sectional study can hardly explain the causality between the variables, so a longitudinal study can be carried out in the future. Thirdly, the use of self-report measures may introduce several biases. In addition to potential recall bias, social desirability bias may have led participants to underreport sensitive experiences (eg, relationship conflicts, high stress levels) and overreport socially acceptable responses. Furthermore, common method variance could inflate the observed relationships between variables since all measures were collected from the same source. Hence, questionnaire surveys and interviews need to be combined in our future work to make the findings more scientific. Finally, although key demographic covariates were controlled for, other potentially influential psychosocial and contextual factors were not measured. Their omission may confound the observed associations. Subsequent studies should include these variables to obtain a more comprehensive understanding of the dyadic dynamics during pregnancy.
Conclusion
Perceived stress significantly predicted dyadic coping among couples during pregnancy, with adult attachment mediating this relationship. Both actor and partner effects were observed, indicating that an individual’s stress and adult attachment influenced not only their own but also their partner’s coping abilities. These findings highlight the dyadic and interdependent nature of stress and coping processes in expectant couples. The mediating role of adult attachment suggests that it represents a key mechanism through which perceived stress impairs couples’ dyadic coping. Consequently, attachment-based interventions should be incorporated into prenatal care to mitigate the adverse effects of stress and enhance dyadic coping by addressing underlying attachment insecurities. Healthcare providers should thus adopt a couple-centered approach, assessing and supporting both partners as an interdependent unit. Future research should continue to develop and evaluate interventions aimed at strengthening attachment security to improve dyadic coping throughout pregnancy.
Data Sharing Statement
The data that underpins the conclusions of this study is not accessible to the public due to its sensitive and confidential nature. Interested parties may obtain the data by submitting a formal request to either of the corresponding authors.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Board of The Xiangya School of Nursing, Central South University (Reference No: E2022120).
Acknowledgments
We would like to express our gratitude to pregnant women and their partners who have participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Hunan Provincial Major Research Development Program of China (grant number 2023SK2028); Changsha Municipal Natural Science Foundation (grant number kq2208357) and Natural Science Foundation of Hunan Province (grant number 2024JJ6611). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wang H, Chen H. Aging in china: challenges and opportunities. China CDC Wkly. 2022;4(27):601–602. doi:10.46234/ccdcw2022.130
2. GBD. 2021 Fertility and Forecasting Collaborators. Global fertility in 204 countries and territories, 1950-2021, with forecasts to 2100: a comprehensive demographic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2057–2099. doi:10.1016/S0140-6736(24)00550-6
3. Tatum M. China’s three-child policy. Lancet. 2021;397(10291):2238. doi:10.1016/S0140-6736(21)01295-2
4. Li Y. The application and development of traditional family theory in contemporary China PhD Thesis. University of Minho; 2021.
5. Zhou H, Wang X, Li M. Parental stress, coercive and encouraging parenting among Chinese one-child, two-child and three-child families. Families Relationships Societies. 2024; 2024:1–21.
6. Martin RA, Kuiper NA, Olinger LJ, Dance KA. Humor, coping with stress, self-concept, and psychological well-being. humr. 1993;6(1):89–104. doi:10.1515/humr.1993.6.1.89
7. Yin X, Sun N, Jiang N, et al. Prevalence and associated factors of antenatal depression: systematic reviews and meta-analyses. Clin Psychol Rev. 2021;83:101932. doi:10.1016/j.cpr.2020.101932
8. Rao WW, Zhu XM, Zong QQ, et al. Prevalence of prenatal and postpartum depression in fathers: a comprehensive meta-analysis of observational surveys. J Affect Disord. 2020;263:491–499. doi:10.1016/j.jad.2019.10.030
