Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
The Relationship Between Patent Foramen Ovale and Unexplained Dizziness: A Prospective Analysis in China
Authors Cao Q ![]() , Shen Y
, Shen Y ![]() , Hou Z, Li D, Tang B, Xu L, Li Y
, Hou Z, Li D, Tang B, Xu L, Li Y ![]()
Received 1 April 2022
Accepted for publication 29 June 2022
Published 26 July 2022 Volume 2022:18 Pages 1495—1505
DOI https://doi.org/10.2147/NDT.S367140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Qian Cao,1,* Yu Shen,1,2,* Zhuo Hou,1 Defu Li,3 Boji Tang,1 Lijun Xu,1 Yanping Li4
1Department of Neurology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Nanchang University, Nanchang, People’s Republic of China; 3Jiangxi Provincial Key Laboratory of Preventive Medicine, Nanchang University School of Public Health, Nanchang, Jiangxi, People’s Republic of China; 4Department of Neuroelectrophysiology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lijun Xu, Department of Neurology, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China, Email [email protected] Yanping Li, Department of Neuroelectrophysiology, The Second Affiliated Hospital of Nanchang University, No. 1, Minde Road, Nanchang, Jiangxi, People’s Republic of China, Email [email protected]
Introduction: Patent foramen ovale (PFO) is potentially associated with abnormal embolisms, and it results in mixing of arteriovenous blood when its right-to-left shunt (RLS) emerges. Present studies have found that PFO is a risk factor that can lead to many diseases. However, few studies have examined the relationship between PFO and dizziness.
Methods: This study was a large single-center, prospective, controlled study. From March 2019 to March 2021, we recruited patients with dizziness were divided into two groups: “explained” and “unexplained”. All patients were submitted to contrast-enhanced transcranial Doppler ultrasound and screened for PFO. Transesophageal heart ultrasound or right heart catheterization was used to confirm PFO. Additionally, multiple factors were collected and statistical analysis was performed between the two groups.
Results: Among the 244 patients included, 123 were in the “explained” group and 121 were in the “unexplained” group. The prevalence of PFO in the “explained” group was 34 (27.4%) compared to 79 (64.7%) in the “unexplained” group. In the “explained” group, 7 were RLS level IV, 6 were level III, 7 were level II, and 14 were level I. For the “unexplained” group, the numbers of patients with levels IV, III, II and I were 27, 26, 12 and 14, respectively. Univariate analysis revealed that PFO (χ2= 34.77, P < 0.001) and age (t = − 3.49, P < 0.001) seemed to be potential risk factor candidates for “unexplained” dizziness. In multiple regression analysis, age (OR = 0.97; 95% CI 0.95– 0.99) and the prevalence of PFO (OR = 4.37; 95% CI 2.50– 7.63) were statistically significant. Massively shunted PFO showed more pronounced risk factors (OR = 8.76; 95% CI 4.04– 19.03).
Conclusion: There was a high prevalence of PFO and a greater RLS level in unexplained dizziness. PFO and age were independent risk factors for unexplained dizziness. When treating with unexplained dizziness, especially among young people, we must pay attention to the presence of PFO.
Keywords: patent foramen ovale, PFO, right to left shunt, RLS, unexplained dizziness, contrast-enhanced transcranial Doppler ultrasound, cTCD
Introduction
The foramen ovale is a natural channel in infants, providing necessary substantial arterial oxygen for fetuses. The septum primum and secundum gradually fuse after birth. Incomplete fusion is termed patent foramen ovale (PFO).1 In the general population, the prevalence of PFO is approximately 25%,2 with the foramen ovale functioning as a heart valve but asymptomatic in silence. However, when the right atrium pressure exceeds the left atrium, such as with the Valsalva maneuver and pulmonary infarction, abnormal channels will open and increase the risk of paradoxical embolization.
As an arguably frequent neurologic complaint, dizziness is described as sensations of vertigo, lightheadedness, unsteadiness, disequilibrium, disorientation, or fainting, affecting 15–35% of the general population.3–5 Previous studies have found that the diagnosis and treatment of dizziness consume considerable medical resources;6 they reportedly exceeded $4 billion per year in U.S emergency rooms.7 Dizziness is present in almost all diseases and remains a challenge for physicians to diagnose. Even in light of extensive sequences of examinations and assessment, 5% of dizziness still cannot be diagnosed precisely, and is called “unexplained” dizziness8 leaving patients with persisting impairment.9 Therefore, it is particularly important to find the cause.
Present studies have demonstrated that the presence of PFO increases the risk of various diseases, such as stroke, migraine and decompression sickness.10–12 These reports have no specific information about whether the patient has concurrent dizziness. In our dizziness clinic, we accidentally discovered that patients with unexplained dizziness have a higher incidence of PFO. Will right-to-left shunts (RLSs) in the PFO incur dizziness? Although previous studies have reported three patients with RLSs with dizziness symptoms, the symptoms improved significantly after the shunts were eliminated. However, the relationship between RLS and unexplained dizziness remains unclear.13 A prospective, cross-sectional study is being conducted to explore the relationship between PFO and unexplained dizziness. We aim to discover the relationship between PFO and unexplained dizziness.
Patients and Methods
Patients
This research is a large, single-center, prospective study. It was carried out in the Second Affiliated Hospital of Nanchang University. This general tertiary hospital specifically operates dizziness clinics to provide medical and health services for 50 million people in the province. From March 2019 to March 2021, all patients with dizziness as the first symptom were included. We tried to clarify the cause of dizziness as much as possible through a series of methods such as detailed medical history inquiry, brain magnetic resonance imaging (MRI), video head pulse, and pure hearing threshold. After the burden of diagnosis and evaluation, patients were divided into two groups (“explained dizziness” and “unexplained dizziness”). The researchers conducted a simple random sampling from the “explained” dizziness group to match the number of the “unexplained” group. The “explained” group had a conclusive cause based on internationally accepted diagnostic criteria, including benign positional paroxysmal vertigo (BPPV), vestibular neuritis, vestibular migraine, Meniere’s disease, bilateral vestibular dysfunction, vestibular paroxysm, orthostatic hypotension, stroke, cerebellar ataxia, sudden deafness, cervical spondylosis, and intracranial space occupation. The other group was “unexplained dizziness”, and a diagnosis could not be established to explain symptoms. Participants in the “unexplained” dizziness group were followed up for six months14 to verify whether there was a new diagnosis.15 Follow-up is considered an important means of accurate diagnosis. All patients were diagnosed by two special neurologists who were unaware of the experiment. When there was disagreement, cases were submitted to a third senior doctor and an otolaryngologist to determine the final diagnosis. The ethics committee (Ethical Commission of the Second Affiliated Hospital of Nanchang University) approved our research protocol.
