")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
The Patient Journey in Facial Aesthetics: Findings from a European Consensus Meeting on Improving the Quality of Life for Patients Receiving Botulinum Toxin Injections
Authors Philipp-Dormston WG, De Boulle K , Gronovich Y, Lowe N, Sayed K, Sykianakis D, Tuncer S
Received 15 November 2023
Accepted for publication 25 January 2024
Published 2 February 2024 Volume 2024:17 Pages 329—337
DOI https://doi.org/10.2147/CCID.S446891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Wolfgang G Philipp-Dormston,1,2 Koenraad De Boulle,3 Yoav Gronovich,4 Nick Lowe,5,6 Karim Sayed,7– 9 Dimitrios Sykianakis,10 Serhan Tuncer11
1Hautzentrum Köln, Cologne, Germany; 2Faculty of Health, University Witten/Herdecke, Witten, Germany; 3Aalst Dermatology Clinic, Aalst, Belgium; 4Department of Plastic and Reconstructive Surgery, Shaare Zedek Medical Center, Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel; 5University of Manchester, Manchester, UK; 6University of California, Los Angeles School of Medicine, Los Angeles, CA, USA; 7Nomi Oslo Clinic, Oslo, Norway; 8Ouronyx Clinic, London, UK; 9University of South-Eastern Norway, Drammen, Norway; 10Well Aging Athens Clinic, Athens, Greece; 11Private Practice, Ankara, Turkey
Correspondence: Wolfgang G Philipp-Dormston, Hautzentrum Köln, Schillingsrotter Str. 39-41, Cologne, 50996, Germany, Tel +49 221 39800200, Fax +49 221 39800201, Email [email protected]
Purpose: Successful treatment of facial lines with botulinum toxin is largely dependent on patient satisfaction; thus, a structured treatment journey that uses patient-reported outcomes (PROs) is helpful for maximizing botulinum toxin results. To develop a patient-centric approach for botulinum toxin injections in facial aesthetics, a group of clinicians met to provide opinions on an optimal treatment journey that uses PROs to quantify treatment benefits on patient quality of life.
Patients and Methods: A multidisciplinary panel of 9 clinicians with expertise in facial aesthetic procedures convened for an advisory board that was preceded by and followed up with a structured, multistep consensus discussion. Based on current literature, the panel’s expertise, structured questions, and group discussion, panelists assessed, reconciled, and agreed upon on a patient journey for botulinum toxin treatment in facial aesthetics.
Results: Panelists agreed that an optimal patient journey includes screening, assessment, treatment, posttreatment, and follow-up visits. A compact, easy-to-complete, and digital PRO questionnaire should be provided before the visit. During screening, thorough assessments are integral for a successful patient journey because they provide an opportunity to understand treatment goals, address patient concerns, discuss risks and benefits, obtain medication lists/medical history, and take pretreatment photographs. Treatment strategies should include discussing and educating on the approach/choice of botulinum toxin and ensuring patients are comfortable. Posttreatment, clinicians should request intense muscle movements to enhance product uptake and be available to address patient concerns. Finally, during follow-up, PRO questionnaires can be provided to gauge patient satisfaction with treatment, and pretreatment photographs can be provided to allow patients to track their progression. Follow-ups should be scheduled with new patients or those reporting low satisfaction.
Conclusion: Establishing a relationship, being aware of the patient’s goals, and developing an individualized care plan allows for a structured, patient-centered treatment journey that promotes positive aesthetic outcomes.
