Back to Journals » Orthopedic Research and Reviews » Volume 14
The Radiological Complications of Short-Segment Pedicle Screw Fixation Combined with Transforaminal Interbody Fusion in the Treatment of Unstable Thoracolumbar Burst Fracture: A Retrospective Case Series Study in Vietnam
Received 18 January 2022
Accepted for publication 22 March 2022
Published 29 March 2022 Volume 2022:14 Pages 91—99
DOI https://doi.org/10.2147/ORR.S356296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ngoc Quyen Nguyen,1 Trong Hau Phan2
1Department of Outpatient Clinic, 108 Military Central Hospital, Hanoi City, Vietnam; 2Department of Spinal Surgery, 108 Military Central Hospital, Hanoi City, Vietnam
Correspondence: Ngoc Quyen Nguyen, Department of Outpatient Clinic, 108 Military Central Hospital, No. 1, Tran Hung Dao Street, Ha Ba Trung District, Hanoi, 113000, Vietnam, Tel +84-989052288, Email [email protected]
Background: The radiological complications including correction loss and hardware failure of short segment posterior pedicle screw fixation in the treatment of unstable thoracolumbar burst fractures remain a main concern. Several procedures aiming to reinforce the anterior column have been introduced to solve these limitations, including transforaminal interbody fusion (TIF). The purposes of this study were to evaluate the radiological complications of short-segment pedicle screw fixation in combination with transforaminal interbody fusion in the treatment of unstable thoracolumbar burst fractures.
Methods: This retrospective case series study enrolled patients with isolated unstable thoracolumbar burst fractures, who were treated by posterior short fixation with TIF between January 2013 and January 2017. Patients were followed up for a minimum of one and half years. For evaluation of correction loss, % loss of anterior vertebral body height (%AVB), vertebral kyphotic angle (VA) and regional kyphotic angle (RA) were collected preoperatively, postoperatively and at the final follow-up. Hardware failure was assessed on radiological images at the last follow-up.
Results: There were 36 patients who met the inclusion criteria with a mean follow-up duration of 53 months. The mean correction loss of %AVB, VA and RA were 10.2%, 2.9° and 5.6°, respectively. There were 6 patients (16.7%) with hardware failure at the final follow-up.
Conclusion: Short-segment posterior pedicle screw fixation with TIF using bone chip grafts does not completely prevent hardware failure and progressive kyphosis in the treatment of unstable thoracolumbar burst fractures.
Keywords: thoracolumbar burst fracture, short-segment fixation, transforaminal interbody fusion, hardware failure, correction loss
Background
Thoracolumbar burst fractures are defined as spinal injuries that result from axial compression with rupture of the anterior and medial structures of the vertebral body, retropulsion of a bone fragment into the spinal canal and an increase in the interpedicular distance.1 It is still controversial about the ideal management for thoracolumbar burst fracture.2 Short-segment posterior pedicle screw fixation is still considered a preferred option because it can reduce blood loss, preserving segmental motion with an acceptable anatomic and functional outcome. However, loss of kyphotic corrections and a high rate of hardware failure due to lack of anterior column support are the main disadvantages of this short spinal fixation.3 Several procedures aiming to reinforce the anterior column have been introduced to solve the limitations of short-segment posterior pedicle screw fixation, including TIF.4,5 In Vietnam, TIF with bone chip grafts has been applied for the treatment of unstable thoracolumbar burst fracture to prevent the limitations of short posterior fixation. However, to the best of our knowledge, there have been no reports about the radiological complications of posterior short-pedicle screw fixation with TIF using bone chip grafts in the treatment of unstable thoracolumbar burst fractures. This study aims to evaluate the radiological complications including hardware failure and correction loss of this surgical procedure for the treatment of unstable thoracolumbar burst fracture in Vietnamese patients.
Methods
Patient Selection
From Jan 2013 to Jan 2017, 40 consecutive patients underwent posterior short-segment pedicle screw fixation and TIF. All patients had a single-level thoracolumbar burst fracture. Among the 40 patients, 2 patients with plain radiograph quality were not sufficient for analysis, and 2 patients did not undergo re-examination at the final follow-up. Finally, a total of 36 patients were enrolled in this study.
