")
Back to Journals » Clinical Interventions in Aging » Volume 17
The Predictive Value of the “Identification of Seniors at Risk” Score on Mortality, Length of Stay, Mobility and the Destination of Discharge of Geriatric Hip Fracture Patients
Authors Knauf T, Buecking B, Geiger L, Hack J, Schwenzfeur R, Knobe M, Eschbach D, Ruchholtz S, Aigner R
Received 10 December 2021
Accepted for publication 10 March 2022
Published 31 March 2022 Volume 2022:17 Pages 309—316
DOI https://doi.org/10.2147/CIA.S344689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Tom Knauf,1 Benjamin Buecking,2 Lukas Geiger,1 Juliana Hack,1 Ruth Schwenzfeur,3 Matthias Knobe,4 Daphne Eschbach,1 Steffen Ruchholtz,1 Rene Aigner1 On behalf of the Registry for Geriatric Trauma DGU
1Center for Orthopaedics and Trauma Surgery, University Hospital Giessen and Marburg, Marburg, Germany; 2Department for Trauma Surgery, Klinikum Hochsauerland, Arnsberg, Germany; 3Working Committee on Geriatric Trauma Registry of the German Trauma Society (DGU), München, Germany; 4Department of Orthopaedic and Trauma Surgery, Cantonal Hospital Lucerne, Lucerne, Switzerland
Correspondence: Tom Knauf, Tel +49-6421-58-63174, Fax +49-6421-58-66721, Email [email protected]
Purpose: The German Society for Geriatrics recommends the “ISAR” questionnaire as a screening tool for patients ≥ 70 for geriatric screening in emergency rooms. Although the ISAR-score is collected routinely in the “AltersTraumaRegister DGU®” (ATR-DGU), to date less is known about the predictive value of the “ISAR”-score in geriatric trauma patients.
Patients and Methods: Currently, 84 clinics participate in the ATR-DGU. This evaluation is limited to the subgroup of proximal femur fractures from 2016– 2018. Patients ≥ 70 years, who underwent surgery for a hip fracture are included in the ATR-DGU. In this evaluation, the influence of the “ISAR”-score on mortality, length of stay, mobility and the destination of discharge was examined.
Results: Overall 10,098 patients were included in the present study. The median age was 85 years (interquartile range (IQ) 80– 89 years). According to the ISAR-score 80.6% (n=8142) of the patients were classified as geriatric patients (cut off “ISAR”-score ≥ 2 points). These group of patients had a length of stay of 16 days (IQ10.1– 22.1) compared to the non-geriatric patient cohort showing a length of stay of 15 days (IQ10.1– 20.1). Patients showing an ISAR-score ≥ 2 had an increased risk of being discharged to a nursing home (OR 8.25), not being able to walk (OR 12.52) and higher risk of mortality (OR 3.45).
Conclusion: The “ISAR”-score shows predictive power for the length of stay, mobility, hospital mortality and discharge after hospital in the collective of geriatric trauma patients. It therefore seems suitable as a screening tool for geriatric trauma patients in the emergency department and should be considered in this context.
Keywords: ISAR-score, hip fracture, geriatric patient, identification of seniors at risk
Introduction
Due to demographic change, the population is getting older and the number of geriatric patients is increasing accordingly. To improve the inpatient treatment of geriatric trauma patients the German Trauma Society (“Deutsche Gesellschaft fuer Unfallchirurgie”, DGU) founded the “Registry for Geriatric Trauma” (AltersTraumaRegister DGU®, ATR-DGU) in 2016. The multidisciplinary orthogeriatric treatment improves patients’ outcome while reducing the perioperative complications.1 An important element in the treatment of those patients is the identification of the “geriatric patient”.2 Therefore, clinical decision algorithms are necessary in order to attempt to formally test, simplify, and increase accuracy of clinicans’ diagnostic and prognostic assessments.3,4 The “Identification of Seniors at risk”-score (ISAR-score) has been established in screening for geriatric patients in clinical routine nowadays.5 In their systematic literature search Galvin et al attest the score only a moderate predictive power.6 Nevertheless, there are studies showing limitations of the ISAR-score and even discuss its usefulness in identifying high-risk patients.7,8 So far, the ISAR-Score has usually been tested in geriatric patients in general. Only few studies focused on geriatric trauma patients.9,10 Still, the ISAR-Score is part of the questionnaire collected from patients at admission in connection with the “Registry for Geriatric Trauma”. Gronewold et al examined the ISAR-Score in combination with a comprehensive geriatric assessment in geriatric trauma patients. They showed that an ISAR-Score ≥ 2 along with a positive geriatric assessment lead to a longer hospital stay, more nursing and physiotherapy hours, as well as higher risk of falling. To the best of our knowledge there is no study that has investigated whether the ISAR-Score is useful to predict clinical course in geriatric trauma patients with regard to mortality and mobility.
