Back to Journals » Psoriasis: Targets and Therapy » Volume 16
The Psoriatic Disease Assessment Index (PSODAI) Score to Evaluate Systemic Involvement of Psoriasis
Authors Liang Y ![]() , Deng B, Ntawuyamara E
, Deng B, Ntawuyamara E ![]() , Bachelez H, Wang F, Zhang H, Zhang Z, Li Z, Dang L, Wang Y, Zou X, Wang L, Duan D, Chen H, Zheng W
, Bachelez H, Wang F, Zhang H, Zhang Z, Li Z, Dang L, Wang Y, Zou X, Wang L, Duan D, Chen H, Zheng W ![]() , Huang H, Zhang M, Cai Q, Chen Y, Zhang Y, Lu Z, Ren Y, Huang J
, Huang H, Zhang M, Cai Q, Chen Y, Zhang Y, Lu Z, Ren Y, Huang J
Received 21 June 2025
Accepted for publication 22 January 2026
Published 16 February 2026 Volume 2026:16 548700
DOI https://doi.org/10.2147/PTT.S548700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Enzo Errichetti
Yanhua Liang,1 Baoqing Deng,2 Epipode Ntawuyamara,3 Hervé Bachelez,4 Fuxi Wang,5 Hao Zhang,6 Zhenying Zhang,7 Zhengfeng Li,7 Lin Dang,8 Yajie Wang,1 Xianbiao Zou,9 Li Wang,10 Dejian Duan,11 Hongxiang Chen,12 Wenjun Zheng,13 Hui Huang,14 Min Zhang,15 Qingxian Cai,16 Ye Chen,17 Yingli Zhang,18 Zeyuan Lu,19 Yalin Ren,20 Jinxian Huang21
1Department of Dermatology, Cosmetology and Venereology, Shenzhen Hospital, Southern Medical University, Shenzhen, Guangdong, People’s Republic of China; 2Department of Dermatology, Shenzhen Baoan Center for Chronic Disease Control, Shenzhen, People’s Republic of China; 3Department of Dermatology and Venereology, University Teaching Hospital of Kamenge, University of Burundi, Bujumbura, Burundi; 4Department of Dermatology, Hôpital Saint-Louis, APHP & INSERM U1183, Imagine Institute for Human Genetic Diseases, Paris Cité University, Paris, France; 5Department of Dermatology, The Second People’s Hospital of Shenzhen, Shenzhen, Guangdong, People’s Republic of China; 6Department of Dermatology, Shenzhen Center for Chronic Disease Control, Shenzhen Institute of Dermatology, Shenzhen, Guangdong, People’s Republic of China; 7Department of Dermatology, the University of Hong Kong-Shenzhen Hospital, Shenzhen, Guangdong, People’s Republic of China; 8Department of Dermatology, Longgang Central Hospital, Shenzhen, Guangdong, People’s Republic of China; 9Department of Dermatovenerology & Medical Cosmetology, South China Hospital, Medical School, Shenzhen University, Shenzhen, People’s Republic of China; 10Department of Dermatology, Shenzhen Hospital Beijing University of Chinese Medicine, Shenzhen, People’s Republic of China; 11Department of Dermatology, Shenzhen Bao’an Chinese Medicine Hospital, Guangzhou University of Chinese Medicine, Shenzhen, People’s Republic of China; 12Department of Dermatology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Shenzhen, Guangdong, People’s Republic of China; 13Department of Dermatology and Venereology, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 14Department of Cardiology, The Eighth Affiliated Hospital of Sun Yat-Sen University, Shenzhen, People’s Republic of China; 15Department of Respiratory, The Second People’s Hospital of Shenzhen, Shenzhen, Guangdong, People’s Republic of China; 16National Clinical Research Center for Infectious Diseases, The Third People’s Hospital of Shenzhen, The Second Affiliated Hospital of Southern University of Science and Technology, Shenzhen, Guangdong, People’s Republic of China; 17Department of Gastroenterology, Integrative Clinical Microecology Center, Shenzhen Hospital, Southern Medical University, Shenzhen, Guangdong, People’s Republic of China; 18Shenzhen Mental Health Center, Shenzhen Kangning Hospital, Shenzhen, Guangdong, People’s Republic of China; 19Department of Endocrinology, The Eighth Affiliated Hospital of Sun Yat-sen University, Shenzhen, People’s Republic of China; 20Department of Ophthalmology, The University of Hong Kong-Shenzhen Hospital, Shenzhen, People’s Republic of China; 21Department of Medicine, Division of Rheumatology, The University of Hong Kong-Shenzhen Hospital, ShenzheN, Guangdong, People’s Republic of China
Correspondence: Yanhua Liang, Department of Dermatology, Cosmetology and Venereology, Shenzhen Hospital, Southern Medical University, 13 Xinhu Road, Shenzhen, Guangdong, 518101, People’s Republic of China, Tel +86-755-23360448, Email [email protected]
Background: To the best of our knowledge, no validated scoring instrument currently exists that comprehensively evaluates both cutaneous manifestations and systemic comorbidities of psoriasis. This multicenter study aimed to develop and validate a novel multidimensional scoring system addressing this clinical gap.
