Back to Journals » International Journal of General Medicine » Volume 17
The Predictive Value of Hemoglobin to Red Cell Blood Distribution Width Ratio Combined with Serum Sodium for MACE of Acute Heart Failure with Preserved Ejection Fraction in Elderly Patients
Authors Yuan X, Lv C, Wu S ![]() , Wang H, Liu X
, Wang H, Liu X
Received 14 January 2024
Accepted for publication 25 February 2024
Published 6 March 2024 Volume 2024:17 Pages 863—870
DOI https://doi.org/10.2147/IJGM.S453538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Xiaoye Yuan, Caixia Lv, Sisi Wu, Huiying Wang, Xiaoyu Liu
Department of Geriatric Cardiovascular, Hebei General Hospital, Shijiazhuang, 050000, People’s Republic of China
Correspondence: Xiaoye Yuan, Department of Geriatric Cardiovascular, Hebei General Hospital, No. 348, Heping West Road, Shijiazhuang, 050000, People’s Republic of China, Tel +86-15511308370, Email [email protected]
Purpose: To investigate the predictive value of hemoglobin (Hb) to red blood cell distribution width (RDW) (Hb/RDW) ratio in combination with serum sodium for major adverse cardiovascular events (MACE) in elderly acute heart failure patients with preserved ejection fraction at 30 days after discharge.
Methods: 130 elderly acute heart failure patients with preserved ejection fraction were enrolled and followed up at 30 days after discharge. They were classified into the MACE group (n=11) and none-MACE group (n=119). On the day of admission, clinical baseline characteristics were measured and results from laboratory tests were gathered. The correlation and predictive value of Hb/RDW and serum sodium with the occurrence of MACE at 30 days after discharge in acute heart failure patients with preserved ejection fraction in the elderly were analyzed.
Results: Spearman correlation analysis showed that the occurrence of MACE was negatively correlated with Hb/RDW, serum sodium (r=− 0.209, r=0.291, p< 0.05) and Hb/RDW (OR=0.484, 95% CI:0.254, 0.922), serum sodium (OR=0.779, 95% CI:0.646,0.939) were independent risk factors (p< 0.05) analyzed by multifactorial logistic. Receiver operating characteristic curves (ROC) analysis showed that the area under the curve (AUC) for the prediction of MACE by Hb/RDW was 0.73, with an optimal threshold of 9.28, sensitivity 81.80%, specificity 70.60%, positive predictive value (PPV) 20.50%, negative predictive value (NPV) 97.70%; the AUC of serum sodium for predicting the occurrence of MACE was 0.76, with an optimal threshold of 140.35 mmol/L, sensitivity 90.90%, specificity 57.10%, PPV 16.40%, NPV 98.60%; and the AUC of Hb/RDW combined serum sodium to predict the occurrence of MACE was 0.83, with sensitivity 90.90%, specificity 78.20%, PPV 27.80% and NPV 98.90%.
Conclusion: Hb/RDW and serum sodium had negative correlation with MACE and were independent risk factors of 30-day MACE; Hb/RDW combined with serum sodium can predict 30-day MACE occurrence in elderly acute heart failure patients with preserved ejection fraction.
Keywords: hemoglobin to red cell blood distribution width ratio, serum sodium, acute heart failure, MACE, predictive value, elderly
Introduction
Heart failure (HF) is the end stage of various heart diseases and it is the fastest growing cardiovascular health burden worldwide.1 HF is a quintessential cardiovascular disease of the elderly, with the incidence increasing from 6% between the ages of 60 and 79 to 12% over the age of 80, while its incidence is likely to continue to rise in the future due to an aging population.2 The incidence of heart failure is likely to continue to rise as the population ages. Heart failure with preserved ejection fraction (HFpEF) is a complex cardiovascular syndrome with a left ventricular ejection fraction (LVEF) greater than or equal to 50%, which is characterized by a failure of the left ventricle to relax properly due to cellular and structural cellular alterations. Inflammatory factors and metabolic abnormalities play an important role in the development of HFpEF. HFpEF is prevalent in elderly patients. Acute heart failure (AHF) is a syndrome, mainly associated with acute systemic congestion, manifesting as new-onset heart failure, or worsening of symptoms and signs of pre-existing heart failure. AHF has high morbidity and mortality. Therefore, for elderly AHF with preserved ejection fraction, simple and rapid identification of its high risk is of great clinical significance for improving rescue and prognosis.
