")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 13
The Prognostic Values of Neutrophil-to-lymphocyte Ratio and Platelet-to-Lymphocyte Ratio at Baseline in Predicting the In-hospital Mortality in Black African Patients with Advanced Hepatocellular Carcinoma in Palliative Treatment: A Comparative Cohort Study
Authors Mahassadi AK , Anzouan-Kacou Kissi H , Attia AK
Received 20 August 2021
Accepted for publication 10 November 2021
Published 8 December 2021 Volume 2021:13 Pages 123—134
DOI https://doi.org/10.2147/HMER.S333980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Alassan Kouame Mahassadi, Henriette Anzouan-Kacou Kissi, Alain Koffi Attia
Gastroenterology and Hepatology Unit, Yopougon Teaching Hospital, Abidjan, Côte d’Ivoire, West Africa
Correspondence: Alassan Kouame Mahassadi
Gastroenterology and Hepatology Unit, Yopougon Teaching Hospital, 21 BP 632 Abidjan 21, Abidjan, Côte d’Ivoire, West Africa
Email [email protected]
Background: The prognostic values of the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) in predicting the in-hospital mortality of Black African patients with advanced hepatocellular carcinoma (HCC) in palliative treatment is unknown.
Aim: To determine the prognostic value of NLR and PLR compared with that of Child–Turcotte–Pugh (CTP), model for end-stage liver disease (MELD) scores and the Barcelona clinic liver cancer staging system (BCLC).
Methods: The cutoffs, accuracies and association with the mortality of these prognostic scores were determined using a time-dependent area under receiver operating characteristic curves (AUC), the log rank test and Cox proportional hazards ratio.
Results: A total of 104 patients with advanced HCC (median age=49.5 years, males=58.7%) were enrolled. All were hospitalized for an enlarged liver mass of at least 15.4 cm in size in the right thoracic quadrant. Overall, 46 (44.2%) patients died in hospital during follow-up. Patients with NLR > 2.5 (log rank test=7.11, p=0.01) or PLR > 92 (log rank test=5.63, p=0.02) had poor survival. Factors associated with the in-hospital mortality were the MELD score (p=0.01), NLR (p=0.03) and hemoglobin level (p=0.02). NLR exhibits better and stable accuracy in predicting the in hospital mortality at time points of 30 (AUC=0.618), 60 (AUC=0.680) and 90 (AUC=0.613) days of follow-up, compared with CTP, MELD scores, BCLC and PLR. However, PLR displayed an enhanced accuracy over 90 days of follow up (AUC=0.688).
Conclusion: NLR is useful in predicting the in-hospital mortality in Black African patients with advanced stage HCC in clinical practice. NLR and PLR may be used concomitantly for long-term follow-up.
Keywords: hepatocellular carcinoma, neutrophil-to-lymphocyte ratio, prognosis, sub-Saharan Africa
Erratum for this paper has been published
Introduction
Hepatocellular carcinoma (HCC) is the serious complication of chronic hepatitis or cirrhosis accounting for 800,000 deaths worldwide annually.1,2 In most advanced cases, the median survival time is less than six months.3 The high incidence of HCC is correlated with that of chronic hepatitis B or C viral infection, the main viral etiologies of HCC in Asian and sub-Saharan African countries.1,3
Risk factors of mortality in patients with HCC are related to the size of tumor, vascular invasion and the severity of the underlying liver disease function.4 These risk factors have led to the establishment of prognostic scores and staging systems that allow physicians to administer an appropriate treatment and predict survival among patients with HCC.5,6
Among these prognostic scores are the Child–Turcotte–Pugh (CTP), the model for end-stage liver disease (MELD) scores which have shown valuable results in predicting survival among patients with HCC.5–7 Moreover, the MELD score in combination with the Barcelona clinic liver cancer staging system (BCLC) allows physicians to select patients with HCC for liver transplantation.7,8 However, the survival predictability of the MELD score and BCLC staging system of Black African patients with advanced HCC in palliative treatment is not well documented as shown in Black American patients with untreated HCC.9
Hepatic carcinogenesis is based on chronic inflammation related to chronic exposure to infection or toxic substance leading to the synthesis of pro-oncogenic cytokines that promote carcinogenetic pathways.10 Moreover, chronic inflammation is correlated with tumor progression, and adaptive immune cells such as lymphocytes, neutrophils and platelets are found to initiate or promote the development of carcinogenetic cells and metastasis.10–12 Therefore, recent studies and meta-analyses have demonstrated that the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) predicted accurately the overall survival in patients with HCC after medical treatment, chemoembolization, radiofrequency ablation, liver resection or transplantation.13,14 However, concerns have been raised regarding the absence of data on the efficacy of NLR in predicting overall survival in patients with advanced HCC that have not received an intensive treatment.15 Furthermore, with regard to NLR, the use of pre- or post-treatment values and the absence of a standardized or consensual cutoff remain a matter of debate and have probably introduced discrepancies on its efficacy in predicting poor survival among patients with HCC in published studies.13–15
In West Africa, the age-adjusted incidence and mortality rate of HCC are respectively of 8.4 and 8.1 per 100,000 person-years.2 Black African patients with HCC are discovered in an advanced stage.3 These patients with advanced HCC are candidates for palliative treatment.3,16,17 Data on the efficacy of CTP, MELD scores and BCLC staging system in predicting mortality in Black African patients with advanced HCC are scanty.3,16,17 Furthermore, to our knowledge, there are no data on the efficacy of NLR and PLR in predicting mortality in these particular patients in Africa.
This study was aimed at evaluating the accuracy and efficacy of CTP, MELD scores, and BCLC staging system; NLR; and PLR in predicting the in-hospital mortality of Black African patients with advanced HCC in palliative treatment.
Methods
Patient Selection
One hundred and four consecutive Black African patients with advanced HCC in palliative treatment (median age: 49.5 years) hospitalized in the Gastroenterology and Hepatology Unit of the teaching hospital of Yopougon, from January 2012 to December 2015, were included in the study. These patients were admitted with an abdominal pain in the right upper quadrant or a clinically perceptible liver mass and liver blood test abnormalities.3,6,18 The diagnosis of HCC was suspected if a liver mass was found on an ultrasonography or computed tomography scan with contrast enhancement and ascertained in the presence of one of the following criteria: radiological finding of portal vein thrombosis, elevation of the alpha-fetoprotein >400 ng/mL, and malignant hepatic cells found in the fine-needle aspiration cytology or histological pattern of HCC on liver biopsy examination.3,6,16,17 Patients with incomplete data for establishing the diagnosis of HCC and those with secondary liver cancer, liver abscess, and benign liver tumors or liver vascular diseases were excluded.
