Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
The Prognostic Value of Circulating Stem Cells Expressing PD-L1 in Patients with Hepatocellular Carcinoma
Authors Roy D, Oppermann E, Vogl TJ ![]() , Büdeyri I
, Büdeyri I ![]() , Shapiro D, Struecker B, Rolfo CD, Abedin N, Zharov VP, Schnitzbauer A, Pascher A, Bechstein WO, Zimmermann MS, Juratli MA
, Shapiro D, Struecker B, Rolfo CD, Abedin N, Zharov VP, Schnitzbauer A, Pascher A, Bechstein WO, Zimmermann MS, Juratli MA
Received 25 January 2026
Accepted for publication 11 April 2026
Published 18 May 2026 Volume 2026:13 598753
DOI https://doi.org/10.2147/JHC.S598753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Imam Waked
Dhruvajyoti Roy,1,* Elsie Oppermann,2,* Thomas J Vogl,3 Ibrahim Büdeyri,4 Dmitry Shapiro,4 Benjamin Struecker,4 Christian D Rolfo,5 Nada Abedin,6 Vladimir P Zharov,7 Andreas Schnitzbauer,8 Andreas Pascher,4 Wolf O Bechstein,2 Markus S Zimmermann,9,* Mazen A Juratli4,*
1Department of Breast Surgical Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, TX, USA; 2Department of General, Visceral and Transplant Surgery, Frankfurt University Hospital, Frankfurt, Germany; 3Department of Diagnostic and Interventional Radiology, Frankfurt University Hospital, Frankfurt, Germany; 4Department of General, Visceral and Transplant Surgery, Muenster University Hospital, Muenster, Germany; 5Center for Thoracic Oncology, The Tisch Cancer Institute, Mount Sinai Health System, New York City, NY, USA; 6Department of Internal Medicine I, Frankfurt University Hospital, Frankfurt, Germany; 7Arkansas Nanomedicine Center, University of Arkansas for Medical Sciences, Fayetteville, AR, USA; 8Department of Visceral, Oncological, and Transplant Surgery, University Hospital Knappschaftskrankenhaus, Bochum, Germany; 9Clinic for General and Visceral Surgery, Schön Clinic Neustadt, Neustadt in Holstein, Germany
*These authors contributed equally to this work
Correspondence: Mazen A Juratli, Department of General, Visceral and Transplant Surgery, Muenster University Hospital, Muenster, Germany, Email [email protected]
Background: Hepatocellular carcinoma (HCC) is associated with high recurrence rates despite curative-intent liver resection. This necessitates improved prognostic tools and novel therapeutic strategies, including immune checkpoint inhibitors (ICIs). Circulating stem cells (CSCs) have emerged as potential prognostic biomarkers.
Aim: To assess the prognostic relevance of CSCs expressing programmed death-ligand 1 (PD-L1+CSCs) in relation to recurrence-free survival (RFS) and overall survival (OS) in patients undergoing surgery for HCC.
Methods: PD-L1+CSCs (CD45−/CD146+/ASGPR+/CD90+/PD-L1+) were analyzed in 27 HCC patients before surgery, immediately after surgery, and at 6 and 12 months after surgery using fluorescence-activated cell sorting and immunofluorescence microscopy. Tumor recurrence was monitored biannually through alpha-fetoprotein (AFP) measurements and imaging (CT/MRI). Control groups included patients with benign liver disease, non-HCC malignancies, and healthy donors.
Results: Before surgery, 29.7% (8/27) of HCC patients had detectable PD-L1+CSCs. Postoperatively, their frequency initially declined to 22.3%, followed by a significant rise to 85% at six months and 88% at twelve months (both p < 0.01). Increasing postoperative PD-L1+CSC levels were associated with tumor recurrence (51.8%). The presence of preoperative PD-L1+CSCs correlated with reduced OS (p = 0.05) and shorter RFS (p = 0.07).
Conclusion: PD-L1+CSCs are associated with poor oncological outcomes and represent promising prognostic and therapeutic targets in HCC.
Keywords: cancer biomarkers, liquid biopsy, cancer stemness, tumor recurrence monitoring
Introduction
Hepatocellular carcinoma (HCC) ranks among the most prevalent cancers globally and is the third leading cause of cancer-related death worldwide.1–3 The overall prognosis for patients with liver cancer remains dismal, with an estimated 5-year survival rate of only 12.7%,4,5 primarily due to recurrence and metastasis postresection. Resection is the preferred treatment for early-stage localized tumors, whereas liver transplantation (LT) is often chosen as an alternative, potentially curative option for HCC. Surgical treatments, encompassing both hepatic resection and LT, have historically been central to curative approaches for HCC, offering the best outcomes, with a 5-year survival rate of approximately 70–80%.6,7 AFP is the most widely used biomarker for early HCC detection and the only biomarker validated for clinical application. However, its routine use in HCC surveillance is controversial because of concerns about its specificity and limited sensitivity as well as poor predictive value.8,9 The well-recognized limitations of AFP have spurred investigation into novel prognostic biomarkers; recent studies identifying the miR-3130-5p/FDX1 cuproptosis axis10 and PRDX6 expression11 as independent prognostic determinants in HCC underscore the unmet clinical need for biomarkers that transcend AFP. However, the absence of sensitive and precise indicators for the early detection of HCC metastasis and recurrence hinder timely intervention, causing many patients to miss out on viable treatment periods. Consequently, the 3- and 5-year survival rates for individuals with HCC remain suboptimal.12
In recent years, immunotherapy has been developed to strengthen cancer immunosurveillance. These monoclonal antibodies targeting the checkpoint molecules PD-1 and programmed cell death ligand 1 (PD-L1) have been shown to be effective in multiple cancers.13–15 The benefit of immune checkpoint inhibitors (ICIs) is achieved in approximately 50% of patients; predictive markers have been widely investigated.16 A recent comprehensive review has further highlighted the expanding role of ICI-based strategies in HCC beyond advanced disease, including their potential as downstaging and conversion modalities and their complex intersection with liver transplantation, reinforcing the critical need for reliable predictive biomarkers to guide patient selection and optimize therapeutic sequencing.17 Hence, it is imperative to identify and employ novel biomarkers to monitor the prognosis of HCC patients effectively.
