Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
The predictive value of somatic and cognitive depressive symptoms for cytokine changes in patients with major depression
Authors Dannehl K, Rief W ![]() , Schwarz MJ, Hennings A, Riemer S, Selberdinger V, Stapf T, Euteneuer F
, Schwarz MJ, Hennings A, Riemer S, Selberdinger V, Stapf T, Euteneuer F ![]()
Received 31 January 2014
Accepted for publication 28 February 2014
Published 28 June 2014 Volume 2014:10 Pages 1191—1197
DOI https://doi.org/10.2147/NDT.S61640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Katharina Dannehl,1 Winfried Rief,1 Markus J Schwarz,2 Annika Hennings,1 Sabine Riemer,1 Verena Selberdinger,3 Theresa Stapf,3 Frank Euteneuer1
1Division of Clinical Psychology and Psychotherapy, Philipps Universität Marburg, Marburg, Germany; 2Institute for Laboratory Medicine, Ludwig-Maximilian Universität, Munich, Germany; 3Department of Psychiatry, Ludwig-Maximilian Universität, Munich, Germany
Context: Elevated concentrations of proinflammatory cytokines have been hypothesized as an important factor in the pathophysiology of depression. Depression itself is considered to be a heterogeneous disorder. Current findings suggest that “cognitive” and “somatic” symptom dimensions are related to immune function in different ways. So far, little research has been done on the longitudinal aspects of inflammation in patients with major depression, especially with respect to different symptom dimensions of depression. Therefore, we investigated which aspects of depression may predict changes in tumor necrosis factor-alpha (TNF-alpha) and interleukin (IL)-6 over 4 weeks.
Methods: Forty-one patients with major depression diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), and 45 healthy controls were enrolled. Serum measurements of TNF-alpha and IL-6 were conducted at baseline and 4 weeks later. Psychometric measures included the assessment of cognitive-affective depressive symptoms and somatic symptoms during the last 7 days as well as somatic symptoms during the last 2 years.
Results: Patients with depression showed increased levels of TNF-alpha (P<0.05) compared to healthy controls. Hierarchical regression analyses indicated that neither depressive nor somatic symptoms predict changes in proinflammatory cytokines in the whole sample of depressed patients. Moderation analyses and subsequent sex-stratified regression analyses indicated that higher somatoform symptoms during the last 2 years significantly predict an increase in TNF-alpha in women with major depression (P<0.05) but not in men. Exploratory analyses indicated that the stability of TNF-alpha and IL-6 (as indicated by intraclass correlation coefficients) over 4 weeks was high for TNF-alpha but lower for IL-6.
Conclusion: The present study demonstrated that a history of somatoform symptoms may be important for predicting future changes in TNF-alpha in women with major depression.
Keywords: interleukin-6, tumor necrosis factor-alpha, symptom dimension
Introduction
Elevated concentrations of cytokines have been hypothesized as an important factor in the pathophysiology of depression. Meta-analytic results indicate increased levels of the proinflammatory cytokines interleukin (IL)-6 and tumor necrosis factor-alpha (TNF-alpha) in depressed patients compared to healthy controls.1,2 A recent study with healthy individuals has shown that depressive symptoms may precede and augment some inflammatory processes.3 Inflammatory mechanisms have been suggested to play a pivotal role in the relationship between depression and cardiovascular disease.4,5
Depression itself is considered to be a heterogeneous disorder. Current findings suggest that “cognitive” and “somatic” symptom dimensions are related in different ways to immune function and cardiovascular outcomes. Somatic symptoms have been shown to be better predictors of cardiovascular mortality and cardiac events in post-myocardial infarction patients and in patients with chronic heart failure (CHF).6–10 Additionally, somatic but not cognitive-affective depressive symptoms have been related to cardiovascular risk factors such as decreased heart rate variability and reduced baroreflex sensitivity.11,12 Somatic symptoms (especially sleeping disorders) predict further depressive episodes better than cognitive-affective symptoms.13 Regarding immunological measures, Duivis et al demonstrated that somatic symptoms of depression and anxiety but not cognitive symptoms are associated with higher inflammatory levels of C-reactive protein (CRP), IL-6, and TNF-alpha in a population-based sample.14 In patients with major depression, increased levels of soluble interleukin-2 receptors (sIL-2R) were associated with higher severity ratings of somatic symptoms but not with cognitive-affective depressive symptoms.15
Though many studies have focused on cross-sectional relationships between depression and proinflammatory cytokines, little research has been done on longitudinal aspects of inflammation in patients with major depression, especially with respect to different symptom dimensions of depression.16 In the present investigation, we aimed to learn whether changes in IL-6 and TNF-alpha over 1 month can be predicted by measures of cognitive-affective and somatic symptoms in patients with major depression. The prediction of changes in these inflammatory markers may be of relevance because an increase of proinflammatory cytokines contributes to several poor health outcomes.17–20 We hypothesized that primarily somatic aspects of depression may predict an increase in proinflammatory cytokines. Since previous research indicates sex differences in depression, immune function, and symptom dimensions, we further focused on the moderating role of sex.21–23 All analyses were performed for the whole sample and separated by sex.
