")
Back to Journals » Patient Preference and Adherence » Volume 17
The Perspective of Patients and Health Professionals on the Prioritization of Assisted Reproductive Techniques. The PRIOFER Study
Authors Lizán Tudela C, Cuevas Sáiz I , Abad de Velasco L, Gregori Navarro L, Comellas M, Pérez-Sádaba FJ, Lizán L
Received 13 June 2023
Accepted for publication 4 October 2023
Published 30 October 2023 Volume 2023:17 Pages 2641—2653
DOI https://doi.org/10.2147/PPA.S421041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
César Lizán Tudela,1 Irene Cuevas Sáiz,2 Lorenzo Abad de Velasco,2 Laura Gregori Navarro,1 Marta Comellas,3 Francisco Javier Pérez-Sádaba,3 Luis Lizán3,4
1Department of Paediatrics, Obstetrics and Gynaecology, Hospital Clínico Universitario, Valencia, 46010, Spain; 2Department of Paediatrics, Obstetrics and Gynaecology, Consorcio Hospital General Universitario de Valencia, Valencia, 46014, Spain; 3Outcomes 10 SLU, Castellón de la Plana, Spain; 4Department of Medicine, Jaume I University, Castellón de la Plana, Spain
Correspondence: César Lizán Tudela, Department of Paediatrics, Obstetrics and Gynaecology, Hospital Clínico Universitario, Avda. Blasco Ibañez, 17, Valencia, 46010, Spain, Tel +34 654662524, Email [email protected]
Purpose: To determine the perspective of patients and professionals in Assisted Reproduction Units (ARU) on the importance of assisted reproductive techniques (ART) compared to other elective procedures, to highlight the relevance of ART as an elective procedure and the impact of delayed interventions on patients.
Design, Patients and Methods: An observational, descriptive, cross-sectional, online survey-based study was conducted in infertility patients and partners (n=98) and ARU healthcare professionals (n=83). The survey included a best-worst scaling (BWS) experiment and an ad-hoc questionnaire to analyze the pandemic impact on ART management and infertility patients in Spain. In the BWS, each respondent established priorities choosing which patient profile should be rated as the highest and lowest priority profile on a waiting list. To understand the importance that they give to assisted reproduction compared to other procedures, three very common elective procedures involving different patient profiles were selected: cataract surgery, knee arthroplasty, and varicose vein surgery. For each procedure, three hypothetical patient profiles corresponding to three different degrees of severity on a waiting list were designed.
Results: Patients attributed greater importance to ART profiles (BWS score: patients 0.14 vs professionals − 0.05; p< 0.01) whereas professionals prioritized cataract surgery (patients 0.06 vs professionals 0.23; p< 0.01). Concerning the profile severity, more severe profiles were prioritized in all procedures by both groups. Patients’ and professionals’ perspectives on the impact of the pandemic were similar, with exceptions: information received for resuming ART; health care provision in crisis situations; and reduction of parenting options. The pandemic affected patients’ ability to conceive a child (70.4% of those surveyed), their psychological well-being (75.5%), and partner, social, and work relationships (69.4%).
Conclusion: Preference studies involving patients and professionals can provide important information to define framework criteria for the management of waiting lists for elective procedures, and to prioritize interventions during pandemic periods. The pandemic impact on infertility patients highlights the relevance of developing measures and strategies to cope with similar future situations in the most appropriate way.
Keywords: assisted reproduction, coronavirus disease, fertility, patients’ perspective, best-worst scaling
Introduction
Infertility affects approximately 10% to 20% of couples in Europe,1 impacting on their quality of life, relationships, sexual satisfaction and psychosocial well-being.2,3 Individuals requesting fertility treatment often spend months or years trying to conceive a child before attending a fertility clinic.4 This, added to the long duration of the treatment, has been associated with an increased risk of psychological distress.5,6
Assisted reproductive techniques (ART) involve several medical procedures aiming to achieve pregnancy, which have become standard medical practice. The number of ART treatments is still rising, and an estimated five million babies have been born with the help of assisted reproduction in the past four decades.7,8 These techniques have not only been a breakthrough in the treatment of infertility, but are of enormous relevance for the fertility preservation in women undergoing cancer treatment.9
Like other elective procedures, such as scheduled orthopedic10 or cataract surgeries,11 ART procedures have been affected by the global coronavirus pandemic.12,13 The COVID-19 pandemic caused major disruption of routine hospital services globally. In a matter of days, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) rapidly spread around the world, leading to the first pandemic of the 21st century.14 Backlogs and delays in non-emergency health care caused by the COVID-19 strained health systems and left millions of people without care in many countries.15 Pre-pandemic, at the end of 2019, there were 700 thousand patients on the surgical waiting list in Spain, 20% of whom had been waiting more than 6 months for an operation.16 However, the Spanish healthcare system guarantees relatively fast access times for some elective procedures. Among the most frequently requested procedures in 2019 are cataract treatment, with an average waiting list time of approximately 70 days, or the treatment of varicose veins or knee prostheses, with an average waiting list time of around 110 days.17 Regarding the waiting list for ART, time varied considerably between Spanish regions, ranging between 6 and 24 months in some cases.18 In addition, the waiting time in this country for ART treatment is not supervised and controlled like other surgical waiting lists within hospital management agreements; in fact, to date, ART treatments are excluded from national framework criteria establishing a maximum access time.19 This was not just a national scenario as it was similar across European countries,20 with important access inequities and vastly different inter- and intra-country waiting times for ART.21 From a clinical perspective, longer waiting lists have a negative impact on the success of ART treatments.22
During the first quarter of 2020, the American Society for Reproductive Medicine (ARSM)23 and the European Society of Human Reproduction and Embryology (ESHRE)24 provided recommendations advising a precautionary approach to the postponement of all ART procedures. In Spain, the Spanish Fertility Society (SEF) and the Association for the Study of Reproductive Biology (ASEBIR) recommend a series of protective measures for Assisted Reproduction Units (ARU).25 Consequently, as of the 1st of April 2020, ART treatments were partially or totally ceased across European Assisted Reproduction Units (ARUs), causing disruption and delay to the fertility treatment received by thousands of patients.26
Despite these recommendations and the enforced restrictions, there was a lack of advice for clinics in two main areas: increasing psychological support and how to prioritize patients.27 Several studies have shown negative consequences on patients’ emotional state (stress, worry, and frustration) and quality of life due to treatment disruption or delay,28–30 and delays in ART procedures are perceived as a threat to attaining the goal of parenthood.28–33 In addition, approximately 30–50% of patients who are seeking ART have a low prognosis. In these cases, the “time” variable is crucial for success in ART, where they tend to lose their fertility potential rapidly. For this, a proposal for individualized treatment based on patient prognosis is necessary, as suggested by other authors.34,35 Despite this, no guidelines were established to prioritize and provide continuity of fertility care for those patients who required it.
