Back to Journals » Psychology Research and Behavior Management » Volume 16
The Relationship Between Mindfulness, Fatigue, and Perceived Symptoms Among Frontline Nurses Who Performed Nucleic Acid Sample Collection During the COVID-19 in China: A Cross-Sectional Study
Authors Chen JQ, Zhang XQ ![]() , Shen JH
, Shen JH ![]() , Guo YF
, Guo YF ![]() , Lei GF, Tong L, Wang H, Li DH
, Lei GF, Tong L, Wang H, Li DH
Received 16 December 2022
Accepted for publication 5 April 2023
Published 13 April 2023 Volume 2023:16 Pages 1165—1180
DOI https://doi.org/10.2147/PRBM.S401764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Jian-qin Chen,1,* Xue-qing Zhang,1,* Jin-hua Shen,1 Ya-fen Guo,1 Guang-feng Lei,1 Li Tong,1 Hui Wang,1 De-hui Li2
1Department of Nursing, The First People’s Hospital of Changde City, Changde, Hunan Province, People’s Republic of China; 2Department of Infectious Diseases, The First People’s Hospital of Changde City, Changde, Hunan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: De-hui Li, Department of Infectious Diseases, The First People’s Hospital of Changde City, 818 Ren min Road, Changde, Hunan Province, People’s Republic of China, Email [email protected]
Objective: Given the immense stress faced by medical staff during the COVID-19 pandemic, this study aimed to evaluate the relationship between mindful attention awareness, fatigue, and perceived symptoms among frontline nurses who performed nucleic acid sample collection during the COVID-19 pandemic, to reduce their fatigue and help them cope with perceived uncomfortable symptoms.
Methods: A convenience sampling method was used to survey nurses who travelled to Hainan for nucleic acid sampling in August 2022 using an online (WeChat) questionnaire. A total of 514 frontline nurses who performed nucleic acid tests completed the questionnaire. The questionnaire covered basic demographic information, Mindful Attention Awareness Scale (MAAS) ratings, and Fatigue Severity Scale (FSS) ratings. Spearman correlation analysis was used to separate the relationship between MASS and FSS, and univariate and multivariate factor analyses were used to explore the relevant influences contributing to the occurrence of fatigue.
Results: A total of 514 individuals completed the survey,93.97% (n=483) were female, mean age was 31.15 ± 5.7, MASS score was 69.01 ± 13.53, and 296 (57.59%) nurses experienced symptoms of fatigue during the auxiliary period. Spearman correlation analysis showed that FSS was associated with MASS. Multifactorial analysis showed that sex, age, marital status, fertility status, years of work, adaptation to dietary habits, hidrorrhea, and MAAS scores affected the presence of fatigue symptoms among the medical staff in Hainan (P< 0.05).
Conclusion: The psychological status of frontline nurses undergoing nucleic acid testing during the pandemic was poor, and the appearance of fatigue symptoms could be effectively reduced by increasing levels of positive thinking among medical staff to help them cope with public health emergencies.
Keywords: COVID-19, nucleic acid testing, nurses, mindfulness, fatigue, perceived symptoms
Introduction
Since December 2019, the coronavirus disease (COVID-19) pandemic has brought significant harm and challenges to over 200 countries worldwide.1 Evidence regarding the global COVID-19 pandemic has shown that many COVID-19 infections are asymptomatic. This means that they test positive based on the detection of nucleic acid in samples but have no typical clinical symptoms or signs and no apparent abnormalities in images, including lung computed tomography. Most asymptomatic infected people do not seek medical assistance due to the lack of obvious clinical signs and poor prevention awareness, and this increases the rapid spread of COVID-19.2 Because of the differences in sociocultural, political, and economic contexts between countries, there has been no consensus about the best public health strategy for managing COVID-19. The Chinese government has adopted a dynamic zero-COVID policy to combat the pandemic, in which restrictive measures are initiated and maintained until there are no documented COVID-19 cases in a particular geographic location.3
The zero-COVID-19 policy is effective in reducing health damage in the mid-and long-term, and nucleic acid testing has played a crucial role in controlling COVID-19, especially in screening asymptomatic infections. In addition, it has worked to control sources of infection and cut off transmission channels.4 Frequent and/or regular population-based broad nucleic acid testing not only largely aggravates the public health burden (eg, cost, volunteers, and resources) but also increases the numbers of medical specialists and laboratories. The National Health Commission of the PRC has transferred many medical personnel, including doctors, nurses, and laboratory technicians, to support nucleic acid testing in several cities and regions (eg, Hong Kong, Shenzhen, Jilin, Shanghai, Hainan, and Xizang) of China in 2022. At the same time, the COVID-19 pandemic has affected the mental health of medical personnel on the frontline of this crisis. A systematic review reported that among Western frontline healthcare professionals, moderate and high levels of stress, anxiety, depression, sleep disturbance, burnout, and even more frequent. Intense symptoms among women and nurses have been discovered during the COVID-19 pandemic.5 A cross-sectional study conducted in Nanjing, China, showed that out-ward healthcare workers were more likely to experience functional gastrointestinal disorder-related symptoms compared to their inward counterparts who were within hospital wards treating COVID-19 patients.6 Another Chinese cross-sectional study showed that during the pandemic, sleep disorders and depression-anxiety-stress levels were high because the frontline nurses performing nucleic acid testing were directly exposed to COVID-19 and the possibility of infection.7 This might partly be because out-ward healthcare workers at uncertain risk of COVID-19 tended to experience related mental problems and symptoms compared to their inward counterparts whose risk of contracting COVID-19 was more definite.8 The COVID-19 pandemic has further exacerbated the prevalence of fatigue in nurses. Profession-related fatigue harms the work efficiency, safety, and health of nurses and even produces symptoms such as anxiety, depression, headache, dizziness, compulsion, and insomnia. This may also increase the risk of medication errors among nurses. These, in turn, are compounded by poorly designed working spaces and environments.9 It is necessary for nurse leaders to implement crisis management based on nurses’ psychological characteristics to promote their health during the critical period of the COVID-19 pandemic.10
In the past two decades, mindfulness has received extensive public, as well as scientific, attention.11 Mindfulness deals with what occurs both within the individual and the environment and which may bring about greater autonomy and self-regulation. Mindfulness may also lead to an increased awareness of internal conditions, such as feelings, needs, and external stimuli, which can act as sources of pressure.12 The Mindful Attention Awareness Scale (MAAS) is a popular self-report tool. It consists of 15 items that describe general tendencies to be attentive to and aware of present-moment experiences in daily life and mindless states that can be experienced in common or specific situations.13
Using three different samples of college students, hospital nurses, and full-time community workers, Reina and Kudesia found that participants’ self-regulatory abilities and metacognitive beliefs were positively associated with positive thoughts. In contrast, mental fatigue and situational stressors were negatively associated with positive thoughts.14 The MAAS has been translated and adapted into different language versions15 (eg, French, Spanish, Turkish, and Italian). The MAAS is the most common tool used in research studies, such as those related to stress, depression, chronic pain, bulimia, and cancer, to assess mindfulness.16 The MAAS was translated into Chinese in 2012.17 It was then used in a study of undergraduates18 to assess the relationship between dispositional mindfulness and suicide risk. Previous studies have shown that the Chinese version of the MAAS is both valid and reliable for use among Chinese populations.17,19 The COVID-19 pandemic is a global health crisis with psychological consequences for healthcare workers, including frontline nurses, who collect nucleic acid samples because they are the main barrier in the fight against public health emergencies. Government and medical institutions must consider professional and psychological factors in ameliorating burnout and increasing nurses’ safety.20 Based on previous studies, we assumed that mindful attention awareness is the factor related to fatigue and perceived symptoms among frontline nurses who performed nucleic acid sample collection during the COVID-19 pandemic.