Several studies have demonstrated the potential of circulating tumor cells (CTCs) as biomarkers for predicting the clinical outcomes of patients with various cancers.18–22 A subpopulation of CTCs with stem cell features, such as self-renewal, multipotency, and tumorigenicity, and likely showing markers of epithelial-to-mesenchymal transition (EMT), may be relevant players during metastasis.23–25 In addition, a subpopulation of CTCs may retain stem cell features that allow these cells to initiate new tumors in distal locations, namely, metastases.22,26,27 Therefore, the identification of circulating stem cell (CSC)-specific biomarkers becomes relevant for assessing the content of tumorigenic CTCs, which may provide a more accurate measure of tumor prognosis.28,29
Currently, interest in identifying and detecting aggressive CSC markers in blood is increasing.24,25,28 CSCs constitute a distinct subpopulation of tumors with the ability to initiate tumor growth and sustain tumor self-renewal. Emerging evidence suggests that CSCs are linked to metastasis, chemotherapy resistance, radiotherapy resistance and recurrence.24,27 CSC markers are frequently upregulated in the CTCs of patients with metastatic breast cancer, and most CTCs exhibit CSC phenotypes characterized by quiescence and chemotherapy resistance.24,30,31 These characteristics imply that the progenitor cells of metastases may originate from the CTC population. Recently, the detection of CTCs, including CSCs in peripheral blood, has been demonstrated to serve as a valuable tool for identifying high-risk recurrence and poor prognosis in patients with Dukes’ stage B and C colorectal cancer.32 CSCs have been identified in several solid tumors, such as colorectal cancer32,33 and breast cancer.24,30,31 The potential prognostic value of CSCs has already been highlighted in a 2011 paper, where CSCs were shown to predict recurrence in HCC patients after surgical resection.34
In the present study, we investigated the clinical significance of perioperative CSCs in HCC patients. We hypothesized that PD-L1+CSCs represent a potential source of HCC recurrence as well as metastasis; therefore, the detection of PD-L1+CSCs might correlate with adverse clinical outcomes. To test this hypothesis, we used standardized fluorescence-activated cell sorting (FACS) and immunofluorescence (IF) microscopy to explore the prevalence, dynamic changes, and prognostic significance of these cells in HCC patients undergoing curative resection in a prospective manner. In this study, we also aimed to investigate whether the quantity of PD-L1+CSCs could predict HCC recurrence after resection.
Materials and Methods
Study Population
Our prospective single-center cohort study was conducted at the Johann Wolfgang Goethe University Frankfurt between August 2016 and July 2018. The study included 27 HCC patients scheduled for liver resection, 13 patients with nonmalignant liver disease (NMLD), 16 patients with tumors other than HCC (non-HCC) and 8 healthy donors. For the HCC group, patients were excluded if they had liver metastases of extrahepatic origin, unresectable intrahepatic disease with major vessel involvement, concurrent HIV infection, or severe comorbidities. Due to tumor-related deaths and other reasons for discontinuation, the number of patients decreased to 20 at the first follow-up (6 months post-resection) and to 17 at the second follow-up (12 months post-surgery).
For tumor staging, the Barcelona Clinic Liver Cancer (BCLC) criteria were applied, and tumor grading was performed according to the Edmondson grading system. While the BCLC guidelines typically recommend that patients with BCLC B/C stage are not suitable for surgical resection, our inclusion criteria allowed surgical intervention after multidisciplinary-team assessment, if liver function was preserved (Child–Pugh A), future liver remnant volume was adequate, and no extrahepatic disease was present. For patients with multiple lesions (BCLC B stage), “tumor size” refers to the diameter of the largest lesion, consistent with BCLC criteria. The HCC Patients received segmental resection or hemihepatectomy and were subsequently monitored for recurrence every six months after resection through alpha-fetoprotein (AFP) and CT or MRI imaging for up to four years. Following tumor resection, none of the patients received adjuvant therapy, as determined by the consensus recommendation of a multidisciplinary tumor board.
Study Design
Blood samples were taken from 27 HCC patients at three points: just before their tumor removal surgery from the central venous catheter, shortly after surgery on the same day, and again during follow-up visits at 6 and 12 months. These patients were monitored for cancer recurrence every six months using CT or MRI scans, with a median follow-up duration of 3.7 years (ranging from 2.5 to 4.3 years). Importantly, none of the patients received additional therapy after surgery. To clarify our study design and patient progress, we have added a flowchart in Figure 1 that shows how patients were enrolled, when blood samples were collected, and the schedule for recurrence monitoring. For the control groups (NMLD and non-HCC patients), blood samples were obtained both before and after surgery, but no follow-up observations were conducted. Healthy donor blood samples were collected only once. All blood draws used EDTA tubes (Sarstedt, Nümbrecht, Germany).
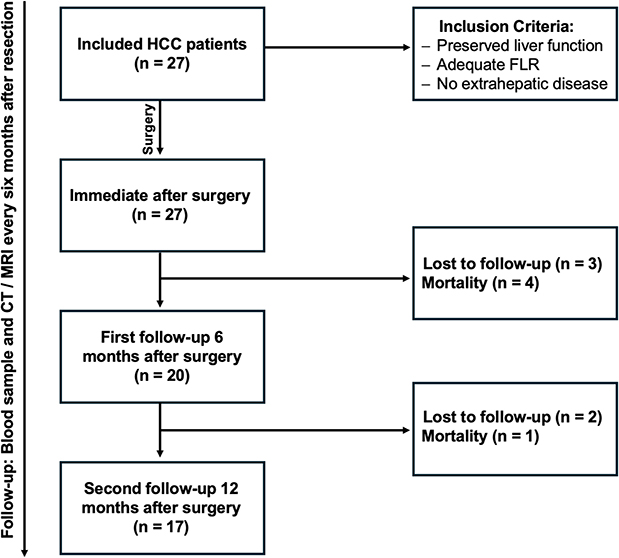 |
Figure 1 A flowchart detailing the study design, patient enrolment procedures, and follow-up protocol. Abbreviations: HCC, Hepatocellular carcinoma; FLR, Future liver remnant. |
This study was approved by the ethics committee of the University of Frankfurt (approval number: 321/16). Written informed consent was obtained from all participants prior to data collection and analysis. The study was registered in the German Clinical Trials Register (DRKS) under the clinical trial number: DRKS00034959, registration date: August 26, 2024. This article does not contain any studies with animal subjects. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2024.
Enrichment and Detection of CSCs
Blood samples (7.5 mL) were collected from each patient, and peripheral blood mononuclear cells (PBMCs) were separated from venous blood via gradient centrifugation via OncoQuick® (Greiner Bio-One, Kremsmünster, Austria). In this step, the blood was pipetted above the filter of the precooled OncoQuick® tube and then centrifuged at 1600 × g and 4 °C for 20 minutes. The isolated cells were washed twice with phosphate-buffered saline (PBS; Gibco/Invitrogen, Karlsruhe, Germany) without Ca++ or Mg++ containing 0.5% bovine serum albumin (BSA; Sigma‒Aldrich Chemie GmbH, Munich, Germany) and transferred into FACS tubes. The cells were incubated with a cocktail of the following fluorescent-labeled antibodies: Anti-human Asialoglycoprotein Receptor 1 antibody (ASGPR-1)-PE (BD Pharmingen, Heidelberg, Germany), anti-human CD146 antibody (also called Melanoma Cell Adhesion Molecule, MCAM-APC; clone: SHM-57 (BioLegend, San Diego, CA, USA), anti-CD274 (PD-L1)-BV421; clone: MIH1 (BD Bioscience), anti-CD90-PerCP/Cy5.5; clone: 5E10; and anti-CD45-FITC; clone: HI30 (BD Pharmingen)) for one hour at 4°C. After the unbound antibodies were washed twice with PBS containing 0.5% BSA, the sample was analyzed via four-laser FACSAria Fusion (BD Biosciences, CA, US) and FACSDiva Software (version BD FACSDiva 8.0.1) (Figure 2). CTCs were defined as CD45-/CD146+/ASGPR+ cells. Additionally, an aggressive subpopulation (PD-L1+CSCs) was defined by the co-expression of PD-L1 (CD274) and CD90.
