Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Practices of Public Hospital Registered Nurses Regarding Post-Stroke Dysphagia, in China
Authors Lu QY, Bu MR, Zhu Y, Huang ZY, Gao SH, Yuan C ![]()
Received 2 April 2025
Accepted for publication 24 July 2025
Published 4 August 2025 Volume 2025:18 Pages 4629—4641
DOI https://doi.org/10.2147/JMDH.S531891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Qing-Yi Lu,1,* Man-Rong Bu,1,* Yang Zhu,1 Zhi-Yu Huang,2 Shi-Hao Gao,1 Changyan Yuan1
1Department of Rehabilitation, Daping Hospital, Army Medical University, Chongqing, 40042, People’s Republic of China; 2Nursing Department, Daping Hospital, Army Medical University, Chongqing, 40042, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Changyan Yuan, Department of Rehabilitation, Daping Hospital, Army Medical University, No. 10, Changjiang Street, Yuzhong District, Chongqing, 40042, People’s Republic of China, Tel +86 023-68746185, Email [email protected] Shi-Hao Gao, Email [email protected]
Background: Dysphagia is one of the most common complications in post-stroke patients, post-stroke medical disease management (eg, thrombectomy procedures) do have a huge influence on the long-term outcomes, with frontline clinical nurses serving as pivotal gatekeepers for early identification and management in post-stroke dysphagia (PSD). However, nurses, especially those in low- and middle-income countries, generally lack the ability to manage PSD, and the current state of Chinese public hospital registered nurses’ relevant clinical practice remains unclear.
Purpose: This study aims to evaluate how registered nurses, on initial clinical contact, screen and manage post-stroke dysphagia. A multi-center descriptive cross-sectional design was utilized.
Participants and Methods: From March 2 to April 18, 2024, 1010 nurses from 14 provinces in China completed an online questionnaire through convenient sampling. After applying inclusion and exclusion criteria, 943 valid questionnaires were included in the final analysis—the self-reported questionnaire collected data on knowledge of dysphagia, attitude and practices. Data were analyzed using descriptive statistics. This study adhered to the STROBE checklist guidelines.
Results: The study involved 943 nurses, mostly from tertiary hospitals (71.05%) and stroke-related departments (68.93%). Only 2.86% were specialized dysphagia nurses. Dysphagia was identified using formal screening tools, with the 30-ml water swallowing test (87.8%) and repeated saliva swallowing test (77.2%) being most common. Screening was often conducted before the first intake of food, water, or medication (65.11%), and involved multiple personnel, including nurses (67.44%) and doctors (77.62%). Management strategies included nutritional support (83.46%), oral hygiene improvements (86.96%), rehabilitation exercises (86.96%), medication adjustments (75.4%), and referrals, primarily to doctors (71.58%), rehabilitation therapists (68.82%) and SLPs were referred after positive testing (44.54%).
Conclusion: This study reflects the current practices of Chinese nurses in screening and managing dysphagia, highlighting gaps between clinical practice and guidelines. The findings provide a theoretical foundation for policymakers to enhance training programs and workforce development, ultimately improving nursing practice quality.
Keywords: post-stroke dysphagia, nursing knowledge, nursing practice, cross-sectional study, China
Introduction
Stroke is the leading cause of death and disability worldwide, affecting approximately 13.7 million individuals annually.1 The prevalence of post-stroke dysphagia (PSD) varies widely, ranging from 8.1% to 80%, depending on factors like the stroke’s cause, patient age, environment, and the source of information.2 PSD can severely impact swallowing safety, leading to complications such as aspiration pneumonia, dehydration, and malnutrition.3 The World Health Organization recognizes PSD as a digestive system disability linked to increased morbidity, mortality, and health-care costs.4 Despite its significant impact on physical and mental health, many patients do not receive timely care, appropriate diagnosis, or effective interventions.5 Therefore, detecting and managing PSD is particularly important for preventing disease complications and reducing hospitalization time and socioeconomic burden.
Nurses, as the primary caregivers, have a crucial role in the identification and management of PSD.6,7 Studies have shown that specialized training in PSD improves nurses’ knowledge, comprehensive management skills, and clinical practice capabilities.8,9 Well-trained nurses can efficiently use screening tools, enhancing the accuracy and effectiveness of the screening process.10 Additionally, nurses can guide patients on food intake and texture modifications to ease swallowing difficulties and improve nutrition.11 They are also vital in optimizing oral drug administration, selecting suitable oral care routines, and implementing effective referral pathways.12–14 Prompt identification and intervention by nurses have a direct impact on patient outcomes.
In low- and middle-income countries (LMICs), stroke and its complications remain prevalent.15 Dysphagia, one of the most common and severe post-stroke complications, highlights the urgent need for comprehensive screening. In the Chinese Stroke Center Alliance, nearly 20% of patients did not receive timely and comprehensive dysphagia screening.16 Nurses often take on the responsibility of early PSD identification and management. If nurses screen for swallowing difficulties within 24 hours of admission, it may shorten the time for patients to lose nutrients and fluids, and increase good clinical outcomes for stroke patients. In addition, nurses should be able to provide advice to doctors and speech-language pathologists (SLPs) on dysphagia symptoms. However, research indicates that nurses in LMICs lack adequate knowledge and skills to effectively early identification and manage PSD.17–19 However, the status of nurses’ practices with post-stroke dysphagia is unclear. Thus, it is vital to assess the current state of nurses’ practices regarding PSD at diverse levels of hospitals in China to provide a theoretical foundation for training programs, improve nursing quality, and ensure patient safety. To this end, an online survey was conducted to describe how registered nurses: (1) screen and (2) manage persons with post-stroke dysphagia.
Materials and Methods
Study Participants and Methods
A convenience sampling method was used to recruit registered nurses from various health-care institutions across China. We searched the official WeChat account of the nursing management department of Chinese public hospitals via Baidu search engine, sent an invitation letter through the nursing department, obtained informed consent from the other party, and sent the questionnaire link to the nursing department through the Questionnaire Star platform. They distributed the link to the nurses and provided a guide for filling out the questionnaire, including explaining the research purpose, methods, content, significance, and filling methods to the participants, so that they could understand the questionnaire and complete it anonymously. Nurses were required to voluntarily participate in the study by filling out the consent form on the first electronic page and filling out the online questionnaire, which would be automatically submitted to the database. Participants meeting the following criteria were included in the study: (1) registered nurses working in Chinese health-care institutions and (2) subjects who were informed and agreed to participate. We excluded nurses employed by private health-care institutions because many guideline policies and specialty training programs operate primarily in public hospitals. After collecting questionnaires, we removed invalid responses including incomplete answers, identical answer patterns, repeated selection patterns, or responses not following the completion guidelines.
Study Instrument
A structured questionnaire was developed to gather data regarding general demographics information as well as the screening and management practices for dysphagia. The questionnaire comprised two main sections. The introductory section outlined the objectives, details, response guidelines, and confidentiality guarantees of the study to ensure participants’ uniform understanding of the questionnaire.
