")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
The Pattern of Initial Presentation of Diabetes, Treatment Outcome and Its Predictors Among Diabetic Pediatrics Attended Service at Selected Public Hospitals of Southern Ethiopia: A Multi-Center Study
Authors Yeheyis T , Hoyiso D , Ekubazgi KW, Chura GK , Alemayehu Y
Received 20 September 2023
Accepted for publication 17 November 2023
Published 21 November 2023 Volume 2023:16 Pages 2485—2495
DOI https://doi.org/10.2147/RMHP.S437361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Tomas Yeheyis,1 Dawit Hoyiso,1 Kinfe Woldu Ekubazgi,2 Gemechu Kediro Chura,3 Yonas Alemayehu1
1School of Nursing, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2School of medicine, College of Medicine and health sciences, Hawassa University, Hawassa, Ethiopia; 3Department of Nursing, College of medicine and health sciences, Meda Welabu University, Shashemene, Ethiopia
Correspondence: Tomas Yeheyis, School of Nursing, College of Medicine and Health Science, Hawassa University, Ethiopia, Tel +251975708574, Email [email protected]
Background: Diabetes mellitus is the most common metabolic disorder in the pediatric population. Globally the incidence of diabetes increased from 11.3 million (95% UI 10.6– 12.1) in 1990 to 22.9 million (21.1– 25.4) in 2017, with a 102.9% increase and there was a 3% increase in diabetes mortality rates by age between 2000 and 2019.
Objective: This study aims to assess the pattern of initial presentation of pediatric diabetes mellitus, treatment outcome, and its predictors among pediatrics who attended service at selected public hospitals in southern Ethiopia from 2015 to 2019.
Methods: A cross-sectional study was conducted among 422 randomly selected pediatrics from October 1st, 2021 to December 30, 2021, and participants were selected randomly from 8 randomly selected public hospitals in southern Ethiopia after proportional to client flow allocation of samples. Data was extracted from clients’ charts using a data extraction checklist. Statistical Package for Social Sciences (SPSS) version 24, and logistic regression analysis were applied to determine the presence of an association between dependent and independent variables, and significance was declared at p-value < 0.05.
Results: In this study, most (74.6%) of the pediatrics initially presented with Diabetic ketoacidosis (DKA). This study found that Two-thirds (67.1%) of the respondents in the study had a good treatment outcome. In this study residence, presenting signs and symptoms; poly symptoms and weight loss, history of hospitalization, and comorbidity were predictors of treatment outcome of pediatric diabetes mellitus.
Conclusion: Diabetes mellitus with Diabetic ketoacidosis is the predominant pattern of initial presentation in the study. The magnitude of poor treatment outcomes of diabetes mellitus among pediatrics in this study is high and unacceptable Residence, signs, and symptoms at initial presentation, history of hospitalization, and comorbidity were found to be significant independent predictors of treatment outcome of pediatric diabetes mellitus.
Keywords: diabetes mellitus, pattern of initial presentation, treatment outcome, predictors, southern Ethiopia
Introduction
Diabetes is an extreme, chronic disorder that happens either whilst the pancreas does not produce enough insulin (a hormone that regulates blood sugar or glucose) or when the frame cannot efficaciously use the insulin it produces.1 These metabolic abnormalities are caused by insufficient insulin to produce an adequate response and/or insulin resistance of target tissues, primarily the liver, adipose tissue, and skeletal muscles, at the level of insulin receptors, signal transduction system, and/or effector enzymes or genes. Diagnosis kind and duration determine the severity of symptoms. Some diabetics, particularly those with type 2 diabetes in its early stages, have no symptoms at all. Another type named Type 1 has severe hyperglycemia, and children who have complete insulin insufficiency are particularly susceptible to symptoms like polyuria, polydipsia, polyphagia, weight loss, and blurred vision.2 Diabetes is a crucial public fitness trouble, one in all 4 preceding non-communicable sicknesses (NCDs) targeted for action by way of global leaders.1
Globally over 1.1 million children under the age of 20 are thought to be affected by diabetes, which is responsible for five million yearly fatalities and accounts for 132,600 new cases each year, or a 3% annual increase.3 A recent report from the International Diabetes Federation depicts that an estimated 108,300 children under 15 years will be diagnosed with DM in 2021, a number rising to 149,500 when the age range extends to under 20 years.4 In 2017, developing nations accounted for 77% of all diabetes cases, with 14.2 million cases in Africa and 5.2% of cases worldwide in Ethiopia.5 Similarly, almost 80% of diabetes-related deaths worldwide take place in low- and middle-income nations.6,7 Over 65,000 children under the age of 15 worldwide are diagnosed with type 1 diabetes every year, and up to 80% of those cases result in DKA.6
