")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
The Prediction of Surgery Outcomes in Abdominal Tumor Patients with Sepsis by Pcv-aCO2/Ca-cvO2
Authors Lyu Y, Han T, Liu M, Cui K, Wang D
Received 13 May 2022
Accepted for publication 13 September 2022
Published 7 October 2022 Volume 2022:18 Pages 989—997
DOI https://doi.org/10.2147/TCRM.S374414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Yang Lyu,1,* Tao Han,1,* Meirong Liu,2 Keliang Cui,1 Donghao Wang1
1Department of Intensive Care Unit, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, Tianjin, People’s Republic of China; 2Department of Infectious Diseases, Tianjin Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Donghao Wang, Department of Intensive Care Unit, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, West Huan-Hu Rd, Ti Yuan Bei, Hexi District, Tianjin, 300060, People’s Republic of China, Email [email protected]
Background: To determine whether Pcv-aCO2/Ca-cvO2 combined with Pcv-aCO2 could predict the outcomes in patients complicated with abdominal infection and sepsis after abdominal tumor operation.
Methods: Total 92 patients admitted to our hospital from January 2017 to December 2020 who underwent abdominal tumor operation were enrolled. Blood gas analysis of artery and central vein, various laboratory indexes, SOFA score, hemodynamic parameters at different time points and treatment outcome were recorded.
Results: ROC curve analysis showed that hemodynamic parameter alone could not predict ICU treatment outcome and mortality of patients, but 72-hour SOFA score could predict treatment outcome of patients (AUC = 0.930, 95% CI: 0.803– 1.000, p = 0.019). The significant hemodynamic parameter for evaluating treatment outcome and prognosis of patients was Pcv-aCO2 + Ratio of T3. Kaplan–Meier univariate survival curve and Log-rank suggested that patients who had higher combined predictive parameter of T3 Ratio + T3 Pcv-aCO2 still had ischemia and hypoxia of tissues and organs after standard fluid resuscitation, and treatment outcome was not good. In subgroup analysis, patients with higher Ratio had higher lactate, higher T72 SOFA score, and poor treatment outcome.
Conclusion: The combination of Ratio and Pcv-aCO2 could evaluate clinical treatment outcome of patients complicated with abdominal infection and sepsis after abdominal tumor operation.
Keywords: ratio, Pcv-aCO2, Ca-cvO2, sepsis, hemodynamic, abdominal tumor
Introduction
Abdominal tumors include gastric cancer, cardia cancer, colorectal cancer, hepatobiliary and pancreatic tumors, and retroperitoneal tumors. In China, the incidence of gastric cancer is high, accounting for about 50% morbidity and mortality of cases worldwide.1 Another example is pancreatic bile duct tumor, which has severe operation trauma, long operation time and poor prognosis. Surgical resection is still the first choice for abdominal tumors in China. However, most abdominal tumors invade the digestive tract, so patients are often accompanied with gastrointestinal dysfunction, insufficient intake, poor nutritional status, low immune function. Recently, gut microbiota has become an important factor in clinical oncology.2,3 Gastrointestinal tract invasion, destruction of gastrointestinal immune barrier, disorder of gut microbiota and trauma of operation itself may lead to abdominal infection and sepsis with abnormal hemodynamics after operation. The basic task of intensive care unit (ICU) is to ensure stable hemodynamic of patients, improve oxygen delivery of tissues and organs, and further improve oxygen metabolism of tissues and even cells.4
At present, in the early stage of fluid resuscitation, central venous oxygen saturation (ScvO2), lactate clearance rate (LCR), Pcv-aCO2 and other hemodynamic parameters have been widely used in clinical treatment. However, all the parameters have limitations, because after normalization of macro hemodynamic parameters and antibiotics treatment, microcirculation damage still affects capillary permeability and leukocyte endothelial interaction, and is considered to be an important factor of organ damage.5,6 Significantly higher ScvO2 than normal range can increase the mortality of patients with septic shock.7 Pcv-aCO2 might be used as an independent parameter to evaluate the effect of fluid resuscitation, and Pcv-aCO2 combined with ScvO2 can better evaluate tissue perfusion during fluid resuscitation than ScvO2 alone.8 However, for patients with severe sepsis and septic shock, Pcv-CO2 can be in a normal range, but they have microcirculation disturbance, tissue ischemia and hypoperfusion.
