Back to Journals » Cancer Management and Research » Volume 17

The Prophylactic Role of Hyperthermic Intraperitoneal Chemotherapy on Spontaneously Ruptured Hepatocellular Carcinoma with Radical Resection: A Retrospective Study
Authors Li Z ![]() , Lin J, Gao K, Dang X, Hua Y
, Lin J, Gao K, Dang X, Hua Y ![]()
Received 4 September 2025
Accepted for publication 9 December 2025
Published 22 December 2025 Volume 2025:17 Pages 3241—3258
DOI https://doi.org/10.2147/CMAR.S555348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Zhichao Li, Junlong Lin, Kai Gao, Xi Dang, Yunpeng Hua
Hepatobiliary and Pancreatic Center, the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China
Correspondence: Yunpeng Hua, Email [email protected]
Background: Spontaneous rupture of hepatocellular carcinoma (srHCC) carries a high risk of peritoneal metastasis and poor prognosis. While hyperthermic intraperitoneal chemotherapy (HIPEC) is established for peritoneal metastases in other cancers, its prophylactic role after radical resection of srHCC remains undefined. This study evaluated the efficacy and safety of HIPEC in improving outcomes for srHCC patients post-hepatectomy.
Methods: In this retrospective study, 77 patients with srHCC undergoing hepatectomy (2016– 2022) were categorized into the HR-HIPEC group (n=30) and the non-HIPEC group (n=47). Clinical features and survival data were analyzed.
Results: The HR-HIPEC group demonstrated significantly superior median overall survival (OS: 44 vs 35 months; P=0.027) and recurrence-free survival (RFS: 44 vs 25 months; P=0.007). The 3-year OS (73.85% vs 44.17%) and RFS (54.72% vs 24.47%) rates were also higher with HIPEC. Multivariate analysis identified HIPEC as an independent protective factor for both OS (HR=9.301, P< 0.001) and RFS (HR=2.159, P=0.044). Postoperative recovery, morbidity, and mortality were comparable between groups. Subgroup analysis of HIPEC regimens (gemcitabine/cisplatin vs oxaliplatin/5-FU/folinic acid) revealed no significant differences in efficacy, though the latter was associated with transiently lower hemoglobin (P=0.006).
Conclusion: Prophylactic HIPEC is a safe and feasible adjunct to hepatectomy that significantly improves survival outcomes in srHCC patients without increasing perioperative risks. The choice between the two chemotherapy regimens studied did not affect efficacy, warranting further investigation to optimize protocols.
Keywords: liver resection, hepatocellular carcinoma, hyperthermic intraperitoneal chemotherapy
Hepatocellular carcinoma (HCC) represents a major global health burden, constituting the third most prevalent cause of cancer-associated mortality as documented in 2020 epidemiological reports.1,2 Projections from the International Agency for Research on Cancer (IARC) and World Health Organization (WHO) indicate a 55% surge in both HCC incidence and mortality by 2040,3 posing substantial challenges to global hepatic oncology management and necessitating urgent development of innovative therapeutic approaches. Of particular clinical significance, spontaneous tumor rupture emerges as a devastating complication associated with acute mortality rates exceeding 60% and representing the third most prevalent cause of HCC-related fatalities.4,5 Although contemporary clinical evidence has established that transcatheter arterial embolization (TAE) combined with surgical resection confers enhanced short-term survival benefits and reduced perioperative morbidity in patients with spontaneous rupture,6 long-term outcomes for these patients remain suboptimal due to peritoneal carcinomatosis and hepatic micrometastases originating from disseminated neoplastic cells.4,7 Therefore, this pathophysiological mechanism underscores the imperative to develop targeted perioperative interventions capable of eradicating residual malignant cells.
Peritoneal lavage with distilled water (DW) has been established as a standard surgical adjunct in the management of abdominal malignancies, particularly colorectal, urological, and gastric carcinomas. One study by Zhou S et al7 provided evidence that DW lavage significantly improved long-term outcomes in patients undergoing liver resection for srHCC, though its therapeutic efficacy appears constrained to mechanical tumor cell clearance without addressing micrometastatic disease.
Hyperthermic intraperitoneal chemotherapy (HIPEC), involving the infusion of chemotherapeutic agents into the abdominal cavity at a controlled temperature (43°C) for a specified duration (30–90 minutes),8 has been shown to be effective in treating peritoneal carcinomatosis (PC) and malignant ascites associated with gastrointestinal, gynecological, and hepatobiliary malignancies.9,10 The tripartite mechanism of HIPEC encompasses: (1) Thermochemical Synergy: Hyperthermia increases peritoneal-tissue drug concentration gradients by 4.7-fold through enhanced vascular permeability; (2) Immunogenic Modulation: Heat shock protein 70 (HSP70) mediated NK cell activation (2.3-fold increase in CD56+ cells); (3) Molecular Targeting: Simultaneous inhibition of VEGF-mediated angiogenesis (78% reduction) and induction of caspase-3 dependent apoptosis.11 However, studies on HIPEC for srHCC patients undergoing hepatectomy are limited, with contradictory results, small sample sizes, and a lack of controlled studies.11,12 Given these considerations, this retrospective study aims to systematically evaluate the safety profile and therapeutic efficacy of HIPEC combined with radical hepatectomy and intraoperative distilled water lavage in patients with srHCC. Through rigorous analysis of a large-scale clinical cohort from our tertiary hepatobiliary center, we seek to establish an evidence-based framework to optimize multimodal therapeutic strategies for HCC management, with particular emphasis on improving oncological outcomes in this high-risk patient population.
Methods
Study Population
This retrospective cohort study meticulously selected patients who underwent hepatectomy for spontaneously ruptured hepatocellular carcinoma at The First Affiliated Hospital of Sun Yat-sen University (Guangzhou, China) between August 2016 and August 2022.
Selections were eligible when meeting the criteria: i) Aged from 18 to 80; ii) Clinical diagnoses of srHCC: acute abdominal pain and peritonitis; blood routine tests: decreased erythrocyte count; increased leucocyte count, especially the proportion of neutrophils; increased alpha-fetoprotein (AFP) and/ or protein induced by vitamin K absence or antagonist-II (PIVKA-II); radiological features: contrast materials extravasation from lesions confirmed by abdominal contrast enhanced computed tomography or gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance imaging (MRI); intraoperative findings of tumor rupture and postoperative pathology are more confidently conclusive; iii) ECOG score of 0–2 points; iv) Child-Pugh class A liver function only; and v) Received emergency laparotomy or staged hepatectomy.
Exclusion criteria were as follows: i) Contraindications of HIPEC, including intra-abdominal adhesions, intestinal obstruction, severe renal insufficiency, myelosuppression, severe cardiovascular system disease, abdominal infection, bleeding tendency or coagulation dysfunction, severe pulmonary system disease, vital signs are unstable, cachexia; ii) Patients who refuse to accept HIPEC; iii) antecedent malignancies or metastatic liver cancer, or established distant metastases; iv) Incomplete resection classified as R1.
This retrospective study was conducted in accordance with the Declaration of Helsinki (2013 revision) and approved by the Institutional Review Board (IRB) of The First Affiliated Hospital of Sun Yat-sen University, China (approval number: [2015]124, date: September 10, 2015).
Due to the retrospective nature of the study and the use of de-identified patient data, the requirement for informed consent was waived by the IRB.
The initial analysis encompassed 107 subjects, which were divided into two groups according to with or without postoperative hyperthermic intraperitoneal chemotherapy (HIPEC): HR-HIPEC group (n=47) and non-HIPEC group (n=60). However, nineteen cases of liver metastasis from colorectal, ovarian, and gallbladder cancers, two cases with distant metastasis evident, were excluded. Additionally, nine cases without HIPEC were lost to follow-up. Finally, 77 patients included HR-HIPEC group (n=30) and non-HIPEC group (n=47), remained eligible for the study, and facilitated a comparative analysis of treatment efficacy and patient outcomes (Figure 1).
 |
Figure 1 Flow diagram of patient selection. |
Surgical & HIPEC’s Technique
All patients underwent surgery, including minimally invasive/open approaches, with surgical strategy determined by multidisciplinary consensus based on preoperative triphasic CT/MRI findings and intraoperative exploration.
Peritoneal lavage with more than 5 L of DW was performed for 15 min after liver resection in all cases of ruptured HCC. The placement of four perfusion tubes was done for intraperitoneal thermal perfusion chemotherapy after hepatectomy. One thermal perfusion tube (inflow tube) was placed at the level of the anterior axillary line in the hepatic and renal fossa or splenic fossa. The other thermal perfusion tube (outflow tube) was placed at the level of the anterior axillary line in the pelvic floor of the bilateral pelvic floor, and the multi-perforated closed drainage system were drained out of the abdomen through the poke holes in the abdominal wall of the two sides, respectively. The up and down perfusion tubes were crossed to form an “X” shape. The inflow tube of the thermal perfusion tube was placed near the primary tumor lesion, and the outflow tube of the thermal perfusion tube was placed far away from the primary tumor area. The abdomen was closed after checking again that there was no abnormality in the operative field and the ports of the drainage tubes (Figure 2).
 |
Figure 2 Schematic diagram of HIPEC. |
Patients in the HR-HIPEC cohort underwent comprehensive physiological assessment 48–72 hours postoperatively to confirm treatment eligibility, including evaluation of hemodynamic stability (sustained MAP ≥65 mmHg for >6 hours, urine output >0.5 mL/kg/h), hematologic parameters (platelet count ≥80×109/L, INR ≤1.5), and biochemical markers (serum creatinine ≤1.5 mg/dL, ALT/AST <3×ULN).