9. Roddy Mitchell A, Gordon H, Atkinson J, et al. Prevalence of perinatal anxiety and related disorders in low- and middle-income countries: a systematic review and meta-analysis. JAMA Network Open. 2023;6(11):e2343711. doi:10.1001/jamanetworkopen.2023.43711
10. Leiferman JA, Farewell CV, Jewell J, et al. Anxiety among fathers during the prenatal and postpartum period: a meta-analysis. J Psychosomatic Obstet Gynecol. 2021;42(2):152–161. doi:10.1080/0167482X.2021.1885025
11. Nisar A, Yin J, Waqas A, et al. Prevalence of perinatal depression and its determinants in Mainland China: a systematic review and meta-analysis. J Affect Disord. 2020;277:1022–1037. doi:10.1016/j.jad.2020.07.046
12. Xiao G, Wang H, Hu J, Zhao Z, Li Q, Qin C. Prevalence of antenatal depression and postpartum depression among Chinese fathers: a systematic review and meta-analysis. Heliyon. 2024;10(15). doi:10.1016/j.heliyon.2024.e35089
13. Yang L, Sun J, Nan Y, et al. Prevalence of perinatal anxiety and its determinants in mainland China: a systematic review and meta-analysis. J Affective Disorders. 2023;323:193–203. doi:10.1016/j.jad.2022.11.075
14. Chhabra J, McDermott B, Li W. Risk factors for paternal perinatal depression and anxiety: a systematic review and meta-analysis. Psychol Men Masculinities. 2020;21(4):593–611. doi:10.1037/men0000259
15. Dachew B, Ayano G, Duko B, Lawrence B, Betts K, Alati R. Paternal depression and risk of depression among offspring: a systematic review and meta-analysis. JAMA Network Open. 2023;6(8):e2329159. doi:10.1001/jamanetworkopen.2023.29159
16. Smith A, Twynstra J, Seabrook JA. Antenatal depression and offspring health outcomes. Obstet Med. 2020;13(2):55–61. doi:10.1177/1753495X19843015
17. Speier DS. Strengthening couple relationships to reduce the risk of perinatal mood and anxiety disorders for parents. J Health Visiting. 2015;3(3):160–165. doi:10.12968/johv.2015.3.3.160
18. Huang Y, Liu Y, Wang Y, Liu D. Family function fully mediates the relationship between social support and perinatal depression in rural Southwest China. BMC Psychiatry. 2021;21(1):151. doi:10.1186/s12888-021-03155-9
19. Collardeau F, Corbyn B, Abramowitz J, Janssen PA, Woody S, Fairbrother N. Maternal unwanted and intrusive thoughts of infant-related harm, obsessive-compulsive disorder and depression in the perinatal period: study protocol. BMC Psychiatry. 2019;19(1):94. doi:10.1186/s12888-019-2067-x
20. Xiao M, Hu Y, Huang S, Wang G, Zhao J, Lei J. Prevalence of suicidal ideation in pregnancy and the postpartum: a systematic review and meta-analysis. J Affective Disorders. 2022;296:322–336. doi:10.1016/j.jad.2021.09.083
21. Seefeld L, Handelzalts JE, Horesh D, et al. Going through it together: dyadic associations between parents’ birth experience, relationship satisfaction, and mental health. J Affect Disord. 2024;348:378–388. doi:10.1016/j.jad.2023.12.044
22. Bodenmann G, Randall AK, Falconier MK. Coping in couples: the Systemic Transactional Model (STM). In: Couples Coping with Stress: A Cross-Cultural Perspective. Routledge/Taylor & Francis Group; 2016:5–22.
23. Bodenmann G. Dyadic coping and its significance for marital functioning. Couples Coping Stress. 2005;2005:33–49. doi:10.1037/11031-002
24. Landolt SA, Weitkamp K, Roth M, Sisson NM, Bodenmann G. Dyadic coping and mental health in couples: a systematic review. Clin Psychol Rev. 2023;106:102344. doi:10.1016/j.cpr.2023.102344
25. Molgora S, Acquati C, Saita E. The role of dyadic coping for the individual and relational well-being of couples during the transition to parenthood. J Family Issues. 2022;43(5):1364–1385. doi:10.1177/0192513X211022394
26. Brandão T, Brites R, Hipólito J, Pires M, Nunes O. Dyadic coping, marital adjustment and quality of life in couples during pregnancy: an actor-partner approach. J Reprod Infant Psychol. 2020;38(1):49–59. doi:10.1080/02646838.2019.1578950
27. Mikulincer M, Shaver PR. Attachment in Adulthood, second Edition: Structure, Dynamics, and Change. Guilford Publications; 2016.
28. Hendrick C, Hendrick SS. Attachment theory and close adult relationships. Psychological Inquiry. 1994;5(1):38–41. doi:10.1207/s15327965pli0501_6
29. Mikulincer M, Goodman GS. Dynamics of Romantic Love: Attachment, Caregiving, and Sex. Guilford Press; 2006.
30. Mikulincer M, Shaver PR. Attachment in Adulthood, First Edition: Structure, Dynamics, and Change. Guilford Publications; 2010.