Recently, we introduced Pcv-aCO2/Ca-cvO2 (Ratio) as a new parameter better than Pcv-aCO2 to detect sepsis with abnormal hemodynamics in patients with abdominal tumor after operation.9,10 In this study, we aimed to determine whether Pcv-aCO2/Ca-cvO2 combined with Pcv-aCO2 could predict the outcomes in patients complicated with abdominal infection and sepsis after abdominal tumor operation.
Materials and Methods
Patients
This was a retrospective study on patients admitted to Tianjin Medical University Cancer Institute and Hospital from January 2017 to December 2020 who underwent abdominal tumor operation. There were 92 hospitalized patients with sepsis and hemodynamic abnormalities after operation, including 61 males and 31 females, with an average age of 63.19 ± 10.81 years for males and 66.90 ± 11.48 years for females (t = −1.536, P = 0.128). This study was approved by the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital (Approval No. bc2016032, date 2016 March).
Inclusion criteria were: Sequential Organ Failure Assessment (SOFA) score >2; complicated with hemodynamic abnormalities after operation: systolic blood pressure <90 mmHg, or lower than baseline blood pressure >40 mmHg, pulse pressure <20 mmHg, urine volume <0.5 mL/kg / Hr, heart rate >100 times/min, Central Venous Pressure (CVP) <5 mmHg, blood lactic acid >2.7 mmol/L, ScvO2 <60%; diagnosis of abdominal infection accompanied with abdominal symptoms (abdominal distension, abdominal pain, bowel sounds weakened or disappeared, tenderness, rebound pain), accompanied by increased white blood cell/procalcitonin or pathogenic microorganisms in abdominal drainage fluid culture. Exclusion criteria were: Age <18 years old; patients with unimproved respiratory disease or chronic obstructive pulmonary disease with Forced expiratory volume in one second (FEV1) <0.50; patients after lobectomy and pneumonectomy; death/abandon treatment within 24 hours after transfer to ICU.
Measures and End Points
Vital signs and hemodynamic parameters, arterial and central venous blood gas analysis parameters at different time points, urine volume per hour, CVP, hemoglobin, serum creatinine, total bilirubin, platelet count, blood lactic acid and Glasgow Coma Score (GCS) were detected. All patients were treated according to 2016 international guidelines for Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016.11 Intravenous fluid, vasoactive drugs, inotropic drugs and red blood cells were used for bundle treatment. The standard of 6-hour Early Goal Directed Therapy (EGDT) was taken as the end point: MAP ≥ 65 mmhg, CVP 8–12 mmhg, urine volume ≥0.5 mL/kg/hr, ScvO2 ≥70%.
The following hemodynamic parameters were recorded at different time points: before fluid resuscitation as T0, after 3 hours of fluid resuscitation beginning as T3, after 6 hours of fluid resuscitation beginning as T6. Meanwhile, the SOFA score before and after 72 hours of treatment was recorded as T0SOFA and T72 SOFA.
Pcv-aCO2, CaO2, CcvO2, Pcv-aCO2 / Ca-cvO2 (Ratio) and 6-hour lactate clearance rate (LCR) were calculated at respective time point; SOFA score was evaluated before treatment and 72 hours after treatment; ICU admission length (days) and ICU treatment outcome (survival, death or automatic abandon treatment) were recorded.
The calculation formula was as follows:
·CaO2=(1.34×SaO2×Hb)+(0.003×PaO2)
·CcvO2=(1.34×ScvO2×Hb)+(0.003×PcvO2)
·Ca-cvO2=CaO2-CcvO2
·Pcv-aCO2=PcvCO2-PaCO2
·Ratio=Pcv-aCO2/Ca-cvO2
Statistical Analysis
SPSS20.0 statistical software was used for data analysis. The measurement data were expressed as mean ± standard deviation (x ± sd). The t-test was used to compare data with normal distribution; the measurement data of non normal distribution were expressed as median (upper and lower quartiles), and the Mann–Whitney U-test or Wilcoxon rank test was used for comparison; the count data were expressed as percentage or rate, and compared by chi-square test or Fisher’s exact test. ROC curve was used to evaluate predictive value of various hemodynamic parameters for treatment outcome. Kaplan–Meier method was used to draw survival curve, Log Rank test was used to compare survival curve between groups, and Cox Regression analysis was used to test predictive value of each parameter for survival. P < 0.05 indicated statistical significance.