Methods: Under the guidance of the Shenzhen Psoriasis Academy, we conducted seven expert meetings to analyze existing evidence from PubMed, Wanfang, and CNKI databases. Through iterative Delphi consensus processes involving 26 specialists across 10 disciplines, we established the Psoriasis Disease Assessment Index (PSODAI). This 60-point composite instrument evaluates cutaneous involvement and nine key organ/system comorbidities. An accompanying online calculator (http://www.psodai.com.cn/) was developed for clinical implementation. Validation involved 254 psoriasis patients from six tertiary centers, with comparative analyses against PASI and DLQI metrics.
Results: The PSODAI framework stratifies disease severity as mild (0– 20), moderate (21– 40), and severe (41– 60). Comparative analysis revealed comparable proportions of moderate-to-severe cases between PSODAI and conventional tools (PASI/DLQI) (p> 0.05). Notably, 11 patients (4.3%) classified as severe by PASI were re-categorized as mild through PSODAI’s systemic evaluation, primarily due to limited extracutaneous manifestations.
Conclusion: As the first comorbidity-integrated assessment tool, PSODAI enables cross-specialty collaboration for holistic patient management. Its clinical adoption may facilitate timely comorbidity detection and preventive interventions. Further multicenter validation is warranted to confirm these preliminary findings.
Keywords: psoriasis, comorbidity, disease severity, systemic scoring, consensus
Introduction
Psoriasis is a chronic, recurrent, inflammatory, systemic disease caused by a combination of genetic and environmental factors.1 In addition to the skin, joints, fingers/toenails, palms and soles can be involved seriously affecting the quality of life of patients, and in a considerable proportion of patients are accompanied by a variety of comorbidities.2 With the development of psoriasis therapeutics, standard treatment should not only be to remove skin lesions but also to control psoriasis-associated comorbidities. Therefore, a practical, systematic evaluation of the patient’s global condition is a mandatory step in the holistic management of psoriasis patients.
A large set of epidemiological research shows that psoriasis is associated with a variety of comorbid conditions.3–5 A real-world study reported by Shah et al based on a total of 469,097 psoriasis patients identified 24 different comorbidities, among which the most common were hyperlipidemia, hypertension, depression, type 2 diabetes, and obesity.6
To now, the current psoriasis disease severity scoring tools are limited to skin lesions such as Psoriasis Area and Severity Index (PASI), Body surface area (BSA), Dermatology Life Quality Index (DLQI) and Patient Global Assessment Numerical Rating Scale (PtGA NRS) and Physician Global Assessment (PtGA).7–10 These scoring scales do not consider the systemic impact of psoriasis, and do not take into account comorbidities. Hence, a new assessment tool addressing both cutaneous disease and comorbid conditions is urgently needed. This article reports the outcome of a multidisciplinary consensus which led to the definition of the so-called Psoriatic Disease Assessment Index (PSODAI) scoring tool, with the objective to provide a practical and reproducible tool allowing the assessment in practice of the multiple organ disease impacts.
Materials and Methods
To improve the systemic psoriasis scoring tool, which we called the Psoriatic Disease Assessment Index (PSODAI), we referred to consensus development for health professionals as developed by Bory Kea and Benjamin.11 We followed five components:12 three inputs, the approach (consensus development), and the output as follow:
Defining the Task
Experts from Shenzhen Psoriasis Academy decided to develop a new scoring tool which helps to evaluate the severity of psoriasis and its comorbidities. SPA is an academic group of clinicians, researchers and dermatologists from different hospitals who are actively involved in psoriasis treatment in Shenzhen City.
Identifying and Recruitment of Participants
We identified and invited experts nationally and internationally involved in treatment of psoriasis including, dermatologists and specialists from other medical disciplines, different hospitals and universities among them rheumatologists, cardiologists, nephrologists, pneumologists, endocrinologists, gastroenterologists and ophthalmologists. Identification of these experts was based on the number of publications, administrative leadership and reputation or peer consensus. We included also psoriatic patients from 6 different hospitals who were scored using PSODAI.
Information
In addition to long experience of the participants, we searched PubMed, Wanfang database and China National Knowledge Infrastructure (CNKI), reviewed a large number of psoriasis studies, discussed in depth in seven group meetings online or on-site. For psoriasis comorbidities frequency weighting, we used data from a study by Shah et al6 which was conducted in USA.
Consensus Approach
We used an implicit approach by voting structure. After 5 months of discussion and 7 meetings, we constructed a final scheme for the PSODAI and an online application (http://www.psodai.com.cn/), which was approved during the round-table brain-storming discussion involving 26 experts from 10 medical specialties. After some comments and inputs to the initial version, all 26 experts approved it by vote.