Identification of geriatric patients is necessary in order to provide a specialized and interdisciplinary treatment for these frail patients. Since a geriatric patient is not defined on the basis of age alone, a screening tool is needed for the identification of frail elder patients that are in need of further treatment. Therefore, we analyzed the data of the “Registry for Geriatric Trauma” to investigate the predictive value of the ISAR score in geriatric trauma patients in terms of mortality, mobility, lengths of hospital stay and place of discharge.
Materials and Methods
The “Registry for Geriatric Trauma” (AltersTraumaRegister DGU®) was founded by the German Trauma Society in 2016. The ATR-DGU ensures pseudonymized and standardized documentation of data on the situation before accident, diagnosis, treatment and outcome in geriatric patients with a proximal femur fracture. Inclusion criteria are patients ≥70 years old who have undergone surgery for a hip fracture. Periprosthetic or peri-implant fractures were excluded. Our analysis used the following data from patients included between 2016 and 2018: age, gender, “American Society of Anesthesiologists” (ASA) – Score,11 Identification of seniors at risk (ISAR) – Score12 (at the time of admission to the hospital), residential status, classification of fracture, time to surgery, length of hospital stay, walking ability on the 7th day after surgery, destination of discharge after hospitalization and in-hospital mortality. The ISAR score has a range of 0–6 points. Patients with a high risk can reach a maximum of 6 points. The 6 questions include topics such as the need for assistance, hospitalizations in the last 6 months, vision or memory problems, and the number of medications. In line with previous literature patients were considered as geriatric patients with an ISAR score ≥ 2. The ISAR score was collected by either the admitting physician or a study nurse. Normally, the results are first recorded on paper and then transferred pseudonymized to the register.
The data was collected at admission, preoperatively, during surgery and one week after surgery at the moment of discharge/transfer and optionally 120 days postoperatively.
The infrastructure for documentation, data management and data analysis is provided by the AUC - Academy for Trauma Surgery (AUC). The scientific management is the responsibility of the Working Committee on Geriatric Trauma Registry DGU® of the DGU. Every certified “Center for Geriatric Trauma” (AltersTraumaZentrum DGU®) is obliged to participate in the ATR-DGU.
Data is submitted pseudonymized via web-based application into a central database. The approval of scientific evaluations from the ATR-DGU is based on a peer-review procedure according to the publication guidelines of the Working Committee on Geriatric Trauma Registry. At the moment of this study 84 hospitals from Germany and Switzerland are currently participating in the ATR-DGU. Each year about 6500 cases are included.
Statistical Analysis
All data were descriptively analysed by calculating frequencies, median and inter quartile ranges (IQR). Group differences between continuous data were examined by the Mann–Whitney U-test in two groups and by the Kruskal–Wallis test for more than two groups. In categorical data groups were compared by the Fisher’s exact test. The p-values from these tests should be interpreted with caution, as in large sample sizes even small differences can be significant. The correlation between the ISAR score and the length of stay were analysed by the Spearman correlation coefficient and graphically. Multinomial and binary logistic regression were performed and odds ratios with their corresponding 95% confidence intervals were calculated to examine the influence of the ISAR score on the walking ability on the 7th post-op day, discharge destination after hospital and mortality. All analyses were performed in R version 3.5.2.