Patient Follow-up and Data Collection
Patients with advanced HCC who were admitted in the gastroenterology unit were followed up since they received an initial diagnostic workup. This comprised a complete blood count; serological testing for viral hepatitis B, C, or D infection; an abdominal ultrasonography or computed tomography scan; and upper digestive endoscopy for esophageal varices detection.3,6 Patients with painful HCC received acetaminophen or opioid analgesics to relieve pain. A paracentesis was performed in those with ascites, then they were treated with oral diuretic medications. In case of hemorrhagic ascites, less than one liter of fluid was evacuated, and the patient received only a blood transfusion without transarterial embolization.6 Patients with spontaneous bacterial peritonitis received antibiotics. Any specific treatments such as liver resection, transarterial chemoembolization, chemotherapy with sorafenib, and radiofrequency ablation were not feasible in all patients with HCC because of the advanced stage of the disease, lack of expertise, or medical facilities.3,16,17 Sorafenib was not affordable for those with an intermediate-stage HCC (BCLC grade C).6 For all patients, data were retrieved from the clinical chart at baseline and comprised the following information: age; gender; past medical history (arterial hypertension, diabetes, and positivity for human immunodeficiency virus test); clinical, radiological and endoscopic futures of the HCC (tumor size; number of nodules and their location on the liver parenchyma; and presence of ascites, encephalopathy, portal vein thrombosis, and esophageal varices); transaminases; total bilirubin;, albumin; prothrombin time; international normalized ratio; serum creatinine; hemoglobin; white blood cells; neutrophils and lymphocyte cells; platelet count; alpha-fetoprotein level; serological testing for hepatitis B, C, and D infection; alcohol intake; and the length of follow-up.
Assessment and Definitions of Prognostic Scores
Overall, the assessment of the prognostic scores was done by two authors (MAK and AKH). In case of discordant results, particularly for the CTP score related to one or two missing biological parameters, these missing parameters were scored with 1 or 2 points for the calculation according to the clinical profile of the patient (ie, presence of jaundice gives 2 points for the missing value of bilirubin; otherwise, 1 point). For the MELD scores, NLR and PLR, only the available data were used for their assessment.4,6
The CTP score assessment is based on three biologic parameters (ie prothrombin time, albumin or international normalized ratio, and bilirubin) and two clinical parameters (ie, encephalopathy and ascites) that allow classification into three classes: A (5–6) points, B (7–9 points) and C (at least 10 points).4,5
The MELD score was determined using a formula8 previously reported as follows: 3.78×ln(bilirubin (mg/dL))+11.2×ln(INR)+9.57×ln(serum creatinine (mg/dL))+6.43.
The BCLC staging system is determined based on the tumor size, location and extension; vascular invasion; CTP stages; and performance status and then classified as follows: stage 0 (very early stage), stage A (initial stage), stage B (intermediate stage), stage C (advanced stage), and stage D (terminal stage).4,6 This score has served to classify all patients enrolled in the study.
The performance status of the enrolled patient was appreciated according to the Eastern Cooperative Oncology Group/WHO classification.19
NLR is calculated as the ratio of the absolute number of neutrophils divided by the absolute number of lymphocytes.13
PLR is calculated as the absolute number of platelets count divided by the absolute number of lymphocytes.13
We have considered patients with advanced HCC in palliative treatment, those admitted with a HCC of BCLC, stage C, D and receiving only medication to relieve pain and paracentesis.6
The censored time was the date of discharge for those having faced one hospitalization or the date of the latest hospitalization for those with multiple hospitalizations. Information on the outcome was assessed at the date of discharge (dead or alive). The participation time was calculated as the date of discharge minus the date of first hospitalization.20
Data Analysis
Categorical variables were presented as numbers and percentages, whereas continuous variables were as medians and ranges. The Fisher's and Mann–Whitney U-tests were used to compare categorical and continuous variables. Correlation between prognostic factors was determined using the nonparametric Spearman rho test. To determine the cutoff values of the CTP, MELD scores, BCLC staging system; NLR; and PLR that best stratify the patients into the two levels of the outcome (dead or alive), we used the Cox proportional hazards method to estimate the significant correlation of these prognostic scores with the survival variable using a SAS macro published by Mandrekar21 The survival probabilities were assessed by plotting the Kaplan–Meier curve stratified on the levels of the CTP, MELD scores, BCLC staging system, NLR and PLR then compared with the log rank test and pairwise comparison if necessary.20 By using the survivalROC package in R, published by Heagerty et al22 the accuracies of these prognostic scores in predicting mortality were determined and expressed as sensitivity, specificity, and negative and positive predictive values30 with their respective plotted time-dependent area under the receiver operating characteristic (AUC) curves (ROC) at three time points (30, 60, and 90 days of follow-up). The prognostic value is calculated as follows: true positive+true negative divided by true positive+true negative+false positive+false negative.23 Cox proportional hazard model was used to determine the prognostic factors associated with the in-hospital mortality in patients with HCC.20 The variance inflation factor of the multicollinearity between predictors was determined using a linear regression analysis before the computation of the multivariate Cox proportional hazards analysis.20,24 A value of the variance inflation factor less than 3 points was considered acceptable indicating the absence or low collinearity between predictors.24 All statistical analysis were computed using SAS version 6.09 (SAS Institute Inc., Cary, NC, USA), SPSS version 16 (SPSS Inc., Chicago, USA), and the R software version 4.0.4 (R Core Team, 2020, R Foundation for Statistical Computing, Vienna, Austria) with the two-sided significance level set at 0.05.
Results
Description of the Enrolled Patients
A total of 104 patients (median age: 49.5 years, range 24–86 years, males: 58.7%) were enrolled in the study. All of them were hospitalized for an enlarged liver mass of at least 15.4 cm in size in the right upper thoracic quadrant. The locations of the liver mass were mostly segmental or diffuse in 48 and 29 patients respectively and lobular in 18. Portal vein thrombosis was found in 23.5% of them. Metastases were mostly localized in the lung (nine patients) and nodes (14 patients). With the BCLC score, 41 patients (39.4%) were classified in intermediate stage B, 30 (28.8%) in advanced stage C, and 33 (31.7%) in the terminal stage D. For the CTP score, 89.4% of them were CTP class B or C. The median score values of MELD, NLR, and PLR were, respectively, 14.5, 2.4, and 89.2 in those with completed data.
Overall, 22 among 104 patients with HCC have had missing data for NLR or PLR. However, patients with completed data were not significantly different compared with those having missing data regarding the mean age (49.0 vs 50.5, p=0.7), gender profile (in number) (males: 47 vs 14, p=0.6), disease severity (CTP score: 8 vs 8, p=0.9), and prognosis (BCLC stages C and D: 59.8 vs 63.6%, p=0.9) and, the mortality rate (47.6 vs 31.8%, p=0.2) (Supplementary Table 1). The same observation was made for those having incomplete data for the MELD score (Supplementary Table 2). The clinical and biological characteristics of the enrolled patients are summarized in Table 1.
