Back to Journals » Journal of Inflammation Research » Volume 18
The Pathological Link Between Elevated Markers of Inflammation, Endothelial Activation, and Cardiovascular Diseases in People Living with HIV on Combination Antiretroviral Therapy: A Systematic Review
Authors Mokoena H ![]() , Hanser S, Mabhida SE, Choshi J, Sekgala MD, Nkambule BB
, Hanser S, Mabhida SE, Choshi J, Sekgala MD, Nkambule BB ![]() , Mchiza ZJ, Ndwandwe DE, Kengne AP
, Mchiza ZJ, Ndwandwe DE, Kengne AP ![]() , Dludla PV
, Dludla PV
Received 9 April 2024
Accepted for publication 24 July 2024
Published 10 December 2025 Volume 2025:18 Pages 17197—17210
DOI https://doi.org/10.2147/JIR.S472896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Haskly Mokoena,1 Sidney Hanser,1 Sihle E Mabhida,2 Joel Choshi,1 Machoene D Sekgala,3 Bongani B Nkambule,4 Zandile J Mchiza,2,5 Duduzile E Ndwandwe,6 André P Kengne,2,7 Phiwayinkosi V Dludla6,8
1Department of Physiology and Environmental Health, University of Limpopo, Sovenga, 0727, South Africa; 2Non-Communicable Diseases Research Unit, South African Medical Research Council, Tygerberg, 7505, South Africa; 3Department of Social Sciences, Center for Social Sciences Research (CSSR), University of Cape Town, Robert Leslie Social Science Building 12 University Avenue, Cape Town 7701, South Africa; 4School of Laboratory Medicine and Medical Sciences, University of Kwazulu-Natal, Durban, 4000, South Africa; 5School of Public Health, University of the Western Cape, Bellville, 7535, South Africa; 6Cochrane South Africa, South African Medical Research Council, Tygerberg, 7505, South Africa; 7Department of Medicine, University of Cape Town, Cape Town, 7700, South Africa; 8Department of Biochemistry and Microbiology, University of Zululand, KwaDlangezwa, 3880, South Africa
Correspondence: Phiwayinkosi V Dludla, Cochrane South Africa, South African Medical Research Council, Tygerberg, 7505, South Africa, Tel +27 21 938 0333, Email [email protected]
Introduction: Despite administering combination antiretroviral therapy (cART), people living with the human immunodeficiency virus (PLWH) have been identified to be at an elevated risk of cardiovascular diseases (CVDs). Notably, inflammation and endothelial activation are likely factors associated with increased CVD risk in PLWH. Thus, the present study reviews evidence reporting on the potential link between increased markers of inflammatory, endothelial activation, and CVD risk in PLWH on cART.
Methodology: Web databases incorporating Cochrane libraries, PubMed, Web of Science, Google Scholar, and ScienceDirect were searched to identify suitable clinical research reports. The validity and reliability of the quality of the included evidence were appraised utilising the Downs and Black checklist.
Results: Fifteen clinical research reports were incorporated within the present study, involving PLWH on cART (n=7117). We classified these research reports based on short-term (≤ 12 months) and prolonged exposure (˃ 12 months) to cART of PLWH. Overwhelming results showed that short- and long-term exposure to cART are closely associated with elevated markers of inflammation that were consistent with the existence of endothelial activation in PLWH on cART. Prominent inflammatory markers, which were elevated included interleukin-6 (IL-6), high sensitivity C-reactive protein (hsCRP) and tumor necrosis factor alpha (TNF-α). While those indicating endothelial activation included soluble intercellular and vascular adhesion molecule-1 (sICAM-1 and sVCAM-1). The quality of included research reports was relatively high, while there was very limited information on the effect of the specific type of cART.
Conclusion: The current study supports the hypothesis indicating a close association between elevated inflammatory markers and endothelial activation potentially contributing to CVDs in PLWH on cART. However, these effects may be associated with prolonged exposure to cART in conjunction to specific cART-drug regimen combinations. Nonetheless, the available evidence is still very limited, and more research is needed to confirm these findings.
Keywords: inflammation, endothelial activation, combination antiretroviral therapy, human immunodeficiency virus
Introduction
The spread of the human immunodeficiency virus (HIV) continues to increase globally, with 39 million recorded cases to date. Consequently, only 29.8 million of people living with HIV (PLWH) globally are undergoing combination antiretroviral therapy (cART) which prolongs their lifespan.1,2 The increase in lifespan among PLWH is accompanied by the manifestation of cardiovascular diseases (CVDs), one of the major factors contributing to increased cases of mortality in PLWH.3,4 Emerging evidence indicates that the continued use of cART may be implicated in the manifestation of endothelial activation in PLWH.5,6 Endothelial activation is considered as one of the major predictors of CVDs and is characterized by sustained blood vessel constriction, which can subsequently lead to heart failure.7,8 Inflammation is the necessary process within the body to respond to an undesired stimulus, however exacerbation of this process may cause undesirable outcomes linked with endothelial dysregulation.9 Evidently, there is a close association between elevated inflammatory markers and increased risk of CVDs among PLWH,10 even independent of cART.11,12 However, such evidence remains to be fully understood, especially with the continued or effective use of cART among PLWH.
Several inflammatory markers including interleukin-6 (IL-6), cluster differentiation-14 (CD14), and high sensitivity C-reactive protein (hsCRP) are continuously deliberated on for their potential implication during the development of CVDs in PLWH.13,14 In fact, our recent review indicates that elevated circulating levels of hsCRP, together with abnormal lipid profiles, may potentially signal increased CVDs in PLWH on cART, in particular those within the African continent.15 However, there is still lack of literature reviewing the pathological involvement of a broad spectrum of inflammatory molecules incorporating tumor necrosis factor alpha (TNF-α) in conjunction to its receptors and monocyte chemoattractant protein-1 (MCP-1) during the development of cardiovascular complications in PLWH. This is essential since it has already been established that persistent levels of inflammation are implicated in the development of many diseases,16,17 beyond their role during the manifestation of endothelial activation in PLWH.18,19
Within a pathological state, endothelial activation may typically be marked by abnormally increased levels of soluble intercellular adhesion molecule-1 (sICAM-1), vascular adhesion molecule-1 (sVCAM-1), endothelial selectin (sE-selectin), and leukocyte selectin (sL-selectin) in PLWH.20,21 Interestingly, this state may persist despite viral suppression in PLWH.22 Thus, it remains essential to review this evidence to understand the potential physiopathology of increased inflammatory and endothelial activation markers in PLWH on cART. Evidence emitting from this systematic review remains essential to inform on relevant markers that could be essential for effective management of PLWH, especially reducing the risk of CVDs that may be linked with sustained exposure to cART-treatment.
Methodology
The present study was assembled following the Cochrane Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA), (Supplementary file 1). Additional guidance in assembling this systematic review was obtained from the updated Cochrane Handbook for Systematic Reviews of Interventions guidelines.23 It is worth noting that the protocol for the present study was not registered with the International Prospective Register for Systematic Reviews (PROSPERO). However, duplication of existing protocols was avoided by screening online registries including PROSPERO, Cochrane Collaboration, and Cochrane libraries for any similar work.