Therefore, in this study, we aimed to evaluate the relationship between mindful attention awareness, fatigue, and perceived symptoms among frontline nurses who performed nucleic acid sample collection during the COVID-19 pandemic, to reduce their fatigue and help them cope with perceived uncomfortable symptoms. This study provides a basis for further intervention and crisis management for hospital nursing administrators during the COVID-19 pandemic.
Materials and Methods
Research Design and Research Participants
This cross-sectional study used a convenience sampling method through an online questionnaire (WeChat). The sample size was calculated by using a single population proportion formula  ,21 where Zα/2 is the confidence level (at α = 0.05, Zα/2 = 1.96), P = expected proportion of the outcome of fatigue (the incidence of fatigue in the preliminary survey was 60%), and
,21 where Zα/2 is the confidence level (at α = 0.05, Zα/2 = 1.96), P = expected proportion of the outcome of fatigue (the incidence of fatigue in the preliminary survey was 60%), and  . The calculated necessary minimum sample size
. The calculated necessary minimum sample size  was 369. Considering the addition of a 20% contingency for non-response, the sample size was estimated to be 433 participants finally, the study sample was 514 research objects.
was 369. Considering the addition of a 20% contingency for non-response, the sample size was estimated to be 433 participants finally, the study sample was 514 research objects.
In this study, online questionnaires were sent to leaders in contact with nucleic acid collection teams from hospitals to assist Hainan. The questionnaires were administered by the leader sent to the nurses from Hunan province to assist Hainan with nucleic acid sampling in August 2022. A total of 520 medical staff from the Hunan assistance team answered the questionnaire; three individuals were excluded because they were physicians, and three were excluded because they were laboratory technicians. Finally, 514 nurses completed the survey.
The inclusion criteria were as follows: transferred nurses from Hunan province who went to Hainan for nucleic acid sampling during the pandemic. These nurses provided informed consent and voluntarily agreed to participate in the study, and they had the ability to fill out the survey truthfully. The exclusion criteria were: time to complete the questionnaire was <3 min, a returned questionnaire with common-sense items that were incorrect, questionnaires returned with the same answer for 85% of the items, and questionnaires returned from local nurses in Hainan and other provinces. This study was approved by the Ethics Committee of the First People’s Hospital of Changde, and all the respondents signed an informed consent form before the online questionnaire was administered. Questionnaires were sent to the Hainan Nucleic Acid Sampling Team through WeChat.
The Measurement Tools
The measurement tools included basic demographic information, the Mindfulness Attention Awareness Scale (MAAS), and the Fatigue Severity Scale (FSS).
Basic Demographic Information
First, general sociodemographic profiles for the nurses sampling for nucleic acids were completed. These profiles included information about sex, age, education level, marital status, fertility status, working years, professional title, hours of sleep every day, and whether they adapted to certain dietary habits. Second, the nurses’ symptoms during the nucleic acid test were investigated. The possibilities included dizziness, chest distress, polypnea, nausea, vomiting, palpitation, hidrorrhea, headache, tinnitus, stuffy nose, faintness, convulsions, and unconsciousness. Each entry had four options, indicating the frequency of symptom occurrence, 0 indicating no symptom occurrence, 1–2 indicating symptom occurrence one or two times, 3–5 indicating symptom occurrence three to five times, and ≥6 indicating symptom occurrence six times or more. Frequencies and percentages were calculated for analysis.
Mindful Attention Awareness Scale (MAAS)
Mindfulness was assessed using the 15-item Mindful Attention Awareness Scale (MAAS).22 Previous studies have shown that the Chinese version of the MAAS is both valid and reliable for Chinese populations.19,23 The internal consistency of Cronbach’s alpha and the confirmatory factor analysis of the Comparative Fit Index for the MAAS were 0.72 and 0.83, respectively.23 The 15 items required the research subjects to identify the frequency with which they experienced feelings, behaviors, or mindful thoughts when they performed the nucleic acid test. Each item’s score ranged from 1 to 6 (from almost never to almost always). Higher scores indicate higher levels of mindfulness. The total scores for all the items ranged from 14 to 90. In this study, Cronbach’sαof the MAASwas0.79, and the confirmatory factor analysis of the Comparative Fit Index CFI was 0.74.
Fatigue Severity Scale (FSS)
The Fatigue Severity Scale (FSS) contains nine items, each with seven options, ranging from strongly disagree to strongly agree. Higher scores indicate higher fatigue.24 The Cronbach’s α coefficient of the FSS was 0.75, and the confirmatory factor analysis for the Comparative Fit Index CFI was 0.70. The Chinese version of the FSS has been used and validated in an Asian population.25 Fatigue was defined as an average FSS score ≥4, and a higher score indicated more severe fatigue.26 In this study, the Cronbach’s α coefficient of the FSS was 0.82, and the confirmatory factor analysis of the Comparative Fit Index CFI was 0.73.
Statistical Analysis
Statistical analyses were performed using SPSS 22.0 software and Jamovi 1.8.1. Statistical analysis was performed using SPSS version 22.0, including simple counting, percentages, mean values, standard deviations of sample demographics and symptoms, as well as the descriptive statistics for the MAAS and FSS. Mann–Whitney U-test was used for the MAAS as measurement data with FSS presence of fatigue. The MAAS as enumeration data was treated with the chi-square test and univariate and multivariate analyses to explore factors leading to fatigue. The internal structure was evaluated by Jamovi 1.8.1, using confirmatory factor analysis, and the internal consistency of the scale was evaluated by Cronbach’s α. All analyses were performed using two-sided tests P<0.05.