The inclusion criteria were: 1. dizziness as the first symptom; 2. younger than 75 years old (including 75); 3. volunteering to join and cooperate to improve various inspections. The exclusion criteria were: 1. functional dizziness; 2. cardiogenic dizziness; 3. combined tumor, endocrine, blood system, liver or kidney failure, and other possible dizziness diseases; 4. pulmonary fistula, patent ductus arteriosus, etc, requiring RLS, except for PFO; and 5. inability to adhere to follow-up.
After admission, the patients completed routine laboratory examinations and imaging examinations, as well as psychological evaluations, including brain MRI and magnetic resonance angiography (MRA), intracranial and cervical vascular color Doppler ultrasound, nystagmus and head pulse video, 24-hour dynamic electrocardiogram and blood pressure, and blood tests (blood routine, liver and kidney function, electrolytes, blood sugar and blood lipids, glycated hemoglobin, immunological index, tumor indicators). In addition, dizziness is associated with many factors.16 Therefore, we collected various related risk factors, including BMI, high blood pressure, diabetes, heart disease, hyperlipidemia, hyperhomocysteinemia, carotid plaque, and white matter lesions. A previous history of deep vein thrombosis, prior history of stroke, and any bad habits such as smoking and drinking, were also recorded.
Enrolled patients were screened for PFO using contrast-enhanced transcranial Doppler ultrasound (cTCD).17 For cTCD test-positive patients, after informing the patient of the condition and following the patient’s consent, transesophageal echocardiography or right heart catheterization was conducted to confirm it. cTCD uses a single-channel dual-depth mode to monitor the middle cerebral artery and chooses the vertebral artery in patients with poor temporal window sound penetration. The patient’s cubital vein venous indwelling catheter was connected to a three-way tube, and then a bolus was injected with mixed-blood activated saline (normal saline: air: patient blood = 8 mL: 1 mL: 1 mL). The patients were monitored for 25 seconds under calm breathing to determine whether there were bubbles in the middle cerebral artery. After the patients rested for 2 minutes, the above steps were repeated twice with the patient performing the Valsalva maneuver for 10 seconds after the bolus injection. The maximum flow rate of microbubbles (MB) detected by calm breathing or Valsalva maneuver was recorded. The RLS subflow classification adopts a 5-level method (Figures 1 and 2): negative (level 0): 0 MBs; level I: 1≤MBs≤10; level II:10<MBs≤25; level III: MBs>25, no rain curtain shape, the air plug can still be distinguished; and level IV: rain curtain-shaped air plug,18–20 RLS can be detected as an intrinsic type under calm breathing if it is a latent type only after Valsalva. Level I is a minor shunt, level II is a medium shunt, and levels III and IV are large shunts. cTCD can only confirm an RLS but cannot distinguish atrial septal defect, pulmonary fistula, and PFO. Therefore, patients with a positive test require perfect transesophageal ultrasound or right heart catheterization to support the diagnosis of PFO.
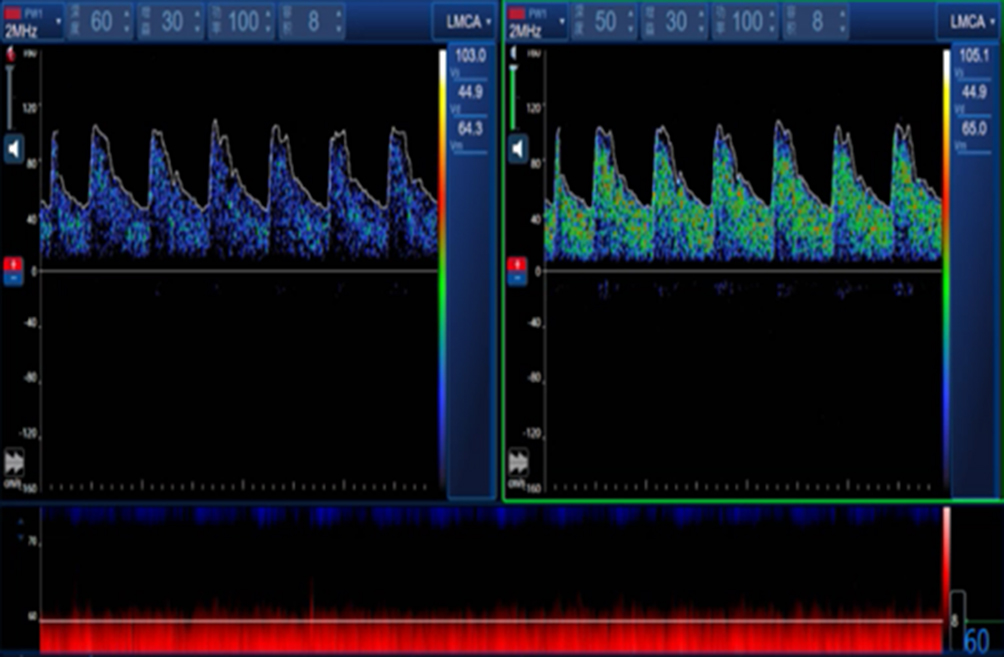 |
Figure 1 The negative result of RLS. |
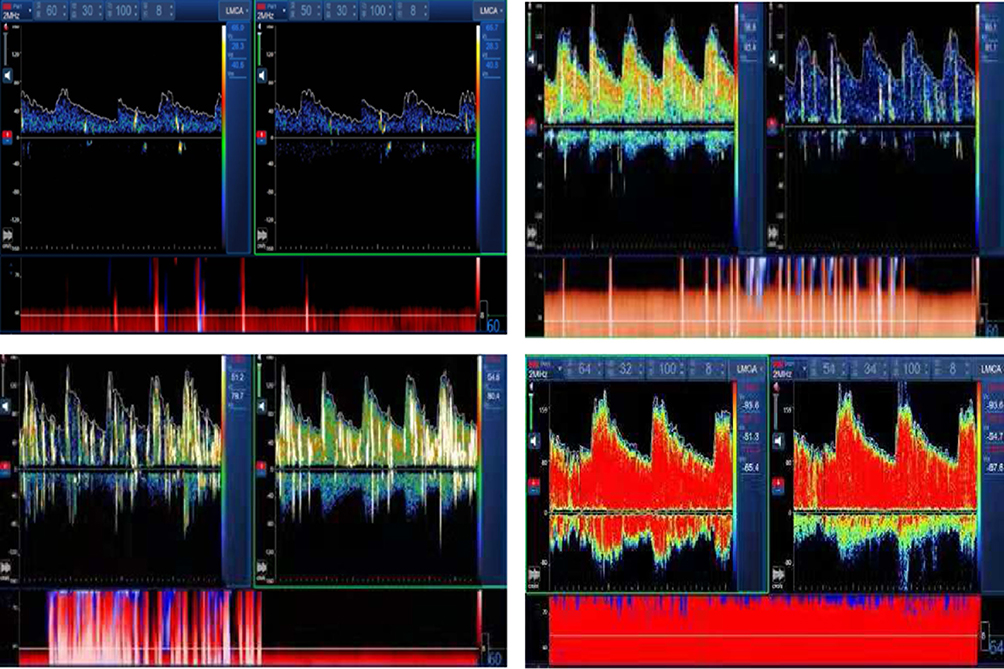 |