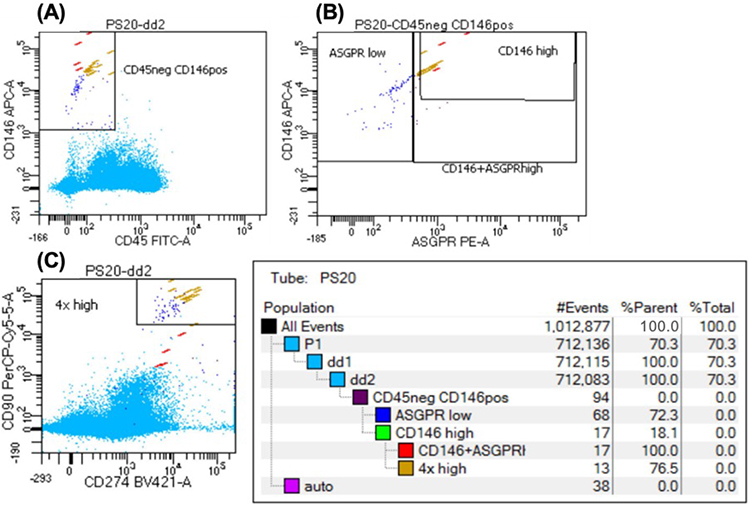 |
Figure 2 Flow cytometry gating strategy for identifying PD-L1+CSCs. (A) Doublet Exclusion: SSC-W vs. SSC-H was used to exclude cell doublets and aggregates. (B) Marker Gating: CD45-neg, CD146-high, and ASGPR-high populations were gated. (C) Further Analysis: CD274 and CD90 were analyzed within these gated populations. |
The protocol described above was developed in previous studies by our research group.35 Pretrials were performed with cell lines (HepG2, Cell Lines Service GmbH, Eppelheim, Germany) and healthy donors to evaluate the sensitivity and specificity of our selected antibodies.
End Points
The primary end point was OS which defined as the time between the date of surgery and death from any cause or last follow-up. Secondary end points included RFS, PD-L1+CSC counts, tumor volume and size, AFP levels, IL-6 levels, microvascular invasion (MVI), tumor-free resection margin (R0). RFS was defined as the interval between surgery and recurrence detection via imaging (CT or MRI). For patients without recurrence or death by the study’s end, RFS and OS were censored at the last follow-up date. We defined early recurrence as tumor recurrence within 12 months following surgical resection keeping in line with the literature.36–39 We assessed the presence of PD-L1+CSCs (≥0.1/mL) in HCC patients at different time points relative to surgery.
Immunofluorescence Microscopy
In this study, we employed distinct antibody cocktails to verify cellular populations by targeting specific cell surface markers. This approach facilitates comprehensive verification through multiparameter analysis, ensuring accurate identification across various research applications. For verification purposes, one antibody cocktail was utilized. The cocktail included anti-CD90-PE, anti-ASGPR-APC, anti-CD45-FITC and FCR-blockers (5 µL each). The cocktail was meticulously applied to samples, followed by immunofluorescence microscopy analysis.
Immunofluorescence microscopy (Zeiss Axio Observer Z-1, Zeiss, Jena, Germany) revealed distinct staining patterns corresponding to the targeted cell surface markers within each cocktail. By scrutinizing fluorescence signals and colocalization patterns, we successfully validated the identity of CSCs within the samples (Figure 3).
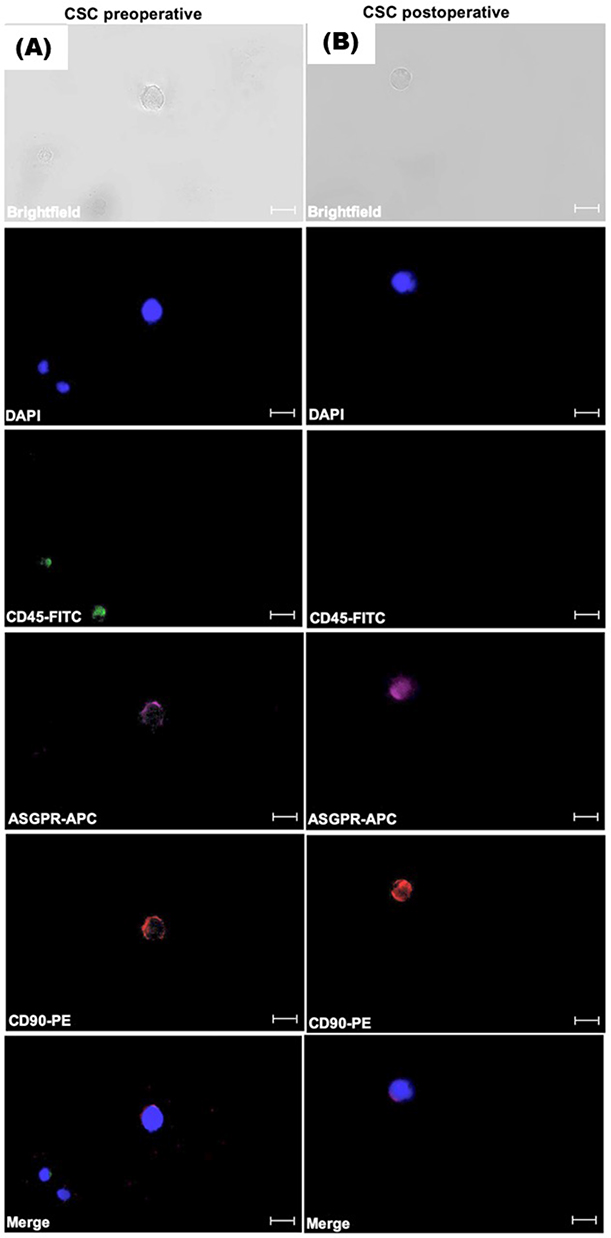 |
Figure 3 Identification of example CSCs via immunofluorescence by DAPI, CD45-FITC, ASGPR-APC and CD90-PE in HCC patients. (A) Identification of CSCs preoperatively. (B) Identification of CSCs postoperatively. Scale bar: 50 μm. |
Statistical Analysis
Cross-sectional analysis was used to compare PD-L1+CSC levels between the HCC group and the control group. PD-L1+CSC enumeration was reported per 1 mL of blood and compared among groups via the nonparametric Mann‒Whitney U-test and the Kruskal‒Wallis test. Changes in the number of CSCs depending on the time of sample collection were analyzed via the Wilcoxon signed rank test.
