Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Relationship Between Depression and Multifactorial Control and Microvascular Complications in Vietnamese with Type 2 Diabetes Mellitus Aged 30–60 Years
Authors Dinh Le T ![]() , Huy Duong H
, Huy Duong H ![]() , Thi Nguyen L, Phi Thi Nguyen N, Tien Nguyen S
, Thi Nguyen L, Phi Thi Nguyen N, Tien Nguyen S ![]() , Van Ngo M
, Van Ngo M
Received 24 December 2021
Accepted for publication 1 April 2022
Published 18 April 2022 Volume 2022:15 Pages 1185—1195
DOI https://doi.org/10.2147/DMSO.S354443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Tuan Dinh Le,1,2,* Hoang Huy Duong,3,* Ly Thi Nguyen,4,5,* Nga Phi Thi Nguyen,2 Son Tien Nguyen,2 Manh Van Ngo6
1Center of Emergency, Critical Care Medicine and Clinical Toxicology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 2Department of Rheumatology and Endocrinology,Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 3Department of Neurology, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 4Department of Internal Medicine, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 5Postgraduate Student, Department of Internal Medicine, Hanoi Medical University, Hanoi, Vietnam; 6Postgraduate Training Management Department, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam
*These authors contributed equally to this work
Correspondence: Tuan Dinh Le, Center of Emergency, Critical Care Medicine and Clinical Toxicology, Military Hospital 103, Vietnam Military Medical University, 160 Phung Hung Street, Phuc La Ward, Ha Dong District, Hanoi City, Vietnam, Tel +840388166078, Email [email protected] Hoang Huy Duong, Department of Neurology, Thai Binh University of Medicine and Pharmacy, 373 Ly Bon Street, Ky Ba Ward, Thai Binh, Vietnam, Tel +84 912675919, Email [email protected]
Background: Depression is a common mental disorder in people with type 2 diabetes mellitus (T2DM). Depression and T2DM have a reciprocal interaction through many factors, of which the most important is the multifactorial control and microvascular complications of T2DM.
Aim: This research aims to determine the rate of depression and the association between depression and multifactorial control and microvascular complications in patients with T2DM aged 30– 60 years in Vietnam.
Methods: A cross-sectional and descriptive study was conducted on 231 outpatients with T2DM at Bach Mai hospital, Hanoi, Vietnam. Depression severity was measured with the Patient Health Questionnaire-9 (PHQ-9).
Results: The rate of depression in patients with T2DM aged 30– 60 years was 16.9% (in which, the rate of mild depression was 15.2% and moderate depression was 1.7%; no serious depression). The prevalence of depression was higher in female patients than in male patients (p = 0.049). There is a statistically significant difference in the rate of depression by age, duration of diabetes, and treatment method for type 2 diabetes. Poor HbA1c control and microvascular complications increase the risk of depression (OR = 2.37; 95% CI 1.11– 5.02, p = 0.033 and OR = 2.62; 95% CI 1.15– 5.93, p = 0.027, respectively). When the multivariate analysis was performed, it was shown that sex, treatment for glycemic control, and microvascular complications had a statistically significant influence on PHQ-9 score.
Conclusion: In Vietnam, there are 16.9% of patients with T2DM aged 30– 60 years suffer from depression. Poor HbA1c control, the presence of microvascular complications, and without antihyperglycemic treatment increase the risk of developing depression.
Keywords: type 2 diabetes mellitus aged 30– 60 years, depression, multifactorial control, microvascular complications
Introduction
The association between depression and type 2 diabetes mellitus (T2DM) was first documented in the literature more than 300 years ago when Willis made the surprising conclusion that diabetes was caused by persistent depression.1 Then, a series of studies around the world focused on the occurrence of depression in diabetic patients or the development of diabetes due to depression and most authors agree that the relationship between depression and diabetes is a reciprocal relationship.2,3 Results from the World Mental Health survey showed that the rate of depression is higher in people with diabetes than in people without diabetes.4
The cause and mechanism of depression in T2DM are not fully understood so far. There are two main hypotheses about whether depression occurs or recurrence in T2DM. Firstly, depression is the result of birth defects. Many studies have reported the general biological background between diabetes and depression.5,6 Alteration of the hypothalamic–pituitary–adrenal axis, such as increased cortisol production in depressed patients, is also observed in diabetics.7 Metabolic disorders of neurotransmitters, especially norepinephrine and serotonin in depressed patients, are also observed in diabetics.8,9 Secondly, depression is a consequence of psychosocial factors related to diabetes. Some studies suggest that depression is associated with difficulty in liking with suspected complications in diabetics.8,10,11 There was a relationship between pathological variables (such as inactivity) and indirect depression through the perception of the harmful effects of diabetes mellitus.12
Depression that occurs in a person with diabetes can have serious consequences both on the physical and mental side of the patient.2,13 Depression makes people with diabetes less physically active, easily abuses alcohol and tobacco, has poor eating habits, and poor adherence to diabetes treatment regimens.11,14 Studies have demonstrated that depression increases the risk of persistent hyperglycemia, increases vascular complications and mortality.15,16 As a result, the patient’s quality of life and the economic burden associated with diabetes become more severe.17–19 Clinically, depression is commonly diagnosed based on diagnostic criteria, questions, or scales to assess depression, such as the International Classification of Diseases tenth revision (ICD-10) depression diagnostic standard, the Patient Health Questionnaire-9 (PHQ-9), Beck’s depression detection scale, Hamilton Depression Rating Scale, and Montgomery Asberg Depression Rating Scale, in which PHQ-9 is considered a short and reliable questionnaire that has been studied and applied in many countries around the world to screen and evaluate depression.20,21 The PHQ-9 is not only suitable for screening for major depressive stages in the community22 but also reliable to diagnose depressive disorders in adults.23
In Vietnam, T2DM accounts for about 5.4–6.0% of the population and continues to increase. Patients face many health problems at the same time, both physical and psychological, the complications of the disease, and the increasing cost of treatment. Therefore, it has a significant effect on the mental health of the patient. To the best of our knowledge, there are very few studies on depression in patients with T2DM who are of working age, so we implemented this study with the aim: to determine the rate of depression and the association between depression and multifactorial control and microvascular complications in outpatient with T2DM aged 30–60 years old.