Surgical Indications
Patients who had one or more of the following: 1. Presence of neurological involvement caused by the fracture; 2. Computed tomography (CT) scanning of the affected level showed more than 50% spinal canal compromise; 3. ≥50% loss of anterior vertebral height;6–8 4. A vertebral kyphosis angle >30°was used for this surgical method.7
All patients were evaluated using load sharing classification (LSC)9 and underwent posterior short-segment pedicle screw fixation with TIF.
Surgical Technique
The patient was placed in the prone position on a radiolucent table The fractured vertebral body was identified by using fluoroscopy. A midline conventional longitudinal spinal incision was routinely used to expose one level above and below the fractured vertebra. Subperiosteal dissection was carried out with an electric cutter until the facet joints on both sides were visualized. Pedicle screws were inserted into the vertebral body at 1 level below and above the affected level without insertion of the pedicle screw at the vertebral fracture. The screws of both sides were distracted axially with contoured longitudinal rods to restore the segmental height and realign the spinal columns and to indirectly perform the reduction of the retropulsed fragment. Then, exposure of one transforaminal zone of the affected level was performed using Kerrison rongeurs to remove a part of the lamina and facet joint until the nerve root and thecal sac were revealed. Epidural veins and radicular veins were cauterized with bipolar forceps to avoid massive bleeding. Then, the thecal sac and nerve root were gently retracted, and the adjacent intervertebral disc was completely removed.
If the patient had neurologic deficits and/or the stenotic degree of the spinal canal was more than 50% of its normal value, the retropulsed fragment of the fractured vertebral body was hammered anteriorly back into the vertebral body by using an “L” shape dissector.
After that, the local bone graft was packed into the intervertebral space. If local bone was not enough, additional allografts or autografts from iliac bone were used. The decompression procedure was performed with a recheck of all the neural elements involved. A drain was placed, and then the wound was closed in a standard fashion.
Evaluation of Radiological Complications
All patients underwent plain radiography preoperatively, postoperatively and at the final follow-up. Evaluation of the plain radiograph included measurements of % AVB and VA and RA. The RA of the fractured segment was measured as the angle between the superior endplate of the upper adjacent vertebra and the inferior endplate of the lower adjacent vertebrae by the Cobb method (Figure 1A).10 VA was measured as the angle between a line drawn parallel to the superior endplate and a line drawn parallel to the inferior endplate of the fracture vertebra (Figure 1A). The anterior body height of the injured and the non-injured adjacent vertebrae above and below were measured on the lateral X-ray film, and % AVB was calculated as the anterior height of the fractured vertebra divided by the mean of the anterior height of the adjacent two vertebrae using the formula % AVB = 100−2b/(a + c)100, which was adopted by Mumford et al.11 The anterior vertebral body height of the proximal vertebra is marked as a; the anterior vertebral body height of the fractured vertebra is marked as b; and c is the anterior vertebral body height of the distal vertebra (Figure 1B).
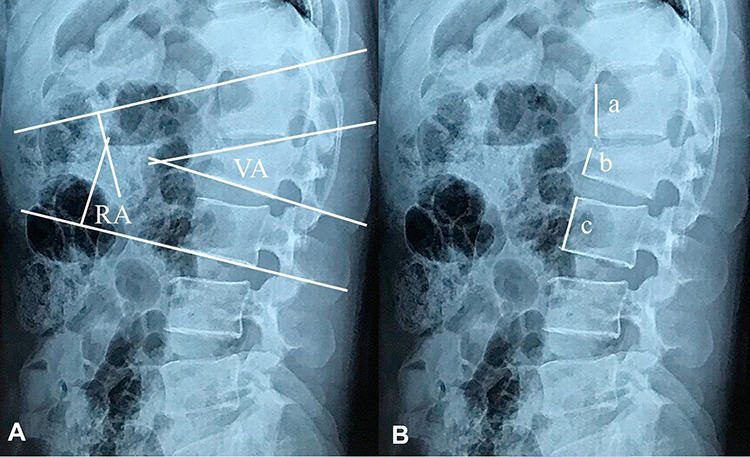 |
Figure 1 Measurement of parameters on plain X-rays: (A) shows measurement of the regional kyphotic angle (RA) and vertebral kyphotic angle (VA); (B) shows measurement of percentage of anterior vertebral body height loss (%AVB), which is calculated by the formula: %AVB = 100–2b/(a + c)* 100, where a is the anterior edge height of the vertebra above the fractured vertebra; b is the anterior edge height of the fractured vertebra; and c is the anterior edge height of the vertebra below the fractured vertebra. |
Fusion was defined based on the criteria of Bridwell12 that was identified by using CT scans taken at the final follow-up. Hardware failure was defined as a correction loss of more than 10° of the RA values at the final follow-up compared to the immediate postoperative period and/or pedicle screw(s) and/or rod(s) breakage.