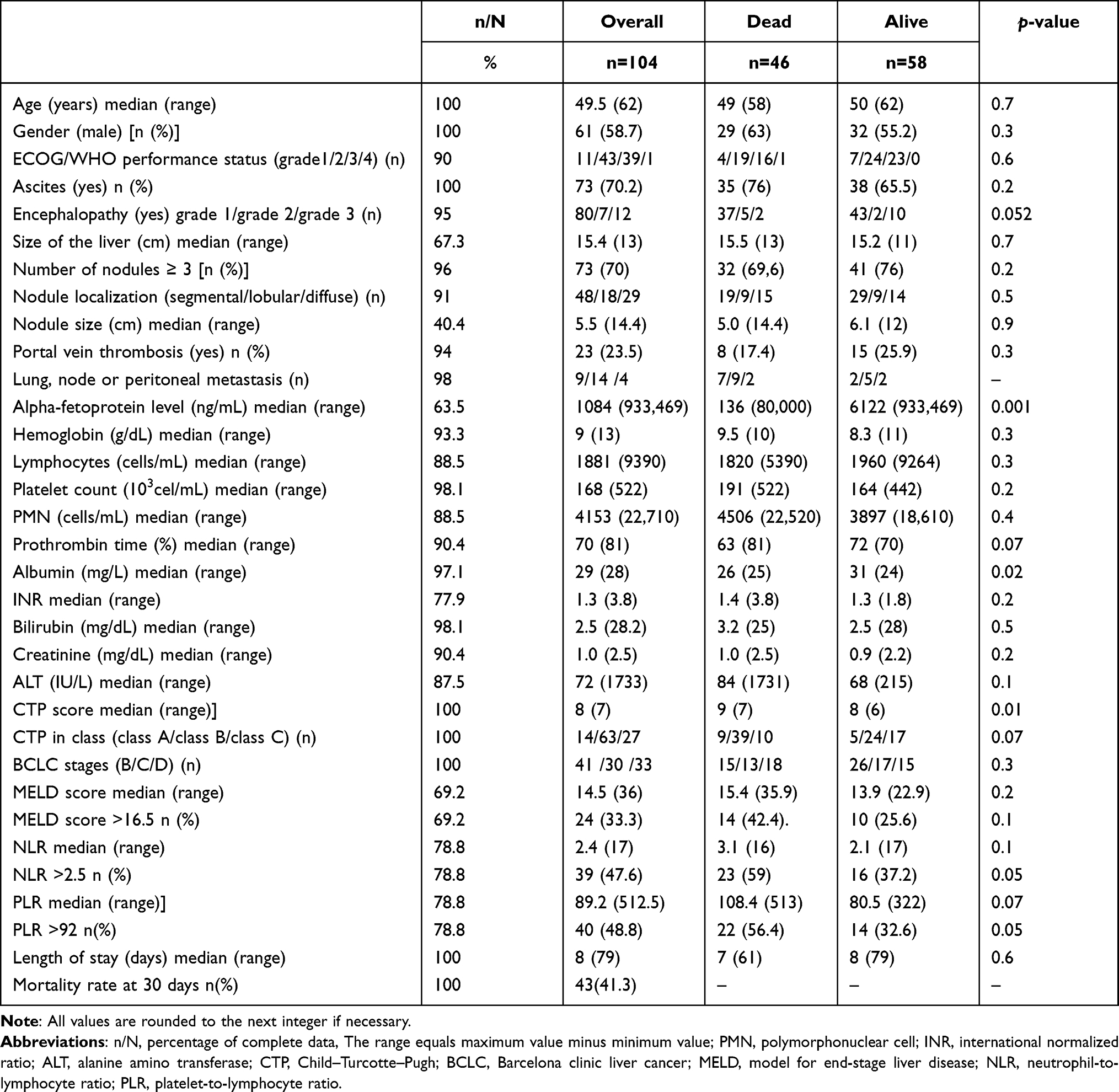 |
Table 1 Baseline Characteristics |
Prediction of Overall Mortality and Determination of Cutoff Values
Overall, 46 patients (44.2%) with HCC died in hospital during a total of 1195 person-days and among them, 43 (87.8) died within 30 days of follow-up. The one-month (30 days) survival probability was of 28% (95%CI: 17–47) and the median survival time was of 17 (95%CI: 11.9–22.1) days. The CTP score (HR=1.28, 95%CI: 1.06–1.55), the MELD score (HR=1.09, 95%CI: 1.04–1.14), the BCLC staging system (HR=1.57, 95%CI: 1.09–2.27), NLR (HR=1.1, 95%CI: 1.01–1.2), and PLR (HR=1.003, 95%CI: 1.001–1.006) were significantly associated with the in-hospital mortality of Black African patients with advanced HCC after computing the Cox proportional univariate analysis (Table 2). Running the macro proposed by Mandrekar et al28 indicated that the best cutoffs that predicted mortality were 2.5 for NLR (C-index=0.756, p=0.04), 92 for PLR (C-index=0.664, p=0.01), and 16.5 for the MELD score (C-index=0.678, p=0.003 (Table 2)). The Kaplan–Meier survival probabilities are plotted in Figure 1. Black African patients with NLR >2.5 (log rank test=7.11, p=0.01) or PLR >92 (log rank test=5.63, p=0.02) experienced poor survival in hospital in comparison with those having low scores. They also experienced poor survival when they were classified in the advanced stages of CTP (class B and C) or BCLC (stage C and D) or had had a MELD score >16.5 (Figure 1). After pairwise comparison, patients with advanced HCC classified CTP class C (p=0.01) and BCLC stage D (p=0.02) were at risk of death compared with those having low stages (Figure 1).
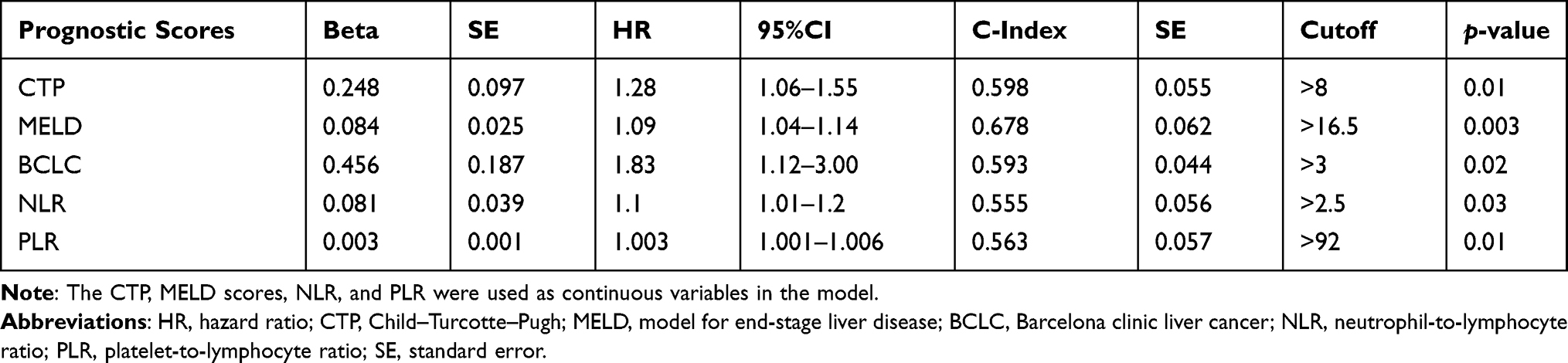 |