Results
Primary Tumors and Etiological results of Enrolled Patients
The primary tumor sites of all patients enrolled in this study are summarized in Table 1. The etiological results of the abdominal drainage fluid were as follows: 5 cases of Morganella morganii ssp morganii (3 cases improved; 2 cases died/abandon treatment, same as followed); 1 case of pharyngeal streptococcus (1/0); 6 cases of Enterobacter Cloacae (6/0); 2 cases of Streptococcus mitis (2/0); 2 cases of Staphylococcus haemolyticus (2/0); 2 cases of Acinetobacter Baumannii (2/0); 1 case of Stenotrophomonas maltophilia (0/1); 1 case of Stephanoascus ciferrii (1/0); 4 cases of Enterococcus faecium (Group D) (4/0); 4 cases of Candida albicans (3/1); 11 cases of Klebsiella pneumoniae ssp pneumoniae (10/1); 1 case of Candida glabrata (1/0); 1 case of Shewanella alga (1/0); 1 case of Staphylococcus epidermidis (0/1); 1 case of Serratia marcescens (1/0); 1 case of Streptococcus oralis (1/0); 1 case of Aeromonas sobria (1/0); 1 case of Cryptococcus laurentii (1/0) and 1 case of Staphylococcus hominis (1/0). In addition, the clinical diagnosis of abdominal infection was established comprehensively, but no pathogenic evidence was found in 22 cases (20/2). It should be pointed out that some patients were infected with mixed bacteria; and some patients were clinically diagnosed with abdominal infection, and were given antibiotics as preemptive therapy, their clinical manifestations were significantly improved, and the infection parameters of laboratory examination tended to be normal.
 |
Table 1 Comparison of Primary Tumor of Enrolled Patients |
Comparison of Hemodynamic Parameters Before and After Treatment
We performed routine fluid resuscitation treatment for all patients enrolled, and recorded various related hemodynamic parameters MAP, CVP, ScvO2, lactic acid, 6-hour LCR (Table 2). MAP, CVP and ScvO2 after fluid resuscitation treatment at T6 of all patients reached standard of EGDT basically, and even LCR, Pcv-aCO2 and other hemodynamic parameters reached standard (LCR > 15%, Pcv-aCO2 ≤6 mmHg). The Wilcoxon rank test showed that the comparison of lactate (T0 vs T6) in different time periods was Z = - 4.001, P < 0.001. However, 12 of 92 patients died or abandoned treatment, and the treatment failure rate was 13.04% (12/92).
 |
Table 2 Comparison of Hemodynamic Parameters of Patients Before and After Treatment |
The Significance of Different Hemodynamic Parameters on the Prognosis of Patients
According to hemodynamic parameters of T0, T3 and T6, including lactate, ScvO2, Pcv-aCO2, Ratio, 6-hour LCR, and SOFA score before treatment (T0SOFA) and 72 hours after treatment (T72SOFA), we predicted treatment outcome of enrolled patients (Table 3). We found that T72SOFA score could better predict the treatment outcome of patients (AUC = 0.930, 95% CI: 0.803~1.000, P = 0.019).
 |
Table 3 Prediction on Treatment Outcome of Enrolled Patients by T0, T3 and T6 Parameters and SOFA Score |
T0, T3, T6 Lactate, ScvO2, Pcv-aCO2, Ratio and T0, T72SOFA were substituted into multivariate Cox regression model analysis (Table 4). During 6-hour period of fluid resuscitation, no single parameter was an independent factor of treatment outcome and mortality of patients. Only 72 hours of SOFA score could be used as an independent factor of treatment outcome for patients with sepsis and abnormal hemodynamics after abdominal tumor operation. However, the SOFA score after 72 hours of treatment might lag behind for severe patients. After early fluid resuscitation for 6 hours, although MAP, CVP, ScvO2 and even LCR reached the EGDT standard, and Pcv-aCO2 and other hemodynamic parameters reached standard (LCR >15%, Pcv-aCO2 ≤6 mmhg), there were still treatment failure cases. Therefore, we need to use more hemodynamic parameters or even combine multiple parameters to predict therapy effect.