Therefore, health policymakers should identify strategies to mitigate cancellations during pandemic periods and develop recovery plans to restore surgical activity safely and efficiently. Consequently, when designing strategies for reproductive medicine, it is essential to consider the perspective of both healthcare professionals and patients, understanding the importance they attribute to ART procedures among other elective procedures as well as the impact that such restrictions have on society.
Best and worst scaling (BWS) is an increasingly recognized method for quantitatively assessing how individuals prioritize different choices.36,37 BWS can be used to determine preferences for a wide range of healthcare issues, by asking the respondent to choose both the most and the least attractive options from a set of choices.38
The main aim of this study was to determine the perspective of patients and professionals in ARUs on the importance of ART compared to other elective procedure. To do so, BWS methodology was used to compare the different priorities of each group. In addition, as a secondary objective, we aimed to appraise the opinion of patients and professionals on the impact of the pandemic on ART management.
Materials and Methods
Design of the Study
An observational, descriptive, cross-sectional study was conducted based on an ad-hoc questionnaire, including a BWS experiment, and questions related to the impact of the pandemic on ART management. The data were collected through an online survey from May to October 2021.
Study Participants
The study population included infertility patients and their partners, on the one hand, and ARU healthcare professionals (gynecologists or biologists), on the other. Patients were invited to participate in the survey through national or local patient advocacy groups related to fertility problems, whereas healthcare professionals were invited by SEF, which disseminated the study to its members through its website and by e-mail.
The study included patients aged 18 years or older, who had received or were disposed to receiving fertility or ovarian reserve treatments or their partners, and gynecologists or biologists working at ARUs within the Spanish public healthcare sector at the moment of survey. All participants gave their consent to participate.
We considered Orme’s approach for discrete choice experiments39 to determine sample size because there is no general basis for determining sufficient sample size for BWS studies.40 In according to Orme’s approach, the minimum size was based on the population proportion estimation. Sample size for both groups of participants was estimated considering the number of Spanish patients receiving fertility treatments and the number of public centers with ARUs and/or in vitro fertilization units.41 We assumed a minimum of three physicians and two biologists practicing in each ARU in Spain. A minimum sample of 96 patients and 77 professionals was required assuming the criterion of maximum variability with a 95% confidence interval and 10% margin of error.34,42 A scientific committee (SC) comprising two experts: CLT (gynecologist) and ICS (biologist), both authors, was involved in the study design.
Ethical Considerations
This study was conducted according to the principles of the Declaration of Helsinki. It was developed to ensure consistency with the principles of the ICH Harmonized Tripartite Guideline for Good Clinical Practice. The study protocol and informed consent were approved by the Drug Research Ethics Committee (CEIm) of the Hospital Puerta de Hierro de Majadahonda (Madrid).
Research Instruments
The ad-hoc questionnaire comprised three sections: (1) participants’ characteristics (patients’ age, gender, marital status, number of children, and infertility history; and professionals’ age, gender, and career-related questions); (2) the BWS experiment; and (3) questions to assess their level of agreement on the impact of the pandemic on ART management in Spain, and four additional questions (yes/no/do not know), to be answered only by the patients, in order to appraise the impact of the pandemic on infertility patients at a personal level (Table S–I [A and B]).
BWS Experiment
We applied BWS methodology to establish priorities.38 We used the BWS profile case method, in which the respondent is asked to choose the best (most attractive) profile, as well as the worst (least attractive) one, in each scenarios.37
In our study, participants were asked to indicated, from their perspective, which patient profile should be rated as the highest priority profile (best) and the lowest priority profile (worst) on the waiting list.
Identification and Selection of Elective Procedures to Include in the BWS
We first reviewed the literature to identify the most common elective procedures and their priority criteria according to published legislation.43,44 Then, four common elective procedures were selected for the experiment based on the opinion of the SC, including assisted reproduction (ART), cataract surgery (CS), knee arthroplasty (KP), and varicose vein surgery (VS).
Construction of Hypothetical Profiles
We designed three hypothetical profiles of patients corresponding to three different degrees of severity (degree 1 > degree 2 > degree 3) on a waiting list for each elective procedure (a total of 12 patient profiles) (Table 1B). Each profile resulted from the combination of a series of predefined attributes related to the priority criteria for the elective procedure and the degree of severity (Table 1A and B). Subsequently, a scientific committee reviewed the resulting hypothetical profiles.