Keywords: patient satisfaction, patient-reported outcome measures, neurotoxins, body image, skin aging
Introduction
Botulinum toxin, a neurotoxin protein derived from the Clostridium botulinum bacterium, inhibits vesicular fusion to the nerve terminal membrane via cleavage of synaptosomal-associated protein-25 (SNAP-25), ultimately inhibiting acetylcholine release from the motor neuron and causing a temporary decrease in muscle activity.1,2 The effects of botulinum toxin in targeted muscles diminish over time as SNAP-25 regenerates, and neuromuscular signaling and muscle contractility are restored.3 Of the 7 botulinum toxin serotypes (A–G), types A and B are currently the most commonly used in cosmetic applications, with serotype A being more frequently used than B.4
OnabotulinumtoxinA (onabotA) has been used effectively and safely to treat facial lines since the early 1990s5,6 and is approved in the European Union for the treatment of moderate to severe glabellar lines, lateral canthal lines, and/or forehead lines, and when the severity of facial lines has an important psychological impact on adult patients.7 Facial lines can negatively influence self-perception, alter the perception of others about age and emotional status, or have unfavorable psychological impacts.8,9 In addition, dissatisfaction with facial appearance can reduce self-esteem and lead to negative psychosocial impacts, such as social anxiety and isolation.10 As such, successful treatment of facial lines is associated with improved self-esteem and quality of life (QoL), as well as psychological and social benefits.11–15
Treatment of facial lines with neurotoxins was among the top nonsurgical procedures performed in 2021,16 and measuring patient-reported outcomes (PROs) is essential in determining the aesthetic benefits of botulinum toxin treatment. PROs measure patient experiences, preferences, and perceptions, each of which contributes to overall satisfaction.17 These measurements are particularly important for aesthetic procedures, where patient satisfaction is strongly tied to issues of self-esteem and body image; thus, a highly satisfied patient is indicative of a successful outcome.13
PROs not only gauge treatment satisfaction but also quantify patient perspectives on QoL assessments that cannot be evaluated from clinical observations alone.15 Validated PRO scales for facial aesthetics include the FACE-Q, Facial Line Outcomes 11 (FLO-11), and Facial Line Satisfaction Questionnaire (FLSQ).18–20 The FACE-Q assesses psychological impact of facial appearance, QoL, satisfaction with outcome, adverse effects, and/or patient experiences,18 whereas the FLSQ and FLO-11 assess the psychological impact of and satisfaction with upper facial lines, including crow’s feet, forehead, and glabellar lines.19,20
Given the social and personal impacts of facial aesthetics on QoL, a consistent and structured patient journey that utilizes PROs is needed to aid clinicians in maximizing results. Presently, PROs may be underutilized in clinical practice,21 and a structured patient journey has yet to be defined in the realm of facial aesthetics. To develop a patient-centric approach for facial aesthetics for botulinum toxin treatments, a group of clinicians met to provide opinions on the patient journey, enhancing patient QoL, and optimal treatment strategies to support the patient experience.
Materials and Methods
On May 12, 2022, a multidisciplinary panel of 9 clinicians with expertise in facial aesthetic procedures, consisting of aesthetic physicians, dermatologists, general practitioners, and plastic surgeons, convened for a consensus meeting in Bonn, Germany. The meeting was preceded by and followed up with a structured, multistep consensus discussion. The objectives of the meeting were to analyze, discuss, and agree upon strategies for supporting patients along the patient journey in botulinum toxin facial aesthetics, understand how patient screening and assessment can be enhanced to support patient experience and optimize clinic flow, and gain insights into capturing and reporting QoL and PROs to support patients and aesthetic clinicians. Based on current literature, the panel’s expertise, structured questions, and group discussion, panelists assessed, reconciled, and agreed upon on an optimal patient journey for botulinum toxin treatment for facial aesthetics. Given the nature of this initiative, no review/approval by an institutional review board was sought or required. Written informed consent for publication of photographs was obtained from the patient.
Results
The Patient Journey
Beyond evaluating the clinical benefits of botulinum toxin in facial aesthetics, increased recognition of patient experiences through their unique journey can guide decision-making for clinicians. In the realm of facial aesthetics, the patient journey often includes screening, assessment, treatment, posttreatment, and follow-up visits (Figure 1).