Demographic Information
Included eight items regarding hospital level, department, nurse title, work experience, education level, status as a dysphagia specialist nurse, training in dysphagia management, and awareness of dysphagia-related guidelines.
Dysphagia Screening and Management Practices
The survey assessed registered nurses’ current practices in screening and managing dysphagia, incorporating recommendations from clinical guidelines and expert consensus documents on dysphagia evaluation, screening, and management. We based on【Chinese Society of Rehabilitation Medicine Dysphagia Rehabilitation Specialty Committee. Guidelines for Dysphagia Rehabilitation Management in China (2023 Edition) [J]. Chinese Journal of Physical Medicine and Rehabilitation, 2023, 45(12):1057–1072. DOI: 10.3760/cma.j.issn.0254–1424.2023.12.001.】【Chinese Stroke Dysphagia and Nutrition Management Consensus Expert Group, Chinese Stroke Society, National Clinical Medical Research Center for Neurological Diseases, National Medical Quality Control Center for Neurological Diseases. Manual for Dysphagia and Nutrition Management in Chinese Stroke Patients [J]. Chinese Stroke Journal, 2019, 14(11):1153–1169. DOI: 10.3969/j.issn.1673–5765.2019.11.014. Chinese Society of Rehabilitation Medicine Rehabilitation Nursing Specialty Committee. Expert Consensus on Dysphagia Rehabilitation Nursing [J]. Journal of Nursing, 2021, 36(15):1–4. DOI:10.3870/j.issn.1001–4152.2021.15.001】. 【Rainer, Dziewas, Emilia et al. European Stroke Organisation and European Society for Swallowing Disorders guideline for the diagnosis and treatment of post-stroke dysphagia. [J]. European stroke journal, 2021, 6(3):LXXXIX-CXV. DOI:10.1177/23,969,873,211,039,721】. 【Cosentino G, Avenali M, Schindler A et al. A multinational consensus on dysphagia in Parkinson’s disease: screening, diagnosis and prognostic value. J Neurol. 2022 Mar; 269(3):1335–1352. doi: 10.1007/s00415-021-10,739-8. Epub 2021 Aug 21. PMID: 34417870; PMCID: PMC8857094】. 【Winstein CJ, Stein J, Arena R et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association [published correction appears in Stroke. 2017 Feb; 48(2):e78. doi: 10.1161/STR.0000000000000120.] [published correction appears in Stroke. 2017 Dec; 48(12):e369. doi: 10.1161/STR.0000000000000156.]. Stroke. 2016; 47(6):e98-e169. doi: 10.1161/STR.0000000000000098】【Teder K, Karjagin J, Antoniak KM, Saar M, Volmer D. Development of an Administration Guideline of Oral Medicines to Patients with Dysphagia. Medicina (Kaunas). 2023; 59(11):1913. Published 2023 Oct 29. doi: 10.3390/medicina59111913】et al.
The final questionnaire was reviewed and revised by three senior nursing experts with extensive experience in dysphagia research and clinical practice. All experts held senior nursing titles and had over 15 years of experience related to dysphagia care.
Then, we conducted a pilot study with the aim of pre-testing the questionnaire to determine if the questions and instructions were clear enough and if the participants understood them correctly. Thirteen respondents were recruited separately for simultaneous cognitive interviews, a pre-testing technique suitable for pilot studies in which participants were asked to complete questionnaires individually and comment on questions or request clarification in case of ambiguity, and these results and recommendations were used to modify the questionnaires to ensure optimal validity and reliability of the research tools.
Data Collection and Processing
The study received approval from the hospital ethics committee. The questionnaire was developed and distributed via an online survey platform called “Questionnaire Star”, which could be accessed via a link or quick response code. The survey was propagated by the hospital’s nursing departments across diverse digital conduits, such as WeChat, email, and QQ, to reach a wider audience. The number of participants match to hospital procedures was based on Kendall’s cross-sectional survey to calculate the sample size,20 as follows: N = independent variable x (5–10). Independent variables include demographic information (8 items), screening timing (5 items), and management of post-stroke swallowing disorders (10 items). Our study includes 23 variables; Therefore, the sample size should be N = 23 (5–10). Considering the possible invalid questionnaire rate, 138–276 participants are required to obtain sufficient data for analysis. A total of 1010 questionnaires were collected within the specified time, and after being included, 943 were included, with an effective response rate of 93.4%.
Before completing the survey, participants were required to read and agree to an informed consent statement. The survey was conducted anonymously, and all responses were automatically collected through the survey platform. Data collection lasted four weeks.
Upon survey completion, an automated screening process in SPSSAU was used to identify and eliminate invalid responses. Two researchers independently reviewed the data to manually exclude any remaining invalid questionnaires.
Statistical Analysis
Data were analyzed using SPSS 23.0. Categorical variables were presented as frequencies and percentages.
Ethical Statements
This study received approval from the Ethics Committee of the Army Characteristic Medical Center (approval number: YIRL (2023) No. 277). Obtaining informed consent from the hospital or department before distributing the questionnaire, then send the questionnaire link, which provides unified instructions to enable survey participants to understand the questionnaire. The first section of the questionnaire included an informed consent form, and participants provided consent by selecting “I agree” before proceeding. The survey was conducted anonymously, and only for research purposes, and the data obtained from the Questionnaire Star platform can only be accessed through secure access by researchers, ensuring that no personal information was disclosed.
Results
Participants Characteristics
The study fills a research gap in PSD screening and management practices among registered nurses in Chinese public hospitals. The results describe according to how registered nurses identify and manage dysphagia. Most nurses are from tertiary hospitals (71.05%), with 68.93% operating in stroke-specific clinical units. Workforce composition analysis revealed a preponderance of junior clinicians, though 47.72% possessed ≥5 years of clinical tenure. Educational attainment data indicated 81.76% held bachelor’s degree, while only 2.86% are swallowing specialist nurses. Although 65.54% reported completing formal dysphagia training modules, guideline awareness rates stagnated at 58.96%, suggesting potential knowledge-to-practice translation barriers. Details are presented in Table 1. Table 1: Participants’ general information (n = 943).