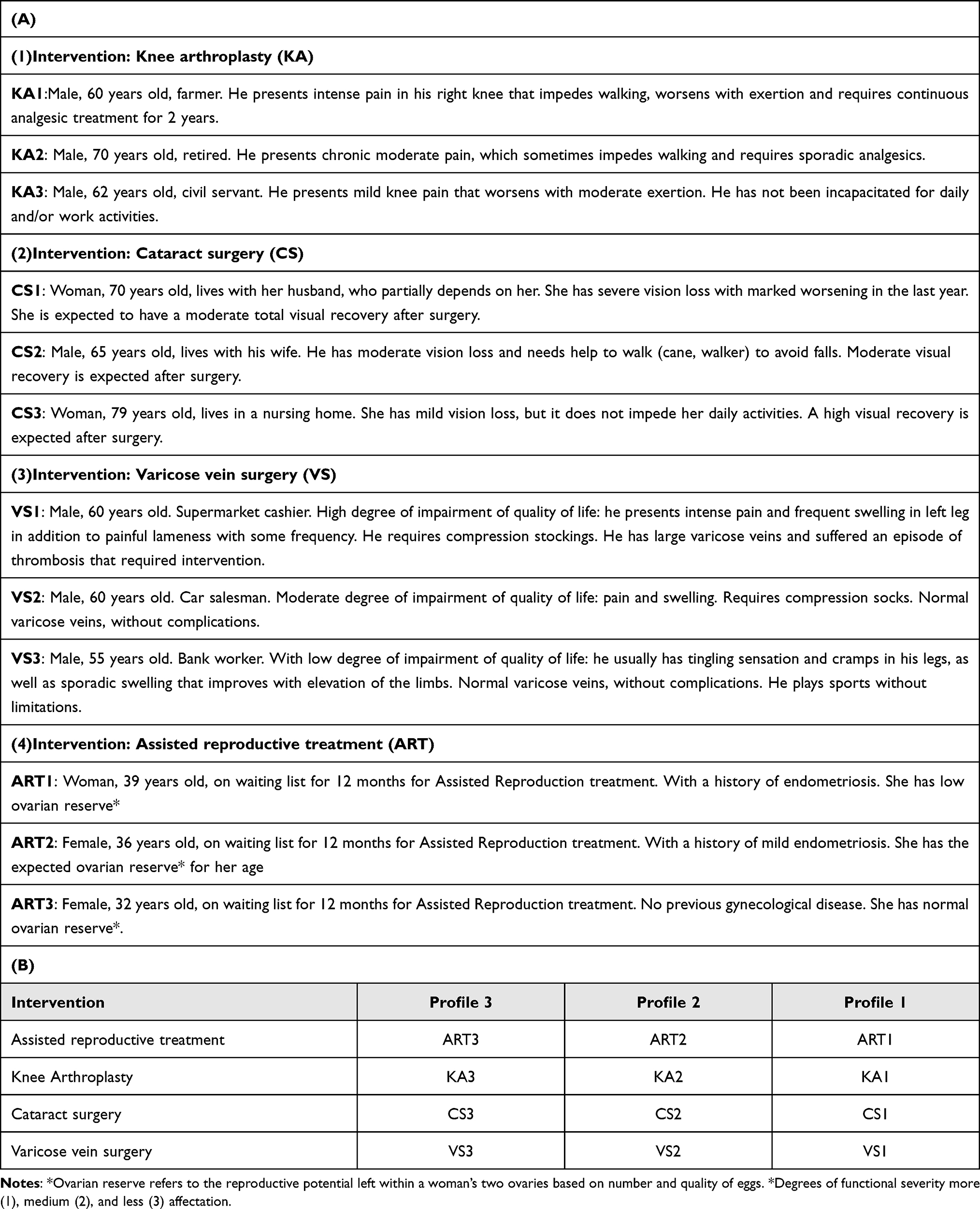 |
Table 1 Description of the Hypothetical Profile of Patients on a Waiting List for Elective Procedures with Three Possible Degrees of Functional Severity (1-A Shows the Definition of Each Profile for Each Procedure and 1-b Shows a Summary of Defined Procedures, Profiles and Degrees) |
Pilot Testing
A pilot test was conducted to verify participants’ comprehension of the designed profiles and confirm that they were clearly formulated and that the difference in severity between profiles was unambiguous. A total of 25 individuals from the general population participated in the pilot test.
When at least 10% of the participants disagreed with the previously established order of severity for each procedure, the profile was considered ambigous and therefore, the wording was modified to clarify the meaning.
Construction of Choice Tasks
The last step consisted of an orthogonal full-factorial design to generate the scenarios. This design was constructed through a specific algorithm to ensure the orthogonality and balance, and minimize the dominance.45 As a result, a total of nine scenarios (with four profiles each one) were generated; however, to reduce the burden on participants, they were divided into three blocks by using a blocked design (Table S-IA). Respondents were randomly assigned to a block and answered the choice questions in that block (three scenarios). Blocking promotes response efficiency by reducing the cognitive effort required by each respondent.46
Data Analysis
Data were analyzed using the STATA v.14 software. A value of p<0.05 was considered significant for all statistical tests. For the descriptive analysis of the qualitative variables, the relative and absolute frequencies were calculated, and for the quantitative variables central tendency and dispersion measures were used for each group of participants.
We analyzed BWS responses of each participants to establish a ranking from most to least important in the prioritization of each scenarios. The BWS scores were on a scale from −1 (worst profile) to +1 (best profile). In each participant, the BWS score for each scenarios was calculated as the difference between the frequency of being chosen as worst vs best divided by the number of times it appeared across the presented scenarios. Finally, the mean of BWS scores in each group of participants was shown. In our design, score toward +1 indicated as highest priority and when score towards −1 indicated as lowest priority on waiting list.
Based on normality (Shapiro–Wilk test), Student’s t-test or Kruskal–Wallis tests were used to compare the differences of BWS scores between both groups. Finally, questions regarding the pandemic’s impact were measured using a 6-points Likert scale (strongly agree; agree; undecided, disagree; strongly disagree; no answer) or nominal scale. Chi-squared test was used to determine the different answers (categorical variables) between participants.
Results
Description of the Participants
The demographic characteristics of the study population are reported in Table 2. A total of 98 patients and 83 professionals completed the online survey. The mean age of patients was 37.4 years (SD: 4.4), the majority were married or had a partner (87.8%), were childless (70.4%) and had previously received fertility treatment (83.7%). Most of the professionals surveyed were women (72.3%) with a mean age of 48.1 years (SD: 9.4) and a mean of 15.5 years (SD: 8.4) experience in ARU, the majority worked in public and private health sectors.
