Back to Journals » Journal of Inflammation Research » Volume 19
The Relationship Between Decreased Serum Klotho Protein and Cognitive Impairment in Patients After Abdominal Surgery
Received 3 January 2026
Accepted for publication 25 March 2026
Published 17 April 2026 Volume 2026:19 593405
DOI https://doi.org/10.2147/JIR.S593405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xuehui Li,1 Feng Ao2
1Department of Anesthesiology, Sijing Hospital, Shanghai, 201601, People’s Republic of China; 2Department of General Surgery, Sijing Hospital, Shanghai, 201601, People’s Republic of China
Correspondence: Feng Ao, Department of General Surgery, Sijing Hospital, No. 389, Sitong Road, Songjiang District, Shanghai, 201601, People’s Republic of China, Tel +86-18918221730, Email [email protected]
Background: Postoperative cognitive dysfunction (POCD) is a common complication in elderly patients undergoing abdominal surgery; however, reliable biomarkers for its early identification are limited. Klotho, an anti-aging protein with neuroprotective and anti-inflammatory properties, may play a role in POCD development. This study investigated the association between serum Klotho levels and POCD, as well as their relationships with inflammation and cognitive outcomes.
Methods: A total of 93 patients undergoing abdominal surgery were enrolled and classified into non-POCD (n = 59) and POCD (n = 34) groups based on their postoperative Montreal Cognitive Assessment (MoCA) scores. Serum Klotho, C-reactive protein (CRP), interleukin (IL)-1β, and IL-6 levels were measured preoperatively and postoperatively. Multivariate logistic regression, receiver operating characteristic (ROC) curve analysis, and Pearson correlation analyses were performed to evaluate associations and predictive value.
Results: Patients who developed POCD had significantly longer durations of anesthesia than those without POCD (all P < 0.001). While preoperative Klotho levels were comparable between the groups, postoperative serum Klotho levels were significantly reduced in the POCD group (561.07 ± 59.27 vs. 654.66 ± 94.63 pg/mL, P < 0.001). Multivariate analysis identified age (odds ratio [OR] = 1.101, 95% confidence interval [CI] = 1.009– 1.201, P = 0.031) and anesthesia duration (OR = 1.059, 95% CI = 1.011– 1.109, P = 0.015) as independent risk factors, whereas higher postoperative Klotho levels were independently associated with a reduced risk of poor outcomes (OR = 0.992, 95% CI = 0.985– 0.998, P = 0.016). Postoperative Klotho levels were negatively correlated with anesthesia duration and inflammatory markers (C-reactive protein, interleukin [IL]-1 β, and IL-6) (all P < 0.05) and positively correlated with postoperative MoCA scores (r = 0.45, P < 0.001). ROC analysis identified an optimal cutoff value of 630.2 pg/mL for Klotho in distinguishing POCD, demonstrating favorable diagnostic performance.
Conclusion: Decreased postoperative serum Klotho levels are closely associated with increased inflammation and cognitive impairment following abdominal surgery. Klotho may serve as a promising biomarker for the early identification of POCD and as a potential therapeutic target to improve postoperative cognitive outcomes.
Keywords: postoperative cognitive dysfunction, POCD, serum klotho, inflammation, abdominal surgery, montreal cognitive assessment, MoCA
Introduction
Postoperative cognitive dysfunction (POCD) is a common neurological complication following major surgery, particularly in elderly patients, and is characterized by impairments in memory, attention, and executive function that can persist for weeks or months after surgery. POCD is associated with prolonged hospitalization, reduced quality of life, and increased morbidity and mortality, imposing a substantial burden on patients and healthcare systems worldwide.1,2 Although advanced age, exposure to anesthesia, and surgical stress are recognized risk factors, the precise molecular mechanisms underlying POCD remain incompletely understood, and reliable circulating biomarkers for early identification and risk stratification are lacking.3,4
Abdominal surgery, including procedures such as gastrectomy, enterectomy, and colectomy, represents a significant physiological stressor that induces both local and systemic inflammatory responses. Surgical trauma leads to the release of proinflammatory cytokines, such as C-reactive protein (CRP), interleukin (IL)-1β, and IL-6, from damaged tissues and activated immune cells.5,6 These systemic inflammatory mediators can disrupt endothelial and blood-brain barrier integrity, promote neuroinflammation, and impair neuronal function, thereby contributing to cognitive decline in the postoperative period.7–9 The magnitude of the inflammatory response is influenced by factors, including the type and extent of surgery, duration of anesthesia, and patient age, which may explain the higher susceptibility of elderly patients to POCD.10,11
Klotho is an anti-aging protein predominantly expressed in the kidney and brain, and is detectable in circulation as a soluble form. It exerts pleiotropic protective effects, including anti-inflammatory, antioxidative, and neuroprotective functions.12,13 Experimental studies have demonstrated that Klotho enhances synaptic function, promotes neuronal resilience, and preserves cognitive performance, whereas Klotho deficiency accelerates cognitive decline and exacerbates neuroinflammation.14–16 Clinically, reduced circulating Klotho levels are associated with aging-related disorders, cardiovascular diseases, and neurodegenerative conditions, including cognitive impairment and dementia.17–19
Despite these findings, the relationship between serum Klotho levels and postoperative cognitive outcomes after abdominal surgery remains unclear. In particular, whether decreased circulating Klotho levels are associated with POCD and how they relate to inflammation and clinical indicators of cognitive function remains unknown. Therefore, this study aimed to investigate changes in serum Klotho levels in patients undergoing abdominal surgery, examine their association with POCD, and explore correlations between Klotho, inflammatory markers, and clinical parameters. Elucidating the role of Klotho in POCD may provide novel insights into the mechanisms underlying POC and identify potential biomarkers for early detection and therapeutic intervention.
