Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
The Relationship Between Diabetes Knowledge and Diabetes Self-Care Behaviors in Relation to Diabetes Distress in Type 2 Diabetes Mellitus: A Cross-Sectional Study in Eastern Taiwan
Authors Chen YC, Huang YH, Lee CH ![]()
Received 30 October 2024
Accepted for publication 29 April 2025
Published 5 May 2025 Volume 2025:18 Pages 1431—1443
DOI https://doi.org/10.2147/DMSO.S503754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Yi-Chien Chen,1,2 Yi-Hua Huang,1 Chao-Hsien Lee2
1Department of Nursing, Taipei Veterans General Hospital, Yuli Branch, Hualien, Taiwan, Republic of China; 2Department of Social Work, Meiho University, Pingtung, Taiwan, Republic of China
Correspondence: Chao-Hsien Lee, Department of Social Work, Meiho University, No. 23, Pingguang Road, Neipu, Pingtung County, 91202, Taiwan, Republic of China, Tel +886-8-7799821 ext. 6400, Fax +886-8-7784416, Email [email protected]
Introduction: Diabetes is a highly prevalent metabolic disease worldwide. In Taiwan, healthcare services emphasize self-management strategies and interventions focusing on self-care. However, there is a lack of literature on diabetes distress (DD). Therefore, this study aims to explore the relationship between demographic characteristics, diabetes knowledge, and diabetes self-care behaviors with diabetes distress among Type 2 diabetes mellitus (T2DM) patients and identify predictive factors.
Methods: This study employs a cross-sectional survey, targeting T2DM patients from the internal medicine outpatient clinic of a regional hospital in eastern Taiwan. Participants were recruited through purposive sampling from April 11, 2023, to May 16, 2023. The study examines the correlation between diabetes knowledge, diabetes self-care behaviors, and diabetes distress, as well as other influencing factors. The data analysis methods include (1) differences in diabetes knowledge, diabetes self-care behaviors, and diabetes distress scores, analyzed using t-tests or ANOVA, (2) Scheffe’s tests for significant differences identified by ANOVA to locate group differences in means, and (3) multiple regression analysis to identify key predictive factors of diabetes distress.
Results: The findings reveal that both diabetes knowledge (β=− 0.046, p=0.029) and diabetes self-care behaviors (β=− 0.186, p=0.006) significantly predict diabetes distress. Additionally, gender (β=0.251, p=0.004), family history of diabetes (β=0.213, p=0.017), and diabetes complications (β=0.228, p=0.018) are significant predictors of diabetes distress. The overall F-test reached significance (F=7.61, p< 0.001), and the explanatory power of the regression model (R²=0.17) is statistically significant, indicating that diabetes knowledge, diabetes self-care behaviors, gender, family history of diabetes, and diabetes complications are important predictors of diabetes distress in T2DM patients. These findings can provide valuable insights for clinicians in identifying risk factors for diabetes distress and understanding the factors that influence diabetes distress in T2DM patients.
Conclusion: It is crucial to integrate the assessment and management of diabetes distress into routine diabetes care and even implement distress screening during the health promotion stage. Strengthening the ability of healthcare professionals to identify diabetes distress through early detection of risk factors and providing individualized interventions and care plans tailored to T2DM patients is of great importance.
Keywords: type 2 diabetes, diabetes knowledge, diabetes self-care behaviors, diabetes distress, diabetes knowledge questionnaire, DKQ-18, diabetes self-care behaviors scale, problem areas in diabetes scale, PAID
Background
Diabetes is a highly prevalent metabolic disease worldwide, posing a significant burden on public health systems.1 Taiwan has the highest prevalence of diabetes in Asia. According to statistics from Taiwan’s Ministry of Health and Welfare, more than one in ten people may have diabetes. In 2023, diabetes ranked fifth among the leading causes of death and was the third-highest expenditure in the National Health Insurance system, amounting to approximately NT$36.4 billion annually.2 This indicates that diabetes has one of the highest incidences among chronic diseases in Taiwan and is a major health issue. Routine clinical care primarily focuses on diabetes self-management plans, such as diet, physical activity, and medication adherence,3 yet often overlooks the psychological distress related to diabetes. One unique and challenging psychosocial issue for diabetes patients is diabetes distress (DD).4,5 The term “diabetes distress” was introduced into psychosocial research in 1995 by a group of psychologists and psychiatrists from the Joslin Diabetes Center, referring to the negative emotions or emotional experiences arising from the challenges of living with the demands of diabetes.6 Diabetes distress is a negative emotional state, not a pathological condition. It is a syndrome composed of multiple dimensions, triggered by stress under specific circumstances or difficulties in coping with diabetes in daily life, and it may be accompanied by worry, conflict, frustration, and depression.7–10 There is a bidirectional relationship between depressive mood and diabetes.11 Diabetes distress differs from clinical depression, which is characterized by distinct symptoms but lacks diabetes-related emotional stress and worry.12 However, when severe or exacerbated by other environmental or personal factors, diabetes distress can become severe enough to lead to depression.13 Therefore, the relationship between diabetes distress and depression, as well as the significant overlap between these conditions, should be considered.14 Addressing diabetes distress can help individuals make clear decisions,3 assisting clinicians in identifying barriers to diabetes management.15
The personal sociodemographic characteristics of T2DM patients have been shown to predict psychological distress, and studies have found that the impact of diabetes distress on diabetes control may be greater than that of depression.16 Diabetes distress is related to changes in blood sugar and HbA1c levels.7,12,14 After health education interventions a 10% reduction in diabetes distress is associated with a 0.25% decrease in HbA1c levels.16,17 Some scholars suggest that diabetes distress is an emotional disorder that negatively affects diabetes self-care behaviors, leading to poor blood sugar control,18 although no direct relationship with HbA1c has been found.19,20 Diabetes distress in adult T2DM patients has been associated with smoking behavior,21 but some studies indicate no correlation.7 Gender is not directly related to diabetes distress, but women are more likely to experience diabetes distress due to gender roles and emotional differences.9,20,22 Lower educational levels are associated with higher diabetes distress.3 Factors such as younger age, higher BMI, marital status, blood lipid levels, diabetes complications, poor self-care ability, and low adherence to nutritional plans may be related to diabetes distress,12,17,23 although some studies report different results.7–9,20,22 Due to the inconsistency in the findings of various studies, further research is needed to clarify the relationship between diabetes distress and demographic characteristics.