However, many low and middle countries have prepared strategies and guidelines to reduce the incidence and burden of diabetes mellitus they lack funding and implementation. Seventy-one percent of nations have country-wide pointers or standards, even though less than 1/2 of countries are fully imposing them. Domestically appropriate implementation of countrywide tips wishes to be explored.1,8
Concerning the availability of drugs, 23% of low-income countries (six nations) report that insulin is normally available, and general availability of insulin within the WHO area of the Americas and European region is more than double that of the WHO African region and Southeast Asia region.9,10
Several studies in African countries show that more than half of diabetic patients have poor glycemic control, although significant progress has been made in reducing the burden of diabetes mellitus in Africa, including through the training of pediatric endocrinologists who are now practicing in 14 African nations.11,12 It is necessary to improve the education of other healthcare professionals, expand access to insulin through corporate and philanthropic initiatives, improve the availability of testing supplies only marginally, and roll out patient education materials in native languages.13
In pediatrics, poor glycemic control is a significant public health concern and a major risk factor for the emergence of diabetes-related short- and long-term problems, stunted growth, and development, disease-related medical costs, reduced life expectancy, and decreased quality of life.11 Many macro and micro-vascular consequences, including neuropathy, nephropathy, retinopathy, cardiovascular illnesses, and early death, are brought on by long-term uncontrolled hyperglycemia.11,12
By concentrating on integration into a three-tiered healthcare system, Ethiopia’s Federal Ministry of Health (FMOH) created a National Strategic Action Plan (NSAP) for four priority Non-Communicable Diseases (NCD), including DM. Unfortunately, due to a lack of resources, the nation has thus far concentrated mostly on infectious diseases.5 According to a recent study by the Ministry of Health (MoH), patients with diabetes have suboptimal glycemic control as a result of inadequate primary healthcare worker training, a lack of access to necessary diabetes medications, a lack of knowledge about the disease, poor adherence to diabetic treatment, and inadequate patient data documentation in healthcare facilities.5
To achieve correct glucose management and maintain normal growth and development, children with diabetes mellitus need to take their medications as prescribed, make necessary lifestyle changes, and periodically check their blood glucose levels. The risk of both short-term and long-term consequences of diabetes mellitus is reduced in both children and adolescents when blood glucose levels are kept at ideal levels. Yet, it is particularly challenging to achieve optimal glycemic control in this age range when you take into account the physiological and behavioral difficulties that children with diabetes mellitus face.5,13
Typically, a multidisciplinary team of professionals skilled in pediatric diabetes control and sensitive to the challenges of youngsters and adolescents with diabetes and their households ought to offer care to this population. This is not available in many low- and middle-income countries, which intern could affect the treatment outcome of children being treated in those areas.8
Moreover, diabetes imposes a big financial burden on the global healthcare gadget and the broader worldwide economic system. This burden can be measured via direct clinical cost, oblique charges associated with productiveness loss, premature mortality, and the poor effect of diabetes on countries’ gross home product (GDP).14,15
Identifying the determinants of poor glycemic control among this age group is particularly important for early modification of diabetic-related end-organ damage, and prevention of growth and developmental delays.16,17 Therefore, this study aims to assess the pattern of the initial presentation of diabetes, treatment outcome, and its predictors among children receiving service at selected public hospitals in southern Ethiopia in the last five years.
Methods and Materials
Study Area
The study was conducted at eight randomly selected public hospitals in southern Ethiopia. These hospitals were Hawassa University Comprehensive Specialized Hospital, Yirgalem General Hospital, Adare General Hospital, Shashemene Referral Hospital, Nigest Elleni Memorial Hospital, Wolaita Sodo Teaching and Referral Hospital, Halaba General Hospital, and Shone Primary Hospital.
Study Design and Period
A cross-sectional study was conducted from October 1st, 2021 to December 30, 2021, at eight selected public hospitals in southern Ethiopia.