Statistical Analyses
SPSS 20.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The paired t-test was used to analyze differences between preoperative, postoperative, and final follow-up radiographic data within each group. The Mann-Whitney test was used to analyze numerical data between the 2 groups. The level of statistical significance was set at p < 0.05.
Results
Demographic Data
A final total of 36 patients were enrolled in this study. The age range was 18 to 59 years old (mean 47 years old), with 20 males and 16 females. The mean follow-up duration was 53 months (range, 17–73 months). The affected levels were T12, L1 and L2 in 4 patients, 22 patients, and 10 patients, respectively. More than two-thirds of the participants had a history of falling from height (28 cases), and the other main sources of trauma were traffic accidents (4 cases), sport accidents (3 cases), and direct trauma (01 case). All the cases were type A3 according to the Magerl/AO classification system.13 The mean LSC was 6.8 (range, 5–9) (Table 1).
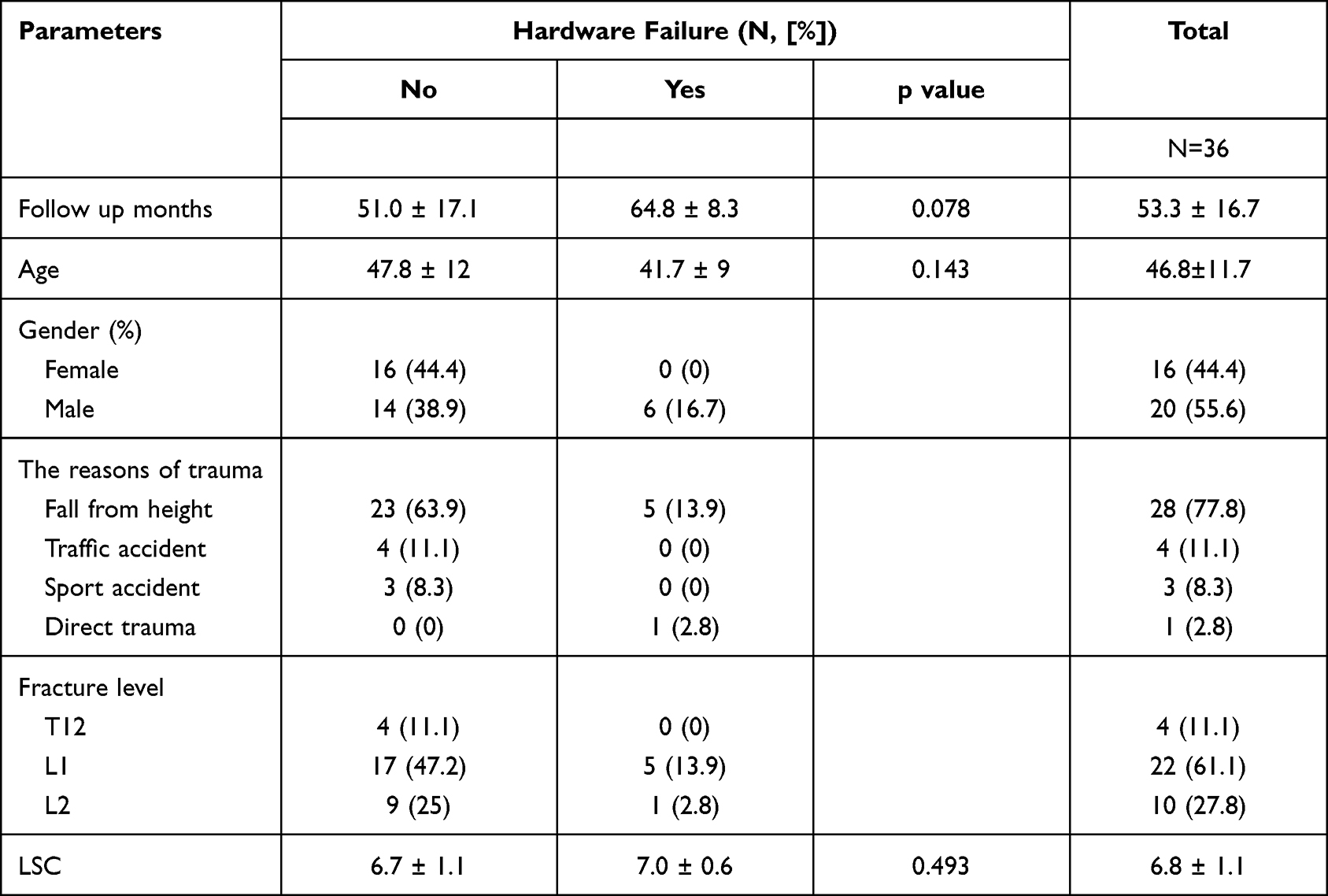 |
Table 1 Demographic Data |
Radiological Outcomes
Table 2 shows the mean %AVB, VA, RA, and the loss of kyphotic correction. All of the parameters were significantly improved after surgery. Nevertheless, they were decreased considerably with statistical significance at the final observation when compared with that postoperatively. The mean correction losses of %AVB, VA, and RA were 10.2%, 2.9°, and 5.6° at the last follow-up, respectively.