Table 2 Univariate Cox Proportional Hazards Regression Analysis with Cutoff Points of the Overall Efficacy of the Prognostic Scores in Predicting Mortality Among Patients with Advanced Hepatocellular Carcinoma in Palliative Treatment |
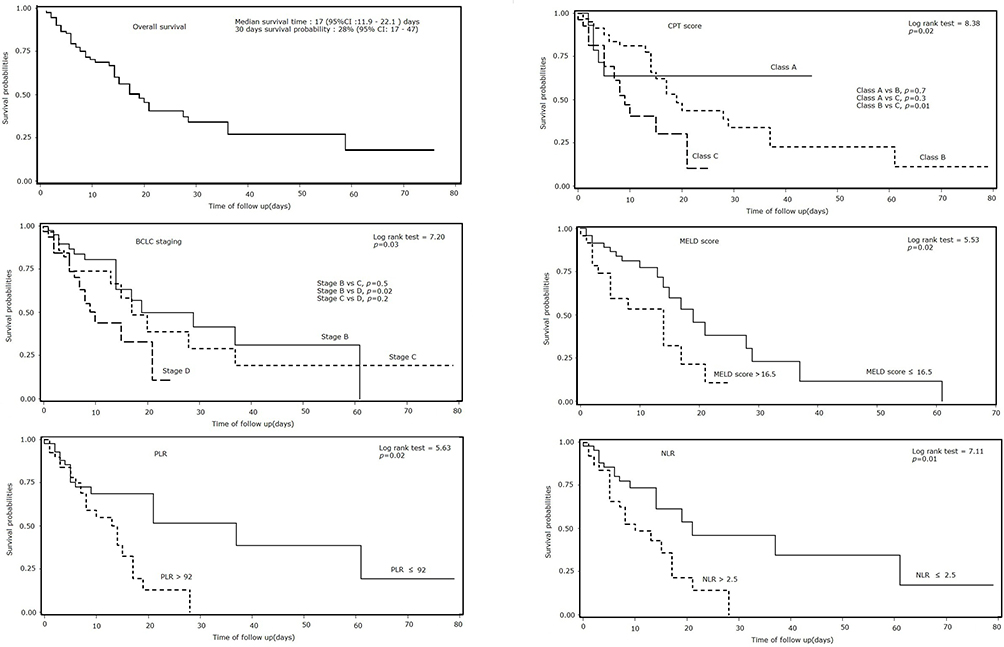 |
Figure 1 Survival probabilities of patients with advanced hepatocellular carcinoma in palliative treatment according to the prognostic scores. Abbreviations: CTP, Child–Turcotte–Pugh; MELD, model for end stage liver disease; BCLC, Barcelona clinic liver cancer; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio. |
Factors Predicting the In-hospital Mortality
Significant correlation was found between CTP and MELD scores (rho test=0.5, p<0.0001), CTP and BCLC scores (rho test=0.5, p<0.0001), MELD and BCLC scores (rho test=0.4; p=0.002), NLR and PLR (rho test=0.4, p<0.0001) and, hemoglobin and ALT (rho test=0.23, p=0.03). However, the linear regression analysis did not show any significant multicollinearity between these predictors as the values of the variance inflation factor were less than 2 points (Supplementary Table 3). Overall, in multivariate analysis (Table 3), factors associated with the in-hospital mortality were as follows: hemoglobin level (HR=1.36, 95%CI: 1.1–1.7, p=0.02), MELD score (HR=1.03, 95%CI: 1.03–1.17, p=0.01), and NLR (HR=1.12, 95%CI = 1.01–1.23, p=0.03). Moreover, in two separate models that encompass NLR or PLR (Table 4), NLR and hemoglobin level showed stable accuracy in predicting mortality whatever the added predictors (CTP, MELD scores and BCLC staging system) compared to PLR. Among CTP, MELD scores and BCLC staging system, only MELD score displayed a prognostic effect when added to NLR or PLR in multivariate analysis (Table 4).
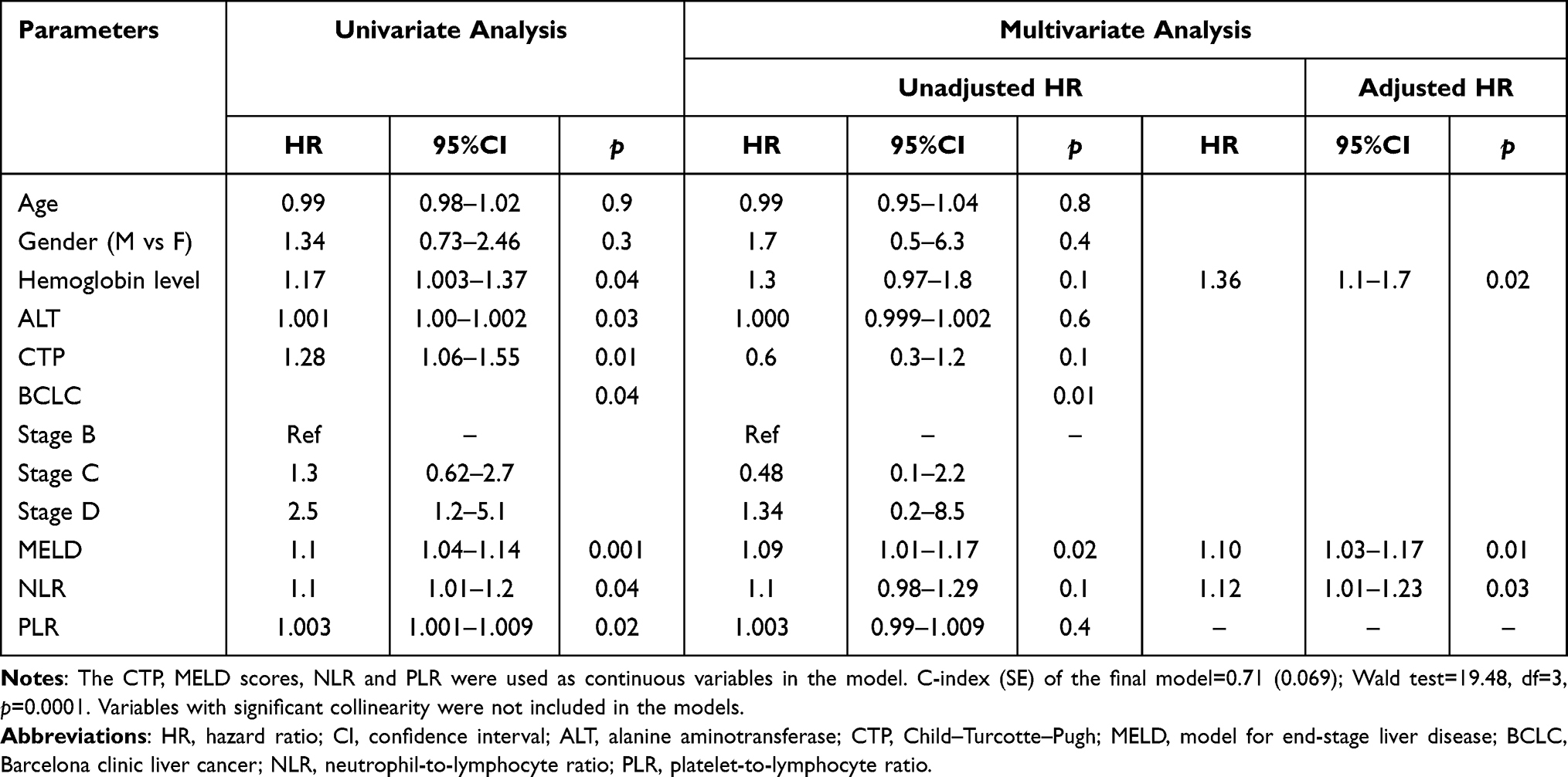 |
Table 3 Prognostic Factors Associated with Mortality Among Patients with Advanced HCC in Palliative Treatment: A Multivariate Cox Regression Univariate and Multivariate Analysis |
