Back to Journals » Journal of Inflammation Research » Volume 18
The Potential of High-Density Lipoprotein as a Predictive Biomarker for Infliximab Efficacy in Crohn’s Disease
Authors Tang K ![]() , Peng Z, Xu D, Li Y
, Peng Z, Xu D, Li Y ![]() , Liu X, Lian G, Peng Y
, Liu X, Lian G, Peng Y ![]()
Received 29 July 2025
Accepted for publication 11 December 2025
Published 26 December 2025 Volume 2025:18 Pages 18137—18149
DOI https://doi.org/10.2147/JIR.S556975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Nadia Andrea Andreani
Keke Tang,1,2,* Ziheng Peng,1,2,* Duo Xu,1,2 Yong Li,1,2 Xiaowei Liu,1– 3 Guanghui Lian,1– 3 Yu Peng1– 3
1Department of Gastroenterology, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China; 2Hunan International Scientific and Technological Cooperation Base of Artificial Intelligence Computer Aided Diagnosis and Treatment for Digestive Disease, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China; 3Research Center for Geriatric Disorder, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Peng, Email [email protected] Guanghui Lian, Email [email protected]
Background: To assess whether baseline serum high density lipoprotein (HDL) levels predict the effectiveness of infliximab in patients with Crohn’s disease (CD).
Methods: This was a retrospective single-center study evaluating CD patients baseline data and effectiveness of infliximab at the Xiangya Hospital, Central South University, between January 2016 and September 2021. The primary endpoint was composite adverse outcome during 52 weeks, defined as clinical activity, changes in treatment, surgical treatment, or unexpected readmission.
Results: Among the 166 enrolled patients, 37 (22.3%) experienced adverse events within the 52-week follow-up period. HDL was identified as a predictor of adverse outcomes at 52 weeks (AUC 0.661, p < 0.05), with an optimal cut-off value of 0.85. Patients with higher HDL levels not only exhibited elevated total cholesterol but were also associated with better nutritional status and lower inflammatory burden. HDL was negatively correlated with white blood cell count and C-reactive protein, and positively correlated with albumin level (p < 0.05). Baseline HDL level was an independent risk factor for adverse events within 52 weeks in CD patients treated with infliximab (p = 0.022). Moreover, the high-HDL group demonstrated a significantly lower risk of developing adverse events (p = 0.0017).
Conclusion: The identification of HDL as an independent risk factor for 52-week adverse events in infliximab-treated CD patients suggests its potential utility as a predictive biomarker.
Trial Registration: The study adhered to the Declaration of Helsinki. All participants provided written informed consent, and the study was approved by the Ethics Committee of Xiangya Hospital, Central South University with approval No. 202108158.
Plain Language Summary: Given the variable therapeutic response to IFX among patients, there exists a critical need for reliable biomarkers to monitor treatment effectiveness and guide individualized clinical decision-making.HDL demonstrated significant inverse correlations with both CRP levels and WBC counts, while showing a positive association with serum albumin concentrations. Multivariate analysis identified HDL as an independent predictor of adverse events within 52 weeks following infliximab therapy in CD patients.HDL measurement represents a promising prognostic tool for IFX-treated CD patients, offering three distinct clinical benefits: first, broader patient applicability compared to existing markers; second, enhanced utility in routine clinical practice; and third, potential cost-saving implications for therapeutic management.
