")
Back to Journals » Clinical Ophthalmology » Volume 17
The Phase 3 INVIGORATE Trial of Reproxalap in Patients with Seasonal Allergic Conjunctivitis
Authors Starr CE, Nichols KK , Lang JR, Brady TC
Received 21 September 2023
Accepted for publication 29 November 2023
Published 13 December 2023 Volume 2023:17 Pages 3867—3875
DOI https://doi.org/10.2147/OPTH.S441009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Christopher E Starr,1 Kelly K Nichols,2 Jacob R Lang,3 Todd C Brady4
1Department of Ophthalmology, Weill Cornell Medicine, New York, NY, USA; 2School of Optometry, University of Alabama, Birmingham, AL, USA; 3College of Optometry, the Ohio State University, Columbus, OH, USA; 4Aldeyra Therapeutics, Lexington, MA, USA
Correspondence: Todd C Brady, Aldeyra Therapeutics, 131 Hartwell Avenue, Suite 320, Lexington, MA, 02421, USA, Email [email protected]
Purpose: There is an unmet need for new treatments for allergic conjunctivitis.
Objective: To assess the activity of reproxalap, a novel reactive aldehyde species modulator, in a real-world model of seasonal allergen exposure.
Methods: The INVIGORATE Trial, a prospective, quadruple-masked, vehicle-controlled, crossover, sequence-randomized Phase 3 trial, tested the efficacy of reproxalap in adults with a history of moderate to severe allergic conjunctivitis, ragweed pollen allergy, and allergen chamber-induced ocular itching and redness. Patients were randomly assigned (1:1) to receive 0.25% reproxalap ophthalmic solution or vehicle, followed by a 2-week washout period before crossing over to the other test article. The primary endpoint was ocular itching from 110 to 210 minutes after chamber entry; the key secondary endpoint was ocular redness over the chamber duration (0– 4 scales for both endpoints).
Results: Of the 95 randomly assigned patients, 89 completed all visits (reproxalap to vehicle: n = 46; vehicle to reproxalap: n = 43). Primary and key secondary endpoints were met: reproxalap significantly reduced ocular itching (mean [SE]: − 0.50 [0.03], p < 0.001) and redness (− 0.14 [0.01], p < 0.001) relative to vehicle. Responder analyses confirmed the clinical relevance of both end points. Reproxalap was safe and well tolerated. No clinically significant changes in safety assessments were observed. No serious or severe treatment-emergent adverse events (TEAEs) were reported. The most commonly reported TEAE was mild and transient installation site irritation after reproxalap versus vehicle administration.
Conclusion: In this well-controlled allergen chamber trial, reproxalap was statistically superior to vehicle across typical symptoms and signs of allergic conjunctivitis.
Trial Registration: NCT04207736.
Keywords: allergic conjunctivitis, reactive aldehyde species, reproxalap, ocular itching, ocular redness
Introduction
Reproxalap, a novel chemical entity in late-stage clinical development for the treatment of ocular inflammation, chemically sequesters a class of small molecules known as reactive aldehyde species (RASP). Via covalent binding to amine and thiol residues, RASP modulate the structure and function of proteins in an analog manner1 depending on the amount of binding, and are upregulated during inflammation before cytokine release, leading to the potentiation of nuclear factor kappa B, inflammasomes, and other proteins.2,3 RASP are associated with the systemic and ocular allergic response,4,5 and RASP-mediated induction of inflammation facilitates the post-histaminic pathology of allergy, including cellular infiltrate and other sub-acute physiological characteristics of allergic conjunctivitis.6 By targeting RASP, reproxalap represents a first-in-class therapeutic approach that does not directly activate or inhibit a specific protein, but rather indirectly modulates systems of proteins involved in the inflammatory cascade. The systems-based mechanism of action of reproxalap affords a theoretical advantage of pluripotent utility in inflammatory ocular disease broadly, reflected not only in allergic conjunctivitis,7–9 but also noninfectious anterior uveitis10 and dry eye disease.11,12
Despite an increasing prevalence of allergic conjunctivitis that includes more than 20% of the US population,13 drugs to treat allergic conjunctivitis with novel mechanisms of action have not been introduced in decades. Furthermore, although most patients with allergic conjunctivitis are treated at least initially with topical antihistamines, the need for adjunctive therapy is common. For example, in one study, up to 60% of patients required non-antihistaminic medication,14 which often includes topical corticosteroids, a class of drugs associated with potentially serious ocular toxicity including elevation of intraocular pressure and development of glaucoma.15