There is a positive correlation between diabetes knowledge and blood sugar levels,17 but no significant correlation between diabetes knowledge and diabetes distress,21 that self-care is correlated with diabetes distress.24 However, higher diabetes knowledge is positively correlated with diabetes self-care behaviors,25 suggesting that diabetes distress may be a result of inadequate self-care.7 Diabetes distress is widespread and significantly impacts self-care, which aids in the early detection and management of diabetes distress. The potential benefit of addressing the link between diabetes distress and self-care lies in enhancing self-care programs for managing diabetes distress.24 Diabetes distress reduces self-care abilities, affecting the individual’s capacity to solve problems necessary for effective diabetes self-care.26
Monitoring diabetes distress as part of routine clinical care has already been incorporated into the guidelines of many countries.26 However, existing research is mostly focused on Western countries, with limited exploration of diabetes distress in Asia or other cultural contexts. in the context of Taiwan’s healthcare culture, healthcare services primarily focus on self-management strategies and interventions related to self-care, leading to a lack of literature on diabetes distress. From the existing literature, it is evident that the factors influencing diabetes distress vary across countries due to differences in culture and healthcare policies. In Taiwan, mental health issues are still not widely recognized. Diabetes patients may be less likely to seek psychological counseling or emotional support, and healthcare professionals may not fully understand the factors contributing to difficulties in managing diabetes. Therefore, the purpose of this study is to explore the relationship between the demographic characteristics, diabetes knowledge, diabetes self-care behaviors, and diabetes distress of T2DM patients, as well as to identify the predictive factors.
Methods
Study Design and Population
This study is a cross-sectional survey, approved by the Institutional Review Board (or Ethics Committee) of Yuli Hospital, Ministry of Health and Welfare (protocol code, YLH-IRB-11203), and the relevant institution. The research subjects were T2DM patients from the internal medicine outpatient clinic of a regional hospital in eastern Taiwan, selected through purposive sampling. The data collection period spanned one month, from 11 April 2023 to 16 May 2023. The study focused on the relationship between diabetes knowledge, diabetes self-care, and diabetes distress in T2DM patients, as well as the exploration of influencing factors. The independent variables include “Demographic Characteristics”, “Diabetes Knowledge Questionnaire”, and “Diabetes Self-Care Behaviors Scale”. The dependent variable is diabetes distress (Figure 1).
 |
Figure 1 Research Framework. |
Inclusion and Exclusion Criteria
The inclusion criteria for the participants were as follows: (1) diagnosed by a physician with T2DM, ICD-10: E11.9; (2) aged 20 years or older; (3) clear consciousness, able to complete the questionnaire independently or through verbal communication; (4) able to clearly express themselves in a Taiwanese language; (5) provided informed consent after being informed of the study’s purpose and methods, and possessed valid blood test results at the time of recruitment. The exclusion criteria were: (1) individuals with cognitive impairment or depression, anxiety or other psychiatric disorders that could interfere with the evaluation of the diabetes distress; (2) individuals unable to communicate; (3) pregnant or breastfeeding women with Type 2 diabetes. The research followed the ethical principles of the World Medical Association’s Declaration of Helsinki, researchers first provide participants with detailed information about the study plan and their rights as respondents. After signing the informed consent form and providing written consent, the participants were given the questionnaire. The questionnaires were completed anonymously, and participants were given a gift as a token of appreciation for their participation in the study. From explaining the consent form to collecting self-reported data, all tasks were completed by the same researcher.
Data Source and Participants
To achieve the necessary statistical power and minimize sample attrition, we conservatively estimated α = 0.05 and power = 0.95, with a correlation coefficient of −0.28 between self-care behaviors and psychological distress.27 Using Pearson’s correlation and a two-tailed test, it was determined that a minimum sample size of 160 participants was required. Taking into account an expected sample attrition rate of 10%, this study aimed to recruit at least 176 T2DM patients. The sample size estimation was conducted using G*Power (version 3.1).28,29
Questionnaire Design
The research tools were divided into two parts: the first consisted mainly of self-administered questionnaires, and the second involved obtaining physiological indicators from the health insurance database’s examination reports on the day of recruitment. The questionnaire collected information on “demographic characteristics”, “Diabetes Knowledge Questionnaire”, “Diabetes Self-Care Behaviors Scale”, and the “Chinese Version of the Problem Area in Diabetes, PAID-C”, all of which were validated and previously published scales, with the participants being Taiwanese nationals. The details are as follows.
Demographic Characteristics
(1) Basic information: Age, Gender, Marital status, Education level, Family history of diabetes, Duration of diabetes, Diabetes complications, Treatment method, Nutritional consultation, Smoking, and Frequency of exercise.
(2) Physiological indicators: BMI, HbA1c, and Total Cholesterol.
Participant’s Demographic Characteristics such as BMI, HbA1c, Cholesterol levels, Complication were obtained from the medical records of the healthcare system at the study site.
Diabetes Knowledge Questionnaire (DKQ-18)
This study used the Diabetes Knowledge Questionnaire (DKQ-18),30 with authorization from the original authors. The DKQ was initially developed in Spanish and English, with a Cronbach’s alpha of 0.78. The simplified Chinese version had a Cronbach’s alpha of 0.89, and it has been translated and validated in several languages, including simplified Chinese.30 To make the DKQ freely available in Chinese-speaking countries, it was translated into traditional Chinese for use in Taiwan, and its factor structure, internal consistency, known-group validity, responsiveness, test-retest reliability, and validity were evaluated. The simplified version of DKQ-18, derived from the original 24-item DKQ, contains 18 items in traditional Chinese. The Cronbach’s α of DKQ-18 is 0.732, and McDonald’s ω is 0.748. DKQ-18 assesses diabetes knowledge across five factors: diabetes etiology and symptoms, intermediate nursing, complications, diet and treatment, and elementary nursing.30 The questionnaire consists of 18 items, with responses categorized as “correct”, “incorrect”, or “do not know”. Eight questions are labeled as correct, and ten are labeled as incorrect. Each correct answer scores 1 point, while incorrect or “do not know” answers score 0. The total score ranges from 0 to 18, with higher scores indicating better diabetes knowledge.
Diabetes Self-Care Behaviors Scale (DSC)
This study used the Diabetes Self-Care Behaviors Scale, which was revised by Wang et al in 1998 from the scale developed by Hurley and Shea in 1992. The original authors authorized its use.31 The reliability analysis yielded a Cronbach’s α of 0.96, with an internal consistency Cronbach α value of 0.82 and a KMO of 0.68. The scale consists of five categories: exercise self-care (4 items), dietary self-care (6 items), medication and blood glucose monitoring self-care (7 items), foot care self-care (5 items), and self-care for the prevention and management of hypoglycemia and hyperglycemia (4 items).31 In total, the structured self-administered questionnaire contains 26 items. All items are positively scored using a Likert 5-point scale, ranging from “not at all” (1 point), “sometimes not possible” (2 points), “fair” (3 points), “can be done” (4 points), to “completely done” (5 points). The total score ranges from 26 to 130, with higher scores indicating better management of self-care behaviors.