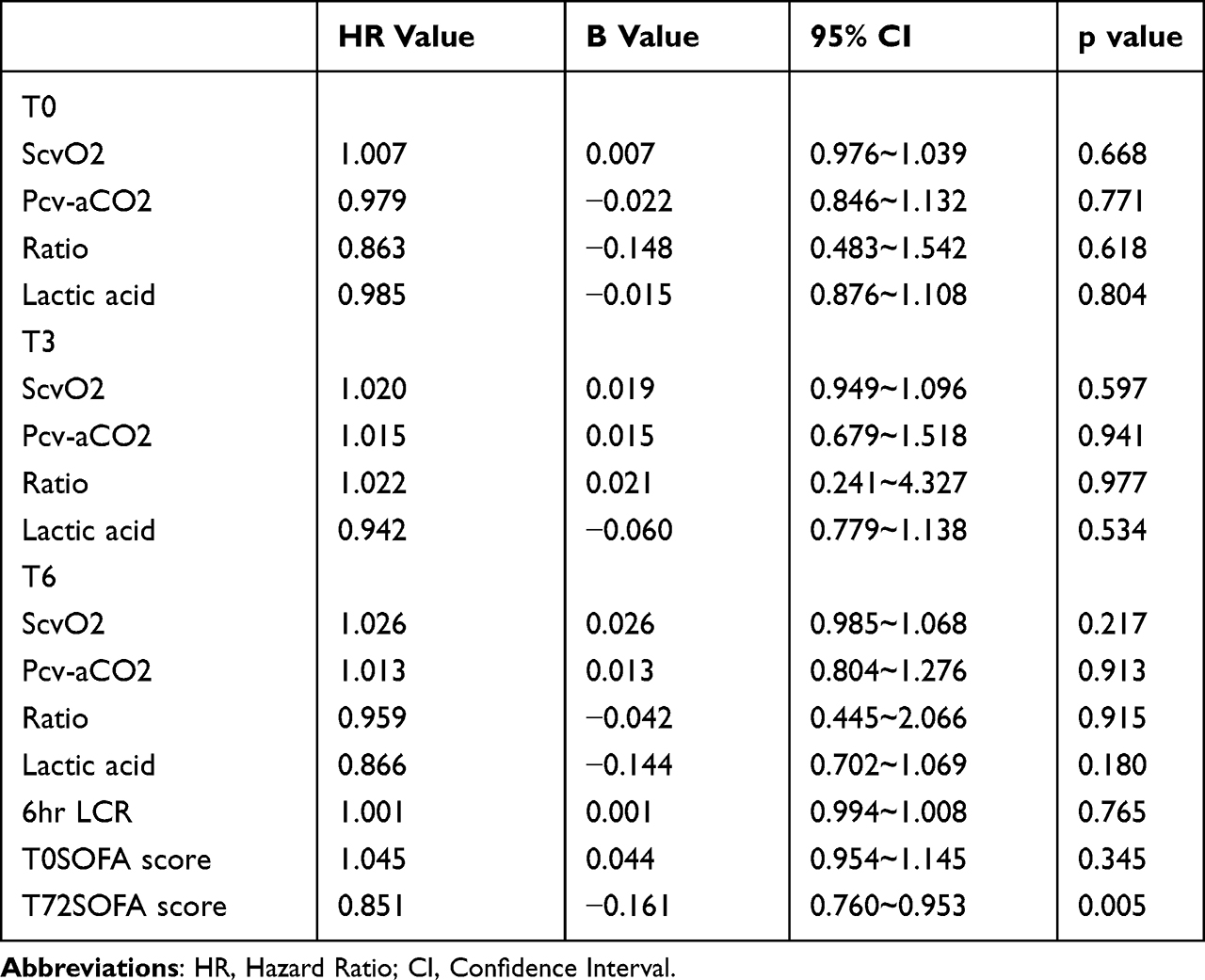 |
Table 4 Survival Prediction of Patients with Different Indicators by Multivariate Cox Regression Model Analysis |
We integrated Pcv-aCO2 and Ratio at T0, T3 and T6 time points utilizing a binary Logistic regression model, and combined with T72sofa for ROC analysis (Figure 1 and Table 5). The results showed that the most significant hemodynamic parameter to evaluate treatment effect and prognosis of patients was Pcv-aCO2 + Ratio of T3 point. Therefore, we selected T3 Pcv-aCO2 + T3Ratio as hemodynamic parameter to predict therapeutic effect of fluid resuscitation in patients with abdominal infection complicated with sepsis. The ROC curve of combined predictive probability at T3 time point showed that the cutoff point was 0.15188789, and T3 combined predictive probability was segmented into two group (<=cutoff point vs > cutoff point).
 |
Table 5 ROC Analysis of Pcv-aCO2 and Ratio at T0, T3 and T6 |
 |
Figure 1 ROC analysis of Pcv-aCO2 and Ratio at T0, T3 and T6 time points based on binary Logistic regression model. AUC of T3 combined prediction probability parameter was the highest (AUC = 0.798, P = 0.005) except for T72 SOFA. |
Influence of Hemodynamic Parameters on Treatment Outcome of Enrolled Patients
We recorded the length in ICU admission and therapy outcome of all enrolled patients after fluid resuscitation and performed univariate Kaplan–Meier survival analysis (Figure 2).