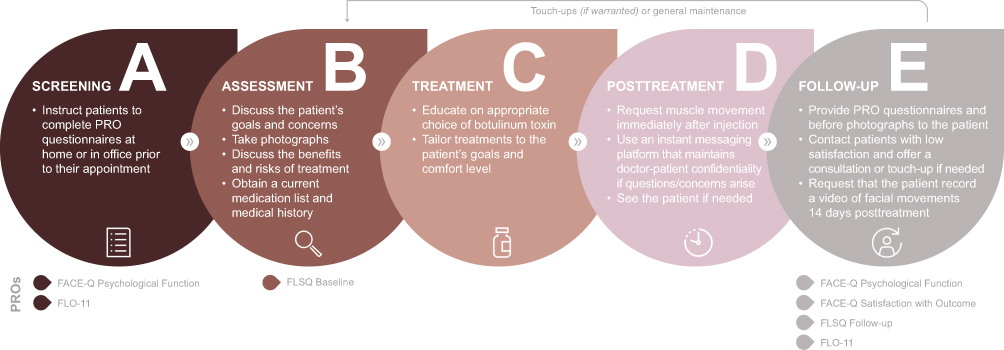 |
Figure 1 The patient journey in facial aesthetics. (A) Screening, (B) assessment, (C) treatment, (D) posttreatment, and (E) follow-up. Abbreviations: FLO-11, Facial Line Outcomes; FLSQ, Facial Line Satisfaction Questionnaire; PRO, patient-reported outcomes. |
Screening
During screening (Figure 1A), clinicians should request patient completion of PRO questionnaires, such as the FACE-Q or FLO-11,18,20 at home before their visit (potentially with appointment reminders) or while waiting to see the clinician. Questionnaires should be straightforward, compact, easy to complete, and digital to promote compliance. Optimal screening strategies are listed in Box 1.
 |
Box 1 Optimal Screening Strategies |
Assessment
During the assessment (Figure 1B), clinicians should focus on the patient’s goals for treatment. It is useful to explain that the patient and clinician are on a journey together, and answering the clinicians’ questions provides an opportunity for personalized treatment. The panelists generally agreed that PRO questionnaires, such as the FLSQ Baseline,19 should be used to gauge self-perception and goals; however, not all parts of an assessment can be standardized, and most must be individualized depending on patient needs. For example, treatment preferences may vary among patients depending on age, gender identity, sex, and race or ethnicity.22–25
Photography is essential in explaining treatment goals, especially at a preliminary consultation.26 Sequential photographs are powerful patient data to capture, considering these allow patients to see their progress or how the formation of new lines has been prevented over time. Ideally, pre- and posttreatment photography should be standardized by using the same camera, lens, settings, magnifications, illumination, and patient positions at each visit.26 In addition, camera position/distance should be uniform at each visit through the use of a tripod to fix the camera’s position and a floor marking.26 Postprocedural photographs should be taken only after an adequate time has passed since the injections.26
It is important to understand each patient’s unique needs because the patient will likely have different outcomes they are looking to achieve. Beyond an initial assessment, it is also important to continue an open dialogue with patients at each visit because priorities may shift with age and tend to vary with gender, including with gender-fluid persons, who may prefer a different look at different times in their lives.22,23
Clinicians should not only discuss the benefits of treatment for meeting the patient’s goals, but also understand concerns and discuss the possibilities of adverse events. It is vital to explain that botulinum toxin can potentially prevent the appearance of aging, rather than just remove wrinkles.27 Cosmetic botulinum toxin injections for persons aged <18 years who have no visible signs of aging are not recommended, in an effort to preserve muscle tone.28,29 In fact, in some countries, including England, aesthetic botulinum toxin treatment is currently not permitted by law to those aged <18 years.30
If unwanted outcomes are considered as adverse events, there are strategies to manage patient expectations to avoid them. Clinicians should obtain a current medication list, as well as a complete medical history (including allergies, illnesses, previous surgeries and immunizations, and if the patient is currently pregnant or breastfeeding) to identify contraindications; it is particularly important to determine recent use of anticoagulants because this may increase the potential risk of bruising.31 Information regarding previous aesthetic procedures, including satisfaction with outcomes from those procedures, should also be obtained. Optimal assessment strategies are listed in Box 2.
 |
Box 2 Optimal Assessment Strategies |
Treatment
During treatment (Figure 1C), clinicians should spend ample time discussing and educating on the best treatment approach. Some patients may be influenced by social media or direct-to-consumer advertising, leading to requests for a specific product; however, product choice should be determined by the clinician.