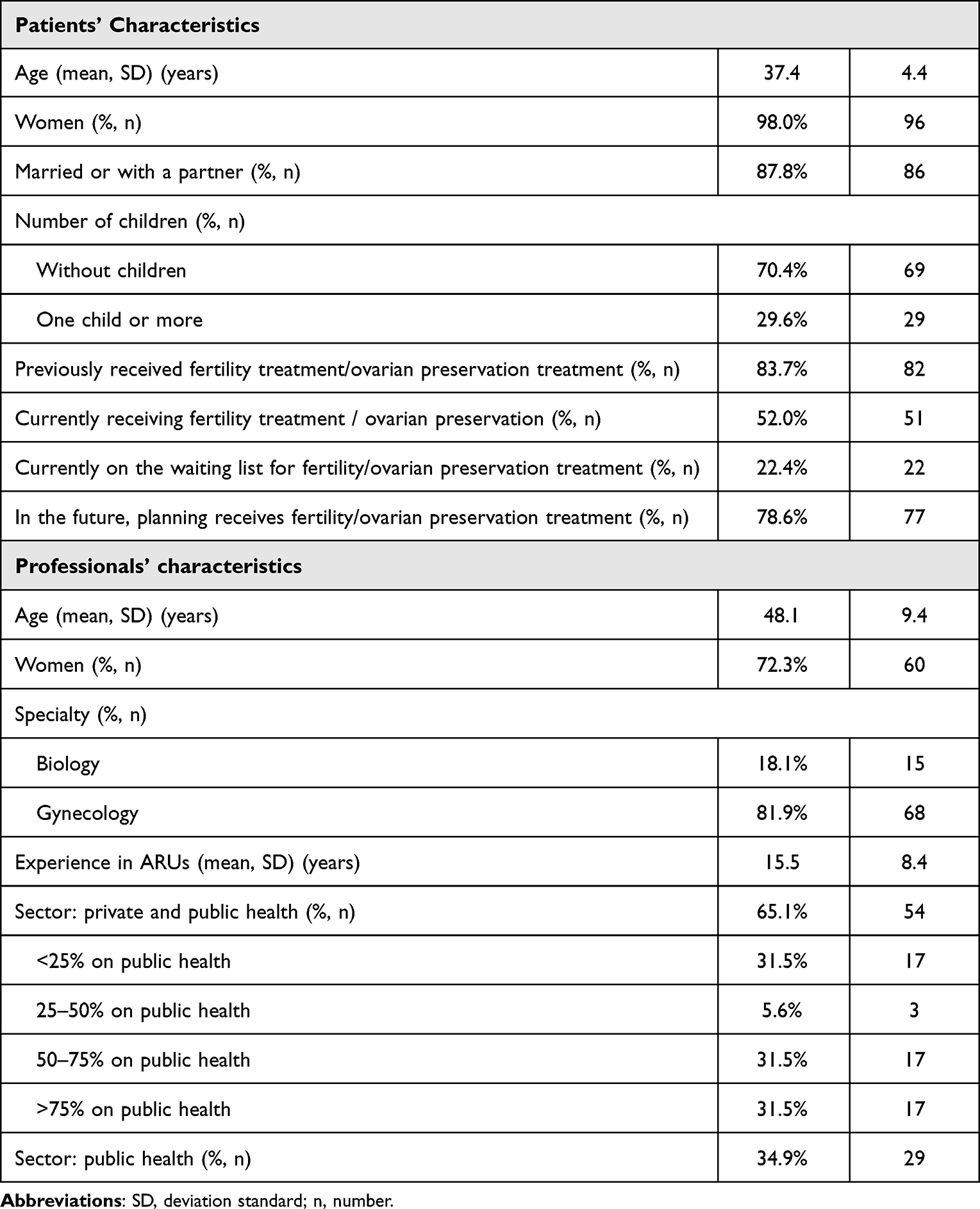 |
Table 2 Description of Demographic Characteristics of the Study Population |
The Perspective of Patients and Professionals at ARUs on the Importance of ART Compared to Other Elective Procedures
According to the BWS methodology, BWS scores of patient profiles were ordered from most to least important for prioritizing procedures. Figure 1 presents the results of the prioritization of procedures provided by patients and professionals. Patients gave greater importance to prioritizing patients on the waiting list for ART and in second place to cataract surgery. In contrast, professionals gave greater importance to cataract surgery and in second place to knee arthroplasty. Significant differences between groups were observed in the prioritization of cataract surgery and ART profiles as shown in Figure 1.
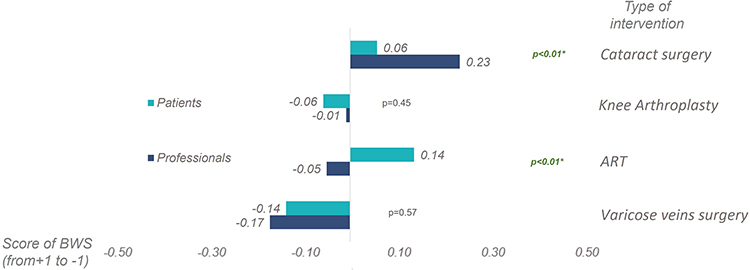 |
Figure 1 Comparison between patients and professionals regarding prioritization results (most to least important) by type of surgical interventions (Score toward +1 indicated as highest priority and when score towards −1 indicated as lowest priority on waiting list). |
Concerning the severity of the profiles, more severe profiles were prioritized in both groups (CS1, KP1, VS1, and ART1) (Figure 2). When analyzing the most severe profiles, patients gave more importance to procedures, such as ART and varicose vein surgery, whereas professionals to cataract and varicose vein surgery. However, professionals prioritize ART profiles as less severe profiles (profiles 2 and 3). Significant differences were also observed in prioritizing the most severe profile of cataract and ART (CS1 and ART1), and the medium profile of ART (ART2) (Figure 2).
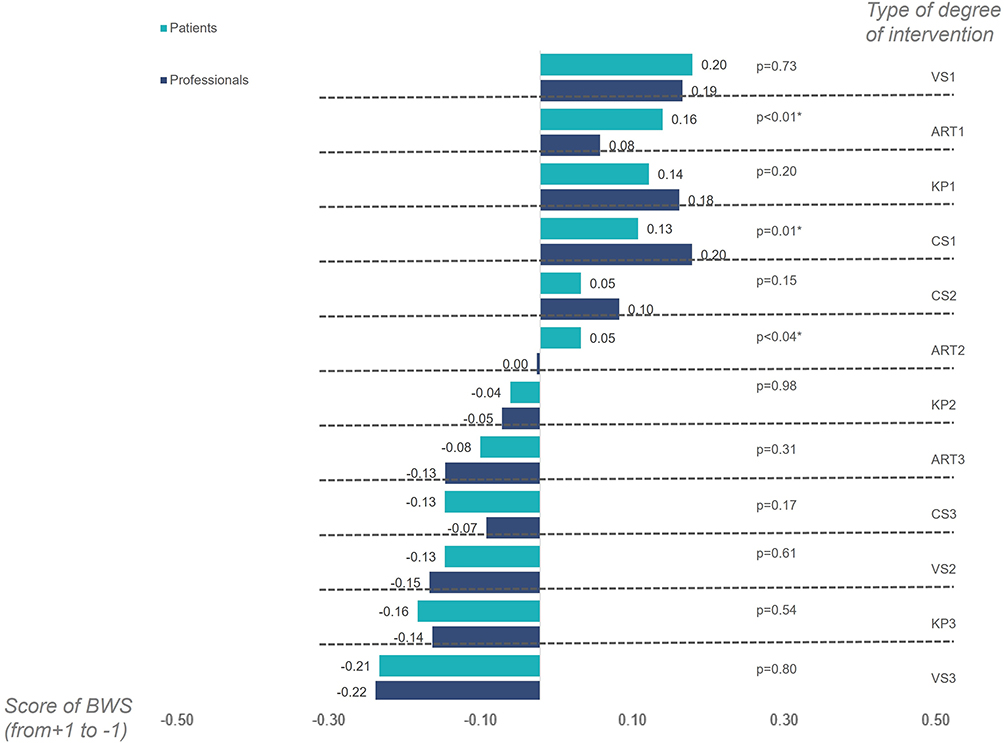 |
Figure 2 Comparison between patients and professionals regarding prioritization results (most to least important) by type of surgical interventions and by severity degrees (Score toward +1 indicated as highest priority and when score towards −1 indicated as lowest priority on waiting list). |
The Impact of the Pandemic on ART Management
Patients and professionals similarly assessed the impact of the pandemic on ART management as shown in Figure 3. A significant difference (p<0.001) between both groups was observed when they were asked about the information received during the pandemic regarding the expected periods for the resumption of ARU services: 61.2% of the patients vs 49.4% of the professionals disagreed or strongly disagreed with it. In addition, regarding the reduction in parenting options for couples undergoing fertility treatments during the pandemic, the response was: 10.2% of patients vs 15.6% of the professionals (p<0.001) disagreed or strongly disagreed with it. And only 2% of professionals disagreed or strongly disagreed with ARU should continue providing healthcare services in this situation, while 8.4% of patients considered this.