Sample Size
The sample size was determined by using a formula for the single population proportion by considering the following assumptions. 95% level of confidence, 5% margin of error, by taking the proportion of good glycemic control 50%. Since there were no recent studies in the study area, a proportion of 50% was used to calculate the sample size.
n = (Zα/2)2p (1-p)/d2
Where:
n = sample size
P = is the proportion of good treatment outcome
d = 5% (degree of freedom maximum margin of error the researcher is willing to allow)
Z = 1.96 (standard normal deviation value corresponding to 95% confidence level)
Finally, 422 Sampled pediatrics who had a follow-up in the last five years in the selected hospitals of southern Ethiopia were recruited for the study.
Population
Source Population
All pediatrics who have a follow-up in the selected public hospitals of southern Ethiopia.
Study Population
All pediatrics who had a follow-up in the last five years in the selected hospitals of southern Ethiopia were included in the study.
Eligibility Criteria
Inclusion Criteria
All pediatric diabetic patients [with age <14 years] who had a follow-up in the last five years in the Public hospitals of southern Ethiopia were recruited for the study.
Exclusion Criteria
Those charts with incomplete data were excluded from the study.
Operational Definition
Treatment outcome was determined using HbA1c where those pediatrics whose HbA1c result >7 or RBG >200mg/dl were categorized as having poor glycemic control and those who had HbA1c result <7 or RBG <200mg/dl were categorized as having a good treatment outcome.15,18
In this study, Pediatrics is defined as all children and adolescents less than 14 years of age.15
Initial presentation: the signs and symptoms the pediatrics present with at diagnosis of DM for the first time.15
Comorbidities: are illnesses that are other than DM and its complications.
Silent presentation in this study is defined as a diabetes mellitus detected while the client comes to the health facility without showing any presenting symptoms of diabetes mellitus.
Data Collection Procedure
Data were extracted using a data extraction checklist developed by the investigator by reviewing different literature from patient charts which cover current diagnosis (including the last blood sugar level), co-morbidities, diabetic complications (long- and short-term complications), type of diabetes, blood glucose level, medication is given, and laboratory results and treatment outcomes. The checklist has two sections. The first section is used to extract data about the socio-demographic characteristics of the pediatric including age, sex, residence, religion, age at first diagnosis, and date of diagnosis. The second section of the checklist extracts data about DM care practice, complications, and treatment outcomes including the type of DM, initial and last blood glucose, type of initial presentation, the treatment being taken, history of hospitalization, history of DKA, family history of DM and presence of comorbidities. Besides a phone call has been made to parents/caregivers in need of additional information when data on the charts are not sufficient. All of the pediatrics charts data were collected by 16 nurses two for each hospital from the client’s chart after a proportional allocation of samples to each hospital depending on patient flow in the last five years. After a proportional to size allocation of samples to each hospital charts of diabetic pediatrics were selected through a systematic sampling technique among diabetic pediatrics who had follow-up in the selected hospital.
Data Processing and Analysis
The entire filled checklist was checked visually by the principal investigator. Data were coded, entered, and cleaned using Epi Data version 3.3.2 software. Errors related to inconsistency were verified using the data cleansing method and finally exported into SPSS version 24 software for analysis. During analysis, frequencies of the different variables were determined and the result was presented in texts, tables, and graphs using summary measures such as percentages, mean, and median. Bivariate logistic regression was carried out between the selected predictor variables and the outcome variable (DM treatment outcome). Multivariable logistic regression analysis was performed to see the independent effect of each variable on the outcome variable. Finally, the results of multivariable logistic regression analysis were presented in crude and adjusted odds ratios with 95% confidence intervals. All tests were two-sided and P < 0.05 was considered statistically significant.
Data Quality Control
Data quality was controlled by translating the structured questionnaire into the local language and then back to English by two people for consistency. Three days of training were given to the data collectors and supervisors. There was a brief discussion with the data collectors about the aim of the research, confidentiality of information, and content of the extraction checklist. The collected data was checked by the principal and co-investigators for its completeness and consistency. Issues were reviewed with the supervisors and data collectors. Data were stored in the form of a file in a safe location where only the investigator had access to them, and confidentiality was secured by omitting names or any other personal information. Before data input, the data were verified once again for completeness, and following data entry, the data were cleaned by performing a basic frequency for consistency. The hard copy questionnaire will be used to check for any inconsistent data, and data analysis will then begin once these tasks have been completed.
Results
Socio-Demographic Characteristics of the Respondents
The study recruited 422 pediatrics with diabetes mellitus. The mean age of study subjects in this study was 11.1+3.1 years. Of the study participants, the majority (69%) were between the ages of 10–14 years, nearly half (51.7%) were female, and 54.7% were from urban. Half of the respondents of the study (54.6%) were diagnosed with diabetes mellitus, while they were 10–14 years old and the mean age at diagnosis of diabetes mellitus was 9.2+ 3.3 years.