To finalize and confirm the scientific validity of the PSODAI, we tested this new scoring method by evaluating 254 psoriatic patients from six hospitals in Shenzhen. These patients were evaluated for the first time using both commonly used methods (the PASI and DLQI) and the new PSODAI. We then compared these two scoring scales. The chi-square test was used to determine whether there was a statistically significant difference in disease severity between the PASI or DLQI, which are based only on skin lesions, and the PSODAI in view of systemic involvement. To determine whether there is a statistically significant difference between the two scoring tools (PASI/DLQI vs PSODAI) in identifying moderate-severe patients, we used McNemar’s Exact Test. The level of significance was set at a p value < 0.05.
Results
Evaluation of the Grade of Each Organ
Cutaneous Dysfunction
The severity of skin involvement is assessed by two scales, the objective PASI and the subjective feeling DLQI.7 Only higher PASI or DLQI scores were considered for scoring.
A PASI < 3 was defined as mild, with a score of 1 point; a PASI score between 3 and 9 was defined as moderate, with a score of 2 points; and a PASI score ≥10 was defined as severe, with a score of 3 points.
A DLQI < 6 is defined as mild, and 1 point is scored; a DLQI ranging from 6 to 9 is defined as moderate, with a score of 2 points; and a DLQI ≥ 10 is defined as severe, with a score of 3 points.
Cardiovascular Dysfunction
This PSODAI scoring system uses hypertension (HTA) and heart failure, the two most commonly seen conditions.
Hypertension
HTA grading standards followed the 2023 ESH Guidelines for The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension.13 Patients with HTA were categorized, and cardiovascular risk was classified as grade 1 (1 point), grade 2 (2 points) or grade 3 (3 points) HTA.
Heart Failure
It was assessed according to the New York Heart Association (NYHA) grading standards for cardiac function:14 grade I (0), II (1), III (2), or IV (3).
Metabolic Dysfunction
We used three evaluation criteria (blood glucose, blood lipids and uric acid) to assess the metabolic effects of psoriasis.15–17 The highest score is included in the total score.
Skeletal Dysfunction
We used the Disease Activity Index for Psoriatic Arthritis (DAPSA) to evaluate psoriasis joint comorbidities. The following PsA activity grades were used: 0–4, remission (0 points); 5–14, low (1 point); 15–28, moderate (2 points); and >28, high disease activity (3 points).18
Neuropsychological Dysfunction
The Depression and Anxiety Rating Scales were used to assess the degree of psychological involvement in psoriasis patients.19,20
Depression
Depression was scored using the 9-item Patient Health Questionnaire (PHQ-9):19 5–9 points for mild depression; 10–14 points for moderate depression; 15–19 points for moderately severe depression; and >20 points for severe depression.
Anxiety
Anxiety was assessed using the Generalized Anxiety Disorder Scale (GAD-7):20 0–4 points as minimal anxiety scored 0; 5–9 points as mild anxiety scored 1; 10–14 points as moderate anxiety scored 2; and 15–21 points as severe anxiety scored 3.
Renal Dysfunction
We used the chronic kidney disease (CKD) score to calculate the psoriasis renal comorbidity score. According to the CKD stage and albuminuria grade, the risk stratification of CKD is 0.5 points for low risk, 1 point for moderately increased risk, 1.5 points for high risk, and 3 points for very high risk.21
Respiratory Dysfunction
The 2021 guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease (COPD)22,23 was used to score the degree of lung involvement associated with psoriasis: Grade 0 (0.5 points), Grade I (1 point), Grade II (1.5 points) and Grade III (3 points).
Hepatic Dysfunction
The degree of hepatic insufficiency was graded according to biochemical indexes.24 We referred to modified Child-Pugh classification of the liver disease: class A (1.0 points), class B (2 points), and class C (3 points).25
Ocular Dysfunction
PSODAI uses the anatomical location classification method developed by the International Uveitis Study Group in 1987 to classify uveitis into anterior uveitis (0.5 points), intermediate uveitis (1 point), posterior uveitis (1.5 points) and panuveitis (3 points).26
Gastrointestinal (GI) Dysfunction
PSODAI score uses ulcerative colitis and Crohn’s disease severity scores to assess psoriatic digestive comorbidities.27,28
Ulcerative Colitis
The severity assessment of ulcerative colitis,29 which is mild (1 point), moderate (2 points) or severe (3 points).
Crohn’s Disease
The severity assessment of Crohn’s disease was mainly based on the Harvey simplified Crohn’s disease activity index,29 which indicated remission (1 point), moderate activity (2 points) and severe activity (3 points).