Search Strategy
To identify clinical research reports in line with achieving the aims and objectives of the present systematic review, a web database search on Cochrane libraries, PubMed, Web of Science, ScienceDirect, and Google Scholar was conducted, until the end of January 2024. The literature search was done by two independent authors, while consulting a librarian when formulating the search strategy (Supplementary file 2). Medical Subject Headings and key terms used on the web databases incorporated, “inflammation and endothelial activation in HIV”, and “respective inflammatory and endothelial activation markers in HIV”. We imposed restrictions on the year of publication to retrieve clinical research reports published in the last decade (from 2014 until January 2024), looking at any association between inflammation and endothelial activation, as a major predictor of CVDs, in PLWH.24,25
Eligibility Criteria
The principal objective of the present study was to establish a link between levels of inflammatory markers and indicators of endothelial function in PLWH on cART. The comparators were cART-naïve PLWH or HIV-negative persons. Included research reports were of varying designs ranging from pilot, cross-sectional, randomized controlled trials, and observational studies on adults (≥ 18-years-old) PLWH. Exclusions incorporated review articles, animal studies or literature not outlining markers of inflammation or endothelial function in PLWH on cART, or those reporting on participants with co-infections such as hepatitis virus, tuberculosis, AIDs, and the corona virus, or those with pre-existing CVD-risks such as hypertension, obesity, and diabetes at participant enrolment. The present systematic review was assembled to evaluate the following: Population, Exposure, Comparison, and Outcomes (PECO).
Population
Study population incorporates adult (≥ 18-years-old) PLWH on cART.
Exposure
Combination antiretroviral therapy (cART) exposed PLWH, with no restrictions on the type of cART regimen. Briefly, these incorporated (but not limited to) drug combinations of efavirenz (EFV), maraviroc (MVC), raltegravir tenofovir disoproxil fumarate (TDF), (RAL), rilpivirine (RPV), or emtricitabine (FTC).
Comparison
Research reports on cART-naïve PLWH or HIV-negative individuals.
Outcome/s
Makers/indicators of inflammation and endothelial function.
Data Extraction
Data extracted from research reports deemed eligible for inclusion was performed by two independent reviewers. This incorporated the authors’ name and publication year, region in which the study was conducted, study design, sample size of PLWH on cART, intervention (type of cART regimen), and the study’s’ key observations in line with our study objectives.
Quality Assessment
The Downs and Black Checklist consisting of twenty-seven (27) questions under five domains, namely reporting bias, internal validity, external validity, selection bias, and power was employed to judge the quality of evidence and risk of bias reported by each of the included research reports26 (Supplementary file 3). The quality of evidence and risk of bias for all the included research reports were evaluated using their full-text articles by two independent authors. Discords were resolved by discussions and taking counsel from an additional independent author. Upon reaching a consensus, rater agreement was determined using the Cohen’s Kappa (K)-value to confirm the validity and reliability of the rating. The K-value was calculated using the IBM Statistical Package for the Social Sciences (SPSS) version 29.0. Cohen’s Kappa rater agreements were classified in accordance with McHugh et al, (2012).27
Results
Characteristic Features of the Included Research Reports
Our web search strategy identified 911 research reports outlining the link between inflammation and endothelial activation in PLWH (Figure 1). After excluding research reports not meeting our eligibility criteria, only Fifteen (15) research reports remained to be included in the present study, making up a total of 7117 included participants (Figure 1). Majority of the incorporated research reports were conducted in the United States (n=7), followed by Italy (n=3). With Spain, the Netherlands, Ireland, Slovenia, and Uganda contributing one (n=1) study each. Briefly, participants had an average age of 48.79 years, predominantly male (n=73%) and of Caucasian ethnicity (64%). However, from the fifteen included research reports four failed to report on the ethnicity of their participants.
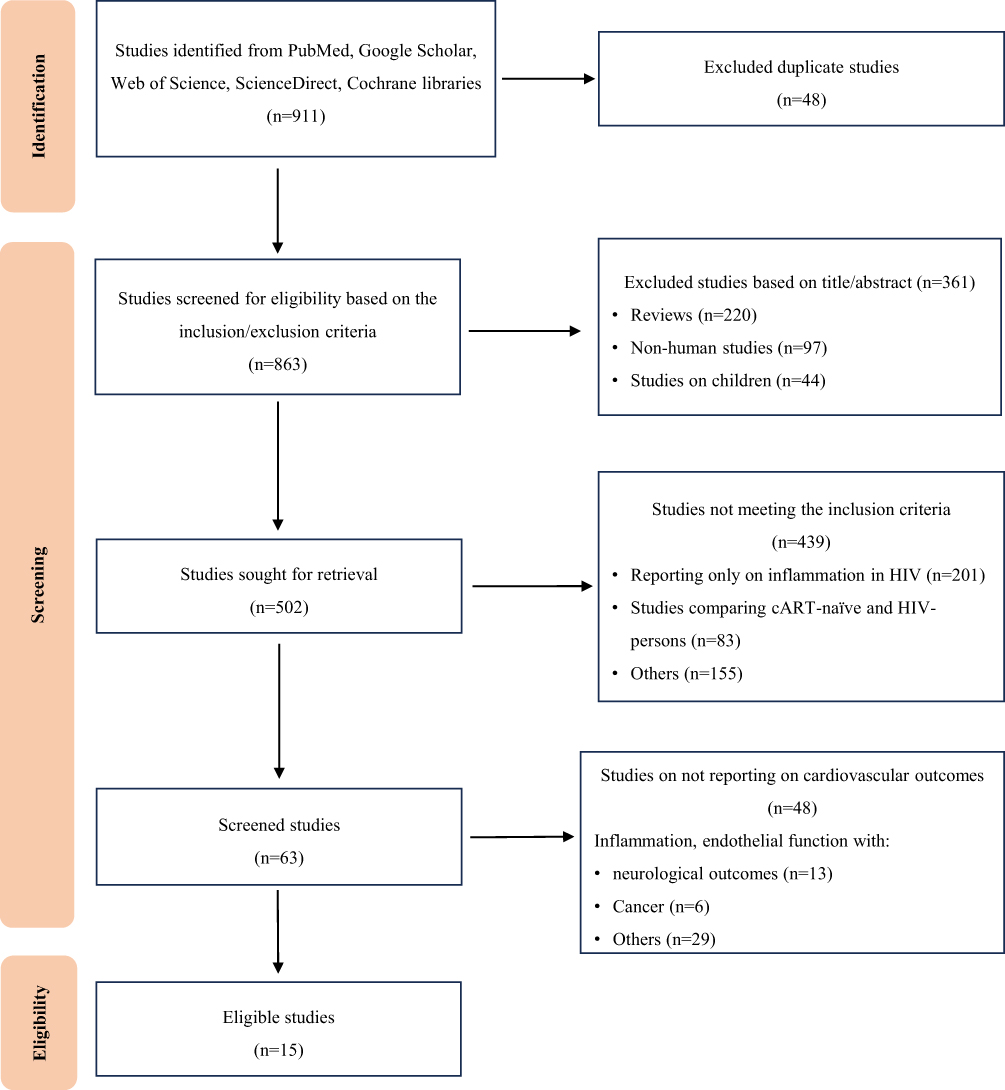 |
Figure 1 A PRISMA flow diagram depicting the study selection an inclusion process. Briefly, our structured search strategy identified a total of 911 research reports from PubMed, Google Scholar, Web of Science, ScienceDirect, and Cochrane libraries. After applying filters to eliminate duplicates, reviews, non-human, and child-health research reports, only 502 research reports were sought for retrieval. Out of the 502 research reports, only 15 research reports were deemed eligible for inclusion in the present systematic review, outlining the link between inflammation and endothelial activation in people living with HIV on combination antiretroviral therapy. |
Descriptive Analysis of Different Types and Duration of cART Regimen within Included Research Reports
Research reports included within this study addresses different cART classes, namely “integrase strand transfer inhibitors (INSTIs), chemokine receptor 5 (CCR5) inhibitors, nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors. (PIs)” 28,29 Apparently, four research reports reported on INSTIs, followed by PIs (n=2) and NRTIs (n=2), respectively. Other research reports reported on switching treatment from NRTIs or PIs to using INSTIs.14,30 Approximately 47% (n=7) of our included research reports did not disclose the cART regimen used by their enrolled participants. Majority (n=10) of the research reports addressed a cART-exposure duration ≤ 12 months (Table 1),14,30–38 while the remaining five (n=5) reported on a treatment exposure duration > 12 months (Table 2).39–43 Interestingly, an exposure duration > 12 months was associated with elevated inflammatory and endothelial activation markers.