Topical conjunctival allergen challenge has typically been used in development of allergic conjunctivitis drugs.7 However, the clinical relevance of applying concentrated allergen to the ocular surface can be questioned, and the assessment of duration of drug activity after challenge is often limited to less than 10 minutes,16 possibly due to waning drug effect resulting from rapidly declining histamine levels, which peak within 5 to 10 minutes of allergen exposure.17 Investigational allergic conjunctivitis drugs may also be tested in field trials, but exposure to pollen is variable, unpredictable, and depends heavily on weather and patient behaviors.9 Allergen chambers, on the other hand, represent a combination of direct conjunctival challenge and field trials, allowing for a controlled exposure to allergens in a simulated real-world setting. In a small, proof-of-concept clinical trial using an allergen chamber, reproxalap demonstrated preliminary activity in patient-reported symptoms and investigator-assessed ocular redness.8 Accordingly, the Phase 3 INVIGORATE Trial was performed to assess the activity of reproxalap in a real-world model of seasonal allergen exposure. Based on published clinical relevance thresholds for patient-reported ocular itching and redness,9 two different within-patient responder analysis methods were used to confirm the clinical relevance of the results.
Materials and Methods
Trial Design
Patients with seasonal allergic conjunctivitis were enrolled in the single-center, crossover, placebo-controlled, sequence-randomized, quadruple-masked (patient, care provider, outcomes assessor, investigator) Phase 3 INVIGORATE Trial. The trial was performed in Canada (Cliantha Research, Mississauga, Ontario) in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Patients, the International Council for Harmonization Guideline on Good Clinical Practice, and all applicable local regulatory requirements and laws. Institutional review board (IRB)/ethics committee approval was obtained from Advarra, Inc. (Columbia, MD, USA). Informed consent was obtained from the patients, and the research followed Health Insurance Portability and Accountability Act and Personal Information Protection and Electronic Documents Act regulations. The clinical trial is registered in the National Library of Medicine database (http://www.clinicaltrials.gov; NCT04207736).
The trial was designed to evaluate the activity and clinical utility of 0.25% topical ocular reproxalap relative to vehicle. Patients were exposed to ambient aerosolized ragweed pollen in an allergen chamber for 3.5 hours, which approximates the average maximum duration of allergen exposure that patients are generally willing to withstand. As described previously,18 commercially obtained ragweed pollen (Ambrosia artemesiifolia; Greer Laboratories, Lenoir, NC, USA) was aerosolized in HEPA-filtered fresh air and maintained at 3500 ± 500 grains/m3 with rigorous temperature and humidity controls.
The trial consisted of four visits: a medical screening visit that included ragweed pollen skin testing; an allergen chamber exposure qualification visit to elicit conjunctival redness and itching; and 2 treatment visits during which patients were treated topically with one drop of test article in each eye within 5 minutes before chamber entry and again 90 minutes after chamber entry, when peak symptoms are typically apparent. The second dose was designed to recapitulate a typical patient-driven scenario during prolonged symptomatic antigen exposure. All allergen chamber visits were separated by 2 weeks ± 3 days. Patients were randomly assigned (1:1) via a predetermined randomization sequence to one of two sequences for the test article visits: reproxalap then placebo or placebo then reproxalap. Reproxalap and vehicle were matched in volume and appearance, and patients and investigators were masked to treatment assignment throughout the trial.
Patient Population
As previously described,8 adult patients aged ≥18 years with a history of ≥2 years of moderate to severe allergic conjunctivitis, a positive skin test result (≥3 mm) for ragweed pollen, and chamber-induced ocular itching and redness scores of ≥2.5 and ≥2 (both scales range from 0 to 4), respectively, were eligible. Patients were excluded for any clinically significant slit lamp findings or a history of inflammatory or infectious disease that could interfere with the conduct of the trial. Other exclusions were use of antihistamines within 7 days before screening and use of corticosteroid or immunotherapeutic agents within 14 days before screening. Patients were excluded or deferred to a later visit if ocular itching and redness scores were >0.5 or >1, respectively, in either eye before any allergen chamber visit.