Materials and Methods
Study Population and Design
Study subjects include all outpatients diagnosed with T2DM according to the American Diabetes Association (ADA 2014) criteria aged from 30 to 60 years old at the Medical Examination Service, Bach Mai Hospital, Hanoi, Vietnam. Exclusion criteria included other types of diabetes (type 1 diabetes, gestational diabetes, specific types of diabetes based on ADA 2014 classification), T2DM with a combination of advanced cancer and other life-threatening conditions, patients are experiencing acute complications (such as ketoacidosis coma, hyperosmolar coma, acute hypoglycemic coma, septic shock, sepsis), abnormal thyroid function, and patients diagnosed with a psychiatric disorder prior to the onset of diabetes or being treated for mental illness. All patients were explained about the study procedure and were given two identical informed consents. One copy was kept by the patient and one was kept by the research team.
The sample size (n) of 231 patients with T2DM was calculated according to the “estimate a population proportion” formula used for qualitative analysis in descriptive and analytical research as follows: n = [Z2(1-α/2) x p(1 – p)]/∆2, where p = 0.183 is the rate of depression in the population of patients with T2DM using the PHQ-9 questionnaire in Zhang’s study in 2013, in Hong Kong,24 Z2(1-α/2) = 1.96 is the value corresponding to α = 0.05 and ∆ is the desired deviation between the rate obtained from our study sample and p of 0.183 of the previous study population. In our study, ∆ = 0.05.
Study Protocol
The following steps were carried out on the day of examination: administrative information (name, age, gender, address, and occupation), previous medical history and current diseases, examination for clinical signs and symptoms and diabetic complications, laboratory tests, and questionnaire PHQ-9.
We used PHQ-9 to detect symptoms and evaluate depression.25 Briefly, patients sat in a quiet private room with an imposing seriousness, openness, and friendliness on the same day with the clinical and paraclinical examination. An experimenter explained carefully and thoroughly for patients to understand each question in PHQ-9. Patients were given enough time to think and answer each question. The experimenter gave points to each reply from patients and summed up all the points. According to PHQ-9: 0–4 points: no depression; 5–9 points: mild depression; 10–14 points: moderate depression; 15–19 points: moderate-severe depression; and 20–27 points: severe depression.
Blood tests were performed at the medical examination and treatment department at the Bach Mai Hospital: blood collection techniques and testing comply with Bach Mai hospital’s procedures. Fasting venous blood samples were taken early in the morning and then were used to measure blood glucose, HbA1c, total cholesterol, triglyceride, HDL-C, and LDL-C by the Roche Cobas 6000 automated biochemistry machine. Twenty-four-hour urine samples were collected on the same day and were used to measure albuminuria by enzymatic turbidimeter autoanalyzer.
Patients were considered to have diabetic microvascular complications when one of the following abnormalities was present: kidney damage with microalbuminuria measurement >30 mg/24 hours;26 ophthalmoscopy showing proliferative or pre-proliferative retinopathies diagnosed by an ophthalmologist; peripheral neuropathies based on the UK screening test (UKST) >2 points.27
Ethical Statement
All patients provided written informed consent and agreed to participate in this study. The protocol was approved by the Institutional Review Board of the Hanoi Medical University, Hanoi, Vietnam (No.3788/QĐ-ĐHYHN). The study was also conducted using good clinical practice following the Declaration of Helsinki.
Statistical Analysis
All results are presented as mean (SD) or, if skewed, as median (interquartile range) for the continuous variables, and as a percentage for categorical variables. Differences between groups were examined with Student’s t-test or Mann–Whitney’s test. The chi-square test or fisher’s exact test of association is used to discover if there is a relationship between two categorical variables. The relationships between indicators of depression (or PHQ-9) and other factors were determined using univariable linear regression and multivariable linear regression. Pearson’s r and standardized B were calculated for the correlation between PHQ-9 indices and variables (such as age, gender, treatment therapy, and HbA1c control). The Kruskal–Wallis H-test was used to determine if there are statistically significant differences between the three groups of treatment options on the PHQ9-score. A p-value <0.05 was considered statistically significant. Data were processed using SPSS software version 26 (64-bit) for Window (SPSS Inc., Chicago, IL).
Results
The median age of the study group was 52 years; the percentage of patients who achieved the target goal of the factors was as follows: 48.9% for BMI <23 kg/m2, 77.5% for accepted control for blood pressure, 29.0% for glucose, 44.6% for HbA1c, 42.0% for triglycerides, 50.6% for total cholesterol, 79.2% for HDL-C, and 72.6% for LDL-C; the rate of accepted control of triglycerides and HDL-C were significantly higher in women than those in men (p < 0.05); the rate of newly diagnosed patients without treatment was 18.2%, the rate of patients with lifestyle modification in combination with oral antihyperglycemic agents was 71.9%, the rate of patients using insulin was 10.0%; the rate of patients with microvascular complications was 15.6% and there was no difference between men and women (p > 0.05) (Table 1).