The Design of the PSODAI Scoring Tool
In the general plan for the systematic evaluation of psoriasis comorbidities, 10 systems, namely, skin, cardiovascular, metabolic, osteoarticular, neuropsychological, renal, pulmonary, hepatic, ocular and gastrointestinal tract; were included in the psoriasis systemic score. Each system was divided into 1 point, 2 points, and 3 points according to severity, for a total of 6 points. A score of zero (0) means normal body condition. Severity of some diseases was divided into 4 grades according to specific criteria, but the total score of 6 remains unchanged. Each system is scored only once, and if the system includes 2 or more comorbidities or scoring indicators, the highest score is taken into the overall assessment.
Then, each system is scored according to its severity. The incidence of psoriasis in different systems varies greatly; for example, direct addition cannot reflect the incidence or degree of psoriasis in different systems in the population. Therefore, to avoid this bias, each system score was multiplied by the corresponding frequency to obtain a weighted score. Finally, for the convenience of calculation, the weighted score is corrected and multiplied by 10 to get retained score. Then, we decided to take into calculation the value which is approximately close to 0 or 5.
The frequency of each system is based on real-world data published by Shah et al6 in 2017 to study the comorbidity burden of psoriasis patients in the United States. The scores are shown in Table 1.
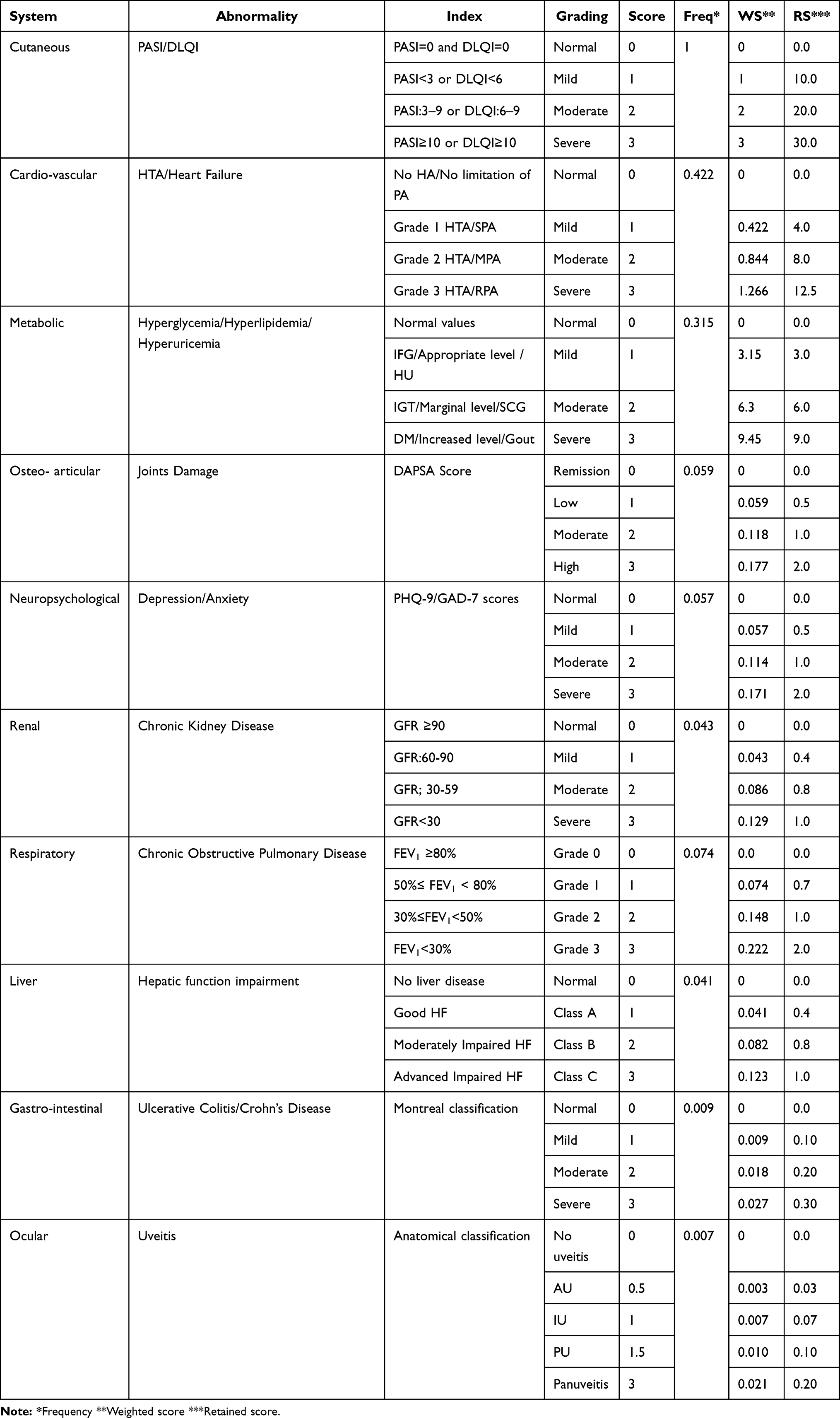 |
Table 1 Summary of the Psoriatic Disease Assessment Index |
The total score for the PSODAI is 60 if all 10 systems achieve severe results. To be consistent and comparable with the current use of the PASI or DLQI, we also classified the PSODAI scores as mild, moderate or severe, as detailed below: 0<20 points: Mild; 20≤PSODAI<40 points: Moderate; 40≤PSODAI≤60 points: Severe.