Hemoglobin (Hb) is an important predictor of prognosis in heart failure, and low level of Hb usually indicates poor clinical status and prognosis. Red blood cell distribution width (RDW) is an important parameter for evaluating the variability of circulating red blood cell volume, and its elevation is associated with increased morbidity and mortality in patients with chronic heart failure. It was found that Hb/RDW-SD was negatively associated with 3-month readmission for heart failure3 and also found that Hb/RDW is a preferable prognostic index than Hb or RDW alone. In light of research advances which is mentioned above, Hb/RDW ratio may be a good option for prognostic assessment of elderly AHF patients with ejection fraction at 30 days after discharge. Serum sodium disorders are common in patients with HF, and hyponatremia is prevalent. Moreover, persistent hyponatremia after hospitalization has been shown to be associated with a 1.5 to 1.7-fold increase risk of 30-day readmission or mortality.4,5 In a word, Hb/ RDW combined serum sodium should be a better choice for elderly AHF patients with preserved ejection fraction when figuring out their risk of occurrence of major adverse cardiovascular events (MACE). However, there are few studies on the Hb/RDW ratio in AHF patients with preserved ejection fraction, especially in the elderly. Therefore, in this study, we proposed to observe the predictive value of Hb/RDW combined with serum sodium on the occurrence of 30-day MACE in the elderly acute heart failure patients with preserved ejection fraction after discharge.
Material and Methods
Study Population
130 elderly acute heart failure patients with preserved ejection fraction discharged from our hospital were selected for retrospective analysis. After follow-up, they were categorized into MACE group (11 cases) and none-MACE group (119 cases) according to whether MACE occurred at 30 days of discharge. According to the 2021 ESC guidelines,6 the diagnosis of acute heart failure was performed and the diagnostic criteria for HFpEF were: (1) Symptoms and signs of HF. (2) An LVEF≥50% (Of note, patients with a history of overtly reduced LVEF≤40%, who later present with LVEF≥50%, should be considered to have recovered HFrEF or “HF with improved LVEF” (rather than HFpEF).) (3) Objective evidence of cardiac structural and/or functional abnormalities consistent with the presence of LV diastolic dysfunction/ raised LV filling pressures, including raised natriuretic peptides. (N-terminal pro-B-type natriuretic peptide (NT-proBNP) >125 (sinus rhythm) or B-type natriuretic peptide(BNP)>365 (atrial fibrillation) pg/mL >35 (sinus rhythm) or >105 (atrial fibrillation) pg/mL. Exclusion criteria included acute coronary syndrome, myocarditis, anemia, active hepatobiliary disease, severe chronic obstructive pulmonary disease, severe liver disease (>3-fold maximum normal values of alanine aminotransferase and aspartate transaminase), and kidney insufficiency (>2-fold maximum normal value of creatinine).
Data Collection
The main categories of collected data included demographic data, baseline clinical characteristics, laboratory results, comorbidities, and ultrasonic parameters. The patient’s age, sex, height, weight, department where the patient was admitted, occupation and date of admission were indicated on the first page of the medical record. On the day of admission, basic clinical characteristics were measured: temperature, heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and body mass index (BMI). The laboratory test results were obtained on the day of admission. Hematological parameters (including Hb and RDW) were measured using a SYSMEXXN3000 blood cell analyzer (Japan). Biochemical parameters (including serum sodium) were assayed using an ECKMAN COULTER AU5800 chemistry analyzer (USA). A COBAS H 232 cardiac system analyzer (Switzerland) was used to detect NT-proBNP levels.