HCC patients were followed up until July 2023. Medical patient data were taken from the electronic patient records. RFS was calculated as the time from surgery to the time of diagnosis of recurrence via MRI. OS was calculated as the time from surgery to death. In the case of nonrecurrence or survival until the end of our observational period, the RFS and OS were assumed until this timepoint. The landmark method was used to analyze time‒event data. Kaplan‒Meier survival curves were compared via the Log rank test.
The statistical analyses were carried out with SAS Version 9.4 (SAS Institute Inc., North Carolina, USA). A p value less than 0.05 was considered statistically significant. An analysis was performed via Prism software version 8.0 (GraphPad, La Jolla, CA). An unpaired t-test with Welch’s correction was performed to assess the significance of differences in data distribution. A p value of less than 0.05 was considered significant. Binary logistic regression analysis was performed, and receiver operating characteristic (ROC) curves were generated to evaluate the ability of the chosen markers to discriminate cancer patients from controls.
The time to recurrence (TTR) was defined as the interval between surgery and recurrence. The cumulative recurrence and survival rates were calculated via the Kaplan–Meier method and analyzed via the Log rank test. Univariate and multivariate analyses were performed with the Cox proportional hazards regression model. All p values were two-sided, with p < 0.05 considered statistically significant.
Results
Patient Characteristics
Table 1 summarizes the clinical demographics and tumor characteristics of the 27 patients with HCC enrolled in our study. Table 2 delineates a comparative distribution of gender and age among 56 patients. The mean (±SD) age of the patients was 62 ± 14.8 years (range 28–83 years), and 74.1% were male. Among these patients, 44.5% had liver cirrhosis, 77.7% had liver fibrosis, and 59.3% were AFP-positive. Most patients (85.1%) had no metabolic-associated steatohepatitis (MASH). More than half of the patients (59.3%) were not diabetic. A total of 74.1% of the patients had no alcohol abuse, and 63% had no hepatitis virus infection in their medical history. According to the BCLC staging, 51.8% (n=14) were classified as stage 0 or A, while 48.2% (n=13) were stage B or C. Five BCLC B/C patients received preoperative down-staging therapy to enable resection. A total of 59.3% of the patients had a tumor larger than 5 cm. The mean tumor volume was approximately 460 cm3. The majority of the patients (85.1%) underwent open surgery rather than laparoscopic surgery. A total of 81.0% of the patients did not receive any preoperative therapy, such as microwave ablation, chemotherapy, radiation, or transarterial chemoembolization. A small portion of the patients (14.9%) had a high-grade tumor (Grade 3). A total of 29.7% had microvascular invasion, and 85.1% had a tumor-free resection margin. Postoperatively, recurrence and mortality rates were both 51.8% (n=14).
 |
Table 1 Clinical Characteristics and Pathological Data of the HCC Patients |
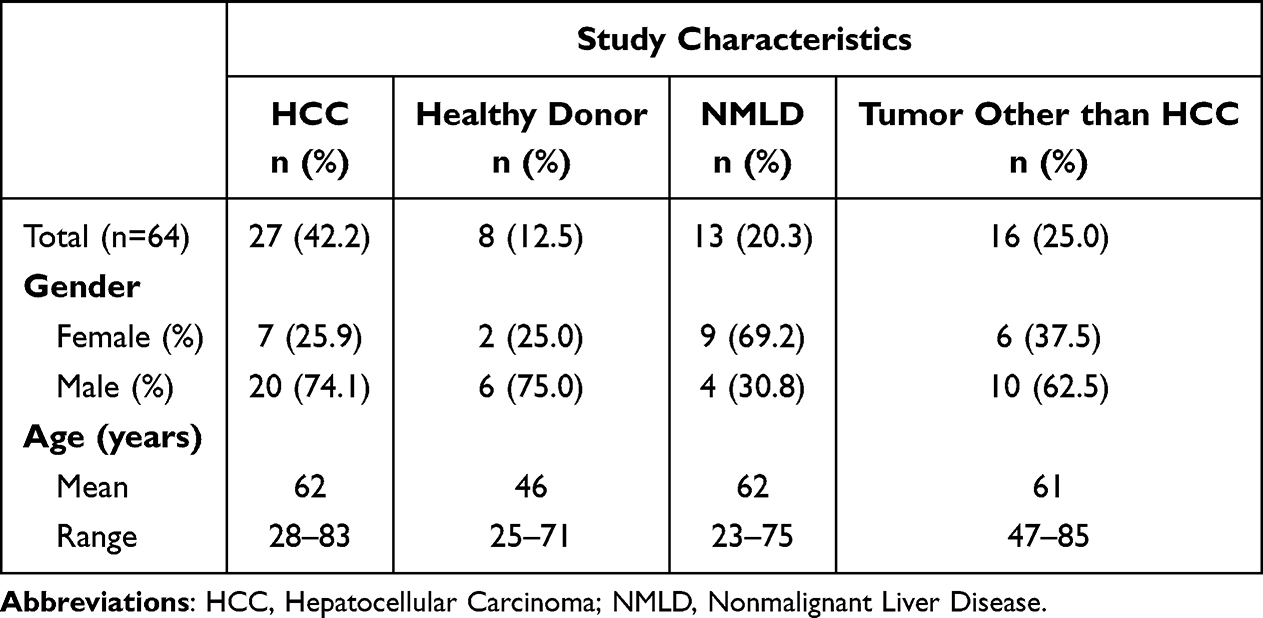 |
Table 2 Clinical Characteristics of the Study Cohort |
PD-L1+CSC Analysis and Dynamics
The detection and dynamics of PD-L1+CSCs in HCC provide intriguing insights into the pathogenesis and prognosis of this disease. Our pilot study revealed a notable prevalence of PD-L1+CSCs among HCC patients, with varying detection rates observed across different time points. Before surgery, PD-L1+CSCs were detected in 29.7% of the HCC patients (n=8/27), with a mean count of 0.27 ± 0.34/mL. One day after tumor resection, the detection rate decreased to 22.3% (n=6/27), with a mean count of 0.57 ± 0.55/mL. However, six months after tumor resection, the detection rate increased significantly to 85% (n=17/20, p<0.01), with a mean count of 1.88 ± 1.83/mL. Twelve months after resection, the detection rate remained high at 88% (n=15/17, p<0.01), with a mean count of 0.9 ± 0.71/mL (Figure 4A). Among the 27 HCC patients, 51.8% (n=14) experienced recurrence after a median follow-up period of nearly 48 months.