Subjects and Methods
Study Population
This cross-sectional study included a total of 93 patients admitted to the Department of General Surgery at our hospital between January 2022 and December 2024. All patients underwent major abdominal surgery under general anesthesia and were prospectively enrolled in the study. The inclusion criteria were as follows: (i) age between 45 and 87 years and (ii) undergoing abdominal surgery under general anesthesia. The exclusion criteria were as follows: (i) language or communication difficulties; (ii) a history of neuropsychiatric diseases, such as depression or schizophrenia; (iii) serious cardiovascular or cerebrovascular diseases; (iv) inability or refusal to complete neuropsychological testing; and (v) a Montreal Cognitive Assessment (MoCA) score < 20. In addition, 80 age- and sex-matched control subjects were recruited from individuals undergoing routine health examinations during the same period. Control subjects had no history of major surgery, neurological, or psychiatric disorders, or cognitive impairment and were included solely for comparative analysis of serum Klotho levels. The study protocol was approved by the Research Ethics Committee of Sijing Hospital, and written informed consent was obtained from all participants prior to enrollment.
Anesthesia Management and Surgical Procedures
All participants underwent standard intraoperative monitoring, including noninvasive blood pressure, electrocardiography, pulse oximetry, body temperature, and depth of anesthesia monitored using the bispectral index (BIS). General anesthesia was induced with fentanyl, propofol, and cisatracurium and maintained with propofol, sevoflurane, sufentanil, and cisatracurium, in accordance with routine clinical practice. Mechanical ventilation parameters were adjusted to maintain normocapnia throughout the surgery. Hemodynamic parameters were maintained within 20% of the baseline values during the perioperative period.
Clinical Characteristics of the Patients
Baseline characteristics were recorded, including age, sex, body mass index (BMI), history of smoking or alcohol intake, hypertension, diabetes mellitus, and serum albumin levels. The indicators of abdominal surgery and anesthesia were recorded, including the ASA scale, surgery type (gastrectomy/enterectomy), surgery duration, and duration of anesthesia.
Measurement of Cognitive Function
The Montreal Cognitive Assessment (MoCA) was used to evaluate cognitive function in all patients.20 Preoperative MoCA assessment was performed one day before surgery. Postoperative MoCA assessment was conducted on postoperative day 3 under standardized conditions. The MoCA score ranges from 0 to 30, with higher scores indicating better cognitive performance. Postoperative cognitive dysfunction (POCD) was defined as a decline of > 1 standard deviation (SD) in the postoperative MoCA score compared with the individual preoperative baseline.21 In this cohort, the SD of postoperative MoCA scores was 2.11.
Measurement of Serum Biomarkers by ELISA
Serum levels of C-reactive protein (CRP), interleukin (IL)-1β, IL-6, and Klotho were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits, according to the manufacturers’ instructions. CRP (catalog no. SEKH-0138) and Klotho (catalog no. SEKH-0280) ELISA kits were purchased from Solarbio (Beijing, China), while IL-1β (catalog no. DLB50) and IL-6 (catalog no. D6050B) ELISA kits were obtained from R&D Systems (Minneapolis). Briefly, serum samples were collected, allowed to clot, and centrifuged to obtain the supernatants, which were stored at −80 °C until analysis. Before measurement, the samples were brought to room temperature and, when necessary, diluted to fall within the linear range of the standard curves. Standards and samples were added in duplicate to antibody-coated 96-well plates and incubated as specified by the manufacturers. After washing to remove unbound components, enzyme-linked detection antibodies were added, followed by the substrate solution. The reaction was terminated using a stop solution, and the absorbance was measured at 450 nm using a microplate reader. The concentrations of CRP, IL-1β, IL-6, and Klotho were calculated from standard curves generated using known concentrations of the recombinant proteins. All assays were performed in duplicate, and the mean values were used for statistical analysis.
Statistical Analysis
SPSS20.0 statistical software was used for data processing. Quantitative data were presented as the mean ± standard deviation (SD) and analyzed using the t-test, Mann–Whitney U-test between two groups, or one-way analysis of variance (ANOVA) with the LSD method for pairwise comparisons. Categorical data are presented as frequencies (percentages) and were analyzed using the chi-square test. The correlation between Klotho and other clinical indicators was analyzed using Pearson’s correlation test. The ROC curve was used to determine the cutoff point of serum Klotho levels between participants with and without POCD. Multivariate logistic regression analysis was used to determine the effect of serum Klotho levels on the risk of POCD; the results are presented as odds ratios, 95% confidence intervals (CIs), and P-values. Statistical significance was set at P < 0.05.
Results
Baseline Characteristics and Clinical Data of the Study Population
A total of 93 patients were included in the final analysis, of whom 59 were classified as non-POCD and 34 as POCD (Table 1). Patients who developed POCD were significantly older than those without POCD (76.38 ± 5.57 vs. 68.39 ± 9.21 years, P < 0.001). There were no significant differences between the two groups with respect to sex distribution, body mass index, smoking or drinking status, prevalence of hypertension or diabetes, American Society of Anesthesiologists (ASA) physical status, type of surgery, surgery duration, or preoperative serum albumin levels (all P > 0.05).