Methods
Subjects
The study was approved by the ethics committees of the German Psychological Society and the Institutional Review Board of Munich University Clinical Center. Forty-one outpatients with major depression were recruited from the Outpatient Clinic for Psychological Interventions of the University of Marburg and the Department of Psychiatry of Munich University. Furthermore, 45 healthy controls were enrolled in the study. All participants underwent a diagnostic session which included the German version of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (SCID for the DSM-IV)24 and an interview that focused on exclusion criteria and on demographic variables. Exclusion criteria were organic illnesses involving the central nervous system (CNS) or affecting immune status (inflammatory diseases, infections, injuries in the last 2 weeks), psychotic symptoms, somatization disorder, pain disorder, alcohol and/or drug abuse, antipsychotics, stimulants, current psychotherapy (to allow reliable and unbiased evaluation of psychopathology), pregnancy and lactation in women, and any psychiatric diagnosis according to DSM-IV in controls.
Procedures
Participants visited the research facility for measurements at baseline (T1) and 4 weeks later (T2), without any intervention in the meantime. Most of these patients were considered for further ongoing longitudinal research after participating in the present investigation. Depressive and somatic symptoms as well as biological parameters were assessed at each visit.
Measures
Psychological variables
As mentioned in Methods, the German version of the SCID24 was used to confirm the diagnosis of major depression and comorbid axis-I disorders. The symptom severity of each participant was assessed using the German version of the Beck Depression Inventory II (BDI II).25 Cognitive-affective symptoms were assessed using the cognitive-affective subscale of the BDI II. To measure somatic symptom dimensions, two screenings for somatoform symptoms were used.26 The Screening for Somatoform Symptoms Scale-7 (SOMS-7) consists of 53 items, and measures somatic symptoms listed for somatization disorder and somatoform autonomic dysfunction in DSM-IV and the International Classification of Diseases, tenth revision (ICD-10) for the last 7 days. The Screening for Somatoform Symptoms Scale-2 (SOMS-2) included 68 items and rates somatic symptoms for the last 2 years. Both scales usually included six sex-related items, which were excluded to assure a better comparability between female and male participants.
Cytokine analysis
Blood samples were collected at 8 am, centrifuged, and stored at -80°C until thawed for assay. Participants were instructed to avoid exercise and alcohol 24 hours prior to blood withdrawal. Also, participants were instructed to avoid rushing and taking public transportation to the laboratory to avoid physical overexertion before blood sampling. Serum concentrations of IL-6 and TNF-alpha were determined using highly sensitive immunoassays according to the manufacturer’s instructions (Human IL-6 Quantikine HS and Human TNF-alpha Quantikine HS; R & D Systems, Minneapolis, MN, USA).
Statistical analysis
The statistical analyses were carried out with SPSS software (v19.0 for Windows; IBM Corporation, Armonk, NY, USA). As the immunological parameters were not normally distributed, the values of inflammatory markers were log-transformed to allow parametric testing. Boxplots were used to control for univariate outliers. Screening for multivariate outliers was performed by calculating Studentized deleted residuals and centered leverage values.27 To test for mean differences of cytokines and psychometric variables between patients and healthy controls, data were analyzed by repeated measures analysis of variance (ANOVA). In the same way, interaction effects of group, sex, and time were calculated. Pearson product-moment correlations were calculated to examine the relationships between cytokines and psychometric measures (BDI II, BDI II subscale, SOMS-7, SOMS-2) at baseline measurement (T1). To examine prospective relationships between depressive and somatic symptoms and changes in proinflammatory cytokines, hierarchical regression analyses were conducted. Baseline levels of cytokines were entered at step 1 while symptom dimensions were entered at step 2 to predict cytokine levels 4 weeks later. A number of moderation analyses were carried out to measure possible interactions between sex and symptom dimension in the prediction of changes in cytokines. Pearson product-moment correlation coefficients were used to examine the relationship between changes in psychometric measurements and changes in cytokine levels. Exploratory analyses of intraclass correlation coefficients (ICC) were conducted to estimate the variability of cytokine levels over time and 95% confidence intervals were calculated.