Results
Baseline Characteristics
A total of 15,099 patients with proximal femoral fractures (femoral neck, pertrochanteric, subtrochanteric) were entered into the register between 2016 and 2018. The median age was 85 years (Interquartile range (IQR) 80–89 years). Most of the patients were females (71.9%, n=10,811). According to the ASA-Score 77.0% (n=11,473) had a least one severe systemic disease or worse (ASA≥3). Nevertheless, 74.2% of the patients were living in their homes and 52.3% (n=4625) had no classification into a nursing care level. The most common fractures documented were pertrochanteric fractures (49.9%; n=7537), followed by femoral neck fractures (45.8%; n=6908). As usual in analyzing registry data, not all information were available for each patient. Therefore, additional information on how many patients were available for each category can be found in Table 1.
 |
Table 1 Baseline Characteristics |
The ISAR-Score was collected in 10,098 of the 15,099 patients. The median ISAR-Score was 3 (IQR 2–4). According to the ISAR-Score 80.6% (n=8142) of documented registry patients were classified as geriatric.
Lengths of Stay
The median length of the survivors was 16.1 days (IQR 10.1–22.0 days). According to the ISAR-Score non-geriatric patients had a median length of stay of 15.0 days (IQR 10.1–20.1 days). Geriatric patients (ISAR-Score 2–6) had a median length of stay of 16.0 days (IQR 10.1–22.1) (p<0.001).
Walking Ability on the 7th Day
11.8% (n=1707) patients were not in need of walking aids or were just dependent on forearm crutches or a walking stick. 67.2% (n=9709) were mobile on a walker. 21.0% (n=3038) were not able to walk at all. Patients walking without walking aids at day 7 of hospitalization showed a significantly lower ISAR-Score p<0.001. Geriatric patients had a 3.69 higher risk to use a walker and a 12.52 higher risk not to walk instead of no need for walking aids or forearm crutches (Tables2 and 3).
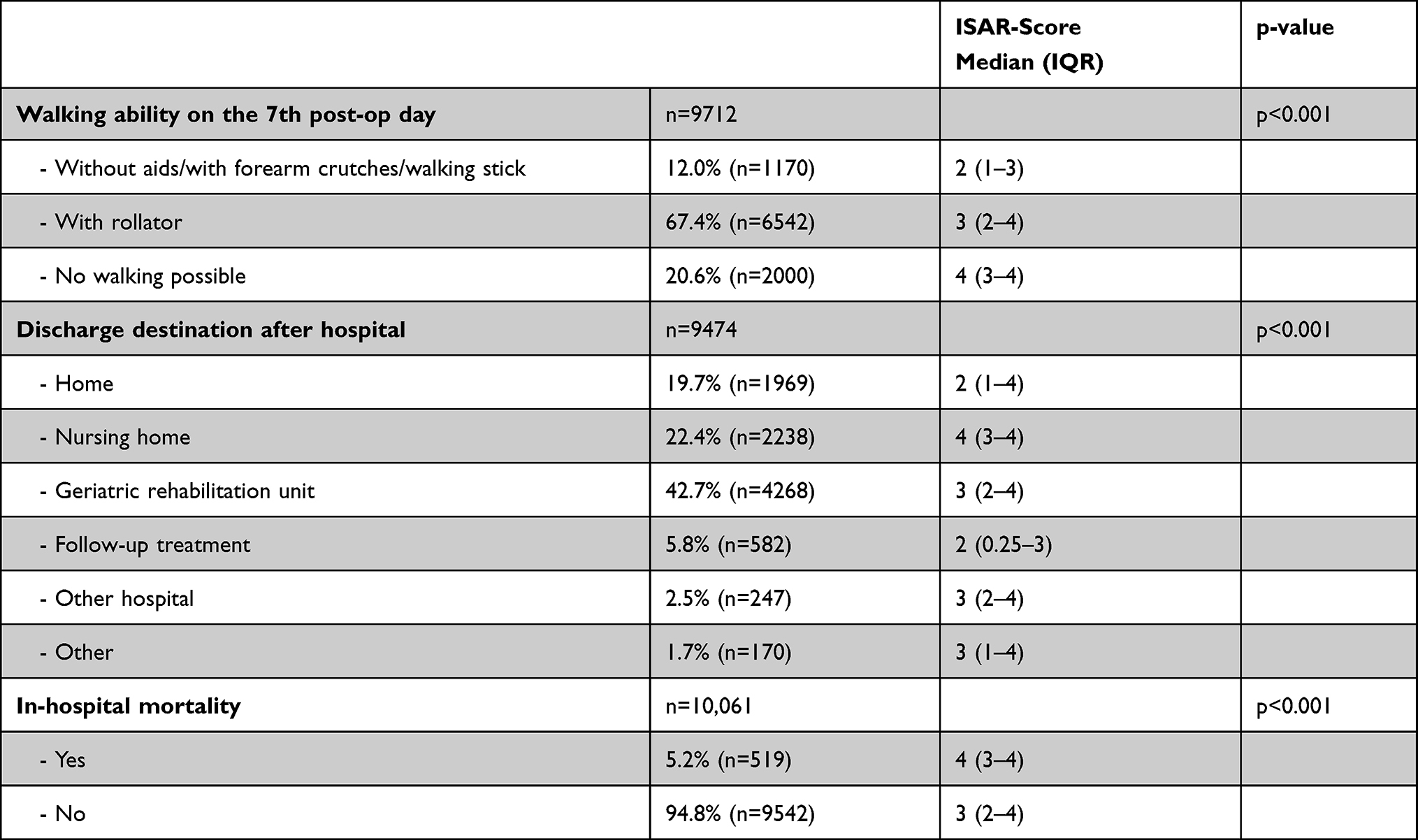 |
Table 2 Influence of the ISAR-Score During Initial Hospitalization |
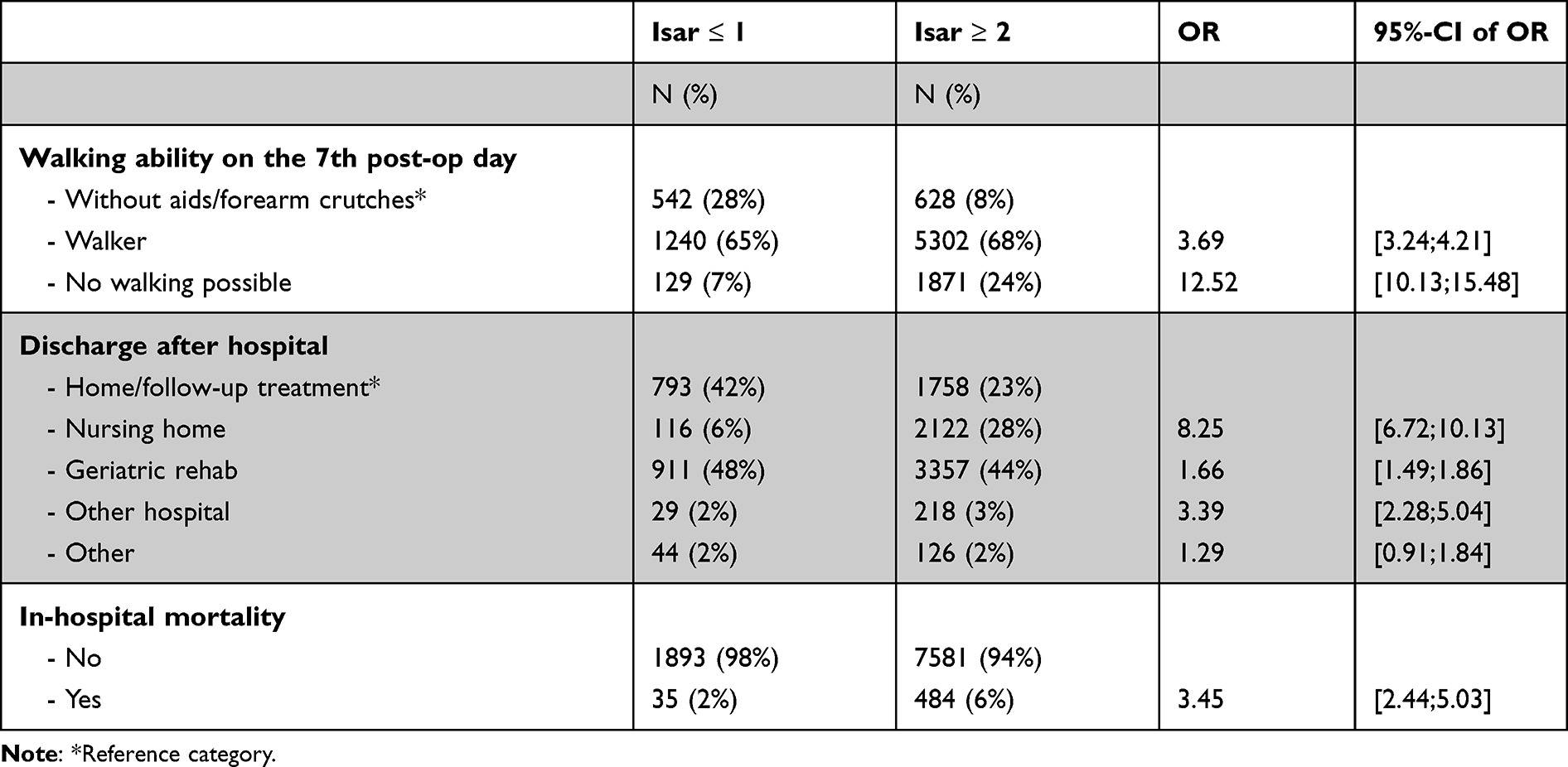 |
Table 3 Results from the Multinomial and Binary Logistic Regression to Examine the Influence of the ISAR-Score (≤1 vs ≥2) During Initial Hospitalization |
Discharge Destination After Hospital