Chinese Version of the Problem Area in Diabetes (PAID-C)
The scale used in this study to measure diabetes distress is the Chinese Version of the Problem Area in Diabetes (PAID-C), developed by Polonsky in 1995 and adapted into Chinese in 2010.32 The confirmatory factor analysis of PAID-C shows good construct validity, with GFI = 0.901 and CFI = 0.905. The scale’s score is significantly correlated with blood glucose levels (r = −0.17, p < 0.05), and the test-retest reliability after four weeks is 0.83 (p < 0.01). This indicates that the scale has good reliability and validity for measuring disease-related stress in diabetes patients and reflecting stress accumulated from medical orders and treatment outcomes.32 The scale contains four dimensions: emotional aspect (11 items), dietary aspect (3 items), treatment aspect (3 items), and social support (3 items), totaling 20 items. It uses a Likert 5-point scale, ranging from “not a problem” (0 points), “minor problem” (1 point), “moderate problem” (2 points), “somewhat serious problem” (3 points), to “serious problem” (4 points). The total score ranges from 0 to 80, with higher scores indicating higher levels of subjective diabetes-related stress.
Statistical Analysis
After collecting the questionnaires, incomplete or patterned responses, as well as invalid questionnaires with only a single response option, were excluded. The valid questionnaires were coded and entered into the computer based on the responses. Data entry and analysis were conducted using SPSS for Windows version 26.0. The data analysis methods were as follows:
Descriptive statistics: 14 demographic variables were analyzed for means, standard deviations, and percentages to describe the sample structure.
Inferential statistics: (1) Two-sample t-test: For variables with two groups, differences in diabetes knowledge, diabetes self-care behaviors, and diabetes distress scores were analyzed. (2) One-way ANOVA: For variables with three or more groups, differences in diabetes knowledge, diabetes self-care behaviors, and diabetes distress scores were analyzed. (3) If the F-value of the one-way ANOVA reached significance (P < 0.05), Scheffé’s method was used to identify which groups had significant differences in their means. (4) Pearson’s correlation analysis was conducted to identify the correlations among diabetes knowledge, diabetes self-care behaviors, and diabetes distress in patients with type 2 diabetes mellitus. (5) Multiple regression analysis was conducted to identify important predictors of diabetes distress from diabetes knowledge, diabetes self-care behaviors, and demographic characteristics.
Results
The study participants were T2DM patients from the internal medicine outpatient clinic of a regional hospital in eastern Taiwan. This study focused on the relationship between diabetes knowledge, diabetes self-care behaviors, and diabetes distress. From April 11, 2023, to May 16, 2023, a total of 220 questionnaires were distributed. Among them, 196 valid questionnaires were collected, while 24 were deemed invalid, yielding a response rate of 89%. Additionally, the normality of continuous variables was assessed using the Kolmogorov–Smirnov test, and all variables were found to be normally distributed.
Demographic Characteristics and Physiological Indicators of Participants
The demographic characteristics are summarized in Table 1, using frequency distribution and percentage analysis. The participant’s ages ranged from 28 to 80 years, with an average age of 59 years. The gender ratio between males and females was roughly equal. Most participants were married, and educational levels were generally low, with over 60% having a family history of diabetes. The majority of participants had been diagnosed with diabetes for fewer than five years. Over 70% of participants had diabetes complications, with oral hypoglycemic agents being the primary treatment method. Among the complications, eye diseases were the most common. More than 40% of participants had not received nutritional consultations in the past year, approximately 30% were smokers, and nearly 70% did not engage in regular physical exercise.
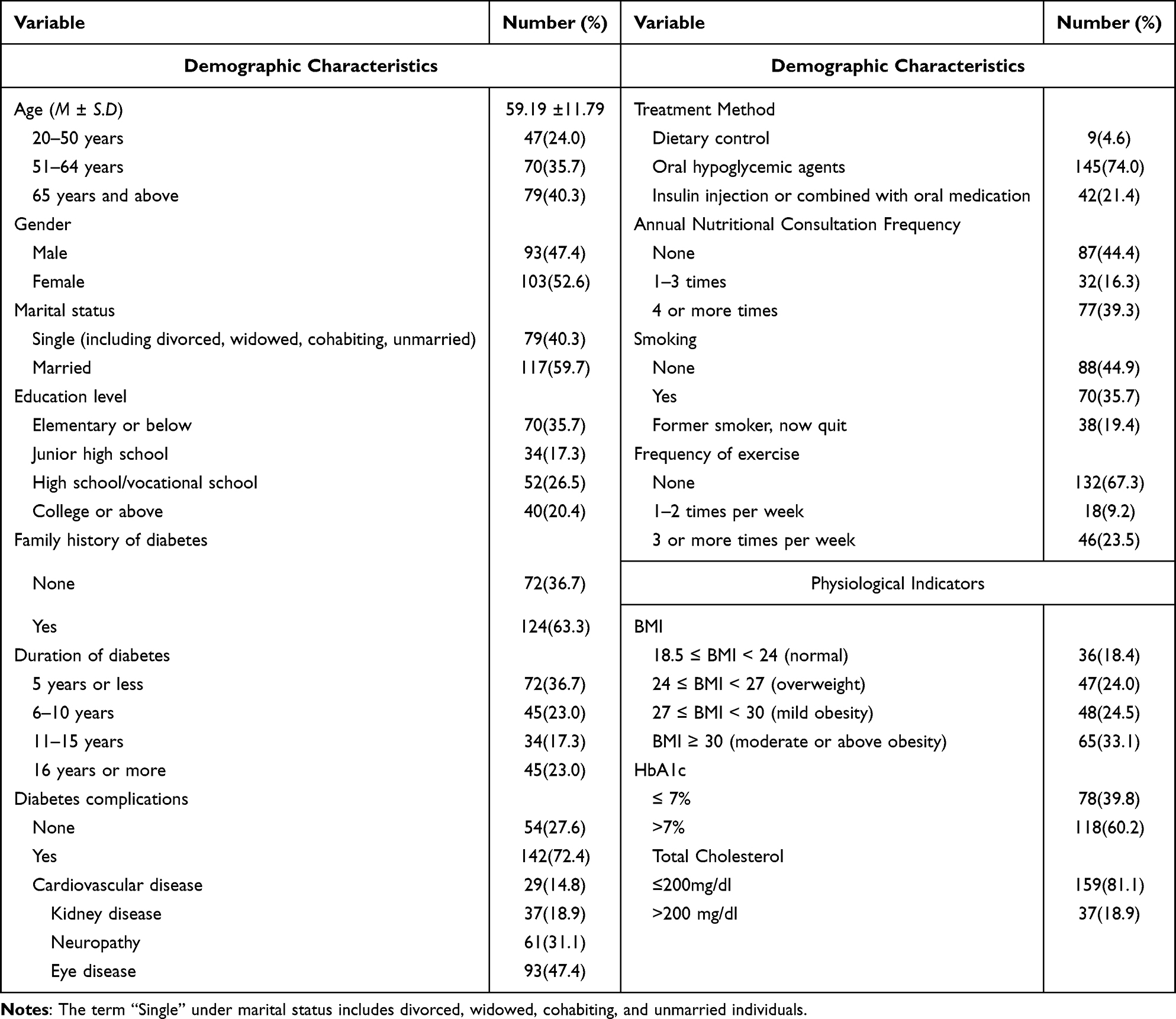 |
Table 1 Demographic Characteristics and Physiological Indicators of Participants (N=196) |
In terms of physiological indicators, only around 20% of participants had a normal BMI, while 60% had an HbA1c level greater than 7.0%, indicating elevated blood sugar levels. Approximately 20% of participants had abnormal total cholesterol levels, exceeding 200 mg/dl (Table 1).