Statistical Analysis
SPSS (version 22.0; SPSS, Chicago, IL, USA) was used for data analysis. Continuous variables are presented as mean±SD for values with normal distributions, median (quartiles) for skewed distributions and frequency or percentile for categorical variables. Group means and proportions were compared for significant differences using one-way ANOVA (normal distribution), Kruskal–Wallis H-test (skewed distribution) and chi-square test (categorical variables). Correlations were evaluated using the Spearman’s rank correlation test. Receiver operating characteristic curves (ROCs) were used for Hb/RDW and serum sodium to determine the predictive value of Hb/RDW combined with serum sodium on the occurrence of 30-day MACE in elderly acute heart failure patients with preserved ejection fraction. Areas under the curve (AUCs) were constructed, and 95% confidence intervals (CI) were calculated. We used the maximum Yuden index to define the optimal cut-off values, sensitivity, and specificity. p-value <0.05.
Results
General Clinical Information and Baseline Characteristics of Blood and Biochemical Indicators
The number of age, sex, smoking, alcohol consumption, hypertension, diabetes mellitus, cerebrovascular disease, atrial fibrillation were compared between the MACE group and the no-MACE group, with no statistical significance (p>0.05), and the number of prevalent cases of coronary artery disease in the MACE group was significantly higher than that of the none-MACE group in the group [10(90.90%),58(50.90%)], with