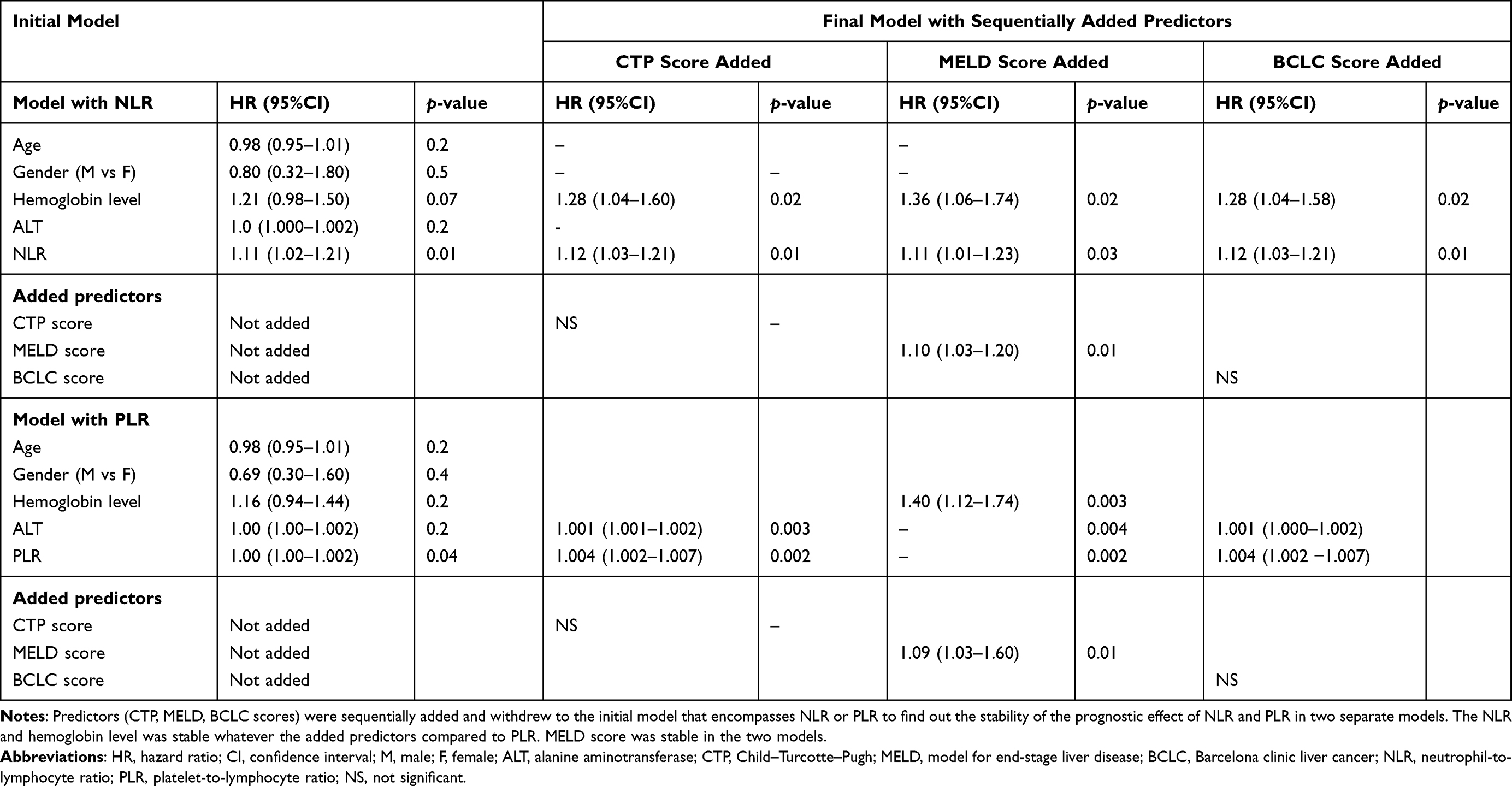 |
Table 4 Prognostic Factors Associated with Mortality Among Patients with Advanced HCC in Palliative Treatment: A Multivariate Cox Regression Analysis with Adjusted Hazard Ratio in Two Separate Models with Neutrophil-to-lymphocyte Ratio and Platelet-to-lymphocyte Ratio |
Accuracy of Prognosis Scores in Predicting the In-hospital Mortality at Different Time Points During Follow-up
Table 5 presents the accuracy and efficacy of the CTP, MELD scores, BCLC staging system; NLR; and PLR in predicting the in-hospital mortality at 30, 60, and 90 days of follow-up. At 30 days, CTP, NLR, and BCLC staging system displayed the most acceptable prognostic values of in-hospital mortality more than 60%. Using a cutoff of 8, the prognostic value of the CTP score reached 69% with a specificity of 83%, positive predictive value of 77% and an AUROC of 0.709. With a cutoff of 2.5, NLR was more accurate at 30 days of follow-up displaying a prognostic value of 87%, a specificity of 68%, and a predictive positive value of 62% and an AUROC of 0.618. Both CTP and NLR were still accurate at day 60 while NLR remained accurate at 90 days of follow-up. In contrast at 90 days of follow-up, the accuracies of BCLC staging system, CTP and MELD scores became statistically nonsignificant as their respective ROC curves crossed the diagonal line of nonsignificant effect (Figure 2). Meanwhile at that time point, PLR displayed an increased predictability with an AUROC ranging from 0.591 at 60 days to 0.688 at 90 days of follow-up (Figure 2). With a cutoff of 92, the specificity and positive predictive value of PLR were respectively of 70 and 67% and the prognostic value of 65% (Table 5, Figure 2).