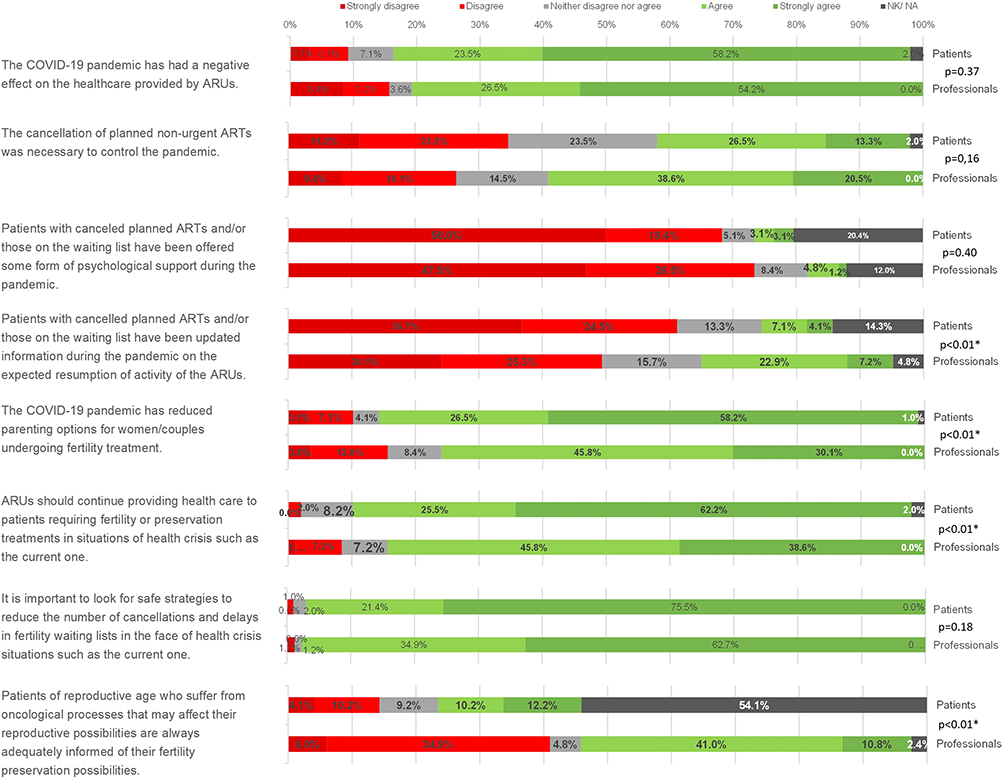 |
Figure 3 Answers to ad-hoc questionnaire by patients and professionals in arus on the impact of the pandemic on art service management (*p-value<0.05). |
Regarding the impact of the pandemic on infertility patients at a personal level, patients confirmed the negative effect of the pandemic on their lives, affecting their ability to conceive a child (70.4%), psychological well-being (75.5%), and partner, social and work relationships (69.4%). Around 40.8% of those surveyed required psychological support from a professional (Figure S1).
Discussion
The management of waiting lists for elective surgery is a critical issue for public healthcare systems47 and COVID-19 has had a substantial influence on waiting times. To our knowledge, this study represents the first analysis of the perspectives of both patients and healthcare professionals on the prioritization of ART compared to other elective procedures within the context of the COVID-19 pandemic.
Our results show differences between patients and healthcare professionals regarding the most prioritized intervention (cataract surgery for physicians and ART for patients). However, both groups have the same opinion in categorizing varicose vein surgery as the lowest priority intervention of those proposed. As expected, individuals with fertility problems, or their partners, who had previously received fertility treatment or were likely to receive it, gave greater importance to ART profiles compared to the other profiles. The inability to have a child may be experienced as a deep personal loss,13 and the pandemic period has exacerbated uncertainty about the chances of parenthood for many couples. On the other hand, health professionals seem to attach greater importance to vision loss, which has a significant impact on patients and society in terms of morbidity, quality of life, and costs.11
A current estimate suggests that more than 50% of all elective surgical cases have the potential to inflict significant harm on patients if cancelled or delayed.48 Therefore, the question is which ones could be considered as priority interventions rather than elective ones. In line with this, our findings show that professionals attach greater importance to prioritizing ART profiles when compared to less severe profiles. This suggests a preference for fertility interventions over other non-urgent elective procedures by professionals. This might be because professionals acknowledge that the mother´s age is a critical factor in the success of ART, so the time variable is more crucial in these elective treatments than in others.
