Back to Journals » International Journal of General Medicine » Volume 14
The Relationship Between Blood Lipid and Attention-Deficit/Hyperactivity Disorder (ADHD) in an Obese Population of Chinese Children: An Obesity-Stratified Cross-Sectional Study
Received 20 August 2021
Accepted for publication 18 October 2021
Published 30 December 2021 Volume 2021:14 Pages 10503—10509
DOI https://doi.org/10.2147/IJGM.S333247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yan Xu, Lijuan Bao, Chengquan Liu
Huai ‘an Maternal and Child Health Hospital, Huai’an City, 223000, Jiangsu Province, People’s Republic of China
Correspondence: Chengquan Liu
Huai ‘an Maternal and Child Health Hospital, No. 104 Renmin South Road, Huai’an City, 223000, Jiangsu Province, People’s Republic of China
Tel +86 0517-80888758
Email [email protected]
Background: Although obesity has been related to attention-deficit/hyperactivity disorder (ADHD), few studies have examined the relationship between blood lipid levels and ADHD in children. We aimed to evaluate whether increased blood lipid levels are associated with the prevalence of ADHD in children.
Methods: A total of 1179 children were studied in the cross-sectional analysis. Multivariate logistic regression and linear regression analyses were performed to evaluate the association of blood lipid levels with the prevalence of ADHD in children.
Results: In 1179 children, the average age was 10.4 years, and the percentage of boys was 50.3%. 97 (8.2%) of the children were diagnosed with ADHD. The logistic regression analysis demonstrated that elevated levels of total cholesterol (OR=2.001, 95% CI 1.247– 3.541, P-trend=0.024), triglycerides (OR=1.776, 95% CI 1.448– 2.187, P-trend=0.003) and LDL (low density lipoprotein; OR=2.016, 95% CI 1.335– 3.966, P-trend< 0.001) and reduced levels of HDL (high density lipoprotein; OR=0.577, 95% CI 0.298– 0.948, P-trend=0.023) were associated with the prevalence of ADHD after adjustments were made for age, sex, body mass index (BMI), residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, maternal and paternal educational levels, and marital status of parents in Model 3. The stratified analysis using “obese” as a covariate showed that elevated levels of total cholesterol, triglycerides and LDL and reduced levels of HDL were independently associated with an increased risk of ADHD in obese children.
Conclusion: Increased blood lipid levels were associated with ADHD in obese children.
Keywords: blood lipids, ADHD, obese, cross-sectional analysis
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of most common neurodevelopmental disorders in childhood and has been found to be closely associated with an increased risk of metabolic syndrome, such as obesity and diabetes mellitus.1–4 The prevalence of ADHD was suggested to increase by more than 30% during 2006–2008,5 and in recent years, the rate of childhood obesity has been significantly rising due to overnutrition.6 Existing studies have shown a high rate of obesity in children with ADHD or a high prevalence of ADHD in obese children.7 Despite mixed findings in some studies, meta-analyses have demonstrated a close association of ADHD with obesity, independent of potential confounding factors such as mental health conditions.7
Metabolic syndrome is an increasing public health concern due to its associations with complications, including hyperlipidemia, hypertension, diabetes, cardiovascular disease (CVD) and cancer.8–10 Recently, a meta-analysis examined the association between obesity and ADHD after controlling for confounding factors such as age, sex and others among children.7 A significant association of ADHD with obesity was found in the meta-analysis, which included more than 700,000 children and adults.7 Metabolic syndrome, which is associated with obesity, includes a series of metabolic abnormalities, including hypertriglyceridemia, low levels of high-density lipoprotein cholesterol (HDL), high levels of low-density lipoprotein cholesterol (LDL), hypertension and insulin resistance.11,12 The incidence of metabolic syndrome has been significantly rising in the past few decades. Recent data have demonstrated that approximately 1/4 of American adults have metabolic syndrome, which accounts for much of the risk for premature cardiovascular death.13,14 Importantly, the median prevalence of metabolic syndrome in the whole population was 3%, with a prevalence of 29% among obese children.15,16
Studies in the literature have investigated this association between blood lipid levels and ADHD.17–19 However, studies investigating the association between blood lipid levels and ADHD in Chinese children are limited. We aimed to investigate whether the relationship between blood lipid levels and ADHD is independent of other confounding factors. We also investigated whether this independent association can be modified by obesity.