19.7% (n=1969) patients were discharged to their homes after the hospital stay. 22.4% (n=2238) of the patients were discharged to a nursing home. The majority of the patients (42.7%; n=4268) was discharged towards a geriatric rehabilitation unit. Patients who were discharged home and to follow up rehabilitation ward had a median ISAR Score of 2 (home: IQR 1–4; rehabilitation ward: (IQR 0.25–3)). Those patients discharged towards a geriatric rehabilitation unit had a median ISAR-Score of 3 (IQR 2–4). If patients had to be discharged to a nursing home, they had a predominant ISAR-Score of 4 (IQR 3–4). Further, the risk for a discharge to a nursing home/geriatric rehabilitation or another hospital was also higher for geriatric patients (Tables 2 and 3).
Mortality
The mortality rate during inpatient treatment was 5.2% (n=519). The median ISAR-Score of died patients was 4 (IQR 3–4) compared to a median ISAR-Score of 3 (IQR 2–4) in patients who survived the in-hospitalization period (Table 2). Geriatric patients had a 3.45 higher risk to die during the inpatient treatment (Table 3).
Discussion
The aim of this study was to evaluate whether the ISAR-Score is suitable predicting in hospital mortality, lengths of stay, mobility and the place of discharge in geriatric hip fracture patients. According to the ISAR-Score 80.6% of the patients were at risk of adverse events (ISAR-Score ≥2). The median ISAR-Score was 3.