a statistical difference (p<0.05). The red blood cell, urea nitrogen, creatinine, and NT-proBNP levels in the MACE group were significantly higher than in the none-MACE group, with statistical differences (p<0.05). The levels of Hb/RDW and serum sodium in the MACE group were significantly reduced compared with those in the none-MACE group (8.78±1.38,10.04±1.66; 137.85 (131.25, 137.85) mmol/L, 141.40 (139.00, 143.28) mmol/L), the difference was statistically significant (p<0.05). There was no statistically significant difference in medication use between the two groups of patients (p>0.05). (Table 1)
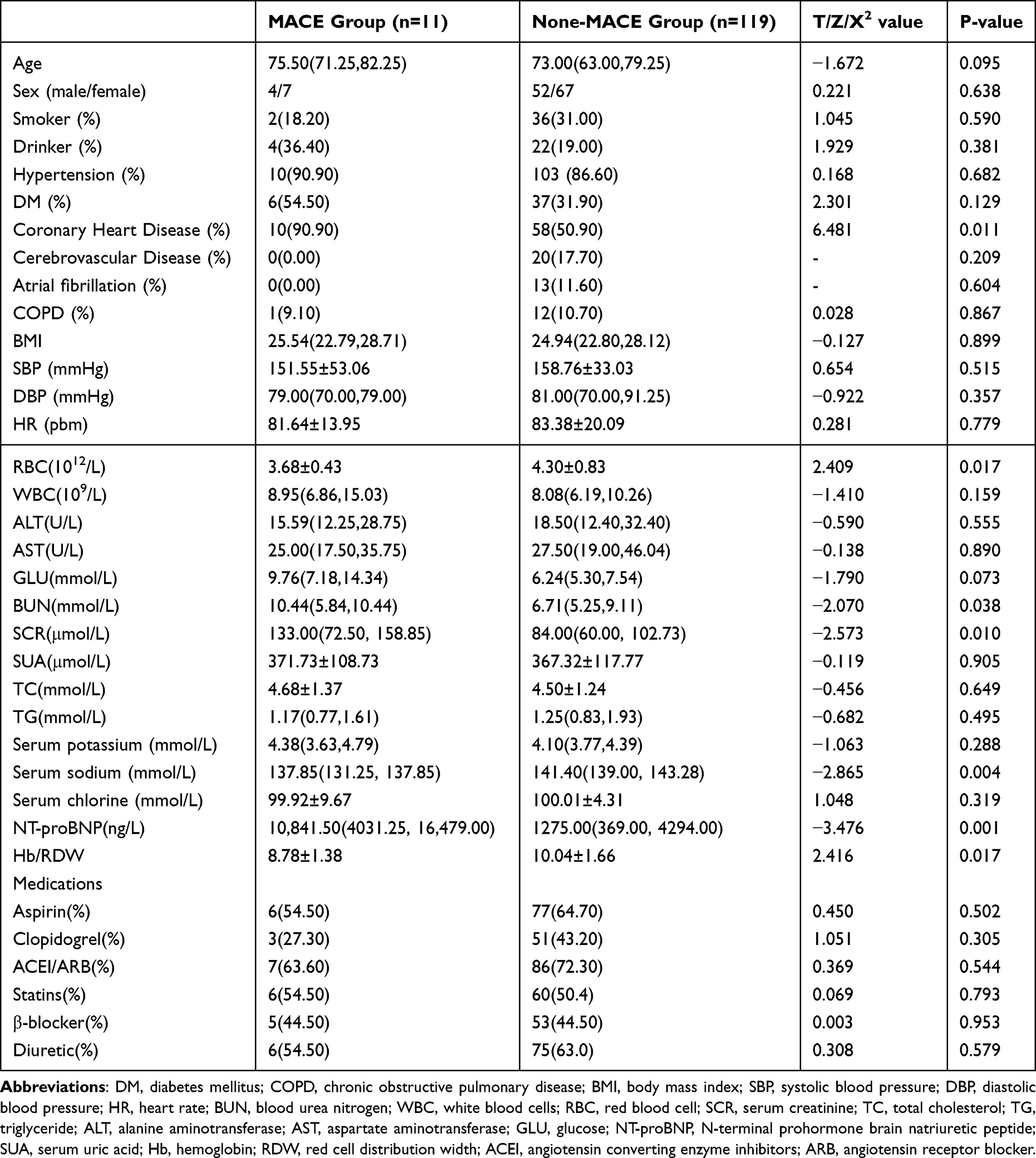 |
Table 1 General Clinical Information and Baseline Characteristics of Blood and Biochemical Indicators |
Spearman Correlation Analysis
Using Spearman’s method, Hb/RDW, serum sodium, and red blood cell levels had a significant negative correlation with MACE (r=−0.209, r=−0.291, and r=−0.208) (p < 0.05), and the levels of creatinine and NT-proBNP were significantly and positively correlated with MACE (r = 0.348, r = 0.351, p<0.05). (Table 2)
 |
Table 2 Spearman Correlation Analysis of MACE Occurrence |
Independent Risk Factors and ROCs Analysis
Multifactorial logistic regression analysis showed that Hb/RDW [OR = 0.484, 95% CI (0.254,0.922)], serum sodium [OR = 0.779, 95% CI (0.646,0.939)], and creatinine [OR = 1.306, 95% CI (1.005,1.068)] were independent risk factors of MACE at 30 days for the elder acute heart failure patients with preserved ejection fraction