Materials and Methods
Study Sample
For the purpose of this study, 1179 children who were registered Clinical Data Repository from January 2010 to December 2020 were included in our analysis. In the study, all children with ADHD were included if they had at least one registered diagnosis of ADHD. The diagnostic criteria for ADHD include the following:19 1) the onset of ADHD is at or before the age of 7; 2) the symptoms of ADHD must manifest in two or more environments, such as school, workplace or home; 3) there is clear clinical impairment in social, academic or occupational functions; and 4) generalized developmental disorder, schizophrenia, emotional disorder or other mental disorders should be excluded. All included children met these 4 criteria. Additionally, the details of blood collection, storage and testing for blood lipid levels, including total cholesterol and triglycerides, LDL and HDL, are available elsewhere.18 Blind-duplicate coefficients of variation ranged from 5% to 10%. According to the Declaration of Helsinki guidelines, the Ethics Committee of the Huai ‘an Maternal and Child Health Hospital approved this study, and all patients gave written informed consent.
Covariates
Sociodemographic characteristics and lifestyle factors, including age, sex, BMI, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, maternal and paternal educational levels, marital status of parents, nutritional status and physical activity. Residence type was defined as “urban” or “rural”. Breastfeeding was classified as “never breastfed” or “ever breastfed”. Maternal smoking during pregnancy was classified as “never smoked during pregnancy”, or “ever smoked during pregnancy”. Maternal and paternal educational levels were defined as “more than primary school” or “primary school and lower”. The marital status of parents was classified as “separated/divorced” or “other”. Nutritional status was dichotomized as “adequate” or “inadequate”. Physical activity was also dichotomized as “appropriate” or “inappropriate”. Additionally, since the growth patterns of boys and girls differ, evaluating the body mass index (BMI) of children is more complicated than and different from evaluating adults. Therefore, the WHO guidelines were used to diagnose obesity in children, with obesity defined as a BMI ≥ 85th percentile and a triceps skinfold thickness and a subscapular skinfold thickness ≥ 90th percentile.
Statistical Analysis
Data were analyzed by using SPSS 25.0. All measurement data in our study were normally distributed or had approximate normal distributions and are expressed as the mean ± standard deviation (M ± SD). Categorical variables are shown as n (%). All individuals in this study were divided into two groups according to whether they were obese (BMI ≥ 24 kg/m2). Then, corrected logistic regression analysis was used to examine the associations between blood lipid levels (total cholesterol, triglycerides, LDL and HDL) and the risk of ADHD in children, with quartile 1 as the reference category. Blood lipid levels were categorized by quartiles (quartile 4: ≥75th percentile, quartile 3: 50th–75th percentile, quartile 2: 25th–50th percentile, quartile 1: <25th percentile). Quartile 1 was defined as a reference group. Confounding factors were corrected as follows: Model 1: adjusted for age and sex; Model 2: adjusted for age, BMI, sex, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length; Model 3: adjusted for age, sex, BMI, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, maternal and paternal educational levels, marital status of parents and physical activity. Then, to further observe whether obesity can modify the relationship between blood lipids and ADHD in children, interaction analysis was performed.
To further assess the predictive value of blood lipid levels for detecting ADHD among children, sensitivity analysis was performed by adding “physical activity” as a covariate in the logistic regression model. P ≤ 0.05 was considered to be statistically significant in all analyses.
Results
Baseline Characteristics of the Study Cohort
Of 1179 children in this cross-sectional analysis (Table 1), 593 (50.3%) were boys. The mean of age was 10.4 (10.4±3.6) years. A total of 793 (67.4%) individuals lived in urban areas, and had BMIs from 18.6±3.4. The number of individuals with maternal smoking during pregnancy was 20 (1.7%), and the number of breastfed individuals was 998 (84.6%) with a breastfeeding length of 6.2 ±3.1 months. Among these children, maternal and paternal educational levels with more than a primary school education were 95.4% and 98.6%, respectively.