31. Simpson JA, Rholes WS. Adult attachment orientations and well-being during the transition to parenthood. Curr Opinion Psychol. 2019;25:47–52. doi:10.1016/j.copsyc.2018.02.019
32. Galbally M, Watson S, Lewis AJ, Power J, Buus N, van IJzendoorn M. Maternal attachment state of mind and perinatal emotional wellbeing: findings from a pregnancy cohort study. J Affect Disord. 2023;333:297–304. doi:10.1016/j.jad.2023.04.016
33. Paley BJ, Cox MJ, Harter KS, Margand NA. Adult attachment stance and spouses’ marital perceptions during the transition to parenthood. Attach Hum Dev. 2002;4(3):340–360. doi:10.1080/14616730210167276
34. Bröning S, Wartberg L. Attachment orientations: associations with romantic partners’ self-regulation and dyadic coping. J Sex Marital Ther. 2024;50(4):512–526. doi:10.1080/0092623X.2024.2322566
35. Gagliardi S, Bodenmann G, Heinrichs N, Maria Bertoni A, Iafrate R, Donato S. Differences in relationship quality and dyadic coping for attachment-related couple types. Psychother Psychosom Med Psychol. 2013;63(5):185–192. doi:10.1055/s-0032-1333291
36. Alves S, Milek A, Bodenmann G, Fonseca A, Canavarro MC, Pereira M. Romantic attachment, dyadic coping, and parental adjustment across the transition to parenthood. Personal Relationships. 2019;26(2):286–309. doi:10.1111/pere.12278
37. Ledermann T, Macho S, Kenny DA. Assessing mediation in dyadic data using the actor-partner interdependence model. Struct Equ Modeling. 2011;18(4):595–612. doi:10.1080/10705511.2011.607099
38. Ackerman RA, Kenny DA. APIMPowerR: an interactive tool for actor-partner interdependence model power analysis. Available from: https://robert-a-ackermanshinyappsio/APIMPowerRdis.
39. Ding Y, Han R, Pan JH, Yuan HB, Gao L. Perceived stress and prenatal depression symptoms among couples with gestational diabetes mellitus: the mediating role of dyadic coping. Midwifery. 2024;139:104190. doi:10.1016/j.midw.2024.104190
40. Gao L, Chan SW, Mao Q. Depression, perceived stress, and social support among first‐time Chinese mothers and fathers in the postpartum period. Research in Nursing & Health. 2009;32(1):50–58. doi:10.1002/nur.20306
41. Xu F, Hilpert P, Randall AK, Li Q, Bodenmann G. Validation of the dyadic coping inventory with Chinese couples: factorial structure, measurement invariance, and construct validity. Psychological Assessment. 2016;28(8):e127. doi:10.1037/pas0000329
42. Zhao L, Hao Z. Reliability and validity of the experiences in close relationships scale-the Chinese short version in Chinese adults. Chin J Behav Med Brain Sci. 2019; 2019:755–759.
43. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
44. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
45. National economy witnessed steady progress amidst stability with major development targets achieved successfully in 2024. National Bureau of Statistics of China. 2025. Available from: https://www.stats.gov.cn/english/PressRelease/202501/t20250117_1958330.html.
46. Lau Y. Traditional Chinese pregnancy restrictions, health-related quality of life and perceived stress among pregnant women in Macao, China. Asian Nurs Res. 2012;6(1):27–34. doi:10.1016/j.anr.2012.02.005
47. Fan W, Ma Y, Xie S, et al. Pregnant women’s dyadic coping and associated factors: a cross-sectional study utilizing latent profile analysis. IJWH. 2024;16:1009–1022. doi:10.2147/IJWH.S458763
48. Liu M, Fang Y, Liu M, et al. The dyadic associations among self-efficacy, dyadic coping, and health-related quality of life between high-risk pregnant women and spouses: a cross-sectional study. Qual Life Res. 2024;33(8):2235–2245. doi:10.1007/s11136-024-03692-2
49. Xue B, Wang X, Tang J, et al. Relationship between dyadic coping, resilience and fear of childbirth in expectant couples: an actor-partner interdependence model approach. Midwifery. 2024;137:104117. doi:10.1016/j.midw.2024.104117
50. Molgora S, Acquati C, Fenaroli V, Saita E. Dyadic coping and marital adjustment during pregnancy: a cross-sectional study of Italian couples expecting their first child. International J Psychol. 2019;54(2):277–285. doi:10.1002/ijop.12476
51. Baldoni F, Giannotti M, Casu G, Luperini V, Spelzini F. A dyadic study on perceived stress and couple adjustment during pregnancy: the mediating role of depressive symptoms. J Family Issues. 2020;41(11):1935–1955. doi:10.1177/0192513X20934834
52. Dickens MJ, Pawluski JL. The HPA axis during the perinatal period: implications for perinatal depression. Endocrinology. 2018;159(11):3737–3746. doi:10.1210/en.2018-00677
53. Rabipoor S, Abedi M. Perceived stress and prenatal distress during pregnancy and its related factors. J Res Develop Nurs Midwifery. 2020;17(1):67–80. doi:10.29252/jgbfnm.17.1.67
54. Conde A, Figueiredo B, Bifulco A. Attachment style and psychological adjustment in couples. Attachment & Human Development. 2011;13(3):271–291. doi:10.1080/14616734.2011.562417
55. Li TG, Zhao LX. Adult attachment and depression level in pregnant women. J Int Reproduc Health. 2011;30(No. 6):440–443.