after discharge (p<0.05). By drawing ROCs, the area under the curve (AUC) of Hb/RDW for predicting the occurrence of MACE was 0.73, with a cutoff value of 9.28, a sensitivity of 81.80%, a specificity of 70.60%, a positive predictive value(PPV) of 20.50%, and a negative predictive value(NPV) of 97.70%. The AUC of serum sodium for the prediction of MACE was 0.76, the cut-off value was 140.35mmol/L, the sensitivity was 90.90%, the specificity was 57.10%, the PPV was 16.40%, and the NPV was 98.60%. For predicting MACE, the AUC of combination of Hb/RDW and sodium was 0.83, the sensitivity was 90.90%, the specificity was 78.20%, and the PPV was 98.90% and the NPV was 27.80%. (Tables 3 and 4) (Figure 1)
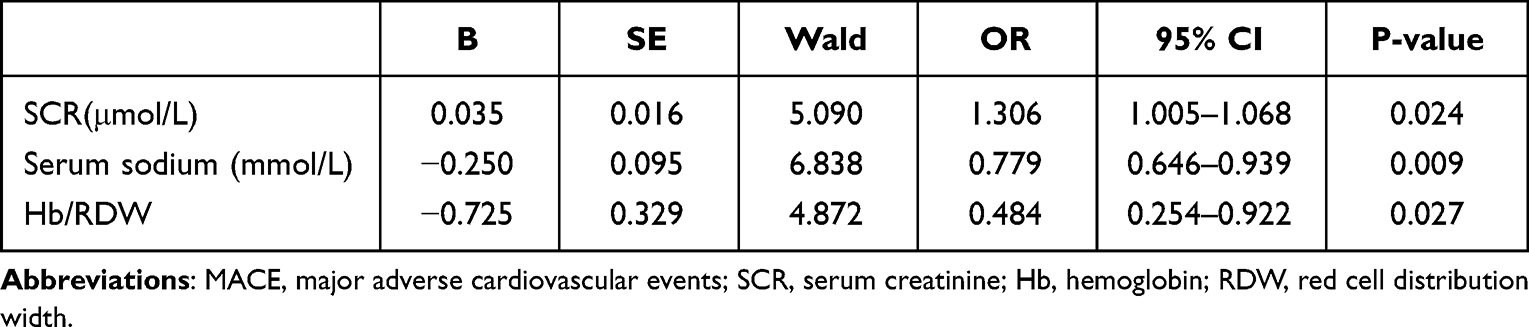 |
Table 3 Logistic Analysis of Risk Factors for the Occurrence of MACE |
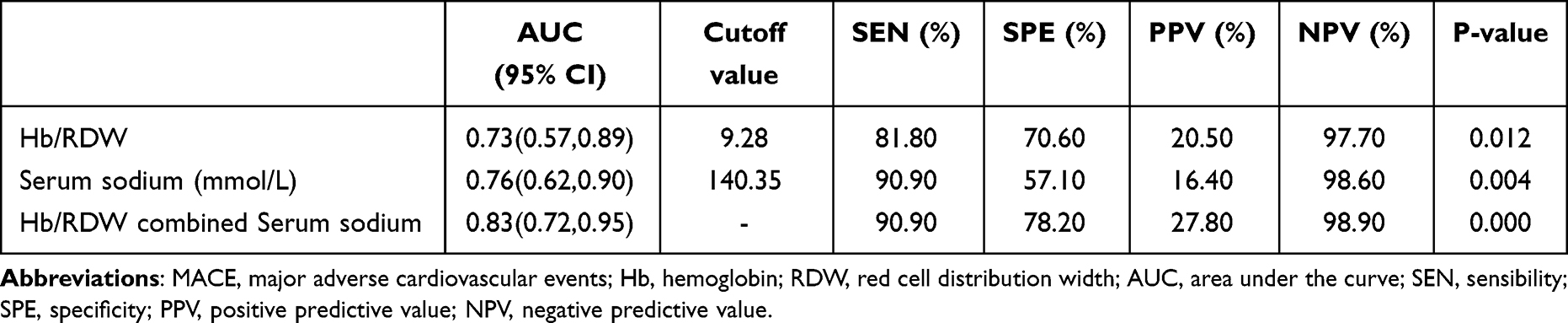 |
Table 4 ROCs Analysis of the Hb/RDW, Serum Sodium Predictive Value on MACE Occurrence in Acute Heart Failure with Ejection Fraction Retention in the Elderly |
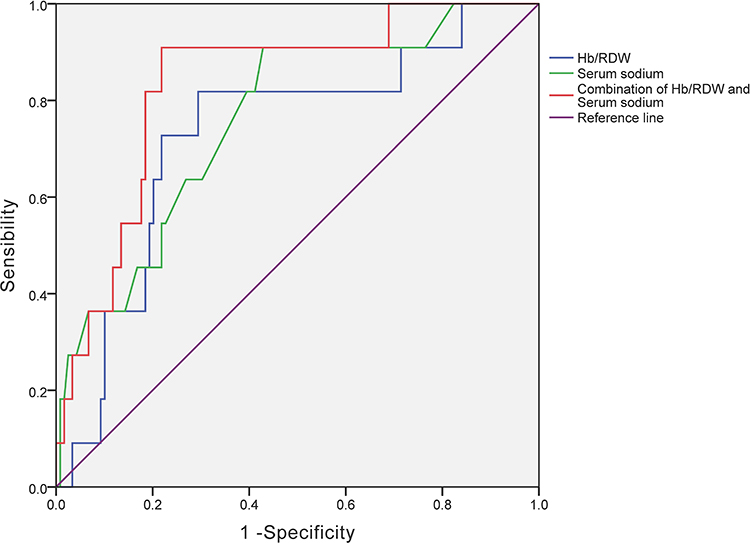 |
Figure 1 AUCs of Hb/RDW, Serum sodium and combination of them to predict the MACE at 30 days. |
Discussion
Our study indicated that the levels of Hb/RDW and serum sodium were lower in the MACE group than in the none-MACE group. They were negatively associated with MACE and were independent risk factors of the 30-day MACE. Hb/RDW combined with serum sodium can predict 30-day MACE occurrence in the elderly acute heart failure patients with preserved ejection fraction.