Qualified patients received three standardized HIPEC cycles using the BR-TRG-I system (Bright Medical Tech, China) under closed-loop temperature feedback control (43.0°C ±0.1°C), with each 60–90-minute session delivering 4–6 L of perfusate to ensure complete peritoneal cavity coverage. The entire process was controlled by a computer-based automated system.
The chemotherapeutic regimens consisted of platinum (cisplatin or oxaliplatin) + pyrimidine (gemcitabine or 5-FU), including 16 patients with gemcitabine (800–1000 mg/m2) + cisplatin (75–100 mg/m2) and 14 patients with oxaliplatin (100–150 mg/m2)+ 5-FU (1000–1500 mg)+ folic acid (200–300 mg/m2) in this study. Procedures were conducted by a multidisciplinary team comprising an attending hepatobiliary surgeon (≥10 years HIPEC experience), certified perfusion technician, and critical care nurse specialist, with continuous physiological monitoring (pulse oximetry, core temperature via esophageal probe) and standardized premedication (promethazine 25 mg IV + midazolam 0.05 mg/kg IV) to optimize patient tolerance.
Pathological Verification and Follow-Up
Histopathological confirmation of hepatocellular carcinoma was universally established through expert review utilizing the Edmondson-Steiner grading system. Postoperative surveillance adhered to a rigorous protocol: clinical evaluations incorporating serum AFP/PIVKA-II quantification and multiphasic imaging (contrast-enhanced ultrasound/CT/MRI) were conducted quarterly during the initial 6-month period, transitioning to biannual assessments thereafter, supplemented by structured telemedicine consultations. Tumor recurrence/metastasis required radiologic confirmation per RECIST 1.1 criteria with concurrent AFP elevation (>20 ng/mL). Primary endpoints included overall survival (OS), defined as the duration from surgical intervention to all-cause mortality (data censored August 10, 2022), and recurrence-free survival (RFS), calculated from resection to first confirmed recurrence. Postoperative complications were classified according to Clavien-Dindo criteria (Grade II–V), encompassing hepatobiliary events (ISGLS-defined posthepatectomy liver failure), surgical complications (bile leakage: bilirubin-rich drainage>5 days with fluid/serum bilirubin ratio>3), and cardiopulmonary dysfunction (PaO2/FiO2 <300). Thirty-day mortality was rigorously documented, with independent adjudication by an endpoint review committee to ensure event attribution accuracy.
Statistical Analysis
All statistical analyses were performed with Statistical Package for the Social Sciences (SPSS) (version 24.0; IBM Inc., Armonk, NY). Categorical data are expressed as frequencies (percentages). Continuous variables are expressed as the mean ± standard deviation for normally distributed variables or as the median (interquartile range) for non-normally distributed variables. Continuous variables were compared using Student t test. Categorical variables were compared using Pearson χ2 test or Fisher exact test. Survival analysis was performed with the Kaplan-Meier method and a Log rank test. Prognostic factors for survival were investigated with univariable and multivariable Cox regression analyses. All P values are 2-sided, and P <0.05 is considered statistically significant.
Results
Patient Characteristics
Between August 1, 2016, and August 10, 2022, 77 patients were included in the study: 47 in the non-HIPEC group and 30 in the HR-HIPEC group. There were no significant differences in age, gender, AFP levels, tumor size, MVI, or liver cirrhosis between the two groups (Table 1).
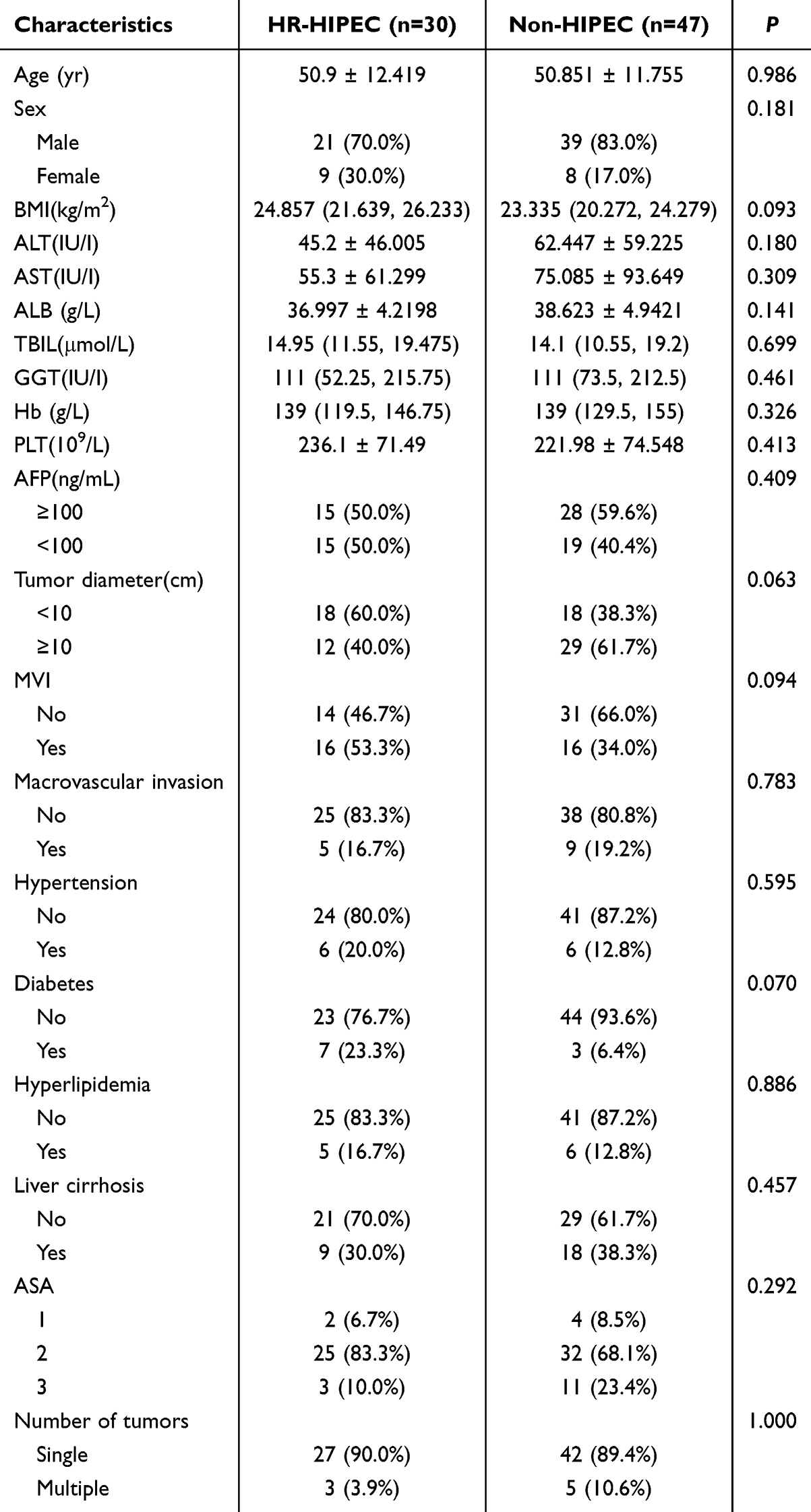 |
Table 1 Baseline Characteristics in HIPEC and Non-HIPEC Groups |
Peri-Operative Outcomes
There were also no statistically significant differences in terms of operative parameters, such as operation time, intraoperative bleeding, the postoperative serum biochemical indices, postoperative hospital stay, postoperative morbidity and mortality, and readmission rate, etc (Table 2).