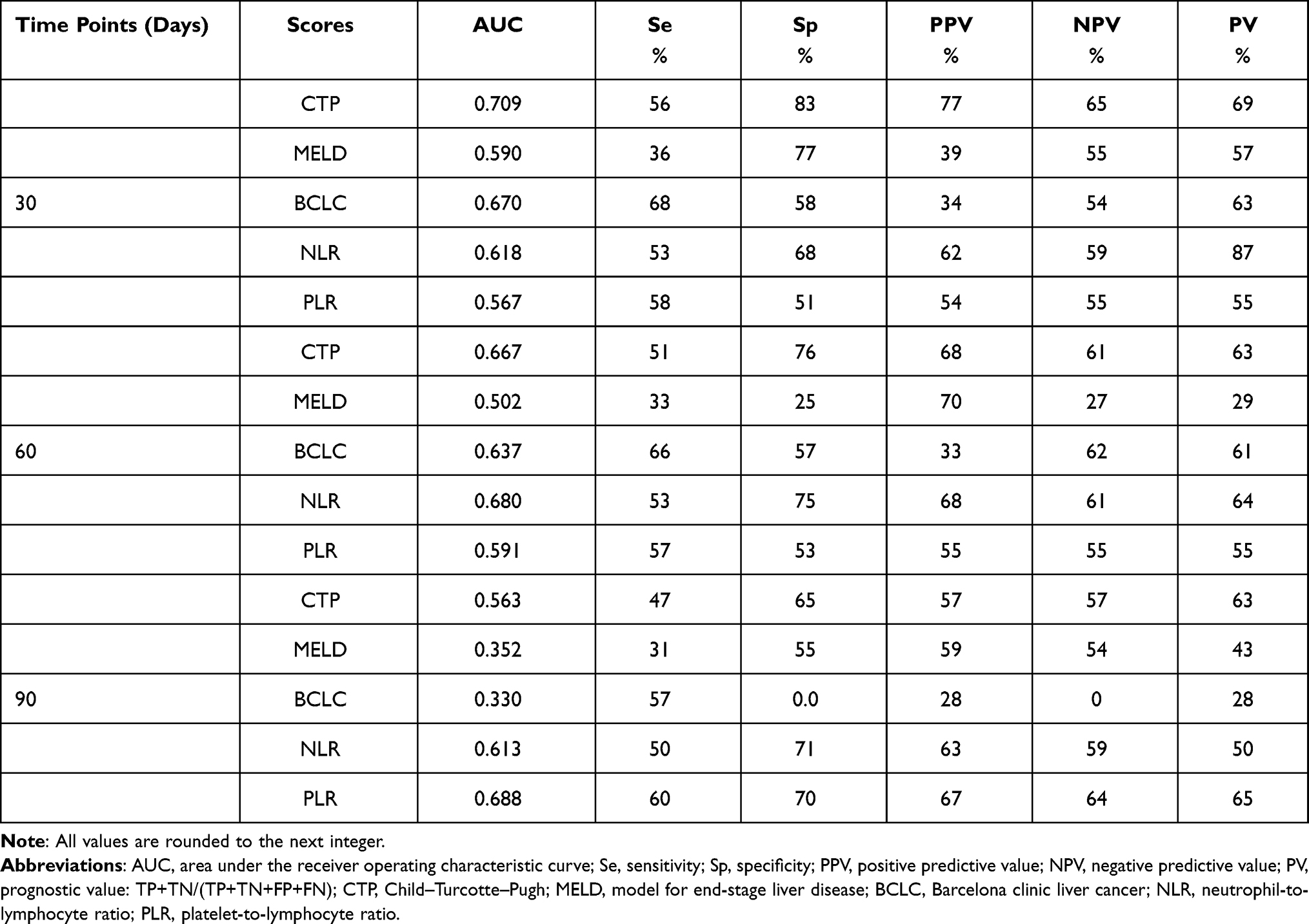 |
Table 5 Values of the Prognostic Scores at Different Time Points in Predicting Mortality Among Patients with Advanced Hepatocellular Carcinoma in Palliative Treatment |
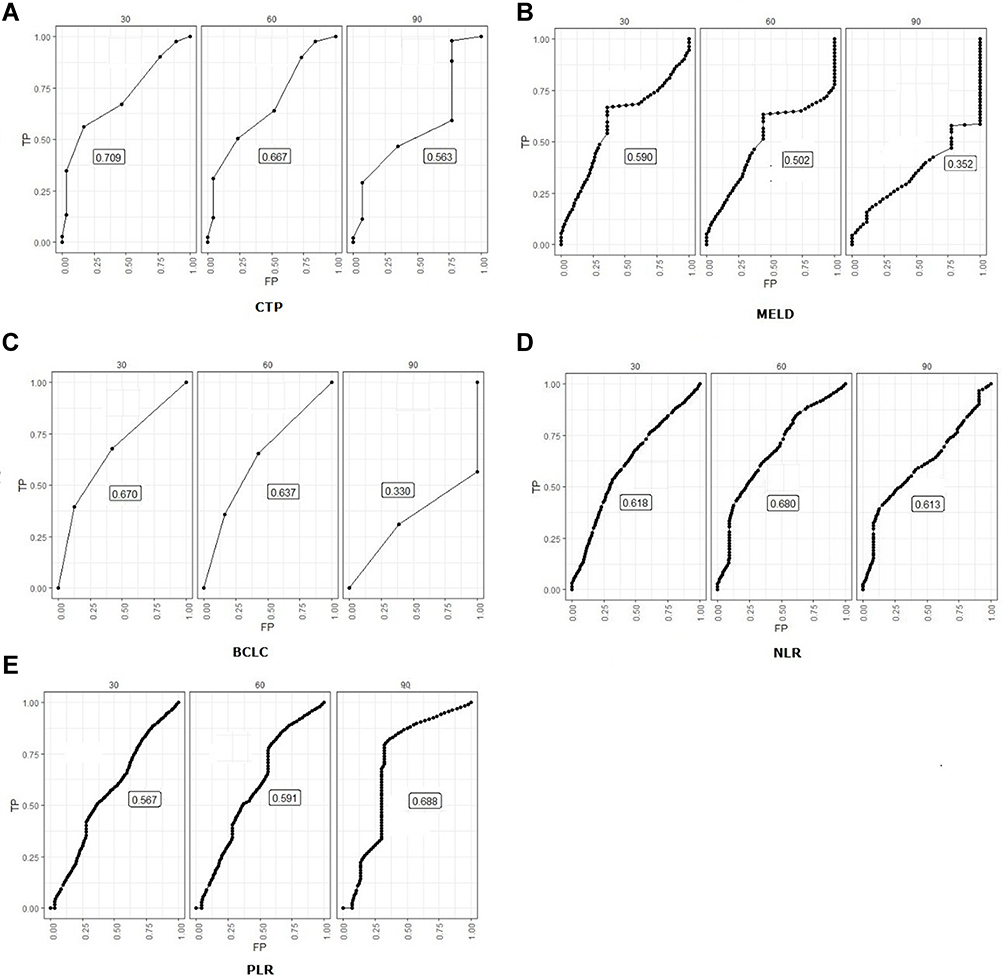 |
Figure 2 Receiver operating characteristic curves depicting the accuracy of the Child–Turcotte–Pugh (A) and MELD (B) scores, Barcelona clinic liver cancer staging system (C), neutrophil-to-lymphocyte ratio (D) and platelet-to-lymphocyte ratio (E) in predicting the in-hospital mortality among patients with advanced hepatocellular carcinoma in palliative treatment at different time points during follow-up. Abbreviations: CTP, Child–Turcotte–Pugh; MELD, model for end stage liver disease; BCLC, Barcelona clinic liver cancer; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet to lymphocyte ratio. |
Discussion
HCC is a challenging condition in sub-Saharan Africa because of its silent course and discovery at the end stage in most patients, the lack of medical facilities or expertise among physicians in-hospital for the administration of an appropriated treatment if necessary.3,16,17,25–27 Our study demonstrates that one month survival was 28% of patients with advanced HCC survived at 30 days. The establishment of a simple and practical tool for routine utilization could be a better approach in these conditions to predict the mortality in such particular patients and to take the appropriate measure for patient treatment or assistance.27 Our study found that NLR, the MELD score and the hemoglobin level predicted the in-hospital mortality in Black Africans with advanced HCC in multivariate analysis. Moreover, NLR displayed a stable accuracy in predicting the in-hospital mortality at different time points during follow-up while PLR seemed to have an increased accuracy after 90 days of follow-up.