Analysis of Current Status of Diabetes Knowledge, Diabetes Self-Care Behaviors, and Diabetes Distress
The Diabetes Knowledge Questionnaire (DKQ-18) consists of five factors with corresponding question numbers: six questions on diabetes etiology and symptoms, four on intermediate nursing, three on complications, two on diet and treatment, and three on elementary nursing. The overall average total score in terms of diabetes knowledge was 11.30 (SD=2.16). The highest scoring questions were in the elementary nursing category, with the following top three correct response rates: “Diabetics should take extra care when cutting their toenails” (98%), “Cuts and abrasions on diabetics heal more slowly” (96.9%), and in the complications category, “Diabetes can cause loss of feeling in my hands, fingers, and feet” (94.9%). The lowest scoring questions were: “A person with diabetes should cleanse a cut with iodine and alcohol” from intermediate nursing (9.2%), “Diabetes is caused by failure of the kidneys to keep sugar out of the urine” from diabetes etiology and symptoms (14.8%), and “An insulin reaction is caused by too much food” (17.3%). Among the five factors, the highest overall average correct response rate was in elementary nursing (95.4%), while the lowest was in diabetes etiology and symptoms (27.3%).
The Diabetes Self-Care Behaviors Scale is organized into five categories: exercise self-care, dietary self-care, medication and blood glucose monitoring self-care, foot care self-care, and prevention and management of hypo- and hyperglycemia, totaling 26 items. On average, participants scored 71.40 (SD=17.48) in overall self-care. The highest average score was in medication and blood glucose monitoring self-care, while the lowest was in exercise participation.
In terms of diabetes distress, the overall average total score was 33.20 (SD=12.91). The top three highest scoring items were: “Worrying about the future and the possibility of serious complications?” with an average score of 2.96 (SD=1.22), “Not having clear and concrete goals for your diabetes care?” with 2.84 (SD=1.05), and “Feeling discouraged with your diabetes treatment plan?” with 2.52 (SD=1.08). The lowest scoring items were: “Feeling unsatisfied with your diabetes physician?” at 0.24 (SD=0.68), “Feeling that your friends and family are not supportive of your diabetes management efforts?” at 0.43 (SD=0.78), and “Feeling alone with your diabetes?” at 0.79 (SD=0.95).
The Role of Demographic Characteristics in Diabetes Knowledge, Diabetes Self-Care Behaviors, and Diabetes Distress
For diabetes knowledge, a significant difference was found in relation to education level (F=3.15, p=0.026), with participants who had a college education or higher scoring better than those with an elementary school education or lower. No statistically significant differences were observed for other demographic characteristics.
In terms of diabetes self-care behaviors, participants with an HbA1c level ≤7.0% scored higher than those with an HbA1c >7.0% (t=2.01, p=0.040), and those with total cholesterol <200 mg/dl scored higher than those with total cholesterol >200 mg/dl (t=2.09, p=0.038), both showing significant differences. The number of nutritional consultations in a year also showed a significant difference in self-care scores (F=3.53, p=0.031), with participants who had four or more consultations scoring better than those who had none. Smoking status was significantly associated with self-care scores (F=5.18, p=0.006), with non-smokers scoring better than smokers. Additionally, exercise frequency showed a significant difference (F=17.02, p<0.001), with those exercising three or more times per week scoring better than those who did not exercise. BMI was also significantly related to self-care behavior scores (F=3.18, p=0.025), with participants having a BMI of 24≤BMI<27 (overweight) scoring higher than those with a BMI ≥30 (moderate obesity).
In the diabetes distress dimension, women had significantly higher distress scores than men (t=−2.19, p=0.030). Participants with a family history of diabetes scored higher in distress than those without (t=−2.04, p=0.042), and those with complications had higher distress scores than those without complications (t=−2.04, p=0.042). No statistically significant differences were found for other variables (Table 2).
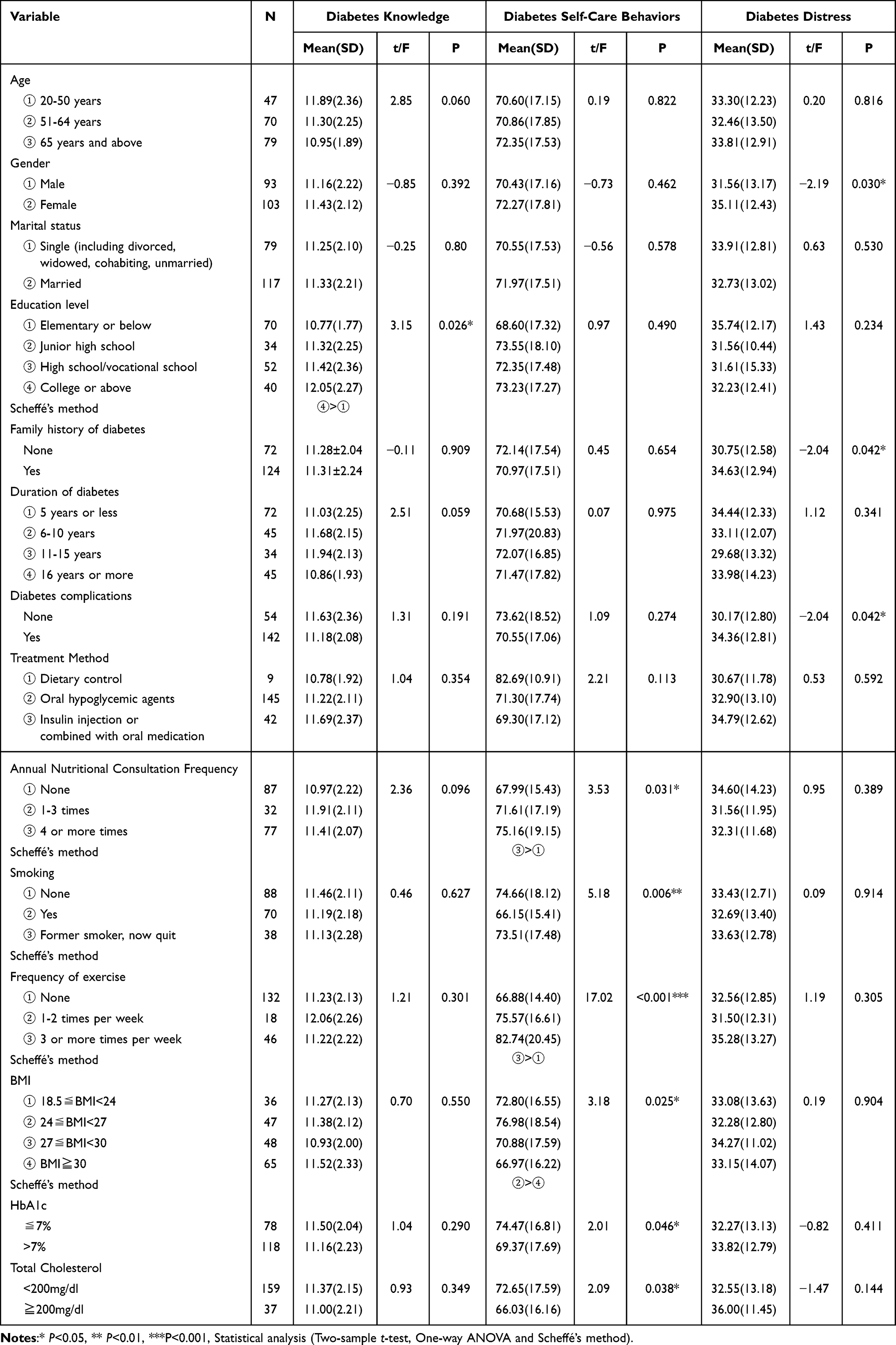 |
Table 2 Analysis of the Role of Demographic Characteristics in Diabetes Knowledge, Diabetes Self-Care Behaviors, and Diabetes Distress (N=196) |
The Correlations Among Diabetes Knowledge, Diabetes Self-Care Behaviors, and Diabetes Distress in Patients with Type 2 Diabetes Mellitus