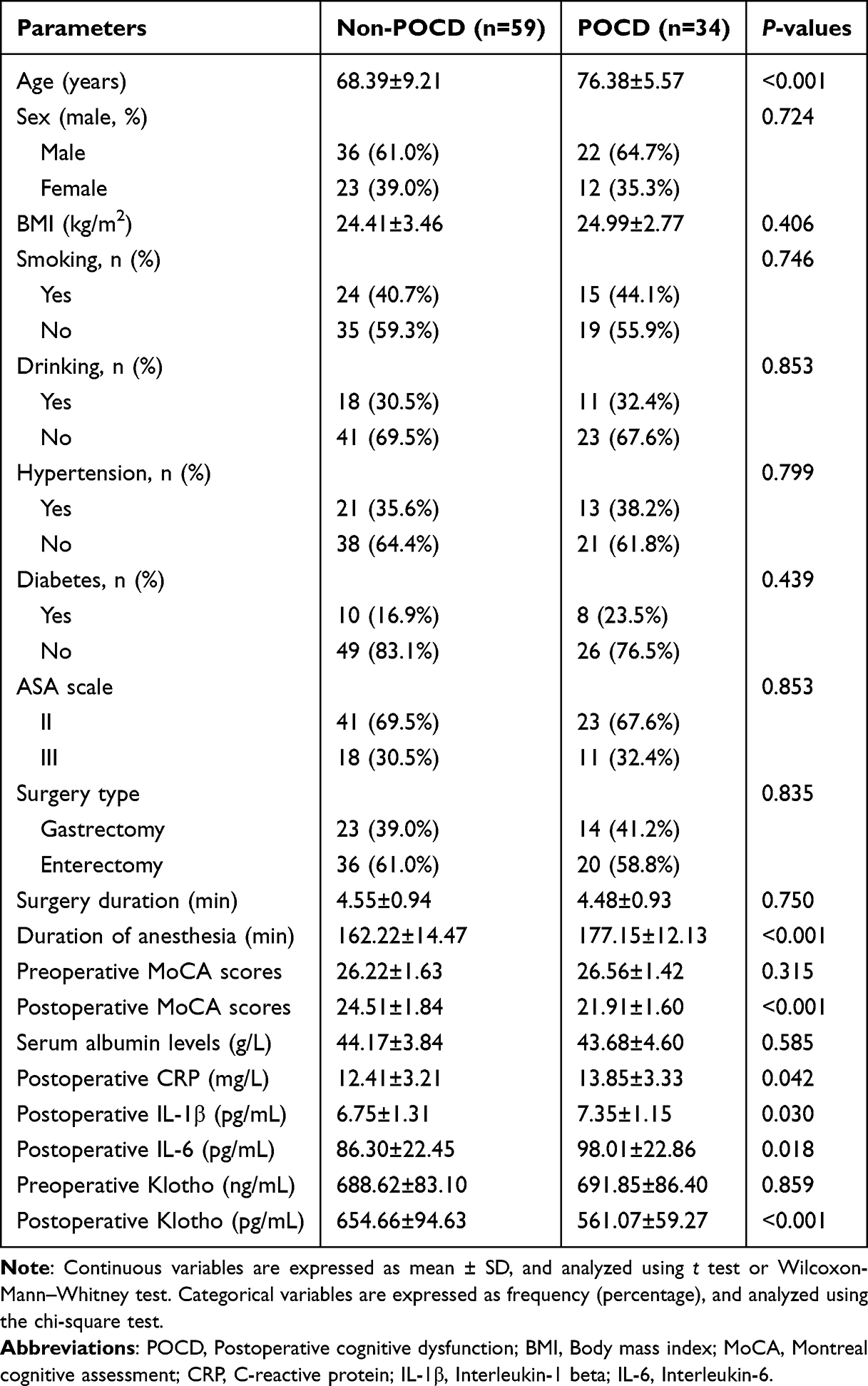 |
Table 1 Baseline Characteristics and Clinical Data of the Study Populations |
The duration of anesthesia was significantly longer in the POCD group than in the non-POCD group (177.15 ± 12.13 vs. 162.22 ± 14.47 min, P < 0.001). Preoperative Montreal Cognitive Assessment (MoCA) scores were comparable between the groups (P = 0.315), indicating similar baseline cognitive function. In contrast, postoperative MoCA scores were markedly lower in patients with POCD than in those without POCD (21.91 ± 1.60 vs. 24.51 ± 1.84, P < 0.001).
Regarding inflammatory markers, postoperative serum levels of CRP, IL-1β, and IL-6 were significantly higher in the POCD group than in the non-POCD group (all P < 0.05). Preoperative serum Klotho levels did not differ significantly between the groups (P = 0.859). However, postoperative serum Klotho levels were significantly lower in patients with POCD than in those without non-POCD patients (561.07 ± 59.27 vs. 654.66 ± 94.63 pg/mL, P < 0.001), suggesting an association between decreased postoperative Klotho levels and the development of POCD.