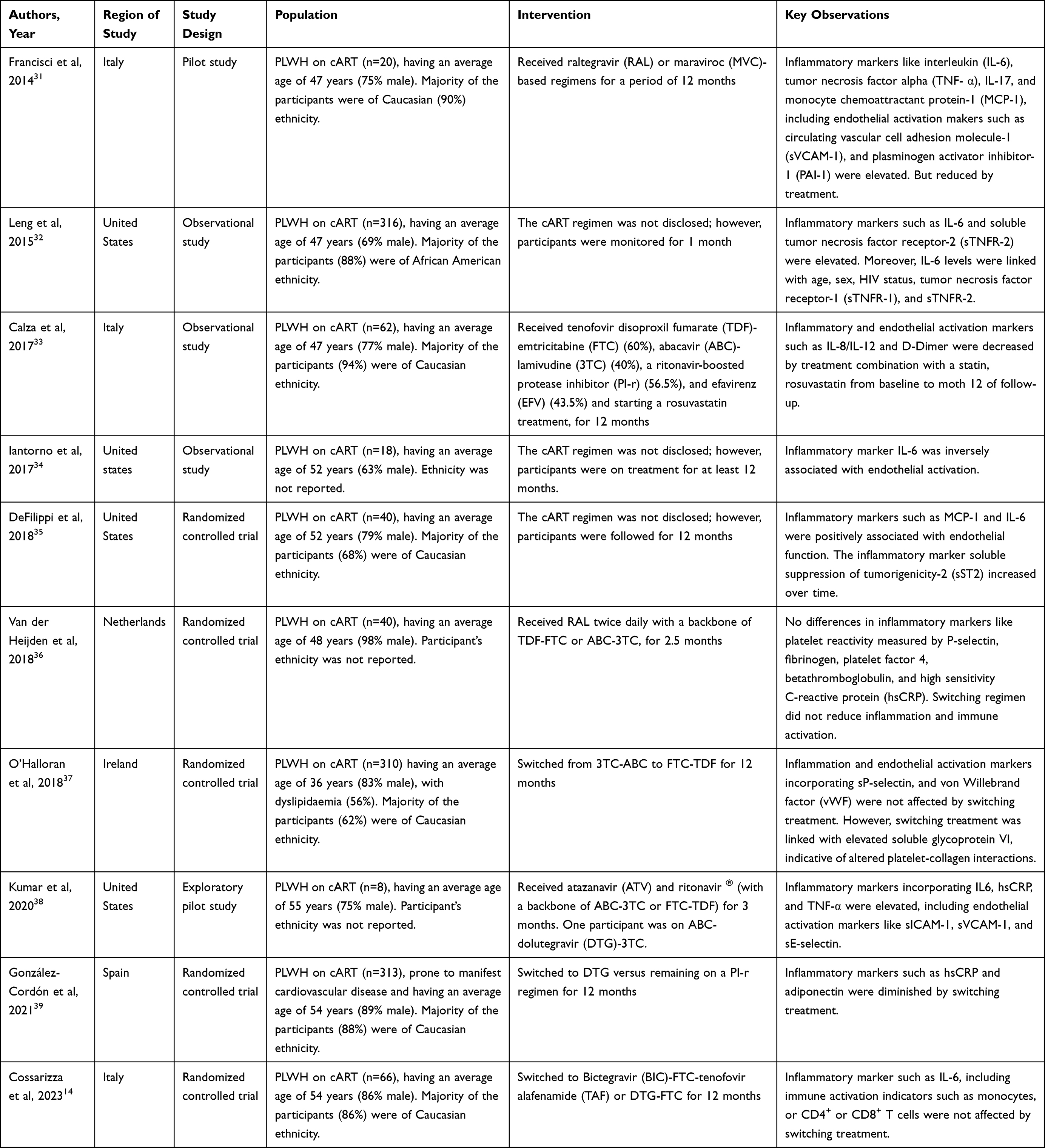 |
Table 1 An Abstract of Research Reports Outlining the Physio-Pathological Link Connecting Inflammation and Endothelial Activation in People Living with the Human Immunodeficiency Virus (PLWH) on Combination Antiretroviral Therapy (cART) for a Period Equal or Less Than 12 months |
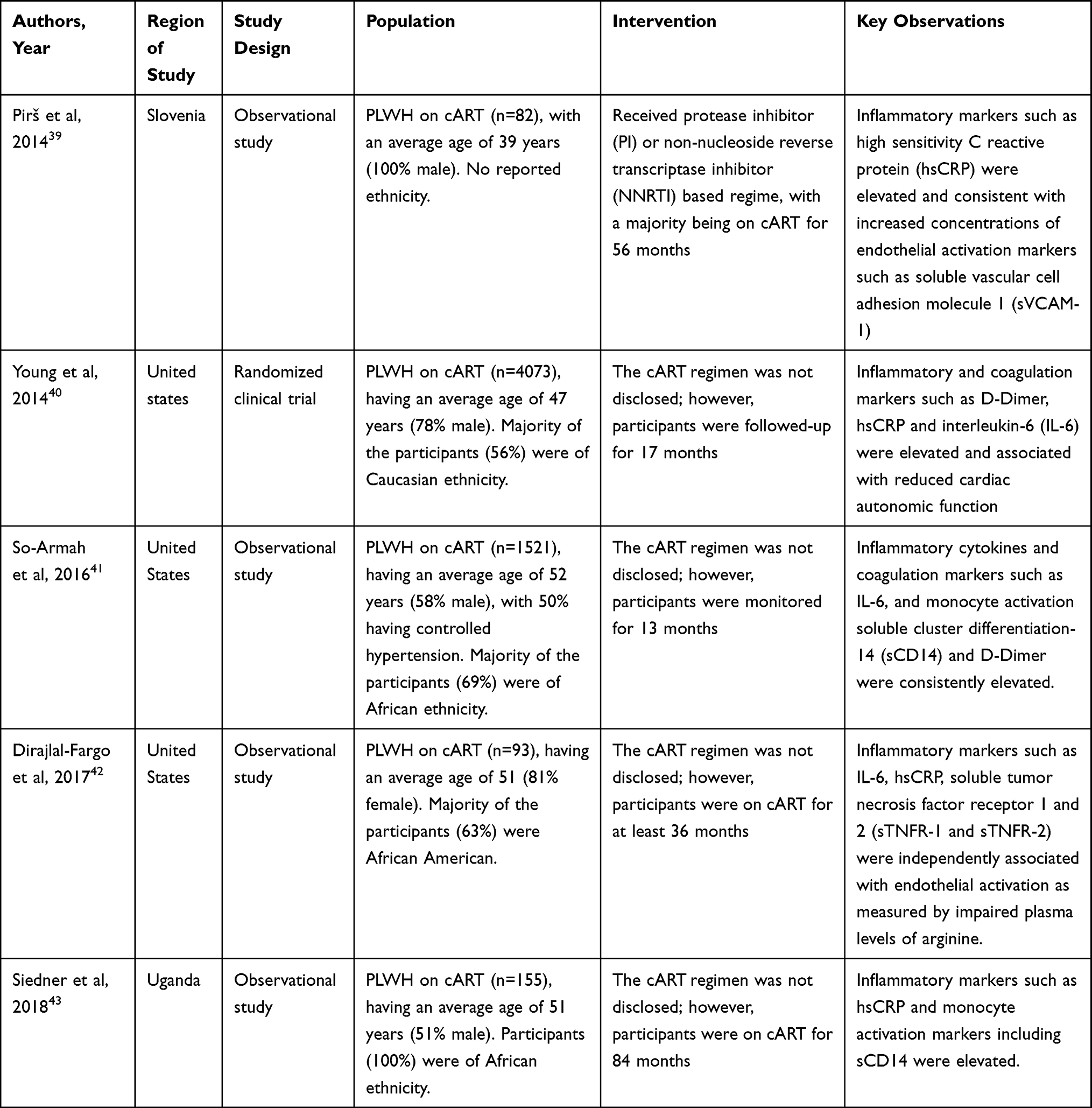 |
Table 2 An Abstract of Research Reports Outlining the Physio-Pathological Link Connecting Inflammation and Endothelial Activation in People Living with the Human Immunodeficiency Virus (PLWH) on Combination Antiretroviral Therapy (cART) for a Period Longer Than 12 months |
Quality of Evidence and Risk of Bias of the Included Research Reports
Two independent reviewers judged the quality of evidence and the risk of bias of the 15 included research reports employing the adjusted Downs and Black checklist (Supplementary file 4). Briefly, all the included research reports had an excellent quality of evidence after scoring at least 22 out of 27 possible points. Moreover, all the included research reports obtained an excellent reporting bias with a mean score of 10.73 (10–11) out of 11 points and a moderate rater agreement noted with a Cohen’s kappa (K)-value of 0.42. This included external validity with a mean score of 2.53 (2–3) out of 3 point and a moderate rater agreement of K= 0.42, and an internal validity with a mean score of 5.20 (5–7) out of 7 points and a good rater agreement of K=0.63. The selection bias of all the included research reports was classified as being fair with a mean score of 4.60 (4–6) out of 6 points and a fair rater agreement of K=0.21 (Supplementary file 4). Importantly, all the included research reports had a good reporting power ≥ 80.0% which is representative of no omission errors to their observations, as supported by a mean score of 0.80 (0–1) and K=0.76 (Supplementary file 4).
Short Term (≤ 12 Months) Effects of cART on Markers of Inflammation and Endothelial Activation in PLWH
Existing literature suggests that PLWH already present with sustained immune activation and chronic inflammation.44,45 That is, despite effective viral suppression with cART, chronic immune activation persists, likely due to ongoing low-levels of viral replication, microbial translocation, and co-infections.10,12 This persistent immune activation stimulates the production of pro-inflammatory cytokines such as IL-6, TNF-α, and IL-1β that are likely to contribute to the sustained activation of immune cells such as monocytes, neutrophils, and T-lymphocytes that may elevate CVD-risk.9,12 Indeed, this phenomenon can lead activation of reactive radicals and impairments on the vascular endothelium, likely causing increased CVD-risk.9–13 The resulting endothelial dysfunction not only compromises vascular integrity but also contributes to the increased cardiovascular risk observed in PLWH on cART.5,10,12