Morbidity Related Characteristics
Of the total participants of the study majority (92.7%) were type 1 diabetes mellitus patients and 94.3% were taking insulin. Regarding the initial pattern of presentation of DM, most (74.6%) present with DKA. The majority (73.5%) of pediatrics recruited in this study had lived with diabetes mellitus for less than 3 years, whereas the rest had lived greater than or equal to three years with an average duration of diabetes mellitus of 28.6 months but only 19.9% had a family history of DM. This study revealed that 73% of the respondents had a history of hospitalization with DKA taking the lead cause (78%) for hospitalization. Among pediatrics who have been hospitalized due to DKA, 85.8% were ketone positive. The average length of hospital stay among those who had a history of hospitalization was 6 days.
In this study, one-fifth (19.9%) had a family history of diabetes mellitus, one-third (34.4%) had DM complications, and the majority (91.7%) had a follow-up. The study also showed that 145 (34.4%) of the respondents in the study had experienced DM complications. Among these respondents, 93.7 had a history of diabetic ketoacidosis (Table 1).
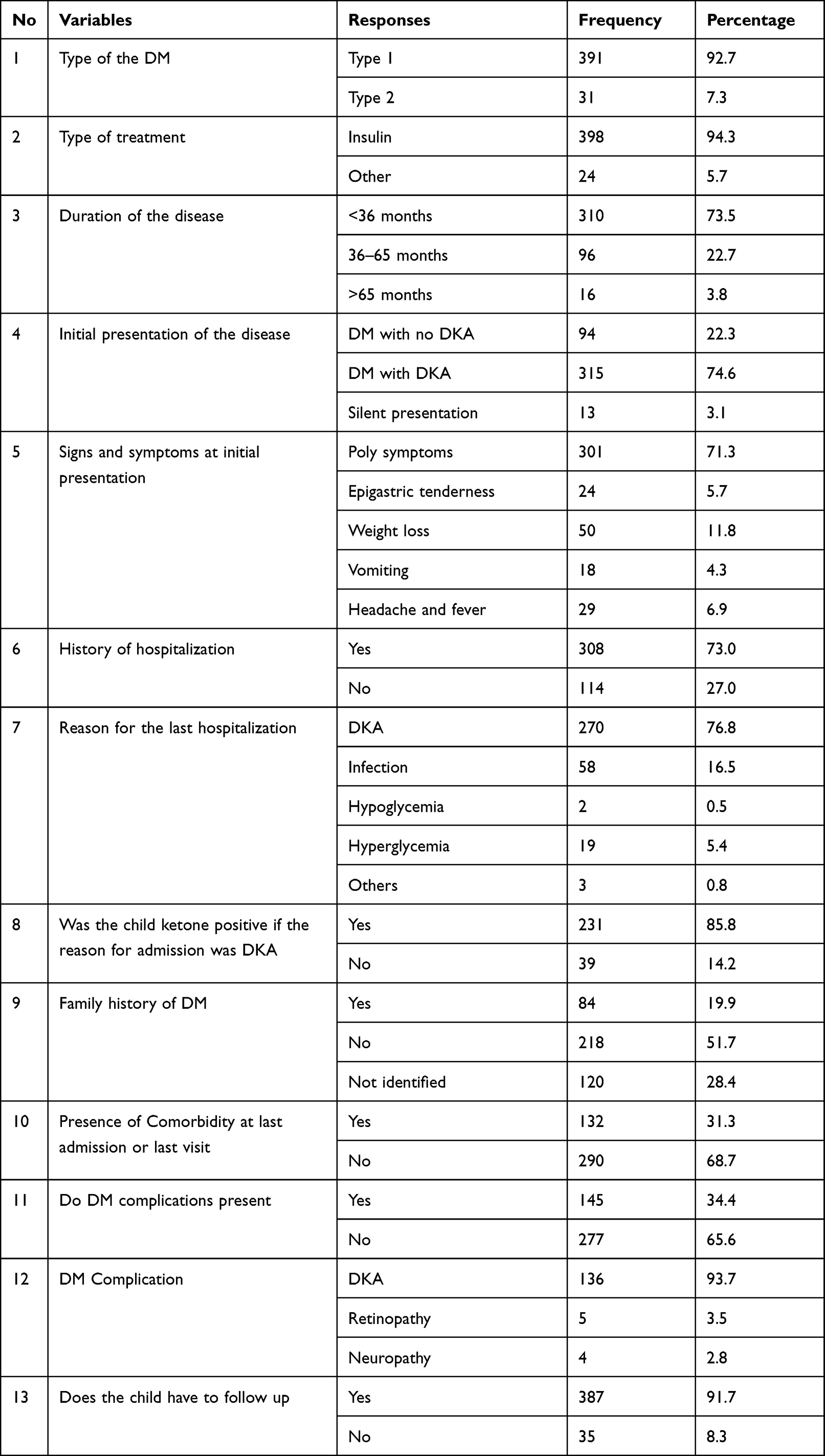 |
Table 1 Morbidity-Related Characteristics of Pediatrics with Diabetes Mellitus in Southern Ethiopia, 2020 |
Treatment Outcome
Two-thirds (67.1%) of the respondents in the study had a good treatment outcome and the rest had poor glycemic control (Figure 1).