Multivariate Logistic Regression Analysis of Factors Associated with Poor Prognosis in OA Patients
Multivariate logistic regression analysis identified several independent predictors associated with poor prognosis in patients with OA (Table 2). Increasing age was significantly associated with a higher risk of poor outcomes (odds ratio [OR] = 1.101, 95% confidence interval [CI]: 1.009–1.201, P = 0.031), indicating that each additional year of age increased the likelihood of poor prognosis. Similarly, a longer duration of anesthesia was found to be an independent risk factor (OR = 1.059, 95% CI: 1.011–1.109, P = 0.015), suggesting that prolonged exposure to anesthesia may adversely affect postoperative recovery. In contrast, higher postoperative serum Klotho levels were significantly associated with a reduced risk of poor prognosis (OR = 0.992, 95% CI: 0.985–0.998, P = 0.016), indicating a potential protective effect. Specifically, each unit increase in postoperative Klotho was associated with a decrease in the odds of poor outcomes. Overall, these findings suggest that advanced age and prolonged anesthesia duration are independent risk factors, whereas elevated postoperative Klotho levels may serve as a protective biomarker for prognosis in patients with OA.
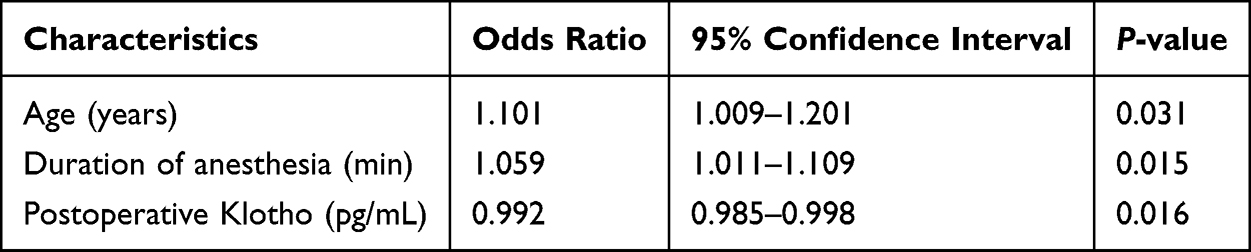 |
Table 2 Logistic Multivariate Regression for Poor Prognosis of OA Patients |
Serum Klotho Levels and Their Diagnostic Value for POCD
Serum Klotho levels were compared among control subjects and patients after abdominal surgery with or without postoperative cognitive dysfunction (POCD). As shown in Figure 1A, one-way analysis of variance (ANOVA) revealed a significant difference in serum Klotho concentrations among control subjects (n = 80), postoperative patients with normal cognition (non-POCD, n = 59), and patients with POCD (n = 34) (P < 0.001). Post hoc analyses demonstrated that serum Klotho levels were significantly reduced in patients with POCD compared to both control subjects and non-POCD patients, whereas no significant difference was observed between control subjects and non-POCD patients.
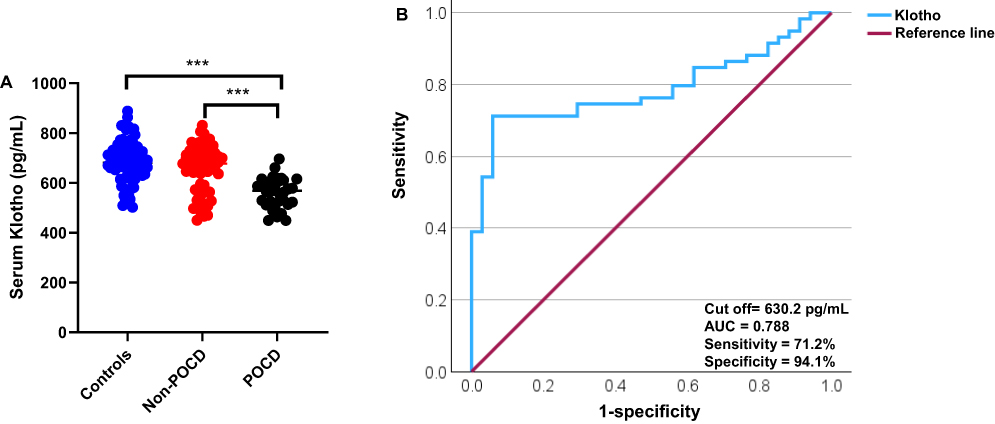 |
Figure 1 Serum Klotho levels in control subjects and patients after abdominal surgery. (A) Comparison of serum Klotho levels between control subjects (n=80), patients after abdominal surgery with normal cognition (Non-POCD, n=59), and patients after abdominal surgery declined cognition (POCD, n=34). ANOVA was applied. (B) The ROC curve was used to obtain the optimal cut-off value of serum Klotho (630.2 pg/mL) that distinguishes the patients after abdominal surgery with POCD from patients without POCD. ***P<0.001. |
To further evaluate the discriminative ability of serum Klotho levels in identifying POCD, a receiver operating characteristic (ROC) curve analysis was performed (Figure 1B). ROC analysis yielded an optimal cutoff value of 630.2 pg/mL for serum Klotho levels to distinguish patients with POCD from those without POCD. At this threshold, serum Klotho exhibited favorable diagnostic performance, indicating that decreased postoperative serum Klotho levels may serve as potential biomarkers for the identification of POCD following abdominal surgery.