Nonetheless, the use of cART has been reported to induce positive effects in viral suppression, sometimes despite elevated levels of inflammation in PLWH.17,46 Thus, it has become empirical to decipher the effects of exposure to cART in PLWH, this includes short- and long-term effects. This is aligned with understanding the pathological link between elevated inflammatory and endothelial activation markers in PLWH on cART. Table 1 gives a synopsis of research reports outlining the potential link between raised makers of inflammation and endothelial activation in PLWH, exposed to cART for a short-term period of ≤ 12 months. Here, ten (n=10) of the incorporated research reports addressed the efficacy of various interventions, ranging from CCR-5 inhibitors such as MVC-based regimens, or combinations of NRTIs such as TDF-FTC, or abacavir (ABC)-lamivudine (3TC), and even ritonavir (RTV)-boosted PIs. Others were exposed to a combination therapy containing NNRTIs such as EFV, with other PLWH allowed to switch from 3TC-based therapy to INSTIs such as dolutegravir (DTG) or the NRTI tenofovir alafenamide (TAF) regiments (Table 1).
A systematic analysis of literature supports a strong correlation between raised markers of inflammation and sustained endothelial activation markers.32,35,38 Although such evidence does not appear to be dependent on the type of cART regimen, the results suggested that inflammatory markers like IL-6 and MCP-1 correlated with indicators of endothelial activation incorporating sICAM-1, sVCAM-1, and sE-selectin (Table 1). However, it was noted that other cART regimens, including RAL-MVC, TDF-FTC, or even the combined use of these drugs with a statin drug such as rosuvastatin could alleviate inflammation and improve endothelial function in PLWH.31,33,34 Some of the inflammatory and endothelial activation makers that were positively affected by treatment included IL-6, TNF-α, MCP-1, sVCAM-1, and plasminogen activator inhibitor-1 (PAI-1). However, from some included research reports it was apparent that some external factors like age, gender, and specific type of cART could influence markers of inflammation, together with endothelial function status in PLWH. For example, Leng et al showed that traditional risk factors of CVDs such as age and gender47,48 were associated with sustained inflammation status in PLWH.32 Further highlighting the importance of adjusting for external risk factors when reporting on the potential influence of cART on markers of inflammation or to determine the potential link with endothelial activation.