Results
Demographic Characteristics of the Assistant Nurses Performing the Nucleic Acid Test
This study investigated the fatigue symptoms and psychological status of 514 frontline nurses performing nucleic acid testing during a new coronavirus-associated pneumonia outbreak in Hainan.514 nurses responded to the survey, and they all returned valid questionnaires with a validity rate of 100%. Among the nurses, 58.37% were married, 93.97% were female (n = 483), and 6.03% were male (n= 31), with a mean age of 31.15 ± 5.73 years. More people were in the 31–40-year-old group (47.67%, n = 245) than in any other group. Moreover, 78.41% had a bachelor’s degree or above, 42.80% of the nurses had not given birth, and 49.23% had worked for more than ten years. Two hundred eighteen (42.41%) had an intermediate title, 99.61% of the nurses slept for 5–8 hours during nucleic acid collection, and 47.86% did not adapt to a local diet. The basic sociodemographic characteristics of nucleic acid collection nurses in Hainan are shown in Table 1.
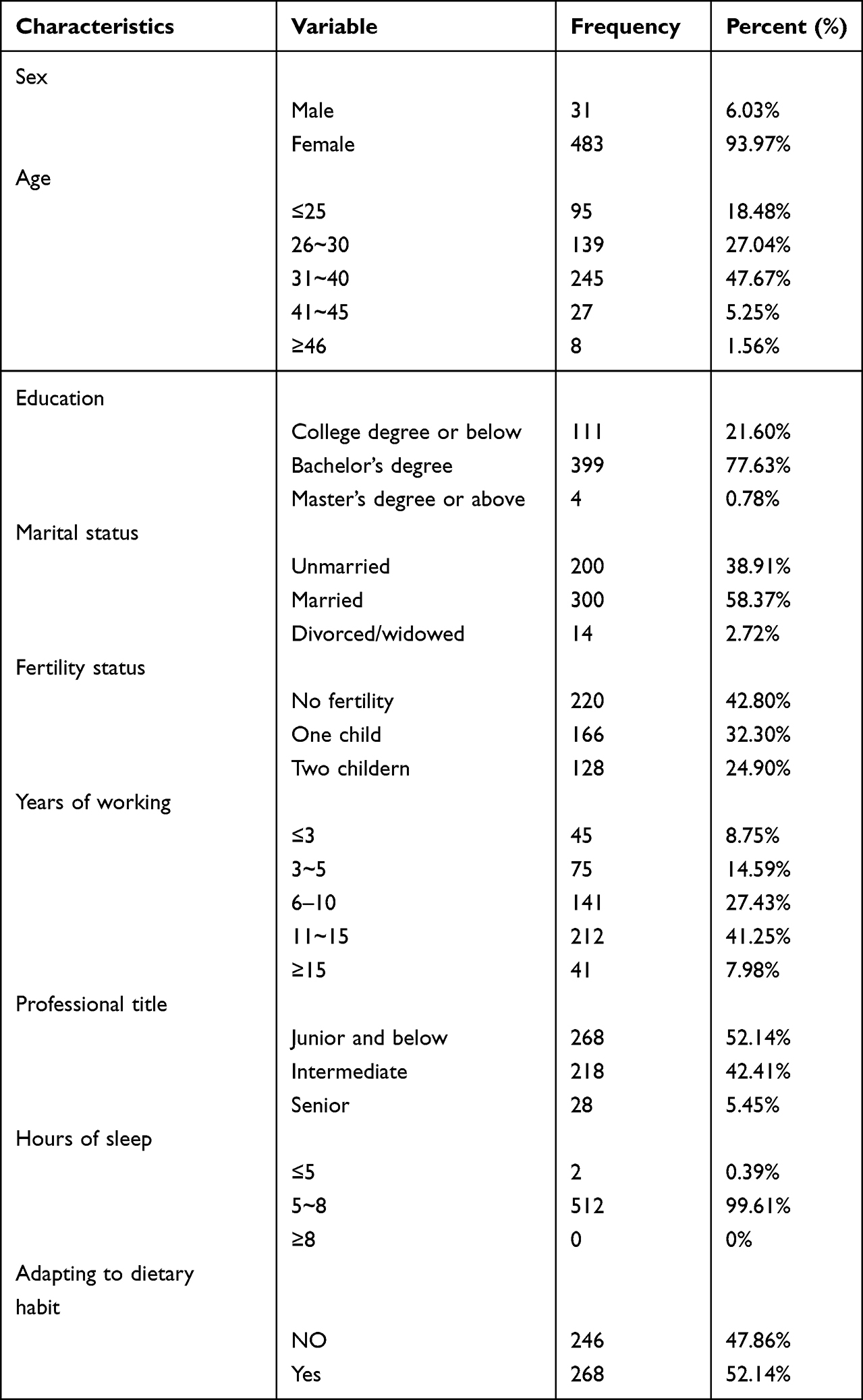 |
Table 1 Demographic of Nurse Performing Nucleic Acid Test (N = 514) |
The Symptoms of the Nurses Performing the Nucleic Acid Test
We assessed the symptoms of heat stroke in nurses who had undergone nucleic acid testing. Specifically, 45.72% did not experience dizziness. Over 40% experienced chest tightness, shortness of breath, nausea, and panic. Further, 73.65% experienced profuse sweating, and a minority experienced ringing in the ears, stuffiness, fainting, twitching of the limbs, and loss of consciousness, as shown in Table 2.
 |
Table 2 The Symptoms in Nurse Performing Nucleic Acid Test (N = 514) |
MAAS Scores of the Nurses Performing the Nucleic Acid Test
The participants scored 69.01±13.53 in positive thinking. Positive thinking was categorized into three levels: poor, moderate, and good. The study results showed that 62.06% of the medical staff had an above-average level of positive thinking, 35.99% had an average level, and 2.05% had a poor level of positive thinking (detailed results are presented in Table 3 and Table 4).
 |
Table 3 MAAS Scores in Nurse Performing Nucleic Acid Test (N = 514) |
 |
Table 4 MAAS Level Classification in Nurse Performing Nucleic Acid Test (N = 514) |
FSS Scores and the Presence of Fatigue Among Nurses Performing the Nucleic Acid Test
Participants had a fatigue score of (36.27 ± 11.17). The study results showed that 57.59% of the medical staff experienced fatigue, and 42.41% did not (detailed results are shown in Table 5 and Table 6).