Correlation Between Serum Klotho Levels and Clinical Indicators
Pearson correlation analyses were performed to evaluate the associations between postoperative serum Klotho levels and clinical indicators in all 93 patients who underwent abdominal surgery (Figure 2). As shown in Figure 2A, serum Klotho levels were significantly negatively correlated with the duration of anesthesia, indicating that a longer exposure to anesthesia was associated with lower postoperative Klotho concentrations. In contrast, serum Klotho levels were significantly positively correlated with postoperative Montreal Cognitive Assessment (MoCA) scores (Figure 2B), suggesting that higher Klotho levels were associated with better postoperative cognitive performance.
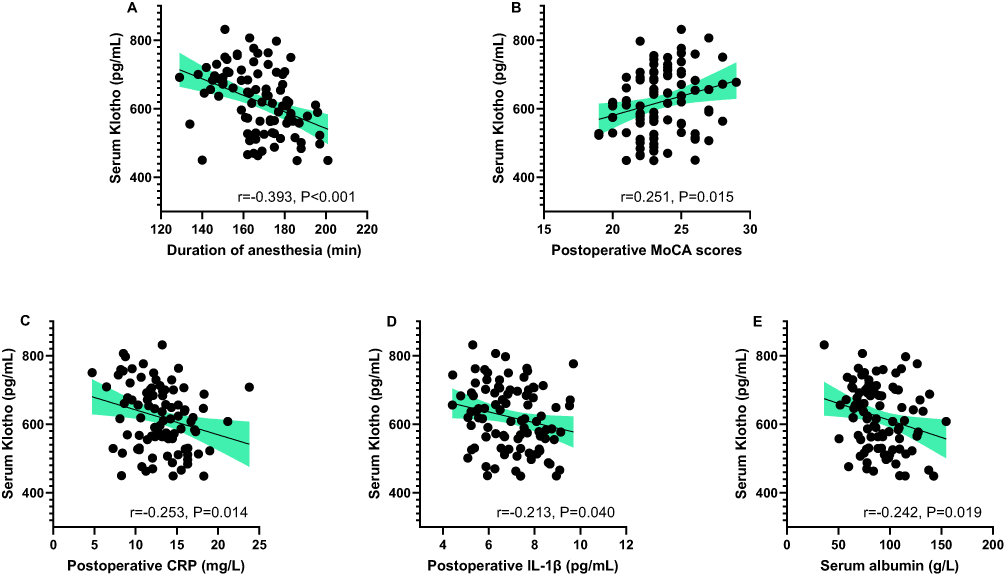 |
Figure 2 The correlation between serum Klotho and clinical indicators. Pearson correlation test was performed between Klotho with (A) duration of anesthesia, (B) postoperative MoCA scores, (C) postoperative CRP, (D) postoperative IL-1β, and (E) postoperative IL-6 in all 93 cases of patients after abdominal surgery. |
Furthermore, serum Klotho levels were inversely correlated with postoperative inflammatory markers, including C-reactive protein (CRP), interleukin (IL)-1β, and IL-6 (Figure 2C–E). Patients with lower serum Klotho levels tended to exhibit higher postoperative CRP, IL-1β, and IL-6 levels, reflecting an enhanced systemic inflammatory response. Collectively, these results indicate that decreased postoperative serum Klotho levels are associated with prolonged anesthesia duration, increased inflammation, and impaired cognitive function in patients who underwent abdominal surgery.
Discussion
In this study, we demonstrated that POCD following abdominal surgery is closely associated with decreased postoperative serum Klotho levels, heightened systemic inflammation, and impaired cognitive performance. Patients who developed POCD were significantly older, experienced longer durations of anesthesia, exhibited elevated postoperative inflammatory responses, and showed markedly reduced postoperative MoCA scores compared with non-POCD patients. Notably, preoperative serum Klotho levels were comparable between the groups, whereas postoperative Klotho levels were significantly lower in patients with POCD and exhibited favorable diagnostic performance for identifying POCD, highlighting Klotho as a potential postoperative biomarker.
Advanced age remains one of the most consistently reported risk factors for POCD, which aligns with our findings. Aging is accompanied by increased vulnerability of the central nervous system to surgical stress, anesthesia, and inflammatory insults.4,22 Klotho, a well-established anti-aging protein, declines with age,12 and reduced Klotho availability may contribute to age-related susceptibility to POCD by diminishing neuronal resilience and cognitive reserve. Our data indicate that postoperative changes in Klotho are more closely linked to cognitive outcomes than preoperative changes, suggesting that surgery- and anesthesia-induced stress may acutely suppress Klotho expression or release.
The negative correlation between anesthesia duration and postoperative serum Klotho levels underscores the impact of perioperative stress. Prolonged anesthesia exposure is associated with increased neuroinflammation, oxidative stress, and blood-brain barrier dysfunction, all of which contribute to POCD pathogenesis.23,24 Experimental studies indicate that Klotho exerts neuroprotective effects by reducing oxidative stress, suppressing inflammatory signaling, and preserving synaptic plasticity.14,25 Thus, a longer duration of anesthesia may exacerbate perioperative stress responses, leading to a greater decline in Klotho levels and subsequent cognitive impairment.
Systemic and neuroinflammation are central mechanisms underlying POCD.26 In our cohort, postoperative CRP, IL-1β, and IL-6 levels were significantly elevated in patients with POCD and inversely correlated with serum Klotho levels. These observations are consistent with previous reports demonstrating that Klotho negatively regulates inflammatory pathways, including NF-κB signaling, and attenuates the production of proinflammatory cytokines.27,28 IL-1β and IL-6 can cross the blood-brain barrier or activate microglia, leading to synaptic dysfunction and cognitive decline.29 Accordingly, reduced postoperative Klotho may amplify systemic inflammation, promoting neuroinflammatory cascades that contribute to POCD.
