Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
The quality of consent form structure in biomedical research: a study from Jordan and Sudan
Authors Ibrahim MA, Alshogran OY ![]() , Khabour OF
, Khabour OF ![]() , Alzoubi KH
, Alzoubi KH ![]()
Received 13 June 2019
Accepted for publication 20 August 2019
Published 2 September 2019 Volume 2019:12 Pages 727—731
DOI https://doi.org/10.2147/JMDH.S219316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mariam Abbas Ibrahim,1 Osama Y Alshogran,2 Omar F Khabour,3 Karem H Alzoubi2
1Department of Clinical Chemistry, Sudan University of Science and Technology, Khartoum, Sudan; 2Department of Clinical Pharmacy, Jordan University of Science and Technology, Irbid 22110, Jordan; 3Department of Medical Laboratory Sciences, Jordan University of Science and Technology, Irbid 22110, Jordan
Correspondence: Omar F Khabour
Department of Medical Laboratory Sciences, Jordan University of Science and Technology, P.O. Box 3030, Irbid 22110, Jordan
Tel +962 655 730 6579
Email [email protected]
Background: Informed consent is one of the primary standards of ethical clinical research. This study assessed the quality of the informed consent forms (ICF) utilized in medical research conducted in Sudan and Jordan.
Subjects and methods: A total of 435 studies that were performed at health sciences schools in Jordan and Sudan were initially screened for the presence of ICF. Of these, 189 studies were reviewed for the major components of ICF using a standard checklist.
Results: The majority of the reviewed ICFs did not achieve the full standards of the universal guidelines for the informed consent structure. The following elements were described in >50% of consent forms reviewed from both countries: study title, objectives, research investigators, description of study procedure, and confidentiality. Other essential elements such as duration of the subject’s participation, risks/benefits, compensation, voluntary participation, and contact information were poorly described.
Conclusion: The major elements of ICFs were not adequately described in medical research studies from Jordan and Sudan. Improved understanding of major elements of ICF among researchers in the examined countries is necessary. Clear and informative consent template can be very valuable in this perspective.
Keywords: informed consent form, human research, medical sciences, Sudan, Jordan
Introduction
Informed consent process is one of the critical ethical and legal aspects of research involving human subjects.1 It reflects the voluntary nature of participation giving that subjects are aware of study objectives, procedures, and consequences. It is derived from the ethical principle of respect of the autonomy, indicating that subjects have the choice to decide whether to participate or not participate in a clinical study.2,3 The informed consent form (ICF) is the document that participants must sign before participating in a research that involves human.
The quality of ICFs varies depending on how much information is disclosed, content, readability, the adequacy of capacity, and level of understanding.4 The regulations of US Department of Health and Human Services reported that the ICF should contain statements that reflect study description, duration, risks and benefits, voluntary participation, confidentiality, ways of compensation to study subjects (if any), the participant’s right to withdraw, and contact information of investigators.5–7 This implies that disclosure, understanding, capacity, and voluntariness are the key elements of a valid ICF.8 One study evaluated the content and readability of ICF designed for diagnostic and therapeutic procedures in Croatia and found that 81% of ICFs included a description of benefits and only 17% mentioned risks and benefits of alternative procedures.9 Despite the presence of Institutional Review Board (IRB) committees that review and approve research protocols, informed consent process remains an ethical issue in medical research that needs further evaluation.10
The practice of obtaining the informed consent from participants is well-established in medical research. However, ICFs may not always satisfy subjects enrolled as necessary and relevant information might be missing.11 In China, 155 consent documents from clinical trials were reviewed.12 The results showed that ICFs used in China were difficult to read and had lower content integrity compared to international ones.12 One review article discussed the quality of informed consent and found that informed consent is worse in developing countries than in developed countries with respect to the comprehension of study information and rates of refusal and withdrawal.13 Proper and robust communication of major elements of ICF is another key feature of the appropriate informed consent process. Thus, studies that evaluate the adequacy of ICF to medical research among developing countries are necessary. This research is essential to monitor the quality of ICF and to suggest potential solutions for improvement.
As medical research in the medical field is expanded in the Middle East and North Africa (MENA) region, the need to comply with medical research ethics guidelines is essential. Yet, no information was found concerning the adequacy of ICF in MENA countries such as Sudan or Jordan. Thus, this study aimed at assessing the quality of ICF structure in biomedical research of indicated countries.