 |
Figure 1 The level of treatment outcome of diabetes mellitus among diabetic pediatrics seeking service in selected public hospitals of south Ethiopia, 2020. |
Factors Associated with the Treatment Outcome
In bivariable logistic regression analysis; the age of the child, residence, the pattern of initial presentation, presenting signs and symptoms, history of hospitalization, family history of DM, duration of illness, comorbidity, and follow-up were statistically associated with the Treatment outcome of DM with p-value <0.25 at 95% C.I.
After adjusting for potential confounders in multivariate logistic regression analysis, only residence, presenting signs and symptoms, history of hospitalization, and comorbidity were significantly associated with the treatment outcome of DM. However, the family history of DM, the initial pattern of presentation, the age of the child, and complications of DM were not significantly associated with the treatment outcome of DM in this study.
In this study, pediatrics who live in urban were 2.574 times more likely to have a good treatment outcome compared to pediatrics living in rural areas (AOR = 2.574 (1.623–4.082)).
This study shows that pediatrics who had an initial presentation of poly symptoms were 0.082 times less likely to have a good treatment outcome compared to those who presented with fever and headache (AOR = 0.082 (0.011–0.643)). Similarly, those pediatrics who had an initial presentation of weight loss were 0.29 times less likely to have a good treatment outcome of DM compared to those who had fever and headache as the initial presentation of the disease (AOR = 0.029 (0.003–0.266)).
This study revealed that pediatrics who have a history of hospitalization were 0.457 times less likely to have a good treatment outcome for DM compared to those who had no history of hospitalization (AOR = 0.4572 (0.252–0.828)).
This study finding shows that the odds of good treatment outcome of DM are reduced by half among those who have comorbid illness than those who had no comorbidity (AOR = 0.513 (0.314–0.836)) (Table 2).
 |
Table 2 Factors Associated with Treatment Outcome of Diabetes Mellitus Among Pediatrics Seeking Service at Public Hospitals in Southern Ethiopia, 2020 |
Discussion
This study aimed to assess the treatment outcome of pediatrics with diabetes mellitus and identify associated factors. In this study, 67.1% of diabetic pediatrics in this study had good glycemic control. This finding is lower than studies conducted in the Gurage zone, southwest Ethiopia, and Brazil with a magnitude of 81.1% and 80.9%, respectively.19,20 These differences could be due to the difference in the determination of treatment outcomes including determining the treatment outcome with random and fasting blood glucose levels and differences in the socio-demographic status of populations recruited in the study, access to healthcare service, knowledge on preventive and treatment measures, and adherence to the treatment of the disease.
On the other hand, this finding is higher than studies conducted in Gondar, northwest Ethiopia, southwest Ethiopia on insulin-treated patients, Metu Karl Hospital in southwest Ethiopia, and Khartoum, Sudan, 18.3%, 27.3%, 39.5%, and 24%, respectively.21–24 The differences in the magnitude of the treatment outcome might be because of the differences in the methods used in determining the treatment outcome of diabetes mellitus as some of these studies used fasting blood glucose most of the studies which is not the case in our study. The other possible explanation is that some of these studies have studied a specific type of diabetes mellitus, whereas this study has recruited a population having either of the two types of diabetes mellitus.