Prognostic scores in chronic liver diseases, such as CTP, MELD scores, and BCLC staging system, trigger mainly the liver function impairment that occurs during the natural course of chronic liver disease.4,6,28,29 These prognostic scores share the same key biological parameters (eg, bilirubin and albumin) that depict the liver function.35,36 However, the bilirubin or albumin level may fluctuate in patients having a chronic liver disease with an ongoing and irreversible liver function deterioration during its natural course.28,29 Therefore, the accuracy of CTP, MELD, or BCLC scores assessed at baseline may have limited accuracy in predicting mortality at different time points during follow-up.28–31 In fact, a previous study found significant variation of the MELD score accuracy in predicting mortality of patients with end-stage liver disease on a waiting list for liver transplantation.32 Furthermore the downregulation of the platelet count is common during the natural course of chronic liver disease related to the irreversible liver function deterioration and the splenic sequestration of platelets in cirrhotic patients.33 In addition, thrombocytosis is found to be frequent in those with large HCC tumors.34 Hence, the kinetic variability of the platelet count may explain the low accuracy of PLR in a short period of follow-up in predicting the in-hospital mortality at days 30 and 60 days. However, our study suggests that PLR gained in predictability at 90 days in indicating probably the effect of the decrease of lymphocyte count which is an independent predictor of mortality in patient with HCC in long-term follow-up.35 However, PLR is found to be less accurate than NLR in predicting mortality of patients with HCC.36
Therefore, there is a need for a simple, stable, and readily available tool assessed at baseline that could predict accurately the outcome in patients with chronic liver disease. In our study, NLR was accurate and stable in predicting the in-hospital mortality of Black African patients with advanced HCC at the three time points (ie, 30, 60, and 90 days) of follow-up, compared with CTP, MELD, and BCLC scores and PLR (Figure 2).
The main explanation of this stable prediction of the in-hospital mortality by NLR is probably related to the role of neutrophils and lymphocytes used in the NLR formula. These two elements are derived from the inflammatory process surrounding the onset and the growth of the tumor in the liver and not influenced by the underlying liver function at baseline or during follow-up.10 Moreover, NLR is accurate in predicting survival, whatever the timing of assessment (at baseline or after a treatment), the type of malignancy, or organ involved.14,15,36–40
In our study, the overall prognostic value of NLR in predicting poor survival of patients with HCC was similar to the findings of previous studies that used a cutoff in the range of 2–5.14,36–41 The overall efficacy of NLR was also similar to that of well-known prognostic scores, such as CTP, MELD, and BCLC scores, in patients with HCC in our study. Moreover, our findings are in line with previous studies on the efficacy of NLR in predicting poor survival of patients with HCC that have received sorafenib, transarterial chemoembolization, liver resection or transplantation.36–41 However, given the variability of NLR cutoffs, there is a need for a consensual or standardized one that encompass all stages of HCC and treatment options as suggested by Shelat.15
MELD score >16.5 was associated with poor survival in our study and failed to predict accurately the mortality over 30 days of follow-up. This finding confirms the need for a dynamic assessment of the MELD score to enhance its accuracy in predicting mortality in patients with end-stage liver disease during follow-up, as demonstrated in patients on a waiting list for liver transplantation.29–31
The other key finding in our study was the association of the hemoglobin level with in-hospital mortality, even though no patients displayed high hemoglobin level. However, our study suggests that higher the hemoglobin level, the higher was the risk of death in multivariate analysis. This may be explained by the presence of erythrocytosis related to the particular figure of HCC in Black African patients, as formerly demonstrated in Asian patients with a large volume of liver tumors.42 Liver tumor synthesizes erythropoietin that promotes liver cell proliferation and the rise of the hemoglobin level during the carcinogenesis.43
The main limitation of our study was the sample size and the number of missing data due to the retrospective design of the study, which could have probably jeopardized the accuracy of CTP, MELD, and BCLC scores and PLR over 30 days of follow-up.44 However, the demographic, clinical and prognostic profile of patients in the subsample with missing data did not differ significantly from those with complete data (Supplementary Tables 1 and 2). The absence of systematic differences between the two samples has probably reduced the impact of these missing data on the accuracy of the NLR in our study.44
However, for the first time, to our knowledge, in sub-Saharan Africa, our study provides new insights on the efficacy of a simple, inexpensive, and readily available tool that allows physicians to predict the in-hospital mortality in patients with advanced HCC. Our findings indicate that NLR could also be used in Black African patients with HCC in palliative treatment to predict poor survival with similar efficacy as found in those on a waiting list for liver transplantation or treated in western or Asian countries.35–41 NLR may be used concomitantly with PLR to monitor patients in long-term follow-up.
In conclusion, NLR predicts the in-hospital mortality in Black African patients with advanced HCC and should be integrated into the panel of prognostic tools to be used in clinical practice in countries with limited resources. Further studies with large samples are required to ascertain the efficacy of NLR in patients with HCC in different sub-Saharan African countries.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki and the approval of the protocol by the ethic committee of the Yopougon Teaching Hospital (Direction médicale et scientifique). Approval number: 061/MSHP/CHUY/DMS/okt/yf/20. The informed consent of patients was waived because of the retrospective aspect of the study, the absence of invasive treatments and commercial use of the results of the study and the mystic beliefs surrounding chronic diseases and cancer in Africa. All data were anonymized during the study process and kept confidentially within the gastroenterology and hepatology unit. Data supporting the study could be obtained upon reasonable request.
Acknowledgments
The authors would like to thank Enago (www.enago.com) for language editing and proofreading.
Disclosure
Dr Alassan Kouame Mahassadi reports personal fees from Sanofi Aventis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology. 2021;73(suppl 1):4–13. doi:10.1002/hep.31288
2. World Health Organization. Globocan 2020–liver cancer factsheet. Available from: http://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf.
3. Yang JD, Mohamed EA, Aziz AO, et al. Characteristics, management, and outcomes of patients with hepatocellular carcinoma in Africa: a multicountry observational study from the Africa Liver Cancer Consortium. Lancet Gastroenterol Hepatol. 2017;2(2):103–111. doi:10.1016/S2468-1253(16)30161-3
4. Tandon P, Garcia-Tsao G. Prognostic indicators in hepatocellular carcinoma: a systematic review of 72 studies. Liver Int. 2009;29(4):502–510. doi:10.1111/j.1478-3231.2008.01957.x
5. Pons F, Varela M, Llovet JM. Staging system in hepatocellular carcinoma. HPB (Oxford). 2005;7(1):35–41. doi:10.1080/13651820410024058
6. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
7. Marrero JA, Fontana RJ, Barrat A, et al. Prognosis of hepatocellular carcinoma: comparison of 7 staging systems in an American cohort. Hepatology. 2005;41(4):707–716. doi:10.1002/hep.20636
8. Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124(1):91–96. doi:10.1053/gast.2003.50016
9. Khalaf N, Ying J, Mittal S, et al. Natural history of untreated hepatocellular carcinoma in a US cohort and the role of cancer surveillance. Clin Gastroenterol Hepatol. 2017;15(2):273–281.e1. doi:10.1016/j.cgh.2016.07.033
10. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. 2018;19(3):222–232. doi:10.1038/s41590-018-0044-z
11. Yu LX, Ling Y, Wang HY. Role of non resolving inflammation in hepatocellular carcinoma development and progression. NPJ Precis Oncol. 2018;2(1):6. doi:10.1038/s41698-018-0048-z
12. Bihari C, Rastogi A, Shasthry SM, et al. Platelets contribute to growth and metastasis in hepatocellular carcinoma. J Pathol Microbiol Immunol. 2016;124(9):776–786.