Results
The characteristics of participants and group differences in study variables are presented in Table 1. Patients with major depression and controls did not differ significantly with respect to age, education, sex, body mass index (BMI), and smoking status. With regards to psychological variables, patients scored significant higher in the BDI II (F[1, 88]=38.61, P<0.001), the cognitive-affective symptoms subscale of the BDI II (F[1, 88]=40.14, P<0.001), the SOMS-7 (F[1, 88]=24.02, P<0.001), and the SOMS-2 (F[1, 83]=92.9, P<0.001). In terms of cytokines, patients had significantly higher concentrations of TNF-alpha (F[1, 87]=0.16, P=0.045). No group difference was found for IL-6. There were no significant interaction effects between group, sex, and time (P>0.05).
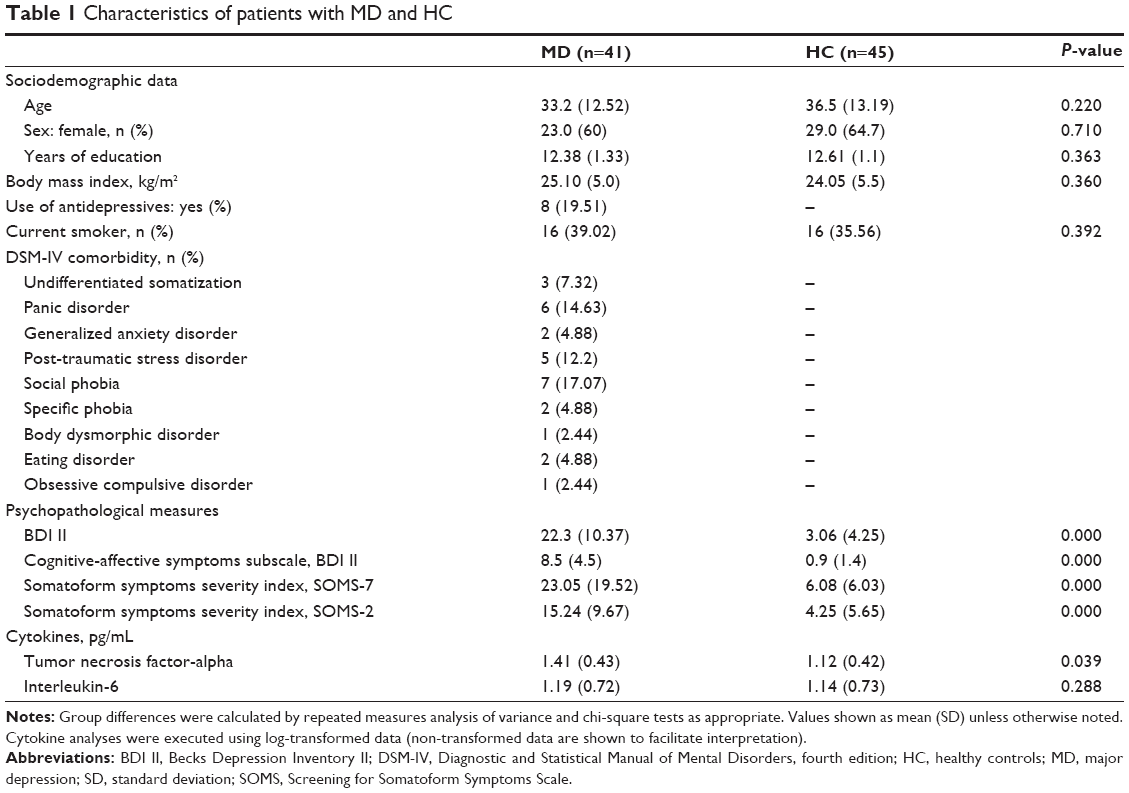 | Table 1 Characteristics of patients with MD and HC |
To test potential cross-sectional relationships between psychological variables and cytokines at baseline, bivariate correlations were performed. IL-6 and TNF-alpha are not significantly associated with BDI II (r=0.24, P=0.15; r=−0.7, P=0.7, respectively), the cognitive-affective symptoms subscale of the BDI II (r=0.11, P=0.52; r=−0.51, P=0.76, respectively), the SOMS-7 (r=0.18, P=0.28; r=−0.001, P=0.97, respectively), or the SOMS-2 (r=0.12, P=0.25; r=0.5, P=0.77, respectively).