Study Assessments and Endpoints
Ocular itching and tearing scores were recorded by patients using an electronic tablet at approximately 2, 7, 12, 17, 22, 32, 42, 52, 72, 92, 97, 102, 107, 112, 122, 132, 142, 152, 172, 192, and 212 minutes after chamber entry on a scale ranging from 0 (no itching) to 4 (severe), allowing half-unit increments, for itching and from 0 (no tearing) to 3 (severe) for tearing. On a similar schedule offset by at least 3 minutes, for the nasal and temporal aspect of each eye, trained technicians visually assessed conjunctival redness without a slit lamp based on a validated descriptive and photographic redness scale from 0 (none) to 4 (severe) with 0.5 increments.19 Similar assessments of ocular itching, tearing, and redness were performed at approximately 2, 7, 12, 17, 22, 32, 42, and 62 minutes after chamber exit. Safety assessments were visual acuity, slit lamp biomicroscopy, undilated fundoscopy, intraocular pressure (non-contact intraocular pressure tonometry), and adverse events. Patients were monitored for symptoms and signs of asthma or other conditions that could affect study conduct or interpretation.
Statistical Analysis
The primary endpoint was change from baseline in ocular itching score from 110 to 210 minutes after chamber entry. Achievement of the endpoint necessitated that ocular itching for the majority of prespecified time points during the 110 to 210 minutes after chamber entry was statistically significantly lower in reproxalap-treated patients than in vehicle-treated patients. The key secondary end point was change from baseline in ocular redness, averaged across both regions and both eyes, over the duration of the chamber. Achievement of the key secondary end point necessitated that, across all chamber time points assessed in aggregate, ocular redness was statistically significantly lower in reproxalap-treated patients than in vehicle-treated patients. The additional secondary endpoint was ocular tearing score over the duration of the chamber.
Assuming a treatment difference from vehicle of 0.5 units in itching score change from baseline, and assuming an estimated standard deviation of 1.35 units, a sample size of 100 participants provided a power of 96% at 2-sided significance level of 0.05 for a crossover design. Mixed-effect models for repeated measures (MMRM) were used to assess each endpoint, with sequence, visit, treatment group, time after chamber entry, and the interaction of treatment group and time as factors. Baseline was defined as the average of scores just before chamber entry. Rank-based nonparametric testing for longitudinal data was used as a sensitivity analysis for the MMRM assessments.20 To assess clinical relevance, based on previously reported clinical relevance threshold estimates of 0.5 units for ocular itching and redness,9 within-patient (reproxalap minus vehicle) time to ocular itching and redness scores of ≥0.5 in the allergen chamber were calculated and compared via 1-way t test to 0 (no difference between reproxalap and vehicle). Binomial generalized estimating equation (GEE) modeling with the same factors as the MMRM analyses was used to assess differences in 0.5-unit responder proportions over the duration of the chamber for ocular itching and redness. Safety assessments were characterized with summary statistics.
Results
Patient Disposition and Characteristics
Patient disposition is diagrammed in Figure 1. A total of 568 patients with allergic conjunctivitis were screened, and 95 were randomly assigned and treated between October 15, 2019, and February 16, 2021. As is typical with allergen chamber trials, the high rate of screening failures was due to exclusions related to allergen chamber itching and redness requirements, potentially reflecting perennial allergy or clinically insignificant ocular allergy to ragweed. There were 6 discontinuations: 3 patients were discontinued because of protocol violations (vehicle to reproxalap sequence), 1 patient voluntarily withdrew (vehicle to reproxalap sequence), 1 patient was discontinued because of scheduling conflicts (reproxalap to vehicle sequence), and 1 patient was lost to follow up (reproxalap to vehicle sequence). Eighty-nine patients completed all treatment periods. Baseline demographic characteristics were generally comparable across sequence groups (Supplemental Table 1); patients identifying as white represented approximately half of the enrolled population, and patients identifying as Asian or Black each represented approximately 20% of the enrolled population.