13. Zheng J, Cai J, Li H, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: a meta-analysis and systematic review. Cell Physiol Biochem. 2017;44(3):967–981. doi:10.1159/000485396
14. Dan J, Zhang Y, Peng Z, et al. postoperative neutrophil-to-lymphocyte ratio change predicts survival of patients with small hepatocellular carcinoma undergoing radiofrequency ablation. PLoS One. 2013;8(3):e58184. doi:10.1371/journal.pone.0058184
15. Shelat VG. Role of inflammatory indices in management of hepatocellular carcinoma-neutrophil to lymphocyte ratio. Ann Transl Med. 2020;8(15):912. doi:10.21037/atm-2020-90
16. Diallo I, Ndiaye B, Touré M, et al. Hepatocellular carcinoma in Senegal: epidemiological, clinical and etiological aspects about 229 cases at hopital principal de Dakar. Pan Afr Med J. 2021;38:99. doi:10.11604/pamj.2021.38.99.25195
17. Tachi K, Agyei-Nkansah A, Archampong T. Hepatocellular carcinoma in Ghana: a retrospective analysis of a tertiary hospital data. Pan Afr Med J. 2020;36(43):43. doi:10.11604/pamj.2020.36.43.21085
18. Venkatesh SK, Chandan V, Roberts LR. Liver masses: a clinical, radiological and pathological perspective for: perspectives in clinical gastroenterology and hepatology. Clin Gastroenterol Hepatol. 2014;12(9):1414–1429. doi:10.1016/j.cgh.2013.09.017
19. West HJ, Jin JO. Performance status in cancer. JAMA Oncol. 2015;1(7):998. doi:10.1001/jamaoncol.2015.3113
20. Colak E, Ozen H, Emir B, Oner S. Pairwise multiple comparison adjustment procedure for survival functions with right-censored data. Comput Math Methods Med. 2017;9270450. doi:10.1155/2017/9270450
21. Mandrekar JN. Cutpoint determination methods in survival analysis using SAS® macro. Available from: https://support.sas.com/resources/papers/proceedings/proceedings/sugi28/261-28.pdf.
22. Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000;56(2):337–344. doi:10.1111/j.0006-341X.2000.00337.x
23. Simundic AM. Measures of prognostic value: basic definitions. J Int Federation. 2009;19(4):203–211.
24. Akinwande OM, Dikko GH, Samson A. Variance inflation factor: as condition for the inclusion of suppressor variable(s) in regression analysis. Open J Statistics. 2015;05:754–767. doi:10.4236/ojs.2015.57075
25. Ladep NG, Lesi OA, Mark P, et al. Problem of hepatocellular carcinoma in West Africa. World J Hepatol. 2014;6(11):783–792. doi:10.4254/wjh.v6.i11.783
26. Mandeville KL, Krabshuis J, Ladep NG, Mulder CJ, Quigley EM, Khan SA. Gastroenterology in developing countries: issues and advances. World J Gastroenterol. 2009;15(23):2839–2854. doi:10.3748/wjg.15.2839
27. Ladep NG, Taylor-Robinson SD. Management of liver disease in Nigeria. Clin Med (Lond). 2007;7(5):439–441. doi:10.7861/clinmedicine.7-5-439
28. D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217–231. doi:10.1016/j.jhep.2005.10.013
29. Botta F, Giannini E, Romagnoli P, et al. MELD scoring system is useful for predicting prognosis in patient with liver cirrhosis and is correlated with residual liver function: a European study. Gut. 2003;52(1):134–139. doi:10.1136/gut.52.1.134
30. Christensen E. Prognostic models including the Child-Pugh, MELD and Mayo risk scores: where are we and where should we go? J Hepatol. 2004;41(2):344–350. doi:10.1016/j.jhep.2004.06.005
31. Bernardi M, Gitto S, Biselli M. The MELD score in patients awaiting liver transplant: strengths and weaknesses. J Hepatol. 2011;54(6):1297–1306. doi:10.1016/j.jhep.2010.11.008
32. Gheorghe L, Iacob S, Iacob R, Gheorghe C, Popescu I. Variation of the MELD score as a predictor of death on the waiting list for liver transplantation. J Gastrointestin Liver Dis. 2007;16(3):267–272.
33. Toghill PJ, Green S, Ferguson F. Platelets dynamics in chronic liver disease with special reference to the role of the spleen. J Clin Pathol. 1977;30(4):367–371. doi:10.1136/jcp.30.4.367
34. Hwang SJ, Luo JC, Li CP, et al. Thrombocytosis: a paraneoplastic syndrome in patient with hepatocellular carcinoma. World J Gastroenterol. 2004;10(17):2472–2477. doi:10.3748/wjg.v10.i17.2472
35. Hong YM, Yoon KT, Hwang TH, Cho M. Pretreatment peripheral neutrophils, lymphocytes and monocytes predict long term survival in hepatocellular carcinoma. Br Med Cancer. 2020;20:
36. Kabir T, Ye M, Noor Mohd NA, Woon W, Junnarkar SP, Shelat VG. Preoperative neutrophil-to-lymphocyte ratio plus platelet-to-lymphocyte ratio predicts the outcomes after curative resection for hepatocellular carcinoma. Inter J Hepatol. 2019;9. doi:10.1155/2019/4239463
37. Shi L, Wang B, Wang B, et al. Prognostic role of pretreatment blood neutrophil-to-lymphocyte ratio in advanced cancer survivors: a systematic review and meta-analysis of 66 cohort studies. M Ei Z Cancer Treat Rev. 2017;58:1–13. doi:10.1016/j.ctrv.2017.05.005
38. Gao F, Li X, Geng M, et al. Pretreatement neutrophil–lymphocyte ratio. An independent predictor of survival in patient with hepatocellular carcinoma. Medicine. 2015;94(11):1–7. doi:10.1097/MD.0000000000000639
39. Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124
40. Xue TC, Zhang L, Xie XY, et al. Prognostic significance of the neutrophil-to-lymphocyte ratio in primary liver cancer: a meta-analysis. PLoS One. 2014;9(5):e96072. doi:10.1371/journal.pone.0096072
41. Harding-Theobald E, Yao FYK, Mehta N. Neutrophil-to-lymphocyte ratio predicts high risk explant features and waitlist survival but is not independently associated with recurrence or survival following liver transplantation for hepatocellular carcinoma. Liver Transpl. 2021;27(6):818–829. doi:10.1002/lt.26010.
42. Luo JC, Hwang SJ, Wu JC, et al. Paraneoplastic syndromes in patients with hepatocellular carcinoma in Taïwan. Cancer. 1999;86(5):799–804.
43. Ribatti D, Marzullo A, Gentile A, et al. Erythropoietin/erythropoietin-receptor system is involved in angiogenesis in human hepatocellular carcinoma. Histopathology. 2007;50(5):591–596. doi:10.1111/j.1365-2559.2007.02654.x
44. Ibrahim JG, Chu H, Chen MH. Missing data in clinical studies: issues and methods. J Clin Oncol. 2012;30(26):3297–3303. doi:10.1200/JCO.2011.38.7589
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.