For patients with major depression, a number of hierarchical regression analyses were conducted to examine if depressive and somatic symptoms (step 2) predict proinflammatory cytokines 4 weeks later after controlling for cytokine levels at baseline (step 1). The results for step 1 indicated that baseline levels of TNF-alpha (T1) were significantly related to TNF-alpha levels 4 weeks later (T2) (β=0.83, R2=0.688, P<0.001). Regarding changes in TNF-alpha, neither total depressive symptoms (β=0.14, ΔR2=0.019, P=0.147), cognitive-depressive symptoms (β=0.15, ΔR2=0.021, P=0.124), somatoform symptoms during the last 7 days (P=0.557, ΔR2=0.003, β=0.06), nor somatoform symptoms during the last 2 years (P=0.147, ΔR2=0.021, β=0.14) were of significant predictive value.
Similar results were found for IL-6: the baseline levels of IL-6 (T1) were significantly related to IL-6 levels 4 weeks later (T2) (β=0.55, R2=0.304, P<0.001). Like TNF-alpha, changes in IL-6 were not predicted neither from total depressive symptoms (β=0.04, ΔR2=0.001, P=0.793), cognitive-depressive symptoms (β=-0.07, ΔR2=0.005, P=0.626), somatoform symptoms during the last 7 days (β=-0.04, ΔR2=0.002, P=0.772), nor somatoform symptoms during the last 2 years (β=0.08, ΔR2=0.006, P=0.581).
Additionally, a number of moderation analyses were conducted to examine whether there were significant interactions between sex and symptom dimension in the prediction of changes in cytokines. Centered symptom scores and sex (dummy coded) were entered at step 2 after accounting for baseline levels of cytokines at step 1. Interaction terms of centered symptom scores and sex were entered at step 3. Results indicated that interaction terms did not significantly explain variance (P>0.1) with one exception: SOMS-2 × sex interaction terms accounted for significant increments of variance in changes of TNF-alpha (β=-0.40, ΔR2=0.046, P=0.027) beyond what was accounted for by sex (β=0.05; P=0.593) and SOMS-2 scores (β=0.14; P=0.167) at step 2 (ΔR2=0.024; P=0.307). Figure 1 illustrates this significant interaction. Follow-up sex-stratified regression analyses indicated that higher somatoform symptoms during the last 2 years significantly predict an increase in TNF-alpha in women with major depression (β=0.31, ΔR2=0.095, P=0.019), but not in men (β=-0.01, ΔR2<0.001, P=0.930).
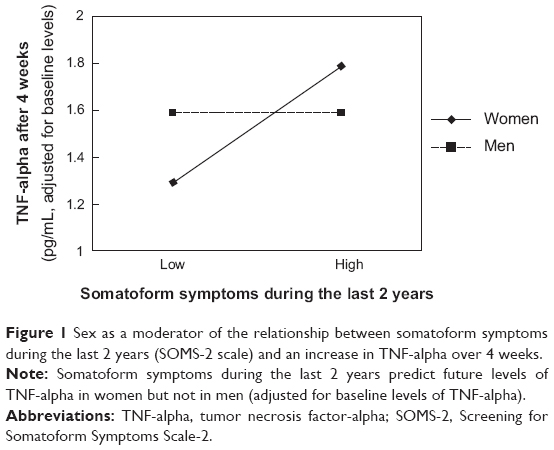 | Figure 1 Sex as a moderator of the relationship between somatoform symptoms during the last 2 years (SOMS-2 scale) and an increase in TNF-alpha over 4 weeks. |
The calculation of ICC in the patient group showed a high ICC of 0.82 for TNF-alpha, which suggests strong stability of TNF-alpha over 1 month. Consistent with these findings, there was a significant correlation for TNF-alpha between T1 and T2 (r=0.83). The ICC for IL-6 was moderate (0.50) and similarly, there was a fair correlation between the two points of measurement (r=0.55). In the healthy control group, the ICC for TNF-alpha (0.55) was moderate as well (r=0.71), whereas the stability of IL-6 over 1 month was fair (ICC =0.43; r=0.43) (see Table 2). Calculations of ICC carried out separated by sex showed essentially equivalent results (data not shown).