 |
Figure 1 Patient disposition. N = number of randomly assigned patients in the population; n = number of patients with data. |
Efficacy
The primary endpoint of ocular itching was achieved: relative to vehicle, treatment with reproxalap led to lower levels of patient-reported ocular itching at all prespecified time points (Figure 2; p < 0.001 for each time point; Supplemental Table 2).
 |
Figure 2 Patient-reported ocular itching score. P value derived from MMRM analysis of change from baseline (just prior to chamber entry) over all time points in aggregate. MMRM = mixed-effect model for repeated measures. |
The key secondary endpoint of investigator-assessed conjunctival redness (Figure 3; p < 0.001; Supplemental Table 2) and the secondary endpoint of patient-reported ocular tearing (Figure 4; p < 0.001; Supplemental Table 2) were also achieved. Non-parametric assessments confirmed the MMRM results (Supplemental Table 2). Escalation of symptoms and redness after prechamber dosing was blunted with reproxalap. Although treatment with both reproxalap and vehicle during the chamber arrested the increase in symptoms and redness, scores after reproxalap treatment remained lower than those after vehicle treatment over the duration of the chamber, as well as over all time points after chamber exit.
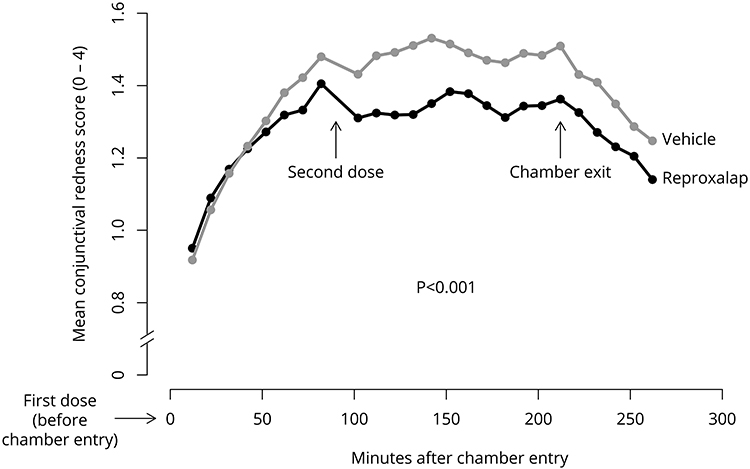 |
Figure 3 Investigator-assessed conjunctival redness score. P value derived from MMRM analysis of change from baseline (just before chamber entry) over all time points in aggregate. MMRM = mixed-effect model for repeated measures. |
 |
Figure 4 Patient-reported ocular tearing score. P value derived from MMRM analysis of change from baseline (just prior to chamber entry) over all time points in aggregate. MMRM = mixed-effect model for repeated measures. |
Clinical Relevance Assessments
Within-patient time to increase of 0.5 points9 for ocular itching (reproxalap minus vehicle mean, 14.7; 95% CI, 4.6–24.8; p = 0.005) and redness (reproxalap minus vehicle mean, 22.1; 95% CI, 2.5–41.7; p = 0.028) in the allergen chamber was longer after reproxalap treatment than after vehicle treatment (Figure 5). The time to event analyses were confirmed with 0.5-unit GEE responder proportions over the duration of the chamber for ocular itching (Supplemental Figure 1; odds ratio [OR], 0.53; 95% CI, 0.35–0.81; p = 0.003) and redness (Supplemental Figure 2; OR, 0.58; 95% CI, 0.39–0.85; p = 0.005), indicating that patients were more likely to demonstrate an increase of 0.5 points after vehicle treatment than after reproxalap.