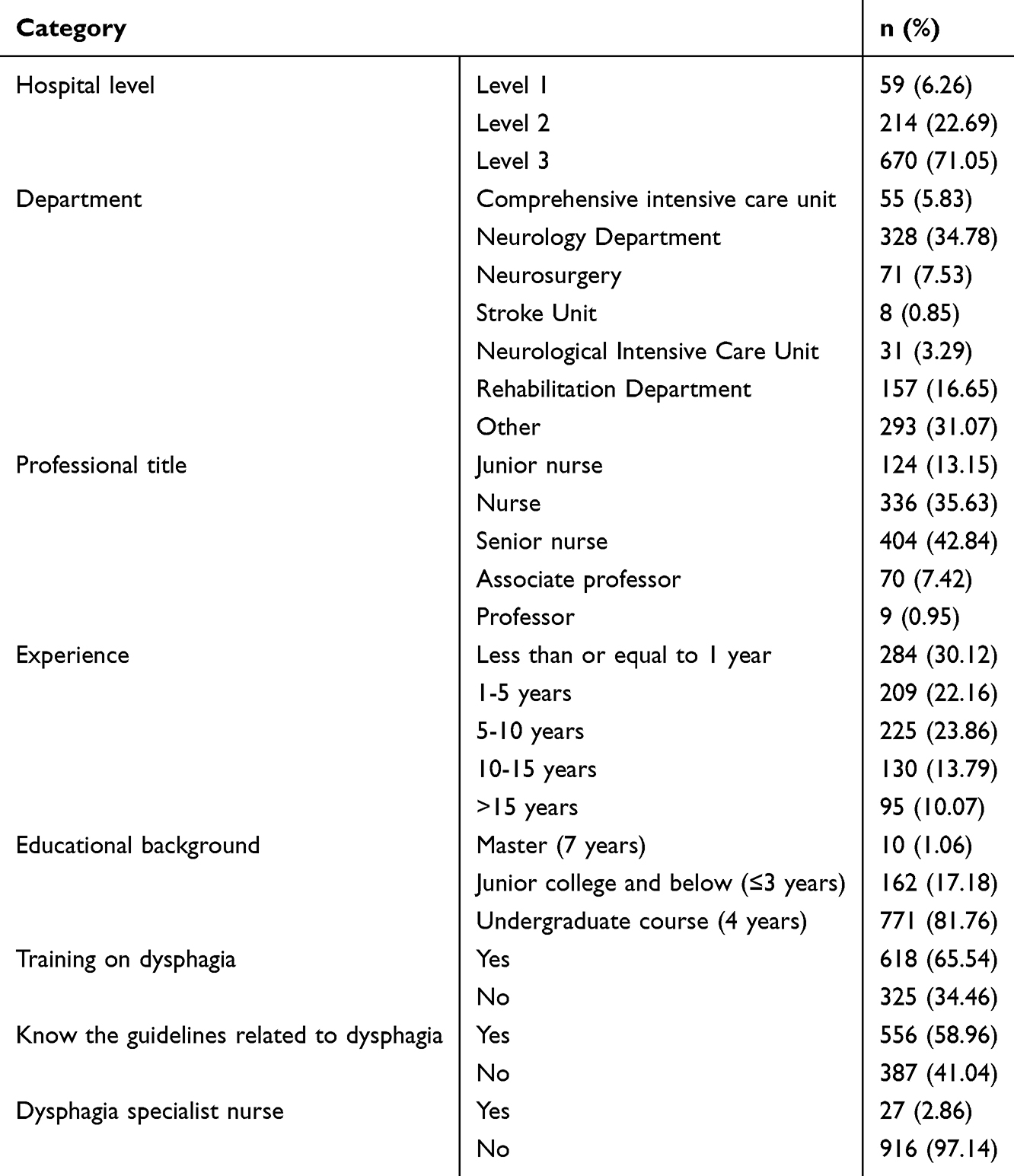 |
Table 1 Participants’ General Information (n = 943) |
Dysphagia Screen Contents
Registered nurses identify dysphagia through formal screening tools. However, there is variability in the timing of screening. Most nurses implement screening prior to screen patients before they take their first bite of food, water, or medicine. The screening criteria are not uniform, with the majority of nurses primarily targeting patients who report coughing and difficulty eating (94.35%), Minimum thresholds for other categories (8.42%). The most frequently used screening tool is the 30-ml water swallowing test (87.8%),21 Minimum thresholds for other categories (3.61%). Crucially, screening authority remained predominantly clinician-driven, with physicians conducting 77.6% of initial evaluations, Minimum thresholds for other categories (2.44%). Comprehensive screening matrices are presented in Figures 1 and 2.
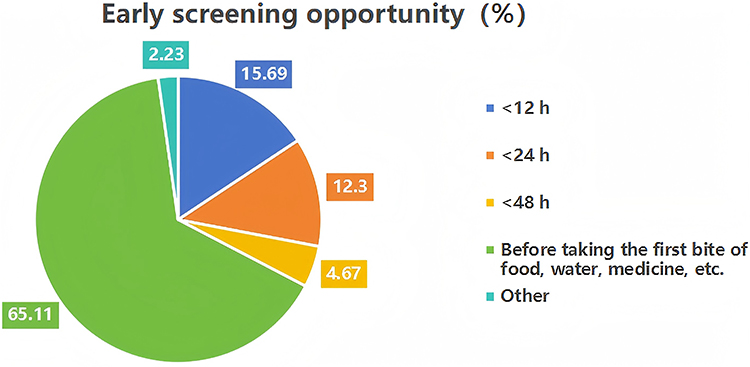 |
Figure 1 Timing of dysphagia screening (n = 943). |
 |
Figure 2 Dysphagia screen contents (n = 943). |
Dysphagia Management for PSD
The intervention measures encompass five key areas: nutrition, oropharyngeal hygiene, rehabilitation exercises, medication management, and referral. Over half of the nurses employ compensatory strategies such as using straws or syringes to administer oral liquids or food to patients, utilizing viscosity-modifying agents to densify liquids or food, offering rehabilitation techniques to patients, altering the form of medications, and 83.46% of nurses reported using IDDSI framework to modified texture food. Thereinto, the highest (87.91%) and lowest (58.96) intervention measures were “adjusting patient’s eating position (eg, sitting right, 45°−60° inch)” and “use of caring agents for liquids/foods”, respectively. Comprehensive details are cataloged in Table 2. In order to explore the factor impact the dysphagia management, we conducted univariate analysis of dysphagia screen and referral to further improve the results and get a better understanding of the data. Details in Tables 3 and 4.