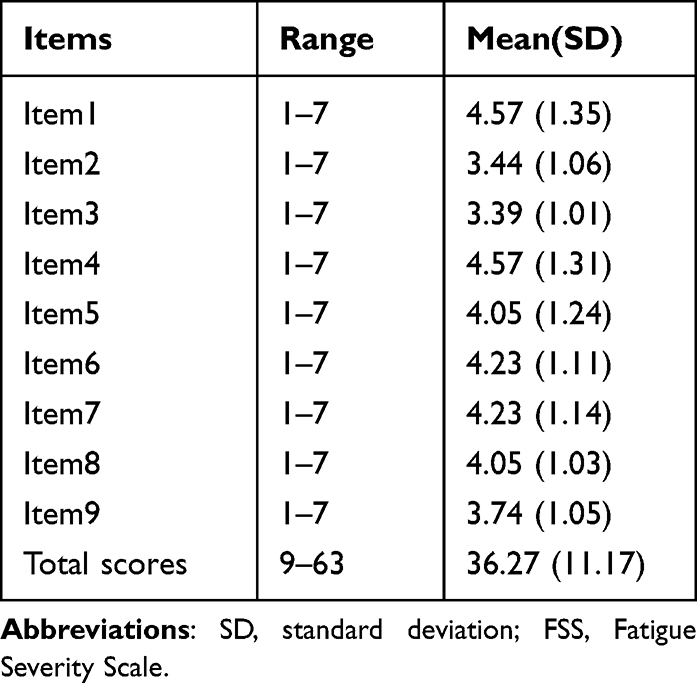 |
Table 5 FSS Scores and Presence of Fatigue in Nurse Performing Nucleic Acid Test (N = 514) |
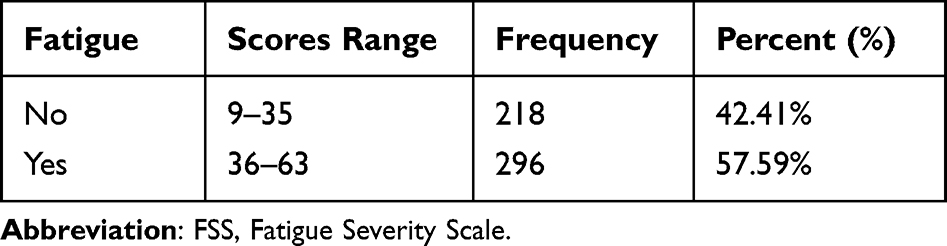 |
Table 6 FSS Presence of Fatigue in Nurse Performing Nucleic Acid Test (N = 514) |
The MAAS Items with FSS Presence of Fatigue Among Nurses Performing the Nucleic Acid Test
The results of this study showed that nurses who experienced fatigue during nucleic acid collection had lower positive thinking scores than those who did not experience fatigue, and the difference between the two was statistically significant (detailed results are shown in Table 7).
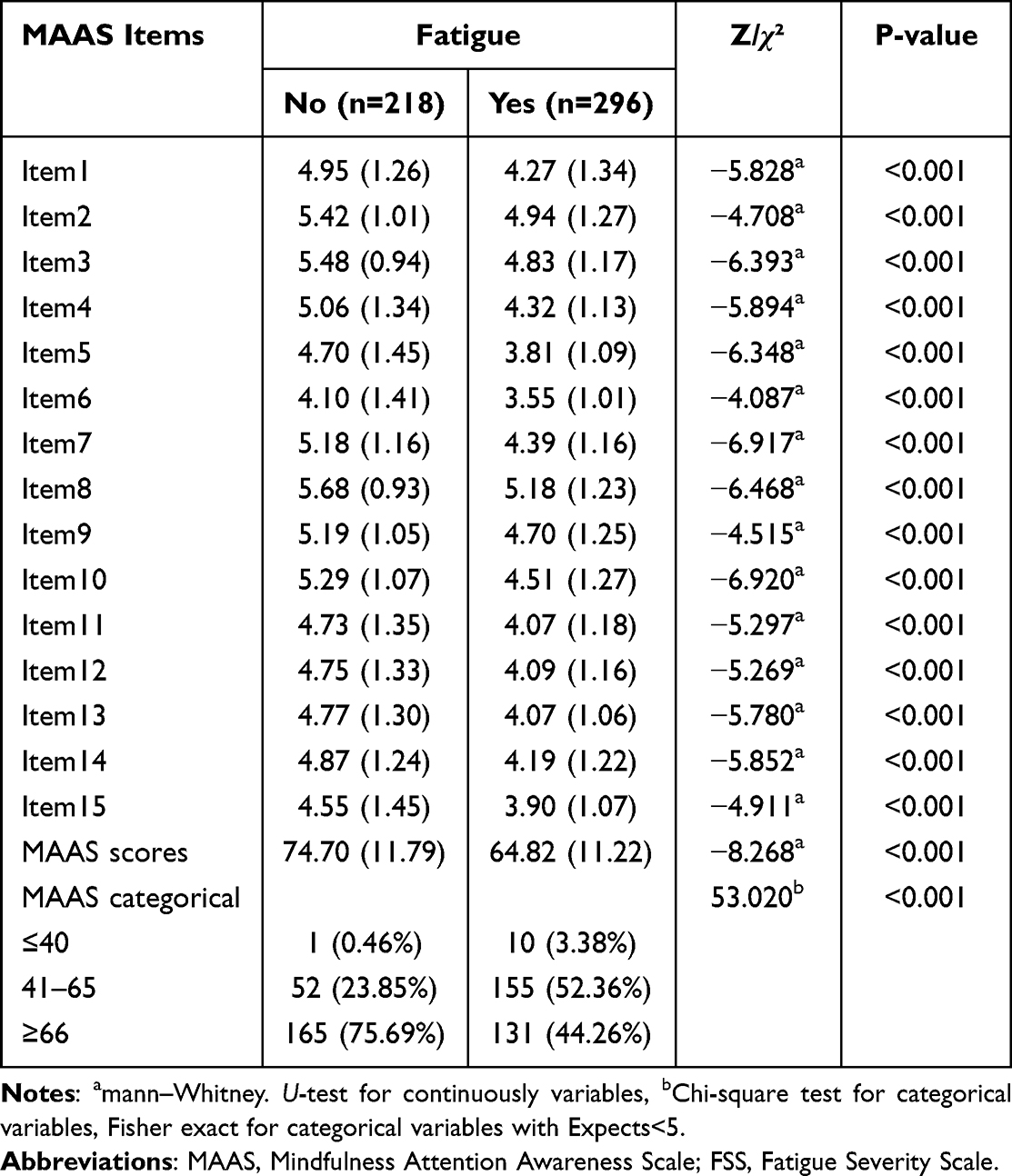 |
Table 7 The MAAS Items with FSS Presence of Fatigue in Nurse Performing Nucleic Acid Test (N = 514) |
The Univariate and Multivariate Analysis of Factors for FSS Presence of Fatigue Among Nurses Performing the Nucleic Acid Test
The results of this study showed that sex, age, marital status, fertility status, years of working, adapting to dietary habits, hidrorrhea, and MAAS scores were independent influences on nurses’ fatigue during nucleic acid collection (detailed results are shown in Table 8).