 |
Figure 5 Mean (± 95% CI) within-patient time to patient-reported ocular itching and investigator-assessed redness score of 0.59 (scale 0–4) for reproxalap minus vehicle during the allergen chamber. P values derived from 1-way t test versus 0 (no difference between reproxalap and vehicle). |
Safety and Tolerability
Reproxalap was considered safe and well tolerated. No clinically significant changes in visual acuity readings, fundus assessments, vital signs, or clinical laboratory parameters were observed with reproxalap. No serious or severe treatment-emergent adverse events (TEAEs) were reported, and no participants were discontinued or withdrew because of a TEAE. The most commonly reported TEAE was mild and transient installation site irritation, reported in 66 patients (69%) after reproxalap administration and in 4 patients (4%) after vehicle administration. Other TEAEs were infrequent and were reported by two or fewer patients following exposure to each treatment (lacrimation, eyelid swelling, pruritis, pain, hyperemia, asthenopia) except for transient and predominantly mild chemosis, which was observed in 8 patients (8.8%) following reproxalap treatment.
Discussion
The INVIGORATE Trial demonstrated rapid and sustained activity of reproxalap in diminishing ocular symptoms and redness in patients with allergic conjunctivitis over a period of 3.5 hours in an allergen chamber (Figures 2–4; p < 0.001 for all assessments). The results are consistent with the activity of reproxalap reported in a field trial, a small proof-of-concept allergen chamber trial, and the Phase 3 ALLEVIATE conjunctival challenge trial in patients with allergic conjunctivitis.7–9 Approximately half the patients with ocular itching, the principal symptom of allergic conjunctivitis, also report ocular dryness, the principal symptom of dry eye disease, suggesting a strong relationship between the two conditions.21 Therefore, the activity of reproxalap in allergic conjunctivitis may also be consistent with reported results in dry eye disease clinical trials.11,12
The clinical relevance analyses for INVIGORATE were exclusively within-patient and used an empirically derived clinical relevance threshold of 0.5 units (0–4 scale) for ocular itching and redness.9 Although intra-chamber escalation to 0.5 units occurred in most patients with regard to ocular itching and in fewer patients with regard to ocular redness, time to response (Figure 5) and GEE responder proportion (Supplemental Figures 1 and 2) analyses, two distinct though possibly correlated statistical methods, statistically favored reproxalap over vehicle for ocular itching (p = 0.005 and p = 0.003, respectively) and redness (p = 0.028 and p = 0.005, respectively). The results suggest that the treatment group differences in changes observed in the allergen chamber were likely meaningful to individual patients. However, clinical utility analyses are limited by the notion that patients are generally not concerned with changes relative to vehicle, but rather changes relative to baseline. Because the change from baseline is larger than that of the change across treatment groups, it is possible that in a real-world treatment setting, patients with allergic conjunctivitis could recognize clinical improvement in ocular itching and redness after reproxalap administration.
Reproxalap is a new chemical entity directed toward the novel pharmaceutical target of RASP, thereby effecting a unique pharmacology distinct from the single-drug, single-protein pharmacology that makes up nearly all of the current therapeutic landscape. Although much of the activity of RASP has been attributed to activation of classic proinflammatory mediators,2,3 RASP theoretically bind any protein with accessible amine and thiol moieties,1 and thus likely modulate the activity of proteins not directly associated with inflammation. Therefore, the rapid activity of reproxalap in the allergen chamber may not exclusively represent immune-modulating activity. For example, RASP have been shown to mediate nociceptive transient receptor potential (TRP) receptor family and vasomotor function,22,23 which could account in part for the symptomatic and redness activity of reproxalap, respectively. However, acute RASP modulation is unlikely to explain long-term activity observed in noninfectious anterior uveitis and dry eye disease clinical trials lasting weeks,10,12 allowing for the possibility that the activity of reproxalap may include distinct acute non–immune-modulating and long-term immune-modulating mechanisms of action.
The drop comfort of reproxalap more than one hour after instillation was previously characterized,24 and in most patients, includes mild instillation-associated irritation, followed by soothing sensations. This is consistent with the INVIGORATE results in which symptom responder rates were superior to those of vehicle, yet more than half the patients reported initial, mild transient irritation. Because TRP receptors modulate nociception and soothing sensations and are intimately regulated by RASP,22 TRP receptor modulation may explain the post-instillation experience observed in INVIGORATE and other trials of reproxalap. If reproxalap does modulate the TRP family, then the significant number of patients who do not report post-instillation irritation (approximately 30%) is puzzling and may be a result of lack of reporting, neurobiological corneal sensation differences from patient to patient, or the presence of mild forms of diseases in which sensation is diminished, such as neurotrophic keratitis. However, post hoc analyses indicated that ocular itching and redness were not different across patients who reported post-instillation irritation versus those who did not (data not shown).