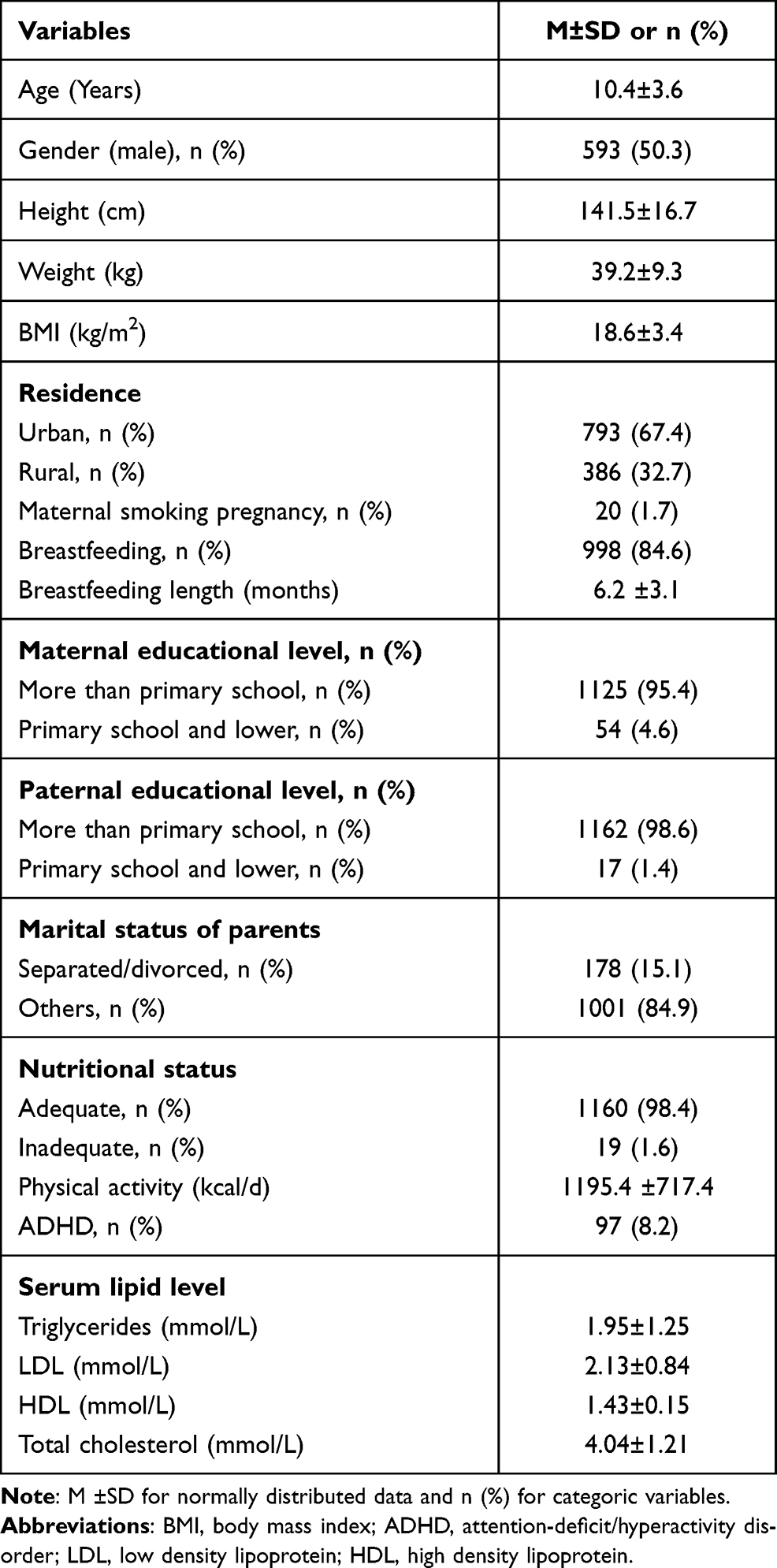 |
Table 1 The Characteristics of Study Population (N=1179) |
The Association Between Blood Lipid Levels and the Risk of ADHD in Children Analyzed by Logistic Regression
We evaluated the association of blood lipid levels (total cholesterol, triglycerides, LDL and HDL) with the risk of ADHD among children by multivariate logistic regression analysis, as shown in Table 2. Model 1 indicated that elevated levels of total cholesterol [2.248 (1.380–4.226), P-trend=0.009], triglycerides [1.885 (1.501–3.099), P-trend<0.001] and LDL [2.326 (1.527–4.772), P-trend<0.001] were associated with a higher risk of ADHD after adjustment for age and sex. After adjusting for age, BMI, sex, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, the results in Model 2 were similar to those of Model 1. This association remained statistically significant and changed little when maternal and paternal educational levels, marital status of parents and physical activity were added to Model 2 (Model 3). Importantly, our results also showed that a higher HDL [0.455 (0.090–0.812), P-trend=0.008] was associated with a reduced risk of ADHD in Model 1 when age and sex were adjusted. Interestingly, the association disappeared in Model 2 and Model 3, when the remaining confounding factors were adjusted for.