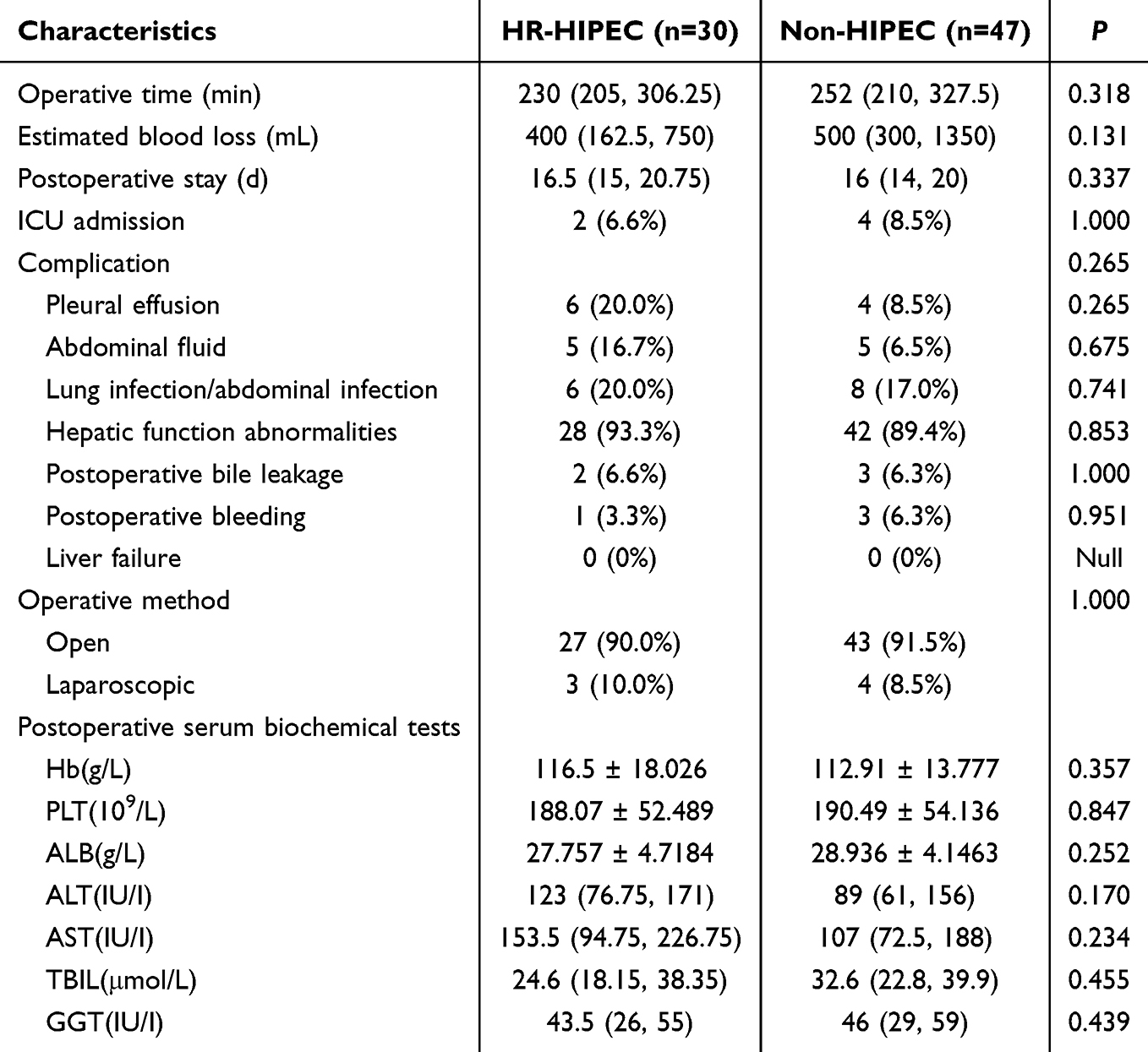 |
Table 2 Peri-Operative Outcomes in HIPEC and Non-HIPEC Groups |
On the fifth day after surgery, the serum biochemical indices after the completion of three hyperthermic perfusion chemotherapy sessions did not reveal any statistically significant differences between the two groups, though the mean levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) in the HR-HIPEC group were somewhat higher (123 and 153.5, respectively) than those in the non-HIPEC group (89 and 107, respectively), but the differences were not statistically significant. (P=0.170 for ALT, P=0.234 for AST). In terms of postoperative complications, 6 (20.0%) patients in the HR-HIPEC group developed pleural effusion, 5 (16.7%) developed peritoneal effusion, 6 (20.0%) developed lung or (and) abdominal cavity infection, 2 (14.3%) developed bile leakage, and 1 (7.1%) developed abdominal hemorrhage. However, in the non-HIPEC group, there were 4 (8.5%) cases of pleural effusion, 5 cases (6.5%) of abdominal effusion, 8 cases (17.0%) of lung/abdominal infection. The above postoperative complications could overlap, and all enrolled cases did not undergo re-operation. There was no significantly statistical difference in postoperative complications between the two groups.
Survival Outcomes
In the HR-HIPEC group, 12 (40.0%) patients experienced recurrence and 9 deaths (33.3%) by the end of the follow-up period. However, in 47 patients of the non-HIPEC group, there were 24 recurrences (51.1%) and 22 deaths (46.8%). In addition, the median overall survival of the HR-HIPEC group was 44 months with a hazard ratio of 2.293 (95% CI: 1.134, 4.639), compared to the non-HIPEC group (median OS: 35 months), which the risk of death was 2.29 times higher than the HR-HIPEC group. Furthermore, the three-year overall survival rates for the two groups were 44.17% and 73.85%, and the five-year overall survival rate for the non-HIPEC group was 15.70%, while it was undefined in the HR-HIPEC group (P= 0.0273; Figure 3A). The median RFS of the HR-HIPEC group was 44months, and it is still more than that of the non-HIPEC group (25 months), with a hazard ratio of 2.253 (95% CI: 1.264, 4.016), P=0.0068 (Figure 3B), means the risk of recurrence was 2.25 times higher in non-HIPEC group. Furthermore, the three-year recurrence-free survival rates for the two groups were 44.17% and 73.85%, and the five-year recurrence-free survival rate for the non-HIPEC group was 15.70%, however it was undefined in the HR-HIPEC group either.
 |
Figure 3 (A) Analysis of overall survival in patients treated with HR-HIPEC group or non-HIPEC group; (B) Analysis of recurrence-free survival in patients treated HR-HIPEC group or non-HIPEC group. |
Risk Factor Analysis of OS and RFS
In the context of overall survival (OS), the univariate Cox regression analysis revealed predictors of prognosis, encompassing elevated total bilirubin (≥17 μmol/L), MVI, Hyperlipidemia, liver cirrhosis, macrovascular invasion, and HIPEC (Table 3). Multivariate analysis further refined the independent predictors of prognosis to tumor size (HR 2.774, P=0.027), MVI (HR 7.987, P<0.001), liver cirrhosis (HR 3.521, P=0.009), macrovascular invasion (HR 4.184, P=0.002), and the conduct of HIPEC (HR 9.301, P<0.001).
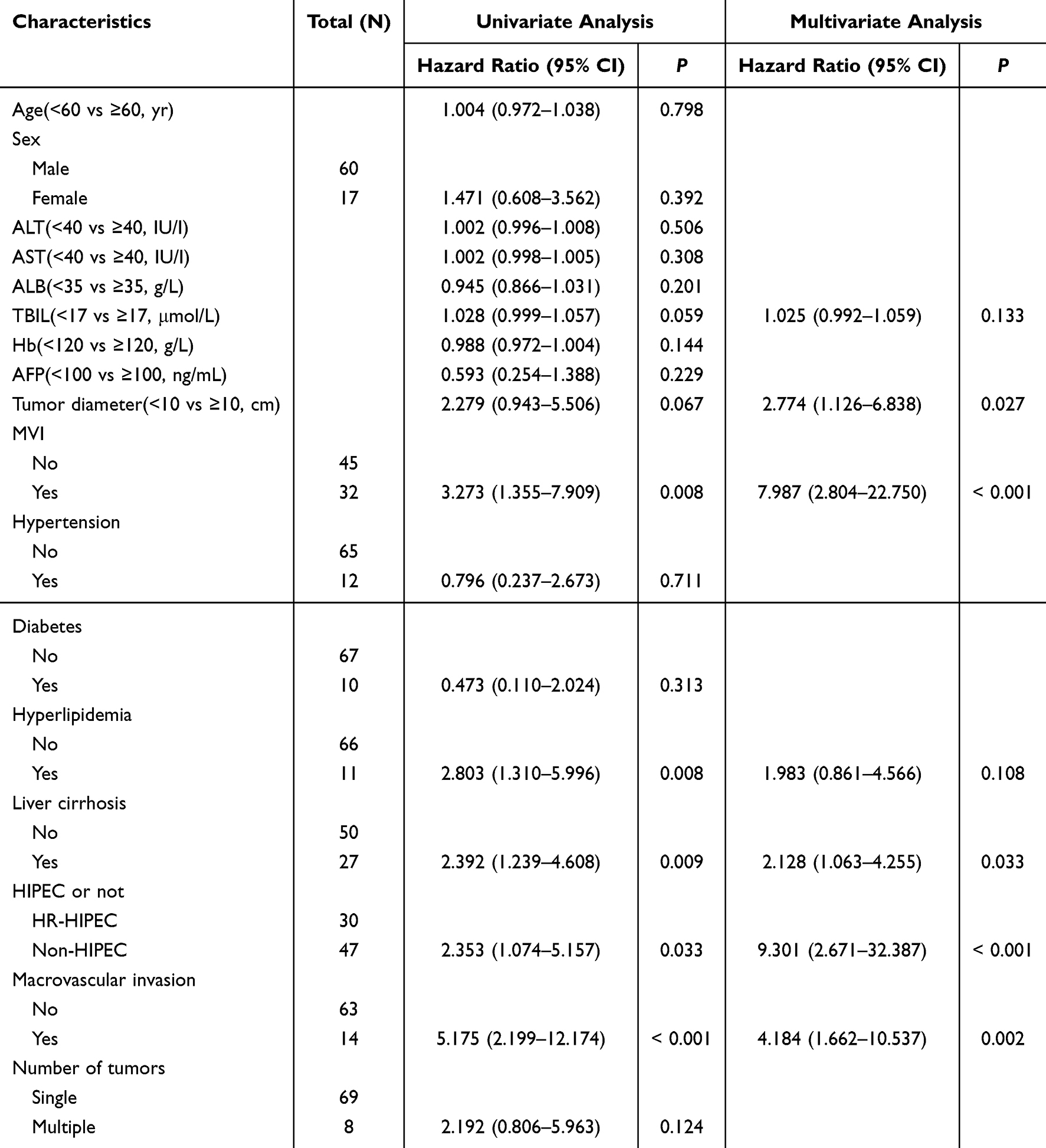 |
Table 3 Cox Regression Analysis for Risk Factors of Overall Survival |
In the univariate Cox proportional hazards regression analysis, several variables were identified as significant predictors of recurrence, including age exceeding 60 years, elevated total bilirubin levels, anemia, MVI, Liver cirrhosis, macrovascular invasion, number of tumors and HIPEC or not (Table 4). Upon multivariate analysis, independent risk factors for recurrence were delineated as follows: age exceeding 60 years, with a hazard ratio (HR) of 1.064 (P=0.015), elevated total bilirubin (HR 1.073, P=0.002), presence of comorbid MVI (HR 4.333, P=0.007), Liver cirrhosis (HR 6.897, P<0.001), and the conduct of HIPEC (HR 2.159, P=0.044).