In addition to circulating inflammatory markers, accumulating evidence has positioned the gut as a critical upstream driver of postoperative inflammation, particularly following abdominal surgery. The gastrointestinal tract contains the largest immune compartment in the body, comprising macrophages, dendritic cells, T cells, and innate lymphoid cells that produce cytokines, interleukins, and interferons in response to surgical stress and tissue injury.30–32 Abdominal surgery, compounded by fasting, bowel preparation, antibiotic use, and surgical stress, can disrupt intestinal barrier integrity and induce gut dysbiosis, characterized by overgrowth of pathogenic bacteria and depletion of beneficial commensals.33,34 These perturbations compromise mucosal barrier function, increase gut permeability, and facilitate the translocation of microbial-derived inflammatory molecules, including lipopolysaccharide and pro-inflammatory cytokines, into systemic circulation.35–37 Fecal biomarkers, such as calprotectin, have been widely applied as noninvasive indicators of intestinal inflammation and immune activation, highlighting the role of gut-derived inflammatory signaling in systemic immune responses.38,39
Once in the circulation, gut-derived inflammatory mediators can amplify systemic inflammation and influence the central nervous system via the gut–brain axis. Circulating inflammatory molecules may disrupt or traverse the blood–brain barrier, activate microglia, impair synaptic plasticity, and exacerbate neuroinflammation, thereby contributing to POCD.40–43 Systemic inflammation has been shown to suppress protective anti-aging and neuroprotective factors, including Klotho, through inflammatory signaling pathways such as nuclear factor-κB activation.12,44 Emerging evidence suggests that Klotho expression is sensitive to both systemic and gut-derived inflammatory signaling, with lower postoperative Klotho levels potentially reflecting amplified inflammation originating from the gut following abdominal surgery.45,46
Although gut-specific inflammatory markers were not measured in this study, the observed inverse association between postoperative serum Klotho levels and circulating inflammatory markers supports a mechanistic framework in which abdominal surgery induces gut immune activation and dysbiosis, leading to systemic inflammation, reduced Klotho levels, and heightened vulnerability to cognitive decline. The positive correlation between serum Klotho and postoperative MoCA scores further supports the protective role of Klotho in cognitive function. These findings highlight an interaction between the gut-brain axis, systemic inflammation, and Klotho-mediated neuroprotection, suggesting that strategies to preserve gut homeostasis, reduce perioperative inflammation, and maintain Klotho levels may mitigate POCD risk. Future studies integrating gut microbiome profiling with Klotho measurement and cognitive assessments are warranted to further elucidate these mechanisms.
Study Limitations and Future Directions
This study has several limitations. It was conducted at a single center with a modest sample size, which may limit generalizability, and its cross-sectional design precludes causal inference between Klotho levels and cognitive decline. Only short-term postoperative cognitive function was assessed; therefore, the persistence of impairment and the prognostic value of Klotho remain unclear. Although circulating inflammatory markers were measured, gut-specific biomarkers, such as fecal calprotectin, were not assessed, limiting the evaluation of gut-derived contributions to systemic inflammation and POCD. Other potential mediators, including oxidative stress markers, neurotrophic factors, and confounders such as preoperative frailty, sleep quality, and medication use, were not fully controlled.
Future studies should validate these findings in larger, multicenter cohorts, assess longitudinal changes in Klotho and cognitive function, and explore its mechanistic role in neuroinflammation. Integrating Klotho with systemic and gut-derived biomarkers may enhance the early identification of patients at risk for POCD and guide interventions to preserve postoperative cognitive function.
Conclusion
In summary, decreased postoperative serum Klotho levels were significantly associated with prolonged anesthesia, elevated systemic inflammation, and impaired cognitive function in patients who underwent major abdominal surgeries (Figure 3). Serum Klotho demonstrates potential as a biomarker for early identification of patients at risk for postoperative cognitive dysfunction. These findings highlight the importance of Klotho in postoperative neuroprotection and suggest that strategies aimed at preserving or restoring Klotho levels may help mitigate POCD.
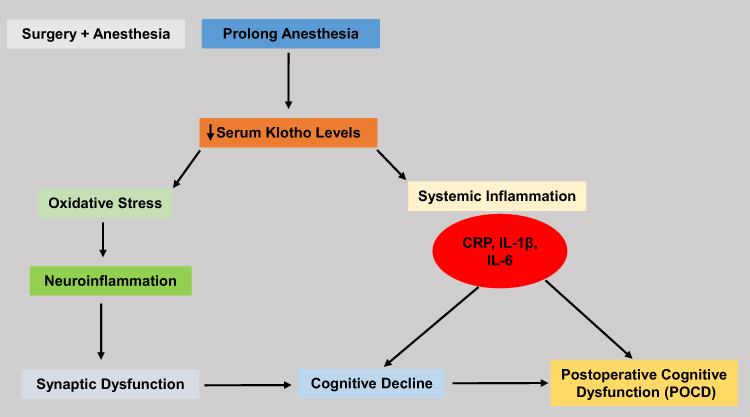 |
Figure 3 Proposed mechanism linking decreased postoperative serum Klotho levels to postoperative cognitive dysfunction (POCD) after abdominal surgery. Surgery and prolonged anesthesia lead to a reduction in serum Klotho levels, which contributes to increased oxidative stress and systemic inflammation, as indicated by elevated levels of CRP, IL-1β, and IL-6. These processes promote neuroinflammation and synaptic dysfunction, resulting in cognitive decline and POCD. Arrows indicate the direction of the effects, illustrating how decreased Klotho mediates the relationship between perioperative stress, inflammation, and postoperative cognitive impairment. |
Declaration of AI Use
We used the AI tool DeepSeek to assist in the preparation of this article, specifically for language editing and improving its readability.