Figure 2 The different level of RLS, level (I) 1≤MBs≤10; level II: 10<MBs≤25; level III: >25 MBs, no rain curtain shape, the air plug can still be distinguished. Level IV: Rain curtain-shaped air plug. |
Patients with intrapulmonary shunts and atrial septal defects could not continue to participate, nor could patients with functional dizziness, cardiogenic dizziness, tumors, or endocrine diseases. For all patients with dizziness related to posture changes, blood oxygen saturation and blood pressure were tested in the supine position. Platypnea-orthodeoxia syndrome caused by PFO disease itself was excluded.21 Moreover, patients with migrainous features (nausea, photophobia, phonophobia, motion intolerance, catamenial association) without concurrent headache suspected diagnosis were also excluded.
Statistical Analysis
The population included was selected from patients who met the enrollment criteria in the past 2 years after screening. Based on clinical diagnosis, they were divided into two groups. The chi-square test was used for single-factor classification data. For continuous variable data, the independent-sample t-test was used for the variables that conformed to a normal distribution, and the Mann–Whitney U-test was used for the nonnormally distributed variables. To make the results more accurate, we included the single variable with P<0.1 in the multivariate logistic regression analysis. At the same time, the stepwise multiple regression model was used to calculate the OR and 95% CI. P<0.05 was considered statistically significant. All tests were conducted by IBM SPSS Statistics 25.0 software (SPSS, Chicago, IL, USA).
Results
In two years, 10,000 patients visited our hospital with the main complaint of dizziness, and most were outpatient visits with incomplete examinations. In nearly 10,000 patients, BPPV and stroke accounted for the vast majority. After screening, 123 patients with “unexplained” dizziness were included, 2 cTCD-positive patients quit during the follow-up examination, one was diagnosed with patent ductus arteriosus, and another was diagnosed with a pulmonary arteriovenous shunt. A total of 123 patients randomly selected for definite diagnosis joined the “explained” group (Figure 3). Finally, 244 patients were recruited (125 women and 119 men). In the “explained” group, there were 123 cases (average age=56.22 SD=12.16); 34 were diagnosed with BPPV, 21 with stroke, 14 with vestibular migraine, 8 with TIA, and 6 with vestibular neuronitis. Table 1 shows more details. Thirty-four people had concurrent PFO (27.4%), of whom VM (n=8; 23.5%) and BPPV (n=6; 16.7%) accounted for the majority. Figure 4 shows the diagnosis of people in the “explained” group concurrent with PFO. Among them, 27 had the intrinsic type (79.4%), and 7 were potential (20.6%). Seven were level IV RLS, 6 were level III, 7 were level II, and 14 were level I. There were 121 cases in the “unexplained” group (average age=49.74 SD=15.19). The prevalence of PFO reached 64.7% (n=79); 51 cases (64.5%) had the intrinsic type, 28 cases had the latent type (35.4%), and there were 27 cases of level IV, and 26 cases of level III, 12 cases of level II, and 14 cases of level I (Figure 5). We compared the two groups and found that the degree of RLS shunt in the “unexplained” group was significantly higher than that in the “explained” group (χ2=41.63 P<0.001). Tables 2 and 3 show detailed demographic statistics and clinical characteristics.