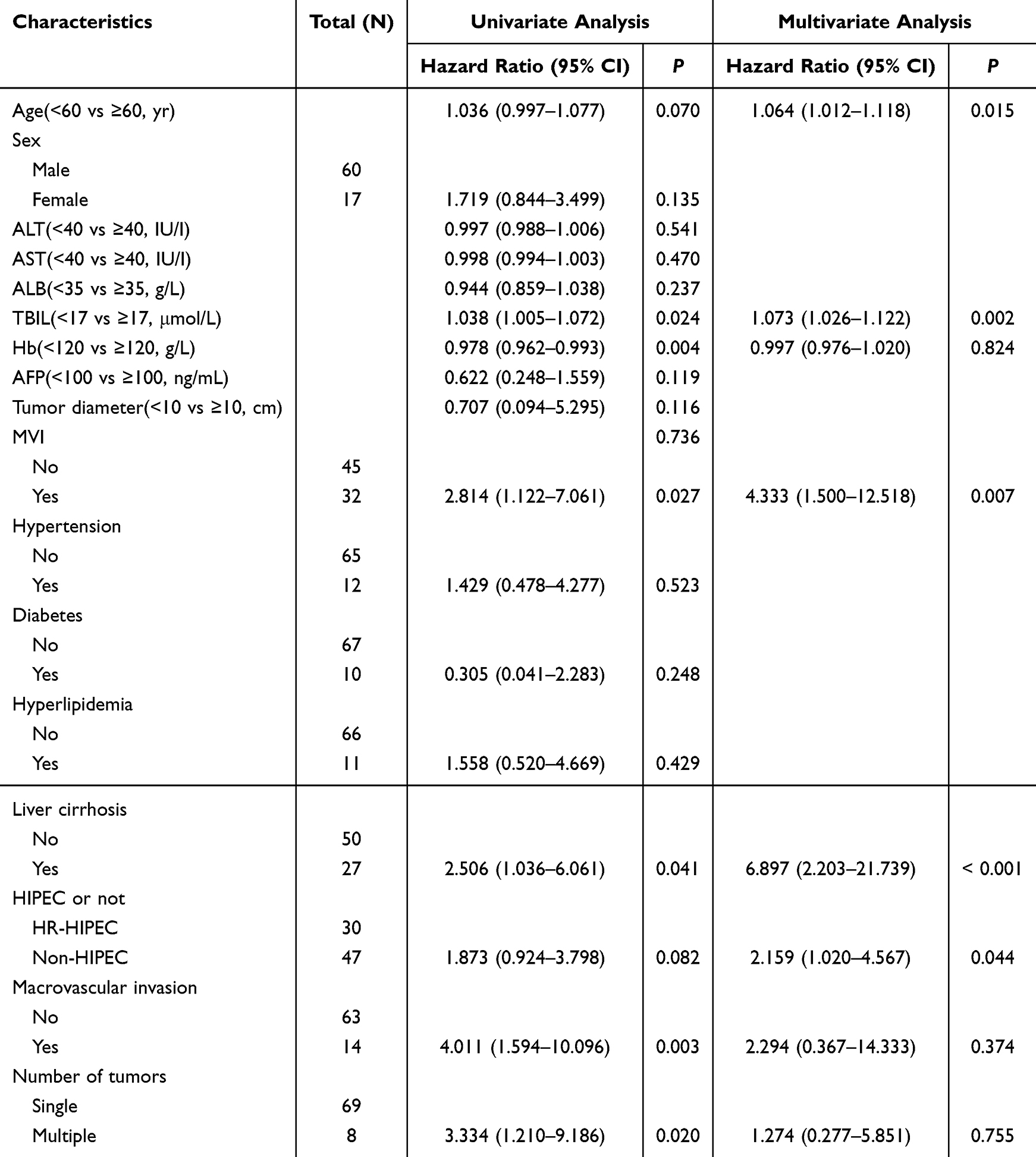 |
Table 4 Cox Regression Analysis for Risk Factors of Recurrence-Free Survival |
Risk Factor Analysis of Early Recurrence and Distant Recurrence and Metastasis
Early recurrences (<2 years) occurred in 27 cases, among which the HR-HIPEC group had 8 cases (26.7%), while the non-HIPEC group had 19 cases (40.4%), and there was a remarkable difference between them (P=0.0276), with a HR of 2.253 (95% CI: 1.264, 4.016) (Figure 4A). Distant recurrences/transfers were noted in 14 cases, including 5 cases (16.7%) in the HR-HIPEC group and 9 cases (19.1%) in the non-HIPEC group, and there is a significant difference between the two groups (P=0.0182), with a HR of 2.311, 95% CI 1.168, 4.572) (Figure 4B).
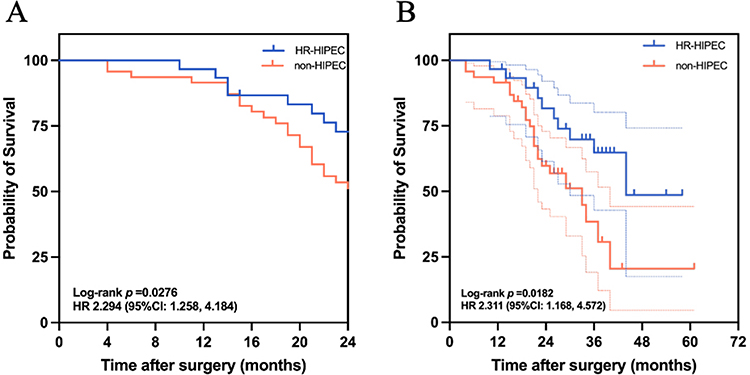 |
Figure 4 (A) Analysis of early recurrence-free survival in patients treated with HR-HIPEC group or non-HIPEC group; (B) Analysis of distant recurrence-free survival in patients treated with HR-HIPEC group or non-HIPEC group. |
In the realm of early tumor recurrence, the univariate Cox regression analysis has discerned several significant predictors, including hypoproteinemia (ALB<35g/L), anemia, MVI, hyperlipidemia, liver cirrhosis, macrovascular invasion, and number of tumors. (Table 5). Liver cirrhosis (HR 3.205, P=0.004) was identified as the only independent risk factor in the multifactorial analysis. The role of HIPEC as a prognostic factor for early recurrence was not supported by the data, with an HR of 1.764 and a P-value of 0.179, indicating that it does not significantly affect the risk of early recurrence.
 |
Table 5 Cox Regression Analysis for Risk Factors of Early Recurrence-Free Survival |
In the specific instance of distant recurrence or metastasis, the univariate Cox regression analysis identified female, elevated total bilirubin levels, anemia, MVI, number of tumors as the significant predictor (Table 6). However, the multivariate analysis did not corroborate these factors as independent risk factors for distant recurrence or metastasis. Interestingly, the administration of HIPEC showed a potential therapeutic role in preventing from distant recurrence or metastasis after the rupture of hepatocellular carcinoma, denoted by an HR of 2.779, which did not reach the conventional level of statistical significance.