Data Sharing Statement
The datasets used/analyzed during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Ethics Committee of the Sijing Hospital approved this study (2022sjyylw-AF/LXH). The authors followed all standard protocols in accordance with the 1964 Declaration of Helsinki. Written informed consent was obtained from all participants prior to study commencement.
Consent for Publication
All participants provided consent for the publication of the participants’ data.
Acknowledgment
We sincerely thank all of the participants in our study.
Author Contributions
Xuehui Li: Conceptualization, Methodology, Data curation, Visualization, Investigation, Writing-original draft. Feng Ao: Conceptualization, Supervision, Funding acquisition, Resources, Writing-review & editing. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Han FF, Wang XM, Zhang HJ, Wang JZ, Bao ZX, Li YL. Predictors and occurrence of postoperative cognitive dysfunction in children undergoing noncardiac surgery: a prospective cohort study. Ibrain. 2022;9(2):148–10. doi:10.1002/ibra.12066
2. Zhao Q, Wan H, Pan H, Xu Y. Postoperative cognitive dysfunction-current research progress. Front Behav Neurosci. 2024;18:1328790.
3. Daiello LA, Racine AM, Yun Gou R, et al. Postoperative delirium and postoperative cognitive dysfunction: overlap and divergence. Anesthesiology. 2019;131(3):477–491.
4. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Anesthesiology. 2018;129(5):872–879. doi:10.1097/ALN.0000000000002334
5. Finnerty CC, Mabvuure NT, Ali A, Kozar RA, Herndon DN. The surgically induced stress response. JPEN J Parenter Enteral Nutr. 2013;37(5S):21–29. doi:10.1177/0148607113496117
6. Bouras M, Asehnoune K, Roquilly A. Immune modulation after traumatic brain injury. Front Med. 2022;9:995044. doi:10.3389/fmed.2022.995044
7. Tseng WC, Lai HC, Huang YH, Chan SM, Wu ZF. Tumor necrosis factor alpha: implications of anesthesia on cancers. Cancers. 2023;15(3):739. doi:10.3390/cancers15030739
8. Paine NJ, Bosch JA, Ring C, Drayson MT, Veldhuijzen van Zanten JJ. Induced mild systemic inflammation is associated with impaired ability to improve cognitive task performance by practice. Psychophysiology. 2015;52(3):333–341. doi:10.1111/psyp.12360
9. Tan XX, Qiu LL, Sun J. Research progress on the role of inflammatory mechanisms in the development of postoperative cognitive dysfunction. Biomed Res Int. 2021;2021:3883204. doi:10.1155/2021/3883204
10. Brodier EA, Cibelli M. Postoperative cognitive dysfunction in clinical practice. BJA Educ. 2021;21(2):75–82. doi:10.1016/j.bjae.2020.10.004
11. Marcantonio ER. Delirium in hospitalized older adults. N Engl J Med. 2017;377(15):1456–1466. doi:10.1056/NEJMcp1605501
12. Kanbay M, Copur S, Ozbek L, et al. Klotho: a potential therapeutic target in aging and neurodegeneration beyond chronic kidney disease-a comprehensive review from the ERA CKD-MBD working group. Clin Kidney J. 2023;17(1):sfad276. doi:10.1093/ckj/sfad276
13. Abraham CR, Li A. Aging-suppressor Klotho: prospects in diagnostics and therapeutics. Ageing Res Rev. 2022;82:101766. doi:10.1016/j.arr.2022.101766
14. Dubal DB, Yokoyama JS, Zhu L, et al. Life extension factor klotho enhances cognition. Cell Rep. 2014;7(4):1065–1076. doi:10.1016/j.celrep.2014.03.076
15. Shen J, Bin W, Lin X, et al. Klotho protein: a multifaceted guardian of healthy aging and its therapeutic potential. Int J Nanomed. 2025;20:7251–7270. doi:10.2147/IJN.S514516
16. Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci. 2011;12(12):723–738. doi:10.1038/nrn3114
17. Semba RD, Cappola AR, Sun K, et al. Plasma klotho and mortality risk in older community-dwelling adults. J Gerontol a Biol Sci Med Sci. 2011;66(7):794–800. doi:10.1093/gerona/glr058
18. Torbus-Paluszczak M, Bartman W, Adamczyk-Sowa M. Klotho protein in neurodegenerative disorders. Neurol Sci. 2018;39(10):1677–1682. doi:10.1007/s10072-018-3496-x
19. Linghui D, Simin Y, Zilong Z, Yuxiao L, Shi Q, Birong D. The relationship between serum klotho and cognitive performance in a nationally representative sample of US adults. Front Aging Neurosci. 2023;15:1053390. doi:10.3389/fnagi.2023.1053390
20. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699.