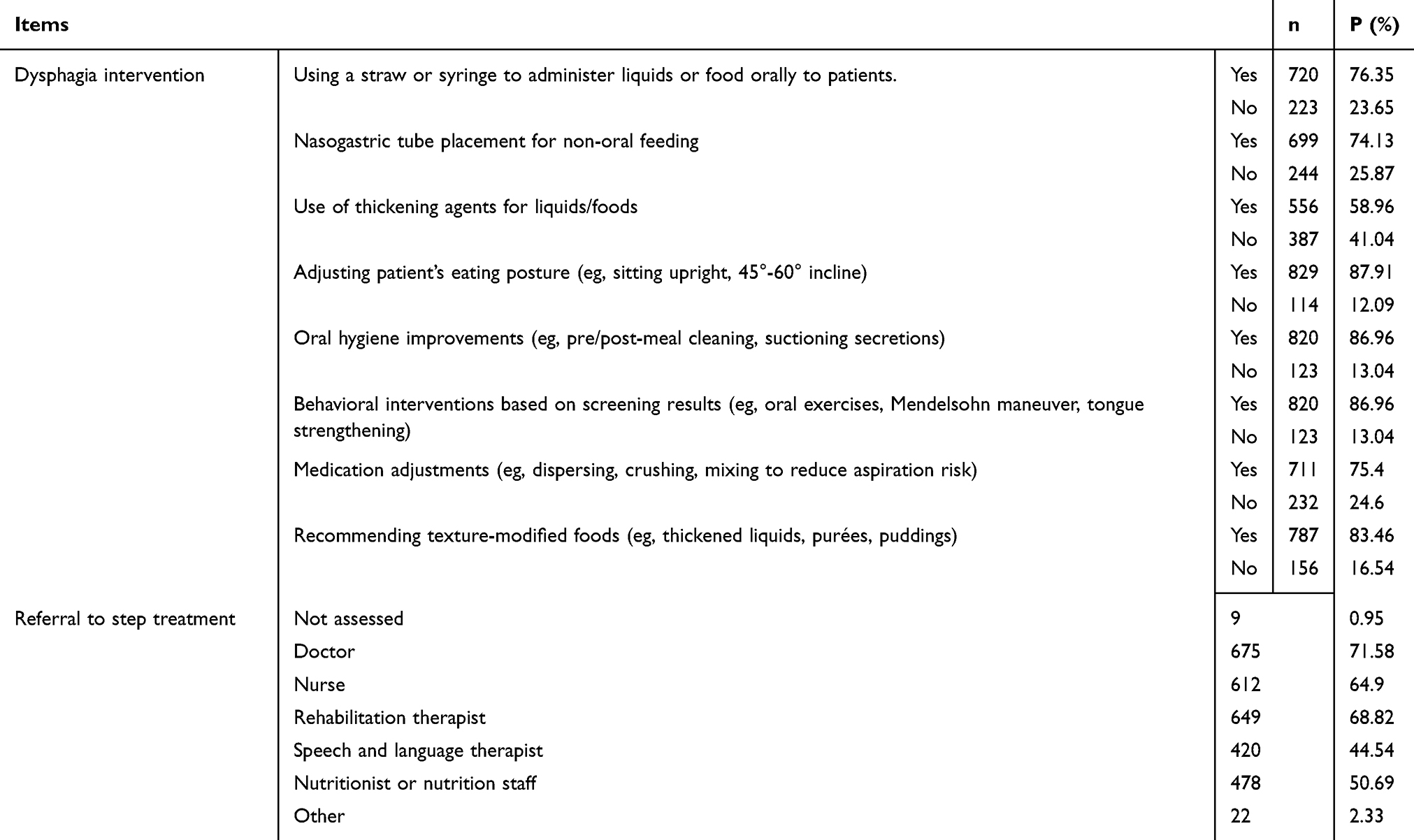 |
Table 2 Dysphagia Management for PSD (n = 943) |
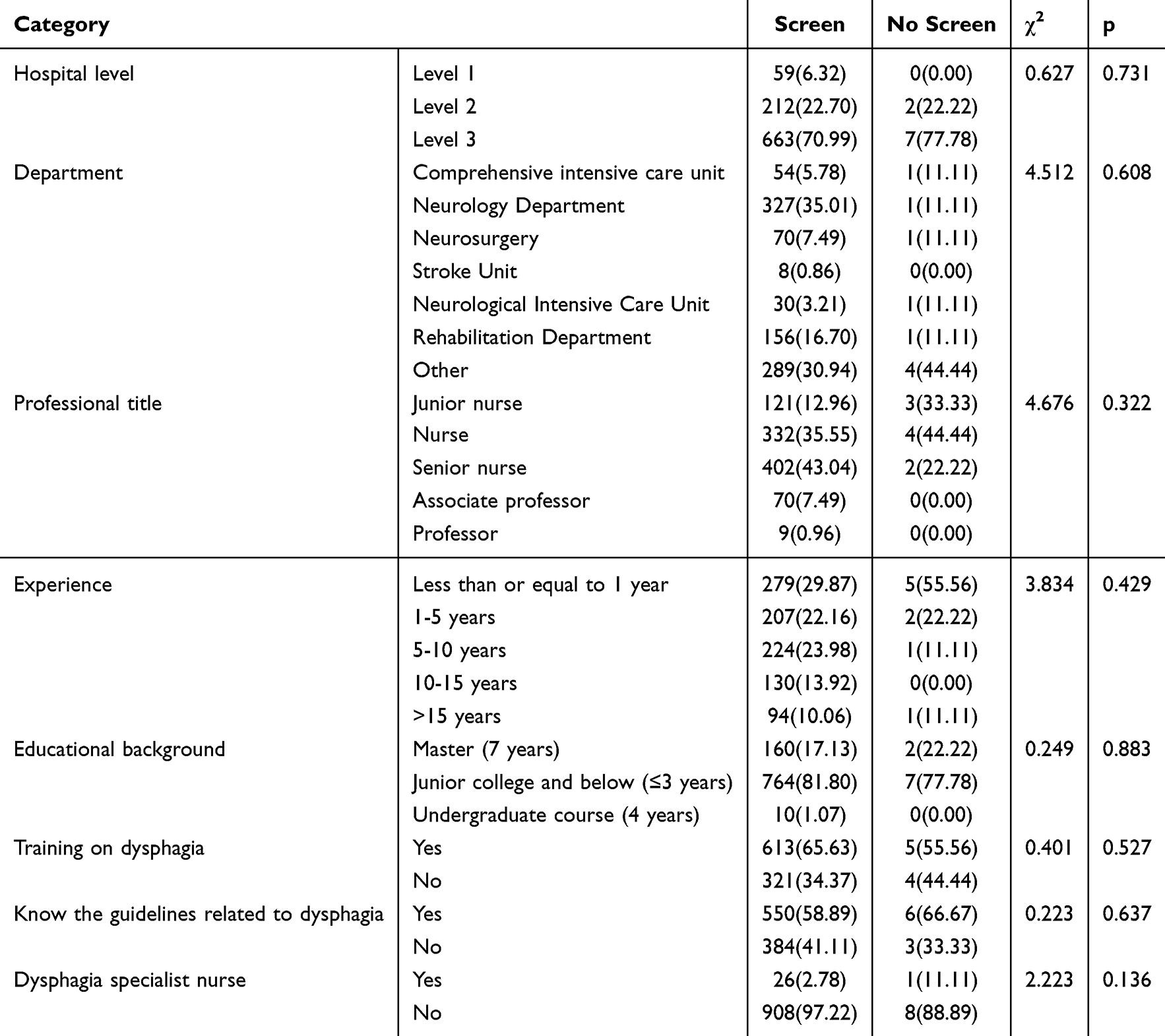 |
Table 3 Univariate Analysis of Dysphagia Screening [(n (%)] |
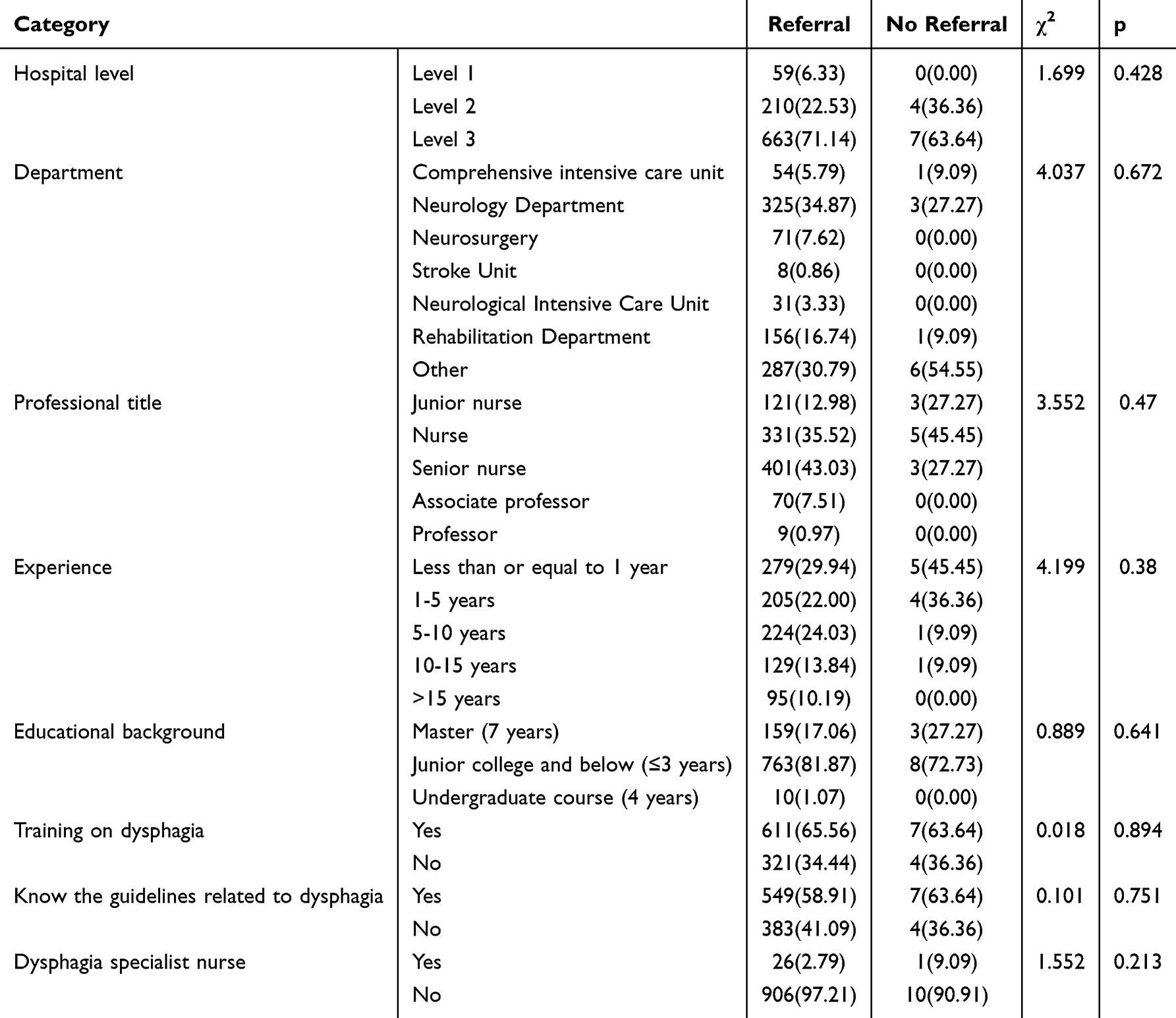 |
Table 4 Univariate Analysis of Referral [(n (%)] |
Discussion
Dysphagia management pathway usually includes screening, assessment, investigation, management, rehabilitation, and feeding. The management of dysphagia in the world is mostly similar, mainly influenced by resources and implementers.22 In this study, we identified implementation gaps between nurses practices and guideline recommendations pertaining to the screening (timing, targets) and management (medicine administration, behavioural interventions and referral) of post-stroke dysphagia (PSD). In a health facility, nurses’ adherence to formal dysphagia guidelines has a significant impact on chest infection and deaths for dysphagia patient.7 The findings were contextualized through comparisons with existing literature to elucidate clinical implications.
Nurses’ Screening Practices for PSD
Screening is often regarded as the initial step in managing dysphagia, by identifying patients at risk of swallowing issues. Substantial variability exists in dysphagia screening protocols (DSPs), with no consensus on optimal methodologies and timing for swallowing function.23,24 Our findings align with prior studies highlighting inconsistencies in screening timing, target populations, and tool selection during the first 72 hours of acute stroke admission.23 These variations may stem from the absence of standardized DSPs, divergent hospital admission pathways, insufficient staff competency, resource limitations, and differences in care workflows.25 Evidence-based guidelines (Level 1B) recommend dysphagia screening by speech-language pathologists (SLPs) or trained health-care professionals.26 However, our data revealed that physicians (highest) and nurses (second-highest) predominantly