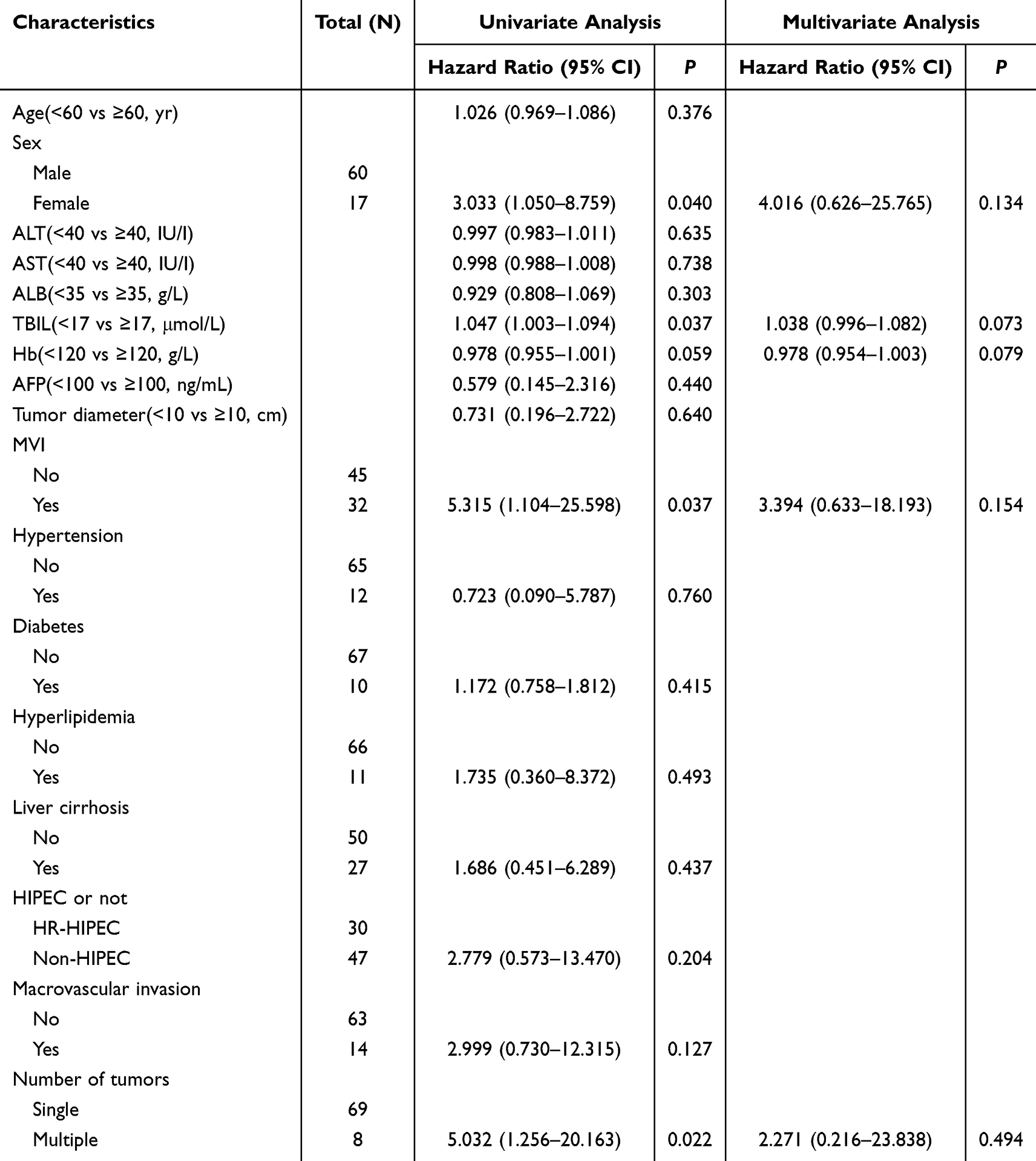 |
Table 6 Cox Regression Analysis for Risk Factors of Distant Recurrence-Free Survival |
Subgroup Analysis of Different Chemotherapy Drug Regimens in HR-HIPEC Group
As mentioned earlier, our center has conducted a preliminary exploration of the drug selection for postoperative HIPEC in hepatocellular carcinoma, and based on the past experience and the latest research results of the relevant adjuvant therapy for hepatocellular carcinoma, two regimens have been adopted since the initiation of postoperative HIPEC treatment, consist of the following gemcitabine + cisplatin and oxaliplatin + 5-FU + folic acid.
Among the 30 patients who underwent postoperative HIPEC in this study, 14 patients were treated with a chemotherapy regimen of gemcitabine + cisplatin, and 16 patients with a chemotherapy regimen of oxaliplatin + 5-FU + folic acid. The general and clinical characteristics, etc. of these patients, are provided in Table 7. No significant differences were still not found.
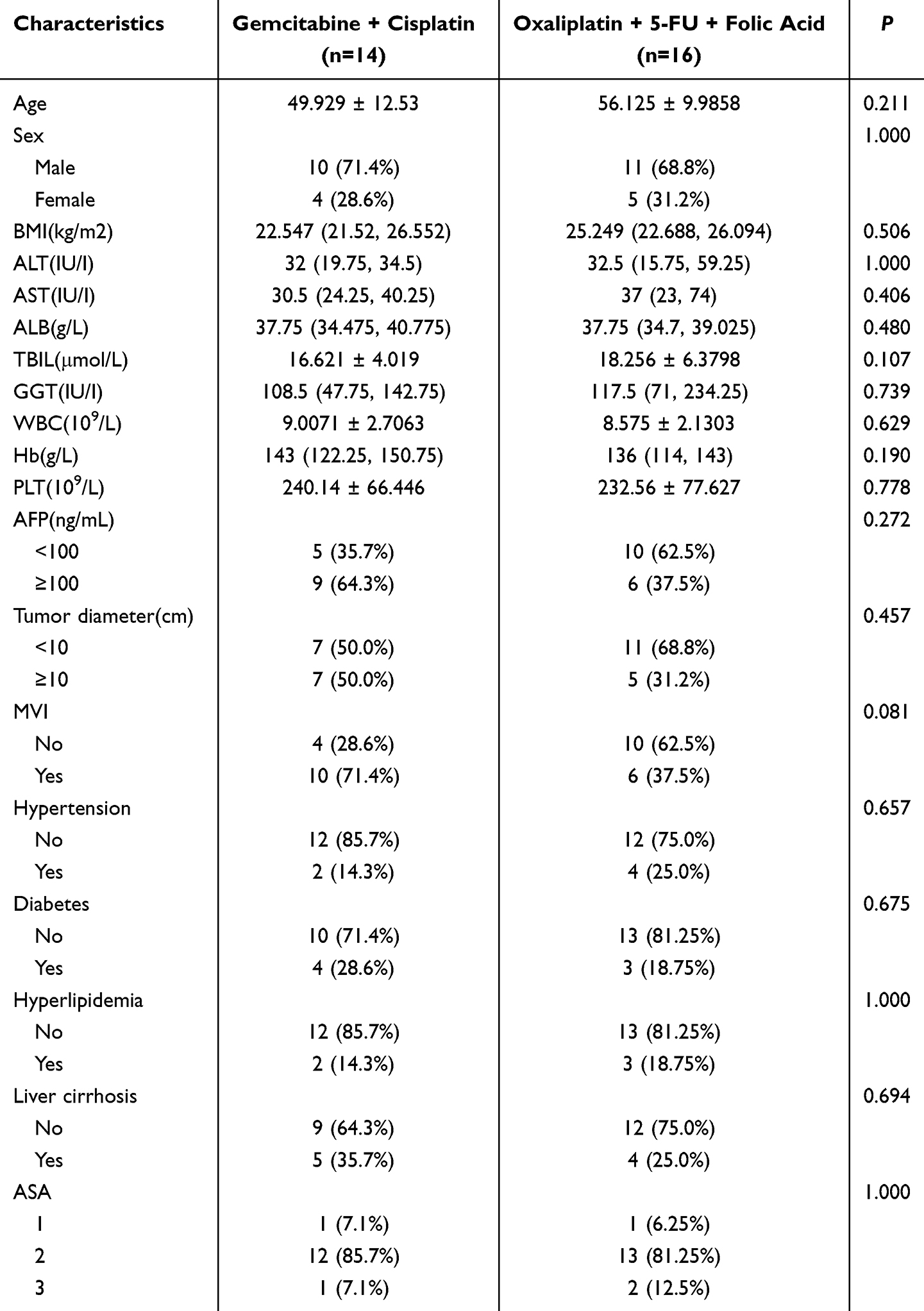 |
Table 7 Subgroup Analysis of Different Chemotherapy Drug Regimens in HIPEC Group |
In a further analysis of the safety of different treatments, the hemoglobin was observed to remarkably lower in patients treated with regimen oxaliplatin + 5-FU + folic acid (P=0.006). Apart from this, no significant differences were observed between the two groups in terms of other hematological parameters and postoperative complications. (Table 8).