Surprisingly, given the significant incidence of allergic conjunctivitis, new mechanisms of action for treatment have not been introduced in decades. Although topical antihistamines are considered standard of care for allergic conjunctivitis, the most common reports submitted to the US Food and Drug Administration Adverse Event Reporting System database for topical antihistamine monotherapy (olopatadine, ketotifen, alcaftadine, epinastine, and bepotastine) are “treatment failure” (45%) and “drug ineffective” (17%),25 which may partially explain why polypharmacy is common in allergic conjunctivitis.14 Histamine is rapidly metabolized and likely peaks soon after allergen exposure, thereby limiting the duration of activity of antihistamines.17 Furthermore, many non-histaminic mediators likely contribute to the clinical presentation of ocular allergy.6 Because of toxicity concerns,15 corticosteroids can only be safely used on a short-term basis. Therefore, novel treatments are needed. The data reported herein suggest that use of the novel RASP modulator reproxalap may be an effective treatment for the symptoms and signs of allergic conjunctivitis. By extension, based on the activity reported herein, RASP modulation may represent a potential therapeutic approach for other allergic diseases.
Additional studies on the mechanism of reproxalap and the pathophysiologic activity of RASP in allergy are warranted. Limitations of the current clinical trial include the use of a single site (the allergen chamber), though the number of validated allergen chambers available for clinical testing worldwide is limited. Exposure was restricted to a single allergen (ragweed) considered representative of seasonal allergy, and it is theoretically possible that exposure to perineal allergens could yield different results. Due to dilution of allergen exposure and potential clearance of allergen from the ocular surface, any ophthalmic solution or suspension will likely demonstrate at least some activity in allergen chamber trials, as was evidenced by the intra-chamber dose of vehicle. Further, although post-instillation site irritation was transient and generally resolved prior to chamber entry, thereby precluding the need for additional measures to prevent unblinding of technicians in the chamber, patients may have noticed a difference in irritation between vehicle and reproxalap administration, which could have affected patient blinding and symptom reporting. However, instillation site irritation is common with topical ocular drugs and represents an unavoidable consequence of using ophthalmic solutions in clinical trials. Had irritation persisted after chamber entry, itching and redness scores may have been higher following reproxalap administration than with vehicle administration, in contrast to the results. Future trials may include active controls, such as antihistamines, although comparison to antihistamines is of limited clinical relevance since topical antihistamines are now available without prescription and many patients seeking medical assistance have already failed antihistamine therapy. Finally, consensus recommendations regarding the utility of allergen chambers in drug development have been summarized,26 and include the importance of confirmatory field trials and other challenge models, as have been described with reproxalap.7,9
Data Sharing Statement
Due to commercial and legal restrictions, supporting data is not available.
Acknowledgments
Data included in this manuscript were presented at the 2022 Annual Meeting of the American Academy of Optometry; October 26–29, 2022; San Diego, CA, USA.
Funding
This study was supported by Aldeyra Therapeutics, Inc., Lexington, MA, USA. The sponsor participated in the design and implementation of the study, the analysis and interpretation of the data, and the preparation, review, and approval of the manuscript.