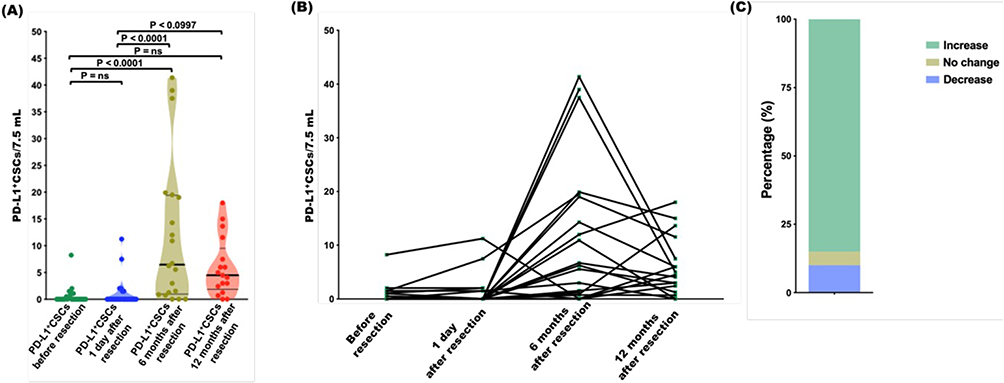 |
Figure 4 Enumeration and longitudinal monitoring of PD-L1+CSC. (A) Frequency distributions of PD-L1+CSC counts before resection and one day, six months and twelve months after resection. (B) Ladder plots displaying PD-L1+CSC counts for each HCC patient before resection and at 1 day, 6 months and 12 months after resection. (C) Percentages of patients who had incidence of increase, no change or decrease in PD-L1+CSC counts at 6 months after resection relative to the PD-L1+CSC counts from the same HCC patient at 1 day after resection. |
Long-Term Dynamics of PD-L1+CSCs
The results of the follow-up examinations revealed that the number of PD-L1+CSCs increased significantly. The mean PD-L1+CSC count before resection was 0.2 PD-L1+CSC/7.5 mL of blood. In comparison, one day after tumor resection, the mean value was 4.3 PD-L1+CSC/7.5 mL, and at 6 months after tumor resection, it was significantly greater at 14 PD-L1+CSC/7.5 mL (p=0.005). Twelve months after tumor resection, the PD-L1+CSC count also remained high, at 6.8 PD-L1+CSC/7.5 mL (Figure 4B). Accordingly, HCC patients presented higher levels of PD-L1+CSCs/7.5 mL 6 and 12 months after resection than before or 1 day after resection. This finding indicates a potential association between surgical intervention and the release of tumor cells into the circulation, contributing to increased levels of PD-L1+CSCs postoperatively. In addition, Figure 4C illustrates the distribution of patients based on the change in PD-L1+CSC counts observed six months after resection, relative to their baseline counts measured one day post-resection. Specifically, the figure shows the percentages of patients who experienced an increase, no change, or decrease in PD-L1+CSC counts over this period. These results highlight the heterogeneity in PD-L1+CSC dynamics among HCC patients following surgical intervention.
Associations with Overall Survival and Recurrence-Free Survival
Patients with positive PD-L1+CSC counts before surgery tended to have significantly shorter OS (p=0.05) and lower RFS (p=0.07) than patients with no detected PD-L1+CSCs (Figure 5A and B). HCC patients presented higher levels of PD-L1+CSCs/7.5 mL at 6 and 12 months after resection than before surgery or at 1 day after surgery. Additionally, HCC patients with a tumor size > 5 cm tended to have a shorter OS (p=0.06) but did not have statistically significant differences in RFS rates (p=0.79) (Figure 5C and D).
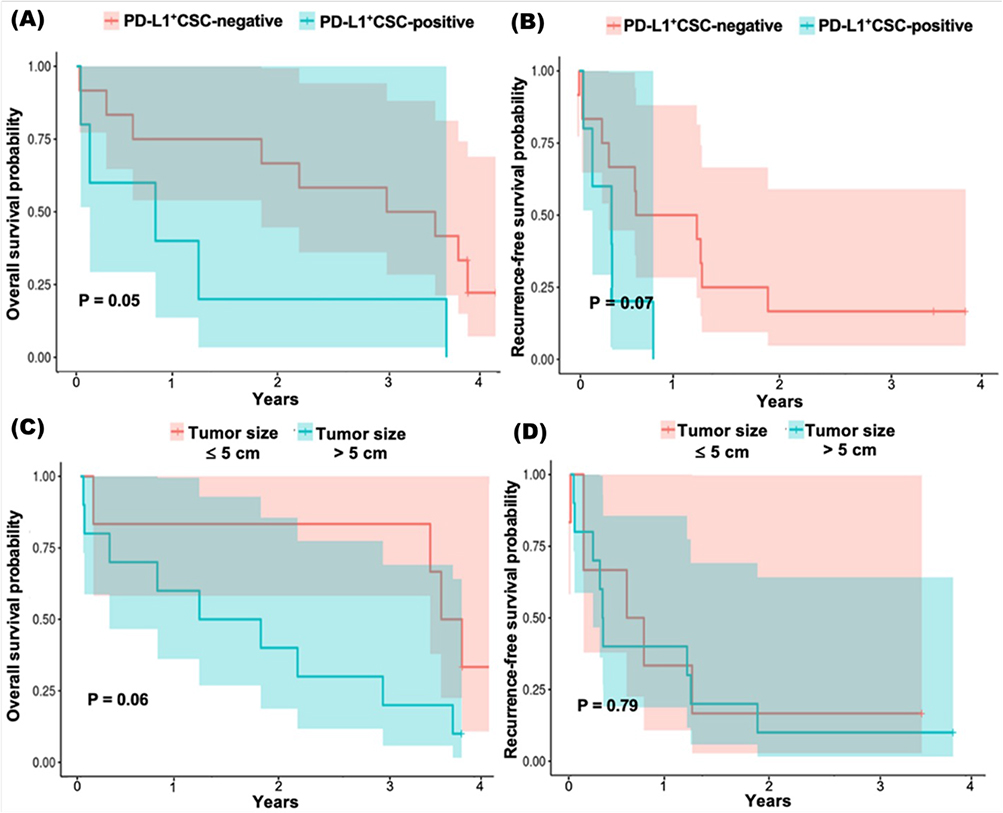 |
Figure 5 Comparison of (A) overall survival and (B) recurrence-free survival between the PD-L1+CSC-positive group and the PD-L1+CSC-negative group in patients with HCC before resection. Comparison of (C) overall survival and (D) recurrence-free survival in patients with a tumor size > 5 cm vs ≤ 5 cm. |
Moreover, patients who underwent open surgery (n=23) experienced higher levels of CSCs/mL at 6 and 12 months after resection than did those who underwent laparoscopic surgery (n=4, p=0.06), although this difference was not statistically significant (data not shown in the figure). This highlights the potential impact of surgical procedures on the release and dissemination of tumor cells, particularly in the context of disease progression.