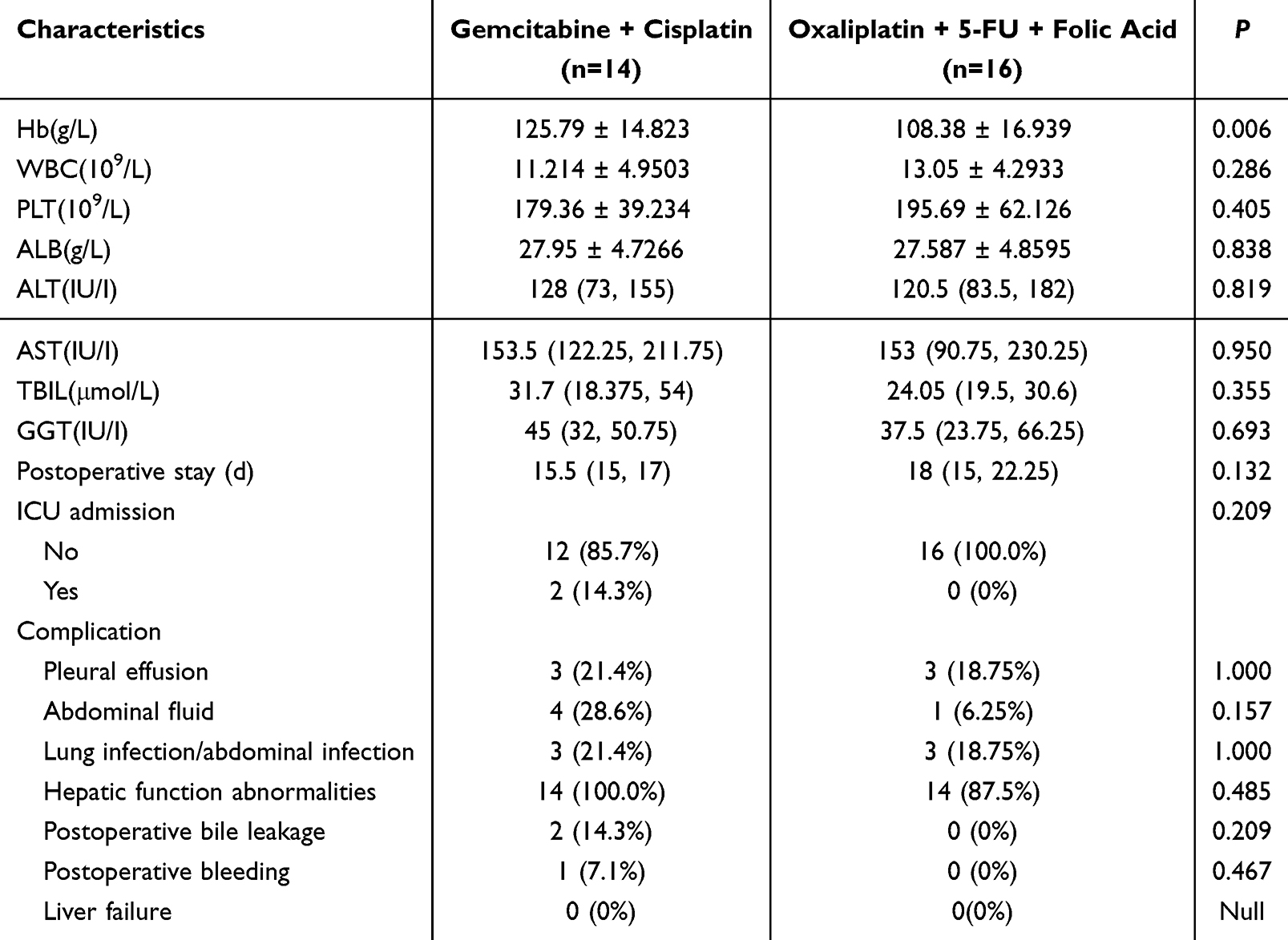 |
Table 8 Subgroup Analysis of Treatment Safety in HIPEC Group |
After conducting a survival analysis on the subgroup of patients, we obtained the following results: Among the 14 patients treated with gemcitabine + cisplatin, 7 patients died (50.0%, 7/14) with tumor recurrence. In the group of 16 patients treated with oxaliplatin + 5-FU + folic acid, 2 patients (12.5%, 2/16) also died with tumor recurrence. In addition, The median overall survival of gemcitabine + cisplatin group was 44 months, while it is not observed in the other group, and the three-year overall survival rates of the two groups were 64.28% and 85.22%, with a hazard ratio of 2.132 (95% CI 0.5544,8.200), P=0.2804 (Figure 5A). The median RFS of the two groups was a same result, with a hazard ratio of 1.182 (95% CI 0.4131,3.382), P=0.7444 (Figure 5B).
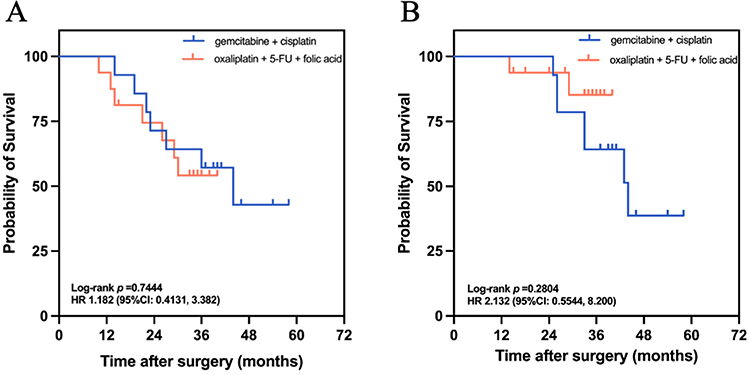 |
Figure 5 (A) Analysis of overall survival in patients treated with gemcitabine + cisplatin or oxaliplatin + 5-FU + folic acid; (B) Analysis of recurrence-free survival in patients treated with gemcitabine + cisplatin or oxaliplatin + 5-FU + folic acid. |
Discussion
Spontaneous rupture of hepatocellular carcinoma represents a critical oncologic emergency, constituting the third leading cause of HCC-related mortality following tumor progression and hepatic decompensation. Although this complication occurs in only 2.3%–15% of HCC cases globally, its incidence demonstrates significant geographic variation, with Asian populations exhibiting 3-fold higher rates compared to European cohorts (10% vs 3.2%).13 Historical data indicate acute mortality rates of 25%–75% in untreated cases, however, contemporary series report substantial risk reduction through advances in hemostatic interventions, particularly transarterial embolization (TAE).4,14,15 Sahu et al and Noike et al demonstrated that TAE effectively controlled hemorrhage in the acute phase of srHCC with unstable hemodynamics, and the overall hemostatic rates reach between 53% and 100%,16 while Kwak et al documented 57% one-year survival rates when combining TAE with staged hepatectomy.17 Due to perforation of the visceral peritoneum, srHCC is classified as T4 disease, a terminal event with a grave prognosis, in the 7th Union for International Cancer Control (UICC) classification.18 Furthermore, peritoneal carcinomatosis development correlates strongly with tumor biology, exhibiting a 7.9-fold increased risk of abdominal dissemination compared to non-ruptured HCC (Baimas-George M. et al5). These pathophysiological insights underscore the imperative to elucidate determinants of long-term survival and develop multimodal therapeutic strategies targeting peritoneal micrometastases in srHCC management.
The therapeutic application of HIPEC traces its origins to Spratt’s pioneering work in 1980, which first demonstrated the feasibility of intracavitary hyperthermic chemotherapy for peritoneal malignancies,8,19 Sugarbaker and other scholars subsequently carried out in-depth researches on the expansion of clinical application of HIPEC, established HIPEC as a cornerstone in peritoneal surface oncology, particularly through the standardization of cytoreductive surgery (CRS) protocols.20,21 In the past decades, HIPEC-related studies mainly originated from the Peritoneal Surface Tumor Collaborative Group International (PSOGI), who mostly focused on the treatment of gastrointestinal (54% of PSOGI trials), appendiceal mucinous (28%), and ovarian cancers (18%),22,23 the application in hepatocellular carcinoma remained limited due to: (1) Lower peritoneal metastasis rates compared to other malignancies (18.7%vs.42–68% in colorectal/ovarian cancers); (2) Historically high acute mortality from spontaneous HCC rupture (pre-TAE era: 25–75%); (3) Technical challenges in cirrhotic patients (Child-Pugh B/C: 62% in Asian HCC cohorts).24 The evolving safety profile of HIPEC (grade III–IV complications <8% in contemporary series) and improved srHCC survival (1-year OS increased from 34% to 57% post-TAE era) have reinvigorated interest in adjuvant HIPEC applications. For peritoneal metastasis (PM) associated with srHCC, Sanket et al collected 21 patients between 1992 and 2016 from 10 reference centers of PSOGI, indicated that the median overall survival (OS) of 16 patients with both HIPEC and complete CRS reached 46.7 months, and their recurrence-free survival (RFS) exceeded 3 years.25 However, conflicting evidence emerges from Ruan et al’s analysis of 57 srHCC cases (2014–2018), demonstrating non-significant survival benefits with HIPEC at 18-month follow-up (median OS: 41 vs 38 months, P=0.17), potentially reflecting insufficient observation duration given HCC’s characteristic late recurrence patterns (median time: 31 months).11
This retrospective cohort study evaluated the prognosis of 77 patients with spontaneous rupture of hepatocellular carcinoma who underwent hepatectomy with or without adjuvant HIPEC. The HIPEC cohort demonstrated significantly prolonged median overall survival (44 vs 35 months; HR=2.29, 95% CI 1.13–4.64, P=0.027) and superior recurrence-free survival (median RFS 44 vs 25 months; HR=2.25, 95% CI 1.26–4.02, P=0.007). In addition, Multivariate analysis identified that performing HIPEC was an independent risk factor affecting patients’ prognosis, rather than a risk factor affecting recurrence, and further analysis for the recurrent patient population showed that HIPEC has the potential to attenuate tumor load and reduce the incidence of early recurrence (P=0.0276, HR 2.294) and effectively decrease the incidence of distant recurrence/metastasis (P=0.0182, HR 2.311), thereby improving patient prognosis. This potential of HIPEC deserves further exploration and validation through larger-scale and longer-term clinical studies in the future.