Keywords: high-density lipoprotein, infliximab, Crohn’s disease, effectiveness, biomarker
Introduction
Crohn’s disease (CD), a chronic inflammatory condition of the gastrointestinal tract, is characterised by recurrent and often intractable symptoms, posing a significant global health challenge.1 Although the precise pathogenic mechanisms are not fully understood, current evidence indicates that the interplay between genetic predisposition, environmental exposures, and gut microbial dysbiosis initiates a dysregulated immune reaction at the mucosal interface, ultimately resulting in epithelial barrier dysfunction.2 Typically, young individuals present with symptoms such as abdominal pain, chronic diarrhoea, weight loss, and fatigue. Over time, approximately 50% of affected individuals develop complications, including strictures, fistulas, and abscesses, often necessitating further surgical interventions.3 Notably, research indicates that intestinal resection impacts fertility in both male and female patients with CD.4 Additionally, up to 90% of individuals exhibit signs of subclinical recurrence detectable via endoscopy within a year of surgery, with 70% requiring subsequent surgical procedures.5 Consequently, the primary goal of current treatment strategies is to achieve sustained deep remission, prevent complications, minimise the need for surgery, and halt disease progression in patients with CD.6
Infliximab (IFX), a chimeric monoclonal antibody directed against tumor necrosis factor-α (TNF-α), represents a cornerstone biologic therapy for moderate-to-severe CD refractory to conventional treatments.7 IFX has demonstrated efficacy in inducing and maintaining clinical remission, promoting mucosal healing, and preventing disease recurrence following endoscopic surgery. Moreover, in cases of complex perianal disease, IFX has proven more effective than other biological agents in achieving and sustaining fistula closure.8 However, infliximab may not be suitable for all patients with CD. Approximately 25% of patients exhibit primary nonresponse, and one-third experience secondary loss of response during treatment, with only about a third maintaining remission by 52 weeks.9 Recent studies have identified several potential predictors for infliximab response, such as the serum free triiodothyronine to thyroxine ratio (fT3/fT4). However, their clinical predictive value remains limited due to suboptimal accuracy and clinical applications.10 This highlights the urgent need for new biomarkers capable of predicting infliximab efficacy, identifying non-responders and those with loss of response at an early stage, and monitoring the disease. Such biomarkers would serve as critical tools for guiding personalised treatment in CD.11
Previous research has indicated that the therapeutic response to infliximab is associated with the complement system. High-density lipoprotein (HDL) also plays a role in modulating complement system activation.12,13 Moreover, our previous research also indicated that improvement in colitis following anti-TNF-α therapy in CD patients is associated with increased HDL-C levels.14 Furthermore, HDL has been reported to suppress intestinal inflammation via autophagy, highlighting its potential as a therapeutic target in IBD.15 Additionally, a study by Markku Voutilainen et al suggested an inverse correlation between HDL and the development of pediatric IBD.16 Moreover, studies have revealed that lower HDL levels are correlated with increased disease severity and a poorer long-term prognosis in patients with inflammatory bowel disease (IBD).17 Based on these findings, we hypothesise that HDL levels, a routinely measured lipid index, may serve as a predictor of infliximab efficacy. This hypothesis is grounded in HDL’s established predictive value for a range of conditions, including coronary heart disease and Alzheimer’s disease.18
In this study, we validated the predictive significance of HDL levels in evaluating the therapeutic efficacy of IFX in the treatment of CD.
Methods
Ethical Considerations
This investigation was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Prior to study commencement, written informed consent was obtained from all participants, and ethical approval was granted by the Institutional Review Board of Xiangya Hospital, Central South University (Approval No. 202108158).
Study Design and Participants
This was a retrospective study conducted at the IBD Centre of Xiangya Hospital, Central South University. From January 2016 to September 2021, 166 patients diagnosed with CD and initially treated with infliximab were included in this study. The diagnostic criteria for CD are based on clinical presentation and endoscopic and histological criteria. The diagnosis for all enrolled patients was established by a consensus of at least two clinicians, endoscopists, and pathologists. The inclusion criteria for this study were as follows: (1) had Crohn’s disease diagnosed at the IBD Centre, Xiangya Hospital, Central South University; (2) were administered infliximab strictly according to the manufacturer’s instructions (the dose was 5 mg/kg, and the second and third doses were administered 2 and 6 weeks after the first dose, respectively, and once every 8 weeks thereafter). The exclusion criteria were as follows: (1) incomplete case data; (2) follow-up time < 52 weeks; (3) lost to follow-up for objective or subjective reasons; (4) pregnancy during follow-up; (5) other malignancies, severe liver disease, severe active infection, congenital or acquired immunodeficiency, cognitive impairment or mental disorders. The study enrollment flowchart (Figure 1) delineates patient progression through screening, eligibility assessment, and final inclusion in the trial.
 |
Figure 1 Flowchart of patients included in this study. |
Clinical Measurements
In this study, the baseline data of 166 participating patients, including general information, laboratory data, site of disease and behaviour, were collected retrospectively. General information included age, sex, body mass index, disease course, and medical history, including history of smoking, history of anal fistula, history of previous surgery, history of hormone use, history of immunosuppressant use (including 6-meropurine, azathioprine, and methotrexate), and history of 5-aminosalicylic acid use. The laboratory data included white blood cell (WBC) counts, platelet counts, haemoglobin counts, albumin levels, serum creatinine levels, fibrinogen levels, erythrocyte sedimentation rates and C-reactive protein (CRP) levels. Crohn’s disease activity index, triglyceride, total cholesterol, HDL and low-density lipoprotein levels were also recorded; disease sites included the small bowel, colon or both. Disease behaviour included penetrating type, stenotic type and nonpenetrating nonstenotic type.
Follow-Up and Endpoints
The follow-up period of this trial was 52 weeks, and the follow-up methods included outpatient examination, telephone interviews and WeChat. The primary endpoint is composite adverse outcome during 52 weeks, defined as clinical activity, changes in treatment, surgical treatment, or unexpected readmission.