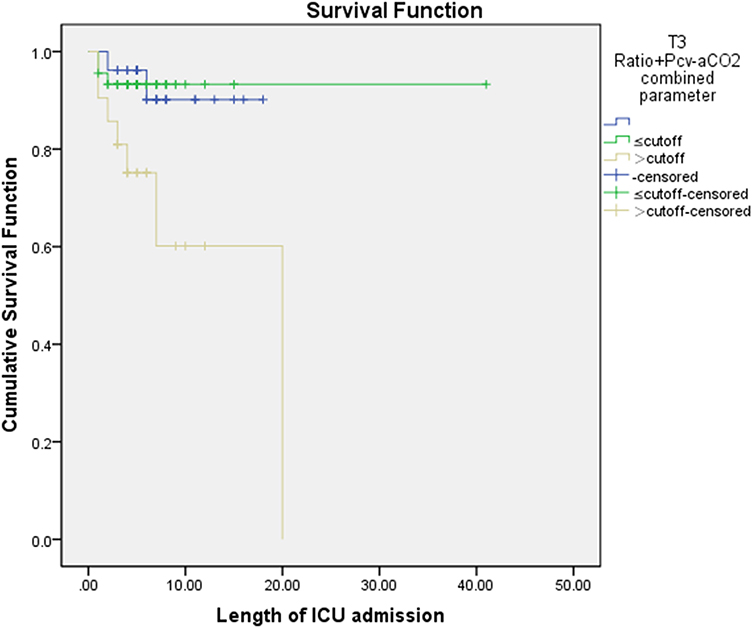 |
Figure 2 Kaplan-Meier survival analysis of patients after fluid resuscitation treatment. Patients with higher than combined predictive probability of T3Ratio + T3Pcv-aCO2 had ischemia and hypoxia of tissues and organs after standard fluid resuscitation, and treatment outcome was poor (chi-square value was 8.487, p = 0.014). |
Kaplan–Meier univariate survival curve was drawn for related hemodynamic parameters, and Log-rank was used to test treatment outcomes between two groups. Patients with a higher predictive probability of T3Ratio + T3Pcv-aCO2 had ischemia and hypoxia after standard fluid resuscitation, and treatment outcome was poor. The best cutoff point of T3Ratio = 1.12 (Sensitivity: 0.700, Specificity: 0.696), and we then used Pcv-aCO2 = 6 mmhg combined with Ratio = 1.12 to refine sub-grouping.
Retrospective Analysis Based on T6Ratio and T6Pcv-aCO2
We further evaluated the role of Ratio and Pcv-aCO2 in the survival of patients with acute hemodynamic abnormalities and fluid resuscitation after abdominal tumor operation complicated with abdominal infection and sepsis. We divided patients into four subgroups: Group1 (Ratio ≤ 1.12 + Pcv-aCO2 ≤ 6 mmhg), Group2 (Ratio > 1.12 + Pcv-aCO2 ≤ 6 mmhg), Group3 (Ratio ≤ 1.12 + Pcv-aCO2 > 6 mmhg), Group4 (Ratio > 1.12 + Pcv-aCO2 > 6 mmhg) (Table 6). We compared MAP, CVP, ScvO2 and lactic acid in four groups. The lactic acid of G2 was higher than that of G1 (t = - 2.193, p = 0.038). For 72 hour SOFA score and length in ICU admission, only G1 patients had lower 72 hour SOFA score than G2 patients (p = 0.019). For treatment outcome, three groups had different treatment outcomes (chi-square value: 9.158, P = 0.010), only G1 patients had better treatment outcome than G2 patients (p = 0.008). Patients with higher Ratio had higher lactate, higher 72 hour SOFA score and poor treatment outcome. However, the outcome of G4 was similar to that of G1, but the success rate of G1 was higher than that of G4.