Most of the postoperative pleural and abdominal effusions were mild and improved after active nutritional support therapy and respiratory exercise, and only 2 cases of pleural fluid were resolved after thoracentesis, and the chest drains were removed within 2 days after the puncture. Six patients with long-term smoking or high risk factors for cirrhosis and ascites had postoperative pulmonary or (and) abdominal infections, which were detected by the daily rise in blood leukocytes and neutrophils, and the persistent increase in procalcitonin and C-reactive protein, and the infection resolved with sensitive antibiotics. Two patients had bile leakage through analysis of the abdominal drain fluid’s characteristics and biochemistry and were discharged after symptomatic treatment without surgical intervention. One patient with postoperative bleeding showed bright red fluid in the abdominal drainage tube and anemia (80g/L) in postoperative review, which was considered to be caused by blood seepage from hepatic cutting surface. Drugs and 2–4U of packed red blood cells were given to stop bleeding, and no interventional or surgical hemostasis was performed. Common adverse reactions and complications of HIPEC include fever, pleural and abdominal effusion, gastrointestinal perforation and obstruction, and abdominal infection.26,27 During HIPEC treatment, there was no statistically significant difference in the incidence of postoperative complications between the two groups, and there were no fatal complications such as severe postoperative hemorrhage, bile leakage, and gastrointestinal perforation, etc. Before discharge from the hospital, the postoperative complications were successfully cured. Therefore, we concluded that HIPEC is safe for the treatment of patients with srHCC. Furthermore, though we observed higher levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) in the HR-HIPEC group (ALT:123IU/L vs 89IU/L, P=0.170; AST:153.5IU/L vs 107IU/L, P=0.234) after all three HIPEC treatments completed, it lacked the statistical significance.
The evolution of HIPEC protocols has achieved disease-specific standardization in gastrointestinal (FOLFOX: oxaliplatin 460 mg/m2 + 5-FU 1500 mg/m2) and ovarian malignancies (cisplatin 75 mg/m2 + paclitaxel 175 mg/m2), as endorsed by Peritoneal Surface Oncology Group International (PSOGI) consensus guidelines.28 In contrast, the therapeutic paradigm for srHCC remains undefined, with global heterogeneity in drug selection and perfusion parameters. Huang et al applied mitomycin C (MMC)-based HIPEC to prevent peritoneal metastasis in srHCC, observed a relatively positive and effective trend of a median local peritoneal recurrence-free survival with a median local peritoneal RFS of 12.3 months and a median overall RFS of 7.5 months.12 Jacquet et al demonstrated that HIPEC achieved high concentrations of chemotherapeutic agents directly on the peritoneum with the limiting systemic absorption, resulting in intraperitoneal drug concentrations, significantly exceeding those found in systemic circulation.29 The PRODIGE 7 study reported on the outcomes of CRS combined with HIPEC alone in patients with completely resectable colorectal peritoneal metastasis. Their results indicated that HIPEC based on oxaliplatin did not significantly improve overall survival or recurrence-free survival, but the mortality rate and early postoperative complications within 30 days were similar to the CRS-only group, suggesting that the safety of HIPEC is controllable.30 These findings suggest that future clinical applications of HIPEC should focus on exploring various aspects, including the selection of different HIPEC drug regimens, dosage of medications, and duration of treatment.
Building upon the findings of previous domestic and international studies, and leveraging our center’s extensive experience in the comprehensive treatment of liver cancer, we have employed two principal chemotherapy regimens for patients undergoing HIPEC: gemcitabine + cisplatin (14 cases) and oxaliplatin + 5-FU + folic acid (16 cases). The former represents a systemic chemotherapy adaptation, while the latter reflects a landmark study validation following the establishment of the mature FOLFOX regimen as the primary adjuvant treatment for liver cancer patients in China.31
In our study, we conducted a subgroup analysis of patients receiving these distinct drug regimens, designated as the gemcitabine + cisplatin group and the FOLFOX group. Regarding the safety assessment of the different drug regimens, no significant differences were observed between the two groups, with the exception of significantly lower hemoglobin level in FOLFOX group. We attribute this difference to variations in intraoperative blood loss, preoperative liver function, and postoperative protocol-driven management use. The reduction in hemoglobin levels may be the result of one or more of these factors acting in concert. These discrepancies were all successfully resolved before discharge, following appropriate postoperative symptomatic treatment and as patients’ physiological functions recovered.
In terms of additional perioperative safety indicators, we noted a higher incidence of abdominal infection in the gemcitabine + cisplatin group, compared to the oxaliplatin + 5-FU + folic acid group (4 cases, 28.6% vs 1 case, 6.25%; P=0.157). There were no significant differences in postoperative infection markers such as white blood cell levels. Previous studies on the main adverse reactions of these regimens have highlighted sensory neurotoxicity, myelosuppression, and gastrointestinal reactions, without mentioning a potential decrease in immune function or increased risk of infection. The risk of abdominal infection is associated with various factors, including the use of hyperthermic perfusion catheters, the strictness of aseptic techniques, and other procedural factors during treatment. Though we cannot conclusively determine which chemotherapy regimen poses a higher risk of abdominal infection, it may be useful to increase the sample size for further study.
In the prognosis analysis of the two groups of patients, our results were similar to those of the aforementioned investigators, with no significant differences in OS and RFS between the two groups. However, oxaliplatin + 5-FU + folic acid group showed a better overall survival trend compared to gemcitabine + cisplatin group (HR 2.132). This difference has not yet reached statistical significance, mainly due to limitations such as the short follow-up duration and small sample size (P=0.2804). Previous studies have indicated that both regimens demonstrate certain therapeutic effects in different types of cancer. For instance, the FOLFOX regimen provides survival benefits and therapeutic effects for patients with advanced hepatocellular carcinoma compared to doxorubicin.31 Hepatic arterial infusion chemotherapy (HAIC) with FOLFOX regimen can significantly reduce the risk of postoperative recurrence in HCC patients with microvascular invasion (MVI), and its safety is good.32 In other types of cancer, the gemcitabine plus cisplatin regimen may have more advantages.33,34 From the aforementioned research results, both regimens show certain safety and tolerability in patient populations, without showing significant differences in efficacy. Currently, there are no studies directly comparing the efficacy and safety of these two regimens. Our study has made preliminary explorations into this practical clinical challenge and obtained results that have certain clinical value and significance.
This study has several limitations. First, the retrospective design and relatively small sample size may introduce inherent biases. Although the incidence of spontaneously ruptured hepatocellular carcinoma is higher in Asian countries than elsewhere, the reported overall incidence remains low, ranging from 2.3% to 26%. Moreover, a considerable proportion of patients with tumor rupture present with massive hemorrhage or impaired liver function, rendering them ineligible for curative resection, which further restricts the potential sample size. Nevertheless, as the largest single-center study on this topic to date, our work provides valuable insights into the oncological outcomes of srHCC and lays a foundation for the design of future prospective studies.
Second, although the follow-up period may be considered somewhat short (median follow-up time: HR-HIPEC group 37 months vs non-HIPEC group 34 months), the aggressive nature of srHCC and its high propensity for peritoneal dissemination often lead to early recurrence and metastasis. Therefore, the primary objectives of this study were to evaluate the safety and short-term efficacy of HIPEC. Encouragingly, even within the current follow-up timeframe, we have observed a strong positive trend toward improved survival outcomes in the HR-HIPEC group. Thus, the follow-up duration is sufficient to address the primary aims of this study. We are continuing to follow this patient cohort, and the present findings establish a preliminary basis for future larger-scale studies with extended follow-up.
Furthermore, though a series of standardized procedures are adopted for HIPEC with the aim of optimizing outcomes and reducing complications, there are no uniform treatment guidelines and standards for the application of HIPEC in srHCC, eg, in terms of the timing of the first HIPEC, the formula of the HIPEC. Our center has established a relatively mature comprehensive treatment protocol of postoperative HIPEC for srHCC. On this basis, we have explored optimal HIPEC regimens for srHCC, and will provide hypotheses or a research basis for future multicenter, prospective studies.