To maintain a good patient-clinician relationship, it is ideal to individualize the treatment plan based on the patient’s goals and comfort level. If a botulinum toxin–naive patient is anxious about receiving injections for the first time, it is recommended to have them come back 7 to 14 days after the initial injection for an evaluation/follow-up to determine if additional treatment is required.31 This can boost the patient’s confidence, and may provide the injector with feedback about future treatment sites and doses. Optimal treatment strategies are listed in Box 3.
 |
Box 3 Optimal Treatment Strategies |
Posttreatment
After botulinum toxin injections (Figure 1D), most panelists agreed that intense, but not rapid, expressive facial movements (eg, looking angry, lifting the brow, and/or smiling) for 5 to 10 minutes within the first 20 minutes following treatment maximize the uptake of botulinum toxin at the neuromuscular junction.32
After patients leave the clinic, use of an instant messaging platform that ensures doctor-patient confidentiality allows patients to readily contact the clinician with any concerns. This method of communication also allows the clinician to potentially assess a high-quality video to determine whether a follow-up is necessary, allowing patients to feel more confident posttreatment. However, messaging platforms may only be useful for those who are interested and have the technical abilities to use them. Ultimately, clinician availability posttreatment is of the utmost importance, especially with botulinum toxin–naive patients, who may be more anxious than those who are more experienced with injections. Optimal posttreatment strategies are listed in Box 4.
 |
Box 4 Optimal Posttreatment Strategies |
Follow-Up
During the follow-up period (Figure 1E), providing PRO questionnaires is recommended, such as the FACE-Q Psychological Function and/or Satisfaction with Outcome, FLSQ Follow-up, or FLO-11,18–20 along with pretreatment photographs to encourage patients to track their results. If a follow-up questionnaire is provided, the clinic should contact patients who reported low satisfaction to better understand the rationale behind their rating. To encourage patients to return to the original clinic for adjustments, the clinic should directly oversee all patient concerns and provide a treatment plan aimed at achieving their intended result.
Touch-ups should be performed only when needed, or per patient request, and not on a regular basis. The dosing and waiting period for touch-ups may vary based on the injector’s preference and indication of the treated area.31,33 The panelists agreed that performing a full repeat treatment in less than 3 months should be avoided due to the risk of neutralizing antibodies;34 however, a recent meta-analysis by Jankovic et al found no clear relationship between neutralizing antibody formation and dosing interval, with the overall incidence of neutralizing antibodies being low (≤1.4%).35
To ensure optimal results, some panelists have found it useful to request that patients bring videos to their next appointment demonstrating their facial muscle movements 14 days posttreatment. This technique tends to be popular with patients in clinical practice. In addition, these posttreatment videos allow the clinician to monitor the results over time and tailor/fine-tune injections at each appointment, considering muscles and behavior change with aging and repeated treatments. Optimal follow-up strategies are listed in Box 5.
 |
Box 5 Optimal Follow-Up Strategies |
Case Study: An Optimal Patient Journey
Representative images of a patient treated with onabotA over an 18-year period are shown in Figure 2. This nearly 2-decade-long treatment is a unique example emphasizing the importance of the patient journey and the patient-physician long-term, life-long relationship, a concept that was recently discussed by Cohen et al36
 |
Figure 2 Representative photographs of a patient treated with onabotulinumtoxinA over an 18-year period. This patient began receiving onabotulinumtoxinA in December 2000, but no digital photographs were available until 2006. Photos were taken upon arrival to the clinic, and images from an interval of approximately every 1–2 years are shown as follows: 2006 (A), 2008 (B), 2010 (C), 2012 (D), 2014 (E), 2016 (F), 2018 (G), 2020 (H), 2022 (I), and 2023 (J). On average, the patient received 3 sessions per year from March 2006 (age, 43 years) to June 2023 (age, 60 years), totaling 58 clinic visits, including 5 touch-ups. The total dose of onabotulinumtoxinA per treatment session for glabellar frown lines, horizontal frontal rhytids, and canthal lines varied between 40 and 60 units. |
Discussion
A group of panelists met to analyze, discuss, and reach a consensus upon optimal patient-centered management of facial botulinum toxin injections and determined that the patient journey typically includes screening, assessment, treatment, posttreatment, and follow-up periods. The panelists’ opinions regarding a structured patient journey and treatment strategies were used to adopt an approach to facial botulinum toxin treatments, with a focus on enhancing PROs and QoL.