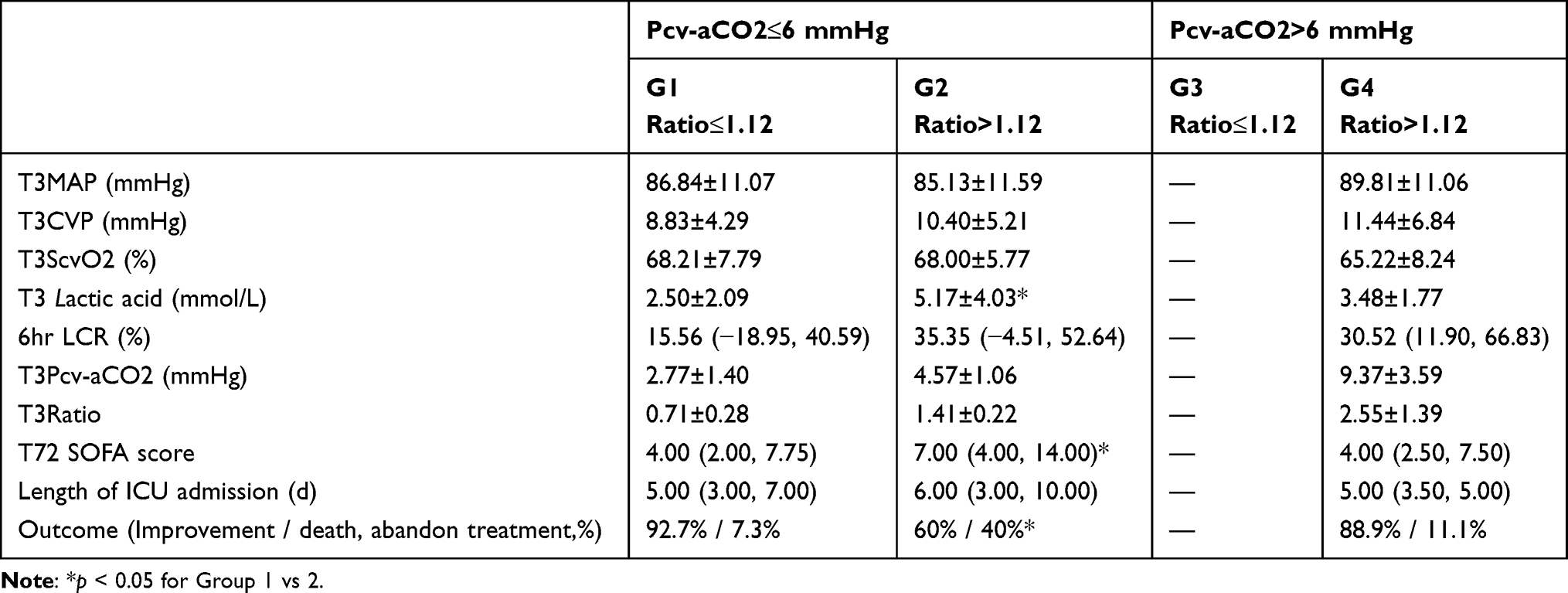 |
Table 6 Comparison of Treatment Efficacy and Survival of Patients with Different Hemodynamic Parameters |
Discussion
Sepsis is a common complication after tumor operation with high mortality.12 Abdominal operation leads to large trauma and high risk of postoperative infection and gastrointestinal dysfunction, which can rapidly progress to sepsis with hemodynamic disorder, circulatory and respiratory failure and multiple organ dysfunctions with high mortality.13 Recent studies suggest fluid therapy for the complication after abdominal operation.14 This study focused on patients with sepsis and hemodynamic instability after abdominal tumor operation, and identified the parameters to predict the effect of early fluid resuscitation.
We found that Ratio combined with Pcv-aCO2 was a key factor to evaluate clinical efficacy of fluid resuscitation in patients with abnormal hemodynamics. Patients with Ratio ≤ 1.12 and Pcv-aCO2 ≤ 6 mmhg had better fluid resuscitation efficacy and better survival outcome.