In this study, pediatrics who live in urban were 2.574 times more likely to have a good treatment outcome compared to pediatrics living in rural areas (AOR = 2.574 (1.623–4.082)). This finding is consistent with the study conducted in Khartoum, Sudan, and Southern Sahara where socio-economic status and residence, respectively, had been associated with glycemic control.24,25 Similarly, a study conducted in northeast Ethiopia showed that those who live in rural areas were 2.6 times more likely to have poor glycemic control compared to those living in urban.25 Living in an urban area is attributed to getting the opportunity to easily access information from different sources regarding the disease process and the need for treatment. Moreover, it will increase the chance of the client’s access to health care.26–28
This study shows that pediatrics who had an initial presentation of poly symptoms were 0.082 times less likely to have a good treatment outcome compared to those who presented with fever and headache (AOR = 0.082 (0.011–0.643)). Similarly, those pediatrics who had an initial presentation of weight loss were 0.29 times less likely to have a good treatment outcome of DM compared to those who had fever and headache as an initial presentation of the disease (AOR = 0.029 (0.003–0.266)). This might be because those who had weight loss and poly symptoms might be considered as symptoms of full-blown diabetes mellitus which might have relatively stayed longer time and affected the client’s body for long compared to those who had fever and headache or it can be associated with poor adherence to insulin therapy as taking insulin can lead to weight gain that, in turn, might have played its part in future treatment outcomes.29,30
This study revealed that pediatrics who have a history of hospitalization were 0.457 times less likely to have a good treatment outcome for DM compared to those who had no history of hospitalization (AOR = 0.4572 (0.252–0.828)). This might be because those who had a history of hospitalization are more likely to have passed through complications and severe illnesses that needed hospitalization. Similar to this finding, a study in western Ethiopia and Turkey where hospitalization due to complications was significantly associated with poor glycemic control.22,31 Admission due to diabetes mellitus is associated with hyperglycemia in critically ill patients, the perioperative management of diabetes, and the treatment of complications of diabetes itself, such as diabetic ketoacidosis. The development of severe illnesses and complications are sometimes associated with poor behavioral characteristics and treatment adherence which in turn affects treatment outcomes.32,33
This study finding shows that the odds of good treatment outcome of DM are reduced by half among those who have comorbid illness than those who had no comorbidity (AOR = 0.513 (0.314–0.836)). This finding is congruent with the findings of a study from Turkey.31 Studies show that about one-quarter of children with type 1 diabetes have thyroid autoantibodies (thyroid peroxidase antibodies or antithyroglobulin antibodies) at the time of diagnosis. Similarly, celiac disease has an increased frequency in patients with type 1 diabetes (1–16% of individuals compared with 0.3–1% in the general population).34 The presence of a comorbid disease weakens the immune system, increases the chance of developing hyperglycemia, and raises the need for insulin. Therefore, if prompt and proper adjustments are not done in the insulin therapy for the clients it can result in poor glycemic control.30,35,36
Conclusion
This study found that type 1 diabetes mellitus is still the dominant type of diabetes mellitus in the pediatric age group. Diabetes mellitus with DKA is the predominant pattern of initial presentation in the study. The magnitude of poor treatment outcomes of diabetes mellitus among pediatrics in this study is high and unacceptable Residence, signs, and symptoms at initial presentation, history of hospitalization, and comorbidity were found to be independent predictors of treatment outcome of pediatric diabetes mellitus in this study.
Recommendations
Hospitals in Southern Ethiopia
Shall provide prior and continuous health education for diabetic pediatrics and their parents about the need for health institution visits during comorbidity for proper treatment of diabetes mellitus.
It would be beneficial to the clients if emphasis is given to diabetic pediatrics with comorbidity so that the comorbid diseases will be treated properly and promptly. Besides, treatment of diabetes in pediatrics with comorbid diseases shall be carried out properly as per guidelines of treatment.
Ministry of Health and Regional Health Bureaus
Shall work to widen the accessibility of health services in the rural area and strengthen the service provided by health institutions in the rural area, so that diabetic pediatrics in the rural area will have easy access and regular and uninterrupted follow-up.
The Ministry of Health through its technical arms shall conduct a nationwide study with analytical methods on the predictors of treatment outcomes of pediatrics with diabetes mellitus.
Researchers
Shall conduct studies on this study area through a better research design by including those in the group between 15 and 17 years as they are not commonly addressed.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available upon request from the corresponding author and co-authors.