Statistical Analysis
This study was a retrospective analysis with a final analytical sample size of 166 patients. To evaluate the statistical power of the current sample size for detecting a clinically meaningful effect, a post-hoc power analysis was conducted. The analysis was based on the following parameters: a significance level (α) of 0.1, and a reference endpoint event rate derived from the 30-week IFX response rate of 41.8% in the ACCENT I randomized trial.19 As this is an exploratory analysis, a medium effect size (Cohen’s f2 = 0.15, OR = 1.5) was selected as the benchmark. The resulting statistical power of this study was calculated to be 80.1%.
The baseline data collected were first classified to describe the baseline characteristics of the patients, with interquartile ranges (IQR) calculated for continuous data and proportions calculated for categorical data. The incidence of adverse events within 52 weeks was calculated, and receiver operating characteristic (ROC) curves for HDL were constructed. Internal validation included bootstrap resampling (1000 iterations) to assess discrimination in ROC analysis using relevant R packages. The cluster bootstrap-adjusted Youden index was calculated to determine the best cut-off value for HDL. Patients were divided into a high-HDL group and a low-HDL group using the best cut-off value. Unpaired t tests, Wilcoxon rank-sum tests or chi-square tests were used to evaluate the indicators that were significantly different between the two groups. The correlation between HDL and common inflammatory markers was analysed via linear regression. Univariate backwards Cox regression analyses were subsequently performed to identify risk factors associated with adverse outcomes. Least Absolute Shrinkage and Selection Operator (LASSO) regression was subsequently performed to narrow down variables for further multivariate Cox regression analysis to determine independent predictors. In addition, multicollinearity was examined using Variance Inflation Factor (VIF) to ensure variable independence in the study. Finally, Kaplan‒Meier curves were plotted to compare the incidence of adverse events in different HDL groups. Statistical significance was defined as two-tailed P values < 0.05. All analyses were conducted using SPSS Statistics (version 21, SPSS, Chicago, Illinois, USA) and R (Version 4.4.1).
Results
Clinical Parameters of the Participants
Between January 2016 and September 2021, 231 patients with CD were treated with IFX, and 166 eligible patients were included in the study. There were 122 male patients (73.5%) and 44 female patients (26.5%), with a median age of 26 years (IQR 18.75–34.00) and a median body mass index of 17.72 kg/m2 (IQR 15.87–19.58). The median disease duration was 12 months (IQR 4.0–24.0); 34 patients (20.50%) had a history of smoking, 87 patients (52.4%) had a history of perianal disease, 25 patients (25.1%) had a history of bowel surgery, and 15 patients (9.0%) had a history of steroid use. 28 patients (16.9%) used immunosuppressants, and 33 patients (19.9%) used 5-aminosalicylic acid drugs. Laboratory parameters are presented in Table 1.
 |
Table 1 Patient Characteristics at Baseline |
Comparison of ROC Curves Before and After Bootstrapping Correction
Of the 166 enrolled patients, 37 (22.3%) experienced adverse events within the 52-week follow-up. The ability of HDLto predict adverse events in CD patients treated with IFX was assessed using ROC curve analysis (Figure 2A). The result was internally validated using bootstrap resampling, yielding an AUC of 0.661[cluster bootstrap-adjusted 95% CI 0.567–0.764, p < 0.05]. Furthermore, the optimal HDL cut-off value derived from the ROC curve was 0.85 (Supplementary Table 1).
 |
Figure 2 Receiver operating characteristic (ROC) curve analysis and linear regression analysis of HDL. ROC curve analysis for high-density lipoprotein cholesterol (HDL) levels to predict (A) Comparison of ROC curves before and after bootstrapping correction. Correlations of high-density lipoprotein cholesterol (HDL) with (B) WBC, white blood cell (C) CRP and (D) albumin (ALB) at baseline. |
Differences Between the High-HDL Group and the Low-HDL Group
The HDL level of the study patients was cut off at 0.85; those with a >0.85 were assigned to the high-HDL group, and those with a ≤0.85 were assigned to the low-HDL group. A comparison of the baseline data between the two groups is shown in Table 2. The WBC (6.50[4.50–8.10] vs 7.10[8.30–81.05], p=0.037) and CRP level (17.05[5.33–36.00] vs 37.05[8.30–81.05], p<0.001) were lower in the high-HDL group than in the low-HDL group. The serum albumin (37.40[31.60–40.70] vs 32.80[27.60–38.10], p<0.001) and total cholesterol levels (3.48[3.02–4.01] vs 3.10[2.68–3.60], p<0.001) were greater in the high-HDL group than in the low-HDL group. The comparative analysis revealed no significant intergroup disparities in other measured parameters. Linear regression of HDL with WBC, CRP and serum albumin levels showed that HDL was negatively correlated with WBC and CRP levels (r=−0.175, p=0.024; r=−0.323, p < 0.001; and that HDL was positively correlated with the serum albumin level (r=0.302, p < 0.001) (Figure 2).