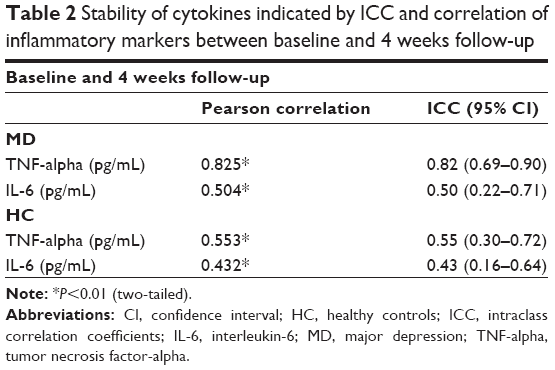 | Table 2 Stability of cytokines indicated by ICC and correlation of inflammatory markers between baseline and 4 weeks follow-up |
Discussion
In the present study, we investigated whether changes in IL-6 and TNF-alpha over 4 weeks can be predicted by measures of cognitive-affective and somatic symptoms in patients with major depression. As a main result, we found that higher somatoform symptoms during the last 2 years significantly predict an increase in TNF-alpha in women with major depression but not in men. While TNF-alpha was significantly higher in patients with major depression, no group differences were observed for IL-6. Exploratory analyses indicated a high stability of TNF-alpha over 4 weeks in patients with major depression and a moderate stability in healthy controls. IL-6 was less stable in both groups.
Former research in healthy populations has shown that elevated cytokines are risk markers for coronary heart diseases.28,29 Our finding that higher somatoform symptoms over the last 2 years significantly predicts an increase in TNF-alpha in depressive women is in line with previous results that link somatic symptoms with inflammatory markers and poor cardiovascular outcomes.5,30 In women with suspected myocardial ischemia, somatic but not cognitive-affective depressive symptoms were associated with an increased risk of cardiovascular-related mortality and events.6 Similarly, there are findings that in patients with CHF, only somatic depressive symptoms predict all-cause mortality in CHF.7 Roest et al demonstrated in 2013 that changes in somatic depressive symptoms, but not in cognitive-affective symptoms of depression, were related to improved outcomes concerning event-free survival following acute myocardial infarction in cardiac patients.31 A cross-sectional study found associations between somatic, but not cognitive symptom dimensions of depression and cardiovascular morbidity in the general population.32 Furthermore, it was shown that only the somatic symptom dimension of depression was associated with increased levels of cytokines (IL-18- and IL-1-receptor antagonists). In patients with major depression, increased concentrations of sIL-2R were related to the severity of somatoform symptoms and somatic anxiety symptoms, but not to cognitive-affective depressive symptoms.15 Considering the aforementioned links between inflammatory markers and cardiovascular health, our findings may support the idea that somatic symptoms can predict cytokine changes, which might be of potential relevance for cardiovascular disease.
Consistent with previous studies, our results confirm the important role of sex concerning the symptoms of depression and inflammation.23,33 Prevalence rates of major depression are higher in women34,35 and there is evidence that they develop more somatic symptoms than men with major depression.36,37 Regarding inflammation, women show enhanced immunoreactivity and a higher risk for autoimmune diseases compared to men.38 In 2004, Lekander et al showed that poorer subjective health was associated with higher levels of IL-1 and TNF-alpha in women but not in men.39 In line with these observed sex differences, the present study demonstrated that for women, but not for men, somatoform symptoms of depression are meaningful predictors for future changes in proinflammatory markers. These markers in turn are predictors for the future course of depression, symptom severity, and potential cardiovascular diseases.28,40,41 Further research as well as therapeutic and medical interventions to treat depression and prevent poor health should keep these findings in mind.
Our results regarding the stability of TNF-alpha and IL-6 show an acceptable stability of the cytokines over 4 weeks for both patients with major depression and controls. In particular, strong stability was observed for TNF-alpha. Compared to TNF-alpha, the ICC of IL-6 was less stable. These results are relevant for the interpretation of studies investigating issues concerning cytokines.