Ethics Approval and Consent to Participant
Ethical clearance was obtained from the Institutional Health Research Ethical Review Board of the College of Medicine and Health Sciences, Hawassa University. Accordingly, permission was obtained from the regional and zonal health Bureaus and an official letter was distributed to the hospitals included in the study. Verbal informed consent was obtained from parents/guardians of the study participants through phone calls after informing the purpose of the study. This was part of the ethical review by the institutional board which garnets the ethical clearance for the study, and the verbal consent from parents/guardians was accepted and approved by the board as the respondents of the study are pediatrics. Permission from the hospital administrators was obtained before field activities started. Informed consent was obtained from participants of the study before the initiation of data collection. No names were recorded on the data collection tools. Permission to enter the facility and to review the medical records of clients was requested at the beginning of data collection. The study protocol was ethically approved by the Institutional Review Board (IRB) of Hawassa University, College of Medicine and Health Sciences with the reference number IRB/116/12.
Acknowledgment
The authors are grateful to the data collectors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Roglic G. WHO Global report on diabetes: a summary. Int J Noncommun Dis. 2016;1(1):3.
2. Kharroubi AT, Darwish HM. Diabetes mellitus: the epidemic of the century. World j Diabetes. 2015;6(6):850. doi:10.4239/wjd.v6.i6.850
3. Fiseha T, Alemayehu E, Kassahun W, Adamu A, Gebreweld A. Factors associated with glycemic control among diabetic adult out-patients in Northeast Ethiopia. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-018-3423-5
4. Ogle GD, James S, Dabelea D, et al. Global estimates of incidence of type 1 diabetes in children and adolescents: results from the International Diabetes Federation Atlas. Diabetes Res Clin Practice. 2022;183:109083. doi:10.1016/j.diabres.2021.109083
5. Non-communicable O. National Strategic Action Plan (Nsap) for Prevention & Control of Non-Communicable Diseases in Ethiopia; 2016.
6. Yigazu DM, Desse TA. Glycemic control and associated factors among type 2 diabetic patients at Shanan Gibe Hospital, Southwest Ethiopia. BMC Res Notes. 2017;10(1):1–6. doi:10.1186/s13104-017-2924-y
7. Gebermariam AD, Tiruneh SA, Ayele AA, et al. Level of glycemic control and its associated factors among type II diabetic patients in Debre Tabor General Hospital, northwest Ethiopia. Metab Open. 2020;8:100056. doi:10.1016/j.metop.2020.100056
8. Tremblay MS, Carson V, Chaput JP, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behavior, and sleep. Appl Physiol Nutr Metab. 2016;41(Suppl. 3):S 311–27. doi:10.1139/apnm-2016-0151
9. Marathe PH, Gao HX, Close KL. American Diabetes Association Standards of Medical Care in Diabetes. Ann Int Med. 2017;168(9):640.
10. Taylor JS, Kacmar JE, Nothnagle M, et al. A systematic review of the literature associating breastfeeding with type 2 diabetes and gestational diabetes. J Am Coll Nutr. 2005;24(5):320–326. doi:10.1080/07315724.2005.10719480
11. Gebreyohannes EA, Netere AK, Belachew SA. Glycemic control among diabetic patients in Ethiopia: a systematic review and meta-analysis. PLoS One. 2019;14(8):e0221790. doi:10.1371/journal.pone.0221790
12. Kibirige D, Akabwai GP, Kampiire L, Kiggundu DS, Lumu W. Frequency and predictors of suboptimal glycemic control in an African diabetic population. Int J Gen Med. 2017;10:33. doi:10.2147/IJGM.S124548
13. Piloya-Were T, Sunni M, Ogle GD, Moran A. Childhood diabetes in Africa. Curr Opinion Endocrinol Diabetes Obesity. 2016;23(4):306–311. doi:10.1097/MED.0000000000000262
14. Henderson M, Benedetti A, Barnett TA, et al. Influence of adiposity, physical activity, fitness, and screen time on insulin dynamics over 2 years in children. JAMA Pediatr. 2016;170(3):227–235. doi:10.1001/jamapediatrics.2015.3909
15. Dejkhamron P, Menon RK, Sperling MA. Childhood diabetes mellitus: recent advances & prospects. IJMR. 2007;125(3):231.