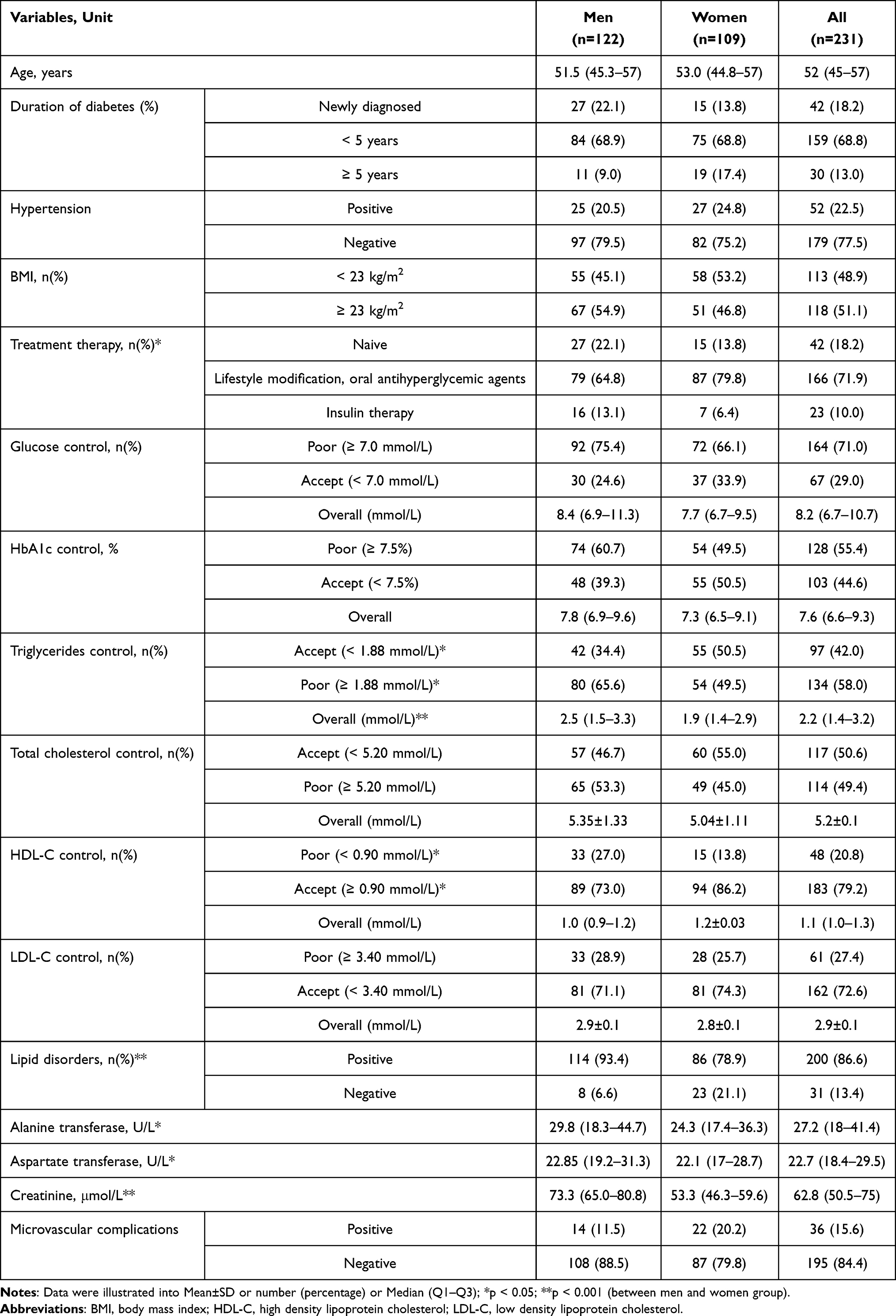 |
Table 1 The Demographic and Biomedical Characteristics of the Study Population |
The rate of depression in patients with type 2 diabetes was 16.9%. Of which, mild depression accounted for 15.2%, moderate depression made up 1.7%, and no serious depression. The prevalence of depression was higher in female patients than in male patients (p = 0.049). The percentage of depression among male patients was 12.3%, whilst it was 22.0% among female patients. The degree of depression and PHQ-9 scores were not statistically different between men and women (p > 0.05) (Table 2).