Discussion
Baseline and longitudinal monitoring are crucial for understanding the risk of recurrence in patients with resected HCC, particularly through the analysis of PD-L1+CSCs in peripheral blood. Our study indicates that these CSCs, which exhibit invasive and metastatic properties, can serve as valuable prognostic markers. Furthermore, other studies have confirmed that PD-L1 expression on CSCs in breast and lung cancer may induce immune evasion40,41 and promote metastasis.41,42
By assessing the presence of circulating PD-L1+CSCs before surgery, we can establish a baseline that helps identify patients who are more likely to experience poorer outcomes. In alignment with the findings of other research groups, the detection of PD-L1+CSCs may indicate rapid disease progression and poor prognosis.42 This baseline provides a crucial point of comparison for evaluating the impact of surgical interventions and initial tumor dynamics. Notably, the absence of a direct relationship between tumor size and PD-L1+CSC levels suggests that traditional metrics may not fully capture the complexities of HCC prognosis, highlighting the need for a broader range of biomarkers. Traditionally, patients with tumors adhering to the Milan criteria (ie, a single tumor with a diameter of ≤5 cm or up to 3 tumors each with a diameter of ≤3 cm, no extrahepatic metastases, and no major vessel involvement) have significantly better survival rates after liver transplantation.43
Through longitudinal monitoring, we observed significant shifts in PD-L1+CSC levels post-surgery, offering insights into their potential role in disease recurrence. The immediate reduction in PD-L1+CSC counts after resection suggests an initial positive response to surgery. An increase in these cells over time suggests that the tumor microenvironment supports CSC survival and may contribute to recurrence, which means surgical resection cannot eliminate all tumor spread. This aligns with the concept of minimal residual disease (MRD), where residual cancer cells remain after treatment and may cause relapse.44,45 This is a significant concern because up to 70% of HCC patients experience recurrence within five years following treatment.46 CTC levels measured before surgery indicate tumor burden, but their prognostic value changes after resection; postoperative persistence or rebound of CTCs serves as a real-time biomarker for MRD. Observing a decrease in CTCs after resection, followed by an increase in relapsing patients, provides an ideal pattern for monitoring recurrence.47
Interestingly, the reduction in PD-L1+CSC levels observed at 12 months compared to 6 months may reflect an adaptive immune response post-surgery. Alternatively, the initial rise in CSCs following resection could stabilize as patients recover. Additionally, the observed decline in PD-L1+CSC counts at 12 months may be attributed to multiple biological mechanisms, including immune system activity or cellular dormancy. The immune response following surgical resection could contribute to a delayed reduction in CSCs, as the immune system gradually recognizes and eliminates residual cancer cells. These observations underscore the need for further investigation through more frequent sampling to better characterize the dynamic fluctuations of PD-L1+CSC populations over time, while dedicated in vitro and in vivo functional studies will further demonstrate the molecular pathways driving these clinical findings. There is rapidly increasing evidence that cancers are composed of heterogeneous populations of cancer cells.48 These findings suggest that PDL1+CSCs are more aggressive and have invasive and metastatic capacity.49–51 Most of these cells exhibit CSC phenotypes characterized by nonproliferation and resistance to chemotherapy.24,30,31,50,51
This study is the first to demonstrate a clinical association between PD-L1+CSCs and oncological outcomes in HCC. Changes in PD-L1+CSC levels before and after surgery support their prognostic relevance. Preoperative PD-L1+CSC positivity was associated with reduced OS and shorter RFS, suggesting a more aggressive, immune-evasive tumor phenotype. Elevated levels may reflect residual microscopic disease and increased recurrence risk despite curative resection. PD-L1+CSCs were detected preoperatively in approximately one-third of patients and were associated with early recurrence and reduced survival. Frequencies increased to 85% and 88% at 6 and 12 months after surgery, correlating with recurrence in over half of the cohort. These observations suggest that PD-L1+CSCs may contribute to immune escape, metastatic progression, and resistance to standard therapies and support the utility of CSC monitoring as a valuable non-invasive biomarker for risk stratification and treatment planning in HCC patients, with biological aggressiveness reflected by CSC dissemination appearing to supersede tumor volume in predicting post-surgical outcomes. This observation suggests that monitoring CSCs could be helpful for the early identification of relapse, making it possible to adjust treatment promptly. It also implies that even after therapy, some cancer cells may remain in the body and seed micrometastases potentially leading to a later recurrence. Integrating CSC analysis into routine follow-up care might help healthcare professionals better assess the risk of relapse and tailor subsequent therapies more precisely, particularly for patients who are at higher risk of the disease returning.
To increase the robustness of our data despite the limited cohort size, we analyzed 108 samples from four time points per patient. Flow cytometry enabled assessment of PD-L1 expression in rare cell populations and of CSC–immune system interactions. Although some p-values were near statistical significance, consistent trends in OS and RFS suggest a biological role of PD-L1+CSCs in HCC progression. This study’s limitations include small sample size and follow-up period. The high postoperative CSC positivity rate likely results from our sensitive flow cytometry method, the inclusion of many advanced-stage patients, and attrition bias at later time points favoring high-risk individuals. Control analyses with healthy participants support assay specificity, indicating biological relevance. A deeper molecular characterization of CSCs would have offered further insight into tumor behavior and CSC dynamics. Our main analysis focused on the immediate postoperative period due to its more complete dataset; other time points suffered from missing data and reduced power. These factors limit the strength of our conclusions, but our results still highlight the prognostic value of CSCs in resected HCC patients. Additional samples are currently being collected as part of an ongoing, larger adequately powered study aimed at validating and extending these observations, enabling robust multivariable and time-dependent biomarker analyses. Larger multicenter studies are recommended to explore variable interactions and their influence on recurrence and CSC dynamics.
Conclusion
Persistent or rising PD-L1+CSC levels in patients with recurrence may support the consideration of targeted immune therapies. ICIs could be beneficial in selected cases, though recurrence in PD-L1−CSC-negative patients indicates additional mechanisms are likely involved. These findings suggest a need to better characterize the regulatory mechanisms of PD-L1 expression in CSCs and their interaction with the tumor microenvironment. Larger studies are required to validate these results and define the clinical utility of PD-L1+CSC monitoring. In summary, PD-L1+CSCs can be reliably detected across treatment stages and are associated with recurrence and survival outcomes. Their detection may assist in risk stratification and therapeutic decision-making in HCC.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of the University of Frankfurt (approval number: 312/16). Informed consent forms were signed by all the patients. Informed consent forms were signed and obtained by all the patients. This article does not contain any studies with animal subjects. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2024.