Markers of inflammation or those indicating endothelial activation were further evaluated in patients switching between different cART regimens (Table 1). For example, it was reported that switching to Bictegravir (BIC)-FTC-TAF containing cART treatment did not affect inflammatory marker such as IL-6 nor could it influence indicators of immune activation such as monocytes, or CD4+ or CD8+ T cells.14,37 While it was partially demonstrated that switching from 3TC-ABC to FTC-TDF therapy was associated with increased levels of soluble glycoprotein VI, an indicator of platelet-aggregation and immune activation marker.37 Similar findings are seen when administering RAL twice daily, together with a cART backbone consisting of TDF-FTC or ABC-3TC, for 2.5 months did not affect in inflammatory markers like platelet reactivity measured by sP-selectin, fibrinogen, platelet factor 4, betathromboglobulin, and hsCRP in PLWH.36 Although cART remains effective in suppressing the virus or improving the lives of PLWH,30 the current results show little or no evidence supporting the efficacy of cART in alleviating or diminishing markers of inflammation or endothelial activation in these PLWH.
Effects of Prolonged Exposure (˃ 12 Months) to cART on Inflammatory and Endothelial Activation Markers in PLWH
Evidence exists elucidating the potential role of raised inflammatory markers during the development of CVDs in PLWH, especially through long-term exposure to cART.34,39 Table 2 gives a synopsis of research reports outlining the potential link between inflammation and endothelial activation in PLWH exposed to cART for a prolonged period of ˃12 months. Here, the majority of included literature supports the close association between elevated markers of inflammation and endothelial activation in PLWH on cART. For example, it was reported that PLWH receiving PI or NNRTI based regime for 56 months presented with elevated levels of hsCRP, an inflammatory marker consistent with increased concentrations of endothelial activation indicator like sVCAM-1.39 Others did not specify the type of cART regimen but did show that prolonged exposure of PLWH to treatment was linked with elevated levels of inflammatory markers incorporating IL-6, sTNFR-1, and hsCRP, together with coagulation biomarkers like D-Dimer, and reduced cardiac autonomic function in PLLWH.40–42 To attain some level of immune activation within these patients, it was also demonstrated that exposure to cART for 84 months was linked with higher levels of monocyte activation (sCD14), corresponding to elevated pro-inflammatory (hsCRP) markers in PLWH.43 The available evidence remains debatable, motivating for future research reports on PLWH looking at prolonged cART exposure on inflammation and endothelial activation with specific focus on different cART-drug combinations.
Other Factors Potentially Enhancing Inflammation and Endothelial Activation in PLWH on cART
In people living with HIV, age and sex, particularly being male, play significant roles in exacerbating inflammatory and endothelial activation.14,39 Thus, with increasing age PLWH are more likely to experience heightened levels of chronic inflammation and immune activation, which can contribute to CVDs and other comorbidities.31,32 Nonetheless, our included evidence predominantly associates being male of >45-years-old and HIV-infected with sustained inflammation and endothelial activation.14,31,32,39 Leng et al, in a study predominately composed of males with an average age of 47 years, demonstrated that elevated inflammatory markers incorporating IL-6 were linked with age and sex.32 Similarly, two studies on 54-year-old males affirmed the probable link between old age elevated inflammatory markers.14,39 However, one of these studies further elaborated that administering INSTI-based cART may suppress inflammation in these persons.39 Thus, addressing these gender and age-specific risks is crucial in managing the long-term health of people living with HIV.
Discussion
It is now well accepted that many PLWH present with chronic inflammation and sustained immune activation despite administering cART.12,49 Thus, there is a lot of interest to understand the potential pathological connection between markers of inflammation or immune activation with the development of endothelial activation in PLWH on cART.12,50 Indeed, it has been of particular interest whether inflammation over short-term exposure to treatment is beneficial or perhaps prolonged exposure to cART could contribute to increased CVD-risk in PLWH. Here, we selected studies based on a systematic review approach, which provides a validated methodological approach to select studies and critically discuss them based on their common primary outcomes and covariances of CVDs, inflammation, and endothelial activation in PLWH on cART.
Starting with short-term exposure/treatment with cART (≤ 12 months), it was obvious that predominant markers of inflammation such as IL-6 and MCP-1 were correlated with indicators of endothelial activation such as sICAM-1, sVCAM-1, and sE-selectin (Table 1). Interestingly, both IL-6 and MCP-1 have been associated with the progression of HIV,51 while IL-6 is known to play an active role in activating peripheral blood mononuclear cells to initiate immune activation and could eventually lead to organ damage.52 Increased circulating levels of IL-6 have been reported to be associated with CVD-related events such as diminished cardiac autonomic function.40 In addition, circulating levels of IL-6 were also reported to have a positive association with GDF-15, a marker of cardiovascular function.35 These findings may potentially explain the increased risk of developing CVD-related complications in PLWH. Anyway, short-term exposure to cART was associated with elevated makers of endothelial activation such as sICAM-1 and sVCAM-1 in PLWH (Table 1).
It is important to decipher whether prolonged exposure to elevated inflammatory markers could have a profound effect in damaging the endothelium. Research already indicated that endothelial activation may develop due to enhanced adhesion molecules, which correspond to the detrimental effects of oxidative stress as well as activation of cytokine secretion.50,53 The systematic analysis of literature did show that prolonged exposure to cART (˃ 12 months) confirmed that elevated markers of inflammation, including sustained immune response are consistent with the existence of endothelial activation in PLWH (Table 2). Prolonged exposure to cART and its potential influence on the general health of PLWH is a well-investigated phenomenon. Although effective in maintaining lives of PLWH,54,55 many questions are raised on whether prolonged exposure to cART could potentially cause increased CVD-risk through enhanced indices of inflammation and endothelial activation.50 To supplement information on detrimental effects of sustained platelet activation,56 some of the findings within the current systematic review show that makers for monocyte activation such as sCD14 are indeed elevated in PLWH on cART. Even accumulative evidence has closely monitored the potential use of activated monocytes or immune activation markers as a therapeutic target to attenuate vascular inflammation and lower CVD-related complications in people with diverse medical conditions.57,58
Furthermore, the use of PI-r or NNRTIs such as EFV appears to be effective in maintaining immune response by diminishing inflammatory cytokines such as IL-6 and IL-12.33 Similarly, the use of INSTIs such DTG diminishes acute phase inflammatory proteins such as hsCRP more effectively when compared to PI-r regimen.30 This evidence requires confirmation on whether specific cART-drug classes hold beneficial outcomes in viral suppression subsequently diminishing inflammation, with INSTIs having the most effective drugs. Notably, research has indicated that switching treatment to DTG containing cART regimen may potentially influence inflammatory markers like IL-6 to influence CVD-related outcomes.14,59 Similarly, however, O’Halloran et al (2018)37 indicated that switching from 3TC-ABC to FTC-TDF containing cART regimen has no beneficial effects on improving inflammation or alleviating endothelial activation markers in PLWH, further opening avenues for more research to investigate the possible detrimental effects of the participant’s prior cART regimen.