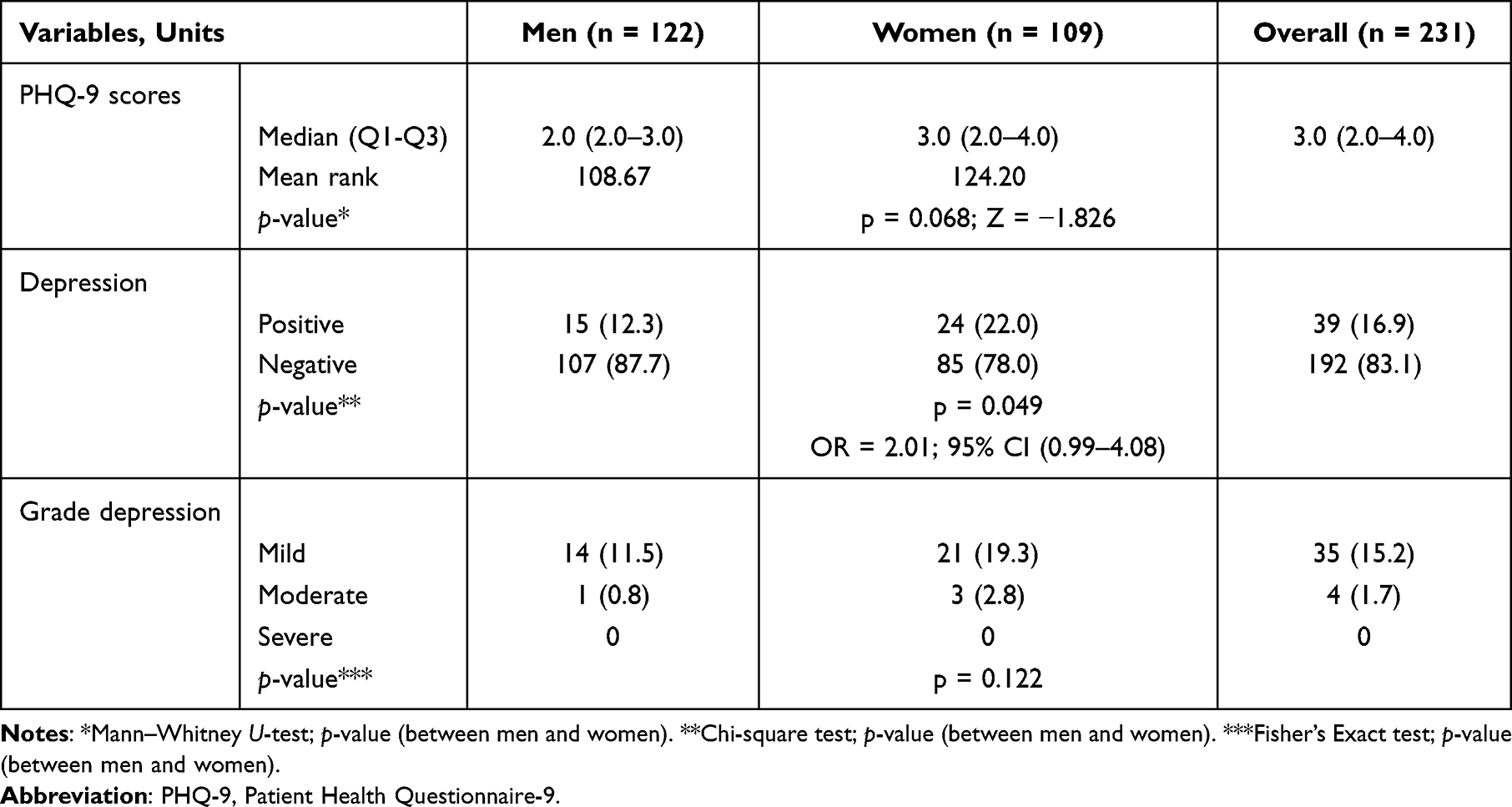 |
Table 2 The Prevalence of Depression in Type 2 Diabetes Mellitus Aged 30–60 Years |
There was a statistically significant difference in the rate of depression by age group (p = 0.026), duration of diabetes (p = 0.001) and treatment method for T2DM (p = 0.002). Poor control of HbA1c and present microvascular complications increased the risk of developing depression (OR = 2.37, 95% CI 1.11–5.02, p = 0.033 and OR = 2.62, 95% CI 1.15–5.93, p = 0.027); The rate of depression was not statistically significant compared with the control levels of blood pressure, BMI, blood lipids, and glucose (p > 0.05) (Table 3).
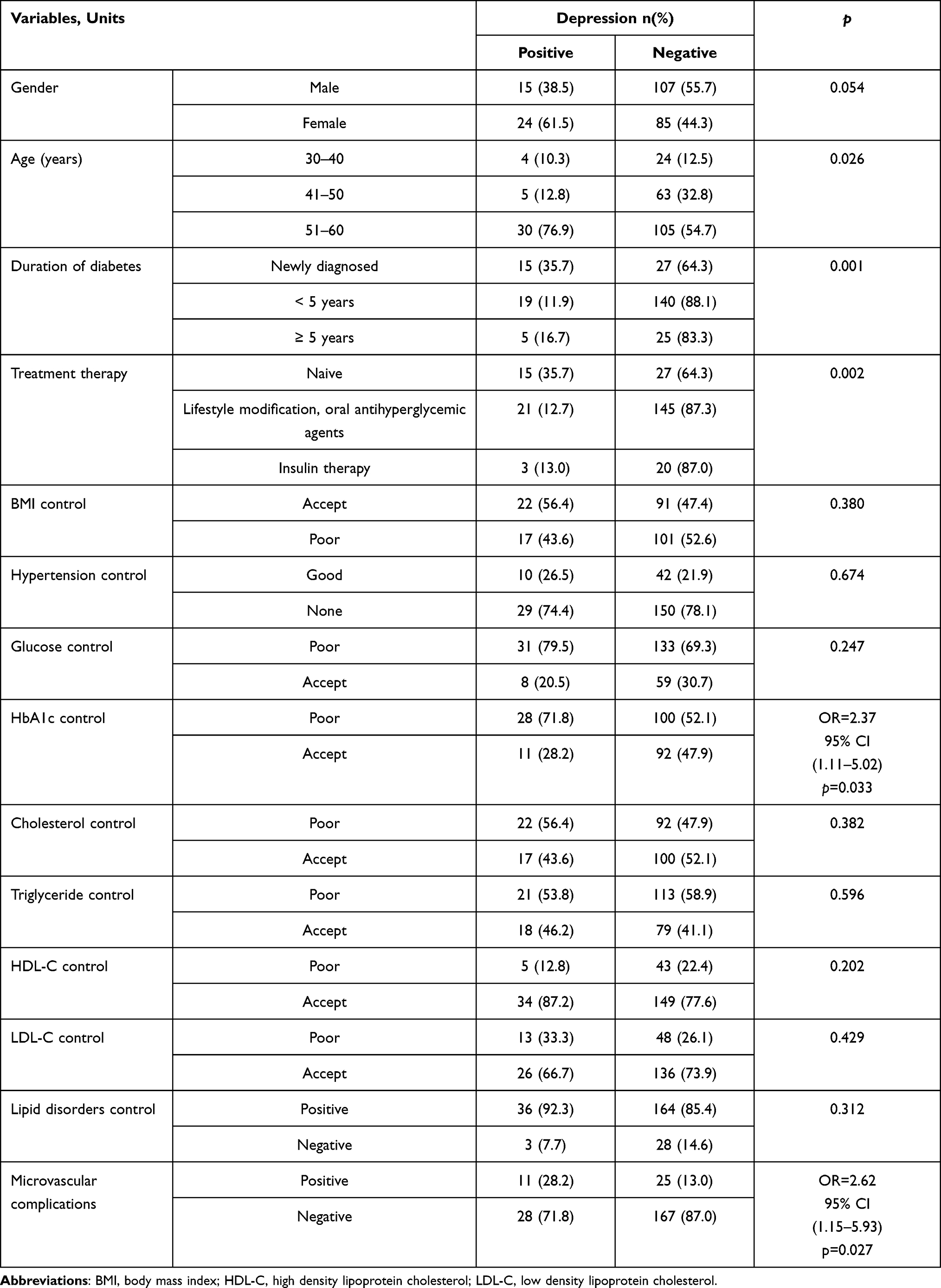 |
Table 3 Relationship Between Depression and Multifactor and Microvascular Complications in Patients with Type 2 Diabetes |
When the multivariate analysis was performed, it was shown that sex, treatment for glycemic control, and microvascular complications had a statistically significant influence on the PHQ-9 score. Regarding therapeutic options, patients without any antihyperglycemic intervention tended to have higher PHQ-9 scores than those treated with insulin (p = 0.01) (Table 4).
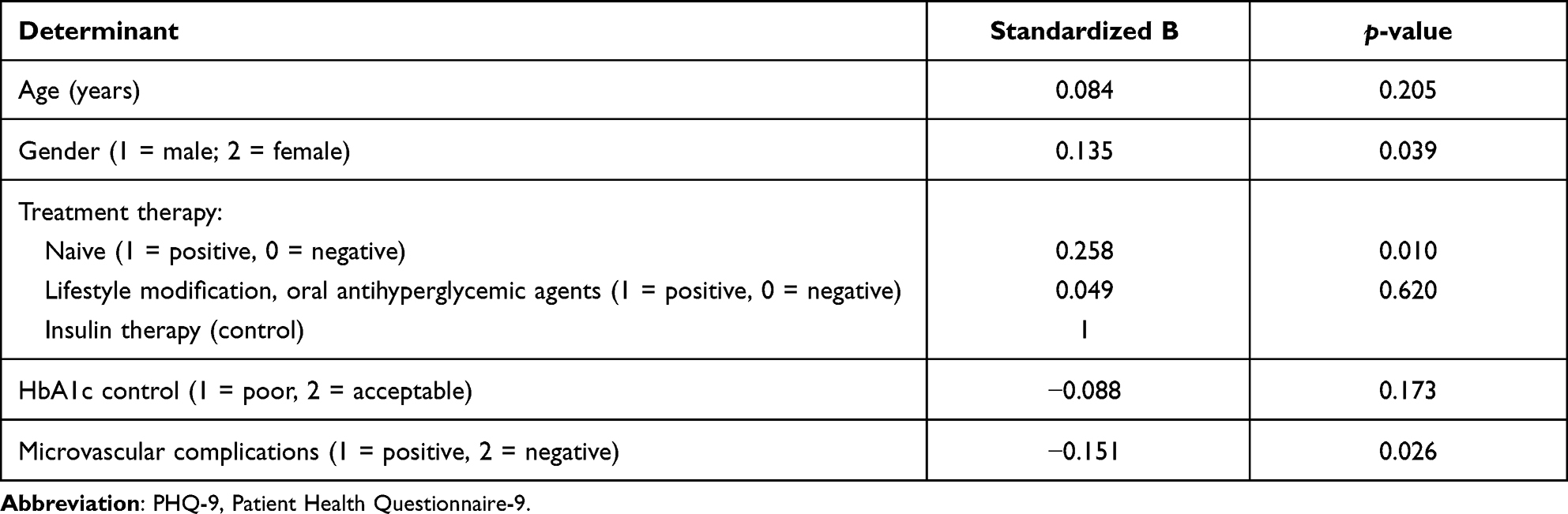 |
Table 4 Multivariate Linear Regression Between PHQ-9 Scores and Age, Gender, Treatment Therapy, HbA1c Control and Microvascular Complications |
Discussion
The Prevalence of Depression in T2DM at Working Age