Methods
This was a retrospective cross-sectional study that included a convenience sample of studies that involved human subjects from various medical disciplines (Medical Laboratory Sciences, Medicine, Pharmacy, and Nursing) and was conducted in Sudan or Jordan during the last 5 years (2013–2018). Data were collected from dissertations/master thesis of medical research, which are publicly available through the library of each of the universities included in the study. A total of 435 (275 from Sudan and 160 from Jordan) dissertation/thesis were initially evaluated for the informed consent process/structure. However, only 41 studies from Sudan and 148 studies from Jordan had ICFs and IRB approval was included in the analysis. The ICFs were reviewed and evaluated for multiple aspects pertaining to the quality and structure. A checklist was used to evaluate what elements and information the investigator used to explain the study to the subjects. Data were collected between July and August 2018 in 2 universities from Jordan and 4 universities from Sudan, which were selected based on their international ranking among other universities from each country (https://www.topuniversities.com/university-rankings/world-university-rankings/2018).
The checklist form included information about discipline and the title of the study. In addition, the checklist covered major basic elements of the ICF including a statement that the study involves research, objectives, the expected duration of the subject’s participation, procedures, risks/potential benefits, compensation for participation, confidentiality statement, contact information of investigators, and signatures. This checklist was developed based on the international guidelines describing the primary elements of ICF.5 Two independent research assistants were involved in rating the consent form according to a prepared checklist. The intra-rater reliability and inter-rater reliability were 0.98 and 0.95, respectively.
Descriptive statistics (frequencies and percentages) were used to present the data. Data are available and will be provided to interested individuals upon request.
Results
The total number of human studies analyzed in this research was 189, comprising 41 (21.7%) studies from Sudan and 148 (78.3%) from Jordan.
Reviewing ICFs of studies from Sudan revealed that the following elements were described in >50% of consent forms: study title, objectives, research investigators, a description of study procedure, and a statement describing to what extent records will be kept confidential (Table 1). Among studies from Jordan, in addition to frequently (>50%) having all the former elements, other parts such as funding were also frequently described in the consent form (>50%) (Table 1). Other elements such as duration of the subject’s participation, risks/benefits, compensation, voluntary participation, and contact information were poorly described.
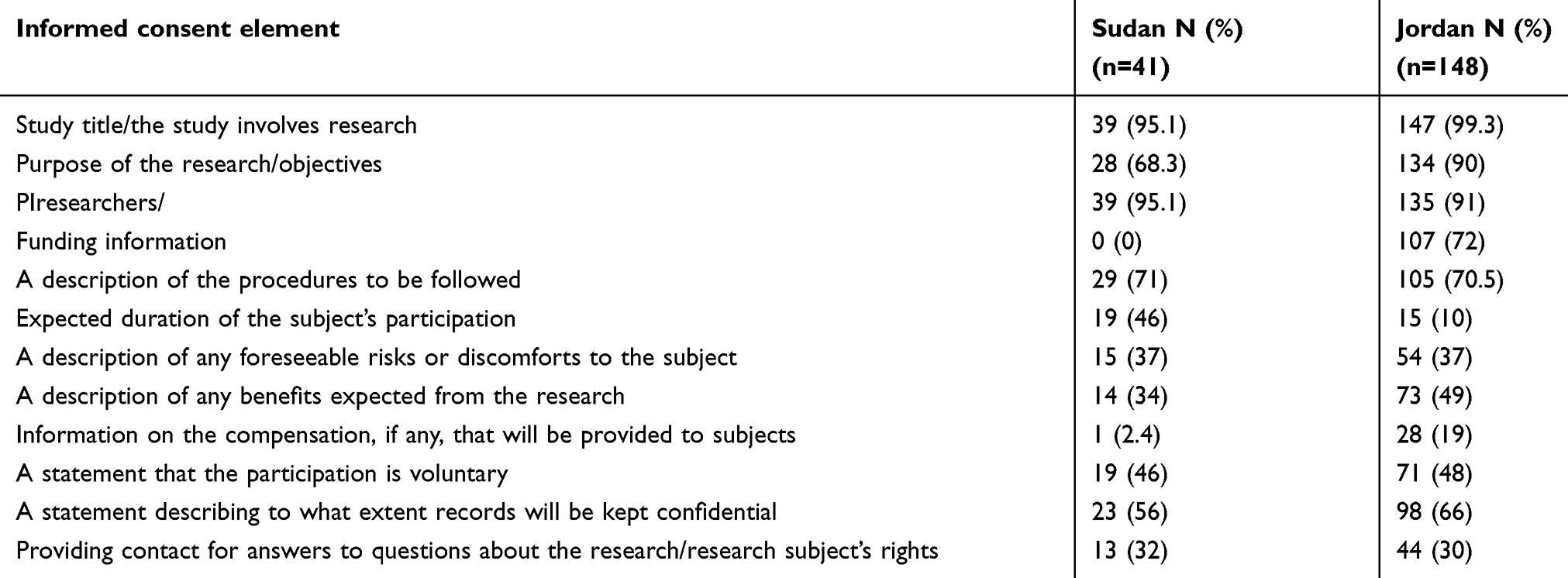 |
Table 1 Components of informed consent form: Sudan versus Jordan |
Discussion
Informed consent process is a fundamental ethical prerequisite of scientific research. Well-designed ICFs are essential to improve understanding of study subjects of the conducted research and to assure adequate protection of human subjects during their participation in research studies. To the best of our knowledge, this was the first study that evaluated the quality of ICFs among research studies from Sudanese versus Jordanian Universities. This retrospective study that covered the past 5 years (2013–2018) revealed that major elements of ICFs were not adequately described in research studies from Jordan and Sudan. More deficiencies have been recognized in the conception of ICF among research studies in Sudan as compared to Jordan. These observations suggest that improving the quality of informed consent process in clinical research in these regions is necessary.