 |
Table 2 Correction Loss of Kyphotic Deformity at Final Follow-Up |
The incidence of hardware failure was 16.7% (6/36). There were no patients who demonstrated screw loosening or loss of RA >10° (Table 3).
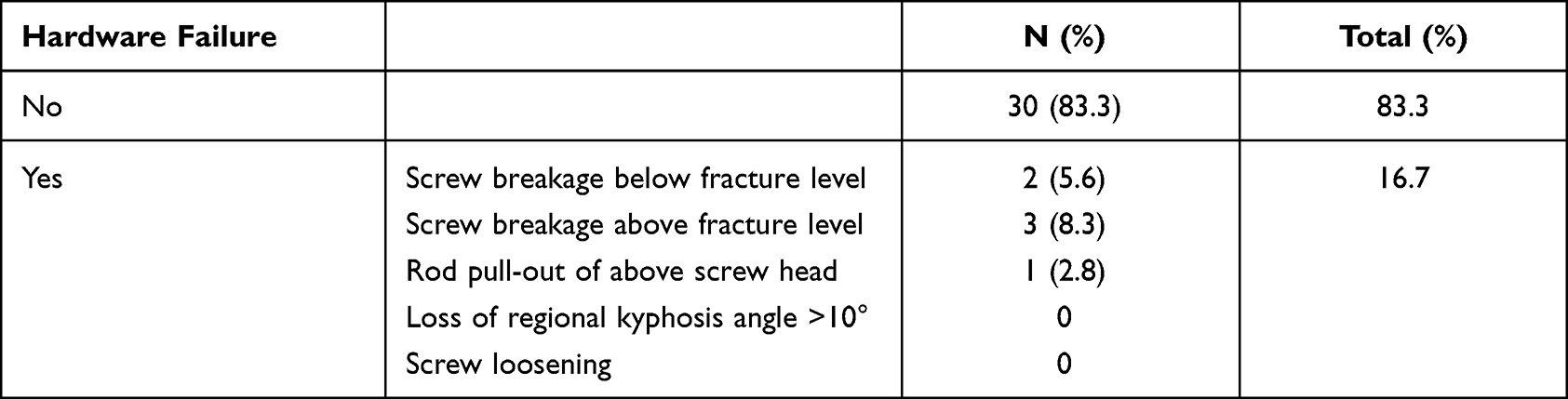 |
Table 3 The Prevalence of Hardware Failure |
According to Bridwell’s fusion grade using CT, six cases of hardware failure were classified as fusion grade I, 3 cases; grade II, 2 cases; and grade III, 01 case (Table 4).
 |
Table 4 CT Grading of Interbody Fusion Based on Bridwell’s Criteria |
Discussion
Traditional posterior surgery for the treatment of thoracolumbar burst fractures is a relatively straightforward surgical technique but can only provide indirect reduction of the fractured vertebral body, and the means of supporting the anterior column are limited.14,15 Several studies have reported that the loss of reduction caused by insufficient anterior column support with or without hardware failure was not uncommon.16,17 The posterior spinal fixation approach can be divided into long-segment fixation (fixation more than two upper and lower vertebral fractures) and short-segment fixation (involving one level above and one below the fractured level).