Disclosure
The authors have made the following disclosures: C.E.S.: Consultant – Novartis, Allergan, TearLab, Sun Pharma, Bruder, BlephEx, Kala Pharmaceuticals, Quidel, Dompe, Johnson & Johnson Vision, Essiri Labs, Tarsus Pharmaceuticals, Oyster Point Pharma, Visionology, CSI Dry Eye, Aerie, Eyebiotech, Versea, Bausch & Lomb and Aldeyra Therapeutics; Stock ownership – Essiri Labs and Visionology. K.K.N.: Consultant – Allergan/AbbVie, Axim, Aerie, Alcon, Alderya, Azura, Bruder, Bausch + Lomb, Cavalry, Dompe, HanAll Biopharma, Kala Pharmaceuticals, Novartis, Shire, Takeda, Nicox, Novaliq, Palatin, Osmotica/RVL, Oyster Point Pharma, Sight Sciences, Sun Pharma, Thea, Tarsus Pharmaceuticals, Topivert, Trukera, Versea, Visionology, and Xequel; Research: Science Based Health, TearScience, Sylentis, Kowa, and Aramis; Grants – Allergan, Kala Pharmaceuticals, NIH, and TearScience; Stock ownership – Alcon Vision/Tear Film Innovations, Axim, and Visionology. She also reports consulting (last 2 years) in the area of Dry Eye/MGD (not ocular allergy) for Abbvie, Allergan, Aerie, Alcon, Axim, Alderya, Azura, Bausch + Lomb Bruder, Cavalry, Dompe, HanAll Bio, Novartis, Shire, Takeda, Osmotica, RVL, Nicox, Novaliq, Oyster Point Pharma, Palatin, Thea, Tarsus, TopiVert, TearSolutions, Trukera, Versea, Xequel; Research for Science Based Health, TearScience, Sylentis, Kowa, and Aramis. J.R.L.: Consultant — Alcon, AscuelaTech, Allergan/AbbVie, Avellino, Aldeyra, Dompé, Envision Biomedical, Kala, Novartis, AOS, Scope, Sight Sciences, Sun Pharma, Tarsus, Quidel, Horizon, Aerie, Ocular Therapeutix, Trukera, Orasis, Oyster Point, Viatris, and Zeiss. T.C.B. Employee – Aldeyra Therapeutics; Patent interests (US11197821 and US9687481) – Aldeyra Therapeutics; Stock ownership – Aldeyra Therapeutics and Evoke Pharma. The authors report no other conflicts of interest in this work.
References
1. Higdon A, Diers AR, Oh JY, et al. Cell signalling by reactive lipid species: new concepts and molecular mechanisms. Biochem J. 2012;442(3):453–464. doi:10.1042/bj20111752
2. Kalariya NM, Ramana KV, Srivastava SK, et al. Carotenoid derived aldehydes-induced oxidative stress causes apoptotic cell death in human retinal pigment epithelial cells. Exp Eye Res. 2008;86(1):70–80. doi:10.1016/j.exer.2007.09.010
3. Kauppinen A, Niskanen H, Suuronen T, et al. Oxidative stress activates NLRP3 inflammasomes in ARPE-19 cells--implications for age-related macular degeneration (AMD). Immunol Lett. 2012;147(1–2):29–33. doi:10.1016/j.imlet.2012.05.005
4. Matés JM, Segura JM, Pérez-Gómez C, et al. Antioxidant enzymatic activities in human blood cells after an allergic reaction to pollen or house dust mite. Blood Cells Mol Dis. 1999;25(2):103–109. doi:10.1006/bcmd.1999.0234
5. Wakamatsu TH, Dogru M, Ayako I, et al. Evaluation of lipid oxidative stress status and inflammation in atopic ocular surface disease. Mol Vis. 2010;16:2465–2475.