The goals of the treating clinician and the patient may vary; a survey found that clinicians tend to emphasize symmetrical and delicate outcomes, whereas patients generally prefer a clean and natural aesthetic result.37 Patients seeking facial aesthetic treatments represent a clinically heterogeneous group, each presenting with an individual set of perceived needs.38,39 Individual patient factors, such as treatment expectations, preferences, budget, sex/gender, age, other medical or cosmetic conditions, ethnic/cultural preferences, and skin type, influence the overall approach. Thus, listening to patient preferences/concerns, recognizing patient involvement, translating patient experiences, and understanding patient outcomes are key elements for an optimal patient journey in facial aesthetics.
Facial treatment preferences and needs often involve multiple factors that may change over time, including aging, atrophy, and behavioral modifications. For example, aesthetically aware women may become more concerned with features of the lower face with age.22 Transgender aesthetic goals likely revolve around acquiring attributes that align with the patient’s self-affirmation, and thus tend to be highly individualized.23 The primary focus of aesthetically aware men is more likely to be the periorbital area,24 whereas the entire upper face may be of more concern to women.22 In addition, unique racial and ethnic features should be respected, because racial variation impacts skin aging and correction.25 Determining and understanding patient preference with a thorough assessment is integral for successful treatment outcomes.
Open communication between the clinician and patient allows for the development of an individualized care plan that lends itself to enhanced patient satisfaction. Systematic reviews have shown that most clinical studies report a high rate of patient satisfaction with botulinum toxin treatment,40,41 and onset of effect and duration of action are factors of efficacy that determine treatment satisfaction.42 In addition to treatment efficacy, assessment of patient satisfaction is an optimal way to determine patients’ opinions about aesthetic procedures, which should be considered the most important factor for defining treatment success.43 An important part of managing patient satisfaction is assessing outcomes with PRO assessments, with scheduling of follow-up appointments being done if touch-ups are needed.
To promote compliance with follow-ups, self-recorded videos are useful for busy patients. Post-injection video analyses are a reliable, clinically feasible measure of botulinum toxin injection efficacy in other indications,44 and are also applicable in facial aesthetics. In addition, routine collection of post-injection PRO data in clinical practice is essential for identifying problems, facilitating communication, and directing appropriate treatment of underappreciated concerns.38
Limitations exist for the validated PRO assessments currently available. Administration of comprehensive questionnaires can lead to patient fatigue and inaccuracy in self-reporting,45 smart phone capabilities are underutilized and could enhance compliance with PROs, and assessments often fail to fully capture highly individualized needs.38 Additional PRO assessments are also needed to better address diverse ethnicities, age groups, and gender identities.45 Ultimately, the development of a simple, standardized, pretreatment questionnaire to collect PRO and QoL data from patients seeking botulinum toxin treatment is needed.
Future areas of research include collecting PRO and QoL data to demonstrate the use of aesthetic treatments in improving diverse psychosocial outcomes, which also has the benefit of mitigating negative stigma around aesthetic medicine. Ideally, more data on the preventive or antiaging value of botulinum toxin treatments should be obtained, but validated endpoints are needed for clinical trials. In addition, common botulinum toxin treatment goals in more diverse patient populations should be assessed, for example, on the goals of gender-fluid persons.
Conclusion
To our knowledge, this is the first manuscript describing a structured patient journey that includes PROs for patients undergoing facial aesthetic treatments with botulinum toxin to increase patient satisfaction and QoL, supporting an approach to treatment that is centered around the patient. The key steps in the facial aesthetics structured patient journey were determined to be screening, assessment, treatment, posttreatment, and follow-up; the structured patient journey and related treatment strategies can be used to help enhance PROs and QoL. Ultimately, establishing a relationship, being aware of the patient’s goals, and developing an individualized care plan that includes and encourages maintenance treatments and the ongoing active participation of both the patient and clinician set the stage for a structured yet patient-centered treatment journey leading to safe, natural, and effective aesthetic outcomes.
Abbreviations
FLO-11, Facial Line Outcomes 11; FLSQ, facial line satisfaction questionnaire; onabotA, onabotulinumtoxinA; PROs, patient-reported outcomes; QoL, quality of life; SNAP-25, synaptosomal-associated protein-25.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications.