Pearson’s correlation analysis revealed a significant positive correlation between diabetes knowledge and diabetes self-care behaviors (r=0.31, p<0.001), indicating that better diabetes knowledge is associated with better self-care behaviors. A significant negative correlation was found between diabetes knowledge and diabetes distress (r=−0.21, p<0.002), suggesting that higher diabetes knowledge is associated with lower distress. Additionally, a significant negative correlation was observed between diabetes self-care behaviors and diabetes distress (r=−0.25, p<0.001), indicating that better self-care behaviors are associated with lower distress.
In summary, among T2DM patients, there is a significant positive correlation between diabetes knowledge and diabetes self-care behaviors, and both diabetes knowledge and self-care behaviors are significantly negatively correlated with diabetes distress (Table 3).
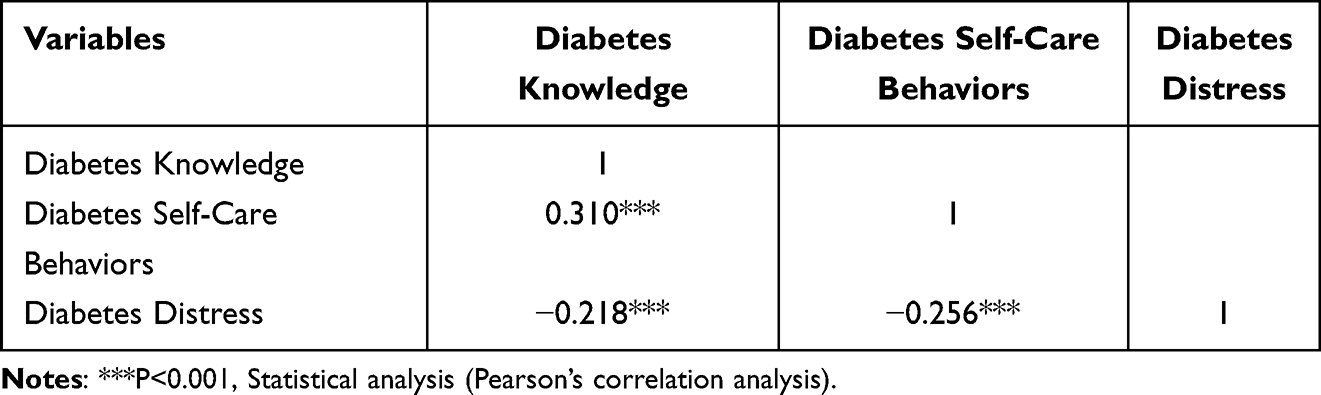 |
Table 3 Analysis of the Correlations Among Diabetes Knowledge, Diabetes Self-Care Behaviors, and Diabetes Distress in Patients With Type 2 Diabetes Mellitus |
Predictive Factors of Psychological Distress in T2DM Patients
A multiple regression analysis was conducted to explore the significant predictors of psychological distress in T2DM patients. The independent variables that showed a significant correlation with psychological distress were gender, family history of diabetes, and diabetes complications. Since these are categorical variables, they were converted into dummy variables before being entered into the regression analysis. Diabetes knowledge and self-care behaviors were also included as independent variables, with diabetes distress as the dependent variable.
The results showed that: Diabetes knowledge (β=−0.046, p=0.029) and diabetes self-care behaviors (β=−0.186, p=0.006) both significantly predicted diabetes distress; Gender (β=0.251, p=0.004), family history of diabetes (β=0.213, p=0.017), and diabetes complications (β=0.228, p=0.018) were also significant predictors of diabetes distress. Specifically, higher diabetes knowledge scores were associated with lower levels of diabetes distress, suggesting that individuals with greater knowledge about diabetes may feel more confident in managing their condition and, consequently, experience less emotional burden. Conversely, lower diabetes knowledge scores were linked to higher diabetes distress, implying that a lack of understanding may contribute to uncertainty and psychological stress. Similarly, higher diabetes self-care behavior scores were associated with lower diabetes distress, indicating that individuals who actively engage in self-care practices, such as medication adherence, regular exercise, and blood glucose monitoring, may feel more in control of their condition and experience reduced emotional burden. In contrast, inadequate self-care behaviors were linked to higher diabetes distress, suggesting that poor self-management may lead to feelings of helplessness and increased psychological stress. Furthermore, gender differences were observed, with females being more likely to experience diabetes distress compared to males, potentially due to differences in psychological coping mechanisms, emotional responses, and social expectations related to health management. Regarding family history of diabetes, individuals with a family history were more likely to report higher levels of diabetes distress than those without, possibly due to increased awareness of the disease’s long-term impact and concerns about its progression. Lastly, diabetes complications were also a significant factor, as individuals with complications experienced greater diabetes distress compared to those without, likely due to the added burden of managing multiple health issues and the fear of further deterioration.
The overall F-test was significant (F=7.61, p<0.001), and the explanatory power of the regression model (R²=0.17) was statistically significant. This suggests that approximately 17% of the variance in diabetes distress can be explained by the independent variables included in the model, such as diabetes knowledge, diabetes self-care behaviors, gender, family history of diabetes, and diabetes complications. While this indicates a moderate explanatory power, it also implies that other unexamined factors may contribute to diabetes distress, highlighting the complexity of psychological and behavioral influences on diabetes management. Nevertheless, these findings confirm that diabetes knowledge, diabetes self-care behaviors, gender, family history of diabetes, and diabetes complications are important predictive factors for diabetes distress in T2DM patients (Table 4).