A valid ICF should contain all necessary information and should be clear and written in a simple easy to read language.14 The current results showed that the majority of ICFs did not achieve the full standards of the template informed consent. This finding indicates that the accomplishment of all standards of ICF may often be not easy to attain. For example, major components of ICF are not adequately described. Funding, compensation, benefits, and contact information of researchers were minimally explained in the ICFs of Sudanese research. Only 37% of ICFs in either Jordan or Sudan described the study risk. This might be intentional as researchers may need to improve the enrollment by not clearly stating the risks of participation. These results are in part consistent with other investigations that showed poor readability and defects in the quality of consent documents among research conducted in China,12 France,15 and Croatia.9 Moreover, ICFs developed for pharmacogenetics research showed deficiencies and lower compliance with respect to sections of risks and benefits (41.7%) and compensation of participants (56.1%).16
The lack of a comprehensive and informative ICF might have negative implications on the quality of research and might potentially threaten subjects safety. For instance, subjects who are not clear about the research to be conducted might initially refuse to participate, withdraw during enrollment, or may be exposed to harm.17 It has been reported that inadequate education and training of researchers responsible for obtaining the informed consent may result in poor communication of research objectives, risks, and benefits.18 Therefore, educational programs about informed consent process would enhance the ability of researchers and the confidence of obtaining informed consent.19
The quality of informed consent depends on the clarity, comprehension, and amount of information disclosed. Much higher percentage (92.5%) of research studies from Jordan versus those from Sudan reported using ICF. This might be attributed to the better training about research ethics in Jordan, improved awareness of researchers about research integrity, the efficient implementation of IRB committees at good standards, and the higher level of education among research participants.20 Nevertheless, training about how to improve the development of ICFs in both regions is essential.
Previous studies have suggested some recommendations to improve the quality, content, length, and readability of ICFs such as use of section headings, illustrations, templates, and sample tests for researchers.15,21–23 Among the proposed solutions to improve ICF in the studied regions is to develop a template with high quality and standards, and so it communicates relevant information effectively and facilitates the process of informed consent. Research ethics committees should monitor the informed consent process to ensure that the clinical research is to be conducted in a way that protects the rights of human participants. Training on research ethics with the emphasis on how to develop an ICF could also significantly improves the quality of research in the region.
This study has some limitations. The ICFs were collected at one given point of time, using a convenient selection strategy aimed at finding documents available in the university’s libraries. The authors acknowledge that they may have missed some research that may contain informed consent documents. In addition, the absence of the ICF from the thesis/dissertation does not mean that the consent form was not utilized in the study. Finally, the study was focused on the presence/absence of essential elements of ICF but not its length, readability, and level of understanding, which are also major concerns of ICF.24–26 Future studies are recommended to cover these points.
Conclusion
Current results suggest the need for increasing awareness about informed consent among medical researchers in the region. In addition, the majority of ICFs used in medical research in Sudan and Jordan were not adequately developed and may not sufficiently fulfill their function of explaining relevant information to study subjects. Thus, training on research ethics with a focus on the development of ICFs is demanded. This would be critical to improve the achievements of the high ethical standards when conducting clinical research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Emanuel EJ, Wendler D, Killen J, Grady C. What makes clinical research in developing countries ethical? The benchmarks of ethical research. J Infect Dis. 2004;189(5):930–937. doi:10.1086/381709
2. del Carmen MG, Joffe S. Informed consent for medical treatment and research: a review. Oncologist. 2005;10(8):636–641. doi:10.1634/theoncologist.10-8-636
3. Nijhawan LP, Janodia MD, Muddukrishna BS, et al. Informed consent: issues and challenges. J Adv Pharm Technol Res. 2013;4(3):134–140. doi:10.4103/2231-4040.116779
4. Bhatt A. Improving quality of informed consent in clinical research. J Postgrad Med. 2015;61(4):221–222. doi:10.4103/0022-3859.166508
5. Grady C. Writing a Consent Form. In: Kelly W, Halabi S, eds. Oncology Clinical Trials: Successful Design, Conduct, and Analysis. Second edition ed. New York: Demos Medical Publishing; 2018:40.