It has been proven that long segment fixation is strong enough to stabilize the fractured spine. However, the fused spine becomes less flexible and more susceptible to low back pain. Meanwhile, short-segment posterior fixation is thought to stabilize the fractured vertebra efficiently while saving motion segments compared to long segment fixation. However, previous studies reported earlier implant failure and correction loss as the most important disadvantages of this method.3,18 McLain et al reported 52.5% implant failure in their study on short-segment fixation in the treatment of thoracolumbar burst fractures.3 Thus, several techniques with anterior column intervention have been suggested as alternative methods to overcome this limitation. The kyphotic deformity was corrected to a considerable extent with posterior fixation and indirect reduction. With the help of the intact anterior longitudinal ligament and annulus of the intervertebral disc, it is easy to correct the kyphotic deformity of the fracture spine by posterior pedicle screw devices. How to address a large amount of bone defects inside the fractured vertebral body is a main problem. The large bone defect created inside the fractured vertebra after height restoration of the injured vertebral body has been speculated to be the most essential cause of that correction loss. Moreover, the restoration of the intervertebral disc height may also contribute to the loss of kyphotic correction.19 In addition, a usual laminectomy for the management of thoracolumbar burst fractures might lead to further spinal instability.20 It was hypothesized that the TIF might solve those problems by minimizing the correction loss. The TIF technique removes a part of the articular process on one side, and almost all spinal structures can be preserved. By impacting bone grafts into the intervertebral space and even into the vertebral body through the fractured endplate after disc excision, it is possible to reconstruct the anterior and middle columns of the fracture spine and stabilize the instability of the fractured vertebral body. Therefore, it may provide additional stability with short pedicle screw fixation. Wang et al recorded favorable outcomes without significant correction loss and hardware failure when short-segment pedicle screw fixation was combined with TIF using granulated bone grafts and cages for the treatment of thoracolumbar unstable burst fractures.5 However, the efficacy of TIF using bone chip grafts has not been reported.
Here, we report the radiological outcomes of short posterior fixation with TIF using bone chip grafts in the treatment of thoracolumbar unstable burst fracture, AO classification type A3, with a mean follow-up of 53 months. The correction of kyphotic deformity, which was evaluated by %AVB, VA and RA, was gradually lost, and the average correction loss was 10.2%, 2.9°, and 5.6°, respectively. Hardware failure occurred in 6 patients (16.7%) during the follow-up period, of which 3 cases of screw breakage above the fracture level (Figure 2A), 2 cases of screw breakage below the fracture level (Figure 2B), and one case with rod pull-out of the screw head (Figure 2C). These outcomes showed that TIF with bone chip grafts did not completely prevent the correction loss and hardware failure of short segment pedicle screw fixation for the treatment of thoracolumbar burst fractures. However, 4 out of 6 cases with hardware failures