We screened and assessed depression using the PHQ-9 questionnaire on 231 patients with T2DM, showing that the number of patients with depression was 16.9%. In which mild depression made up 15.2%, moderate depression accounted for 1.7%, and no patient had a serious level. A World Health Survey, which estimated the prevalence of depression (based on ICD-10 diagnostic criteria) in 245,404 people in 60 countries from various regions of the world, results showed that in one year, the rate of a single depressive episode was 3.2% and the rate of depression in people with diabetes was 9.3%.28 Another study, which combined 10 controlled studies with a total of 51,331 people, found that the rate of depression in subjects with T2DM was 17.6% and this rate in subjects without diabetes was 9.8%, the rate of depression in women was higher than in men with diabetes.29 A study in a rural community in Pakistan showed that the rate of depression in diabetes patients was 14.7% and 4.9% of people without diabetes.30 In Hong Kong, China in 2013, the rate of depression in T2DM outpatients surveyed by the PHQ-9 questionnaire was 18.3%.24 The rate of patients with depression was in T2DM patients in this study tended to be lower in Vietnam than in many other studies, this may be due to the difference in age of the patients participating in the survey and the unique characteristics of the conditions of society. Currently, in Vietnam, the situation of diabetes control has been receiving more and more attention from the Government with large-scale action programs nationwide, such as that diabetic patients are provided with anti-diabetic drugs, educated of basic understandings of diabetes, counseled on nutrition issues and treatment methods and shared from family and community.