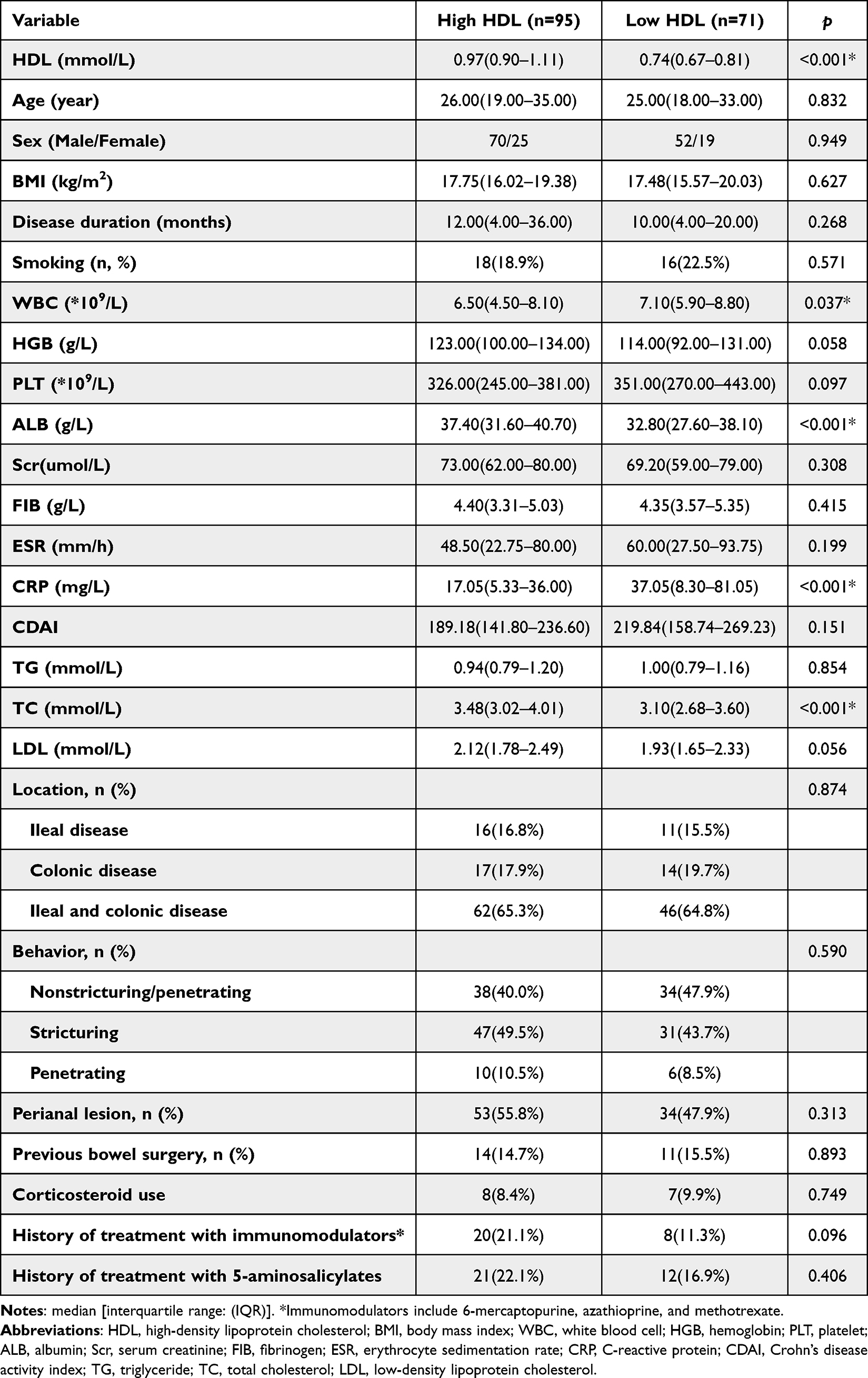 |
Table 2 Associations of High-Density Lipoprotein Cholesterol with Clinical Characteristics of Patients with Crohn’s Disease |
Association of HDL with the Therapeutic Effect of Infliximab
Univariate and multivariate Cox regression analyses are shown in Table 3. Moreover, univariate Cox regression analysis revealed that smoking history; serum albumin level; and serum creatinine, CRP and HDL levels were risk factors for adverse events in patients with CD treated with infliximab within 52 weeks. In addition, LASSO regression analysis identified two predictors (Figure 3): HDL and CRP. These variables were incorporated into a multivariate Cox regression model, which demonstrated that HDL was an independent risk factor for adverse events in patients with CD treated with infliximab within 52 weeks (HR=0.430, 95% CI=0.209–0.884; p=0.022). Collinearity diagnosis confirmed the absence of significant multicollinearity between HDL and CRP (Tolerance = 0.895, VIF = 1.117).