21. Rudolph JL, Schreiber KA, Culley DJ, et al. Measurement of post-operative cognitive dysfunction after cardiac surgery: a systematic review. Acta Anaesthesiol Scand. 2010;54(6):663–677. doi:10.1111/j.1399-6576.2010.02236.x
22. Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008;108:18–30. doi:10.1097/01.anes.0000296071.19434.1e
23. Berger M, Terrando N, Smith SK, et al. Neurocognitive function after cardiac surgery. Anesthesiology. 2018;129(4):829–851. doi:10.1097/ALN.0000000000002194
24. Vacas S, Degos V, Tracey KJ, Maze M. High-mobility group box 1 protein initiates postoperative cognitive decline by engaging bone marrow-derived macrophages. Anesthesiology. 2014;120(5):1160–1167. doi:10.1097/ALN.0000000000000045
25. Hasannejad M, Samsamshariat SZ, Esmaili A, Jahanian-Najafabadi A. Klotho induces insulin resistance possibly through interference with GLUT4 translocation and activation of Akt, GSK3β, and PFKfβ3 in 3T3-L1 adipocyte cells. Res Pharm Sci. 2019;14(4):369–377. doi:10.4103/1735-5362.263627
26. Safavynia SA, Goldstein PA. The role of neuroinflammation in postoperative cognitive dysfunction: moving from hypothesis to treatment. Front Psychiatry. 2019;10:752. doi:10.3389/fpsyt.2018.00752
27. Liu F, Wu S, Ren H, Gu J. Klotho suppresses RIG-I-mediated senescence-associated inflammation. Nat Cell Biol. 2011;13(3):254–262. doi:10.1038/ncb2167
28. Xu Y, Sun Z. Molecular basis of Klotho: from gene to function in aging. Endocr Rev. 2015;36(2):174–193. doi:10.1210/er.2013-1079
29. Cunningham C, Hennessy E. Co-morbidity and systemic inflammation as drivers of cognitive decline. Brain Behav Immun. 2015;49:8–19.
30. Belkaid Y, Hand TW. Role of the microbiota in immunity and inflammation. Cell. 2014;157(1):121–141.
31. Honda K, Littman DR. The microbiota in adaptive immune homeostasis and disease. Nature. 2016;535(7610):75–84.
32. Levy M, Kolodziejczyk AA, Thaiss CA, Elinav E. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219–232.
33. Zaborin A, Smith D, Garfield K, et al. Membership and behavior of ultra-low-diversity pathogen communities present in the gut of humans during prolonged critical illness. mBio. 2014;5:e01361–14.
34. O’Keefe SJ, Li JV, Lahti L, et al. Fat, fibre and cancer risk in African Americans and rural Africans. Nat Commun. 2015;6(1):6342. doi:10.1038/ncomms7342
35. Alverdy JC, Krezalek MA. Collapse of the microbiome, emergence of the pathobiome, and the immunopathology of sepsis. Crit Care Med. 2017;45(2):337–347. doi:10.1097/CCM.0000000000002172
36. Assimakopoulos SF, Bhagani S, Aggeletopoulou I, Tsounis EP, Tsochatzis EA. The role of gut barrier dysfunction in postoperative complications in liver transplantation: pathophysiological and therapeutic considerations. Infection. 2024;52(3):723–736. doi:10.1007/s15010-024-02182-4
37. Kelly JR, Borre Y, O’Brien C, et al. Transferring the blues: depression-associated gut microbiota induces neurobehavioural changes in the rat. J Psychiatr Res. 2016;82:109–118. doi:10.1016/j.jpsychires.2016.07.019
38. Walsham NE, Sherwood RA. Fecal calprotectin in inflammatory bowel disease. Clin Exp Gastroenterol. 2016;9:21–29. doi:10.2147/CEG.S51902
39. Lehmann FS, Burri E, Beglinger C. The role and utility of faecal markers in inflammatory bowel disease. Ther Adv Gastroenterol. 2015;8(1):23–36. doi:10.1177/1756283X14553384
40. Cryan JF, O’Riordan KJ, Cowan CSM, et al. The microbiota–gut–brain axis. Physiol Rev. 2019;99(4):1877–2013. doi:10.1152/physrev.00018.2018
41. Perry VH, Holmes C. Microglial priming in neurodegenerative disease. Nat Rev Neurol. 2014;10(4):217–224. doi:10.1038/nrneurol.2014.38
42. Cibelli M, Fidalgo AR, Terrando N, et al. Role of interleukin-1β in postoperative cognitive dysfunction. Ann Neurol. 2010;68(3):360–368. doi:10.1002/ana.22082
43. Forsythe P, Kunze WA, Bienenstock J. On communication between gut microbiota and the brain. Curr Opin Gastroenterol. 2016;32:253–258.
44. Hui H, Zhai Y, Ao L, et al. Klotho suppresses the inflammatory responses and ameliorates cardiac dysfunction in aging endotoxemic mice. Oncotarget. 2017;8(9):15663–15676. doi:10.18632/oncotarget.14933
45. Hanson K, Fisher K, Hooper NM. Exploiting the neuroprotective effects of α-klotho to tackle ageing- and neurodegeneration-related cognitive dysfunction. Neuronal Signal. 2021;5(2):NS20200101. doi:10.1042/NS20200101
46. Gallo A, Passaro G, Gasbarrini A, Landolfi R, Montalto M. Modulation of microbiota as treatment for intestinal inflammatory disorders: an uptodate. World J Gastroenterol. 2016;22(32):7186–7202. doi:10.3748/wjg.v22.i32.7186
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.