 |
Table 8 TheUnivariate and Multivariate Analysis on Factors for FSS Presence of Fatigue Among Nurse Performing Nucleic Acid Test (N = 514) |
Discussion
The Hainan Province is located in southern China at the edge of the tropics. A tropical province with a tropical maritime monsoon climate is a world-renowned tourist destination. In August 2022, Hainan Province was severely affected by COVID-19, with a cumulative total of 1604 confirmed cases by August 9, while Sanya had a cumulative total of 1164 confirmed cases. More than 80,000 tourists were stranded in Sanya, Hainan Province, and 5000 medical personnel from across the country began to rush to help Hainan. According to the China Meteorological Administration, a heatwave in China lasted for more than two months in summer, which was the longest record since 1960. The temperatures in Hainan are particularly high in August. Going out into protective clothing to collect nucleic acids in scorching heat was the biggest challenge for nurses. A meta-analysis27 of 93 cross-sectional studies with 93,112 nurses reported pooled prevalence estimates of anxiety, stress, depression, and sleep disorders among nurses during the COVID-19 outbreak. The reason for this is that nurses are closest to COVID-19 patients and are at high risk of infection from patients or asymptomatic cases in their work. The stress they experience may lead to many problems, such as sleep disturbance, stress, anxiety, and depression.28 Therefore, performing nucleic acid testing in such a harsh environment in Hainan can easily pose a great psycho-physiological threat to nurses.
The current study showed that 93.97% of the nurses who participated in the survey were female, and 6.03% were male. In China, the nursing profession is still predominantly female, and the proportion of men involved remains low, with data showing that, by 2019, 4.09 million people were registered as nurses in China, but only 2.3% were male.29 Although previous studies have shown that gender does not affect depressive symptoms and sleep quality among the public during the COVID-19 pandemic,30 the results of this study showed that men are at higher risk of experiencing fatigue. This may be related to the small sample size of the present study.
The majority of nurses performing nucleic acid testing assistance had a bachelor’s level education (77.63%), 58.37% were married, had the highest number of intermediate-level titles, and 99.61% slept between 5–8 hours during nucleic acid collection. All nurses took the initiative to fight COVID-19 because of the strong responsibility and strong sense of mission and dedication Chinese healthcare providers feel to overcome this pandemic.31 Existing studies have shown that the current status of psychological problems among healthcare workers during the COVID-19 is higher than in previous pandemics.32 In this study, the nurses’ FSS score was 36.27±11.17, and we found fatigue among the 296 nurses performing nucleic acid testing. This is probably due to the fact when the nurses were assisting Hainan with nucleic acid testing, they were confronted with extreme infectivity, especially in an unfamiliar and hot environment in which they could not relax at any time. Some of them were worried about not being able to adapt to sleeping, eating, and other living habits (49.23%). The results of our previous study showed that the quality of sleep and psychological status of frontline nurses performing nucleic acid testing during the new coronavirus-related pneumonia epidemic was poor, and they had severe sleep disturbances during the pandemic.7 In a cross-sectional study of 95 medical students in Saudi Arabia, stress, anxiety, and depression were strongly linked with poor sleep.33 It was also reported that inadequate sleep duration and, consequently, fatigue might affect mental health to such a degree that recurrent suicidal thoughts, and even suicidal attempts, may occur more frequently.34 This suggests it is particularly important to pay close attention to the psychological state of medical staff during the fight against the pandemic.
The main mental health burden on the public was higher during the COVID-19 outbreak, while healthcare workers were at higher risk.30 Stress among the public may come from lack of knowledge about the disease, receiving unconfirmed false news, etc., whereas the main mental health burden among health care workers comes from fear of spreading the virus to family members, close people, or patients.35 Some studies36–38 have shown that psychological stress during COVID-19 is associated with female gender, fatigue during work and (dis)availability of coping tools, such as mindfulness management. Coherence and a sense of work engagement have also been suggested as protective factors against the psychological stress associated with exposure to people infected with Neocoronavirus.39,40 The present study explored the psychological profile of nucleic acid sampling nurses under the influence of a Neo coronavirus pandemic and a hostile environment. During the collection of nucleic acids, nurses must wear protective clothing, goggles, and three-layer gloves according to strict isolation requirements. This not only affects their senses of sight, hearing, and touch but also poses difficulties and dangers in the completion of various nursing treatments and operations. At the same time, tight protection in a high-temperature environment puts nurses in a more severe state of hypoxia, which, coupled with a high level of psychological stress over a long period of time, causes them to experience general fatigue and weakness and reduced muscle strength, accompanied by symptoms of soreness and physical fatigue, such as incomplete and uncoordinated performance of various movements. The pathophysiology of fatigue is not well understood. However, fear and anxiety can increase body stress. The inflammatory response to anxiety and fear-related fatigue has consistently been found to affect anxiety-related brain regions.41
It has also been found in previous studies that while protective gear reduces the risk of infection for medical personnel, a variety of physical health problems can occur, including skin, respiratory, musculoskeletal, neurological, urinary, and circulatory problems, with skin problems being the most common.42 These findings are consistent with those of previous studies on the spread of severe acute respiratory syndrome (SARS).43 Long-term use of the facial protective gear is associated with a high rate of adverse skin reactions. In addition, according to systematic evaluations,44 the use of personal facial protective equipment may lead to allergies, followed by an acneiform rash and contact urticaria, especially during increased and prolonged use. In hot conditions, PPE limits evaporation and heat exchange with the environment,45 and health workers are more likely to experience various discomforts in the extreme heat of Hainan. Similar to the results of previous studies, physical problems caused by wearing PPE by health workers in Singapore and India can lead to impaired physical function, difficulty in work, impaired communication with patients and colleagues, and a negative impact on health workers’ productivity.46,47
In a study investigating the environmental impact on the health and safety of medical personnel during a new crown epidemic, it was shown that approximately 65% of respondents reported that one or more cognitive tasks were impaired when wearing PPE.46 This impairment in cognition may not only affect performance but also compromise the health and safety of HCWs and patients. The prevalence of occupational heat stress has been strongly associated with workplace accident rates, with the majority of accidents reported in certain workplaces found to occur in wet-bulb globe temperatures >25℃.48 But the temperature of Hainan is well above 25℃. In this study, 73.65% of the nurses experienced heavy sweating and dizziness during nucleic acid collection, and the hot weather in Hainan seriously affected the safety and work status of the medical staff.