These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://vivli.org/ourmember/abbvie/ then select “Home”.
Acknowledgments
The authors acknowledge the contributions of the late Dr. Massimo Signorini. Medical writing support was provided to the authors by Jessica Brunquell, PhD of Peloton Advantage, LLC (an OPEN Health company) and was funded by Allergan Aesthetics, an AbbVie Company.
Funding
Allergan Aesthetics, an AbbVie Company, funded this study and participated in the study design, research, analysis, data collection, interpretation of data, reviewing, and approval of the publication. All authors had access to relevant data and participated in the drafting, review, and approval of this publication. No honoraria or payments were made for authorship.
Disclosure
Wolfgang Philipp-Dormston is a consultant to, speaker for, clinical trial investigator for, and has received scientific grants and honoraria from Allergan, an AbbVie Company, Evolus, Galderma, and Merz. He is senior president of the German Society for Aesthetic Botulinum- and Filler-Therapy (DGBT).
Koenraad De Boulle is a consultant to, speakers bureau member for, and has received grants and honoraria from Allergan, an AbbVie Company; he is an IBSA consultant.
Yoav Gronovich is a consultant for Allergan, an AbbVie Company.
Nick Lowe owns stock in and received consultant payments from AbbVie/Allergan.
Karim Sayed is a consultant to, speaker for, and has received honoraria from Teoxane, L’oréal/Skinceuticals, and Allergan, an AbbVie Company.
Dimitrios Sykianakis is a consultant to, speaker for, and has received honoraria from Allergan, an AbbVie Company.
Serhan Tuncer is a consultant to, speaker for, and has received honoraria from Allergan, an AbbVie Company.
References
1. Blasi J, Chapman ER, Link E, et al. Botulinum neurotoxin A selectively cleaves the synaptic protein SNAP-25. Nature. 1993;365(6442):160–163. doi:10.1038/365160a0
2. Burgen AS, Dickens F, Zatman LJ. The action of botulinum toxin on the neuro-muscular junction. J Physiol. 1949;109(1–2):10–24. doi:10.1113/jphysiol.1949.sp004364
3. Small R. Botulinum toxin injection for facial wrinkles. Am Fam Physician. 2014;90(3):168–175.
4. Satriyasa BK. Botulinum toxin (Botox) A for reducing the appearance of facial wrinkles: a literature review of clinical use and pharmacological aspect. Clin Cosmet Invest Dermatol. 2019;12:223–228. doi:10.2147/CCID.S202919
5. Carruthers A, Carruthers JDA. Botulinum toxin in the treatment of glabellar frown lines and other facial wrinkles. In: Jankovic J, Hallett M, editors. Therapy with Botulinum Toxin. New York, NY: Marcel Dekker, Inc.; 1994:577–595.
6. Carruthers JD, Carruthers JA. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J Dermatol Surg Oncol. 1992;18(1):17–21. doi:10.1111/j.1524-4725.1992.tb03295.x