 |
Table 3 Predictive Factors for Poor Outcomes at 52 weeks by Univariate and Multivariate Analysis |
 |
Figure 3 Prediction Model Based on LASSO Logistic Regression: Variable Selection Using the Optimal Lambda Value. (A) The tuning parameter (λ = 0.09633866) was selected by applying LASSO-penalized logistic regression with ten-fold cross-validation using the minimum criterion. A plot of the partial likelihood deviance (binomial deviance) against log (λ) is shown. Vertical dashed lines indicate the optimal values selected by the minimum criterion and the one-standard-error rule (ie, within one standard error of the minimum). (B) LASSO coefficient profile for the two radiomics features. The coefficient paths are plotted against log (λ). Each colored line represents the coefficient of a corresponding feature. Abbreviation: LASSO, Least Absolute Shrinkage and Selection Operator. |
Comparison of Adverse Events Between the High-HDL Group and Low-HDL Group
The Kaplan‒Meier curve showed that the incidence of adverse events was lower in the group with high HDL levels than in the group with low HDL levels (p =0.0017) (Figure 4).
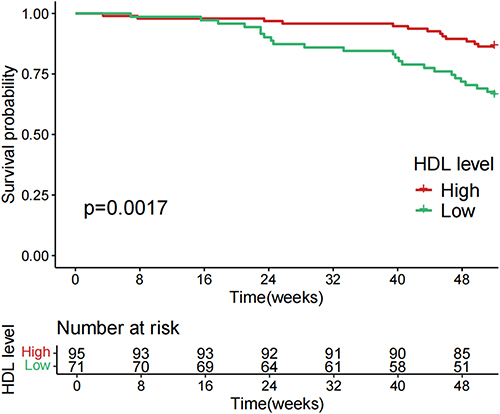 |
Figure 4 K‒M curve of the incidence of nonpoor outcomes according to baseline high-density lipoprotein cholesterol (HDL) level. |
Discussion
Key Results
A total of 166 patients with CD were included in the study. Adverse events occurred in 37 patients during the 52-week follow-up period (22.3%). Linear regression showed that HDL was negatively correlated with CRP and WBC counts and positively correlated with the serum albumin level. HDL was identified as a predictor of adverse outcomes at 52 weeks (AUC 0.661, p < 0.05), with an optimal cut-off value of 0.85. In addition, LASSO regression and Cox regression analyses identified HDL level as an independent risk factor for adverse events within 52 weeks in Crohn’s disease patients treated with infliximab (p = 0.022).
Interpretation
Few studies have explored the relationship between HDL and the efficacy of infliximab treatment. Our study provides crucial evidence supporting HDL’s predictive value in this context. In our analysis, linear regression revealed a negative correlation between HDL and both CRP (r=−0.323, P < 0.001) and WBC (r=−0.175, p =0.024), consistent with findings by Yan Zhang et al.20 CRP and WBC are widely recognized as markers of inflammation, with their serum levels significantly elevated during inflammatory responses.21 HDL has been shown to neutralize CRP’s pro-inflammatory effects in endothelial cells by oxidizing its major phospholipids, thereby preventing CRP-induced upregulation of inflammatory adhesion molecules via its phospholipid component.22 Additionally, Carol Wadham et al23 demonstrated that HDL significantly inhibits CRP-induced protein and mRNA expression of E-selectin, intercellular adhesion molecule, and vascular cell adhesion molecule. Furthermore, HDL has been shown to inhibit monocyte and neutrophil production by mediating cholesterol efflux from bone marrow haematopoietic stem and progenitor cells, reducing leukocyte proliferation.24 Moreover, linear regression also revealed a positive correlation between serum HDL and albumin levels (r=0.302, p< 0.001). Albumin, an endogenous protein with potent antioxidant and immunomodulatory properties, serves as a crucial regulator of systemic homeostasis.25 Albumin can bind to advanced oxidation protein products (AOPP), and the AOPP-albumin complex can effectively block HDL’s scavenger receptor class B type I, reducing plasma HDL clearance rates.26 In summary, HDL may interact directly or indirectly with CRP, WBC, and serum albumin, providing a plausible explanation for the observed correlations between these parameters and HDL.