The results of this study showed that being male, older, having one child, adapting to dietary habits, and experiencing hidrorrhea were risk factors for fatigue during nurses’ nucleic acid collection. Being married, having more than ten years of work experience, and having a high MAAS score reduced the risk of fatigue. Similar to previous studies, the risk factors for fatigue after COVID included being female and being older.49 Male nurses generally outperformed female nurses in terms of physical strength; therefore, they showed lower levels of fatigue. However, nurses with more work experience were better able to cope with highly contagious diseases than younger nurses, who were less experienced and less likely to be calm in situations and, therefore, more prone to fatigue. Married nurses, in contrast, had the support of their families to help alleviate the harmful consequences of stress.50
In a study by Kemper et al,51 increasing the MASS score was effective in reducing sleep disturbance and improving psychological resilience among the clinical staff. In this study, 514 nurses had a MASS score of 69.01±13.53 during nucleic acid collection, 62.06% had a good level of MASS, and 35.99% had a moderate level of MASS, while nurses’ level of MASS was closely related to fatigue. The higher the MASS score, the lower the FSS score and the less severe the fatigue symptoms. This finding is consistent with those of previous studies. A good MASS level can effectively regulate participants’ emotions, enhance their emotional control and relaxation, and improve their sense of self-control, which will enable them to reduce their negative emotions and clinical symptoms.52,53 Ghawadra et al reported that mindfulness training could reduce anxiety and depression, alleviate psychological distress, and improve job satisfaction and subjective well-being among nurses.54 This suggests that nursing managers should consider the role and mechanisms of positive psychology and develop targeted interventions to improve nurses’ positive thinking to further reduce negative emotions, such as fatigue, and improve nurses’ sense of professional well-being, thereby ensuring quality and safety of care.55
On December 7, 2022, China’s National Health and Wellness Commission issued measures to further optimize the implementation of prevention and control of the COVID-19 epidemic.56 The ten measures call for the scientific and precise delineation of risk areas, focusing on nucleic acid testing in personnel at high risk of infection in certain areas, not conducting full-scale nucleic acid testing by administrative area, and further narrowing the scope and reducing the frequency of nucleic acid testing. With the adjustment of China’s policy, the large-scale nucleic acid collection is not always possible. Rather, this policy shift will put healthcare institutions and medical staff at greater risk and pressure. By focusing on the level of positive thinking and fatigue of medical staff, this study provides a basis for the need to focus on the physical and mental health of medical staff and reduce the fatigue experienced in regular work aimed at fighting new coronavirus-related pneumonia.
Limitations
This study has several limitations. First, biases existed in the methods used to collect data through online surveys. The use of scales is based on individuals’ perceptions of their own behavior, and there are limitations in the survey distribution method. Some people may have refused to complete the questionnaire; therefore, the potential information may have been lost. In addition, the medical staff supporting Hainan were from all over the country, but most of the questionnaires we received were from foreign-body staff in Hunan Province. Therefore, the results may be biased, and we plan to conduct a multicenter study in the future.
Conclusions
During the COVID-19 pandemic, fatigue was more common among nurses performing nucleic acid testing, especially among assistive nurses. The MASS and FSS scores were negatively correlated, and multiple measures should be taken to improve MASS levels and reduce FSS among nurses.
Data Sharing Statement
The original data presented in the Supplementary Materials and further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
Ethical approval was issued by the Ethics Committee of The First People’s Hospital of Changde City (2023-005-01), and all respondents signed an informed consent form before the study was initiated. The study was conducted in accordance with the regulations and ethics followed in compliance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas. The authors drafted, revised, or critically reviewed the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Changde Science and Technology Bureau for the Emergency Special Project of COVID-19 in Changde City, Hunan Province (2020SK003).
Disclosure
The authors assert they have no competing interests to declare.
References
1. Gao Z, Xu Y, Sun C, et al. A systematic review of asymptomatic infections with COVID-19. J Microbiol Immunol Infect. 2021;54(1):12–16. doi:10.1016/j.jmii.2020.05.001
2. Chen Y, Wang AH, Yi B, et al. 宁波市新型冠状病毒肺炎密切接触者感染流行病学特征分析. [Epidemiological characteristics of infection in COVID-19 close contacts in Ningbo city]. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(5):667–671. Chinese. doi:10.3760/cma.j.cn112338-20200304-00251
3. Bai W, Sha S, Cheung T, Su Z, Jackson T, Xiang YT. Optimizing the dynamic zero-COVID policy in China. Int J Biol Sci. 2022;18(14):5314–5316. doi:10.7150/ijbs.75699
4. Wan Z, Lu R, Zhao Y, Zhang C. Diagnostic strategy of SARS-CoV-2 for containment under China’s zero-COVID-19 policy. J Infect. 2022;85(1):e7–e9. doi:10.1016/j.jinf.2022.04.044
5. Danet Danet A. Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Med Clin. 2021;156(9):449–458. doi:10.1016/j.medcli.2020.11.009
6. Zhang Y, Guan Y, Shen Y, Qiao H, Yuan J, Xu F. The prevalence of functional gastrointestinal disorders related symptoms and the association with working place among healthcare workers who were in the fighting against COVID-19 in regional China. Front Public Health. 2022;10:1048935. doi:10.3389/fpubh.2022.1048935
7. Chen X, Liu P, Lei GF, Tong L, Wang H, Zhang XQ. Sleep quality and the depression-anxiety-stress state of frontline nurses who perform nucleic acid sample collection during COVID-19: a cross-sectional study. Psychol Res Behav Manag. 2021;14:1889–1900. doi:10.2147/PRBM.S338495