7. Botox [summary of product characteristics]. Bucks, UK: Allergan; 2020.
8. Finn JC, Cox SE, Earl ML. Social implications of hyperfunctional facial lines. Dermatol Surg. 2003;29(5):450–455. doi:10.1097/00042728-200305000-00003
9. Dayan S, Yoelin SG, De Boulle K, Garcia JK. The psychological impacts of upper facial lines: a qualitative, patient-centered study. Aesthet Surg J Open Forum. 2019;1(2):1–10. doi:10.1093/asjof/ojz015
10. Gupta MA, Gilchrest BA. Psychosocial aspects of aging skin. Dermatol Clin. 2005;23(4):643–648. doi:10.1016/j.det.2005.05.012
11. Cohen JL, Rivkin A, Dayan S, et al. Multimodal facial aesthetic treatment on the appearance of aging, social confidence, and psychological wellbeing: HARMONY study. Aesthet Surg J. 2022;42(2):NP115–NP124. doi:10.1093/asj/sjab114
12. Dayan S, Rivkin A, Sykes JM, et al. Aesthetic treatment positively impacts social perception: analysis of subjects from the HARMONY study. Aesthet Surg J. 2019;39(12):1380–1389. doi:10.1093/asj/sjy239
13. Dayan SH, Arkins JP, Patel AB, Gal TJ. A double-blind, randomized, placebo-controlled health-outcomes survey of the effect of botulinum toxin type A injections on quality of life and self-esteem. Dermatol Surg. 2010;36(suppl 4):2088–2097. doi:10.1111/j.1524-4725.2010.01795.x
14. Rivkin AZ, Ogilvie P, Dayan S, Yoelin SG, Weichman BM, Garcia JK. OnabotulinumtoxinA for simultaneous treatment of upper facial lines: subject-reported satisfaction and impact from a Phase 3 study. Dermatol Surg. 2020;46(1):50–60. doi:10.1097/DSS.0000000000001883
15. Dayan S, Coleman WP, Dover JS, et al. Effects of onabotulinumtoxinA treatment for crow’s feet lines on patient-reported outcomes. Dermatol Surg. 2015;41(suppl 1):S67–S74. doi:10.1097/DSS.0000000000000146
16. The Aesthetic Society. Aesthetic Plastic Surgery National Databank Statistics 2020–2021; 2022. Available from: https://cdn.theaestheticsociety.org/media/statistics/2021-TheAestheticSocietyStatistics.pdf.
17. Clancy CM, Eisenberg JM. Outcomes research: measuring the end results of health care. Science. 1998;282(5387):245–246. doi:10.1126/science.282.5387.245
18. Klassen AF, Cano SJ, Schwitzer JA, Scott AM, Pusic AL. FACE-Q scales for health-related quality of life, early life impact, satisfaction with outcomes, and decision to have treatment: development and validation. Plast Reconstr Surg. 2015;135(2):375–386. doi:10.1097/PRS.0000000000000895
19. Pompilus F, Burgess S, Hudgens S, Banderas B, Daniels S. Development and validation of a novel patient-reported treatment satisfaction measure for hyperfunctional facial lines: Facial Line Satisfaction Questionnaire. J Cosmet Dermatol. 2015;14(4):274–285. doi:10.1111/jocd.12166
20. Yaworsky A, Daniels S, Tully S, et al. The impact of upper facial lines and psychological impact of crow’s feet lines: content validation of the Facial Line Outcomes (FLO-11) Questionnaire. J Cosmet Dermatol. 2014;13(4):297–306. doi:10.1111/jocd.12117
21. Greenhalgh J. The applications of PROs in clinical practice: what are they, do they work, and why? Qual Life Res. 2009;18(1):115–123. doi:10.1007/s11136-008-9430-6
22. Narurkar V, Shamban A, Sissins P, Stonehouse A, Gallagher C. Facial treatment preferences in aesthetically aware women. Dermatol Surg. 2015;41(suppl 1):S153–S160. doi:10.1097/DSS.0000000000000293
23. De Boulle K, Furuyama N, Heydenrych I, et al. Considerations for the use of minimally invasive aesthetic procedures for facial remodeling in transgender individuals. Clin Cosmet Invest Dermatol. 2021;2021(14):513–525. doi:10.2147/CCID.S304032
24. Jagdeo J, Keaney T, Narurkar V, Kolodziejczyk J, Gallagher CJ. Facial treatment preferences among aesthetically oriented men. Dermatol Surg. 2016;42(10):1155–1163. doi:10.1097/DSS.0000000000000876
25. Alam M, Tung R. Injection technique in neurotoxins and fillers: planning and basic technique. J Am Acad Dermatol. 2018;79(3):407–419. doi:10.1016/j.jaad.2018.01.034
26. Nair AG, Santhanam A. Clinical photography for periorbital and facial aesthetic practice. J Cutan Aesthet Surg. 2016;9(2):115–121. doi:10.4103/0974-2077.184047
27. Humphrey S. Neurotoxins: evidence for prevention. J Drugs Dermatol. 2017;16(6):s87–s90.
28. Mobayed N, Nguyen JK, Jagdeo J. Minimally invasive facial cosmetic procedures for the millennial aesthetic patient. J Drugs Dermatol. 2020;19(1):100–103. doi:10.36849/JDD.2020.4641
29. Bonati LM, Fabi SG. Treating the young aesthetic patient: evidence-based recommendations. J Drugs Dermatol. 2017;16(6):s81–s83.