 |
Table 2 Logistic Regression Analysis of the Relationship Between the Lipid Levels and Risk of ADHD in Children |
Stratified Analysis of the Association Between Blood Lipid Levels and the Risk of ADHD in Children
All included children were classified into two groups according to obesity status (obese group and nonobese group). We found that elevated levels of total cholesterol (OR=2.234, 95% CI 1.112–5.103, P<0.001), triglycerides (OR=1.585, 95% CI 1.037–2.572, P=0.010) and LDL (OR=2.568, 95% CI 1.358–4.267, P<0.010) were still independently associated with an increased risk of ADHD in obese children after adjustments for age, sex, BMI, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, maternal and paternal educational levels, and marital status of parents were made (Table 3). Importantly, the associations of these indices, including levels of total cholesterol (OR=1.232, 95% CI 1.008–2.336, P=0.205), triglycerides (OR=1.458, 95% CI 1.016–2.752, P=0.176) and LDL (OR=1.649, 95% CI 1.204–3.135, P=0.071), with ADHD were not significant in nonobese children. Similarly, HDL levels were still related to a lower risk of ADHD in obese children (OR=0.446, 95% CI 0.125–0.802 P=0.008) but not in nonobese children (OR=0.679, 95% CI 0.133–1.089, P=0.059). The P values for interactions in the stratified analysis were 0.003 (total cholesterol), 0.003 (triglycerides), 0.005 (LDL) and 0.014 (HDL).
 |
Table 3 Logistic Regression Analysis for the Relationship Between the Lipid Levels and Risk of ADHD in Children by Stratified Analysis Using “Obese” |
Importantly, to further assess the predictive value of blood lipid levels for detecting ADHD among children, sensitivity analysis was performed by adding “physical activity” as a covariate in the logistic regression model. After adjusting for age, sex, BMI, residence type, maternal smoking during pregnancy, breastfeeding and breastfeeding length, maternal and paternal educational levels, marital status of parents and physical activity, our results were consistent with those in Tables 3 and 4. The P values for interactions in the stratified analysis were 0.004 (total cholesterol), 0.002 (triglycerides), 0.007 (LDL) and 0.018 (HDL), as shown in Table 4.
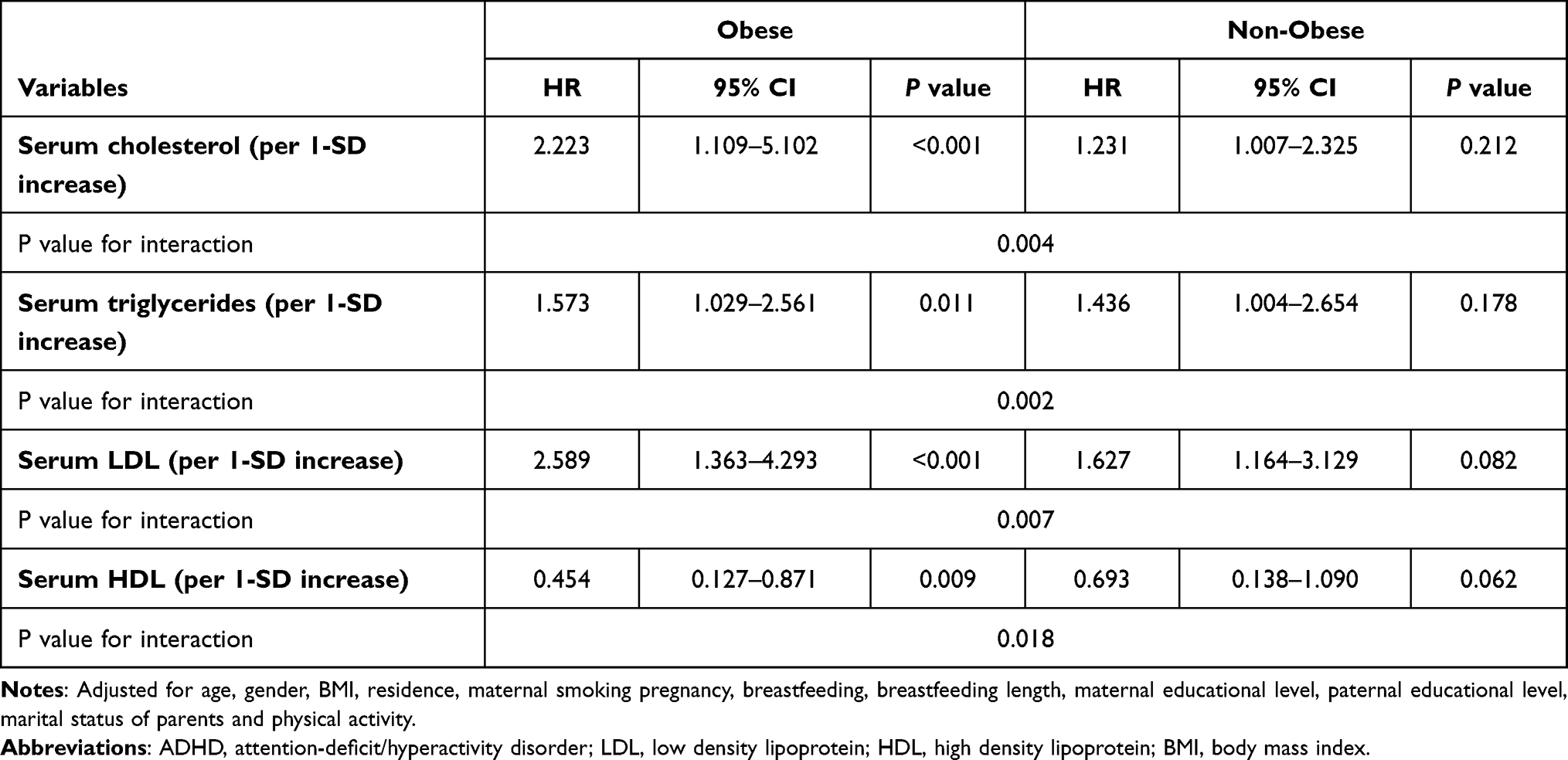 |
Table 4 Sensitivity Analysis for the Relationship Between the Lipid Levels and Risk of ADHD in Children by Using “Physical Activity” |
Discussion
We found that elevated levels of blood lipids were related to an increased risk of ADHD in children when adjusting for potential confounding factors. This independent relationship can be significantly modified by obesity.