The context of the pandemic has brought to the fore a previously existing reality, the high emotional burden of infertility on patients, and the contrast with health professionals’ views on the relevance of infertility or ovarian reserve treatments. This may be explained by the fact that, as pointed by Wiltshire et al, the decision to treat or not to treat infertility is multifactorial.49 For patients, the decision may not only reflect gestational desire, but also the impact of previous treatment failures, pregnancy loss or a cancer diagnosis. While from the physician’s perspective, other factors must be considered, such as the risk to the health of the patient and foetus, as well as that of the entire professional involved in the process.49 In the case of fertility preservation, when women undergo cancer treatment or affected by gynaecological cancer, the individual autonomy of patients to make an informed decision should be considered unless the process may pose a risk to children or others.9 The psychological wellbeing of these patients may be more affected by the loss of fertility than by the cancer diagnosis itself.50 For this reason, the complexity of the decision to treat makes it essential that the approach be multidisciplinary, and may be necessary psychological support.51
Although little evidence is available on the difference between patients’ and professionals’ views on the use of different health services during the pandemic,52 other authors have also analyzed potential discrepancies in other therapeutic areas. In this respect, Antonacci et al, performed a survey to compare perceptions of urgency for musculoskeletal complaints between patients and physicians, showing significant differences between the diagnoses considered urgent between the two groups.52 Discrepancies between patients and professionals are nothing new in the literature. A systematic review of discrete choice experiments shows that discordance between the preferences of the two groups on decisions about health interventions is more common than concordance.53
There is limited evidence regarding the factors to be considered in the prioritization of surgical interventions, and existing evidence is heterogeneous. Some studies show the different perspectives between physicians and patients on the prioritization of patients on waiting lists with a view to establishing a strategy to improve the timeliness and robustness of waiting-time management.54–56 Through a multiple case study, Déry et al compared the perspective between patient and provider regarding patient prioritization criteria in two rehabilitation programs, showing similar opinions about the criteria to prioritize patients on waiting lists between both groups (coinciding on almost half of the criteria). Their results revealed that the point of views of all stakeholders on prioritization criteria is an important part of the decision-making process. Other authors agree that patients’ quality of life should be one of the main factors to consider in waiting list management.11,57 In this respect, it is important to bear in mind that measures adopted by governments during the COVID-19 pandemic have increased anxiety and psychological distress for infertile couples.26,28–30 Although the decision to suspend the activity of ARUs was undeniably difficult and justified for the protection of health professionals and society at large, it is important that health professionals and policymakers understand the impact on the quality of life and psychological well-being of already vulnerable infertile patients.58
This cross-sectional survey sought the views of patients and professionals on the impact of the pandemic on ART management in Spain as a secondary objective. Our findings suggest that both groups agreed on the negative impact that the pandemic has had on ARUs, revealing the need to seek strategies to minimize cancellations of fertility or preservation treatments and to continue providing healthcare to fertility patients during health crises. Our results are in line with other studies that reflect the negative impact that the pandemic has had on infertility patients or the lack of psychological support experienced by patients during this period.26,28–30,59 Although a temporary delay in ART might be prudent at the beginning of a pandemic, a prolonged suspension on fertility treatments might have severe consequences for patients.32,34 In such a situation, there is a need to define plans and recommendations for reestablishing treatments and thus minimize the uncertainty experienced by patients regarding future situations of service cessation.34 Furthermore, it is necessary to define framework criteria that guarantee access to assisted reproduction in adequate time. In a scenario of increasing patient-centered care, patients’ opinion and preferences must be taken into account in defining prioritization criteria, giving them an increasingly active role in health planning.60–62
Our study has some limitations, most of which are inherent to the methodology applied. The first is related to the study participants. We only consider the opinion of infertile couples and professionals from ARUs, so selection bias could be an issue. However, we framed our survey in this specific population to give value to the importance that this population attaches to a medical condition that is not generally considered to have a high social impact. Secondly, the BWS method provides a prioritization among those attributes included in the questionnaire, so results are limited and relative among the attributes included. Different approaches are available when analyzing multiple criteria to guide healthcare decision-making. Here, we selected a BWS experiment because it is an increasingly popular method to investigate the preferences of different key players in the health sector, as it is an easy and accessible method to quantify importance among a series of specific profiles or scenarios.38 Identified limitations were overcome by including a SC and pilot tests answered by the general population, thus contributing to the selection of attributes and testing the experiment’s comprehensibility, respectively.
Despite of these limitations, this study makes the patients’ and professionals’ perspectives visible to society and health policy decisors, to give greater relevance to the ART procedures and they may be considered as other surgical elective procedures. This could have an impact on waiting lists and also in future health crisis situations, such as the one experienced with COVID-19.
Conclusion
Infertility patients and professionals from ARUs differ in the priority they give to assisted reproduction over other elective procedures. Preference studies can provide important information to support decisions made by healthcare decision-makers on waiting-list management.
This study further shows that delays and cancellations in ART interventions in specific periods, such as the COVID-19 pandemic, not only compromises treatment success, it could also negatively impact on patients’ psychological well-being and quality of life. Therefore, plans and recommendations must be defined for reestablishing treatments and minimizing the uncertainty experienced by patients in future situations of service cessation.
Abbreviations
ART, assisted reproductive technology; BWS, best-worst scaling; ARSM, American Society for Reproductive Medicine; ESHRE, European Society of Human Reproduction and Embryology; SEF, Spanish Fertility Society; ASEBIR, Association for the Study of Reproductive Biology; ARU, Assisted Reproduction Units; SC, scientific committee; CEIm, Drug Research Ethics Committee; CS, cataract surgery; KP, knee arthroplasty; VS, varicose vein surgery; SD, standard deviation.
Acknowledgments
The authors wish to thank all fertility patients and professionals who contributed to this study. The authors are also grateful to the Spanish Fertility Society, the Association for the Study of Reproductive Biology, the National Association for Infertility Problems, and Redinfertiles as well as other advocacy groups (SheOAK, MSPE) who helped to distribute the questionnaire. Finally, the authors would like to thank María Soler and Clara Pérez from Outcomes’10 for their support in the statistical analysis and medical writing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roustaei Z, Räisänen S, Gissler M, Heinonen S. Fertility rates and the postponement of first births: a descriptive study with Finnish population data. BMJ Open. 2019;9(1):e026336. doi:10.1136/bmjopen-2018-026336
2. Agostini F, Monti F, Andrei F, Paterlini M, Palomba S, La Sala GB. Assisted reproductive technology treatments and quality of life: a longitudinal study among subfertile women and men. J Assist Reprod Genet. 2017;34(10):1307–1315. doi:10.1007/s10815-017-1000-9
3. Namdar A, Naghizadeh MM, Zamani M, Yaghmaei F, Sameni MH. Quality of life and general health of infertile women. Health Qual Life Outcomes. 2017;15(1):1–7. doi:10.1186/s12955-017-0712-y
4. Farr SL, Anderson JE, Jamieson DJ, Warner L, Macaluso M. Predictors of pregnancy and discontinuation of infertility services among women who received medical help to become pregnant, national survey of family growth, 2002. Fertil Steril. 2009;91(4):988–997. doi:10.1016/j.fertnstert.2008.01.057
5. Stevenson EL, Hershberger P. Fertility and Assisted Reproductive Technology (ART): Theory, Research, Policy and Practice for Health Care Practitioners. Springer Publishing Company; 2016.