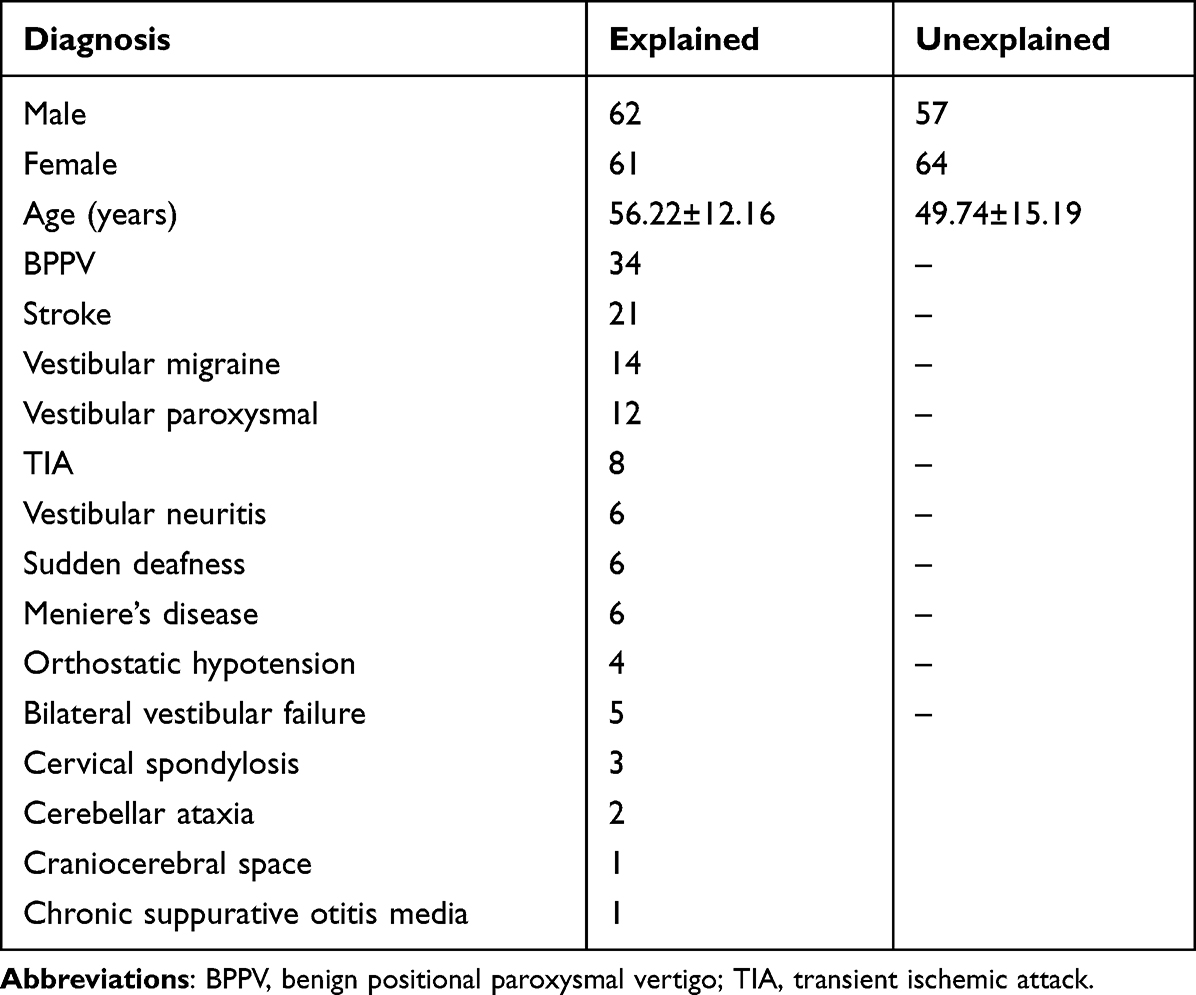 |
Table 1 Diagnoses of Explained and Unexplained Dizziness Groups |
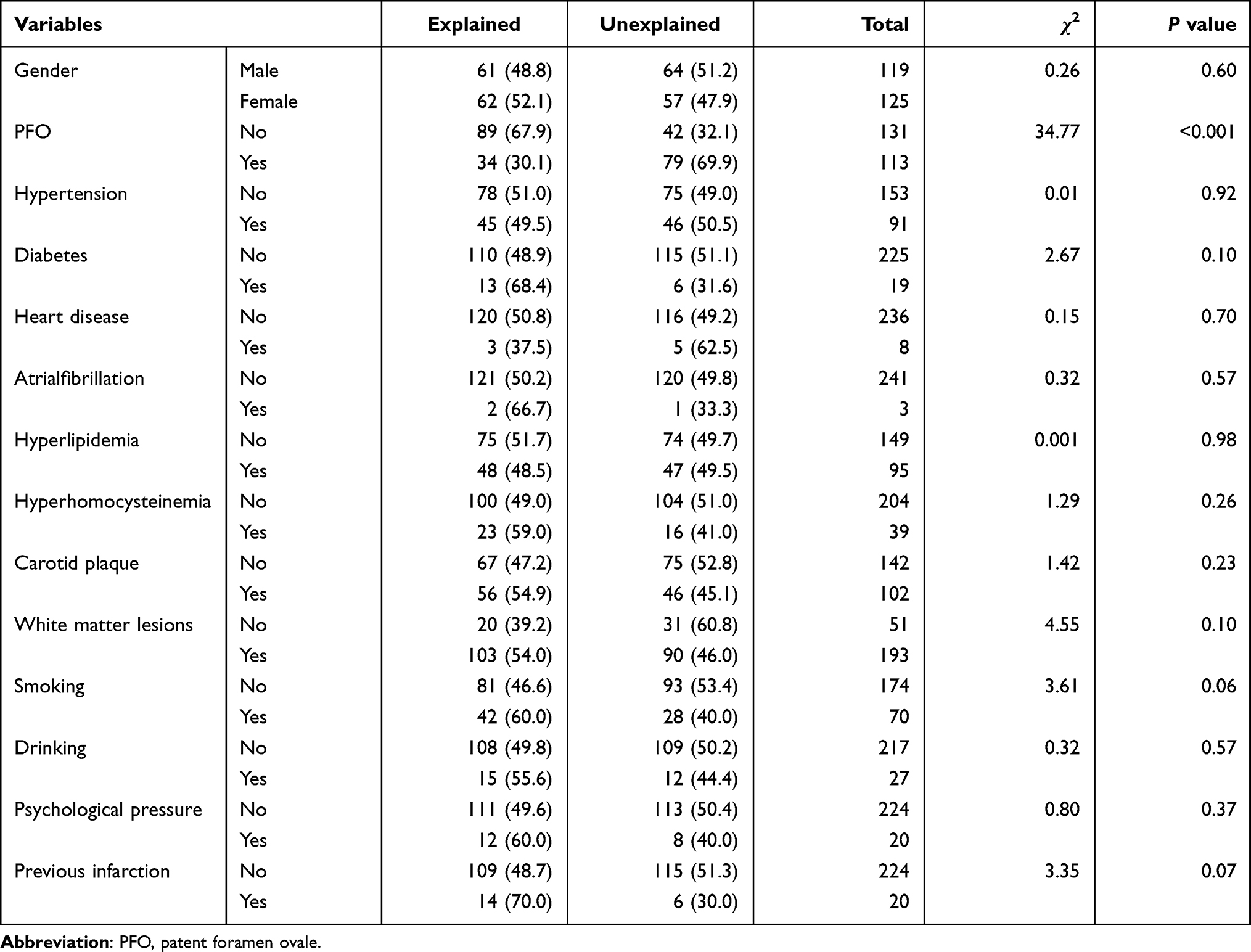 |
Table 2 Baseline Patient Characteristics in categorical variables analysis |
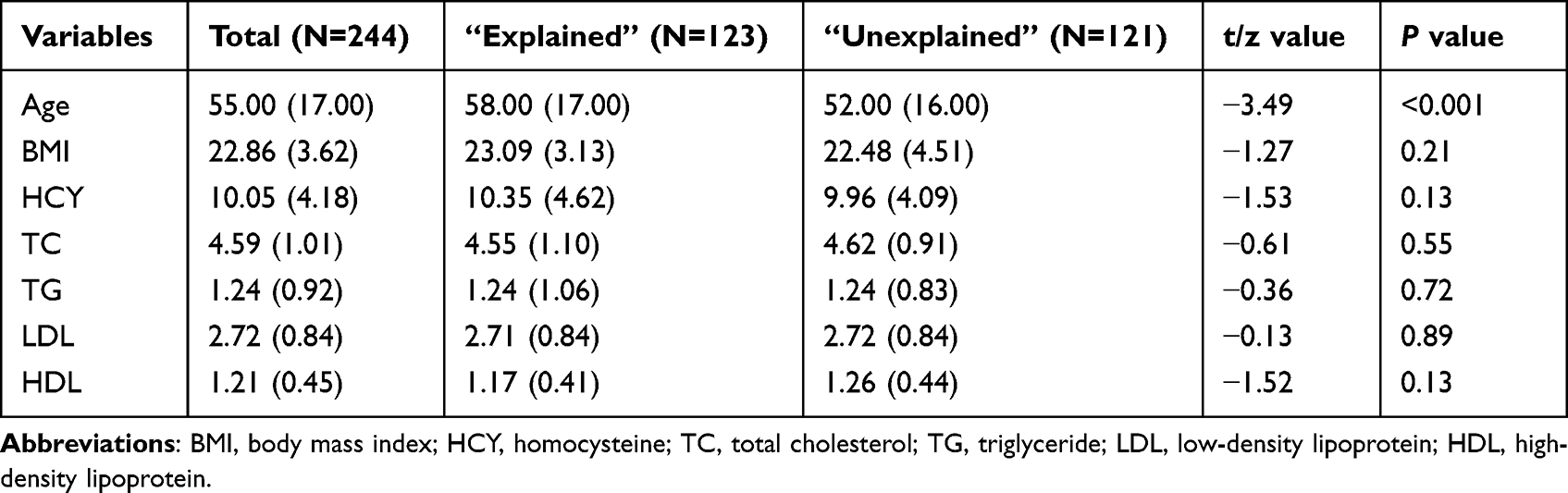 |
Table 3 Baseline Patient Characteristics in continuous variables analysis |
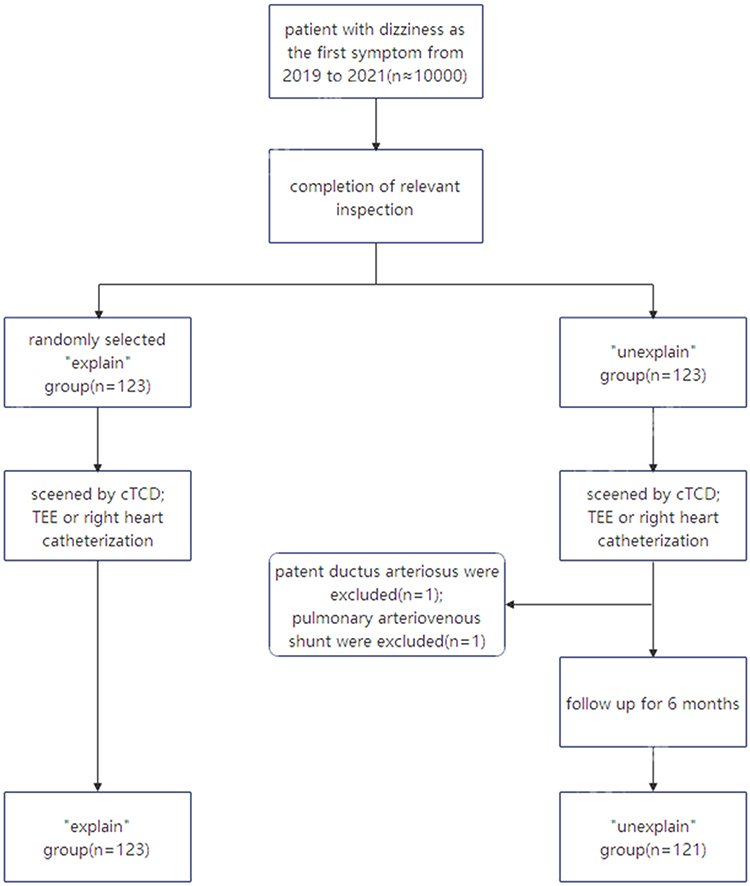 |
Figure 3 Flowchart in the study. |
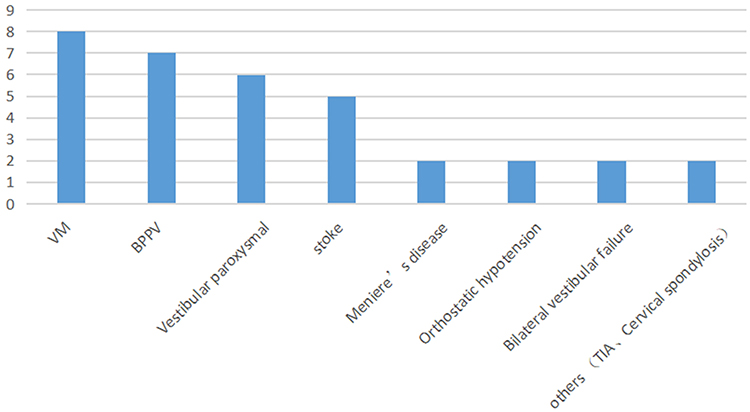 |
Figure 4 The number of cases in diagnosis concurrent with PFO in explained group. |
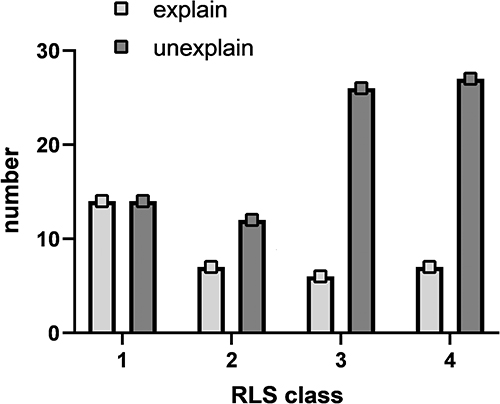 |
Figure 5 The number of cases in different degree of RLS shunt between the explained group and unexplained group. |
In univariate analysis, PFO (χ2=34.77, P<0.001) and age (t= −3.49, P<0.001) seemed to be potential candidates. A multiple regression analysis was performed and it was found that age (OR=0.97; 95% CI 0.95–0.99) and PFO (OR=4.37; 95% CI 2.50–7.63) were statistically significant, indicating that PFO and age were related to unexplained dizziness. To evaluate the relationship between the degree of RLS shunt and unexplained dizziness, we