Many studies focused on the identification of predictors of the clinical course of geriatric hip fracture patients.13 Gronewold et al showed in their study similar results for such a cohort of geriatric trauma patients. 85.8% of their patients had a positive ISAR-Score.9 Most of the other studies analyzing the ISAR-Score tested geriatric patients in general, having no focus on geriatric trauma patients. In our opinion, however, this is a different collective. Geriatric patients without trauma usually reach the hospital because of the acute worsening of a chronic disease. Geriatric trauma patients also suffer from all these chronic pre-existing conditions, however a sudden fall event occurred from a usually compensated health condition. The above mentioned studies showed a range of positive ISAR-Scores between 61.2%-84%.14–16 The differences between the various ISAR-Scores are most likely due to the different study collectives. In this study 80.6% of the patients showed a positive ISAR-Score at admission. This seems to be quite a high number, but it is consistent with the ASA-Score, which was collected in the register as well. An ASA-Score ≥3 had 77% (n=11,473) of the patients, which indicates that patients suffer from a severe systemic disease. These different scores are all also indicators for the frailty of those patients.
Influence of the ISAR-Score on Lengths of Stay
Patients with an ISAR-Score of 0–1 points stayed 15 days at the hospital in contrast to patients with an ISAR-Score of 2–6 points who stayed 16 days at the hospital. Scharf et al showed similar results in internal medicine patients. They collected the ISAR-Score in 547 patients prospectively. In consistency to our study 2 points of the ISAR-Score represented the cutoff. In case of a positive ISAR-Score they added a comprehensive geriatric (CGA) assessment. They were able to show that patients having a positive ISAR-Score stayed longer at the hospital than patients with negative results.17 The same working group examined these characteristics in geriatric trauma and orthopedic patients. Here, a positive ISAR-Score alone did not show an increased length of stay compared to a negative ISAR-Score. Only in case of an abnormal CGA a longer hospital stay could be detected.9 Asomaning et al stated in their observational study a longer inpatient stay of patients with positive ISAR-Screening (cutoff ≥ 2) results.14 According to the literature further factors that prolonged in hospital stay were ASA-Score,18 delayed surgery19 and comorbidities.19 In our study only one day difference was detected between a positive and a negative ISAR-Score. Although the results present a significant p-value (p<0.001), this might be a trend, but probably it does not make any notable difference to the patient.
Influence of the ISAR-Score on Mobility
To the best of our knowledge no study focused on the predictivity of the ISAR-Score on mobility in geriatric hip fracture patients. Although, none of the six items of the Score focusses on mobility itself the score seems to predict the patient’s mobility on day 7 after hip fracture surgery. Patients with a positive ISAR-Score (≥ 2) had an increased risk of walking on a walker (Odds ratio (OR) 3.69) or being unable to walk (OR 12.52) compared to patients who were mobile with almost no walking aids. (Table 3) Factors that affect mobility after hip fracture in general are comorbidities20,21 (neurological and kidney-related diseases22), pre fracture hospitalization23 and disability in activities of daily living.21 Disability in activities of daily living are represented indirectly in the questions of the ISAR-Score by the first question “Need for assistance”. The other factors are not included in the ISAR-Score.
Based on our and other study results the ISAR the ISAR score thus has a predictive value with regard to postoperative mobility.
Influence of the ISAR-Score on Place of Discharge
Patients with a higher ISAR-Score had to be transferred on discharge to a facility that offered more nursing care. Patients with a positive ISAR-Score had an increased risk of being discharged to a nursing home (OR 8.25). (Table 3) After the hip fracture only slightly more patients lived in a nursing home (26.4% vs 24.0%). Gronewald et al showed that patients with a positive ISAR-Score and an abnormal CGA were transported to another hospital and a nursing home more often compared to a negative ISAR-Score. These results were not significant.9
The ISAR-Score seems to capture the patients’ need for care appropriately and acts as a predictor for the place of discharge.
Influence of the ISAR-Score on Mortality
Patients that died during hospitalization presented a higher ISAR-Score (deceased: 4 survivors 3). Patients with an ISAR-Score ≥2 had an increased risk of dying during inpatient treatment (OR 3.45). (Table 3) Similar results were shown by Di Bari et al in their cohort study examining the ISAR-Score (cutoff ≥ 2). ISAR-positive participants had an odds ratio of 5.23 (95% confidence interval 2.27–12.04) of dying.15 According to the literature certain comorbidities,22,24,25 male sex,24 time to surgery (> 2 days/< 2 days),25 advanced age,24 institutionalization,24,25 dementia24 and presence of vision disorders are linked with an increased mortality after hip fractures. Dementia and vision disorders are represented in the ISAR-Score as well.