The results of this study also showed that the prevalence of T2DM at working age was lower than that compared with other age groups. The study of patients with T2DM showed that patients who were over 60 years old had a higher rate of depression (higher than other age groups).31 In Vietnam, a study showed that the rate of depression in T2DM patients aged 18 years and older in Hue city was 23.2%,32 while the proportion of patients with signs of depression susceptibility in elderly patients with T2DM was 79.4%.33 The more they are aging, the more adverse factors they will have to face such as difficulty in controlling blood glucose, increasing chronic complications, increasing treatment costs, other pressures from social families.8,29
In our study, the rate of depression in the patients with newly diagnosed T2DM was the highest (35.7%). The effect of the duration of diabetes on depression varies by a study.34,35 Patients with newly diagnosed T2DM have not been consulted for treatment, but they are often confused, worried, and scared about the disease, considering it was a dangerous and uncured disease they had to adopt and adapt for the rest of their lives, leaving economical and psychological consequences.
The Relationship Between Depression and Multifactorial Control and Microvascular Complications Patients with T2DM
The results of our study showed that the percentage of depression was different among patients stratified by diabetes treatments, in which the depression rate was the highest in the group of patients who had not been treated for diabetes. Previous studies showed that patients with diabetes treated with oral drugs had lower depression scores than patients using insulin.31,36 However, in our study, we studied subjects aged from 30 to 60 years old. The majority of patients were controlled blood glucose by lifestyle modifies, adjusting their diet, and using oral drugs (71.9%), the proportion of patients using insulin was very low (10.0%) so the effect of insulin usage on depression could not be assessed. Besides, for the youngest subjects, especially working-age people with diabetes, in addition to worrying about the disease, having to regularly take medicine and visit medical facilities was also a big challenge, which even made them drop out of diabetes treatment. As a result, the rate of depression in this group was quite high.
When considering the association between multifactorial control (glucose, BMI, lipid profiles, and blood pressure) and depression, we found that the percentage of patients whose control level reached the goal of glucose was quite low (29.0%), that of HbA1c was 44.6% and the poor control of HbA1c increased the risk of depression significantly (OR = 2.37, p = 0.033), while the rate of control reached the goal of other factors, such as blood pressure, blood lipids achieved higher goals. In fact, the relationship between poor blood glucose control and depression has a reciprocal nature: people with depression often experience behaviors of fatigue, depression, eating, living in moderation, even they do not adhere to treatment easily lead to difficulty in controlling blood glucose.37 In contrast, diabetic patients with poor blood glucose control had a higher risk of depression due to the presence of more metabolic stress as well as anxiety about their medical status.38–40 T2DM is characterized by concomitant insulin resistance and hyperglycemia, and both have the potential to induce systemic inflammation, which in turn releases cytokines including tumor necrosis factor (TNF)-α, interferon (INF)-γ, interleukin (IL)-2, IL-4, IL-8, IL-10, and IL-12. These cytokines may induce depressive symptoms through effects on monoamines and other neurotransmitters, effects on neuroplasticity, effects on the hypothalamic–pituitary–adrenal system.41,42
Both univariate and multivariate analyses showed that patients with T2DM with microvascular complications were at increased risk for depression. And patients without any antihyperglycemic intervention had higher PHQ-9 scores than those treated with insulin. Previous studies have shown that the presence of microvascular complications increases the risk of depression.29,43,44 Psychological stress increases sharply in the first two years after patients have concomitant retinopathy, and retinopathy is an important risk factor for increased rates of depression in patients with T2DM.45 There is an association between diabetic neuropathy and anxiety and depression degree through perceptions of diabetic neuropathy symptom unpredictability and the lack of treatment control and restrictions in activities of daily living and changes in social self-perception.46 Renal disease progression may be associated with increased risk and severity of depression, albuminuria being more strongly associated with depression than glomerular filtration rate.47
There were some limitations of our study. This study was implemented on a relatively small sample size. Besides, we had not been able to associate between the social factors and depression of the participants.
Conclusion
The prevalence of depression in patients aged 30–60 years with T2DM in Vietnam is 16.9%. Regarding the severity of depression, mild depression accounts for 15.2%, moderate depression makes up 1.7%. Diabetes management, HbA1c control, and microvascular complications have a statistically significant effect on the rate of depression.