Acknowledgments
This research was conducted with the joint efforts of two senior authors, Markus S. Zimmermann and Mazen A. Juratli who contributed equally to the study. Dhruvajyoti Roy and Elsie Oppermann are co-first authors for this study. We thank Annette Trzmiel and Stefan Stein from the Flow Cytometry Unit, Georg-Speyer-Haus, Frankfurt for performing the FACS-Analyzes. We thank Michel Kostantin, Roxana Chaichun, Natascha Kohl and Darius Zokai for helping with data curation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Rudolf Geißendoerfer-Stiftung in the form of a grant awarded to MAJ (2015); Frankfurter Forschungsfoerderung in the form of a grant awarded to MAJ [FFF 2017]; and B. Braun-Stiftung in the form of a grant awarded to MAJ (2018).
Disclosure
Dr Christian Rolfo reports Advisory Board/ Speaker: AstraZeneca, Daiichi Sankyo, Regeneron and Novocure; Bristol-Myers Squibb (BMS), Novartis, Guardant Health,COR2ED, Bayer, Boehringer Ingelheim, Abbvie, Invitae, Janssen, EMD Serono, OneCell Dx, Neogenomics, Touch Oncology, Pfizer; Research Grant: Astra Zeneca, Thermo Fisher, Oncohost, Lung Cancer Research Foundation, National Foundation for Cancer Research, and U54 (National Institute of Health); Research collaboration: GuardantHealth, Foundation Medicine, Roche Diagnostics, EMD Serono, Janssen Pharmaceutical (LUNGMAP S1900J trial); Scientific advisory board member of Imagene AI; Leadership roles: International Society of Liquid Biopsy, The European School of Oncology, International Association for Study of Lung Cancer, and Oncology Latin American Association; Editor role: Editor in chief of CROH and Honorary editor at Journal of Liquid Biopsy Elsevier; Editorial board: Lung Cancer and ILCN (IASLC). The authors report no other conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–15. doi:10.3322/caac.21660
2. Dimitroulis D, Damaskos C, Valsami S, et al. From diagnosis to treatment of hepatocellular carcinoma: an epidemic problem for both developed and developing world. World J Gastroenterol. 2017;23(29):5282. doi:10.3748/wjg.v23.i29.5282
3. El-Serag HB. Epidemiology of hepatocellular carcinoma in USA. Hepatol Res. 2007;37(s2):S88–S94. doi:10.1111/j.1872-034X.2007.00168.x
4. Khalaf N, Ying J, Mittal S, et al. Natural history of untreated hepatocellular carcinoma in a US cohort and the role of cancer surveillance. Clin Gastroenterol Hepatol. 2017;15(2):273–281.e1. doi:10.1016/j.cgh.2016.07.033
5. Gomaa AI, Khan SA, Toledano MB, Waked I, Taylor-Robinson SD. Hepatocellular carcinoma: epidemiology, risk factors and pathogenesis. World J Gastroenterol. 2008;14(27):4300–4308. doi:10.3748/wjg.14.4300
6. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
7. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
8. Galle PR, Foerster F, Kudo M, et al. Biology and significance of alpha‐fetoprotein in hepatocellular carcinoma. Liver Int. 2019;39(12):2214–2229. doi:10.1111/liv.14223
9. Bruix J, Sherman M. Management of hepatocellular carcinoma: an updateδσ. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
10. Xu W, Liao S, Hu Y, Huang Y, Zhou J. Upregulation of miR-3130-5p enhances hepatocellular carcinoma growth by suppressing ferredoxin 1: miR-3130-5p enhances HCC growth via inhibiting FDX1. Curr Mol Pharmacol. 2024;17:e18761429358008. doi:10.2174/0118761429358008250305070518
11. Mu R, Chang M, Feng C, et al. Analysis of the expression of PRDX6 in patients with hepatocellular carcinoma and its effect on the phenotype of hepatocellular carcinoma cells. Curr Genom. 2024;25(1):2–11. doi:10.2174/0113892029273682240111052317
12. Villanueva A, Longo DL. Hepatocellular carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
13. Li Q, Han J, Yang Y, Chen Y. PD-1/PD-L1 checkpoint inhibitors in advanced hepatocellular carcinoma immunotherapy. Review. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.1070961
14. Xia L, Liu Y, Wang Y. PD‐1/PD‐L1 blockade therapy in advanced non‐small‐cell lung cancer: current status and future directions. oncologist. 2019;24(s1):S31–S41. doi:10.1634/theoncologist.2019-IO-S1-s05
15. Yi M, Zheng X, Niu M, Zhu S, Ge H, Wu K. Combination strategies with PD-1/PD-L1 blockade: current advances and future directions. Mol Cancer. 2022;21(1):28. doi:10.1186/s12943-021-01489-2
16. Aguiar PN Jr, De Mello RA, Barreto C, et al. Immune checkpoint inhibitors for advanced non-small cell lung cancer: emerging sequencing for new treatment targets. ESMO Open. 2017;2(3):e000200. doi:10.1136/esmoopen-2017-000200
17. Sensi B, Angelico R, Toti L, et al. Mechanism, potential, and concerns of immunotherapy for hepatocellular carcinoma and liver transplantation. Curr Mol Pharmacol. 2024;17:e18761429310703. doi:10.2174/0118761429310703240823045808
18. Aramini B, Masciale V, Arienti C, et al. Cancer Stem Cells (CSCs), Circulating Tumor Cells (CTCs) and their interplay with Cancer Associated Fibroblasts (CAFs): a new world of targets and treatments. Cancers. 2022;14(10):2408. doi:10.3390/cancers14102408
19. Lin D, Shen L, Luo M, et al. Circulating tumor cells: biology and clinical significance. Signal Transd Target Ther. 2021;6(1):404. doi:10.1038/s41392-021-00817-8
20. Liu J, Lian J, Chen Y, et al. Circulating Tumor Cells (CTCs): a unique model of cancer metastases and non-invasive biomarkers of therapeutic response. mini review. Front Genetics. 2021;12. doi:10.3389/fgene.2021.734595
21. Earl J, Garcia-Nieto S, Martinez-Avila JC, et al. Circulating tumor cells (CTC) and KRAS mutant circulating free DNA (cfDNA) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer. 2015;15(1):797. doi:10.1186/s12885-015-1779-7
22. Poruk KE, Blackford AL, Weiss MJ, et al. Circulating tumor cells expressing markers of tumor-initiating cells predict poor survival and cancer recurrence in patients with pancreatic ductal adenocarcinoma. Clin Cancer Res. 2017;23(11):2681–2690. doi:10.1158/1078-0432.Ccr-16-1467
23. Yang M-H, Imrali A, Heeschen C. Circulating cancer stem cells: the importance to select. Chin J Cancer Res. 2015;27(5):437. doi:10.3978/j.issn.1000-9604.2015.04.08