Conclusion
In conclusion, HIPEC represents a safe and feasible treatment modality for patients with srHCC and is associated with improved recurrence-free survival (RFS) and overall survival (OS). Among patients receiving HIPEC, no significant differences in safety or efficacy were observed between the oxaliplatin plus 5-FU and folinic acid regimen and the gemcitabine plus cisplatin regimen. Although the oxaliplatin-based regimen showed a trend toward more favorable survival outcomes, this difference did not reach statistical significance in our cohort. Future studies with larger sample sizes and extended follow-up are warranted to validate these preliminary findings and to elucidate the optimal chemotherapeutic regimen and underlying mechanisms of HIPEC in srHCC.
Funding
This work was supported by the Natural Science Foundation of Guangdong Province [Grant Numbers: 2022A1515010537, 2023A1515012531] and the Guangzhou Science and Technology Program [Grant Number: 2024B03J1256].
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
2. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598–1606. doi:10.1016/j.jhep.2022.08.021
3. ScienceDirect. Global burden of primary liver cancer in 2020 and predictions to 2040. Available from: https://www.sciencedirect.com/science/article/pii/S0168827822030227.
4. Sahu SK, Chawla YK, Dhiman RK, et al. Rupture of Hepatocellular Carcinoma: a Review of Literature. J Clin Exp Hepatol. 2019;9(2):245–256. doi:10.1016/j.jceh.2018.04.002
5. Joliat GR. Long-term outcomes of ruptured hepatocellular carcinoma: international multicentre study. Br J Surg. 2024;111(4):znae093.
6. Aziz H, Kwon YIC, Park A, Kwon Y, Aswani Y, Pawlik TM. Comprehensive review of clinical presentation, diagnosis, management, and prognosis of ruptured hepatocellular carcinoma. J Gastrointestinal Surg. 2024;28(8):1357–1369. doi:10.1016/j.gassur.2024.05.018
7. Zhou S, Zhang E, Liang B, Zhang Z, Chen X, Huang Z. Distilled Water Lavage During Surgery Improves Long-Term Outcomes of Patients with Ruptured Hepatocellular Carcinoma. J Gastrointestinal Surg. 2015;19(7):1262–1270. doi:10.1007/s11605-015-2797-0
8. Dong FH, Shan YQ, Kong WC, et al. Hyperthermic intraperitoneal chemotherapy: ideal and reality. Asian Journal of Surgery. 2024;2024:1. doi:10.1016/j.asjsur.2024.10.155
9. Hübner M, van Der Speeten K, Govaerts K, et al. 2022 Peritoneal Surface Oncology Group International Consensus on HIPEC Regimens for Peritoneal Malignancies: colorectal Cancer. Ann Surg Oncol. 2024;31(1):567–576. doi:10.1245/s10434-023-14368-5
10. Filis P, Mauri D, Markozannes G, Tolia M, Filis N, Tsilidis K. Hyperthermic intraperitoneal chemotherapy (HIPEC) for the management of primary advanced and recurrent ovarian cancer: a systematic review and meta-analysis of randomized trials. ESMO Open. 2022;7(5):100586. doi:10.1016/j.esmoop.2022.100586
11. Ruan S, Shi N, Chen Z, et al. The role of hyperthermic intraperitoneal chemotherapy in the treatment of spontaneously ruptured hepatocellular carcinoma: a pilot study. Ann Transl Med. 2020;8(18):1132. doi:10.21037/atm-20-5829
12. Hou Z, Qiu G, Xie Q, Jin Z, Mi S, Huang J. The prophylactic role of mitomycin C-based hyperthermic intraperitoneal chemotherapy (MMC-based HIPEC) on peritoneal metastasis of spontaneously ruptured hepatocellular carcinoma (srHCC): a pilot study. Glob Health Med. 2023;5(6):336–344. doi:10.35772/ghm.2023.01081
13. Nature. Global trends in hepatocellular carcinoma epidemiology: implications for screening, prevention and therapy | nature Reviews Clinical Oncology. Available from: https://www.nature.com/articles/s41571-023-00825-3.
14. Battula N, Madanur M, Priest O, et al. Spontaneous rupture of hepatocellular carcinoma: a Western experience. Am J Surg. 2009;197(2):164–167. doi:10.1016/j.amjsurg.2007.10.016
15. Foglia B, Turato C, Cannito S. Hepatocellular Carcinoma: latest Research in Pathogenesis, Detection and Treatment. Int J Mol Sci. 2023;24(15):12224. doi:10.3390/ijms241512224
16. Sandomenico F, Arpaia V, De Rosa F, et al. Spontaneously Ruptured Hepatocellular Carcinoma: computed Tomography-Based Assessment. Diagnostics. 2023;13(6):1021. doi:10.3390/diagnostics13061021
17. Xu K, Ryu DH, Choi JW, et al. Clinical impact of surgical treatment for the spontaneously ruptured resectable hepatocellular carcinoma: a single institution experience. Medicine. 2022;101(35):e30307. doi:10.1097/MD.0000000000030307
18. Chua DW, Koh YX, Allen JC, et al. Impact of spontaneous rupture on the survival outcomes after liver resection for hepatocellular carcinoma: a propensity matched analysis comparing ruptured versus non-ruptured tumors. Eur J Surg Oncol. 2019;45(9):1652–1659. doi:10.1016/j.ejso.2019.03.044
19. Della Corte L, Conte C, Palumbo M, et al. Hyperthermic Intraperitoneal Chemotherapy (HIPEC): new Approaches and Controversies on the Treatment of Advanced Epithelial Ovarian Cancer-Systematic Review and Meta-Analysis. J Clin Med. 2023;12(22):7012. doi:10.3390/jcm12227012
20. Sugarbaker PH. Review of Options to Traditional HIPEC for Prevention and Treatment of Peritoneal Metastases. J Surg Oncol. 2024;2024:3. doi:10.1002/jso.27913
21. Kusamura S, Barretta F, Yonemura Y, et al. The Role of Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery. JAMA Surg. 2021;156(3):e206363. doi:10.1001/jamasurg.2020.6363
22. Bhatt A, Glehen O, Zivanovic O, et al. The 2022 PSOGI International Consensus on HIPEC Regimens for Peritoneal Malignancies: epithelial Ovarian Cancer. Ann Surg Oncol. 2023;30(13):8115–8137. doi:10.1245/s10434-023-13932-3
23. Bushati M, Rovers KP, Sommariva A, et al. The current practice of cytoreductive surgery and HIPEC for colorectal peritoneal metastases: results of a worldwide web-based survey of the Peritoneal Surface Oncology Group International (PSOGI). Eur J Surg Oncol. 2018;44(12):1942–1948. doi:10.1016/j.ejso.2018.07.003
24. Spiliotis J, Nikolaou G, Kopanakis N, Vassiliadou D, Terra A, Efstathiou E. Hepatocellular Carcinoma Peritoneal Metastasis: role of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). Gulf J Oncolog. 2017;1(24):20–23.
25. PubMed. Is there an oncological interest in the combination of CRS/HIPEC for peritoneal carcinomatosis of HCC? Results of a multicenter international study. Available from: https://pubmed.ncbi.nlm.nih.gov/29885982/.
26. Ray MD, Dhall K. Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in the management of peritoneal surface malignancies – an evidence-based review. Curr Problems Cancer. 2021;45(6):100737. doi:10.1016/j.currproblcancer.2021.100737
27. Hu J, Wang Z, Wang X, Xie S. Side-effects of hyperthermic intraperitoneal chemotherapy in patients with gastrointestinal cancers. PeerJ. 2023;11:e15277. doi:10.7717/peerj.15277
28. González-Moreno S, González-Bayón L, Ortega-Pérez G. Hyperthermic Intraperitoneal Chemotherapy: methodology and Safety Considerations. Surg Oncol Clin. 2012;21(4):543–557. doi:10.1016/j.soc.2012.07.001
29. Gelissen JH, Adjei NN, McNamara B, et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. Ann Surg Oncol. 2023;30(9):5597–5609. doi:10.1245/s10434-023-13757-0
30. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, Phase 3 trial - PubMed. https://pubmed.ncbi.nlm.nih.gov/33476595/.
31. Ascopubs. Randomized, Multicenter, Open-Label Study of Oxaliplatin Plus Fluorouracil/Leucovorin Versus Doxorubicin As Palliative Chemotherapy in Patients With Advanced Hepatocellular Carcinoma From Asia | journal of Clinical Oncology. https://ascopubs.org/doi/10.1200/JCO.2012.44.5643?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed.
32. Li SH, Mei J, Cheng Y, et al. Postoperative Adjuvant Hepatic Arterial Infusion Chemotherapy With FOLFOX in Hepatocellular Carcinoma With Microvascular Invasion: a Multicenter, Phase III, Randomized Study. J Clin Oncol. 2023;41(10):1898–1908. doi:10.1200/JCO.22.01142
33. Zhang Y, Chen L, Hu GQ, et al. Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. N Engl J Med. 2019;381(12):1124–1135. doi:10.1056/NEJMoa1905287
34. Ostwal V, Patkar S, Engineer R, et al. Adjuvant Gemcitabine Plus Cisplatin and Chemoradiation in Patients With Gallbladder Cancer: a Randomized Clinical Trial. JAMA Oncol. 2024;10(8):1116–1120. doi:10.1001/jamaoncol.2024.1944
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.