There is also scarce evidence supporting an inverse association between elevated inflammatory markers and the development of endothelial activation in PLWH. For instance, Iantorno et al, (2017)34 who reported an inverse association between IL-6 and coronary endothelial function in PLWH. Thus, these observations may evocate that sustained inflammation and endothelial dysfunction in PLWH may be a result of age and sex predispositions. For instance, males infected with HIV, in particular, may face a greater risk of inflammation induced endothelial dysfunction compared to their female counterparts.32,55 This sex disparity may be due to differences in immune responses, and lifestyle factors that can impact the vascular system. Studies have shown that older men living with HIV exhibit increased markers of inflammation and impaired endothelial function,43,48 which can lead to a higher prevalence of cardiovascular complications. Notably, our reporting presents some bias in that the included studies predominantly consistent of male participants than their female counterparts. However, it remains ambiguous to assign such level of bias in influencing the outcomes of these studies because there is no evidence indicating a systematic under‐representation of females in clinical studies.60 Nonetheless, more evidence is required to clarify the role of inflammation during the pathogenesis of endothelial activation, in association with other prevailing markers and covariances of CVD in PLWH. This is essentially true to understand potential effects of specific cART regimen combinations.
Strengths and Limitations
This systematic review gives knowledge on the currently existing evidence reporting on the potential link between inflammation and endothelial activation following the manifestation of CVDs. To ensure quality, reliability, and minimum bias of our reporting, the included studies were selected based on a systematic review approach, which provides a validated methodological approach to select studies and critically discusses them based on their findings in relation to inflammation, endothelial activation, and CVDs. All the included research reports reported evidence of excellent quality and risk of bias as determined using the Downs and Black check list, making their research findings accurate and reliable. However, the present systematic review holds some limitations worth considering. Including the retrieval of a few research reports (n=15) reporting on the link between inflammation and cardiovascular outcomes. In addition, the diversity of these research reports hindered us from performing a meta-analysis. It is also important to note that the incorporated studies poorly dined the health status of their participants, which might have had HIV-linked co-infections with the capacity to influence inflammation and endothelial activation pathway. Consequently, influencing the outcomes of our reporting. Our extracted research reports predominately reported on males, which might have impacted the quality of their conclusions. It is also worth mentioning that the reported information by the included studies does not consider a broad spectrum of CVD-related outcomes which may predict CVD-risk in PLWH on cART.
Conclusion
The pathological role of HIV and cART in the manifestation of CVDs is poorly understood. The present review systematically identified and appraised clinical research reports addressing the potential pathological link between elevated markers of inflammation and the development of endothelial activation in PLWH on cART. This was further motivated by existing evidence that PLWH present with persisting inflammation that may be detrimental to cardiovascular health.12,61 Our findings highlight that cART exposure enhances immune activation leading to the constant expression of inflammatory markers which potentially contribute to increased CVD-risk via the pathogenesis of endothelial activation in PLWH. This may however be elucidated through various factors incorporating the cytotoxic effects of cART on cells, inducing inflammation and oxidative stress known to cause damage to the vascular wall.9,12 An additional factor that could aid in elucidating the persistent expression of inflammatory markers in the presence of long-term exposure to cART, is the ability of the virus to acclimatize to the inhibitory effects of the treatment.62,63 All these while taking into consideration individual differences in adhering and responding to cART, as well as HIV-linked co-infections, age, and sex predisposition. Nonetheless, more findings are required to confirm this, especially longitudinal research reports to bridge the gap on cART-mediated inflammation and closely related cardiovascular events.
Acknowledgments
The work reported herein was made possible through partial funding by the National Research Foundation (NRF), together with the research collaboration between Phiwayinkosi V. Dludla from the South African Medical Research Council (SAMRC) and Sidney Hanser from the University of Limpopo Department of Physiology and Environmental Health. Sihle E. Mabhida was partly funded by SAMRC through its division of Research Capacity Development (RCD) under the Intra-Mural Postdoctoral and doctoral Fellowship Programme from funds awarded by the South African Treasury. Joel Choshi was also partly funded by SAMRC through the RCD division, under the Internship Scholarship Programme. The content reported in this manuscript remains the sole responsibility of the authors and do not necessarily representative of the official views of our funders nor the respective institutions.
Author Contributions
All authors made a significant contribution to the work reported in this study, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Phiwayinkosi V. Dludla is partly funded by the National Research Foundation (NRF) (Grant numbers: 117829 and 141929307). Sidney Hanser is also funded by the NRF (Grant number: TTK2204082828). The content presented in the current review remains the sole responsibility of the authors and do not necessarily represent the official views of our sponsors.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Grand M, Bia D, Diaz A. Cardiovascular risk assessment in people living with HIV: a systematic review and meta-analysis of real-life data. Curr HIV Res. 2020;18(1):5–18. doi:10.2174/18734251MTAyoOTM05
2. Verstraeten R, Vos-Seda AG, Boateng D, et al. No evidence for an association of HIV and antiviral treatment with changes in framingham cardiovascular risk score in the ndlovu cohort study. J Am Heart Assoc. 2024;13(2):e029637. doi:10.1161/JAHA.123.029637
3. Gersh BJ, Sliwa K, Mayosi BM, Yusuf S. Novel therapeutic concepts the epidemic of cardiovascular disease in the developing world: global implications. Eur Heart J. 2010;31(6):642–648. doi:10.1093/eurheartj/ehq030