16. Al Zahrani AM, Al SA. Glycemic control in children and youth with type 1 diabetes mellitus in Saudi Arabia. Clin Med Insights Endocrinol Diabetes. 2019;12:1179551418825159. doi:10.1177/1179551418825159
17. Dumrisilp T, Supornsilchai V, Wacharasindhu S, Aroonparkmongkol S, Sahakitrungruang T. Factors associated with glycemic control in children and adolescents with type 1 diabetes mellitus at a tertiary-care center in Thailand: a retrospective observational study. Asian Biomed. 2017;11(6):443–450. doi:10.1515/abm-2018-0021
18. Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes. 2018;19 Suppl 27(19):155–177. doi:10.1111/pedi.12701
19. Gebre BB, Assefa ZM. The magnitude and associated factors of diabetic complication among diabetic patients attending Gurage zone hospitals, South West Ethiopia. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4808-9
20. Andrade CJ, Alves CD. Influence of socioeconomic and psychological factors in glycemic control in young children with type 1 diabetes mellitus. J de Pediatria. 2019;95(1):48–53. doi:10.1016/j.jped.2017.11.002
21. Fasil A, Biadgo B, Abebe M. Glycemic control and diabetes complications among diabetes mellitus patients attending at University of Gondar Hospital, Northwest Ethiopia. Diabetes Metab Syndr Obes. 2019;12:75. doi:10.2147/DMSO.S185614
22. Oluma A, Abadiga M, Mosisa G, Etafa W. Magnitude and predictors of poor glycemic control among patients with diabetes attending public hospitals of Western Ethiopia. PLoS One. 2021;16(2):e0247634. doi:10.1371/journal.pone.0247634
23. Sheleme T, Mamo G, Melaku T, Sahilu T. Glycemic control and its predictors among adult diabetic patients attending Mettu Karl Referral Hospital, Southwest Ethiopia: a prospective observational study. Diabetes Therapy. 2020;11(8):1775–1794. doi:10.1007/s13300-020-00861-7
24. Taha Z, Eltoum Z, Washi S. Predictors of glucose control in children and adolescents with type 1 diabetes: results of a cross-sectional study in Khartoum, Sudan. Open Access Maced J Med Sci. 2018;6(11):2035. doi:10.3889/oamjms.2018.423
25. Camara A, Baldé NM, Sobngwi-Tambekou J, et al. Poor glycemic control in type 2 diabetes in the South of the Sahara: the issue of limited access to an HbA1c test. Diabetes Res Clin Practice. 2015;108(1):187–192. doi:10.1016/j.diabres.2014.08.025
26. Mazza S. Does Urbanization or Industrialization Have More Impact on the Increasing Prevalence of Diabetes in Developing Countries?. 2020.
27. Gassasse Z, Smith D, Finer S, Gallo V. Association between urbanisation and type 2 diabetes: an ecological study. BMJ Global Health. 2017;2(4):e000473. doi:10.1136/bmjgh-2017-000473
28. Stojanović M, Cvetanović G, Anđelković Apostolović M, Stojanović D, Rančić N. Impact of socio-demographic characteristics and long-term complications on quality of life in patients with diabetes mellitus. Central Eur j Public Health. 2018;26(2):104–110. doi:10.21101/cejph.a5022
29. Roberts I. Nelson’s textbook of pediatrics. Kliegman R, Stanton B, St. Geme J, Schor N, editors.
30. Asche C, LaFleur J, Conner C. A review of diabetes treatment adherence and the association with clinical and economic outcomes. Clin Ther. 2011;33(1):74–109. doi:10.1016/j.clinthera.2011.01.019
31. Kayar Y, Ilhan A, Kayar NB, et al. Relationship between the poor glycemic control and risk factors, lifestyle and complications. Biomed Res. 2017;28(4):1581–1586.
32. Sarwar N, Gao P, Seshasai SR, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Emerging Risk Factors Collaboration. Lancet. 2010;26(375):2215–2222.
33. Inzucchi SE Management of diabetes mellitus in hospitalized patients. Available from: https://www.Up-to-date.Com/contents/management-of-diabetes-mellitus-in-hospitalized-patients.
34. Chiang JL, Kirkman MS, Laffel LM, Peters AL. Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care. 2014;37(7):2034. doi:10.2337/dc14-1140
35. Cho YY, Cho SI. Treatment variation related to comorbidity and complications in type 2 diabetes: a real world analysis. Medicine. 2018;97(37):e12435. doi:10.1097/MD.0000000000012435
36. Pantalone KM, Hobbs TM, Wells BJ, et al. Clinical characteristics, complications, comorbidities and treatment patterns among patients with type 2 diabetes mellitus in a large integrated health system. BMJ Open Diabetes Res Care. 2015;3(1):e000093. doi:10.1136/bmjdrc-2015-000093
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.