conducted screenings, with SLPS being the least involved. This deviation likely reflects systemic challenges in mainland China, including a critical shortage of SLPS, delayed development of speech-language therapy as a specialized discipline, and insufficient educational infrastructure for training qualified professionals. Despite recent policy improvements, resource allocation remains suboptimal. Given that nurses and physicians are often the first points of contact for PSD patients, enhancing their knowledge and standardized screening competencies is imperative.
Swallowing screening tools come in various forms, including questionnaire surveys (such as the EAT-10), 30-ml water swallowing tests, screening tools that utilize a combination of water and foods of varying viscosities, screening tools integrated with oxygen saturation monitoring, and scales that necessitate professional training for their implementation. Limited comparative evidence complicates the identification of optimal protocols. Clinicians typically select tools based on diagnostic accuracy (eg, sensitivity, specificity), clinical feasibility, and workflow compatibility.27 The water swallow test (87.8%) was the most frequently utilized tool in our cohort. In China, nursing human resources are in an absolute shortage and often face heavy health-care tasks,28 its likely simplicity in resource-constrained settings. However, there is no evidence to suggest which single screening tool has the highest accuracy.29 The best performing combined water swallow and instrumental tool was the Bedside Aspiration test, the best performing water plus other consistencies tool was the Gugging Swallowing Screen (GUSS), and the best water only swallow screening tool was the Toronto Bedside Swallowing Screening Test (TOR‐BSST).30 Caution is warranted, as these conclusions derive from small-sample studies. Further large-scale investigations are needed to establish evidence-based guidelines for tool selection.