The Application of the PSODAI and Comparison with the PASI/DLQI
We evaluated a sample of 254 psoriatic patients from 6 hospitals by using the PASI and DLQI for the first time and the PSODAI for the second time. We classified the outcomes as mild, moderate or severe. For the first method, more patients had severe cutaneous involvement indicated by PASI or DLQI (94.49%), but more severe PASI/DLQI patients presented moderate scoring based on the newly assessment tool PSODAI (83.85%). It is worthy to mention that a few patients with severe skin lesions (11/240, 4.58%) may only show a mild systemic involvement. The difference between the two techniques was statistically significant (p=0.025) as shown in Table 2.
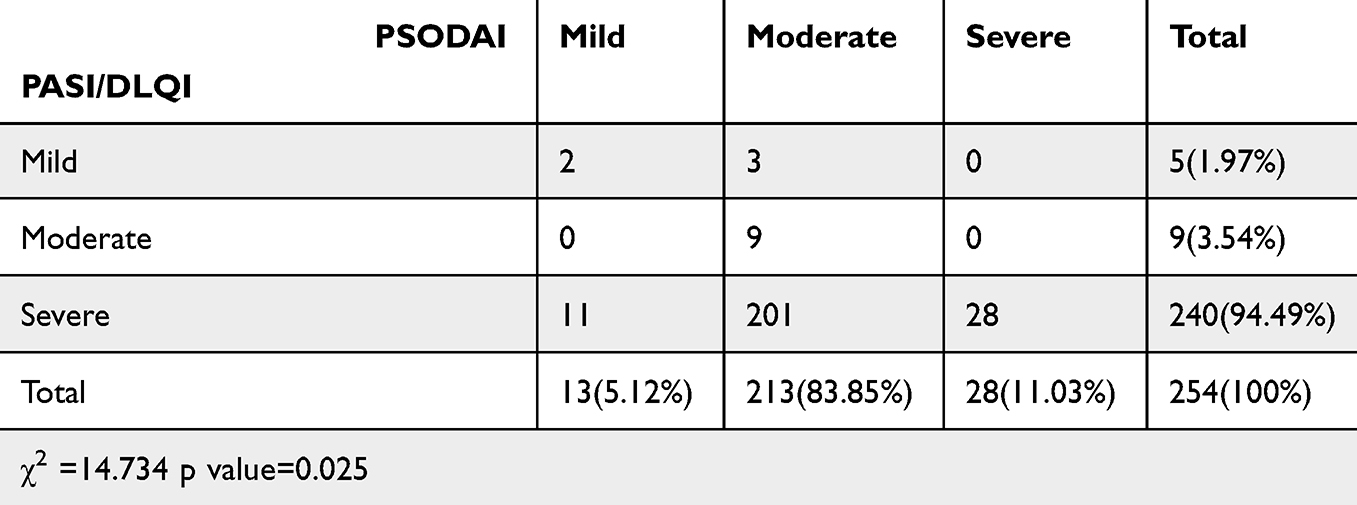 |
Table 2 Application of the PSODAI and Its Simultaneous Comparison to the PASI/DLQI Among 254 Patients |
Considering the criteria of biological use on psoriasis patients with the inclusion of moderate-severe condition, among these 254 patients, the total of moderate-severe patients respectively accounted for 249 (98.03%) in the PASI/DLQI pool and 241 (94.88%) among PSODAI group, showing no significant difference (p=0.057) in the proportion of moderate-severe form, clinically consistent for the decision to consider systemic treatments including biologics.