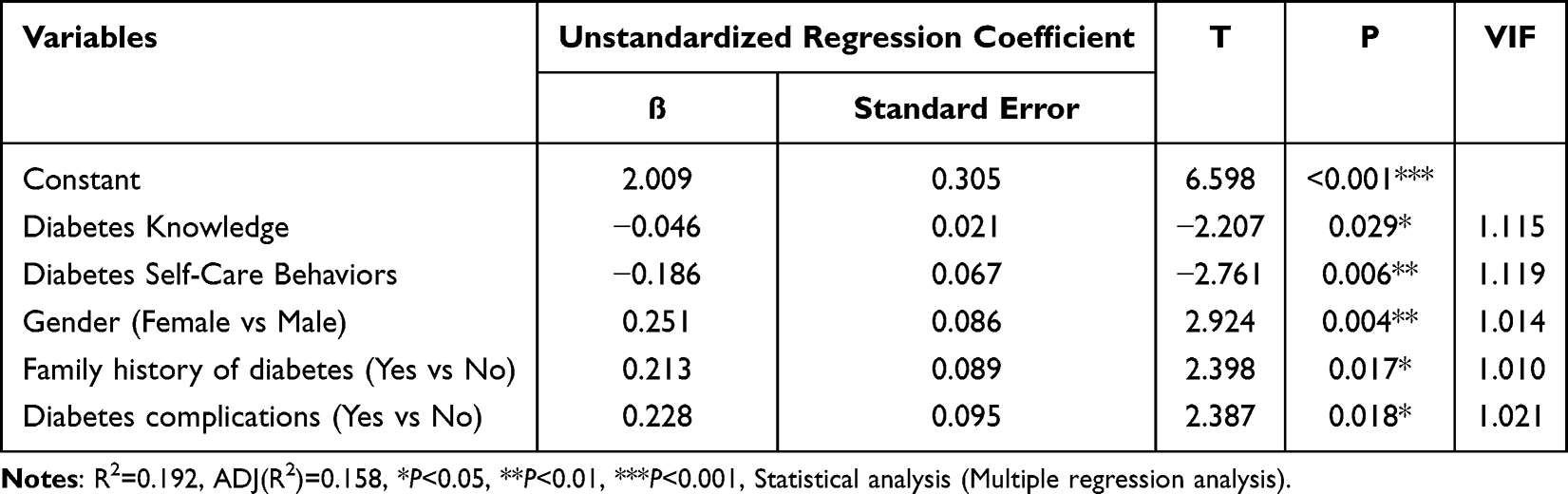 |
Table 4 Regression Analysis of Diabetes Distress in Patients With Type 2 Diabetes Mellitus |
Discussion
Two validated scales are used to assess diabetes distress: the Problem Areas in Diabetes Scale (PAID)6 and the Diabetes Distress Scale (DDS).33 These scales differ in their focus areas.34 The PAID includes questions on emotional states, anxiety symptoms, behavioral issues, and social interactions,6 while the DDS focuses mainly on sleep problems, emotional states, physical symptoms, appetite changes, concentration, self-worth, and interest in activities.33 The PAID covers a broader range of emotional issues, whereas the DDS is more appropriate when investigating factors closely related to diabetes self-management.14 The choice of scale should be based on the assessment goals and the specific circumstances of the patient.
In the five categories of the DSC, the highest mean score (SD) was for medication and blood glucose monitoring self-care (3.18±0.59), followed by hypoglycemia/hyperglycemia management (3.1±0.84), foot care (2.84±0.88), dietary control (2.7±0.85), and the lowest score was for exercise participation (1.9±1.17). This shows that while participants adhered well to medication and blood glucose monitoring, they were less engaged in exercise, even though systematic reviews and meta-analyses indicate that exercise is an effective non-pharmacological intervention for improving blood glucose control in T2DM patients.35 This underscores the need to strengthen interventions related to exercise in diabetes health education.
The PAID-C results showed that the highest distress levels were related to “Worrying about the future and the possibility of serious complications?” followed by “Not having clear and concrete goals for your diabetes care?” This correlates with the participants focus on complications in the knowledge dimension, but it also indicates that the lack of clear goals for care was a significant source of distress. Taiwan’s diabetes care policies emphasize shared decision-making between patients and healthcare providers, which is vital for reducing or delaying complications and maintaining patient health. However, this study’s results suggest that healthcare providers need to review and adjust care plans, ensuring comprehensive, patient-centered care that empowers patients to understand and achieve their care goals. This will not only boost patient confidence in self-care but also improve healthcare professionals job satisfaction.
A significant difference was found in diabetes knowledge scores related to education level, with those having a higher education performing better. This aligns with Chen CC et al (2020), who found that knowledge scores are related to education level.36 Older patients and those with lower education levels often have misunderstandings about diabetes management, requiring healthcare providers to communicate more effectively to help patients control their condition. Various personal lifestyle habits such as the number of nutritional consultations, smoking, exercise, BMI, HbA1c, and blood lipid levels were associated with Diabetes Self-Care Behaviors, suggesting a bidirectional relationship between personal lifestyle habits and self-care behaviors, as well as a correlation between diabetes self-care behaviors and diabetes distress.8
The PAID-C analysis showed that, although the number of male and female participants was similar, women exhibited higher levels of diabetes distress. Gender was found to be a predictor of diabetes distress, consistent with the findings of Perrin et al in a systematic review and meta-analysis.14 While gender roles in Taiwan are evolving towards equality, the study area remains a traditional rural community where Female diabetes patients are generally more likely than males to experience diabetes-related psychological distress, which may be related to social roles, family responsibilities, and greater sensitivity to health issues. On the other hand, male patients may be less likely to express emotional distress, leading to underassessment or inadequate management of their stress. Healthcare professionals should address the psychological needs of patients of different genders by providing appropriate mental health support. Through early screening and personalized health plans, the incidence of complications can be reduced, thereby alleviating patients psychological distress. Regarding smoking, only 35.7% of participants were smokers, and the study results are consistent with Kintzoglanaki’s findings, indicating no correlation between smoking and diabetes distress.7
Although numerous studies have shown a relationship between diabetes distress and HbA1c,7,12,14 no direct association was found in this study’s participants. The relationship between diabetes distress and HbA1c may differ across populations and countries, making it difficult to clarify the physiological mechanisms through which diabetes distress affects HbA1c The study results showed no significant association between age, marital status, education level, duration of diabetes, treatment method, nutritional consultations, exercise, BMI, or total cholesterol, contrasting with other studies.3,7,9,12,20,24 These differences may stem from regional variations or differing healthcare practices. Additionally, some scholars have suggested that insulin use is associated with higher diabetes distress,7 although others argue that medication type does not impact self-care or distress levels in diabetes patients.9 In this study, no significant difference was observed in treatment methods, as only 20.4% of participants used insulin or a combination of insulin and oral medication, which may explain the lack of significant findings. Future studies could further investigate the relationship between treatment type and diabetes distress using a more homogeneous sample.