4. Swathy M, Saruladha K. A comparative study of classification and prediction of cardiovascular diseases (CVD) using machine learning and deep learning techniques. ICT Express. 2022;8(1):109–116. doi:10.1016/j.icte.2021.08.021
5. Marincowitz C, Genis A, Goswami N, De Boever P, Nawrot TS, Strijdom H. Vascular endothelial dysfunction in the wake of HIV and ART. FEBS J. 2019;286(7):1256–1270. doi:10.1111/febs.14657
6. Padayachee S, Govender N, Naicker T. Does CART dysregulate angiogenesis in HIV infected preeclampsia? Nigerian J Physiological Sci. 2022;37(1):29–34. doi:10.54548/njps.v36i2.4
7. Paulo M, Costa DE, Bonaventura D, Lunardi CN, Bendhack LM. Nitric oxide donors as potential drugs for the treatment of vascular diseases due to endothelium dysfunction. Curr Pharm Des. 2020;26(30):3748–3759. doi:10.2174/1381612826666200519114442
8. Ray A, Maharana KC, Meenakshi S, Singh S. Endothelial dysfunction and its relation in different disorders: recent update. Health Sci Rev. 2023;7:1–11. doi:10.1016/j.hsr.2023.100084
9. Panda P, Verma HK, Lakkakula S, et al. Biomarkers of oxidative stress tethered to cardiovascular diseases. Oxid Med Cell Longev. 2022;2022(1):9154295. doi:10.1155/2022/9154295
10. Islam RK, Donnelly E, Islam KN. Circulating hydrogen sulfide (H2S) and nitric oxide (NO) levels are significantly reduced in hiv patients concomitant with increased oxidative stress biomarkers. J Clin Med. 2021;10(19):4460. doi:10.3390/jcm10194460
11. Majonga ED, Yindom L, Hameiri-Bowen D, et al. Proinflammatory and cardiovascular biomarkers are associated with echocardiographic abnormalities in children with HIV taking antiretroviral therapy. AIDS. 2022;36(15):2129–2137. doi:10.1097/QAD.0000000000003368
12. Perkins MV, Joseph SB, Dittmer DP, Mackman N. Cardiovascular disease and thrombosis in HIV infection. Arteriosclerosis Thrombosis Vasc Biol. 2023;43(2):175–191. doi:10.1161/ATVBAHA.122.318232
13. Dirajlal-Fargo S, Funderburg N. HIV and cardiovascular disease: the role of inflammation. Curr Opin HIV AIDS. 2022;17(5):286–292. doi:10.1097/COH.0000000000000755
14. Cossarizza A, Cozzi-Lepri A, Mattioli M, et al. Evaluating immunological and inflammatory changes of treatment-experienced people living with HIV switching from first-line triple cART regimens to DTG/3TC vs. B/F/TAF: the DEBATE trial. Front Immunol. 2023;14:1279390. doi:10.3389/fimmu.2023.1279390
15. Mabhida SE, Mchiza ZJ, Mokgalaboni K, et al. High-sensitivity C-reactive protein among people living with HIV on highly active antiretroviral therapy: a systemic review and meta-analysis. BMC Infect Dis. 2024;24(1):160. doi:10.1186/s12879-024-09050-4
16. Mahlangu T, Dludla PV, Nyambuya TM, et al. A systematic review on the functional role of Th1/Th2 cytokines in type 2 diabetes and related metabolic complications. Cytokine. 2020;126:154892. doi:10.1016/j.cyto.2019.154892
17. Nyambuya TM, Dludla PV, Mxinwa V, Nkambule BB. The effect of successful antiretroviral therapy on immune activation and reconstitution in HIV infected adults: a systematic review and meta-analysis. AIDS Rev. 2020;23(1):1–12. doi:10.24875/AIDSRev.20000039
18. Lembas A, Załęski A, Peller M, Mikuła T, Wiercińska-Drapało A. Human immunodeficiency virus as a risk factor for cardiovascular disease. Cardiovasc Toxicol. 2023;24(1):1–14. doi:10.1007/s12012-023-09815-4
19. Nalado AM, Waziri B, Ismail A, et al. Prevalence and determinants of endothelial dysfunction among adults living with HIV in Northwest Nigeria. Global Heart. 2023;18(1):57. doi:10.5334/gh.1264
20. Vachiat A, Dix-Peek T, Duarte R, Manga P. Endothelial dysfunction in HIV-positive patients with acute coronary syndromes. Cardiovasc J Africa. 2020;31(2):58–64. doi:10.5830/CVJA-2019-040
21. Hanser S, Mphekgwana PM, Moraba MM, Erasmus L, van Staden M. Increased endothelial biomarkers are associated with HIV antiretroviral therapy and C-reactive protein among a African rural population in Limpopo Province, South Africa. Front Public Health. 2022;10:980754. doi:10.3389/fpubh.2022.980754
22. Nyambuya TM, Dludla PV, Mxinwa V, Nkambule BB. T-cell activation and cardiovascular risk in adults with type 2 diabetes mellitus: a systematic review and meta-analysis. Clin Immunol. 2020;210:108313. doi:10.1016/j.clim.2019.108313
23. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3. 2022. Available from. www.training.cochrane.org/handbook.
24. Little PJ, Askew CD, Xu S, Kamato D. Endothelial dysfunction and cardiovascular disease: history and analysis of the clinical utility of the relationship. Biomedicines. 2021;9(6):699. doi:10.3390/biomedicines9060699
25. Benincasa G, Coscioni E, Napoli C. Cardiovascular risk factors and molecular routes underlying endothelial dysfunction: novel opportunities for primary prevention. Biochem Pharmacol. 2022;202:1–15. doi:10.1016/j.bcp.2022.115108
26. O’Connor SR, Tully MA, Ryan B, Bradley JM, Baxter GD, McDonough SM. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: a comparison study. BMC Res Notes. 2015;8(1):224. doi:10.1186/s13104-015-1181-1
27. McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. 2012;22:276–282. doi:10.11613/BM.2012.031
28. Eggleton JS, Nagalli S. Highly active antiretroviral therapy (CART). In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from https://www.ncbi.nlm.nih.gov/books/NBK554533/.
29. Ifeyinwa E, Obiechefu MC, Adnan M, et al. The imbalance of body electrolytes in HIV patients using highly active antiretroviral therapy. Children. 2023;5:100.
30. González-Cordón A, Assoumou L, Moyle G, et al. Switching from boosted Pis to dolutegravir decreases soluble CD14 and adiponectin in high cardiovascular risk people living with HIV. J Antimicrob Chemother. 2021;76(9):2380–2393. doi:10.1093/jac/dkab158
31. Francisci D, Falcinelli E, Baroncelli S, et al. Potential anti-inflammatory effects of maraviroc in HIV-positive patients: a pilot study of inflammation, endothelial dysfunction, and coagulation markers. Scand J Infect Dis. 2014;46(6):466–470. doi:10.3109/00365548.2014.898332
32. Leng SX, Dandorf S, Li H, et al. Associations of circulating soluble tumor necrosis factor-α receptors 1 and 2 with interleukin-6 levels in an aging cohort of injection drug users with or at high risk for HIV infection. AIDS Res Hum Retroviruses. 2015;31(12):1257–1264. doi:10.1089/aid.2015.0134
33. Calza L, Colangeli V, Magistrelli E, et al. Significant decrease in plasma levels of D-dimer, interleukin-8, and interleukin-12 after a 12-month treatment with rosuvastatin in HIV-infected patients under antiretroviral therapy. AIDS Res Hum Retroviruses. 2017;33(2):126–132. doi:10.1089/aid.2016.0134
34. Iantorno M, Schär M, Soleimanifard S, et al. Coronary artery endothelial dysfunction is present in HIV-positive individuals without significant coronary artery disease. AIDS. 2017;31(9):1281–1289. doi:10.1097/QAD.0000000000001469
35. deFilippi C, Christenson R, Joyce J, et al. Brief report: statin effects on myocardial fibrosis markers in people living with HIV. J Acquired Immune Deficiency Syndromes. 2018;78(1):105–110. doi:10.1097/QAI.0000000000001644