Abbreviations
T2DM, type 2 diabetes mellitus; PHQ-9, Patient Health Questionnaire-9; ICD-10, international classification of diseases tenth revision; BMI, body mass index; SD, standard deviation; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; OR, odds ratio; CI, confidence interval.
Acknowledgments
We thank the staff in the Medical Examination Service, Bach Mai Hospital, Hanoi, Vietnam for collecting the samples and supporting the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
References
1. Willis T. Pharmaceutice Rationalis Sive Diabtriba de Medicamentorum Operantionibus in Humano Corpore. Oxford; 1675.
2. Mezuk B, Eaton WW, Albrecht S, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care. 2008;31:2383–2390. doi:10.2337/dc08-0985
3. Golden SH. Examining a bidirectional association between depressive symptoms and diabetes. JAMA. 2008;299(23):2751. doi:10.1001/jama.299.23.2751
4. Lin EHB, Von Korff M. Mental disorders among persons with diabetes—results from the world mental health surveys. J Psychosom Res. 2008;65:571–580. doi:10.1016/j.jpsychores.2008.06.007
5. Champaneri S, Wand GS, Malhotra SS, Casagrande SS, Golden SH. Biological basis of depression in adults with diabetes. Curr Diab Rep. 2010;10:396–405. doi:10.1007/s11892-010-0148-9
6. Golden S. A Review of the evidence for a neuroendocrine link between stress, depression and diabetes mellitus. Curr Diabetes Rev. 2007;3:252–259. doi:10.2174/157339907782330021
7. Stetler C, Miller GE. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom Med. 2011;73:114–126.
8. Talbot F, Nouwen A. A review of the relationship between depression and diabetes in adults: is there a link? Diabetes Care. 2000;23:1556–1562. doi:10.2337/diacare.23.10.1556
9. Boland R. Depression in medical illness (secondary depression). In: Stein DJ, Kupfer DJ, editors. The American Psychiatric Publishing Textbook of Mood Disorders. American Psychiatric Publishing, Inc; 2006:639–652.
10. Peyrot M, Rubin RR. Persistence of depressive symptoms in diabetic adults. Diabetes Care. 1999;22:448–452. doi:10.2337/diacare.22.3.448
11. Kanter JW, Busch AM, Weeks CE, Landes SJ. The nature of clinical depression: symptoms, syndromes, and behavior analysis. Behav Anal. 2008;31:1–21. doi:10.1007/BF03392158
12. Cakmak S. Relationship between quality of life, depression and anxiety in type 1 and type 2 diabetes. Dusunen Adam J Psychiatry Neurol Sci. 2020. doi:10.14744/DAJPNS.2020.00075
13. Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat. 2011;3. doi:10.2147/NDT.S19617
14. Knol MJ, Twisk JWR, Beekman ATF, et al. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia. 2006;49:837–845. doi:10.1007/s00125-006-0159-x
15. Otieno F, Kanu J, Karari E, et al. Glucose-lowering therapies, adequacy of metabolic control, and their relationship with comorbid depression in outpatients with type 2 diabetes in a tertiary hospital in Kenya. Diabetes Metab Syndr Obes Targets Ther. 2017;10:141–149. doi:10.2147/DMSO.S124473
16. Ahmadieh H, Itani H, Itani S, et al. Diabetes and depression in Lebanon and association with glycemic control: a cross-sectional study. Diabetes Metab Syndr Obes Targets Ther. 2018;11:717–728. doi:10.2147/DMSO.S179153
17. Egede LE. Effect of comorbid chronic diseases on prevalence and odds of depression in adults with diabetes. Psychosom Med. 2005;67:46–51. doi:10.1097/01.psy.0000149260.82006.fb
18. Egede LE, Walker RJ, Bishu K, Dismuke CE. Trends in costs of depression in adults with diabetes in the United States: medical expenditure panel survey, 2004–2011. J Gen Intern Med. 2016;31:615–622. doi:10.1007/s11606-016-3650-1
19. Ding X, Rong S, Wang Y, et al. The association of the prevalence of depression in type 2 diabetes mellitus with visual-related quality of life and social support. Diabetes Metab Syndr Obes Targets Ther. 2022;15:535–544. doi:10.2147/DMSO.S343926
20. Gelaye B, Williams MA, Lemma S, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210:653–661. doi:10.1016/j.psychres.2013.07.015
21. Kocalevent RD, Hinz A, Brähler E. Standardization of the depression screener Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2013;35:551–555. doi:10.1016/j.genhosppsych.2013.04.006
22. Santos IS, Tavares BF, Munhoz TN, et al. Sensibilidade e especificidade do Patient Health Questionnaire-9 (PHQ-9) entre adultos da população geral. Cad Saude Publica. 2013;29:1533–1543. doi:10.1590/S0102-311X2013001200006
23. van Steenbergen-Weijenburg KM, de Vroege L, Ploeger RR, et al. Validation of the PHQ-9 as a screening instrument for depression in diabetes patients in specialized outpatient clinics. BMC Health Serv Res. 2010;10:235. doi:10.1186/1472-6963-10-235
24. Zhang Y, Ting R, Lam M, et al. Measuring depressive symptoms using the patient health questionnaire-9 in Hong Kong Chinese subjects with type 2 diabetes. J Affect Disord. 2013;151:660–666. doi:10.1016/j.jad.2013.07.014
25. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9 validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
26. Weir MR. Microalbuminuria in type 2 diabetics: an important, overlooked cardiovascular risk factor. J Clin Hypertens. 2004;6:134–143. doi:10.1111/j.1524-6175.2004.02524.x
27. Oguejiofor OC, Odenigbo CU, Oguejiofor CBN. Evaluation of the effect of duration of diabetes mellitus on peripheral neuropathy using the United Kingdom screening test scoring system, bio-thesiometry and aesthesiometry. Niger J Clin Pract. 2010;13:240–247.