In this study, HDL was identified as an independent risk factor for infliximab treatment outcomes in patients with CD, potentially due to two primary factors. First, the anti-inflammatory properties of HDL merit consideration. In our previous study, we observed an inverse correlation between HDL levels and inflammatory status in patients with IBD. Furthermore, experiments in a mouse model demonstrated that inhibition of cholesteryl ester transfer protein (CETP) may promote anti-inflammatory reprogramming of macrophages and enhance intestinal barrier function, potentially through induction of the transcriptional repressor ATF314 Moreover, apolipoprotein A-I (ApoA-I), the primary component of HDL, mediates the removal of membrane cholesterol and may influence antigen presentation and the induction of adaptive immune responses.27 Dominic De Nardo et al demonstrated that HDL exerts a broad anti-inflammatory effect by downregulating the expression of proinflammatory cytokines induced by Toll-like receptors through the transcriptional regulator Activating Transcription Factor 3.28 A high inflammatory burden at the initiation of infliximab therapy has been associated with reduced treatment efficacy.29 A higher baseline serum HDL level may predict a lower pretreatment inflammatory burden, as evidenced by its negative correlation with inflammatory markers such as CRP and WBC, suggesting a more favourable therapeutic response and a reduced incidence of adverse events. Second, the formation of anti-drug antibodies (ADA) plays a crucial role. ADA formation is one of the key causes of infliximab treatment failure, as it not only reduces therapeutic efficacy but also increases the risk of adverse events.30 Related studies have demonstrated that following the activation of innate immunity, the infliximab-tumor necrosis factor complex can stimulate the production of ADA within the gut,31 HDL, on the other hand, may play a role in regulating the complement system and innate immunity by inhibiting the formation of the peripheral complement complex,11,13,32,33 which could indirectly reduce ADA formation. Furthermore, serum albumin levels have been linked to IFXtransport, with lower serum albumin associated with a shorter IFX half-life and increased IFX clearance.34 Pharmacokinetic assessments have revealed that patients with reduced serum albumin levels exhibit undetectably low early IFX trough levels, thereby increasing their risk of ADA development.35 As HDL is positively correlated with serum albumin, low baseline HDL levels may indirectly indicate a higher risk of ADA formation in IFX-treated patients.
Recently, several biomarkers have been proposed as potential predictors of infliximab efficacy. For instance, Lin et al10 reported that the ratio of serum triiodothyronine to thyroxine (fT3/fT4) could identify patients with primary nonresponse to anti-TNF therapy; however, its clinical utility is constrained by low accuracy. Additionally, Pesole et al36 demonstrated a positive correlation between 90K (a ligand of galectin-2) and serum CRP levels (R = 0.42, p= 0.0032); despite this, 90K has not been adopted in clinical practice due to the weak strength of this association. Similarly, the neutrophil/albumin ratio (NAR) and neutrophil/bilirubin ratio (NBR) have shown potential in distinguishing infliximab responders from primary nonresponders, but these results are yet to be validated in long-term clinical trials.37 Our study suggests that HDL may serve as a simpler and more cost-effective biomarker for predicting infliximab efficacy in Crohn’s disease. Compared with these emerging biomarkers, HDL offers advantages in terms of convenience, accessibility, and widespread availability. If our findings are validated through further clinical trials, the predictive utility of HDL could provide a convenient and cost-effective approach for patients.
Limitations of the Study
However, our study has several limitations. First, the exclusive recruitment of all participants from a single center, rather than from multiple centers or the general population, along with the relatively small sample size, limits the generalizability of our findings. Secondly, the observational nature of this retrospective analysis constrains causal inference and precise temporal sequence establishment. Thirdly, our study did not address the ethnicity of the enrolled patients or the homogeneity of the sample, which represents another limitation. Additionally, the analysis should have accounted for additional variables such as albumin levels, steroid use, and immunomodulator use at baseline, which represents another limitation of this study. Lastly, while HDL shows promise in predicting adverse events, its broader application and clinical utility need to be validated through large-scale, multicenter, prospective clinical trials.
Conclusion
Based on our findings, HDL is an independent risk factor for poor prognosis in CD patients treated with IFX and shows promise as a biomarker for treatment response. However, this finding requires validation through larger, multicenter, prospective clinical studies.