36. van der Heijden WA, van Crevel R, de Groot PG, et al. A switch to a raltegravir containing regimen does not lower platelet reactivity in HIV-infected individuals. AIDS. 2018;32(17):2469–2475. doi:10.1097/QAD.0000000000001993
37. O’Halloran JA, Dunne E, Tinago W, Denieffe S, Kenny D, Mallon PWG. Switching from Abacavir to tenofovir disoproxil fumarate is associated with rises in soluble glycoprotein VI, suggesting changes in platelet-collagen interactions. AIDS. 2018;32(7):861–866. doi:10.1097/QAD.0000000000001783
38. Kumar P, Liu C, Suliburk JW, et al. Supplementing glycine and N-acetylcysteine (GlyNAC) in aging HIV patients improves oxidative stress, mitochondrial dysfunction, inflammation, endothelial dysfunction, insulin resistance, genotoxicity, strength, and cognition: results of an open-label clinical trial. Biomedicines. 2020;8(10):390. doi:10.3390/biomedicines8100390
39. Pirš M, Jug B, Eržen B, et al. Relationship between markers of endothelial dysfunction and inflammation and subclinical atherosclerosis in HIV-infected male patients below 55 years of age. Acta Dermatovenerol Alp Pannonica Adriat. 2014;23(3):49–52. doi:10.15570/actaapa.2014.12
40. Young LC, Roediger MP, Grandits G, et al. Relationship between inflammatory and coagulation biomarkers and cardiac autonomic function in HIV-infected individuals. Biomarkers Med. 2014;8(9):1073–1083. doi:10.2217/bmm.14.27
41. VACS Project Team; So-Armah KA, Tate JP, Chang CH, et al. Do biomarkers of inflammation, monocyte activation, and altered coagulation explain excess mortality between HIV infected and uninfected people? J Acquired Immune Deficiency Syndromes. 2016;72(2):206–213. doi:10.1097/QAI.0000000000000954
42. Dirajlal-Fargo S, Alam K, Sattar A, et al. Comprehensive assessment of the arginine pathway and its relationship to inflammation in HIV. AIDS. 2017;31(4):533–537. doi:10.1097/QAD.0000000000001363
43. Siedner MJ, Zanni M, Tracy RP, et al. Increased systemic inflammation and gut permeability among women with treated HIV infection in rural Uganda. J Infect Dis. 2018;218(6):922–926. doi:10.1093/infdis/jiy244
44. Mazzuti L, Turriziani O, Mezzaroma I. The many faces of immune activation in HIV-1 infection: a multifactorial interconnection. Biomedicines. 2023;11(1):159. doi:10.3390/biomedicines11010159
45. Singh K, Natarajan V, Dewar R, et al. Prolonged persistence of transcriptionally active ‘defective’ HIV-1 proviruses: implications for persistent immune activation during antiretroviral therapy. Aids. 2023;37(14):2119–2130. doi:10.1097/QAD.0000000000003667
46. Mutuma B, Omedo R, Wafula P, et al. Hepatic function and its association with clinical outcomes in non-adherent HIV-1 adults. Afro-Egyptian J Infect Endemic Dis. 2023;13:146–156.
47. Bots SH, Peters SAE, Woodward M. Sex differences in coronary heart disease and stroke mortality: a global assessment of the effect of ageing between 1980 and 2010. BMJ Global Health. 2017;2(2):1–8. doi:10.1136/bmjgh-2017-000298
48. Wahabi H, Esmaeil S, Zeidan R, Fayed A. Effects of age, metabolic and socioeconomic factors on cardiovascular risk among Saudi women: a subgroup analysis from the heart health promotion study. Medicina. 2023;59(3):623. doi:10.3390/medicina59030623
49. Taglieri N, Bonfiglioli R, Bon I, et al. Pattern of arterial inflammation and inflammatory markers in people living with HIV compared with uninfected people. J Nucl Cardiol. 2022;29(4):1566–1575. doi:10.1007/s12350-020-02522-5
50. Mokoena H, Mabhida SE, Choshi J, et al. Endothelial dysfunction and cardiovascular diseases in people living with HIV on specific highly active antiretroviral therapy regimen: a systematic review of clinical research reports. Atherosclerosis Plus. 2024;55:47–54. doi:10.1016/j.athplu.2024.01.003
51. Ngcobo S, Molatlhegi RP, Osman F, et al. Pre-infection plasma cytokines and chemokines as predictors of HIV disease progression. Sci Rep. 2022;12(1):2437. doi:10.1038/s41598-022-06532-w
52. Biswas P, Delfanti F, Bernasconi S, et al. Interleukin-6 induces monocyte chemotactic protein-1 in peripheral blood mononuclear cells and in the U937 cell line. Blood. 1998;91(1):258–265. doi:10.1182/blood.V91.1.258
53. Ye H, Liu Q, Wang Y, Zhen X, Yan N. The effect of cholesterol efflux on endothelial dysfunction caused by oxidative stress. Int J Mol Sci. 2023;24(6):5939. doi:10.3390/ijms24065939
54. Spanish Group of Paediatric HIV Infection; Resino S, Resino R, Micheloud D, et al. Prolonged effects of highly active antiretroviral therapy in pretreated, vertically HIV type 1-infected children: 6 years of follow-up. Clin Infect Dis. 2006;42(6):862–869. doi:10.1086/500412
55. Nittayananta W, Talungchit S, Jaruratanasirikul S, et al. Effects of prolonged use of CART on oral health status of HIV-infected subjects. J Oral Pathol Med. 2010;39(5):397–406. doi:10.1111/j.1600-0714.2009.00875.x
56. Mesquita EC, Hottz ED, Amancio RT, et al. Persistent platelet activation and apoptosis in virologically suppressed HIV-infected individuals. Sci Rep. 2018;8(1):14999. doi:10.1038/s41598-018-33403-0
57. Ngcobo SR, Nkambule BB, Nyambuya TM, et al. Activated monocytes as a therapeutic target to attenuate vascular inflammation and lower cardiovascular disease-risk in patients with type 2 diabetes: a systematic review of preclinical and clinical research reports. Biomed Pharmacother. 2022;146:112579. doi:10.1016/j.biopha.2021.112579
58. Mokgalaboni K, Dludla PV, Nyambuya TM, Yakobi SH, Mxinwa V, Nkambule BB. Monocyte-mediated inflammation and cardiovascular risk factors in type 2 diabetes mellitus: a systematic review and meta-analysis of pre-clinical and clinical research reports. JRSM Cardiovasc Dis. 2020;9:2048004019900748. doi:10.1177/2048004019900748
59. WHO (World Health Organization). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. 2016. Available from: https://iris.who.int/bitstream/handle/10665/208825/9789241549684_eng.pdf?sequence=1.
60. Labots G, Jones A, de Visser SJ, Rissmann R, Burggraaf J. Gender differences in clinical registration trials: is there a real problem? Br J Clin Pharmacol. 2018;84(4):700–707. doi:10.1111/bcp.13497
61. Bloch M, John M, Smith D, Rasmussen TA, Wright E. Managing HIV‐associated inflammation and ageing in the era of modern ART. HIV Med. 2020;21(S3):2–16. doi:10.1111/hiv.12952
62. Nastri BM, Pagliano P, Zannella C, et al. HIV and drug-resistant subtypes. Microorganisms. 2023;11(1):221. doi:10.3390/microorganisms11010221
63. Ndashimye E, Avino M, Olabode AS, et al. Accumulation of integrase strand transfer inhibitor resistance mutations confers high-level resistance to dolutegravir in non-B subtype HIV-1 strains from patients failing raltegravir in Uganda. J Antimicrob Chemother. 2020;75(12):3525–3533. doi:10.1093/jac/dkaa355
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.