In recent years, the incidence and prevalence of heart failure is increasing year by year globally, affecting nearly 23 million people, with a high prevalence especially among the elderly population, and the number of hospitalizations and deaths due to heart failure is on the rise. According to China’s National Bureau of Statistics 2020, by the end of 2019, there were approximately 254 million people over the age of 60, accounting for 18.1% of the total population7. HFpEF is the dominant form of HF in the older population. The most often mentioned prevalence estimate for the adult population at large is 2% (1–3%), and 5–9% selectively in those aged 65 years and over.8,9 AHF is a new onset or worsening of heart failure signs and symptoms and is the most common cause of unplanned hospitalization in patients 65 years of age.10 Therefore, it is particularly important to effectively identify the occurrence of MACE at 30 days when the elderly acute heart failure patients with preserved ejection fraction discharge, which can provide effective treatment for the patients for improving prognosis.
To our knowledge, Hb reflects the level of malnutrition and inflammation in the body, which is a marker of the severity of heart failure and is an important predictor of the prognosis of heart failure. RDW is the range of variability in the size or shape of red blood cell volume, and is an indicator of the average heterogeneity of red blood cell volume in routine blood tests. Initially, higher levels of RDW were used to identify malnutritional anemia due to the deficiency of iron, folate, and vitamin B12. Duchnowski P11 et al showed that RDW could predict various cardiovascular diseases. Currently, RDW has gradually become a strong predictor of heart failure. Several studies in recent years have shown that Hb/RDW may be a better predictor of disease than a single indicator. This concept was first proposed by Sun12 et al and was demonstrated in patients with esophageal squamous cell carcinoma. Subsequently, Qu13 et al demonstrated that Hb/RDW is an independent risk factor for predicting frailty in coronary patients. Therefore, our study investigated the effect of Hb/RDW on short-term prognosis in elderly acute heart failure patients with preserved ejection fraction. The results showed that Hb/RDW was significantly lower in the MACE group than in the none-MACE group and was negatively correlated with the occurrence of MACE. Hb/RDW is an independent risk factor for MACE. This is due to the damage of cardiomyocytes in HFpEF patients, the cell membrane permeability increases and the osmotic pressure of tissue fluid rises, leading to the accumulation of a large amount of water in the body, which causes an increase in cardiac load and blood dilution, and a decrease in the secretion of erythropoietin and iron-regulating hormone, which affects the secretion of transferrin and the absorption of iron from food, and the appearance of a decrease in Hb.14 In addition, due to the significant elevation of pro-inflammatory cytokines in the body fluids of patients with HFpEF, RDW increases by enhancing oxidative stress, inhibiting bone marrow, impairing iron mobilization and inhibiting erythropoietin-induced erythrocyte maturation.14 Moreover, when AHF occurs, glomerular filtration rate decreases in patients, tubular water and sodium reabsorption increases, blood volume increases, leading to sodium retention and dilutional anemia, as well as a decrease in Hb;15 at the same time, due to inflammatory response and oxidative damage, erythropoietic cell maturation is affected in the bone marrow, which results in altered morphology of erythropoiesis and affects its overall homogeneity, causing an increase in RDW level. Therefore, the lower the Hb/RDW, the worse the short-term prognosis of acute heart failure with preserved ejection fraction in the elderly. Further ROC analysis showed that Hb/RDW has a good predictive value for the occurrence of 30-day MACE in elderly acute heart failure patients with preserved ejection fraction.