Diabetes Self-Management Support (DSMS) has been shown to improve diabetes knowledge and reduce diabetes distress.37 Although this study did not examine the impact of DSMS on diabetes distress, the results demonstrate a significant correlation between diabetes knowledge and diabetes distress. These findings contrast with research conducted in China, another Asian country.21 Higher diabetes knowledge is positively correlated with better self-care behaviors,25 which was also observed in this study.7 While Devarajooh (2017) reported no direct relationship between diabetes self-care behaviors and diabetes distress,9 this study identified a significant statistical relationship between diabetes knowledge, self-care behaviors, and diabetes distress in the regression analysis. The predictive factors for diabetes distress in T2DM patients include diabetes knowledge, diabetes self-care behaviors, gender, family history of diabetes, and diabetes complications, accounting for 17% of the variance. These findings can provide valuable insights for clinicians in identifying risk factors for diabetes distress and understanding the factors that influence diabetes distress in T2DM patients.
Although Taiwan’s National Health Insurance (NHI) provides diabetes care and management programs, such as the Diabetes Shared Care Network (DCMP), factors such as patient adherence, medical resource distribution, and regional characteristics may affect the effectiveness of these policies. The study area is characterized by abundant medical resources and a high elderly population. In the participant characteristics, most had only completed elementary education and attended annual nutrition counseling. However, the majority did not engage in physical activity and had diabetes complications, poor HbA1c control, and an excessively high BMI. Despite all participants having equal access to healthcare services, this study has three limitations. First, the sample was limited to one regional hospital in Taiwan, and further validation is needed in different populations or countries to generalize the results. Second, participation was voluntary, which may limit the generalizability of the findings. Third, the study utilized a survey method, which cannot establish causal relationships. Since diabetes distress is largely a subjective experience, future studies should consider employing qualitative research methods to explore this issue in greater depth.
Conclusions
This study utilized the Diabetes Knowledge Questionnaire, Diabetes Self-Care Behaviors Scale, and the Chinese Version of the Problem Area in Diabetes to explore the significant correlations between demographic characteristics, diabetes knowledge, self-care behaviors, and diabetes distress in T2DM patients. Based on our findings, healthcare professionals should reduce diabetes distress by enhancing self-care behaviors in diabetes patients. This can be achieved by providing personalized diabetes education to stimulate patients intrinsic motivation, collaboratively setting feasible health goals, and offering positive reinforcement to strengthen their engagement and commitment. Ensuring that patients adhere to self-care practices can lead to better blood glucose control, a lower risk of complications, and reduced psychological stress and diabetes distress. It is necessary to incorporate the assessment and management of diabetes distress into routine diabetes care. Screening for related distress should be provided even during the health promotion stage. It is crucial to strengthen healthcare professionals ability to identify diabetes distress early through risk factors, in order to offer personalized interventions and care plans tailored to T2DM patients. Furthermore, healthcare professionals must ensure that the health education they provide does not increase patients frustration with self-care. Instead, a problem-oriented approach should be adopted to enhance patients self-care abilities.
Abbreviations
T2DM, Type 2 diabetes patient; DKQ, Diabetes Knowledge Questionnaire; DSC, Diabetes self-care scale; PAID, Chinese Version of the Problem Area in Diabetes; DD, diabetes distress.
Data Sharing Statement
The dataset was not publicly available during the current study, as it contains potentially identifiable information for each patient. However, it is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All methods were performed in accordance with the Declaration of Helsinki38 and approved by the Institutional Review Board (or Ethics Committee) of the Yuli Hospital, Ministry of Health and Welfare (protocol code, YLH-IRB-11203, and date of approval, 10 April 2023). Informed consent and signed informed consent statement forms was obtained from all subjects involved in the study, and publish anonymized data. All participants knew their right, could withdraw the study any time and provided written informed consent. All data were deidentified.
Acknowledgments
We thank the National Army Veterans Affairs Council for their research funding and the director of the Taipei Veterans General Hospital Yuli Branch for their support in the successful realization of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors state that they have no known competing financial interests or personal ties that may have seemed to affect the work presented in this publication; hence, no possible conflicts of interest are required to be disclosed.
References
1. Bazpour M, Rostampour S, Kamel-Khodabandeh A. Assessment of Quality of Life and Self-care Behaviors in Patients with Type 2 Diabetes Mellitus in Mashhad, Iran. Jundishapur J Chronic Dis Care. 2021;10(1):e105910. doi:10.5812/jjcdc.105910
2. Ministry of Health and welfare. R.O.C (Taiwan). The mortality statistics for the year 112 in Taiwan. 2020. Available from: https://www.mohw.gov.tw/cp-16-79055-1.html.
3. Misra R, Shawley-Brzoska S, Khan R, Kirk BO, Wen S, Sambamoorthi U. Addressing Diabetes Distress in Self-Management Programs Results of a Randomized Feasibility Study. J Appalachian Health. 2021;3(3):68–85. doi:10.13023/jah.0303.06
4. Arditi C, Zanchi A, Peytremann-Bridevaux I. Health status and quality of life in patients with diabetes in Switzerland. Primary Care Diabet. 2019;13(3):233–241. doi:10.1016/j.pcd.2018.11.016
5. Martinez-Vega IP, Doubova SV, Pérez-Cuevas R. Distress and its association with self-care in people with type 2 diabetes. Salud mental. 2017;40(2):47–55. doi:10.17711/SM.0185-3325.2017.007
6. Polonsky WJ, Anderson BJ, Lohrer PA, et al. Assessment of Diabetes-Related Distress. Diabetes Care. 1995;18(6):754–760. doi:10.2337/diacare.18.6.754
7. Kintzoglanakis K, Gkousiou A, Vonta P, Sagmatopoulos A, Copanitsanou P. Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: different roles for glycemic control and self-care. SAGE Open Medicine. 2022;10:1–9. doi:10.1177/20503121221096605
8. Hoogendoorn CJ, Schechter CB, Llabre MM, Walker EA, Gonzalez JS. Distress and Type 2 Diabetes Self-Care: putting the Pieces Together. Ann Behav Med. 2021;55(10):938–948. doi:10.1093/abm/kaaa070
9. Devarajooh C, Chinna K, Khamseh ME. Depression, distress and self-efficacy: the impact on diabetes self-care practices. PLoS One. 2017;12(3):e0175096. doi:10.1371/journal.pone.0175096
10. Thanakwang K, Thinganjana W, Konggumnerd R. Psychometric properties of the Thai version of the Diabetes Distress Scale in diabetic seniors. Clin Interventions Aging. 2014;9:1353–1361. doi:10.2147/CIA.S67200
11. Rubin RR, Peyrot M. Psychological issues and treatments for people with diabetes. J Clin Psychol. 2001;57(4):457–478. doi:10.1002/jclp.1041
12. Fisher L, Gonzalez JS, Polonsky WH. The confusing tale of depression and distress in patients with diabetes: a call for greater clarity and precision. Diabetic Med. 2014;31(7):764–772. doi:10.1111/dme.12428
13. Gonzalez JS, Delahanty LM, Safren SA, Meigs JB, Grant RW. Differentiating symptoms of depression from diabetes-specific distress: relationships with self-care in type 2 diabetes. Diabetologia. 2008;51(10):1822–1825. doi:10.1007/s00125-008-1113-x
14. Perrin NE, Davies MJ, Robertson N, Snoek FJ, Khunti K. The prevalence of diabetes-specific emotional distress in people with Type 2 diabetes: a systematic review and meta-analysis. Diabetic Med. 2017;34(11):1508–1520. doi:10.1111/dme.13448
15. Gracey M, Burke V, Martin DD, Johnston RJ, Jones T, Davis EA. Assessment of risks of “lifestyle” diseases including cardiovascular disease and type 2 diabetes by anthropometry in remote Australian Aborigines.. Asia Pacific J Clin Nutr. 2007;16(4):688–697.