Discussion
Psoriasis is a complex chronic inflammatory skin disease caused by the dynamic interplay between multiple genetic risk foci, environmental risk factors, and excessive immunological abnormalities. It was once thought to affect only the skin and skeletal system of the human body, but it finally has been confirmed that psoriasis is a systemic inflammatory disease involving multiple systems.30 TNF-α and other inflammatory mediators can expose the body to chronic systemic inflammatory conditions that can induce insulin resistance, endothelial cell dysfunction and related cardiovascular diseases, as well as other comorbid diseases, such as MetS, CKD, and gastric or intestinal disorders and malignancies.30–33
Approximately 10 to 30% of patients with psoriasis develop PsA.34 PsA is an important subtype of psoriasis that requires the joint attention and management of dermatologists and rheumatologists. In addition, previous studies have shown that patients with PsA are more likely to have eye complications than are those with psoriasis. Routine eye examination is recommended for patients with PsA.35,36 Also, patients with PsA have a greater incidence of cardiovascular disease and MetS than other patients with inflammatory arthritis.37
Diverse risk factors; social (smoking, alcohol, physical activity); environmental (obesity), psychological (stress) are shared by psoriasis and cardiovascular diseases.38,39 Cardiovascular risk factors, such as hypercholesterolemia, diabetes, HTA, alcohol excess, and chronic kidney disease, should be screened for early psoriatic patients. Patients with psoriasis should be screened for these factors to avoid early occurrence of cardiac insufficiency or HTA. Obesity, type 2 diabetes, and insulin resistance are associated with inflammatory pathways involving specific inflammatory cytokines, such as TNF-α and IL-6, which are significantly elevated in psoriasis.40
Studies of related adipokines (such as leptin) have also indirectly confirmed the link between psoriasis and endocrine system diseases.41,42 Hyperleptinemia in psoriasis patients may be one of the causes of MetS.43
Psoriasis seriously affects the mental health of patients, and the risk ratio of depression is approximately 1.4~1.5 and increases with increasing disease severity.44,45 In patients with psoriasis, depression is associated with an increased risk of myocardial infarction, stroke, and cardiovascular death events, especially during acute depression.46
At present, traditional scores for the severity of psoriasis, such as the PASI, BSA, DLQI, and PtGA, only assess and determine the severity of skin lesions.7,10, However, the relevant standards for the overall assessment of psoriasis and its comorbidities are still lacking. To overcome this issue, we constructed a scoring method that includes all organs/systems targeted by psoriatic disease. The PSODAI considers not only skin lesions but also comorbid or systemic diseases associated with psoriasis. The PSODAI is the sum of points obtained by adding the maximum score for each system as follows: 30 points for skin, 12.5 points for cardiovascular, 9 points for endocrine, 1.5 points for osteoarticular, 1.5 points for neuropsychological, 1 point for urinary, 2 points for respiratory, 2.3 points for digestive and 0.2 points for eyes. The total score is 60 points. After obtaining scores from 10 organs/systems, the PSODAI classifies psoriatic disease into three forms as follows: mild, 0 to 20 points; moderate, >20–40 points; and severe, >40–60 points. If the retained score is zero, it will mean a normal body condition.
To confirm the accuracy of this scoring method for psoriatic disease, we evaluated a sample of 254 patients from 6 hospitals who were evaluated using traditional methods (PASI and DLQI). The evaluation results of the two methods were significantly different (p value=0.025). More patients (94.49%) had severe skin lesions according to the PASI or DLQI, and many patients (83.85%) are found to be moderate systemically evaluated by PSODAI method. The PSODAI plays a particular role in that case because, in addition to showing the severity of psoriasis and skin lesions, it can also show which comorbid disease the patient has and its severity. This will lead the physician who will consider the score to manage treatment or transfer patients if needed. This will also remind clinicians to begin early background treatment, such as biological treatment, to prevent the appearance of new comorbidities or worsening of existing comorbidities in psoriatic patients.
Limitations and Strengths
The formulation of this psoriatic disease scoring tool has some shortcomings, including but not limited to: (1) We used data from a study by Shah et al (2017)6 as reference for comorbidity frequency weighting. We basically made PSODAi referred to psoriasis vulgaris, the most common type of psoriasis which made difficult the correlation between different types of psoriasis and their score. Relying on one source for weighting may introduce bias. To our knowledge, this study remains of its kind with a sufficient sample size which shows different comorbidities related to psoriasis. We made a first step and recommend other studies which may or not adjust our application. (2) The PSODAI includes scoring for 10 systems, which may be overly complex and time-consuming for clinical application. We made online software which will help to fulfill this gap. (3) Even if we tested PSODAI on a sample of 254 patients from 6 different hospital of Shenzhen to validate it, the sample size is relatively small. We suggest more studies with larger and diverse patient population to strengthen PSODAI generalizability (4).
Conclusion
We developed a new severity scoring tool for systemic psoriasis, including 10 systems, which opens new perspectives for the exploration in practice of comprehensive and objective multidimensional evaluation of psoriasis including comorbidities by dermatologists and transdisciplinary specialists. After head-to-head real-world study in 254 patients, we found PSODAI is mostly consistent with PASI, with more accurate systemic evaluation. Such rigorous approach aims to improve the systematized concept of global management of psoriasis patients at an early stage of the disease.
IRB Approval Status
Reviewed and approved by Shenzhen Hospital of Southern Medical University IRB; approval number: NYSZYYCT2020017.