divided the positive PFO into mild shunts (level I), moderate shunts (level II), and massive shunts (level III and IV) and performed multivariate logistic regression again. Finally, compared with a mild shunt, a moderate shunt was not statistically significant, while a massive shunt was statistically significant (OR=8.76; 95% CI 4.04–19.03). The detailed analysis results are shown in Table 4.
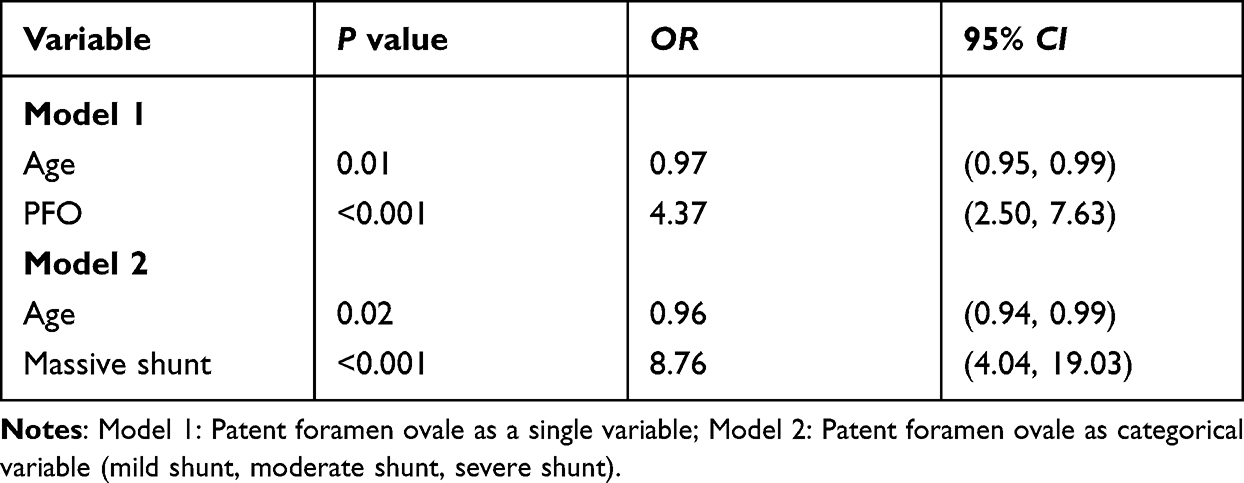 |
Table 4 The Significant Factors in Stepwise Multiple Regression Model |
Discussion
Dizziness is usually combined with the clinical manifestations of impaired vision and somatosensory and proprioceptive organs,22 and it is affected by many factors.16 Because of the complexity and variability of symptoms, unexplained dizziness require further exploration. To the best of our knowledge, we are the first to research the relationship between unexplained dizziness and PFO. The incidence of PFO and the degree of the RLS shunt in the “unexplained” group were significantly higher than those in the “explained” group. There was no significant difference in other factors, such as lifestyle or vascular factors, so we basically believe that PFO is a risk factor for unexplained dizziness.
Our research found that PFO and age are associated with the incidence of unexplained dizziness. PFO showed a strong positive correlation. Generally, the incidence of PFO in adults is approximately 25%,2 which is basically the same as the incidence obtained in the “explained” group. In our sample, PFO-positive patients in the “explained” group were primarily diagnosed with vestibular migraine (23.5%). Studies such as the MIST-trial have confirmed the correlation,23 followed by BPPV (16.7%), which is the most common cause of dizziness. The incidence of PFO in the “unexplained” dizziness group was significantly higher than that in the other group, and the number of shunts on the RLS scale was also more significant. The classification of latent type and inherent type seems to have no meaning. Although the prevalence of PFO in the “unexplained” group might be higher than actual rate because of the age limitation in inclusion criteria, PFO does act as a potential risk factor in dizziness and massively shunt PFO showed more pronounced risk factors.