6. Slade P, O’Neill C, Simpson AJ, Lashen H. The relationship between perceived stigma, disclosure patterns, support and distress in new attendees at an infertility clinic. Hum Reprod. 2007;22(8):2309–2317. doi:10.1093/humrep/dem115
7. Wyns C, De Geyter C, Calhaz-Jorge C, et al. ART in Europe, 2017: results generated from European registries by ESHRE. Hum Reprod Open. 2021;2021(3):hoab026. doi:10.1093/hropen/hoab026
8. Adamson GD, Tabangin M, Macaluso M, de Mouzon J. The number of babies born globally after treatment with the assisted reproductive technologies (ART). Fertil Steril. 2013;100(3):S42. doi:10.1016/j.fertnstert.2013.07.1807
9. Zaami S, Stark M, Signore F, Gullo G, Marinelli E. Fertility preservation in female cancer sufferers: (only) a moral obligation? Eur J ContrAcept Reprod Health Care. 2022;27(4):335–340. doi:10.1080/13625187.2022.2045936
10. Logishetty K, Edwards TC, Subbiah Ponniah H, et al. How to prioritize patients and redesign care to safely resume planned surgery during the COVID-19 pandemic. Bone Jt Open. 2021;2(2):134–140. doi:10.1302/2633-1462.22.BJO-2020-0200.R1
11. Tognetto D, Brézin AP, Cummings AB, et al. Rethinking elective cataract surgery diagnostics, assessments, and tools after the COVID-19 pandemic experience and beyond: insights from the EUROCOVCAT group. Diagnostics. 2020;10(12):1035. doi:10.3390/diagnostics10121035
12. COVIDSurg-Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. J Br Surg. 2020;107(11):1440–1449.
13. Gross MS, Harrington BJ, Sufrin CB, Faden RR. Rethinking “Elective” procedures for women’s reproduction during Covid-19. Hastings Cent Rep. 2020;50(3):40–43. doi:10.1002/hast.1130
14. Sohrabi C, Alsafi Z, O’neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
15. World Health Organization. COVID-19 Has Caused Major Disruptions and Backlogs in Health Care, New WHO Study Finds. World Health Organization; 2022.
16. Ministerio de Sanidad B. Sistema de Información de Listas de Espera del Sistema Nacional de Salud (SISLE-SNS). Sanidad M, editor. Sanitaria SGd. Ministerio de Sanidad ed; 2020:20. Available from: https://www.sanidad.gob.es/estadEstudios/estadisticas/inforRecopilaciones/listaEspera.htm.
17. Secretaria General de Sanidad, Dirección General de Salud Pública, Calidad e Innovación, BOE MdS; 2019. Available from: https://www.sanidad.gob.es/estadEstudios/estadisticas/inforRecopilaciones/docs/LISTAS_PUBLICACION_dic19.pdf.
18. Arroyo J. Hasta tres años de espera para poder ser madre. El País; 2019.
19. BOE MdS. Real Decreto 1039/2011, de 15 de julio, por el que se establecen los criterios marco para garantizar un tiempo máximo de acceso a las prestaciones sanitarias del Sistema Nacional de Salud; 2011. Available from: https://www.boe.es/buscar/pdf/2011/BOE-A-2011-14190-consolidado.pdf.
20. Calhaz-Jorge C, Kupka MS, Wyns C, et al. Survey on ART and IUI: legislation, regulation, funding and registries in European countries: the European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod Open. 2020;2020(1). doi:10.1093/hropen/hoz044
21. ESHRE. Comparative analysis of medically assisted reproduction in the EU: regulation and technologies SANCO/2008/C6/051; 2008. Available from: https://ec.europa.eu/health/system/files/2016-11/study_eshre_en_0.pdf:FinalReport.
22. Alon I, Pinilla J. Assisted reproduction in Spain, outcome and socioeconomic determinants of access. Int J Equity Health. 2021;20(1):156. doi:10.1186/s12939-021-01438-x
23. ASRM. American Society for reproductive medicine (ASRM) patient management and clinical recommendations during the coronavirus (Covid-19) pandemic; 2020. Available from: https://www.asrm.org/globalassets/asrm/asrm-content/news-and-publications/covid-19/covidtaskforce.pdf.
24. ESHRE. Coronavirus Covid-19: ESHRE statement on pregnancy and conception; 2020. Available from: https://www.eshre.eu/Press-Room/ESHRE-News/2020.
25. ASEBIR. Recomendaciones para la seguridad y reducción de riesgos ante la infección por coronavirus (SARS-CoV-2) en las unidades de reproducción asistida. Sociedad Española de Fertilidad y Asociación para el estudio de la biología de la Reproducción; 2020:11.
26. Gürtin ZB, Jasmin E, Da Silva P, Dennehy C, Harper J, Kanjani S. Fertility treatment delays during COVID-19: profiles, feelings and concerns of impacted patients. Reprod Biomed Soc Online. 2022;14:251–264. doi:10.1016/j.rbms.2021.12.004
27. Cutting E, Catt S, Vollenhoven B, Mol BW, Horta F. The impact of COVID-19 mitigation measures on fertility patients and clinics around the world. Reprod Biomed Online. 2022;44(4):755–763. doi:10.1016/j.rbmo.2021.12.016
28. Boivin J, Harrison C, Mathur R, Burns G, Pericleous-Smith A, Gameiro S. Patient experiences of fertility clinic closure during the COVID-19 pandemic: appraisals, coping and emotions. Hum Reprod. 2020;35(11):2556–2566. doi:10.1093/humrep/deaa218
29. Haham LM, Youngster M, Shani AK, et al. Suspension of fertility treatment during the COVID-19 pandemic: views, emotional reactions and psychological distress among women undergoing fertility treatment. Reprod Biomed Online. 2021;42(4):849–858. doi:10.1016/j.rbmo.2021.01.007
30. Lawson AK, McQueen DB, Swanson AC, Confino R, Feinberg EC, Pavone ME. Psychological distress and postponed fertility care during the COVID-19 pandemic. J Assist Reprod Genet. 2021;38(2):333–341. doi:10.1007/s10815-020-02023-x
31. Rodríguez-Varela C, Mariani G, Dolz P, et al. Impact of COVID-19 on infertility treatments: not even a global pandemic was strong enough to hamper successful pregnancies. Life. 2021;12(1):6. doi:10.3390/life12010006
32. Wedner-Ross S, Schippert C, von Versen-Höynck F. The impact of the COVID-19 pandemic on women seeking fertility treatment: the patient’s perspective. Arch Gynecol Obstet. 2022;305(6):1–10.