Swallowing Management
Compensatory Strategies
Most nurses reported using compensatory strategies aligned with Chinese expert consensus,31 such as administering liquids via syringes or straws. However, limited evidence exists on the safety and efficacy of delivery tools (spoons, cups, straws). Studies indicate that spoons and straws demonstrate superior safety performance in swallowing (eg, reducing aspiration risk and pharyngeal residue) compared to cups. In terms of food volume delivery, cups outperform straws but are more prone to spillage from the corners of the mouth. Regarding transportation efficiency, straws are advantageous over other tools, as they ensure consistent bolus transport while preserving bolus integrity.32,33 Additionally, over half of the nurses reported recommending modified food textures and utilizing thickening agents for liquids or foods based on screening results. Using thickened liquids and texture-modified diets is a safe and physiologically effective way to improve swallowing function in patients with dysphagia.34 However, there is a lack of robust evidence demonstrating that such interventions reduce the risk of dysphagia-related complications, including aspiration pneumonia.35 Furthermore, a growing body of studies suggests that this approach is associated with adverse clinical outcomes, including dehydration, malnutrition, reduced health-related quality of life, and compromised water and medication bioavailability.36,37 Although thickened liquids may reduce aspiration pneumonia risk and are endorsed by clinical guidelines alongside diet texture modifications,38 their implementation necessitates rigorous swallowing assessments, guidance from nutrition specialists, and collaborative clinician-patient decision-making to formulate individualized optimal care plans.
Medicines Administration
In this study, most participants adopted strategies such as pill dispersion, medication crushing, and combined use of thickening agents to enhance care quality and mitigate aspiration and choking risks during oral medication administration for patients with dysphagia. However, sustained-release formulations and enteric-coated medications, when manually crushed, undergo altered pharmacokinetic profiles. For patients with feeding tubes, crushed medications may result in complications such as feeding tube obstruction or modified drug bioavailability. Additionally, patients may refuse crushed medications due to unpalatable taste. Furthermore, the concurrent use of crushed medications with thickening agents may interfere with drug efficacy and absorption, compromising therapeutic efficacy or jeopardizing patient safety.39–41 Although physicians typically prescribe medications for patients with dysphagia, they often overlook administration methods, creating significant challenges for caregivers (primarily nursing staff). Studies demonstrate that individuals with swallowing impairments face a threefold higher risk of medication errors compared to non-dysphagic patients in the same ward. In some cases, dysphagia patients receive entirely different administration methods due to ad hoc adjustments made by caregivers based on subjective interpretations of situational factors.42,43 Therefore, nurses should prioritize comprehensive medication management for dysphagia patients, including considerations of administration routes, drug texture, formulation modifications, and the concurrent use of thickening agents. In clinical practice, it is critical to strengthen interdisciplinary communication with physicians, pharmacists, speech-language pathologists (SLPs), patients, and their families. By optimizing oral medication regimens to mitigate adverse effects and tailoring personalized dosing strategies, nurses can significantly enhance the standardization and efficacy of oral medication care for this population.
Swallowing Exercise
According to the neuroplasticity theory, early implementation of rehabilitation exercises in patients with post-stroke dysphagia can effectively improve swallowing function, prevent aspiration pneumonia, and reduce hospitalization duration.44 Our survey revealed that the majority of nurses provide targeted rehabilitation interventions—such as the effortful swallow, supraglottic swallow, super-supraglottic swallow, Mendelsohn maneuver, Shaker exercise, and Masako maneuver—based on screening outcomes to enhance swallowing physiology in these patients. However, it is noteworthy that while existing studies demonstrate the efficacy of nurse-led rehabilitative interventions in reducing aspiration risk and improving oral intake capacity among dysphagia patients, insufficient evidence supports nurses’ prescriptive authority and clinical competency to independently prescribe or execute such protocols.8 Furthermore, nurses must undergo formal training before administering rehabilitation exercises—even after comprehensive evaluations by speech-language pathologists (SLPs) —as these interventions fall under the purview of SLPs rather than within the standard scope of nursing practice.45
Referral
Comprehensive management of dysphagia patients necessitates an interprofessional, multidisciplinary team. Following swallowing screenings, appropriate and timely referrals are critical. In this study, most nurses referred patients to physicians for further swallowing evaluation and treatment, followed by occupational therapists, other nurses, and nutritionists, with speech-language pathologists (SLPs) receiving the lowest referral rates. The observed referral bias may stem from nurses’ limited familiarity with the roles of other multidisciplinary team (MDT) members and insufficient recognition of the critical contributions of speech-language pathologists (SLPs) in dysphagia assessment, management, and rehabilitation. Additionally, most nurses expressed confusion regarding the distinct responsibilities of interprofessional team members. Ambiguous role delineation within the MDT likely contributes to referral inaccuracies, treatment delays, and diminished clinical efficiency. Furthermore, mainland China faces a critical shortage of speech-language pathologists (SLPs), with some departments in primary care hospitals lacking SLPS staffing entirely. Consequently, adherence to guideline-recommended referral protocols is often unattainable. Nevertheless, multidisciplinary teams (MDTs) remain essential for delivering optimal stroke care. Effective collaboration within MDTs hinges on nurses’ understanding of interprofessional roles and robust communication skills.46 It is recommended to strengthen mutual understanding, appreciation, and shared recognition of scopes of practice and professional responsibilities between nurses and other health-care professionals (eg, speech-language therapists). Concurrently, enhancing dysphagia management knowledge and training for non-SLPS health-care staff is imperative to address the shortage of SLPSs and meet the urgent need for timely identification and treatment of dysphagia. These measures are critical to ensuring the consistent implementation of patient-centered care principles across diverse clinical environments.
Under the set conditions and target population of this study, in order to explore the factor impact the dysphagia management, we conducted univariate analysis of dysphagia screen and referral to further improve the results and get a better understanding of the data. We found that there was no statistically significant difference (p > 0.05) in the screening rate and referral rate of nurses’ general information, indicating that simply increasing the training rate may not be enough to improve the level of screening and referral. The reason may be that using univariate analysis in this study may not be able to control for confounding variables, and then sampling errors may result in this result not being displayed. In future research, more complex multi-level factors can be designed, such as using comprehensive incentive system optimization methods for improvement. Secondly, the current consensus guidelines have not established a standard path for screening and referral of post-stroke swallowing disorders, and the reference standards for clinical screening and referral practices have not been unified.
Although clinical guidelines provide detailed recommendations for screening and management, deviations persist in the nursing practices for post-stroke dysphagia in China. These discrepancies may stem from insufficient awareness of guidelines among nurses (58.96%), inadequate training in dysphagia management (65.54%), and an acute shortage of specialized dysphagia nurses (2.86%). Additionally, nurses often express uncertainty regarding their scope of practice and responsibilities in managing post-stroke dysphagia, which may lead to reliance on experiential knowledge rather than evidence-based protocols in clinical decision-making. Furthermore, staffing shortages, excessive workloads, and insufficient time allocated to fulfilling nursing responsibilities may contribute to deviations from evidence-based practices in dysphagia care.47 Therefore, we suggest that nursing educators and leaders prioritize the training of swallowing specialist nurses. They should develop standardized clinical practice pathways suited to China’s context, establish evaluation criteria, and regularly assess nurses’ grasp of swallowing disorder knowledge and practices. Training content should also be dynamically updated per actual needs to enhance nurses’ clinical evidence-based practice abilities and boost nursing quality.