ADHD has a high prevalence of approximately 5% in school children worldwide.7 The average annual costs for ADHD have significantly risen in the past few years.20 Although many existing studies have suggested a significant association of obesity with ADHD,21–23 others did not confirm this finding.24,25 The uncertain association between obesity and ADHD seems to be paradoxical because obese children are usually described as being lazy.14 The effect of potential confounding factors, such as obesity, psychiatric comorbidities and low socioeconomic status, for explaining the association between levels of blood lipids and ADHD is still not entirely certain, especially among children.21–23,26
One study suggested that no significant difference in triglycerides and HDL levels was found between a small sample of adults with ADHD who did not undergo treatment and adults without ADHD,27 but individuals with ADHD had LDL levels above 160 mg/dl. Another study, based on the population-based German Health Interview and Examination Survey for children and adolescents, reported that 9.7% (666) of individuals were diagnosed with ADHD or suspected ADHD, and compared serum total cholesterol, triglycerides, LDL and HDL levels between children with ADHD and children without ADHD.28 The results from the children’s data showed that differences in total cholesterol and LDL levels, rather than triglycerides and HDL levels, were found between individuals with ADHD and individuals without ADHD. A weakly inverse association was found between LDL levels and ADHD symptoms. The above results are partly consistent with our findings that total cholesterol, triglycerides and LDL levels were associated with a higher risk of ADHD. Nigg et al found no relationship between the lipid profile and ADHD.29 Pinho et al found an inverse relationship between LDL levels and ADHD.30 In our study, a significant association existed only in obese children. These four indices of blood lipid levels had no association with ADHD risk among nonobese children. The heterogeneity of these study results might be at least partly explained by the different study designs used and hypotheses investigated, different confounding factors adjusted for, the populations of different ages selected and varying serum measurement methods and instruments. For instance, blood lipid levels under different physiological conditions and different questionnaires assessing confounding variables can account for some of these variations.