24. Papadaki MA, Stoupis G, Theodoropoulos PA, Mavroudis D, Georgoulias V, Agelaki S. Circulating tumor cells with stemness and epithelial-to-mesenchymal transition features are chemoresistant and predictive of poor outcome in metastatic breast cancer. Mol Cancer Ther. 2019;18(2):437–447. doi:10.1158/1535-7163.Mct-18-0584
25. Obermayr E, Koppensteiner N, Heinzl N, et al. Cancer stem cell-like circulating tumor cells are prognostic in non-small cell lung cancer. J Person Med. 2021;11(11):1225. doi:10.3390/jpm11111225
26. Schulte L-A, López-Gil JC, Sainz B, Hermann PC. The cancer stem cell in hepatocellular carcinoma. Cancers. 2020;12(3):684. doi:10.3390/cancers12030684
27. Valle S, Martin-Hijano L, Alcalá S, Alonso-Nocelo M, Sainz Jr B. The ever-evolving concept of the cancer stem cell in pancreatic cancer. Cancers. 2018;10(2):33. doi:10.3390/cancers10020033
28. Watanabe T, Okumura T, Hirano K, et al. Circulating tumor cells expressing cancer stem cell marker CD44 as a diagnostic biomarker in patients with gastric cancer. Oncol Lett. 2017;13(1):281–288. doi:10.3892/ol.2016.5432
29. Li M, Zhang B, Zhang Z, et al. Stem cell-like circulating tumor cells indicate poor prognosis in gastric cancer. Biomed Res Int. 2014;2014:981261. doi:10.1155/2014/981261
30. Barrière G, Riouallon A, Renaudie J, Tartary M, Rigaud M. Mesenchymal and stemness circulating tumor cells in early breast cancer diagnosis. BMC Cancer. 2012;12(1):114. doi:10.1186/1471-2407-12-114
31. Theodoropoulos PA, Polioudaki H, Agelaki S, et al. Circulating tumor cells with a putative stem cell phenotype in peripheral blood of patients with breast cancer. Cancer Lett. 2010;288(1):99–106. doi:10.1016/j.canlet.2009.06.027
32. Iinuma H, Watanabe T, Mimori K, et al. Clinical significance of circulating tumor cells, including cancer stem-like cells, in peripheral blood for recurrence and prognosis in patients with Dukes’ stage B and C colorectal cancer. J Clin Oncol. 2011;29(12):1547–1555. doi:10.1200/jco.2010.30.5151
33. Grillet F, Bayet E, Villeronce O, et al. Circulating tumour cells from patients with colorectal cancer have cancer stem cell hallmarks in ex vivoculture. Gut. 2017;66(10):1802–1810. doi:10.1136/gutjnl-2016-311447
34. Fan ST, Yang ZF, Ho DWY, Ng MNP, Yu WC, Wong J. Prediction of posthepatectomy recurrence of hepatocellular carcinoma by circulating cancer stem cells: a prospective study. Ann Surg. 2011;254(4):569–576. doi:10.1097/SLA.0b013e3182300a1d
35. Vogl TJ, Riegelbauer LJ, Oppermann E, et al. Early dynamic changes in circulating tumor cells and prognostic relevance following interventional radiological treatments in patients with hepatocellular carcinoma. PLoS One. 2021;16(2):e0246527. doi:10.1371/journal.pone.0246527
36. Herrero A, Toubert C, Bedoya JU, et al. Management of hepatocellular carcinoma recurrence after liver surgery and thermal ablations: state of the art and future perspectives. Hepatob Surg Nutr. 2024;13(1):71–88. doi:10.21037/hbsn-22-579
37. Shah SA, Greig PD, Gallinger S, et al. Factors associated with early recurrence after resection for hepatocellular carcinoma and outcomes. J Am Coll Surg. 2006;202(2):275–283. doi:10.1016/j.jamcollsurg.2005.10.005
38. Toubert C, Guiu B, Al Taweel B, et al. Prolonged survival after recurrence in HCC resected patients using repeated curative therapies: never give up! Cancers. 2022;15(1):232. doi:10.3390/cancers15010232
39. Xing H, Zhang W-G, Cescon M, et al. Defining and predicting early recurrence after liver resection of hepatocellular carcinoma: a multi-institutional study. Hpb. 2020;22(5):677–689. doi:10.1016/j.hpb.2019.09.006
40. Di Nicola MA, Castagnoli L, Cancila V, et al. Role of PD-L1 expression in triple-negative breast cancer stem cells. J Clin Oncol. 2018;36(15_suppl):12081. doi:10.1200/JCO.2018.36.15_suppl.12081
41. Zhang J, Liu B, Lyu M, Duan Y. Cutting the root: the next generation of T cells engagers against cancer stem cells to overcome drug resistance in triple-negative breast cancer. Cancer Biol Med. 2023;20(3):169–173. doi:10.20892/j.issn.2095-3941.2022.0745
42. Raniszewska A, Vroman H, Dumoulin D, Cornelissen R, Aerts JGJV, Domagała-Kulawik J. PD-L1+ lung cancer stem cells modify the metastatic lymph-node immunomicroenvironment in nsclc patients. Cancer Immunol Immunother. 2021;70(2):453–461. doi:10.1007/s00262-020-02648-y
43. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–700. doi:10.1056/NEJM199603143341104
44. Berardi G, Guglielmo N, Mariano G, Ettorre GM. Surgical margins for hepatocellular carcinoma. In: Hepatocellular Carcinoma. Springer International Publishing Cham; 2022:113–120.
45. Sun Y-F, Yang X-R, Zhou J, Qiu S-J, Fan J, Xu Y. Circulating tumor cells: advances in detection methods, biological issues, and clinical relevance. J Cancer Res Clin Oncol. 2011;137(8):1151–1173. doi:10.1007/s00432-011-0988-y
46. Nevola R, Ruocco R, Criscuolo L, et al. Predictors of early and late hepatocellular carcinoma recurrence. World J Gastroenterol. 2023;29(8):1243. doi:10.3748/wjg.v29.i8.1243
47. Wu CY, Lee CL, Wu CF, et al. Circulating tumor cells as a tool of minimal residual disease can predict lung cancer recurrence: a longitudinal, prospective trial. Diagnostics. 2020;10(3):144. doi:10.3390/diagnostics10030144
48. Hausser J, Alon U. Tumour heterogeneity and the evolutionary trade-offs of cancer. Nat Rev Cancer. 2020;20(4):247–257. doi:10.1038/s41568-020-0241-6
49. Agnoletto C, Corrà F, Minotti L, et al. Heterogeneity in circulating tumor cells: the relevance of the stem-cell subset. Cancers. 2019;11(4):483. doi:10.3390/cancers11040483
50. Baccelli I, Schneeweiss A, Riethdorf S, et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat Biotechnol. 2013;31(6):539–544. doi:10.1038/nbt.2576
51. Yu M, Bardia A, Wittner BS, et al. Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science. 2013;339(6119):580–584. doi:10.1126/science.1228522
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.