6. Ackerman S, Smith LM, Gomes PJ. Ocular itch associated with allergic conjunctivitis: latest evidence and clinical management. Ther Adv Chronic Dis. 2016;7(1):52–67. doi:10.1177/2040622315612745
7. Clark D, Cavanagh B, Shields AL, et al. Clinically relevant activity of the novel RASP inhibitor reproxalap in allergic conjunctivitis: the Phase 3 ALLEVIATE Trial. Am J Ophthalmol. 2021;230:60–67. doi:10.1016/j.ajo.2021.04.023
8. Clark D, Karpecki P, Salapatek AM, et al. Reproxalap improves signs and symptoms of allergic conjunctivitis in an allergen chamber: a real-world model of allergen exposure. Clin Ophthalmol. 2022;16:15–23. doi:10.2147/opth.S345324
9. Cavanagh B, Gomes PJ, Starr CE, et al. Reproxalap activity and estimation of clinically relevant thresholds for ocular itching and redness in a randomized allergic conjunctivitis field trial. Ophthalmol Ther. 2022;11(4):1449–1461. doi:10.1007/s40123-022-00520-z
10. Mandell KJ, Clark D, Chu DS, et al. Randomized Phase 2 trial of reproxalap, a novel reactive aldehyde species inhibitor, in patients with noninfectious anterior uveitis: model for corticosteroid replacement. J Ocul Pharmacol Ther. 2020;36(10):732–739. doi:10.1089/jop.2020.0056
11. Clark D, Sheppard J, Brady TC. A randomized double-masked phase 2a trial to evaluate activity and safety of topical ocular reproxalap, a novel RASP inhibitor, in dry eye disease. J Ocul Pharmacol Ther. 2021;37(4):193–199. doi:10.1089/jop.2020.0087
12. Clark D, Tauber J, Sheppard J, et al. Early onset and broad activity of reproxalap in a randomized, double-masked, vehicle-controlled phase 2b trial in dry eye disease. Am J Ophthalmol. 2021;226:22–31. doi:10.1016/j.ajo.2021.01.011
13. Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010;126(4):778–783.e6. doi:10.1016/j.jaci.2010.06.050
14. Leonardi A, Piliego F, Castegnaro A, et al. Allergic conjunctivitis: a cross-sectional study. Clin Exp Allergy. 2015;45(6):1118–1125. doi:10.1111/cea.12536
15. McGhee CN, Dean S, Danesh-Meyer H. Locally administered ocular corticosteroids: benefits and risks. Drug Saf. 2002;25(1):33–55. doi:10.2165/00002018-200225010-00004
16. Torkildsen G, Narvekar A, Bergmann M. Efficacy and safety of olopatadine hydrochloride 0.77% in patients with allergic conjunctivitis using a conjunctival allergen-challenge model. Clin Ophthalmol. 2015;9:1703–1713. doi:10.2147/opth.S83263
17. Leonardi A. Role of histamine in allergic conjunctivitis. Acta Ophthalmol Scand Suppl. 2000;230:18–21. doi:10.1034/j.1600-0420.2000.078s230018.x
18. Rønborg SM, Mosbech H, Johnsen CR, et al. Exposure chamber for allergen challenge. The development and validation of a new concept. Allergy. 1996;51(2):82–88. doi:10.1111/j.1398-9995.1996.tb04562.x
19. Schulze MM, Jones DA, Simpson TL. The development of validated bulbar redness grading scales. Optom Vis Sci. 2007;84(10):976–983. doi:10.1097/OPX.0b013e318157ac9e
20. Noguchi K, Gel YR, Brunner E, Konietschke F. nparLD: an R software package for the nonparametric analysis of longitudinal data in factorial experiments. J Statistical Software. 2012;50(12):1–23. doi:10.18637/jss.v050.i12
21. Hom MM, Nguyen AL, Bielory L. Allergic conjunctivitis and dry eye syndrome. Ann Allergy Asthma Immunol. 2012;108(3):163–166. doi:10.1016/j.anai.2012.01.006
22. Hellenthal KEM, Brabenec L, Gross ER, et al. TRP channels as sensors of aldehyde and oxidative stress. Biomolecules. 2021;11(10). doi:10.3390/biom11101401
23. Guivernau M, Baraona E, Lieber CS. Acute and chronic effects of ethanol and its metabolites on vascular production of prostacyclin in rats. J Pharmacol Exp Ther. 1987;240(1):59–64.
24. McMullin D, Clark D, Cavanagh B, et al. A post-acute ocular tolerability comparison of topical Reproxalap 0.25% and Lifitegrast 5% in patients with dry eye disease. Clin Ophthalmol. 2021;15:3889–3900. doi:10.2147/opth.S327691
25. US Food and Drug Administration. FDA Adverse Event Reporting System (FAERS). US Food and Drug Administration. Available from: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers.
26. Pfaar O, Calderon MA, Andrews CP, et al. Allergen exposure chambers: harmonizing current concepts and projecting the needs for the future - an EAACI Position Paper. Allergy. 2017;72(7):1035–1042. doi:10.1111/all.13133
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.