8. Levine L, Kay A, Shapiro E. The anxiety of not knowing: diagnosis uncertainty about COVID-19. Curr Psychol. 2022;1–8. doi:10.1007/s12144-022-02783-y
9. Ma M, Adeney M, Long H, He B. The environmental factors associated with fatigue of frontline nurses in the infection disease nursing unit. Front Public Health. 2021;9:774553. doi:10.3389/fpubh.2021.774553
10. Zhang Y, Wei L, Li H, et al. The psychological change process of frontline nurses caring for patients with COVID-19 during its outbreak. Issues Ment Health Nurs. 2020;41(6):525–530. doi:10.1080/01612840.2020.1752865
11. Oberleiter S, Wainig H, Voracek M, Tran US. No effects of a brief mindfulness intervention on controlled motivation and amotivation, but effect moderation through trait mindfulness: a randomized controlled trial. Mindfulness. 2022;13(10):2434–2447. doi:10.1007/s12671-022-01968-7
12. Donald JN, Bradshaw EL, Ryan RM, et al. Mindfulness and its association with varied types of motivation: a systematic review and meta-analysis using self-determination theory. Pers Soc Psychol Bull. 2020;46(7):1121–1138. doi:10.1177/0146167219896136
13. Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. doi:10.1037/0022-3514.84.4.822
14. Reina CS, Kudesia RS. Wherever you go, there you become: how mindfulness arises in everyday situations. Organ Behav Hum Decis Process. 2020;159:78–96. doi:10.1016/j.obhdp.2019.11.008
15. Chiesi F, Donati MA, Panno A, Giacomantonio M, Primi C. What about the different shortened versions of the mindful attention awareness scale? Psychol Rep. 2017;120(5):966–990. doi:10.1177/0033294117711132
16. Nooripour R, Ghanbari N, Hassani-Abharian P, Radwin LE, Hosseinian S, Hasanvandi S. Validation of Persian version of Mindful Attention Awareness Scale (MAAS) in Iranian women with breast cancer. Arch Iran Med. 2022;25(5):300–307. doi:10.34172/aim.2022.49
17. Deng Y-Q, Li S, Tang -Y-Y, Zhu L-H, Ryan R, Brown K. Psychometric properties of the Chinese translation of the mindful attention awareness scale (MAAS). Mindfulness. 2012;3(1):10–14. doi:10.1007/s12671-011-0074-1
18. Fang Y, Zeng B, Chen P, et al. Mindfulness and suicide risk in undergraduates: exploring the mediating effect of alexithymia. Front Psychol. 2019;10:2106. doi:10.3389/fpsyg.2019.02106
19. Huang -C-C, Chen Y, Greene L, Cheung S, Wei Y. Resilience and emotional and behavioral problems of adolescents in China: effects of a short-term and intensive mindfulness and life skills training. Child Youth Serv Rev. 2019;100:291–297. doi:10.1016/j.childyouth.2019.03.015
20. Noh EY, Park YH, Chai YJ, Kim HJ, Kim E. Frontline nurses’ burnout and its associated factors during the COVID-19 pandemic in South Korea. Appl Nurs Res. 2022;67:151622. doi:10.1016/j.apnr.2022.151622
21. Tesfaye Y, Agenagnew L, Anand S, et al. Knowledge of the community regarding mental health problems: a cross-sectional study. BMC Psychol. 2021;9(1):106. doi:10.1186/s40359-021-00607-5
22. Brown KW, West AM, Loverich TM, Biegel GM. Assessing adolescent mindfulness: validation of an adapted mindful attention awareness scale in adolescent normative and psychiatric populations. Psychol Assess. 2011;23(4):1023–1033. doi:10.1037/a0021338
23. Huang C, Yang M, Geng Y, et al. Adverse childhood experiences and mindfulness in Chinese college students during the COVID-19 pandemic. Front Psychiatry. 2021;12:619128. doi:10.3389/fpsyt.2021.619128
24. Bahadur A, Mundhra R, Sharma S, Ajmani M, Zaman R, Chaturvedi J. Psychological distress and post-COVID sequelae in postpartum females after clinically stable COVID-19 infections: a single-center observational study from India. Int J Appl Basic Med Res. 2022;12(3):185–188. doi:10.4103/ijabmr.ijabmr_173_22
25. Wang MY, Liu IC, Chiu CH, Tsai PS. Cultural adaptation and validation of the Chinese version of the fatigue severity scale in patients with major depressive disorder and nondepressive people. Qual Life Res. 2016;25(1):89–99. doi:10.1007/s11136-015-1056-x
26. Rosti-Otajarvi E, Hamalainen P, Wiksten A, Hakkarainen T, Ruutiainen J. Validity and reliability of the fatigue severity scale in Finnish multiple sclerosis patients. Brain Behav. 2017;7(7):e00743. doi:10.1002/brb3.743
27. Salari N, Khazaie H, Hosseinian-Far A, et al. The prevalence of sleep disturbances among physicians and nurses facing the COVID-19 patients: a systematic review and meta-analysis. Global Health. 2020;16(1):92. doi:10.1186/s12992-020-00620-0
28. Chong MY, Wang WC, Hsieh WC, et al. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br J Psychiatry. 2004;185:127–133. doi:10.1192/bjp.185.2.127
29. Chen Y, Zhang Y, Jin R. Professional identity of male nursing students in 3-year colleges and junior male nurses in China. Am J Mens Health. 2020;14(4):1557988320936583. doi:10.1177/1557988320936583
30. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi:10.1016/j.psychres.2020.112954
31. Liu YE, Zhai ZC, Han YH, Liu YL, Liu FP, Hu DY. Experiences of front-line nurses combating coronavirus disease-2019 in China: a qualitative analysis. Public Health Nurs. 2020;37(5):757–763. doi:10.1111/phn.12768
32. Dong ZQ, Ma J, Hao YN, et al. The social psychological impact of the COVID-19 pandemic on medical staff in China: a cross-sectional study. Eur Psychiatry. 2020;63(1):e65. doi:10.1192/j.eurpsy.2020.59
33. Al-Khani AM, Sarhandi MI, Zaghloul MS, Ewid M, Saquib N. A cross-sectional survey on sleep quality, mental health, and academic performance among medical students in Saudi Arabia. BMC Res Notes. 2019;12(1):665. doi:10.1186/s13104-019-4713-2
34. Lock AM, Bonetti DL, Campbell ADK. The psychological and physiological health effects of fatigue. Occup Med. 2018;68(8):502–511. doi:10.1093/occmed/kqy109
35. Gomez-Salgado J, Palomino-Baldeon JC, Ortega-Moreno M, Fagundo-Rivera J, Allande-Cusso R, Ruiz-Frutos C. COVID-19 information received by the Peruvian population, during the first phase of the pandemic, and its association with developing psychological distress: information about COVID-19 and distress in Peru. Medicine. 2022;101(5):e28625. doi:10.1097/MD.0000000000028625
36. Ruiz-Frutos C, Palomino-Baldeon JC, Ortega-Moreno M, et al. Effects of the COVID-19 pandemic on mental health in Peru: psychological distress. Healthcare. 2021;9(6):691.