Although our study has strengths, such as the longitudinal design, some limitations have to be noted. The results should be interpreted with caution given the relatively small sample size. In addition, the larger number of women may bias our results. Finally, we measured TNF-alpha and IL-6 just over 1 month. To get more meaningful results, longer periods of measurement are needed.
In conclusion, our results provide further evidence for the importance of the differentiation between somatic and cognitive-affective symptoms in major depression. Somatic symptoms seem to be better predictors for changes in TNF-alpha than cognitive-affective symptoms in women with major depression.
Acknowledgments
We wish to thank all participants and our students Anina Burgbacher and Benedikt Bedenk for helping with the recruitment of participants.
This study was funded by a grant from the German Research Foundation (DFG) to Dr Rief (Ri 574/13). The DFG had no further role in the study design; in the collection, analysis, and interpretation of the data; in the writing of the report or in the decision to submit the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71(2):171–186. | ||
Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67(5):446–457. | ||
Stewart JC, Rand KL, Muldoon MF, Kamarck TW. A prospective evaluation of the directionality of the depression-inflammation relationship. Brain Behav Immun. 2009;23(7):936–944. | ||
Halaris A. Inflammation, heart disease, and depression. Curr Psychiatry Rep. 2013;15(10):400. | ||
Vaccarino V, Johnson BD, Sheps DS, et al. Depression, inflammation, and incident cardiovascular disease in women with suspected coronary ischemia: the National Heart, Lung, and Blood Institute-sponsored WISE study. J Am Coll Cardiol. 2007;50(21):2044–2050. | ||
Linke SE, Rutledge T, Johnson BD, et al. Depressive symptom dimensions and cardiovascular prognosis among women with suspected myocardial ischemia: a report from the National Heart, Lung, and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation. Arch Gen Psychiatry. 2009;66(5):499–507. | ||
Schiffer AA, Pelle AJ, Smith OR, Widdershoven JW, Hendriks EH, Pedersen SS. Somatic versus cognitive symptoms of depression as predictors of all-cause mortality and health status in chronic heart failure. J Clin Psychiatry. 2009;70(12):1667–1673. | ||
Myint AM, Kim YK, Verkerk R, Scharpé S, Steinbusch H, Leonard B. Kynurenine pathway in major depression: evidence of impaired neuroprotection. J Affect Disord. 2007;98(1–2):143–151. | ||
de Jonge P, Ormel J, van den Brink RH, et al. Symptom dimensions of depression following myocardial infarction and their relationship with somatic health status and cardiovascular prognosis. Am J Psychiatry. 2006;163(1):138–144. | ||
Smolderen K, Spertus J. The association of cognitive and somatic depressive symptoms with depression recognition and outcomes after myocardial infarction. Circ Cardiovasc Qual Outcomes. 2009;2(4):328–337. | ||
Bosch NM, Riese H, Dietrich A, Ormel J, Verhulst FC, Oldehinkel AJ. Preadolescents’ somatic and cognitive-affective depressive symptoms are differentially related to cardiac autonomic function and cortisol: the TRAILS study. Psychosom Med. 2009;71(9):944–950. | ||
de Jonge P, Mangano D, Whooley MA. Differential association of cognitive and somatic depressive symptoms with heart rate variability in patients with stable coronary heart disease: findings from the heart and soul study. Psychosom Med. 2007;69(8):735–739. | ||
Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry. 1996;39(6):411–418. | ||
Duivis HE, Vogelzangs N, Kupper N, de Jonge P, Penninx BWJH. Differential association of somatic and cognitive symptoms of depression and anxiety with inflammation: findings from the Netherlands Study of Depression and Anxiety (NESDA). Psychoneuroendocrinology. 2013;38(9):1573–1585. | ||
Euteneuer F, Schwarz MJ, Dannehl K, Hartung A, Westermann S, Rief W. Increased soluble interleukin-2 receptor levels are related to somatic but not to cognitive-affective features in major depression. Brain Behav Immun. 2012;26(8):1244–1248. | ||