had good interbody fusion with Bridwell grade I or II (Figure 3), and none of these cases required revision surgery. To prevent hardware failure and correction loss of short-segment fixation in the treatment of thoracolumbar unstable burst fractures, several additional procedures have been introduced, but no ideal techniques have been proven.5 Vu et al reported the radiological outcomes of short posterior fixation and fusion for 31 patients with thoracolumbar burst fracture. They recorded 29% implant failure, while the mean correction losses of RA and VA were 2.3° and 7°, respectively.21 Liao et al reported the outcomes of 27 patients with thoracolumbar burst fracture who were treated with a six pedicle screw construct (group 1), and twenty-nine patients underwent a four screw construct and fractured vertebral augmentation by injectable calcium sulfate/phosphate cement (group 2). The authors found that the rate of hardware failure and the mean correction loss of %AVB and RA were 11.1%, 8.9° and 4.2° in group 1 and 27.6%, 13.3° and 6.3° in group 2, respectively.22
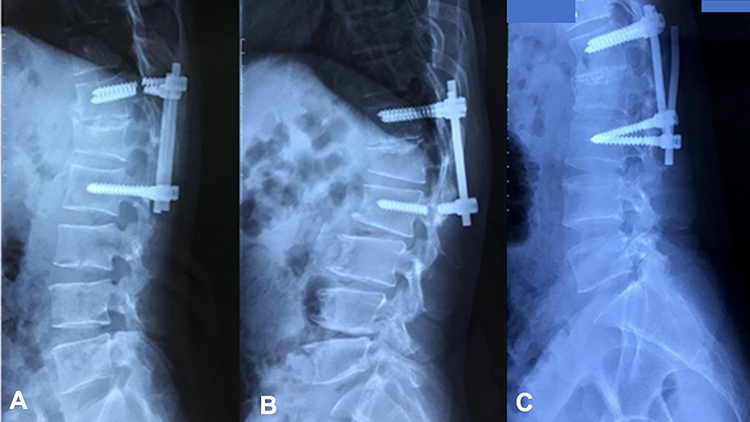 |
Figure 2 Implant failure: (A) breakage of pedicle screws above the fracture level; (B) breakage of pedicle screws below the fracture level; (C) rod pull out of the pedicle screw head. |
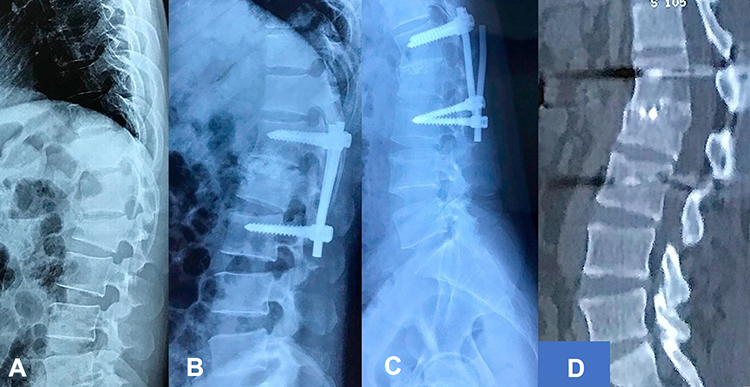 |
Figure 3 Good bone union in the patient with hardware failure: (A) preoperative X-ray; (B) postoperative X-ray; (C) final follow-up X-ray with hardware failure; (D) sagittal CT at last follow-up with good bone union. |
The role of posterior/posterolateral fusion in minimizing the late complications of short-segment fixation in the treatment of thoracolumbar burst fractures has been unclear, and several authors have suggested that posterior/posterolateral fusion is not necessary when treating thoracolumbar burst fractures with posterior pedicle screw fixation.23–25 Furthermore, we also wanted to accurately evaluate the outcomes of TIF with bone chip grafts in the prevention of poor radiological outcomes of short posterior instrumentation, so posterior/posterolateral fusion was not added in these case series. However, we suppose that posterior/posterolateral fusion in combination with TIF may provide better prevention of the disadvantages of short posterior fixation. Nevertheless, based on this study, we think that removal of implants after achievement of solid interbody fusion might be better than supplementation of posterior/posterolateral fusion in terms of reducing the hardware failure of short-segment posterior instrumentation, particularly in relation to implant failure of the distal unfused spine level, because it also simultaneously restores the motion of the unfused spine by the removal of instrumentation. However, further studies are needed to confirm these issues. There have been reports that posterior short-segment pedicle screw fixation combined with intermediate screw fixation at the fractured vertebrae can help improve biomechanical stability and achieve better reduction, cause less correction loss, and cause fewer hardware failures.26 However, Liao et al reported 3 cases of implant failure after using a six-screw construct in the treatment of 27 patients with thoracolumbar unstable burst fracture.22 Thus, we suppose that this technique combined with TIF using bone chip grafts may obtain better outcomes. However, further research is needed on this issue.