Hemodynamic abnormalities combined with severe sepsis and septic shock are common causes of death in critically ill patients.15,16 At present, hemodynamic parameters of fluid resuscitation include EGDT, lactate and LCR, which are widely used to evaluate the efficacy of fluid resuscitation. However, each parameter has its limitation and is affected by other factors.17,18 In addition, Pcv-aCO2 was reported to show no relationship with poor prognosis of patients with sepsis.19 Mekontso-Dessap et al found that prediction ability of Pv-cCO2/Da-vO2 for hyperlactemia was significantly better than that of Pv-aCO2 and SvO2 in critically ill patients.9 Therefore, we introduced Pcv-aCO2/Ca-cvO2 (Ratio) combined with Pcv-aCO2 to evaluate therapeutic effect and prognosis of early fluid resuscitation in patients with sepsis and abnormal hemodynamics.
In this study, 92 patients with abdominal tumor complicated with abdominal infection, sepsis and hemodynamic disorders were included. We performed standard fluid resuscitation for all patients, and introduced T3 and T6 Ratio after resuscitation as one of hemodynamic parameters to evaluate the efficacy of fluid resuscitation. However, we integrated hemodynamic parameters of T0, T3 and T6, including lactate, ScvO2, Pcv-aCO2, Ratio, and 6-hour LCR, and T0 and T72 SOFA scores before treatment (T0) and 72 hours after treatment (T72) into ROC curve, and only T72 SOFA score could be used as a predictor parameter. Furthermore, by multivariate Cox regression model analysis only T72 SOFA score could be used as an independent factor of treatment outcome for patients receiving fluid resuscitation after abdominal tumor operation. Based on the concept of early diagnosis and early prediction, we need to identify the parameters to predict treatment success or failure in a period of 6-hours fluid resuscitation. Kaplan–Meier survival curve showed that T3 combined prediction probability could predict the efficacy of fluid resuscitation and prognosis.
Next, the patients were divided into four groups according to Pcv-aCO2 and Ratio, and hemodynamic parameters and prognosis at different time points were compared. We found that the outcome of patients with Ratio <= 1.12 and Pcv-aCO2 <= 6 mmHg was better. Unfortunately, we found no differences in treatment outcome and SOFA score between patients whose Ratio + Pcv-aCO2 were not up to standard and up to standard, which might be related to small number of patients in subgroup. Therefore, we need to expand the sample size for the comparison. Consistent with our findings, Monnet et al reported that P (v-a) CO2 / C (a-v) O2 value and plasma lactic acid concentration had guiding significance in fluid resuscitation of shock patients, with advantages of quick response to hypoxia and few influencing factors.20
This study has several limitations. First, as we mentioned above the sample size of this study is relatively small. Second, this study is a retrospective study. Third, we did not identify the risk factors for developing sepsis in patients with abdominal tumor. Recent studies reported that in colorectal cancer patients, postoperative sepsis was significantly more common among patients over 65 years old, with ASA score >2, and with associated comorbidities such as diabetes and cardiovascular disease.21,22
In conclusion, we evaluated the role of Ratio and Pcv-aCO2 in the survival of patients with acute hemodynamic abnormalities and fluid resuscitation after abdominal tumor operation complicated with abdominal infection and sepsis. Our results suggest that in early stage of sepsis with abnormal hemodynamics, the combination of Ratio and Pcv-aCO2 could better evaluate hemodynamic status and clinical treatment outcome of patients.
Data Sharing Statement
All data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital. All patients provided written informed consent. All patients were treated according to 2016 international guidelines for Surviving Sepsis Campaign:
International Guidelines for Management of Sepsis and Septic Shock:2016.
Funding
This study was funded by Tianjin Key Medical Discipline (Specialty) Construction Project.