Limitations
Sampling method: Convenience sampling may lead to sampling bias. In the future, stratified sampling or cluster random sampling can be used if conditions permit. Questionnaire collection: Using Questionnaire star for data collection may make it difficult to collect data in underdeveloped or remote areas, resulting in a lack of information in this area. In the future, the data collection time can be extended or multi-channel joint promotion can be adopted to improve the response rate and sample representativeness of the questionnaire. This study only investigates nurses’ practice status based on PSD and did not explore the influencing factors of nursing practice Future research will aim to develop a new tool to evaluate this connection.
Conclusion
There is a gap between the current status and guidelines of Chinese nurses’ screening and management of swallowing difficulties. Nurses’ understanding and acceptance of guidelines related to swallowing disorders are still insufficient. To fill this gap, we will optimize the questionnaire content in future research, increase stratified sampling and grassroots sampling methods, improve sample size, and further explore the influencing factors of swallowing disorder management practices among Chinese nurses to ensure accurate solution strategies are provided. We advocate that nursing decision-makers should increase training on swallowing related knowledge for nurses and cultivate specialized swallowing nursing talents to improve and enhance the quality of nursing practice. This study reveals the practical shortcomings of nurses in PSD management in China, nurses neglect the importance of specialists as SLPs in the multidisciplinary team, besides, medication provision and management of exercise needs training and should not solely be decided by nurses, providing a key direction for optimizing the quality of stroke care through standardized screening, interdisciplinary collaboration, specialized capacity building, and resource allocation. Swallowing related complications can be significantly reduced, patient prognosis can be improved, and medical costs can be reduced.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author Changyan Yuan upon reasonable request.
Public Contribution
There was no contribution from patients or the public in this study.
Funding
This work is supported by the Chongqing Science and Health Joint Medical Research Project, China (2024QNXM002).
Disclosure
All of the authors declare that they have no competing interests.
References
1. Lindsay MP, Norrving B, Sacco RL, et al. World stroke organization (WSO): global stroke fact sheet 2019. Int J Stroke. 2019;14(8):806–817. doi:10.1177/1747493019881353
2. Takizawa C, Gemmell E, Kenworthy J, Speyer R. A systematic review of the prevalence of oropharyngeal dysphagia in stroke, parkinson’s disease, alzheimer’s disease, head injury, and pneumonia. Dysphagia. 2016;31(3):434–441. doi:10.1007/s00455-016-9695-9
3. Banda KJ, Chu H, Chen R, et al. Prevalence of oropharyngeal dysphagia and risk of pneumonia, malnutrition, and mortality in adults aged 60 years and older: a meta-analysis. Gerontology. 2022;68(8):841–853. doi:10.1159/000520326
4. WHO. International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
5. Chen BJ, Suolang D, Frost N, Faigle R. Practice patterns and attitudes among speech-language pathologists treating stroke patients with dysphagia: a nationwide survey. Dysphagia. 2022;37(6):1715–1722. doi:10.1007/s00455-022-10432-6
6. Khoja MA. Registered nurses’ knowledge and care practices regarding patients with dysphagia in Saudi Arabia. Int J Health Care Qual Assur. 2018;31(8):896–909. doi:10.1108/IJHCQA-06-2017-0106
7. Hines S, Kynoch K, Munday J. Nursing interventions for identifying and managing acute dysphagia are effective for improving patient outcomes: a systematic review update. J Neurosci Nurs. 2016;48(4):215–223. doi:10.1097/JNN.0000000000000200
8. Ye J, Wu C, Chen J, et al. Effectiveness of nurse-delivered stepwise swallowing training on dysphagia in patients with Alzheimer’s disease: a multi-center randomized controlled trial [published correction appears in Int J Nurs Stud. 2025 Feb;162:104966. doi: 10.1016/j.ijnurstu.2024.104966.]. Int J Nurs Stud. 2024;150:104649. doi:10.1016/j.ijnurstu.2023.104649
9. Tan L, Gan G, Hum A, Lee A. A stepwise, mixed-method study approach to identify the barriers to dysphagia care in hospice care nurses. J Hosp Palliat Nurs. 2018;20(1):88–94. doi:10.1097/NJH.0000000000000404
10. Abu-Snieneh HM, Saleh MYN. Registered nurse’s competency to screen dysphagia among stroke patients: literature review. Open Nurs J. 2018;12:184–194. doi:10.2174/1874434601812010184
11. Benfield JK, Wilkinson G, Everton LF, Bath PM, England TJ. Diagnostic accuracy of the dysphagia trained nurse assessment tool in acute stroke. Eur J Neurol. 2021;28(8):2766–2774. doi:10.1111/ene.14900
12. Austbø Holteng LB, Frøiland CT, Corbett A, Testad I. Care staff perspective on use of texture modified food in care home residents with dysphagia and dementia. Ann Palliat Med. 2017;6(4):310–318. doi:10.21037/apm.2017.06.24
13. Blaszczyk A, Brandt N, Ashley J, Tuders N, Doles H, Stefanacci RG. Crushed tablet administration for patients with dysphagia and enteral feeding: challenges and considerations. Drugs Aging. 2023;40(10):895–907. doi:10.1007/s40266-023-01056-y
14. Murray J, Scholten I. An oral hygiene protocol improves oral health for patients in inpatient stroke rehabilitation. Gerodontology. 2018;35(1):18–24. doi:10.1111/ger.12309
15. Miles A, Lee YY, McLellan N, Gillham M. Implementing a systematic care pathway for management of dysphagia after cardiothoracic surgery. Intensive Crit Care Nurs. 2022;70:103224. doi:10.1016/j.iccn.2022.103224
16. Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurol. 2007;6(2):182–187. doi:10.1016/S1474-4422(07)70031-5
17. Hines S, Kynoch K, Munday J. Identification and nursing management of dysphagia in individuals with acute neurological impairment: a systematic review protocol. JBI Database Rev Implementation Rep. 2014;12(5):195–236. doi:10.1097/01.XEB.0000455128.74875.d2
18. Dondorf K, Fabus R, Ghassemi AE. The interprofessional collaboration between nurses and speech-language pathologists working with patients diagnosed with dysphagia in skilled nursing facilities. J Nurs Educ Pract. 2016;6(4):17–20.
19. Hines S, Wallace K, Crowe L, Finlayson K, Chang A, Pattie M. Identification and nursing management of dysphagia in individuals with acute neurological impairment (update). Int J Evid Based Healthc. 2011;9(2):148–150. doi:10.1111/j.1744-1609.2011.00211.x
20. Gong Y, Liu Y, Chen Y. Factors influencing coping with death competence among Chinese oncology nurses: a national cross-sectional study. J Multidiscip Healthc. 2024;17:4781–4789. doi:10.2147/JMDH.S489758 PMID: 39434826; PMCID: PMC11492920.