The ISAR score shows predictive power for in-hospital mortality.
Strengths and Limitations of the Study
Limiting factors of this study are that not all items were collected from all patients. Unfortunately, this is common in registry data. Results become significant though they are only slightly different from each other and differences are not always relevant for patients. Instead of relying on p-values, the strength of relation between outcome and risk factor were therefore here examined by odds ratios. Nevertheless, strengths of this study are the high number of participants and the high congruence of surgical and inpatient treatment of these patients. This makes the present collective a very uniform one and reduces the multiple confounding factors that make the evaluation of such treatment data difficult. Patients from multiple centers all over Germany and Switzerland were included in this study.
Conclusion
We cannot change anything about the frailty of those patients, but we can improve the framework of the treatment to provide these patients the best possible therapy. They have to be treated with an increased level of care in a multidisciplinary setting to improve their outcomes. One element in this treatment is the earliest possible identification of patients at risk. For this purpose, we need reliable screening tools for identifying patients at risk. In the case of mobility, place of discharge and mortality the ISAR-Score seems to identify the frail patients reliably in a collective of geriatric trauma patients.
Ethics Statement
The protocol for the research project has been approved by the Ethics committee of Philipps University Marburg (Ethical Approval Code: AZ 46/16; date: 5 April 2018).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Knobe M, Böttcher B, Coburn M, et al. Geriatric Trauma Center DGU®: evaluation of clinical and economic parameters: a pilot study in a German university hospital. Unfallchirurg. 2019. doi:10.1007/s00113-018-0502-y
2. Thiem U, Greuel HW, Reingräber A, et al. Consensus for the identification of geriatric patients in the emergency care setting in Germany. Z Gerontol Geriatr. 2012. doi:10.1007/s00391-012-0342-2
3. McGinn TG, Guyatt GH, Wyer PC, Naylor CD, Stiell IG, Richardson WS. Users’ guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence-Based Medicine Working Group. JAMA. 2000;284:79. doi:10.1001/jama.284.1.79
4. Weinrebe W, Schiefer Y, Weckmüller K, et al. Does the identification of seniors at risk (ISAR) score effectively select geriatric patients on emergency admission? Aging Clin Exp Res. 2019;31(12):1839–1842. doi:10.1007/s40520-018-1105-8
5. Pinter G, Rudolf L, Schippinger W, Janig H, Kada O, Cernic K. Geriatrische Notfallversorgung - Strategien Und Konzepte” „ISAR Notaufnahme Screening. Springer Verlag; 2013.
6. Galvin R, Gilleit Y, Wallace E, et al. Editor’s Choice: adverse outcomes in older adults attending emergency departments: a systematic review and meta-analysis of the identification of Seniors at risk (ISAR) screening tool. Age Ageing. 2017. doi:10.1093/ageing/afw233
7. Rivero-Santana A, Del Pino-Sedeño T, Ramallo-Fariña Y, Vergara I, Serrano-Aguilar P. Usefulness of scoring risk for adverse outcomes in older patients with the identification of seniors at risk scale and the triage risk screening tool: a meta-analysis. Emergencias. 2017;29:49–60.
8. Yao JL, Fang J, Lou QQ, Anderson RM. A systematic review of the identification of seniors at risk (ISAR) tool for the prediction of adverse outcome in elderly patients seen in the emergency department. Int J Clin Exp Med. 2015;8:4778.