Our study has three main contributions to the literature. First, our study data are from the cross-sectional analysis with a large sample size.18,19 The analysis of the results suggested that elevated levels of blood lipids were closely related to ADHD among nonobese children, which expands national sample research on the association. Second, our results demonstrated that obesity is an important modifying variable that affects the association between blood lipid levels and ADHD. We found that the relationship between blood lipid levels and ADHD can be significantly affected, which seems to explain the heterogeneity of previous studies on the association between ADHD and obesity. Additionally, we conducted a robust and accurate calibration analysis to exclude the effects of other potential confounding factors, such as sociodemographic characteristics and lifestyle factors, environmental factors, and nutritional status, which have been associated with ADHD and blood lipid levels.
Of course, a limitation of our study is the cross-sectional study design in which the causal relationship between serum lipid levels and ADHD is uncertain. Future research is necessary to identify the prognostic value of levels of blood lipids for predicting ADHD in children. Moreover, blood lipid levels were measured only once in each individual. Under different times, environments and physiological states, blood lipid levels will change and eventually affect the stability and reliability of the results.
In conclusion, the cross-sectional analysis revealed that blood lipid levels were related to an increased risk of ADHD among obese children but not in nonobese children. This study may provide further evidence that obesity is an important factor in the development of ADHD in children.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest and have nothing to disclose.
References
1. Pinhas-Hamiel O, Levek-Motola N, Kaidar K, et al. Prevalence of overweight, obesity and metabolic syndrome components in children, adolescents and young adults with type 1 diabetes mellitus. Diabetes Metab Res Rev. 2015;31(1):76–84. doi:10.1002/dmrr.2565
2. Bielorai B, Pinhas-Hamiel O. Type 2 diabetes mellitus, the metabolic syndrome, and its components in adult survivors of acute lymphoblastic leukemia and hematopoietic stem cell transplantations. Curr Diab Rep. 2018;18(6):32. doi:10.1007/s11892-018-0998-0
3. Kassm SA, Hoertel N, Naja W, et al. Metabolic syndrome among older adults with schizophrenia spectrum disorder: prevalence and associated factors in a multicenter study. Psychiatry Res. 2019;275:238–246. doi:10.1016/j.psychres.2019.03.036
4. Pinhas-Hamiel O, Livne M, Harari G, et al. Prevalence of overweight, obesity and metabolic syndrome components in multiple sclerosis patients with significant disability. Eur J Neurol. 2015;22(9):1275–1279. doi:10.1111/ene.12738
5. Feldman HM, Reiff MI. Attention deficit–hyperactivity disorder in children and adolescents — NEJM. Pediatr Clin North Am. 2014;50(5):1049–1092.
6. Cortese S, Tessari L. Attention-Deficit/Hyperactivity Disorder (ADHD) and obesity: update 2016. Curr Psychiatry Rep. 2017;19(1). doi:10.1007/s11920-017-0754-1
7. Polanczyk G, Lima MD, Horta BL, et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–948. doi:10.1176/ajp.2007.164.6.942
8. Costa LA, Canani LH, Lisboa HR, Tres GS, Gross JL. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in type 2 diabetes. Diabetic Med. 2004;21(3):252–255.
9. Costa LA, Canani LH, Lisba HRK, et al. Aggregation of features of the metabolic syndrome is associated with increased prevalence of chronic complications in type 2 diabetes. Diabetic Med. 2010;21(3):252–255. doi:10.1111/j.1464-5491.2004.01124.x
10. Isomaa B, Henricsson M, Almgren P, et al. The metabolic syndrome influences the risk of chronic complications in patients with type II diabetes. Diabetologia. 2001;44(9):1148–1154. doi:10.1007/s001250100615
11. Virgin SE, Schmitke JA. Metabolic syndrome. Aaohn J. 2003;51(1):28. doi:10.1177/216507990305100108
12. Després JP, Lemieux I. Abdominal obesity and metabolic syndrome. Nature. 2006;444(7121):881–887. doi:10.1038/nature05488
13. Ginsberg HN, Maccallum PR. The obesity, metabolic syndrome, and type 2 diabetes mellitus pandemic: II. Therapeutic management of atherogenic dyslipidemia. J Clin Hypertens. 2010;11(9):520–527. doi:10.1111/j.1559-4572.2009.00060.x
14. Farid S, Gooren LJ. The role of testosterone in the etiology and treatment of obesity, the metabolic syndrome, and diabetes mellitus type 2. J Obes. 2011;2011:2090–2708.