Disclosure
Tao Han and Yang Lyu are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
2. Murphy CL, O’Toole PW, Shanahan F. The gut microbiota in causation, detection, and treatment of cancer. Am J Gastroenterol. 2019;114(7):1036–1042. doi:10.14309/ajg.0000000000000075
3. Meng C, Bai C, Brown TD, Hood LE, Tian Q. Human gut microbiota and gastrointestinal cancer. Genomics Proteomics Bioinformatics. 2018;16(1):33–49. doi:10.1016/j.gpb.2017.06.002
4. Saugel B, Flick M, Bendjelid K, Critchley LAH, Vistisen ST, Scheeren TWL. Journal of clinical monitoring and computing end of year summary 2018: hemodynamic monitoring and management. J Clin Monit Comput. 2019;33(2):211–222. doi:10.1007/s10877-019-00297-w
5. Baudry N, Starck J, Aussel C, et al. Effect of preconditioned mesenchymal stromal cells on early microvascular disturbance in a mouse sepsis model. Stem Cells Dev. 2019;28(24):1595–1606. doi:10.1089/scd.2019.0134
6. Su H, Li K, Liu X, et al. Microfluidic chips for the endothelial biomechanics and mechanobiology of the vascular system. Biocell. 2021;45(4):797–811. doi:10.32604/biocell.2021.014900
7. Xantus G, Kiss B, Molnar G, Matheson C, Gyarmathy VA, Kanizsai PL. Lactate reloaded–reevaluation of the importance of lactate monitoring in the management of adult sepsis in the emergency department. Biocell. 2021;45(3):445–449. doi:10.32604/biocell.2021.014754
8. Mallat J, Pepy F, Lemyze M, et al. Central venous-to-arterial carbon dioxide partial pressure difference in early resuscitation from septic shock: a prospective observational study. Eur J Anaesthesiol. 2014;31(7):371–380. doi:10.1097/EJA.0000000000000064
9. Mekontso-Dessap A, Castelain V, Anguel N, et al. Combination of venoarterial PCO2 difference with arteriovenous O2 content difference to detect anaerobic metabolism in patients. Intensive Care Med. 2002;28:272–277. doi:10.1007/s00134-002-1215-8
10. Mesquida J, Saludes P, Pérez-Madrigal A, et al. Respiratory quotient estimations as additional prognostic tools in early septic shock. J Clin Monit Comput. 2018;32(6):1065–1072. doi:10.1007/s10877-018-0113-8
11. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
12. Rosolem MM, Rabello LS, Lisboa T, et al. Critically ill patients with cancer and sepsis: clinical course and prognostic factors. J Crit Care. 2012;27(3):301–307. doi:10.1016/j.jcrc.2011.06.014
13. Blot S, Antonelli M, Arvaniti K, et al.; Abdominal Sepsis Study (AbSeS) group on behalf of the Trials Group of the European Society of Intensive Care Medicine. Epidemiology of intra-abdominal infection and sepsis in critically ill patients: ”AbSeS”, a multinational observational cohort study and ESICM trials group project. Intensive Care Med. 2019;45(12):1703–1717. doi:10.1007/s00134-019-05819-3
14. Myles PS, Bellomo R, Corcoran T, et al. Australian and New Zealand college of anaesthetists clinical trials network and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Restrictive versus liberal fluid therapy for major abdominal surgery. N Engl J Med. 2018;378(24):2263–2274. doi:10.1056/NEJMoa1801601
15. Miller RR 3rd, Dong L, Nelson NC, et al. Intermountain healthcare intensive medicine clinical program. multicenter implementation of a severe sepsis and septic shock treatment bundle. Am J Respir Crit Care Med. 2013;188(1):77–82. doi:10.1164/rccm.201212-2199OC
16. Moreira H, Sinert R. How effective is the early management bundle for severe sepsis/septic shock? JAMA Intern Med. 2020;180(5):716–717. doi:10.1001/jamainternmed.2020.0180
17. Lipcsey M, Castegren M, Bellomo R. Hemodynamic management of septic shock. Minerva Anestesiol. 2015;81(11):1262–1272.
18. Zhang J, Luo W, Xiong J, Wang Y, Jia W, Han J. Ischemic postconditioning plays a protective role in brain through regulating autophagy by LncRNAs. Neuropsychiatric Sci Mol Biol. 2021;2:1–9.
19. Araujo DT, Felice VB, Meregalli AF, Friedman G. Value of central venous to arterial CO2 difference after early goal-directed therapy in septic shock patients. Indian J Crit Care Med. 2019;23(10):449–453. doi:10.5005/jp-journals-10071-23262
20. Monnet X, Julien F, Ait-Hamou N, et al. Lactate and venoarterial carbon dioxide difference/arterial-venous oxygen difference ratio, but not central venous oxygen saturation, predict increase in oxygen consumption in fluid responders. Crit Care Med. 2013;41(6):1412–1420. doi:10.1097/CCM.0b013e318275cece
21. Mulita F, Liolis E, Akinosoglou K, et al. Postoperative sepsis after colorectal surgery: a prospective single-center observational study and review of the literature. Prz Gastroenterol. 2022;17(1):47–51. doi:10.5114/pg.2021.106083
22. Kaplanis C, Tchabashvili L, Vailas M, Maroulis I. Risk of surgical site infections after colorectal surgery and the most frequent pathogens isolated: a prospective single-centre observational study. Med Glas. 2021;18(2):438–443. doi:10.17392/1348-21
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.