37. Ruiz-Frutos C, Ortega-Moreno M, Soriano-Tarin G, et al. Psychological distress among occupational health professionals during coronavirus disease 2019 pandemic in Spain: description and effect of work engagement and work environment. Front Psychol. 2021;12:765169. doi:10.3389/fpsyg.2021.765169
38. Gomez-Salgado J, Pomares-Herrera F, Fagundo-Rivera J, Ortega-Moreno M, Garcia-Iglesias JJ, Ruiz-Frutos C. Use of preventive measures, beliefs and information received about COVID-19 and their effects on mental health, in two stages of the pandemic in Colombia. Ann Med. 2022;54(1):2246–2258. doi:10.1080/07853890.2022.2109057
39. Dominguez-Salas S, Gomez-Salgado J, Guillen-Gestoso C, Romero-Martin M, Ortega-Moreno M, Ruiz-Frutos C. Health care workers’ protection and psychological safety during the COVID-19 pandemic in Spain. J Nurs Manag. 2021;29(7):1924–1933. doi:10.1111/jonm.13331
40. Gomez-Salgado J, Ortega-Moreno M, Soriano G, Fagundo-Rivera J, Allande-Cusso R, Ruiz-Frutos C. History of contact with the SARS-COV-2 virus and the sense of coherence in the development of psychological distress in the occupational health professionals in Spain. Sci Prog. 2021;104(2):368504211026121. doi:10.1177/00368504211026121
41. Felger JC. Imaging the role of inflammation in mood and anxiety-related disorders. Curr Neuropharmacol. 2018;16(5):533–558. doi:10.2174/1570159X15666171123201142
42. Manookian A, Dehghan Nayeri N, Shahmari M. Physical problems of prolonged use of personal protective equipment during the COVID-19 pandemic: a scoping review. Nurs Forum. 2022;57(5):874–884. doi:10.1111/nuf.12735
43. Foo CC, Goon AT, Leow YH, Goh CL. Adverse skin reactions to personal protective equipment against severe acute respiratory syndrome--a descriptive study in Singapore. Contact Dermatitis. 2006;55(5):291–294. doi:10.1111/j.1600-0536.2006.00953.x
44. Yu J, Chen JK, Mowad CM, et al. Occupational dermatitis to facial personal protective equipment in health care workers: a systematic review. J Am Acad Dermatol. 2021;84(2):486–494. doi:10.1016/j.jaad.2020.09.074
45. Potter AW, Gonzalez JA, Xu X. Ebola response: modeling the risk of heat stress from personal protective clothing. PLoS One. 2015;10(11):e0143461. doi:10.1371/journal.pone.0143461
46. Davey SL, Lee BJ, Robbins T, Randeva H, Thake CD. Heat stress and PPE during COVID-19: impact on healthcare workers’ performance, safety and well-being in NHS settings. J Hosp Infect. 2021;108:185–188. doi:10.1016/j.jhin.2020.11.027
47. Lee J, Venugopal V, Latha PK, et al. Heat stress and thermal perception amongst healthcare workers during the COVID-19 pandemic in India and Singapore. Int J Environ Res Public Health. 2020;17(21):8100.
48. Flouris AD, Dinas PC, Ioannou LG, et al. Workers’ health and productivity under occupational heat strain: a systematic review and meta-analysis. Lancet Planet Health. 2018;2(12):e521–e31. doi:10.1016/S2542-5196(18)30237-7
49. Ceban F, Ling S, Lui LMW, et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain Behav Immun. 2022;101:93–135. doi:10.1016/j.bbi.2021.12.020
50. Tselebis A, Lekka D, Sikaras C, et al. Insomnia, perceived stress, and family support among nursing staff during the pandemic crisis. Healthcare. 2020;8(4). doi:10.3390/healthcare8040434
51. Kemper KJ, Mo X, Khayat R. Are Mindfulness and Self-Compassion Associated with Sleep and Resilience in Health Professionals?. J Altern Complement Med. 2015;21(8):496–503. doi:10.1089/acm.2014.0281
52. Vitale E. The mindfulness and the emotional regulation skills in Italian nurses during the COVID-19 pandemic: a descriptive survey-correlational study. J Holist Nurs. 2021;39(4):345–355. doi:10.1177/08980101211015804
53. Hepburn SJ, Carroll A, McCuaig L. The relationship between mindful attention awareness, perceived stress and subjective wellbeing. Int J Environ Res Public Health. 2021;18(23):12290. doi:10.3390/ijerph182312290
54. Ghawadra SF, Lim Abdullah K, Choo WY, Danaee M, Phang CK. The effect of mindfulness-based training on stress, anxiety, depression and job satisfaction among ward nurses: a randomized control trial. J Nurs Manag. 2020;28(5):1088–1097. doi:10.1111/jonm.13049
55. Yu J, Song Y, Hua D, Shi Y, Zhao J. Factors influencing mindfulness among clinical nurses in China: an observational cross-sectional study. J Nurs Manag. 2022;30(3):758–766. doi:10.1111/jonm.13560
56. China NHCotPsRo. Notice on further optimising the implementation of measures to prevent and control the new coronary pneumonia outbreak; 2022. Available from: http://www.nhc.gov.cn/xcs/gzzcwj/202212/8278e7a7aee34e5bb378f0e0fc94e0f0.shtml.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of the Working Hours Among Malaysian Nurses on Their Ill-Being, Intention to Leave, and the Perceived Quality of Care: A Cross-Sectional Study During the COVID-19 Pandemic
Jarrar M, Binti Ali N, Shahruddin R, Al-Mugheed K, Aldhmadi BK, Al-Bsheish M, AlSyouf A, AlBaker W, Alumran A
Journal of Multidisciplinary Healthcare 2023, 16:119-131
Published Date: 13 January 2023
The Impact of Psychological Interventions with Elements of Mindfulness on Burnout and Well-Being in Healthcare Professionals: A Systematic Review
Selič-Zupančič P, Klemenc-Ketiš Z, Onuk Tement S
Journal of Multidisciplinary Healthcare 2023, 16:1821-1831
Published Date: 29 June 2023
Anxiety and Insomnia Mediate the Association of Fear of Infection and Fatigue: A Cross-Sectional Survey of Nurses Deployed to a COVID-19 Epicenter in China
Liu Z, Zhang H, Wang N, Feng Y, Liu J, Wu L, Liu Z, Liu X, Liang L, Liu J, Wu Q, Liu C
Journal of Multidisciplinary Healthcare 2023, 16:2439-2448
Published Date: 24 August 2023
The Nexus Between Ethical Leadership and Employees’ Perception of Workplace Safety During COVID-19 Under Mediation and Moderation Model
Sun J, Sarfraz M, Asghar M
Risk Management and Healthcare Policy 2023, 16:1815-1837
Published Date: 12 September 2023
Levels and Factors of Nurses’ Alarm Fatigue in Critical Care Settings in Saudi Arabia: A Multicenter Cross-Sectional Study
Alkubati SA, Alsaqri SH, Alrubaiee GG, Almoliky MA, Alqalah TAH, Pasay-An E, Alrasheeday AM, Elsayed SM
Journal of Multidisciplinary Healthcare 2024, 17:793-803
Published Date: 22 February 2024