16. Zagarins SE, Allen NA, Garb JL, Welch G. Improvement in glycemic control following a diabetes education intervention is associated with change in diabetes distress but not change in depressive symptoms. J Behav Medi. 2012;35(3):299–304. doi:10.1007/s10865-011-9359-z
17. Sun F, Wardian J. Factors Associated With Diabetes-Related Distress: implications for Diabetes Self-Management. Social Work Health Care. 2014;53(4):364–381. doi:10.1080/00981389.2014.884038
18. Fisher L, Glasgow RE, Mullan JT, Skaff MM, Polonsky WH. Development of a brief diabetes distress screening instrument. Annals of family medicine. Ann Family Med. 2008;6(3):246–252. doi:10.1370/afm.842
19. Indelicato L, Dauriz M, Santi L, et al. Psychological distress, self-efficacy and glycemic control in type 2 diabetes. Nutr Metab Cardiovasc Dis. 2017;27(4):300–306. doi:10.1016/j.numecd.2017.01.006
20. Fayed A, AlRadini F, Alzuhairi RM, et al. Relation between diabetes related distress and glycemic control: the mediating effect of adherence to treatment. Primary Care Diabet. 2022;16(2):293–300. doi:10.1016/j.pcd.2021.12.004
21. Hu Y, Li L, Zhang J. Diabetes Distress in Young Adults with Type 2 Diabetes: a Cross-Sectional Survey in China. J Diabet Res. 2020;4814378:1–6. doi:10.1155/2020/4814378
22. Habtewold TD, Alemu SM, Haile YG. Sociodemographic, clinical, and psychosocial factors associated with depression among type 2 diabetic outpatients in Black Lion General Specialized Hospital, Addis Ababa, Ethiopia: a cross-sectional study. BMC Psychiatry. 2016;16(103):2–7. doi:10.1186/s12888-016-0809-6
23. Kugbey N, Atindanbila S, Nyarko K, Atefoe EA. T2DM Patients Demographic Characteristics as Moderators of the Relationship between Diabetes Perception and Psychological Distress. Intl J Appl Psychol. 2015;5(3):59–63. doi:10.5923/j.ijap.20150503.01
24. Kader AIAE, Ibrahim ME, Mohamed HS, Osman BM. Diabetes Distress and Self-Care Activities Among Patients With Diabetes Type II: a Correlation Study. Sage Open Nurs. 2023;9:1–9. doi:10.1177/23779608231189944
25. Kugbey N, Asante KO, Adulai K. Illness perception, diabetes knowledge and self‑care practices among type‑2 diabetes patients: a cross‑sectional study. BMC Res Notes. 2017;10(1):381. doi:10.1186/s13104-017-2707-5
26. Tsenkova VK, Love GD, Singer BH, Ryff CD. Socioeconomic status and psychological well-being predict cross-time change in glycosylated hemoglobin in older women without diabetes. Psychosomatic Med. 2007;69(8):777–784. doi:10.1097/PSY.0b013e318157466f
27. Chen DA, Wang PC, Lin YH. The Relationship among Perceived Stress, Self-efficacy, Self-care Behaviors, Psychological Distress and Type D Personality in Type 2 Diabetes Mellitus. J Internal Med Taiwan. 2019;30(4):247–254. doi:10.6314/JIMT.201908_30(4).03
28. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
29. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behavior Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
30. Hsieh MH, Chen YC, Ho CH, Lin CY. Validation of Diabetes Knowledge Questionnaire (DKQ) in the Taiwanese Population-Concurrent Validity with Diabetes-Specific Quality of Life Questionnaire Module. Diab Metab Syndrome Obesity. 2022;15:2391–2403. doi:10.2147/DMSO.S369552
31. Wang JS, Wang RH, Lin CC. Self-care behaviors, self-efficacy, and social support effect on the glycemic control of patients newly diagnosed with non-insulin-dependent diabetes mellitus. Kaohsiung J Med Sci. 1998;14(12):807–815.
32. Huang MF, Courtney M, Edwards H, McDowell J. Validation of the Chinese Version of the Problem Areas in Diabetes (PAID-C) Scale. Diabetes Care. 2010;33(1):38–40. doi:10.2337/dc09-0768
33. Polonsky WH, Fisher L, Earles J, et al. Assessing psychosocial distress in diabetes: development of the Diabetes Distress Scale. Diabetes Care. 2005;28(3):626–631. doi:10.2337/diacare.28.3.626
34. Schmitt A, Reimer A, Kulzer B, Haak T, Ehrmann D, Hermanns N. How to assess diabetes distress: comparison of the Problem Areas in Diabetes Scale (PAID) and the Diabetes Distress Scale (DDS). Diabetic Med. 2016;33(6):835–843. doi:10.1111/dme.12887
35. Kumar S, Maiya AG, Shastry BA, et al. Exercise and insulin resistance in type 2 diabetes mellitus: a systematic review and meta-analysis. Ann Phys Rehabil Med. 2019;62(2):98–3103. doi:10.1016/j.rehab.2018.11.001
36. Chen CC, Chen CL, Ko Y. The Misconceptions and Determinants of Diabetes Knowledge in Patients with Diabetes in Taiwan. J Diabet Res. 2020;2020:2953521. doi:10.1155/2020/2953521
37. Heise M, Heidemann C, Baumert J, et al. Structured diabetes self-management education and its association with perceived diabetes knowledge, information, and disease distress: results of a nationwide population-based study. Primary Care Diabet. 2022;16(Suppl 2):387–394. doi:10.1016/j.pcd.2022.03.016
38. Jimenez G, Tan WS, Virk AK, et al. Overview of Systematic Reviews of Advance Care Planning: summary of Evidence and Global Lessons. J Pain Sympt Manage. 2018;56(3):436–459.e25. doi:10.1016/j.jpainsymman.2018.05.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.