30. UK Department of Health and Social Care. Botulinum toxin and cosmetic fillers for under 18s; 2021. Available from: https://www.gov.uk/government/publications/botulinum-toxin-and-cosmetic-fillers-for-under-18s.
31. Carruthers J, Fagien S, Matarasso SL. Consensus recommendations on the use of botulinum toxin type a in facial aesthetics. Plast Reconstr Surg. 2004;114(6 suppl):1S–22S. doi:10.1097/01.PRS.0000144795.76040.D3
32. Hallett M. Explanation of timing of botulinum neurotoxin effects, onset and duration, and clinical ways of influencing them. Toxicon. 2015;107(Pt A):64–67. doi:10.1016/j.toxicon.2015.07.013
33. Flynn TC. Botulinum toxin: examining duration of effect in facial aesthetic applications. Am J Clin Dermatol. 2010;11(3):183–199. doi:10.2165/11530110-000000000-00000
34. Torres S, Hamilton M, Sanches E, Starovatova P, Gubanova E, Reshetnikova T. Neutralizing antibodies to botulinum neurotoxin type A in aesthetic medicine: five case reports. Clin Cosmet Invest Dermatol. 2014;7:11–17. doi:10.2147/CCID.S51938
35. Jankovic J, Carruthers J, Naumann M, et al. Neutralizing antibody formation with OnabotulinumtoxinA (BOTOX®) treatment from global registration studies across multiple indications: a meta-analysis. Toxins. 2023;15(5):342. doi:10.3390/toxins15050342
36. Cohen JL, Goodman GJ, De Almeida AT, et al. Decades of beauty: achieving aesthetic goals throughout the lifespan. J Cosmet Dermatol. 2023;22(11):2889–2901. doi:10.1111/jocd.15968
37. Fabi S, Alexiades M, Chatrath V, et al. Facial aesthetic priorities and concerns: a physician and patient perception global survey. Aesthet Surg J. 2022;42(4):NP218–NP229. doi:10.1093/asj/sjab358
38. Klassen AF, Cano SJ, Scott A, Snell L, Pusic AL. Measuring patient-reported outcomes in facial aesthetic patients: development of the FACE-Q. Facial Plast Surg. 2010;26(4):303–309. doi:10.1055/s-0030-1262313
39. Liew S, Silberberg M, Chantrey J. Understanding and treating different patient archetypes in aesthetic medicine. J Cosmet Dermatol. 2020;19(2):296–302. doi:10.1111/jocd.13227
40. Smit R, Gubanova E, Kaufman J, et al. Patient satisfaction with abobotulinumtoxinA for aesthetic use in the upper face: a systematic literature review and post-hoc analysis of the APPEAL study. J Clin Aesthet Dermatol. 2021;14(2):E69–E88.
41. Cohen JL, Scuderi N. Safety and patient satisfaction of abobotulinumtoxinA for aesthetic use: a systematic review. Aesthet Surg J. 2017;37(suppl 1):S32–S44. doi:10.1093/asj/sjx010
42. Nestor M, Ablon G, Pickett A. Key parameters for the use of abobotulinumtoxinA in aesthetics: onset and duration. Aesthet Surg J. 2017;37(suppl 1):S20–S31. doi:10.1093/asj/sjw282
43. Ching S, Thoma A, McCabe RE, Antony MM. Measuring outcomes in aesthetic surgery: a comprehensive review of the literature. Plast Reconstr Surg. 2003;111(1):469–480. doi:10.1097/00006534-200301000-00085
44. Kim WJ, Kumthornthip W, Oh BM, Yang EJ, Paik NJ. Feasibility of video clip analysis on effect of botulinum toxin-A injection for post-stroke upper limb spasticity. Toxins. 2013;5(5):983–991. doi:10.3390/toxins5050983
45. Wang J, Rieder EA. A systematic review of patient-reported outcomes for cosmetic indications of botulinum toxin treatment. Dermatol Surg. 2019;45(5):668–688. doi:10.1097/DSS.0000000000001878
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.