9. Gronewold J, Dahlmann C, Jäger M, Hermann DM. Identification of hospitalized elderly patients at risk for adverse in-hospital outcomes in a university orthopedics and trauma surgery environment. PLoS One. 2017;12:e0187801. doi:10.1371/journal.pone.0187801
10. Gurlit S, Möllmann H. Preoperative risk identification using the Identification of Seniors at Risk?: Suitability as sole screening tool for inpatient aged risk patients. Z Gerontol Geriatr. 2018;51(4):388–393. doi:10.1007/s00391-018-1401-0
11. ASo, Anesthesiologists. ASA physical status classification system. ASA House of Delegates; 2014.
12. McCusker J, Bellavance F, Cardin S, Trépanier S, Verdon J, Ardman O. Detection of older people at increased risk of adverse health outcomes after an emergency visit: the ISAR screening tool. J Am Geriatr Soc. 1999;47(10):1229–1237. doi:10.1111/j.1532-5415.1999.tb05204.x
13. Aigner R, Buecking B, Hack J, et al. Pre-fracture hospitalization is associated with worse functional outcome and higher mortality in geriatric hip fracture patients. Arch Osteoporos. 2017;12. doi:10.1007/s11657-017-0327-2
14. Asomaning N, Loftus C. Identification of Seniors at Risk (ISAR) screening tool in the emergency department: implementation using the plan-do-study-act model and validation results. J Emerg Nurs. 2014;40:357–364.e1. doi:10.1016/j.jen.2013.08.014
15. Di Bari M, Salvi F, Roberts AT, et al. Prognostic stratification of elderly patients in the emergency department: a comparison between the “identification of seniors at risk” and the “silver code.”. J Gerontol - Ser a Biol Sci Med Sci. 2012;67A:544–550. doi:10.1093/gerona/glr209
16. Suffoletto B, Miller T, Shah R, Callaway C, Yealy DM. Predicting older adults who return to the hospital or die within 30 days of emergency department care using the ISAR tool: subjective versus objective risk factors. Emerg Med J. 2016;33:4–9. doi:10.1136/emermed-2014-203936
17. Scharf AC, Gronewold J, Dahlmann C, et al. Health outcome of older hospitalized patients in internal medicine environments evaluated by Identification of Seniors at Risk (ISAR) screening and geriatric assessment. BMC Geriatr. 2019;19. doi:10.1186/s12877-019-1239-3
18. Garcia AE, Bonnaig JV, Yoneda ZT, et al. Patient variables which may predict length of stay and hospital costs in elderly patients with hip fracture. J Orthop Trauma. 2012;26(11):620–623. doi:10.1097/BOT.0b013e3182695416
19. Castelli A, Daidone S, Jacobs R, Kasteridis P, Street AD, Icks A. The determinants of costs and length of stay for hip fracture patients. PLoS One. 2015;10(7):e0133545. doi:10.1371/journal.pone.0133545
20. González-Zabaleta J, Pita-Fernandez S, Seoane-Pillado T, López-Calviño B, Gonzalez-Zabaleta JL. Comorbidity as a predictor of mortality and mobility after hip fracture. Geriatr Gerontol Int. 2016;16:561–569. doi:10.1111/ggi.12510
21. Nuotio M, Luukkaala T. Factors associated with changes in mobility and living arrangements in a comprehensive geriatric outpatient assessment after hip fracture. Disabil Rehabil. 2016;38(12):1125–1133. doi:10.3109/09638288.2015.1074728
22. Bliemel C, Buecking B, Oberkircher L, Knobe M, Ruchholtz S, Eschbach D. The impact of pre-existing conditions on functional outcome and mortality in geriatric hip fracture patients. Int Orthop. 2017;41(10):1995–2000. doi:10.1007/s00264-017-3591-2
23. Aigner R, Meier Fedeler T, Eschbach D, et al. Patient factors associated with increased acute care costs of hip fractures: a detailed analysis of 402 patients. Arch Osteoporos. 2016;11. doi:10.1007/s11657-016-0291-2
24. Guzon-Illescas O, Perez Fernandez E, Crespí Villarias N, et al. Mortality after osteoporotic hip fracture: incidence, trends, and associated factors. J Orthop Surg Res. 2019;14(1). doi:10.1186/s13018-019-1226-6
25. Chang W, Lv H, Feng C, et al. Preventable risk factors of mortality after hip fracture surgery: systematic review and meta-analysis. Int J Surg. 2018;52:320–328. doi:10.1016/j.ijsu.2018.02.061
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.