Abbreviations
PSODAI, Psoriatic Disease Assessment Index; GFR, Glomerular filtration rate; PASI, Psoriasis Area and Severity Index; DLQI, Dermatology Life Quality Index; HTA, Hypertension; PA, Physical Activity; SPA, Slight limitation of physical activity; MPA, Marked limitation of physical activity; RPA, Limitation of physical activity at rest; IFG, Impaired Fasting Glucose; IGT, Impaired glucose tolerance; DM, Diabetes mellitus; HU, Hyperuricemia; SCG, Subclinical gout; DAPSA, Disease Activity Index for Psoriatic Arthritis; PHQ, Patient Health Questionnaire; GAD, Generalized Anxiety Disorder; GOLD, Global Initiative for Chronic Obstructive lung Disease; FEV1, Forced Expiratory Volume in the first second of expiration; HF, Hepatic Function.
Data Sharing Statement
Data are available to the corresponding author and can be obtained upon written request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Patient Consent
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Funding
There is no funding to report.
Disclosure
Dr Hervé Bachelez reports personal fees from Anaptysbio, Boehringer Ingelheim, Eli Lilly, Janssen, Novartis, Sanofi, and UCB, outside the submitted work. The authors declare no other conflicts of interest in this work.
References
1. Zhang Xuejun ZJ. Dermatovenereology.
2. Armstrong AW, Pathophysiology RC. Clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–10. doi:10.1001/jama.2020.4006
3. Yang YW, Keller JJ, Lin HC. Medical comorbidity associated with psoriasis in adults: a population-based study. Br J Dermatol. 2011;165(5):1037–1043. doi:10.1111/j.1365-2133.2011.10494.x
4. Yamazaki F. Psoriasis: comorbidities. J Dermatol. 2021;48(6):732–740. doi:10.1111/1346-8138.15840
5. Bu J, Ding R, Zhou L, Chen X, Shen E. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol. 2022;13:880201. doi:10.3389/fimmu.2022.880201
6. Shah K, Paris M, Mellars L, Changolkar A, Mease PJ. Real-world burden of comorbidities in US patients with psoriatic arthritis. RMD Open. 2017;3(2):e000588. doi:10.1136/rmdopen-2017-000588
7. Zhang, et al. Guidelines for the Diagnosis and Treatment of Psoriasis in China: 2019 Concise Edition#. Int J Dermatology Venereol. 2020;3(1). https://journals.lww.com/ijdv/fulltext/2020/03000/guidelines_for_the_diagnosis_and_treatment_of.3.aspx.
8. Puzenat E, Bronsard V, Prey S, et al. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24(SUPPL. 2):10–16. doi:10.1111/j.1468-3083.2009.03562.x
9. Nikiphorou E, Radner H, Chatzidionysiou K, et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Ther. 2016;18(1):251. doi:10.1186/s13075-016-1151-6
10. Yu N, Peng C, Zhou J, et al. Measurement properties of the patient global assessment numerical rating scale in moderate-to-severe psoriasis. The British Journal of Dermatology. 2023;189:437–446. doi:10.1093/bjd/ljad188
11. Kea B, Sun BCA. Consensus development for healthcare professionals. Intern Emerg Med. 2015;10(3):373–383. doi:10.1007/s11739-014-1156-6
12. Eccles MP, Grimshaw JM, Shekelle P, Schünemann HJ, Woolf S. Developing clinical practice guidelines: target audiences, identifying topics for guidelines, guideline group composition and functioning and conflicts of interest. Implement Sci. 2012;7:60. doi:10.1186/1748-5908-7-60
13. Mancia G, Kreutz R, Brunström M, et al. ESH Guidelines for the management of arterial hypertension the task force for the management of arterial hypertension of the european society of hypertension: endorsed by the international society of hypertension (ish) and the european renal associat. J Hypertens. 2023;41(12):1874–2071. doi:10.1097/HJH.0000000000003480
14. White PD, Myers MM. The classification of cardiac diagnosis. J Am Med Assoc. 1921;77(18):1414–1415. doi:10.1001/jama.1921.02630440034013
15. Association AD. 2. classification and diagnosis of diabetes: standards of medical care in diabetes—2021. Diabetes Care. 2020;44(Supplement_1):S15–S33. doi:10.2337/dc21-S002
16. Reiner Ž, Catapano AL, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011;32(14):1769–1818. doi:10.1093/eurheartj/ehr158
17. Yamamoto T. Definition and classification of hyperuricemia. Nihon Rinsho. 2008;66(4):636–640.
18. Schoels MM, Aletaha D, Alasti F, Smolen JS. Disease activity in psoriatic arthritis (PsA): defining remission and treatment success using the DAPSA score. Ann Rheum Dis. 2016;75(5):811–818. doi:10.1136/annrheumdis-2015-207507
19. Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire (PHQ-9) - Overview. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
20. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
21. Cheung AK, Chang TI, Cushman WC, et al. KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3):S1–S87. doi:10.1016/j.kint.2020.11.003
22. Society COPDG of CT, Physician COPDC of CA of C. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021). Chin J Tuberc Respir Dis. 2021;44(3):170–205. doi:10.3760/cma.j.cn112147-20210109-00031
23. Laisure M, Covill N, Ostroff ML, Ostroff JL. Summarizing the 2021 updated GOLD guidelines for COPD. US Pharm. 2021;46(7):30–35.