Regarding the surgical treatments of thoracolumbar burst fracture, temporary fixation or minimally invasive surgery may be a good choice. Temporary posterior instrumentation without fusion may be considered one of the useful alternative treatments for thoracolumbar unstable burst fracture in place of traditional posterior pedicle screw fixation and fusion. However, it was reported that this procedure was an effective treatment in patients with thoracolumbar unstable burst fracture who had a McCormack load-sharing score of less than 7 points.27 Percutaneous fixation alone28 without grafting or with thoracoscopically assisted corpectomy29 is sufficient for treating thoracolumbar burst fractures with satisfactory results. Minimally invasive techniques provide more advantages than traditional open approaches in the treatment of thoracolumbar burst fractures.30 However, these techniques also have drawbacks, such as increasing the radiation exposure to the patient and the surgeon because of fluoroscopy and a long learning curve.28 In addition, our technique may be changed to minimally invasive surgery by applying percutaneous pedicle screw fixation.
A limitation of this study was that patients who were involved in the research were all classified as having AO type A3 thoracolumbar burst fractures. This is a robust result of the study, on the one hand, by the AO type A3 classified as one of the most common types of fractures. On the other hand, there was a lack of comparisons of hardware failure and progressive kyphosis between the two LSC groups because of the small sample size. In addition, this study did not present an ideal method for the prevention of late complications of short-segment pedicle screw fixation in the treatment of thoracolumbar burst fractures. Nevertheless, this is the first report of these complications of short posterior fixation with TIF using bone chip grafts for the treatment of unstable thoracolumbar burst fractures in Vietnam.
Conclusions
TIF with bone chip grafts has not completely solved the disadvantages of short-segment pedicle screw fixation in the treatment of thoracolumbar unstable burst fractures. Correction loss after surgical management following this technique in long-term follow-up still occurred, and the incidence of hardware failure was 16.7%.
Abbreviations
TIF, transforaminal interbody fusion; %AVB, % loss of anterior vertebral body heights; VA, vertebral kyphotic angle; RA, regional kyphotic angle; CT, computed tomography; LSC, load sharing classification.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval and Consent to Participate
This research had already been approved by ethical committee in 108 Military Central Hospital, Hanoi city, Vietnam. Informed consent was obtained from all study participants, and the guidelines outlined in the Declaration of Helsinki were followed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983;8(8):817–831. doi:10.1097/00007632-198311000-00003
2. Alpantaki K, Bano A, Pasku D, et al. Thoracolumbar burst fractures: a systematic review of management. Orthopedics. 2010;33(6):422–429. doi:10.3928/01477447-20100429-24
3. McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am. 1993;75(2):162–167. doi:10.2106/00004623-199302000-00002
4. Schmid R, Krappinger D, Blauth M, Kathrein A. Mid-term results of PLIF/TLIF in trauma. Eur Spine J. 2011;20(3):395–402. doi:10.1007/s00586-010-1615-3
5. Wang L, Li J, Wang H, et al. Posterior short segment pedicle screw fixation and TLIF for the treatment of unstable thoracolumbar/lumbar fracture. BMC Musculoskelet Disord. 2014;15:40. doi:10.1186/1471-2474-15-40
6. Chadha M, Bahadur R. Steffee variable screw placement system in the management of unstable thoracolumbar fractures: a Third World experience. Injury. 1998;29(10):737–742. doi:10.1016/s0020-1383(98)00173-9
7. Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004;12(6):424–435. doi:10.5435/00124635-200411000-00007
8. Domenicucci M, Preite R, Ramieri A, et al. Thoracolumbar fractures without neurosurgical involvement: surgical or conservative treatment? J Neurosurg Sci. 1996;40(1):1–10.
9. McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine. 1994;19(15):1741–1744. doi:10.1097/00007632-199408000-00014
10. Farcy JP, Weidenbaum M, Glassman SD. Sagittal index in management of thoracolumbar burst fractures. Spine. 1990;15(9):958–965. doi:10.1097/00007632-199009000-00022
11. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The Clinical efficacy and outcome of nonoperative management. Spine. 1993;18(8):955–970. doi:10.1097/00007632-199306150-00003
12. Bridwell KH, Lenke LG, McEnery KW, Baldus C, Blanke K. Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine. 1995;20(12):1410–1418. doi:10.1097/00007632-199506020-00014
13. Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J. 1994;3(4):184–201. doi:10.1007/BF02221591
14. Been HD, Bouma GJ. Comparison of two types of surgery for thoraco-lumbar burst fractures: combined anterior and posterior stabilisation vs. posterior instrumentation only. Acta Neurochir. 1999;141(4):349–357. doi:10.1007/s007010050310
15. Hitchon PW, Torner J, Eichholz KM, Beeler SN. Comparison of anterolateral and posterior approaches in the management of thoracolumbar burst fractures. J Neurosurg Spine. 2006;5(2):117–125. doi:10.3171/spi.2006.5.2.117
16. Alanay A, Acaroğlu E, Yazici M, Aksoy C, Surat A. The effect of transpedicular intracorporeal grafting in the treatment of thoracolumbar burst fractures on canal remodeling. Eur Spine J. 2001;10(6):512–516. doi:10.1007/s005860100305
17. Knop C, Fabian HF, Bastian L, Blauth M. Late results of thoracolumbar fractures after posterior instrumentation and transpedicular bone grafting. Spine. 2001;26(1):88–99. doi:10.1097/00007632-200101010-00016
18. Müller U, Berlemann U, Sledge J, Schwarzenbach O. Treatment of thoracolumbar burst fractures without neurologic deficit by indirect reduction and posterior instrumentation: bisegmental stabilization with monosegmental fusion. Eur Spine J. 1999;8(4):284–289. doi:10.1007/s005860050175
19. Kerttula LI, Serlo WS, Tervonen OA, Pääkkö EL, Vanharanta HV. Post-traumatic findings of the spine after earlier vertebral fracture in young patients: clinical and MRI study. Spine. 2000;25(9):1104–1108. doi:10.1097/00007632-200005010-00011
20. Verlaan JJ, Diekerhof CH, Buskens E, et al. Surgical treatment of traumatic fractures of the thoracic and lumbar spine: a systematic review of the literature on techniques, complications, and outcome. Spine. 2004;29(7):803–814. doi:10.1097/01.brs.0000116990.31984.a9
21. Vu TT, Morishita Y, Yugue I, et al. Radiological outcome of short segment posterior instrumentation and fusion for thoracolumbar burst fractures. Asian Spine J. 2015;9(3):427–432. doi:10.4184/asj.2015.9.3.427
22. Liao JC, Fan KF. Posterior short-segment fixation in thoracolumbar unstable burst fractures - Transpedicular grafting or six-screw construct? Clin Neurol Neurosurg. 2017;153:56–63. doi:10.1016/j.clineuro.2016.12.011
23. Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012;94(8):1101–1106. doi:10.1302/0301-620X.94B8.28311
24. Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone Joint Surg Am. 2009;91(5):1033–1041. doi:10.2106/JBJS.H.00510
25. Wang ST, Ma HL, Liu CL, et al. Is fusion necessary for surgically treated burst fractures of the thoracolumbar and lumbar spine?: a prospective, randomized study. Spine. 2006;31(23):264652. doi:10.1097/01.brs.0000244555.28310.40
26. Li K, Zhang W, Liu D, et al. Pedicle screw fixation combined with intermediate screw at the fracture level for treatment of thoracolumbar fractures: a meta-analysis. Medicine. 2016;95(33):e4574. doi:10.1097/MD.0000000000004574
27. Ko S, Jung S, Song S, Kim J-Y, Kwon J. Long-term follow-up results in patients with thoracolumbar unstable burst fracture treated with temporary posterior instrumentation without fusion and implant removal surgery: follow-up results for at least 10 years. Medicine. 2020;99(16):e19780–e19780. doi:10.1097/MD.0000000000019780
28. Sebaaly A, Rizkallah M, Riouallon G, et al. Percutaneous fixation of thoracolumbar vertebral fractures. EFORT Open Rev. 2018;3(11):604–613. doi:10.1302/20585241.3.170026
29. Shawky A, Al-Sabrout AM, El-Meshtawy M, Hasan KM, Boehm H. Thoracoscopically assisted corpectomy and percutaneous transpedicular instrumentation in management of burst thoracic and thoracolumbar fractures. Eur Spine J. 2013;22(10):2211–2218. doi:10.1007/s00586-013-2835-0
30. Kocis J, Kelbl M, Kocis T, Návrat T. Percutaneous versus open pedicle screw fixation for treatment of type A thoracolumbar fractures. Eur J Trauma Emerg Surg. 2020;46(1):147–152. doi:10.1007/s00068-018-0998-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.