28. Moussavi S, Chatterji S, Verdes E, et al. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370:851–858. doi:10.1016/S0140-6736(07)61415-9
29. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of co-morbid depression in adults with type 2 diabetes: a systematic review and meta-analysis. Diabet Med. 2006;23:1165–1173. doi:10.1111/j.1464-5491.2006.01943.x
30. Zahid N, Asghar S, Claussen B, Hussain A. Depression and diabetes in a rural community in Pakistan. Diabetes Res Clin Pract. 2008;79:124–127. doi:10.1016/j.diabres.2007.07.006
31. Joseph N, Unnikrishnan B, Raghavendra Babu Y, Kotian MS, Nelliyanil M. Proportion of depression and its determinants among type 2 diabetes mellitus patients in various tertiary care hospitals in Mangalore city of South India. Indian J Endocrinol Metab. 2013;17:681. doi:10.4103/2230-8210.113761
32. Tran NMH, Nguyen QNL, Vo TH, Le TTA, Ngo NH. Depression among patients with type 2 diabetes mellitus: prevalence and associated factors in Hue City, Vietnam. Diabetes Metab Syndr Obes Targets Ther. 2021;14:505–513. doi:10.2147/DMSO.S289988
33. Vu HTT, Nguyen TX, Nguyen HTT, et al. Depressive symptoms among elderly diabetic patients in Vietnam. Diabetes Metab Syndr Obes Targets Ther. 2018;11:659–665. doi:10.2147/DMSO.S179071
34. Khuwaja AK, Lalani S, Dhanani R, et al. Anxiety and depression among outpatients with type 2 diabetes: a multi-centre study of prevalence and associated factors. Diabetol Metab Syndr. 2010;2:72. doi:10.1186/1758-5996-2-72
35. Miyaoka Y, Miyaoka H, Motomiya T, Kitamura SI, Asai M. Impact of sociodemographic and diabetes-related characteristics on depressive state among non-insulin-dependent diabetic patients. Psychiatry Clin Neurosci. 1997;51:203–206. doi:10.1111/j.1440-1819.1997.tb02583.x
36. Rahman M, Rahman A. Depression and associated factors in diabetic patients attending an urban hospital of Bangladesh. Int J Collab Res Intern Med Public Heal. 2015;3:65–76.
37. Holt RIG, de Groot M, Golden SH. Diabetes and depression. Curr Diab Rep. 2014;14:491. doi:10.1007/s11892-014-0491-3
38. Alonso-Morán E, Satylganova A, Orueta JF, Nuño-Solinis R. Prevalence of depression in adults with type 2 diabetes in the Basque Country: relationship with glycaemic control and health care costs. BMC Public Health. 2014;14:769. doi:10.1186/1471-2458-14-769
39. Téllez-Zenteno JF, Cardiel MH. Risk factors associated with depression in patients with type 2 diabetes mellitus. Arch Med Res. 2002;33:53–60. doi:10.1016/S0188-4409(01)00349-6
40. Ganasegeran K, Renganathan P, Manaf RA, Al-Dubai SAR. Factors associated with anxiety and depression among type 2 diabetes outpatients in Malaysia: a descriptive cross-sectional single-centre study. BMJ Open. 2014;4:e004794. doi:10.1136/bmjopen-2014-004794
41. Stuart MJ, Baune BT. Depression and type 2 diabetes: inflammatory mechanisms of a psychoneuroendocrine co-morbidity. Neurosci Biobehav Rev. 2012;36:658–676. doi:10.1016/j.neubiorev.2011.10.001
42. Edwards KM, Bosch JA, Engeland CG, Cacioppo JT, Marucha PT. Elevated Macrophage Migration Inhibitory Factor (MIF) is associated with depressive symptoms, blunted cortisol reactivity to acute stress, and lowered morning cortisol. Brain Behav Immun. 2010;24:1202–1208. doi:10.1016/j.bbi.2010.03.011
43. Lin EHB, Rutter CM, Katon W, et al. Depression and advanced complications of diabetes: a prospective cohort study. Diabetes Care. 2010;33:264–269. doi:10.2337/dc09-1068
44. Eren MA, et al. The relationship between microvascular complications and depression in patients with type 2 diabetes mellitus who use insulin. J Clin Exp Investig. 2013;4. doi:10.5799/ahinjs.01.2013.01.0230
45. Rees G, et al. Association between diabetes-related eye complications and symptoms of anxiety and depression. JAMA Ophthalmol. 2016;134(9):1007–1014. doi:10.1001/jamaophthalmol.2016.2213
46. Vileikyte L, et al. Diabetic peripheral neuropathy and depressive symptoms: the association revisited. Diabetes Care. 2005;28:2378–2383.
47. Takasaki K, Babazono T, Ishizawa K, Miura J, Uchigata Y. Relationship between diabetic nephropathy and depression: a cross-sectional analysis using the Diabetes Study from the Center of Tokyo Women’s Medical University (DIACET). BMJ Open Diabetes Res Care. 2016;4:e000310. doi:10.1136/bmjdrc-2016-000310
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.