Kupper N, Widdershoven JW, Pedersen SS. Cognitive/affective and somatic/affective symptom dimensions of depression are associated with current and future inflammation in heart failure patients. J Affect Disord. 2012;136(3):567–576. | ||
Shanahan JC, St Clair W. Tumor necrosis factor-α blockade: a novel therapy for rheumatic disease. Clin Immunol. 2002;103(3):231–242. | ||
Coussens L, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. | ||
Cesari M, Penninx BWJH, Newman AB, et al. Inflammatory markers and onset of cardiovascular events: results from the Health ABC study. Circulation. 2003;108(19):2317–2322. | ||
Salanitro AH, Ritchie CS, Hovater M, et al. Inflammatory biomarkers as predictors of hospitalization and death in community-dwelling older adults. Arch Gerontol Geriatr. 2012;54(3):e387–e391. | ||
Shanmugasegaram S, Russell KL, Kovacs AH, Stewart DE, Grace SL. Gender and sex differences in prevalence of major depression in coronary artery disease patients: a meta-analysis. Maturitas. 2012;73(4):305–311. | ||
Steiner M. Serotonin, depression, and cardiovascular disease: sex-specific issues. Acta physiol (Oxf). 2011;203(1):253–258. | ||
Pennell LM, Galligan CL, Fish EN. Sex affects immunity. J Autoimmun. 2012;38(2–3):J282–J291. | ||
Wittchen HU, Wunderlich U, Gruschitz S, Zaudig M. Strukturiertes Klinisches Interview für DSM-IV, Achse I (SKID-I) [The structured clinical interview for DSM-IV, Axis-I, SCID-I]; 1997. German. | ||
Hautzinger M, Keller F, Kühner C. Das Beck Depressions Inventar II. Deutsche Bearbeitung und Handbuch zum BDI II. Frankfurt: Harcourt Test Services; 2006. German. | ||
Rief W, Hiller W. Screening für Somatoforme Störungen: SOMS (2., vollständig überarb. und neu normierte Aufl.). Bern, Göttingen, Toronto, Seattle: Huber; 2003. German. | ||
Fox J. Regression Diagnostics: An Introduction. Thousand Oaks, CA: Sage Publications; 1991. | ||
Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000;1(8):1066–1067. | ||
Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation. 2000;101(15):1767–1772. | ||
Shimbo D, Chaplin W, Crossman D, Haas D, Davidson KW. Role of depression and inflammation in incident coronary heart disease events. Am J Cardiol. 2005;96(7):1016–1021. | ||
Roest AM, Carney RM, Freedland KE, Martens EJ, Denollet J, de Jonge P. Changes in cognitive versus somatic symptoms of depression and event-free survival following acute myocardial infarction in the Enhancing Recovery In Coronary Heart Disease (ENRICHD) study. J Affect Disord. 2013;149(1–3):335–341. | ||
Michal M, Wiltink J, Kirschner Y, et al. Differential associations of depressive symptom dimensions with cardio-vascular disease in the community: results from the Gutenberg health study. PLoS one. 2013; 8(8):e72014. | ||
Oertelt-Prigione S. The influence of sex and gender on the immune response. Autoimmun Rev. 2012;11(6–7):A479–A485. | ||
Delisle VC, Beck AT, Dobson KS, Dozois DJ, Thombs BD. Revisiting gender differences in somatic symptoms of depression: much ado about nothing? PLoS one. 2012;7(2):e32490. | ||
Heim C, Newport DJ, Mletzko T, Miller AH, Nemeroff CB. The link between childhood trauma and depression: insights from HPA axis studies in humans. Psychoneuroendocrinology. 2008;33(6):693–710. | ||
Silverstein B. Gender differences in the prevalence of somatic versus pure depression: a replication. Am J Psychiatry. 2002;159(6):1051–1052. | ||
Kroenke K, Spitzer RL. Gender differences in the reporting of physical and somatoform symptoms patient characteristics. Psychosom Med. 1998;60(2):150–539. | ||
Cannon J, Pierre BS. Gender differences in host defense mechanisms. J Psychiatr Res. 1997;31(1):99–113. | ||
Lekander M, Elofsson S, Neve IM, Hansson LO, Undén AL. Self-rated health is related to levels of circulating cytokines. Psychosom Med. 2004;66(4):559–563. | ||
Lindqvist D, Janelidze S, Hagell P, et al. Interleukin-6 is elevated in the cerebrospinal fluid of suicide attempters and related to symptom severity. Biol Psychiatry. 2009;66(3):287–292. | ||
Gimeno D, Kivimaki M. Associations of C-reactive protein and interleukin-6 with cognitive symptoms of depression: 12-year follow-up of the Whitehall II study. Psychol Med. 2009;39(3):413–423. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.