56. Hobfoll SE. Conservation of resources. A new attempt at conceptualizing stress. Am Psychol. 1989;44(3):513–524. doi:10.1037//0003-066x.44.3.513
57. Martos T, Sallay V, Nagy M, Gregus H, Filep O. Stress and dyadic coping in personal projects of couples - A pattern-oriented analysis. Front Psychol. 2019;10:400. doi:10.3389/fpsyg.2019.00400
58. Zheng J, Gao L. Parenting self-efficacy and social support among parents in mainland China across the first six months postpartum: a prospective cohort study. Midwifery. 2023;123:103719. doi:10.1016/j.midw.2023.103719
59. Ogan MA, Monk JK. Does stress promote or inhibit romantic partner support? A systematic review of competing hypotheses. J Family Theo Revie. 2025;17(3):742–773. doi:10.1111/jftr.12633
60. Daum C, Singer J, Schneider S, Shen MJ, Loggers ET. Attachment avoidance and anxiety impacting dyadic coping and communication in patients with metastatic sarcoma and their family caregivers. JCO. 2023;41(16_suppl):e24002–e24002. doi:10.1200/JCO.2023.41.16_suppl.e24002
61. Wendołowska A, Steć M, Czyżowska D. Supportive, delegated, and common dyadic coping mediates the association between adult attachment representation and relationship satisfaction: a dyadic approach. Int J Environ Res Public Health. 2022;19(13):8026. doi:10.3390/ijerph19138026
62. Campbell L, Marshall T. Anxious attachment and relationship processes: an interactionist perspective. J Personality. 2011;79(6):1219–1250. doi:10.1111/j.1467-6494.2011.00723.x
63. Mikulincer M, Shaver PR. Attachment orientations and emotion regulation. Cur Opinion Psychol. 2019;25:6–10. doi:10.1016/j.copsyc.2018.02.006
64. Brandão T, Brites R, Pires M, Hipólito J, Nunes O. Anxiety, depression, dyadic adjustment, and attachment to the fetus in pregnancy: actor-partner interdependence mediation analysis. J Fam Psychol. 2019;33(3):294–303. doi:10.1037/fam0000513
65. Arriaga XB, Eller J, Kumashiro M, Rholes WS, Simpson JA. Self-efficacy and declines over time in attachment anxiety during the transition to parenthood. Soc Psychol Personal Sci. 2021;12(5):658–666. doi:10.1177/1948550620933411
66. Wiebe SA, Johnson SM. A review of the research in emotionally focused therapy for couples. Fam Process. 2016;55(3):390–407. doi:10.1111/famp.12229
67. Wendołowska A, Czyżowska N, Czyżowska D. The role of attachment and dyadic coping in shaping relational intimacy: actor-partner interdependence model. Int J Environ Res Public Health. 2022;19(23):16211. doi:10.3390/ijerph192316211
68. Simpson JA, Steven Rholes W. Adult attachment, stress, and romantic relationships. Curr Opin Psychol. 2017;13:19–24. doi:10.1016/j.copsyc.2016.04.006
69. Georgiadis B, Wilkinson R. Dyadic coping and attachment dimensions in young adult romantic relationships. Am Res J Humanities Social Sci. 2023;2023.
70. Kardatzke KN. Perceived stress, adult attachment, dyadic coping, and marital satisfaction of counseling graduate students. The University of North Carolina at Greensboro; 2009. Available from: https://search.proquest.com/openview/059c3e8d427b1c4e2a10f843663e99af/1?pq-origsite=gscholar&cbl=18750.
71. Caldwell-Harris C, Kronrod A, Yang J. Do more, say less: saying “I love you” in Chinese and American cultures. Intercult Pragmat. 2013;10(1):41–69. doi:10.1515/ip-2013-0002
72. Berke DS, Reidy D, Zeichner A. Masculinity, emotion regulation, and psychopathology: a critical review and integrated model. Clinic Psychol Rev. 2018;66:106–116. doi:10.1016/j.cpr.2018.01.004
73. Chae JY. The influence of pregnant couples’ attachment representation for parents of origin on their psychological symptoms. Fam Environ Res. 2019;57(1):41–50. doi:10.6115/fer.2019.004
74. Kenny DA, Kashy DA, Cook WL. Dyadic Data Analysis. Guilford Press; 2006.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.