Migraine and dizziness can originate from the same pathogenesis.24 Animal models have confirmed that serotonin receptors (1 B) and serotonin receptors (1 D) are simultaneously expressed in the peripheral vestibular system and the trigeminal nervous system.25 Regarding dizziness in patients with PFO, microemboli and vasoactive substances bypass the pulmonary circulation through the abnormal channel and directly enter the brain, acting on the vestibular system and causing dizziness. Alternatively, dizziness is related to local vestibular cortex suppression caused by a microbubble embolism that does not cause cerebrovascular embolism. This scenario is a possible mechanism by which PFO causes dizziness or headaches. In addition, animal studies have found that serotonin receptors (1 F) and calcitonin-producing peptide (CGRP) are centrally expressed in the vestibular nucleus.25 Such substances in the blood enter the brain directly without being filtered by the pulmonary circulation, and act on the vestibular nucleus area to cause dizziness.26 Of course, the specific mechanism has not been elucidated, and more basic research is needed to confirm this hypothesis in the future.
It is worth noting that age is negatively correlated with unexplained dizziness. The mean and median age in the unexplained group were relatively young, indicating that younger individuals could have a high risk of unexplained dizziness. Younger people have a relatively higher incidence of PFO, strengthening the association between PFO and unexplained dizziness. The vascular risk factors for the two groups were not statistically significant. From another point of view, unexplained dizziness might not be considered for vascular causes.27
It has been reported that dizziness of unknown cause is related to the degree of white matter lesions. However, no correlations were shown in this study. The difference in results could be explained by the characteristics of the included population, younger people have better vascular condition. The incidence of white matter lesions is positively correlated with age. The prevalence rate in the 75-year-old population is 10%, and the prevalence rate is as high as 85% in the 90-year-old population.28 In this experiment, patients older than 75 years of age were excluded. Most of the magnetic resonance images showed mild white matter lesions, with a grade of 0–1 (Fazekas scale). Perhaps the elderly individuals with unexplained dizziness can be diagnosed with “cerebral microvascular disease dizziness”.29 Clearly, our study cannot be explained according to this view.
As a result of this study, we believe that patients with unexplained dizziness should routinely undergo cTCD and screening for RLS, especially among young people. A better understanding of the factors influencing dizziness can provide clinicians with clues to the management and treatment of dizziness. The advantages of our study are clear, with a large prospective study looking for factors that contribute to unexplained dizziness, excluding confounding factors, a generally well-defined diagnosis, and well-collected information. However, it is undeniable that the study has certain limitations: 1) we cannot be sure that we included all risk factors for unexplained dizziness, and there might be some factors of which clinicians are not aware; 2) we only graded the RLS but did not grade the severity of the dizziness symptoms. It is unknown whether a higher RLS level will lead to more severe unexplained dizziness symptoms.
In summary, our study found that PFO was an independent risk factor for unexplained dizziness. In subsequent clinical work, when a series of examinations did not find a clear cause of dizziness, we should consider whether it is related to PFO and confirm it through cTCD. Future studies will address the limitations of this study. Increasing the sample size and extending the follow-up time, patients should be scored for the degree of dizziness and summarize the clinical symptoms quantitatively.
PFO closure has demonstrated its effect in migraine patients with PFO,30–33 and a small sample study also demonstrated that it could significantly improve headache and dizziness in vestibular migraine with PFO.30–34 Although current guidelines do not include unexplained dizziness as a surgical indication for PFO, we found many patients with unexplained dizziness and only the presence of PFO, and long-term drug treatment did not work, with the patients suffering from dizziness for a long time. Therefore, in the next step, we plan to recruit volunteers with unexplained dizziness accompanied by PFO to undergo PFO surgical closure, and to evaluate the dizziness symptoms before and after the operation, in the hope that the dizziness symptoms can be relieved or disappear after the operation.
Conclusions
There was a high prevalence of PFO and a greater RLS level in unexplained dizziness. PFO and age were independent risk factors for unexplained dizziness, but more research is needed to confirm these findings in the future. However, in patients with unexplained dizziness, especially among young people, we should pay attention to the presence of PFO. Conventional treatment may not relieve symptoms and only increase financial burden. We also look forward to recruiting patients with unexplained dizziness and PFO for surgical treatment to evaluate the efficacy.
Statement of Ethics
The study protocol complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University. All patients recruited the study voluntarily and signed an informed consent form. The procedures obey institutional guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Science and Technology Program of the Jiangxi Provincial Health Commission (202110056).
Disclosure
The authors have no conflict of interests to declare.
References
1. Homma S, Messé SR, Rundek T, et al. Patent foramen ovale. Nat Rev Dis Primers. 2016;2:15086. doi:10.1038/nrdp.2015.86
2. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc. 1984;59(1):17–20. doi:10.1016/S0025-6196(12)60336-X
3. Whitman GT. Dizziness. Am J Med. 2018;131(12):1431–1437. doi:10.1016/j.amjmed.2018.05.014
4. Neuhauser HK. The epidemiology of dizziness and vertigo. Handb Clin Neurol. 2016;137:67–82. DOI: 10.1016/B978-0-444-63437-5.00005-4
5. Alyono JC. Vertigo and dizziness: understanding and managing fall risk. Otolaryngol Clin North Am. 2018;51(4):725–740. doi:10.1016/j.otc.2018.03.003
6. Wang X, Strobl R, Holle R, Seidl H, Peters A, Grill E. Vertigo and dizziness cause considerable more health care resource use and costs: results from the KORA FF4 study. J Neurol. 2019;266(9):2120–2128. doi:10.1007/s00415-019-09386-x
7. Saber Tehrani AS, Coughlan D, Hsieh YH, et al. Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med. 2013;20(7):689–696. doi:10.1111/acem.12168
8. Chinese Medical Association. Chinese medical journals publishing house, Chinese society of general practice. guideline for primary care of dizziness/vertigo: practice version (2019). Chin Med J Publ House. 2020;19(3):201–216.