21. Nishiwaki K, Tsuji T, Liu M, et al. Identification of a simple screening tool for dysphagia in patients with stroke using factor analysis of multiple dysphagia variables. J Rehabil Med. 2005;37(4):247–251. doi:10.1080/16501970510026999 PMID: 16024482.
22. Smithard DG. Dysphagia management and stroke units. Curr Phys Med Rehabil Rep. 2016;4(4):287–294. doi:10.1007/s40141-016-0137-2 Epub 2016 Nov 23. PMID: 28018754; PMCID: PMC5148787.
23. Eltringham SA, Kilner K, Gee M, et al. Impact of dysphagia assessment and management on risk of stroke-associated pneumonia: a systematic review. Cerebrovasc Dis. 2018;46(3–4):99–107. doi:10.1159/000492730
24. Zhang T, Zhao J, Li X, et al. Chinese stroke association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of stroke rehabilitation. Stroke Vasc Neurol. 2020;5(3):250–259. doi:10.1136/svn-2019-000321
25. Eltringham SA, Smith CJ, Pownall S, Sage K, Bray B. Variation in dysphagia assessment and management in acute stroke: an interview study. Geriatrics. 2019;4(4):60. doi:10.3390/geriatrics4040060
26. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association [published correction appears in Stroke. 2017 Feb;48(2):e78. doi: 10.1161/STR.0000000000000120.] [published correction appears in Stroke. 2017 Dec;48(12):e369. doi: 10.1161/STR.0000000000000156.]. Stroke. 2016;47(6):e98–e169. doi:10.1161/STR.0000000000000098
27. Speyer R, Cordier R, Farneti D, et al. White paper by the European Society for Swallowing Disorders: screening and non-instrumental assessment for dysphagia in adults. Dysphagia. 2022;37(2):333–349. doi:10.1007/s00455-021-10283-7
28. Chen W, Ma Y, Yu C. Unmet chronic care needs and insufficient nurse staffing to achieve universal health coverage in China: analysis of the global burden of disease study 2019. Int J Nurs Stud. 2023;144:104520. doi:10.1016/j.ijnurstu.2023.104520
29. Kiekens C, Tognonato C. Which screening tool should be used for identifying aspiration risk associated with dysphagia in acute stroke? A Cochrane Review summary with commentary.NeuroRehabilitation.2022;51(3):533–535. doi:10.3233/NRE-228024
30. Boaden E, Burnell J, stroke. Cochrane Database Syst Rev. 2021;10
31. Dou Z, Wen H. Chinese rehabilitation medicine association swallowing disorder rehabilitation professional committee guidelines for rehabilitation management of swallowing disorders in China (2023 edition). Chin J Phys Med Rehabil. 2023. doi:10.3760/cma.j.issn.0254-1424.2023.12.001
32. Veiga HP, Fonseca HV, Bianchini EM. Sequential swallowing of liquid in elderly adults: cup or straw? Dysphagia. 2014;29(2):249–255. doi:10.1007/s00455-013-9503-8
33. Kuhlemeier KV, Palmer JB, Rosenberg D. Effect of liquid bolus consistency and delivery method on aspiration and pharyngeal retention in dysphagia patients. Dysphagia. 2001;16(2):119–122. doi:10.1007/s004550011003
34. Newman R, Vilardell N, Clavé P, Speyer R. Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: white paper by the European Society for Swallowing Disorders (ESSD) [published correction appears in Dysphagia. 2016 Oct;31(5):719. doi: 10.1007/s00455-016-9729-3]. Dysphagia. 2016;31(2):232–249. doi:10.1007/s00455-016-9696-8
35. Beck AM, Kjaersgaard A, Hansen T, Poulsen I. Systematic review and evidence based recommendations on texture modified foods and thickened liquids for adults (above 17 years) with oropharyngeal dysphagia - An updated clinical guideline. Clin Nutr. 2018;37(6 Pt A):1980–1991. doi:10.1016/j.clnu.2017.09.002
36. Wu XS, Miles A, Braakhuis A. Nutritional intake and meal composition of patients consuming texture modified diets and thickened fluids: a systematic review and meta-analysis. Healthcare. 2020;8(4):579. doi:10.3390/healthcare8040579
37. Steele SJ, Ennis SL, Dobler CC. Treatment burden associated with the intake of thickened fluids. Breathe. 2021;17(1):210003. doi:10.1183/20734735.0003-2021
38. Burgos R, Bretón I, Cereda E, et al. ESPEN guideline clinical nutrition in neurology. Clin Nutr. 2018;37(1):354–396. doi:10.1016/j.clnu.2017.09.003
39. Gudin J, Cooperman N, Kopecky EA, Fleming AB. extended-release oxycodone formulations with abuse-deterrent properties. Pain Med. 2015;16(11):2142–2151. doi:10.1111/pme.12834
40. Bankhead R, Boullata J, Brantley S, et al. Enteral nutrition practice recommendations. JPEN J Parenter Enteral Nutr. 2009;33(2):122–167. doi:10.1177/0148607108330314
41. Wright DJ, Potter JF, Clark A, et al. Administration of aspirin tablets using a novel gel-based swallowing aid: an open-label randomised controlled cross-over trial. BMJ Innov. 2019;5(4):113–119. doi:10.1136/bmjinnov-2018-000293
42. Kelly J, Wright D, Wood J. Medicine administration errors in patients with dysphagia in secondary care: a multi-centre observational study. J Adv Nurs. 2011;67(12):2615–2627. doi:10.1111/j.1365-2648.2011.05700.x
43. Kelly J, Eggleton A, Wright D. An analysis of two incidents of medicine administration to a patient with dysphagia. J Clin Nurs. 2011;20(1–2):146–155. doi:10.1111/j.1365-2702.2010.03457.x
44. Minelli C, Luvizutto GJ, Cacho RO, et al. Brazilian practice guidelines for stroke rehabilitation: part II. Diretrizes brasileiras para reabilitação no acidente vascular cerebral: part II. Arq Neuropsiquiatr. 2022;80(7):741–758. doi:10.1055/s-0042-1757692
45. American Speech-Language-Hearing Association (ASHA) (2015). Speech-language pathology medical review guidelines. Available from: https://www.asha.org/uploadedFiles/SLP-Medical-Review-Guidelines.pdf.
46. Li H, Yu X, An D, et al. Investigation and analysis of the influencing factors of nurses’ core competencies after swallowing specialist training. Chin J Phys Med Rehabil. 2019;12:941–944.
47. Rowe K, Du Toit MN, Pillay SB, Krüger E. Nurses’ practices in stroke-related dysphagia in low- and middle-income countries. Curationis. 2024;47(1):e1–e9. doi:10.4102/curationis.v47i1.2499
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Analysis of Trends in the Burden of Maternal Hemorrhage Attributable to Iron Deficiency in China from 1990 to 2023: A Population-Based Study
Yang L, Cai Z, Xu W, Wang L
International Journal of Women's Health 2026, 18:485066
Published Date: 14 July 2026