Patients with AHF are prone to hyponatremia due to activation of the renin angiotensin system and elevated levels of antidiuretic hormone. Serum sodium disorder during HF episodes correlates with poor clinical prognosis. Several studies have demonstrated that patients with chronic heart failure, HFpEF, heart failure with reduced ejection fraction, and AHF combined with hyponatremia have increased hospital mortality rates, increased rates of unplanned rehospitalization.16–19 Matsue et al19 found that persistently low serum sodium level was a better predictor of prognosis in patients with HF. Davison’study20 demonstrated that lower serum sodium levels in patients with heart failure were associated with readmission within 30 days of discharge and death within 90 days. In our study, serum sodium was significantly lower in the MACE group than in the none- MACE group and correlation analysis showed that serum sodium was negatively correlated with MACE, which indicated that the lower the serum sodium level, the more likely MACE occur in elderly acute heart failure patients with preserved ejection fraction. This is due to sodium is a key substance in the systolic and diastolic regulation of cardiomyocytes, and a decrease in sodium concentration will aggravate heart failure.21 Through multifactor regression analysis, we found that serum sodium was an independent risk factor for the occurrence of MACE at 30 days. Further ROC analysis showed that when serum sodium was less than or equal to 140.35 mmol/l, it had strong sensitivity and positive predictive value for predicting the occurrence of MACE at 30 days. Therefore, serum sodium has a good predictive value for the short-term prognosis of acute heart failure in the elderly with preserved ejection fraction.
Based on the above research, we further combined Hb/RDW with serum sodium to perform ROC analysis, in order to observe whether the combined index had better predictive value than the single index. Therefore, the following results were obtained: the AUC of the combined index for predicting the occurrence of MACE was 0.83, the sensitivity was 90.90%, the specificity was 78.20%, the PPV was 27.80%, and the NPV was 98.90%. All were significantly higher than the single-indicator projection. Therefore, the application of combined indexes to predict the short-term prognosis of acute heart failure with preserved ejection fraction in the elderly has better sensitivity, specificity and positive predictive value.
In addition, coronary artery disease is the basis of heart failure, and the number of coronary artery disease was significantly higher in the MACE group than in the non-mace group, which consistented with previous studies. But all the patients with previous history of coronary artery diseases are subjected to corresponding treatment with no statistical difference in terms of the medication and the patients in both groups were stabilized.
Our experiment had shortcomings, First, this was a pilot study, and our sample size was limited. A larger sample size study will be needed to validate our results. Second, in our study, we only observed the value of Hb/RDW and serum sodium in predicting short-term prognosis at 30 days. Therefore, we need to investigate Hb/RDW and serum sodium in relation to long-term prognosis in the future.
In summary, due to Hb, RDW, and serum sodium play an important role in the development and progression of acute heart failure with preserved ejection fraction, combination of Hb/RDW and serum sodium can be used to assess the prognosis of acute heart failure in the elderly with preserved ejection fraction from different dimensions. Meanwhile, serum sodium, Hb, and RDW are routine clinical indicators, which are obtained conveniently and fastly. Therefore, combination Hb/RDW, serum sodium can be used as an effective indicator to assess the occurrence of MACE at 30 days after discharge in acute heart failure patients with preserved ejection fraction in the elderly.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki, and the samples were approved by the ethics committee of Hebei General Hospital (K-2021-1163). The written informed consent was obtained from each patient and their family for clinical data and publication.
Consent for Publication
The subjects provided written informed consent for publication of any associated data and accompanying images.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. Simmonds SJ, Cuijpers I, Heymans S, Jones EAV. Cellular and molecular differences between HFpEF and HFrEF: a step ahead in an improved pathological understanding. Cells. 2020;9(1):242. doi:10.3390/cells9010242
2. Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528. doi:10.1161/cir.0000000000000659
3. Song J, Yu T, Yan Q, Zhang Q, Wang L. Association of Hemoglobin to red blood cell distribution width-standard deviation (RDW-SD) ratio and 3-month readmission in elderly Chinese patients with heart failure: a retrospective cohort Study. Int J Gene Med. 2023;16:303–315. doi:10.2147/ijgm.S396805
4. Donzé JD, Beeler PE, Bates DW. Impact of hyponatremia correction on the risk for 30-Day Readmission and death in patients with congestive heart failure. Am j Med. 2016;129(8):836–842. doi:10.1016/j.amjmed.2016.02.036
5. De Vecchis R, Di Maio M, Di Biase G, Ariano C. Effects of hyponatremia normalization on the short-term mortality and rehospitalizations in patients with recent acute decompensated heart failure: a retrospective study. J Clin Med. 2016;5:1.
6. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Rev esp cardiologia. 2022;75(6):523. doi:10.1016/j.rec.2022.05.005
7. Wei N, Sun D, Huang W. Effects of WeChat use on the subjective health of older adults. Frontiers in Psychology. 2022;13:919889. doi:10.3389/fpsyg.2022.919889
8. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Euro J Heart Fail. 2012;14(8):803–869. doi:10.1093/eurjhf/hfs105
9. Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46–e215. doi:10.1161/circulationaha.109.192667
10. Mebazaa A, Yilmaz MB, Levy P, et al. Recommendations on pre-hospital and early hospital management of acute heart failure: a consensus paper from the heart failure association of the European society of cardiology, the European society of emergency medicine and the society of academic emergency medicine--short version. Eur Heart J. 2015;36(30):1958–1966. doi:10.1093/eurheartj/ehv066
11. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymański P. Anisocytosis predicts postoperative renal replacement therapy in patients undergoing heart valve surgery. Cardiol j. 2020;27(4):362–367. doi:10.5603/CJ.a2019.0020
12. Sun P, Zhang F, Chen C, et al. The ratio of hemoglobin to red cell distribution width as a novel prognostic parameter in esophageal squamous cell carcinoma: a retrospective study from southern China. Oncotarget. 2016;7(27):42650–42660. doi:10.18632/oncotarget.9516
13. Qu J, Zhou T, Xue M, et al. Correlation analysis of hemoglobin-to-red blood cell distribution width ratio and frailty in elderly patients with coronary heart disease. Front Cardiovasc Med. 2021;8:728800. doi:10.3389/fcvm.2021.728800
14. Abebe TB, Gebreyohannes EA, Bhagavathula AS, Tefera YG, Abegaz TM. Anemia in severe heart failure patients: does it predict prognosis? BMC Cardiovasc Disorder. 2017;17(1):248. doi:10.1186/s12872-017-0680-5
15. Reck M, Rabe KF. Precision Diagnosis and Treatment for Advanced Non-Small-Cell Lung Cancer. New Engl J Med. 2017;377(9):849–861. doi:10.1056/NEJMra1703413
16. Breen T, Brueske B, Sidhu MS, et al. Abnormal serum sodium is associated with increased mortality among unselected cardiac intensive care unit patients. J Am Heart Assoc. 2020;9(2):e014140. doi:10.1161/jaha.119.014140
17. Cavusoglu Y, Kaya H, Eraslan S, Yilmaz MB. Hyponatremia is associated with occurrence of atrial fibrillation in outpatients with heart failure and reduced ejection fraction. Hellenic J Cardiol. 2019;60(2):117–121. doi:10.1016/j.hjc.2018.03.006
18. Patel YR, Kurgansky KE, Imran TF, et al. Prognostic significance of baseline serum sodium in heart failure with preserved ejection fraction. J Am Heart Assoc. 2018;7:12. doi:10.1161/JAHA.117.007529
19. Matsue Y, Yoshioka K, Suzuki M, et al. Prognostic importance of sodium level trajectory in acute heart failure. Heart Vess. 2017;32(12):1498–1505. doi:10.1007/s00380-017-1020-5
20. Davison BA, Metra M, Senger S, et al. Patient journey after admission for acute heart failure: length of stay, 30-day readmission and 90-day mortality. Euro J Heart Fail. 2016;18(8):1041–1050. doi:10.1002/ejhf.540
21. Verbree-Willemsen L, Zhang YN, Ibrahim I, et al. Extracellular vesicle Cystatin C and CD14 are associated with both renal dysfunction and heart failure. ESC Heart Fail. 2020;7(5):2240–2249. doi:10.1002/ehf2.12699
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum sST2, IL-33, and Hcy Expression in Older Adults Patients with Myocardial Infarction and Their Predictive Value for MACE
Zheng LC, Liu F, Zheng PM, Xiao Z, Cui FC
Clinical Interventions in Aging 2025, 20:495-504
Published Date: 25 April 2025