33. Gordon JL, Balsom AA, Doering S. The psychological impact of fertility treatment suspensions during the COVID-19 pandemic. PLoS One. 2020;15(9):e0239253. doi:10.1371/journal.pone.0239253
34. Alviggi C, Esteves SC, Orvieto R, et al. COVID-19 and assisted reproductive technology services: repercussions for patients and proposal for individualized clinical management. Reprod Biol Endocrinol. 2020;18(1):45. doi:10.1186/s12958-020-00605-z
35. Eijkemans MJC, Lintsen AME, Hunault CC, et al. Pregnancy chances on an IVF/ICSI waiting list: a national prospective cohort study. Hum Reprod. 2008;23(7):1627–1632. doi:10.1093/humrep/den132
36. Wittenberg E, Bharel M, Bridges JF, Ward Z, Weinreb L. Using best-worst scaling to understand patient priorities: a case example of Papanicolaou tests for homeless women. Ann Fam Med. 2016;14(4):359–364. doi:10.1370/afm.1937
37. Cheung KL, Wijnen BF, Hollin IL, et al. Using best–worst scaling to investigate preferences in health care. Pharmacoeconomics. 2016;34(12):1195–1209. doi:10.1007/s40273-016-0429-5
38. Flynn TN, Louviere JJ, Peters TJ, Coast J. Best–worst scaling: what it can do for health care research and how to do it. J Health Econ. 2007;26(1):171–189. doi:10.1016/j.jhealeco.2006.04.002
39. Orme BK. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research.
40. Mühlbacher AC, Kaczynski A, Zweifel P, Johnson FR. Experimental measurement of preferences in health and healthcare using best-worst scaling: an overview. Health Econ Rev. 2016;6(1):1–14. doi:10.1186/s13561-016-0080-z
41. Sociedad Española de Ferlitidad y Ministerio de Sanidad. Informe estadístico de Técnicas de Reproducción Asistida Registro Nacional de Actividad Ministerio de Sanidad y Sociedad Española de Fertilidad. Sociedad Española de Ferlitidad y Ministerio de Sanidad; 2018:62.
42. Severin F, Schmidtke J, Mühlbacher A, Rogowski WH. Eliciting preferences for priority setting in genetic testing: a pilot study comparing best-worst scaling and discrete-choice experiments. Eur J Med Genet. 2013;21(11):1202–1208. doi:10.1038/ejhg.2013.36
43. BOE MdSyC. Real Decreto 605/2003, de 23 de mayo, por el que se establecen medidas para el tratamiento homogéneo de la información sobre las listas de espera en el Sistema Nacional de Salud; 2003.
44. BOE MdSPSeI. Real Decreto 1039/2011, de 15 de julio, por el que se establecen los criterios marco para garantizar un tiempo máximo de acceso a las prestaciones sanitarias del Sistema Nacional de Salud. BOE-A-2011-14190; 2011.
45. Louviere J, Flynn T, Marley A. (2015) The BWS profile case. In: Marley AAJ, Louviere JJ, Flynn TN, editors. Best-Worst Scaling: Theory, Methods and Applications. Cambridge: Cambridge University Press; 2015:56–88.
46. Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
47. Valente R, Testi A, Tanfani E, et al. A model to prioritize access to elective surgery on the basis of clinical urgency and waiting time. BMC Health Serv Res. 2009;9(1):1. doi:10.1186/1472-6963-9-1
48. Zhang S. What it really means to cancel elective surgeries: to make room for coronavirus patients, hospitals are delaying procedures that would make major differences in people’s lives. Atlantic. 2020;2020:17.
49. Wiltshire A, Jackson-Bey T, Walker Z, et al. To treat or not to treat: perceptions of the initial American Society for Reproductive Medicine COVID-19 recommendations among women’s health providers. J Assist Reprod Genet. 2021;38(3):621–626. doi:10.1007/s10815-021-02064-w
50. La Rosa VL, Garzon S, Gullo G, et al. Fertility preservation in women affected by gynaecological cancer: the importance of an integrated gynaecological and psychological approach. Ecancermedicalscience. 2020;14:1035. doi:10.3332/ecancer.2020.1035
51. Burgio S, Polizzi C, Buzzaccarini G, et al. Psychological variables in medically assisted reproduction: a systematic review. Prz Menopauzalny. 2022;21(1):47–63. doi:10.5114/pm.2022.114404
52. Antonacci CL, Omari AM, Zaifman J, et al. Differences in patient and physician perceptions of urgency for musculoskeletal conditions during the COVID-19 pandemic. Orthopedics. 2021;44(4):e534–e8. doi:10.3928/01477447-20210618-13
53. Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ Open. 2017;7(5):e014719. doi:10.1136/bmjopen-2016-014719
54. Oudhoff JP, Timmermans DR, Knol DL, Bijnen AB, Van der Wal G. Prioritising patients on surgical waiting lists: a conjoint analysis study on the priority judgements of patients, surgeons, occupational physicians, and general practitioners. Soc Sci Med. 2007;64(9):1863–1875. doi:10.1016/j.socscimed.2007.01.002
55. Conner-Spady BL, Sanmugasunderam S, Courtright P, Mildon D, McGurran JJ, Noseworthy TW. Patient and physician perspectives of maximum acceptable waiting times for cataract surgery. Can J Ophthalmol. 2005;40(4):439–447. doi:10.1016/S0008-4182(05)80003-1
56. Déry J, Ruiz A, Routhier F, et al. Patient and provider perspectives regarding criteria for patient prioritization in two specialized rehabilitation programs. Patient Exp J. 2021;8(1):174–183. doi:10.35680/2372-0247.1530
57. Rovers MM, Wijn SR, Grutters JP, et al. Development of a decision analytical framework to prioritise operating room capacity: lessons learnt from an empirical example on delayed elective surgeries during the COVID-19 pandemic in a hospital in the Netherlands. BMJ Open. 2022;12(4):e054110. doi:10.1136/bmjopen-2021-054110
58. Kirubarajan A, Patel P, Tsang J, Prethipan T, Sreeram P, Sierra S. The psychological impact of the COVID-19 pandemic on fertility care: a qualitative systematic review. Hum Fertil. 2021;26(1):1742–8149.
59. Lee D. The impact of COVID-19 on human reproduction and directions for fertility treatment during the pandemic. Clin Exp Reprod Med. 2021;48(4):273. doi:10.5653/cerm.2021.04504
60. Say RE, Thomson R. The importance of patient preferences in treatment decisions--challenges for doctors. BMJ. 2003;327(7414):542–545. doi:10.1136/bmj.327.7414.542
61. Lette M, Stoop A, Lemmens LC, Buist Y, Baan CA, De Bruin SR. Improving early detection initiatives: a qualitative study exploring perspectives of older people and professionals. BMC Geriatr. 2017;17(1):1–13. doi:10.1186/s12877-017-0521-5
62. Williams CP, Miller‐Sonet E, Nipp RD, Kamal AH, Love S, Rocque GB. Importance of quality‐of‐life priorities and preferences surrounding treatment decision making in patients with cancer and oncology clinicians. Cancer. 2020;126(15):3534–3541. doi:10.1002/cncr.32961
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.