9. Van Leeuwen RB, van der Zaag-Loonen HJ. Unexplained dizziness does not resolve in time. Acta Neurol Belg. 2012;112(4):357–360. doi:10.1007/s13760-012-0082-5
10. Lee PH, Song JK, Kim JS, et al. Cryptogenic stroke and high-risk patent foramen ovale: the DEFENSE-PFO trial. J Am Coll Cardiol. 2018;71(20):2335–2342. doi:10.1016/j.jacc.2018.02.046
11. Rayhill M, Burch R. PFO and migraine: is there a role for closure? Curr Neurol Neurosci Rep. 2017;17(3):20. doi:10.1007/s11910-017-0730-5
12. Honěk J, Šrámek M, Honěk T, et al. Patent foramen ovale closure is effective in divers: long-term results from the DIVE-PFO registry. J Am Coll Cardiol. 2020;76(9):1149–1150. doi:10.1016/j.jacc.2020.06.072
13. Cao L. Characteristics and analysis of right-to-left shunt-related dizziness in patients without hypoxemia. J Int Med Res. 2019;47(7):2921–2928. doi:10.1177/0300060519850940
14. Stam H, van Vugt VA, Twisk JWR, et al. The prevalence and persistence of dizziness in older European home care recipients: a prospective cohort study. J Am Med Dir Assoc. 2020;21(3):338–343.e331. doi:10.1016/j.jamda.2019.09.008
15. Stone J, Carson A, Duncan R, et al. Symptoms ‘unexplained by organic disease’ in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain. 2009;132(Pt 10):2878–2888. doi:10.1093/brain/awp220
16. Chang J, Hwang SY, Park SK, et al. Prevalence of dizziness and associated factors in South Korea: a cross-sectional survey from 2010 to 2012. J Epidemiol. 2018;28(4):176–184. doi:10.2188/jea.JE20160113
17. Yang X, Wang H, Wei Y, Zhai N, Liu B, Li X. Diagnosis of patent foramen ovale: the combination of contrast transcranial Doppler, contrast transthoracic echocardiography, and contrast transesophageal echocardiography. Biomed Res Int. 2020;2020:8701759. doi:10.1155/2020/8701759
18. Jauss M, Zanette E. Detection of right-to-left shunt with ultrasound contrast agent and transcranial Doppler sonography. Cerebrovasc Dis. 2000;10(6):490–496. doi:10.1159/000016119
19. Gilbert GJ, Anzola GP, Onorato E, Morandi E, Casilli F. Different degrees of right-to-left shunting predict migraine and stroke: data from 420 patients. Neurology. 2006;67(5):919–920. doi:10.1212/01.wnl.0000239682.19745.e7
20. Wessler BS, Kent DM, Thaler DE, Ruthazer R, Lutz JS, Serena J. The RoPE score and right-to-left shunt severity by transcranial Doppler in the CODICIA study. Cerebrovasc Dis. 2015;40(1–2):52–58. doi:10.1159/000430998
21. Tobis JM, Abudayyeh I. Platypnea-orthodeoxia syndrome: an overlooked cause of hypoxemia. JACC Cardiovasc Interv. 2016;9(18):1939–1940. doi:10.1016/j.jcin.2016.08.0029
22. Lopez C. The vestibular system: balancing more than just the body. Curr Opin Neurol. 2016;29(1):74–83. doi:10.1097/WCO.0000000000000286
23. Dowson A, Mullen MJ, Peatfield R, et al. Migraine intervention with STARFlex Technology (MIST) trial: a prospective, multicenter, double-blind, sham-controlled trial to evaluate the effectiveness of patent foramen ovale closure with STARFlex septal repair implant to resolve refractory migraine headache. Circulation. 2008;117(11):1397–1404. doi:10.1161/CIRCULATIONAHA.107.727271
24. Eggers SD, Staab JP, Neff BA, Goulson AM, Carlson ML, Shepard NT. Investigation of the coherence of definite and probable vestibular migraine as distinct clinical entities. Otol Neurotol. 2011;32(7):1144–1151. doi:10.1097/MAO.0b013e31822a1c67
25. Ahn SK, Khalmuratova R, Jeon SY, et al. Colocalization of 5-HT1F receptor and calcitonin gene-related peptide in rat vestibular nuclei. Neurosci Lett. 2009;465(2):151–156. doi:10.1016/j.neulet.2009.09.008
26. Wilmshurst P, Nightingale S. Relationship between migraine and cardiac and pulmonary right-to-left shunts. Clin Sci. 2001;100(2):215–220. doi:10.1042/CS20000231
27. Nozari A, Dilekoz E, Sukhotinsky I, et al. Microemboli may link spreading depression, migraine aura, and patent foramen ovale. Ann Neurol. 2010;67(2):221–229. doi:10.1002/ana.21871
28. Wardlaw JM, Smith C, Dichgans M. Mechanisms of sporadic cerebral small vessel disease: insights from neuroimaging. Lancet Neurol. 2013;12(5):483–497. doi:10.1016/S1474-4422(13)70060-7
29. Kaski D, Rust HM, Ibitoye R, Arshad Q, Allum JHJ, Bronstein AM. Theoretical framework for “unexplained” dizziness in the elderly: the role of small vessel disease. Prog Brain Res. 2019;248:225–240.
30. Liu K, Wang BZ, Hao Y, Song S, Pan M. The correlation between migraine and patent foramen ovale. Front Neurol. 2020;11:543485. doi:10.3389/fneur.2020.543485
31. Wang SB, Liu KD, Yang Y, et al. Prevalence and extent of right-to-left shunt on contrast-enhanced transcranial Doppler in Chinese patients with migraine in a multicentre case-control study. Cephalalgia. 2018;38(4):690–696. doi:10.1177/0333102417708203
32. Mattle HP, Evers S, Hildick-Smith D, et al. Percutaneous closure of patent foramen ovale in migraine with aura, a randomized controlled trial. Eur Heart J. 2016;37(26):2029–2036. doi:10.1093/eurheartj/ehw027
33. Tobis JM, Charles A, Silberstein SD, et al. Percutaneous closure of patent foramen ovale in patients with migraine: the PREMIUM trial. J Am Coll Cardiol. 2017;70(22):2766–2774. doi:10.1016/j.jacc.2017.09.1105
34. Jing W, Libo Z, Chao L, et al. Curative effect observation of patent foramen ovale interventional closure in the treatment of vestibular migraine. Beijing Med. 2021. 2021:6–9.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.