15. Friend A, Craig L, Turner S. The prevalence of metabolic syndrome in children: a systematic review of the literature. Metab Syndr Relat Disord. 2013;11(2):71–80. doi:10.1089/met.2012.0122
16. Friend AJ, Craig L, Turner SW.The prevalence of metabolic syndrome in children – a systematic review. Arch Dis Child.2012;97:
17. Avcil S. Association between altered lipid profiles and attention deficit hyperactivity disorder in boys. Nord J Psychiatry. 2018;72:361–366. doi:10.1080/08039488.2018.1465591
18. Spahis S, Vanasse M, Bélanger SA, Ghadirian P, Grenier E, Levy E. Lipid profile, fatty acid composition and pro and anti-oxidant status in pediatric patients with attention-deficit/hyperactivity disorder. Prostaglandins Leukot Essent Fatty Acids. 2008;79(1–2):47–53. doi:10.1016/j.plefa.2008.07.005
19. Ugur C, Uneri OS, Goker Z, Sekmen E, Aydemir H, Solmaz E. The assessment of serum lipid profiles of children with attention deficit hyperactivity disorder. Psychiatry Res. 2018;264:231–235. doi:10.1016/j.psychres.2018.04.006
20. Doshi JA, Hodgkins P, Kahle J, et al. Economic impact of childhood and adult attention-deficit/hyperactivity disorder in the United States. J Am Acad Child Adolesc Psychiatry. 2012;51(10):990–1002.e2. doi:10.1016/j.jaac.2012.07.008
21. Zwaan MD, Gru DB, Müller A, et al. Association between obesity and adult attention-deficit/hyperactivity disorder in a German community-based sample. Obes Facts. 2011;4(3):204–211. doi:10.1159/000329565
22. Hle A, Stoy M, Wrase J, et al. Reward anticipation and outcomes in adult males with attention-deficit/hyperactivity disorder. NeuroImage. 2008;39(3):966–972. doi:10.1016/j.neuroimage.2007.09.044
23. Waring ME, Lapane KL. Overweight in children and adolescents in relation to attention-deficit/hyperactivity disorder: results from a national sample. Pediatrics. 2008;122(1):e1–e6. doi:10.1542/peds.2007-1955
24. Cortese S, Ramos Olazagasti MA, Klein RG, et al. Obesity in men with childhood ADHD: a 33-year controlled, prospective, follow-up study. Pediatrics. 2013;131(6):e1731–e1738. doi:10.1542/peds.2012-0540
25. Dubnov-Raz G, Perry A, Berger I. Body mass index of children with attention-deficit/hyperactivity disorder. J Child Neurol. 2011;26(3):302–308. doi:10.1177/0883073810380051
26. Cortese S, Faraone SV, Bernardi S, et al. Adult attention-deficit hyperactivity disorder and obesity: epidemiological study. Br J Psychiatr. 2013;203(1):24–34. doi:10.1192/bjp.bp.112.123299
27. Nigg JT. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev. 2012;33(2):215–228. doi:10.1016/j.cpr.2012.11.005
28. Pinho R, Wang B, Becker A, et al. Attention-deficit/hyperactivity disorder is associated with reduced levels of serum low-density lipoprotein cholesterol in adolescents. Data from the population-based German KiGGS study. World J Biol Psychiatry. 2018;19:1–9. doi:10.1080/15622975.2018.1419025
29. Hawkey E, Nigg JT. Omega-3 fatty acid and ADHD: blood level analysis and meta-analytic extension of supplementation trials. Clin Psychol Rev. 2014;34(6):496–505. doi:10.1016/j.cpr.2014.05.005
30. Pinho R, Wang B, Becker A, et al. Attention-deficit/hyperactivity disorder is associated with reduced levels of serum low-density lipoprotein cholesterol in adolescents. Data from the population-based German KiGGS study. World J Biol Psychiatry. 2019;20(6):496–504. doi:10.1080/15622975.2017.1417636
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.