6. Tanne JH. President’s commission considers how to protect human rights after guatemala experiment. BMJ. 2011;342:d3232. doi:10.1136/bmj.d3232
7. Shahnazarian D, Hagemann J, Aburto M, Rose S. Informed consent in human subjects research. University of Southern California: Office for the Protection of Research Subjects. 2017.
8. Tam NT, Huy NT, Thoa LTB, et al. Participants’ understanding of informed consent in clinical trials over three decades: systematic review and meta-analysis. Bull World Health Organ. 2015;93(3):186h–198h. doi:10.2471/BLT.14.141390
9. Vucemilo L, Borovecki A. Readability and content assessment of informed consent forms for medical procedures in Croatia. PLoS One. 2015;10(9):e0138017. doi:10.1371/journal.pone.0138017
10. Bhutta ZA. Beyond informed consent. Bull World Health Organ. 2004;82(10):771–777.
11. Montalvo W, Larson E. Participant comprehension of research for which they volunteer: a systematic review. J Nurs Scholarsh. 2014;46(6):423–431. doi:10.1111/jnu.12097
12. Wen G, Liu X, Huang L, et al. Readability and content assessment of informed consent forms for phase II-IV clinical trials in China. PLoS One. 2016;11(10):e0164251. doi:10.1371/journal.pone.0164251
13. Mandava A, Pace C, Campbell B, Emanuel E, Grady C. The quality of informed consent: mapping the landscape. A review of empirical data from developing and developed countries. J Med Ethics. 2012;38(6):356–365. doi:10.1136/medethics-2011-100178
14. Paasche-Orlow MK, Taylor HA, Brancati FL. Readability standards for informed-consent forms as compared with actual readability. N Engl J Med. 2003;348(8):721–726. doi:10.1056/NEJMsa021212
15. Menoni V, Lucas N, Leforestier JF, et al. The readability of information and consent forms in clinical research in France. PLoS One. 2010;5(5):e10576. doi:10.1371/journal.pone.0010576
16. Ruiz Ramos J, Cueto-Sola M, Garcia Robles A, Perez Huertas P, Tordera Baviera M, Poveda Andres JL. [Quality and legibility of written informed consent form in pharmacogenetic research]. Cuad Bioet. 2015;26(86):129–138.
17. Thaker SJ, Figer BH, Gogtay NJ, Thatte UM. An audit of consent refusals in clinical research at a tertiary care center in India. J Postgrad Med. 2015;61(4):257–263. doi:10.4103/0022-3859.166515
18. Nusbaum L, Douglas B, Damus K, Paasche-Orlow M, Estrella-Luna N. Communicating risks and benefits in informed consent for research: a qualitative study. Glob Qual Nurs Res. 2017;4:2333393617732017.
19. Koller SE, Moore RF, Goldberg MB, et al. An informed consent program enhances surgery resident education. J Surg Educ. 2017;74(5):906–913. doi:10.1016/j.jsurg.2017.02.002
20. Ahram M, Othman A, Shahrouri M. Public support and consent preference for biomedical research and biobanking in Jordan. Eur J Hum Genet. 2013;21(5):567–570. doi:10.1038/ejhg.2012.213
21. Koonrungsesomboon N, Laothavorn J, Chokevivat V, Hirayama K, Karbwang J. SIDCER informed consent form: principles and a developmental guideline. Indian J Med Ethics. 2016;1(2):83–86. doi:10.20529/IJME.2016.023
22. Koonrungsesomboon N, Teekachunhatean S, Hanprasertpong N, Laothavorn J, Na-Bangchang K, Karbwang J. Improved participants’ understanding in a healthy volunteer study using the SIDCER informed consent form: a randomized-controlled study. Eur J Clin Pharmacol. 2016;72(4):413–421. doi:10.1007/s00228-015-2000-2
23. Tait AR, Voepel-Lewis T, Malviya S, Philipson SJ. Improving the readability and processability of a pediatric informed consent document: effects on parents’ understanding. Arch Pediatr Adolesc Med. 2005;159(4):347–352. doi:10.1001/archpedi.159.4.347
24. Cheung WY, Pond GR, Heslegrave RJ, Enright K, Potanina L, Siu LL. The contents and readability of informed consent forms for oncology clinical trials. Am J Clin Oncol. 2010;33(4):387–392. doi:10.1097/COC.0b013e3181b20641
25. Christopher PP, Foti ME, Roy-Bujnowski K, Appelbaum PS. Consent form readability and educational levels of potential participants in mental health research. Psychiatr Serv. 2007;58(2):227–232. doi:10.1176/ps.2007.58.2.227
26. Sivanadarajah N, El-Daly I, Mamarelis G, Sohail MZ, Bates P. Informed consent and the readability of the written consent form. Ann R Coll Surg Engl. 2017;99(8):645–649. doi:10.1308/rcsann.2017.0188
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.