Abbreviations
HDL, high density lipoprotein; IFX, infliximab; CD, Crohn’s disease; IBD, inflammatory bowel disease; WBC, white blood cell; CRP, C-reactive protein; IQR, interquartile ranges; ROC, receiver operating characteristic; AUC, area under the curve; AOPP, advanced oxidation protein products; ADA, anti-drug antibodies.
Data Sharing Statement
All the data included in this study are available upon request by contacting the corresponding author.
Ethical Considerations
The research study was conducted according to the guidelines stipulated in the Declaration of Helsinki and was approved by the ethical committee of Xiangya Hospital of Central South University (No. 202108158). We have obtained published written informed consent from the patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82070651).
Disclosure
The authors have no relevant financial or non financial interests to disclose.
References
1. Kaplan GG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12(12):720–727. doi:10.1038/nrgastro.2015.150
2. Glassner KL, Abraham BP, Quigley EMM. The microbiome and inflammatory bowel disease. J Allergy Clin Immunol. 2020;145(1):16–27. doi:10.1016/j.jaci.2019.11.003
3. Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology. 2010;139(4):1147–1155. doi:10.1053/j.gastro.2010.06.070
4. Druvefors E, Myrelid P, Andersson RE, Landerholm K. Female and male fertility after colectomy and reconstructive surgery in inflammatory bowel disease: a national cohort study from Sweden. J Crohns Colitis. 2023;17(10):1631–1638. doi:10.1093/ecco-jcc/jjad079
5. Olaison G, Smedh K, Sjödahl R. Natural course of Crohn’s disease after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut. 1992;33(3):331–335. doi:10.1136/gut.33.3.331
6. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389(10080):1741–1755. doi:10.1016/S0140-6736(16)31711-1
7. Keating GM, Perry CM. Infliximab: an updated review of its use in Crohn’s disease and rheumatoid arthritis. BioDrugs. 2002;16(2):111–148. doi:10.2165/00063030-200216020-00005
8. Singh S, Murad MH, Fumery M, et al. Comparative efficacy and safety of biologic therapies for moderate-to-severe Crohn’s disease: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(12):1002–1014. doi:10.1016/S2468-1253(21)00312-5
9. Kennedy NA, Heap GA, Green HD, et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: a prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol. 2019;4(5):341–353. doi:10.1016/S2468-1253(19)30012-3
10. Lin S, Chanchlani N, Carbery I, et al. Understanding anti-TNF treatment failure: does serum triiodothyronine-to-thyroxine (T3/T4) ratio predict therapeutic outcome to anti-TNF therapies in biologic-naïve patients with active luminal Crohn’s disease? Aliment Pharmacol Ther. 2022;56(5):783–793. doi:10.1111/apt.17089
11. Vermeire S, Van Assche G, Rutgeerts P. Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut. 2006;55(3):426–431. doi:10.1136/gut.2005.069476
12. Li Y, Pan J, Zhou N, et al. A random forest model predicts responses to infliximab in Crohn’s disease based on clinical and serological parameters. Scand J Gastroenterol. 2021;56(9):1030–1039. doi:10.1080/00365521.2021.1939411
13. Sina C, Kemper C, Derer S. The intestinal complement system in inflammatory bowel disease: shaping intestinal barrier function. Semin Immunol. 2018;37:66–73. doi:10.1016/j.smim.2018.02.008
14. Wang X, Li X, Liu K, et al. Targeting to high density lipoprotein cholesterol: new insights for inflammatory bowel disease treatment. J Lipid Res. 2025;66(7):100836. doi:10.1016/j.jlr.2025.100836
15. Gerster R, Eloranta JJ, Hausmann M, et al. Anti-inflammatory function of high-density lipoproteins via autophagy of IκB kinase. Cell Mol Gastroenterol Hepatol. 2015;1(2):171–187.e171. doi:10.1016/j.jcmgh.2014.12.006
16. Voutilainen M, Hutri-Kähönen N, Tossavainen P, et al. Low childhood high density lipoprotein cholesterol levels and subsequent risk for chronic inflammatory bowel disease. Dig Liver Dis. 2018;50(4):348–352. doi:10.1016/j.dld.2018.01.121
17. Liu Z, Tang H, Liang H, et al. Dyslipidaemia is associated with severe disease activity and poor prognosis in ulcerative colitis: a retrospective cohort study in China. Nutrients. 2022;14(15):3040 doi:10.3390/nu14153040..