24. Du XZZCYSG. Overview of graded approaches to hepatic insufficiency. Chinese Pharm. 2012;15(3):18–421.
25. Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 2005;60(8):646–649. doi:10.1002/bjs.1800600817
26. Discussion on the characteristics and causes of blindness caused by uveitis. Chinese J Fundus Dis. 2002;18(4):53–255.
27. Egeberg A, Thyssen JP, Burisch J, Colombel JF. Incidence and risk of inflammatory bowel disease in patients with psoriasis-a nationwide 20-year cohort study. J Invest Dermatol. 2019;139(2):316–323. doi:10.1016/j.jid.2018.07.029
28. Alinaghi F, Tekin HG, Burisch J, Wu JJ, Thyssen JP, Egeberg A. Global prevalence and bidirectional association between psoriasis and inflammatory bowel disease-a systematic review and meta-analysis. J Crohn’s Colitis. 2020;14(3):351–360. doi:10.1093/ecco-jcc/jjz152
29. Jiyao W. Internal Medicine.
30. Davidovici BB, Sattar N, Jörg PC, et al. Psoriasis and systemic inflammatory diseases: potential mechanistic links between skin disease and co-morbid conditions. J Invest Dermatol. 2010;130(7):1785–1796. doi:10.1038/jid.2010.103
31. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
32. Boehncke WH, Boehncke S, Tobin AM, Kirby B. The “psoriatic march”: a concept of how severe psoriasis may drive cardiovascular comorbidity. Exp Dermatol. 2011;20(4):303–307. doi:10.1111/j.1600-0625.2011.01261.x
33. Puig L. Cardiometabolic comorbidities in psoriasis and psoriatic arthritis. Int J Mol Sci. 2017;19(1):58. doi:10.3390/ijms19010058
34. Mease PJ. Psoriatic arthritis: update on pathophysiology, assessment and management. Ann Rheum Dis. 2011;70(1):i77–84. doi:10.1136/ard.2010.140582
35. Abbouda A, Abicca I, Fabiani C, et al. Psoriasis and psoriatic arthritis-related uveitis: different ophthalmological manifestations and ocular inflammation features. Semin Ophthalmol. 2017;32(6):715–720. doi:10.3109/08820538.2016.1170161
36. Vicente Delmás A D, Sanchez-Bilbao L, Calvo-Río V, et al. Uveitis in psoriatic arthritis: study of 406 patients in a single university center and literature review. RMD Open. 2023;9(1). doi:10.1136/rmdopen-2022-002781
37. Haque N, Lories RJ, De Vlam K. Comorbidities associated with psoriatic arthritis compared with non-psoriatic spondyloarthritis: a cross-sectional study. J Rheumatol. 2016;43(2):376–382. doi:10.3899/jrheum.141359
38. Zwain A, Aldiwani M, Taqi H. The association between psoriasis and cardiovascular diseases. Eur Cardiol. 2021;16e19. doi:10.15420/ecr.2020.15.R2
39. Masson W, Lobo M, Molinero G. Psoriasis and cardiovascular risk: a comprehensive review. Adv Ther. 2020;37(5):2017–2033. doi:10.1007/s12325-020-01346-6
40. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–867. doi:10.1038/nature05485
41. Taylor EB. The complex role of adipokines in obesity, inflammation, and autoimmunity. Clin Sci. 2021;135(6):731–752. doi:10.1042/CS20200895
42. Pestel J, Blangero F, Watson J, Pirola L, Eljaafari A. Adipokines in obesity and metabolic-related-diseases. Biochimie. 2023;212:48–59. doi:10.1016/j.biochi.2023.04.008
43. Chen YJ, Wu CY, Shen JL, et al. Psoriasis independently associated with hyperleptinemia contributing to metabolic syndrome. Arch Dermatol. 2008;144(12):1571–1575. doi:10.1001/archderm.144.12.1571
44. Schmitt J, Ford DE. Psoriasis is independently associated with psychiatric morbidity and adverse cardiovascular risk factors, but not with cardiovascular events in a population-based sample. J Eur Acad Dermatol Venereol. 2010;24(8):885–892. doi:10.1111/j.1468-3083.2009.03537.x
45. Kurd SK, Troxel AB, Crits-Christoph P, Gelfand JM. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146(8):891–895. doi:10.1001/archdermatol.2010.186
46. Egeberg A, Khalid U, Gislason GH, Mallbris L, Skov L, Hansen PR. Impact of depression on risk of myocardial infarction, stroke and cardiovascular death in patients with psoriasis: a Danish nationwide study. Acta Derm Venereol. 2016;96(2):218–221. doi:10.2340/00015555-2218
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.