18. Khera AV, Cuchel M, de la Llera-Moya M, et al. Cholesterol efflux capacity, high-density lipoprotein function, and atherosclerosis. N Engl J Med. 2011;364(2):127–135. doi:10.1056/NEJMoa1001689
19. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359(9317):1541–1549. doi:10.1016/S0140-6736(02)08512-4
20. Zhang Y, Li S, Xu RX, et al. Systemic inflammatory markers are closely associated with atherogenic lipoprotein subfractions in patients undergoing coronary angiography. Mediators Inflamm. 2015;2015:235742. doi:10.1155/2015/235742
21. Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation. 2005;111(25):3481–3488. doi:10.1161/CIRCULATIONAHA.105.537878
22. Vales-Villamarín C, de Dios O, Pérez-Nadador I, Gavela-Pérez T, Soriano-Guillén L, Garcés C. Sex-dependent relationship of C-reactive protein levels with HDL-cholesterol and HDL-phospholipid concentrations in children. Sci Rep. 2022;12(1):3214. doi:10.1038/s41598-022-07271-8
23. Wadham C, Albanese N, Roberts J, et al. High-density lipoproteins neutralize C-reactive protein proinflammatory activity. Circulation. 2004;109(17):2116–2122. doi:10.1161/01.CIR.0000127419.45975.26
24. Groenen AG, Bazioti V, van Zeventer IA, et al. Large HDL particles negatively associate with leukocyte counts independent of cholesterol efflux capacity: a cross sectional study in the population-based LifeLines DEEP cohort. Atherosclerosis. 2022;343:20–27. doi:10.1016/j.atherosclerosis.2022.01.008
25. Bernardi M, Angeli P, Claria J, et al. Albumin in decompensated cirrhosis: new concepts and perspectives. Gut. 2020;69(6):1127–1138. doi:10.1136/gutjnl-2019-318843
26. Marsche G, Frank S, Hrzenjak A, et al. Plasma-advanced oxidation protein products are potent high-density lipoprotein receptor antagonists in vivo. Circ Res. 2009;104(6):750–757. doi:10.1161/CIRCRESAHA.108.193169
27. Barter PJ, Nicholls S, Rye KA, Anantharamaiah GM, Navab M, Fogelman AM. Antiinflammatory properties of HDL. Circ Res. 2004;95(8):764–772. doi:10.1161/01.RES.0000146094.59640.13
28. De Nardo D, Labzin LI, Kono H, et al. High-density lipoprotein mediates anti-inflammatory reprogramming of macrophages via the transcriptional regulator ATF3. Nat Immunol. 2014;15(2):152–160. doi:10.1038/ni.2784
29. Magro F, Rodrigues-Pinto E, Santos-Antunes J, et al. High C-reactive protein in Crohn’s disease patients predicts nonresponse to infliximab treatment. J Crohns Colitis. 2014;8(2):129–136. doi:10.1016/j.crohns.2013.07.005
30. Bots SJ, Parker CE, Brandse JF, et al. Anti-drug antibody formation against biologic agents in inflammatory bowel disease: a systematic review and meta-analysis. BioDrugs. 2021;35(6):715–733. doi:10.1007/s40259-021-00507-5
31. Bar-Yoseph H, Pressman S, Blatt A, et al. Infliximab-tumor necrosis factor complexes elicit formation of anti-drug antibodies. Gastroenterology. 2019;157(5):1338–1351.e1338. doi:10.1053/j.gastro.2019.08.009
32. Heinecke JW. The HDL proteome: a marker--and perhaps mediator--of coronary artery disease. J Lipid Res. 2009;50 Suppl(Suppl):S167–171. doi:10.1194/jlr.R800097-JLR200
33. Norata GD, Pirillo A, Ammirati E, Catapano AL. Emerging role of high density lipoproteins as a player in the immune system. Atherosclerosis. 2012;220(1):11–21. doi:10.1016/j.atherosclerosis.2011.06.045
34. Hemperly A, Vande Casteele N. Clinical pharmacokinetics and pharmacodynamics of infliximab in the treatment of inflammatory bowel disease. Clin Pharmacokinet. 2018;57(8):929–942. doi:10.1007/s40262-017-0627-0
35. Brandse JF, Mould D, Smeekes O, et al. D’Haens GR: a real-life population pharmacokinetic study reveals factors associated with clearance and immunogenicity of infliximab in inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(4):650–660. doi:10.1097/MIB.0000000000001043
36. Pesole PL, Liso M, Donghia R, et al. 90K/Mac-2 BP is a new predictive biomarker of response to infliximab therapy in IBD patients. Int J Mol Sci. 2023;24(4):3955. doi:10.3390/ijms24043955
37. Zhou Z, Zhang Y, Yang X, et al. Clinical significance of novel neutrophil-based biomarkers in the diagnosis and prediction of response to infliximab therapy in Crohn’s disease. Front Immunol. 2022;13:865968. doi:10.3389/fimmu.2022.865968
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.